
Abstract
The World Health Organization identifies adolescent girls as particularly prone to anaemia due to reproductive changes, with challenges being more pronounced in India’s ‘Aspirational Districts’ (ADs), which suffer from poor education and health. The study examines the prevalence of anaemia among adolescent girls in ADs and identifies associated determinants from 2015 to 2021. Data from the National Family Health Survey (NFHS)-4 and NFHS-5, covering 21,637 and 19,879 adolescent girls aged 15–19 in ADs, were analyzed. Multivariable logistic regression was used to identify the determinants of anaemia among adolescents. The results show a notable increase in anaemia among adolescent girls in ADs, where anaemia rates have climbed from 58.3% to 62.4%, surpassing the national average rise. Over this period, more than 65% of ADs saw an uptick in anaemia prevalence, affecting 75 out of 112 districts. Specifically, Barpeta in Assam recorded the highest increase in anaemia prevalence at 45.1% points, while Haridwar in Uttarakhand reported a decrease of 25.8% points. Additionally, anaemia prevalence was found higher among girls with higher parity, Muslim girls, and those from poorer households. Pooled regression revealed that adolescent girls with a higher number of children (AOR: 1.29), formerly married (AOR: 1.57), Scheduled Tribe (ST) girls (AOR: 1.44), and girls with amenorrhoea (AOR: 1.57) were highly associated with anaemia. Specialized healthcare and nutrition programs for adolescent girls, similar to those for pregnant women in ADs, are crucial. Focusing on formerly married girls, ST girls, and those with amenorrhoea will enhance access to health resources, reduce anaemia rates, and improve overall well-being.
Similar content being viewed by others
Introduction
Anaemia, in simpler terms, is a condition marked by a decreased amount of hemoglobin (the red pigment of blood that carries oxygen) in the blood (World Health Organization, 2017). Due to iron deficiency in the diet, the number of hemoglobin molecules reduces, resulting in thinner, less red blood and a reduced supply of oxygen to various parts of the body (Sachdev et al. 2021; WHO, 2018). Adolescence is the second most critical stage of development, marking the transition from childhood to adulthood. Due to changing nutritional needs, adolescents, especially girls, are vulnerable to nutritional deficiencies and malnutrition (Casey et al. 2010; Elder and Ransom, 2003).
Among adolescent girls, anaemia is diagnosed when hemoglobin levels fall below 12 grams per deciliter (g/dL) (WHO, 2018; World Health Organization, 2017). The World Health Organization (WHO) has reported that more than 50% of adolescent girls are anaemic in Southeast Asia (Gardner et al. 2023; World Health Organization, 2017). In India, anaemia is even more concerning. The latest National Family Health Survey (NFHS-5) reported an increase in anaemia prevalence among women in India, rising from 53% in 2015–16 to 57% in 2019–21 (IIPS and ICF, 2017, 2019). However, among adolescent women, this rate rose from 55.8% to 59.1% during the same period, underscoring a significant public health challenge (Chakrabarty et al. 2023). A study conducted in India using NFHS data found that 47.5% of adolescent girls had anaemia, compared to only 18.3% of adolescent boys (Chakrabarty et al. 2023; Sachdev et al. 2021). Furthermore, a study based on the Comprehensive National Nutrition Survey previously reported that anaemia affected 40% of Indian adolescent girls, with its prevalence in Aspirational Districts (ADs) surpassing the national average (Chauhan et al. 2022; Let et al. 2024; Scott et al. 2022).
Earlier studies on anaemia, both in India and globally, have shown that several factors contribute to its prevalence among adolescent girls. During periods of rapid growth, adolescents require more iron; however, many do not consume sufficient iron-rich foods (Sharma et al. 2018; World Health Organization, 2017). Social issues such as early marriage and adolescent pregnancy also play a role (Aikawa et al. 2006; Arabyat et al. 2019; Mog et al. 2023). Additionally, factors such as low economic status, limited educational opportunities, higher rates of childbearing, residence in rural areas, inadequate dietary intake, and lack of exposure to mass media significantly influence anaemia status (Ahankari et al. 2017; Let et al. 2024; Mistry et al. 2017; Srivastava et al. 2022; Sunuwar et al. 2023; World Health Organization, 2017; Yang et al. 2023). These vulnerabilities are worsened by the onset of menstruation and the potential for pregnancy, both of which increase the need for iron (World Health Organisation, n.d.-a).
The importance of examining anaemia in ADs is highlighted by its association with low economic status and limited educational attainment, which are prevalent in these districts. The government of India launched the “Aspirational Districts Programme” (ADP) in 2018, which identified 112 least developed districts in the country (NITI Aayog, 2018; United Nations Development Program, 2020). These districts were selected based on a composite index that considers factors such as high poverty levels, poor health and nutritional outcomes, low educational attainment, and inadequate infrastructure, contributing to a cycle of disadvantage (NITI Aayog, 2018; Porter et al. 2018; Puri, 2020; United Nations Development Program, 2020). Furthermore, anaemia prevalence among women in ADs is notably higher than the national average, making it a critical public health issue, particularly for adolescent girls (Let et al. 2024). The socio-economic challenges in these districts—such as poor access to healthcare, inadequate nutrition, and limited educational opportunities—exacerbate the vulnerability of adolescent girls to anaemia (Centre for Social and Behaviour Change, A. U., 2022; Gardner et al. 2023; Let et al. 2024; NITI Aayog, 2018; Puri, 2020).
To give a thorough understanding of anaemia trends in ADs, both NFHS-4 and NFHS-5 were utilized. The NFHS-4 data reflect the situation in these districts before the launch of the ADs programme in 2018, as these districts were not yet designated as aspirational at that time. In contrast, the NFHS-5 data capture the conditions after the programme’s implementation, providing a comparison point to assess the impact of the programme. By analyzing the change over time, we can evaluate how much progress has been made in addressing anaemia in these districts and identify areas where further efforts are needed. This approach helps us understand both the current status of anaemia and the effectiveness of policies aimed at improving health outcomes in ADs.
Therefore, our study aims to identify the vulnerable subgroups of adolescent girls with anaemia in the ADs of India. Additionally, we analyzed district-wise changes in anaemia prevalence from 2015–16 to 2019–21 within these districts and identified determinants of anaemia. By identifying districts with the highest and lowest prevalence rates, as well as the changes over time, this study will provide policymakers with essential insights for effectively targeting areas most impacted by anaemia. These insights can help optimize resource distribution, facilitating targeted interventions that address the unique needs of each district. For instance, districts with high prevalence rates may benefit from focused nutritional programs and health education initiatives that address local risk factors. Furthermore, our investigation into the associated determinants enhances the understanding of the key factors influencing anaemia prevalence, which can inform national and district-level policy formulation.
Methods
Data source
This study uses data from NFHS-4 (2015–16) and NFHS-5 (2019–21), conducted by Ministry of Health and Family Welfare and The International Institute for Population Sciences, using a two-stage stratified sampling method (IIPS and ICF, 2017, 2019). The NFHS-4 collected information from 699,686 women, while NFHS-5 expanded its sample to 724,116 women aged 15–49 years. The surveys also covered around 572,000 and 636,669 households, respectively.
Study sample
In total, 112 districts across 27 Indian states were designated as ADs (NITI Aayog, 2018).
For our study, we focused on girls aged 15–19 years from 112 ADs with complete data on anaemia. From the initial dataset of 699,686 observations in NFHS-4, we excluded 574,808 observations of women aged 20–49 years, and an additional 103,241 observations were removed due to being from non-aspirational districts or having missing data on independent variables. Similarly, from the 724,115 observations in NFHS-5, we excluded 601,635 observations of women aged 20–49 years, and 102,601 observations were removed for being from non-aspirational districts or having missing data on independent variables. As a result, the final sample included 21,637 adolescent girls from NFHS-4 and 19,879 from NFHS-5.
Dependent variable
This study’s dependent variable measured the presence or absence of anaemia among the adolescent girls. The NFHS classified anaemia into four categories recommended by the WHO, no anaemia, mild anaemia (hemoglobin level 10.0–11.9 g/dl), moderate anaemia (hemoglobin level 7.0–10.9 g/dl), and severe anaemia (hemoglobin level less than 7.0 g/dl) (WHO, 2018). The study variable was dichotomous: ‘1’ indicated “anaemic” (if any adolescent girl had mild, moderate, or severe anaemia), and ‘0’ indicated “not anaemic.”
Independent variables
The independent variables were identified through review of existing literature on anaemia in various countries, including India (Ahankari et al. 2017; Balarajan et al. 2013; Chakrabarty et al. 2023; Let et al. 2024, 2025; Sachdev et al. 2021; Srivastava et al. 2022; Sunuwar et al. 2023; Wiafe et al. 2023; Yang et al. 2023). The independent variables included marital status which was categorized as currently married, not married, or formerly married. Parity, indicating the total number of children ever born, was classified into three groups: no children, one to two children, and three to four children. Both breastfeeding and pregnancy statuses were dichotomized as not breastfeeding or breastfeeding, and not pregnant or pregnant, respectively. Education level was classified into four categories: no education, primary, secondary, and higher education. Social groups were categorized into four groups: Scheduled Castes (SC), Scheduled Tribes (ST), Other Backward Classes (OBC), and the general category (Others) (also referred to as General, which includes individuals not belonging to SC, ST, or OBC groups). Religion was classified into four groups: Hindu, Muslim, Christian, and Others, which included individuals identifying as Sikh, Buddhist/Neo-Buddhist, Jain, Jewish, Parsi/Zoroastrian, or those with no religious affiliation. Household wealth was divided into five tiers: poorest, poorer, middle, richer, and richest. Residential location was categorized as either urban or rural. Mass media exposure was assessed across four levels: no exposure, low, medium, and high exposure. The frequency of egg, fish, and chicken consumption variables were each categorized as never, occasionally, and frequently. Alcohol consumption (yes/no) was based on a self-report of drinking alcohol. Body Mass Index (BMI) was classified based on WHO guidelines into the following categories: underweight (<18.5 kg/m²), normal weight (18.5–24.9 kg/m²), overweight (25.0–29.9 kg/m²), and obese (≥30.0 kg/m²) (World Health Organization, 2016). Additionally, the variables indicating current diabetes status and amenorrhoea were categorized as yes or no, respectively. Noteworthy, the variable “currently having diabetes” in this study is based on self-reported diabetes. Diabetes was categorized into two categories: ‘no’ (coded as 0) if the woman didn’t have diabetes, and ‘yes’ (coded as 1) if the woman had diabetes.
Statistical analysis
Bivariate analysis was conducted to examine the prevalence of anaemia among adolescent girls across different background characteristics. Chi-squared tests were utilized to assess the statistical significance of the relationships between each independent variable and the outcome variable (Chen and Chen, 2010). Furthermore, data from NFHS-4 and NFHS-5 were combined, and multivariable binary logistic regression was employed to evaluate the independent effects of various determinants on anaemia using the pooled dataset (Mertler et al. 2021).
Prior to performing multivariable logistic regression, we computed unadjusted odds ratios (UORs) with 95% confidence intervals (CIs) to assess the individual relationships between each independent variable and anaemia status. Only variables with significant associations were included in the final model to ensure relevance. Logistic regression results were presented as adjusted odds ratios (AOR), with p-values (p < 0.05) and 95% CIs. To check multicollinearity among independent variables variance inflation factors (VIFs) were used, confirming that VIFs were below 5 (Midi et al. 2010) (see appendix file 1). Model fit was evaluated using Nagelkerke’s R-square and the Hosmer-Lemeshow test (Hosmer and Stanley, 2007). The selection of the model was based on the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), and log-likelihood values (Weiß and Markus, 2011). Statistical analyses were performed using Stata 16, applying the ‘svyset’ command to account for NFHS-4 and NFHS-5’s complex survey design and sampling weights (StataCorp, 2017).
Results
Respondents’ characteristics
Table 1 revealed, that over 80% of adolescent girls were not married, and more than 90% had no children. Similarly, more than 90% were neither breastfeeding nor pregnant. In terms of education, a significant majority, over 75%, had attained secondary education and only a minuscule portion had higher education. Additionally, half of the adolescent girls belonged to OBC, and more than 80% identified as Hindu. Socioeconomic status was skewed towards the lower end, with over one-third of the adolescent girls falling into the lowest socioeconomic class. Only a small proportion living in urban areas in both survey rounds. Furthermore, dietary habits showed that one-third of adolescent girls occasionally consumed eggs, fish, and chicken.
Changes in anaemia among adolescent girls in ADs of India from 2015 to 2021
Figure 1 illustrates the prevalence of anaemia among adolescent girls aged 15–19 across India, ADs, and remaining districts, in NFHS-4 and NFHS-5. Nationally, anaemia among adolescent girls increased from 54.1% in NFHS-4 to 59.1% in NFHS-5. However, in ADs, the prevalence rose more sharply from 58.3% to 62.4%. In contrast, the remaining districts saw a smaller increase, from 53.5% to 58.6%. This comparison highlights that ADs not only had higher initial levels of anaemia but also experienced a steeper rise compared to other districts and the national average.

The left stack of bars represents anaemia across India, the middle stack represents anaemia in Aspirational Districts, and the right stack represents anaemia in remaining districts.
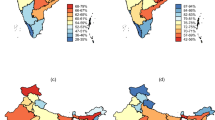
Anaemia among adolescent girls in ADs of India has shown notable changes from NFHS-4 to NFHS-5 (see Fig. 2). Over 65% of ADs saw an increase in anaemia, impacting 75 out of 112 ADs. Assam experienced the highest increase in anaemia prevalence among states, with a rise of 29.4% points, while Uttarakhand recorded the lowest change, showing a decrease of 15.3% points. Notably, Barpeta in Assam recorded the highest increase in anaemia prevalence by 45.1% points, whereas Haridwar in Uttarakhand showed the greatest decrease 25.8% points.

The left map is showing prevalence in anaemia in NFHS-4 and the right map is showing prevalence of anaemia in NFHS-5.
Furthermore, Fig. 3 illustrates that from 2015 to 2021, distinct patterns emerged across different states. In addition to Assam, several other states have reported increased anaemia prevalence in their ADs, including Mizoram, Gujarat, Chhattisgarh, Manipur, Rajasthan, Maharashtra, Tripura, Jammu & Kashmir, Nagaland, Tamil Nadu, Bihar, Odisha, Telangana, Madhya Pradesh, Punjab, and Haryana. In these states, nearly all ADs, with a few exceptions, have shown a rising trend in anaemia. Specific districts, such as Barpeta, Udalguri, and Darrang in Assam; Mizoram and Mamit in Mizoram; Narmada and Dahod in Gujarat; Korba and Bastar in Chhattisgarh; Manipur and Chandel in Manipur; Karauli and Dholpur in Rajasthan; Osmanabad and Washim in Maharashtra; Dhalai in Tripura; and Baramulla and Kupwara in Jammu & Kashmir, have all reported significant increases in anaemia prevalence.

The blue columns indicate an increase in anaemia, the red columns indicate a decrease, and the green columns represent changes in anaemia prevalence in each state.
Conversely, several states have witnessed a decrease in anaemia prevalence in their ADs. These include Arunachal Pradesh (Namsai), Jharkhand (Dumka and Latehar), Uttar Pradesh (Fatehpur and Balrampur), Himachal Pradesh (Chamba), Meghalaya (Ribhoi), Andhra Pradesh (Y.S.R. Kadapa), Kerala (Wayanad), Sikkim (West District), and Uttarakhand (Udham Singh Nagar and Uttarkashi).
Pattern of change in anaemia among adolescent girls in ADs by background characteristics
Table 2 shows significant changes in anaemia prevalence across various subgroups. Parity emerged as a notable characteristic, with adolescent girls who had 3–4 children experiencing a marked increase in anaemia prevalence, rising by 9.2% points from 56.3% in NFHS-4 to 65.5% in NFHS-5.
Socioeconomic status, as indicated by household wealth, reveals a significant pattern in anaemia prevalence. Among girls in the poorer wealth category, anaemia rose by 5.9% points, increasing from 57.1% to 63.1% over the period. In contrast, the wealthiest subgroup saw a decrease in anaemia prevalence, dropping from 55.9% to 52.3%. These results highlight the disparities in health outcomes linked to household wealth, with poorer adolescent girls experiencing higher rates of anaemia. Additionally, anaemia prevalence increased among girls from OBC by 2.9% points, and among girls from the Muslim community, where the increase was 5.9% points compared to other groups. Moreover, girls who are currently amenorrheic experienced a notable rise in anaemia, with prevalence increasing from 69.1% in NFHS-4 to 70% in NFHS-5.
Factors associated with anaemia among adolescent girls in ADs of India
The findings from Table 3 revealed adolescent girls with one to two children had 29% higher odds of anaemia (AOR: 1.29, 95% CI: 1.02–1.62) than those without children. Formerly married girls had 57% higher odds of anaemia (AOR: 1.57, 95% CI: 0.94–2.60). Additionally, ST girls exhibit 44% higher odds of anaemia (AOR: 1.44, 95% CI: 1.34–1.55) than those in other social groups. Economic status also significantly influences anaemia risk, as adolescent from the wealthiest households have 22% lower odds of anaemia (AOR: 0.78, 95% CI: 0.71–0.85) compared to those from the lowest income quintile. Regarding BMI, obese girls had a 15% lower odds of anaemia than underweight girls. Furthermore, anaemia risk is 26% higher among girls experiencing amenorrhoea (AOR: 1.26, 95% CI: 1.04–1.52) than among those without amenorrhoea.
Discussion
This study identified the vulnerable subgroups of adolescent girls with anaemia in ADs and the factors associated with anaemia. Additionally, it revealed changes in anaemia prevalence across different ADs from 2015 to 2021. During this period, anaemia among adolescent girls in India has increased, with a particularly sharp rise observed in ADs (IIPS and ICF, 2019). According to WHO guidelines, anaemia above 40% is considered a serious public health problem (McLean et al. 2009), and the rise in anaemia among adolescent girls in ADs from 58.3% to 62.4% highlights the severity of this health concern. Furthermore, the findings revealed that 75 out of 112 ADs witnessed an increase in anaemia among adolescent girls. Higher rates of anaemia were found among girls having higher parity, those from Muslim backgrounds, and girls belonging to poorer households. Moreover, formerly married girls, ST girls, and girls experiencing amenorrhoea were associated with anaemia.
This study’s findings on anaemia among adolescent girls have a similar result to some earlier studies conducted in India and other countries (Ahankari et al. 2017; Chauhan et al. 2022). For instance, studies conducted among adolescent girls aged 10–19 years in Maharashtra, Uttar Pradesh and Bihar found that anaemia was more prevalent among adolescent girls than adolescent boys (Ahankari et al. 2017; Chauhan et al. 2022; Srivastava et al. 2022). Some earlier studies have predominantly identified children and adolescent girls as high-risk groups for anaemia in India and other developing countries (Chauhan et al. 2022; Mistry et al. 2017; Srivastava et al. 2022; Sunuwar et al. 2023).
This study also revealed that formerly married adolescents were more likely to have anaemia, consistent with earlier research findings (Hakizimana et al. 2019; Let et al. 2024; Sharif et al. 2023; World Health Organization, 2017). One potential explanation is that formerly married adolescents who are separated from their husbands frequently lack the essential support needed to care for their families (Apouey, 2013). This circumstance places them at risk of economic hardship, poverty, malnutrition, and restricted access to healthcare services (Arpey et al. 2017; Hakizimana et al. 2019). As a result, they may not receive adequate nutrition and may struggle to afford healthcare, both of which are essential for preventing and treating anaemia (Mawani and Aziz Ali, 2016). Consistent with earlier studies, our research also found that higher parity is linked to a greater likelihood of anaemia (Al-farsi et al. 2011; Arabyat et al. 2019; Armah-Ansah, 2023; Ntenda et al. 2018; Opitasari and Andayasari, 2015; Räisänen et al. 2014). One possible reason for this increased risk is that high parity exposes women to more frequent haemorrhaging, which can occur before, during, or after each delivery (Al-farsi et al. 2011; Arabyat et al. 2019). Furthermore, some studies suggest that the more frequently women give birth, the greater their blood loss, which results in lower hemoglobin levels, especially when combined with poor-quality diets (Armah-Ansah, 2023; Dwumoh et al. 2014; Opitasari and Andayasari, 2015).
This study also revealed that ST adolescents were at a higher risk of anaemia compared to girls from other social groups. This can be attributed to a combination of socio-economic disadvantages, undernutrition, early childbearing, and health disparities (Chakrabarty et al. 2023; De et al. 2006; Ghosh, 2023b, 2023a; Let et al. 2024; Rose-Clarke et al. 2019). Limited access to nutritious foods among ST adolescents might contribute to the higher anaemia rates among them (Ghosh et al. 2023; Rose-Clarke et al. 2019; Saha et al. 2021). Additionally, poor sanitation practices, restricted educational access, high unemployment levels, cultural norms like early marriage, inadequate maternal care, and existing taboos may contribute to the increased prevalence of anaemia among ST adolescent girls (Ghosh et al. 2022; Rose-Clarke et al. 2019; Sharif et al. 2023; Vart et al. 2015). Our study also found that in ADs, adolescents girls from wealthier backgrounds were less likely to have anaemia compared to those from less affluent backgrounds. This finding aligns with other studies conducted in Ethiopia, Pakistan, India and Asia (Abate et al. 2021; Chakrabarty et al. 2023; Let et al. 2024; Soofi et al. 2017; Worku et al. 2022). Adolescents from the highest socioeconomic status tend to have better nutritional status and greater access to healthcare services, which facilitates the diagnosis and treatment of anaemia (Let et al. 2024; Saha et al. 2021; Sharma et al. 2018, 2020). Conversely, those from the poorest backgrounds often face insufficient access to food, and skip meals, these might contribute to higher rates of anaemia among the poorest adolescents (Abate et al. 2021; Let et al. 2024). Furthermore, similar to earlier studies conducted in India and Ghana, our study finds that adolescents who consumed fish were more likely to have anaemia (Armo-Annor et al. 2021; Let et al. 2024; Mog et al. 2023). In contrast, other research from India and among Vietnamese women indicates that fish consumption does not increase the risk of anaemia (Aikawa et al. 2006; Chakrabarty et al. 2023; Van Thuy et al. 2003). Whereas, a study on Malawian children revealed that consuming large fish has minimal effect on anaemia and small fish consumption can improve iron status and it does help to improve good dietary practices and improve overall iron status in the body (Werner et al. 2024).
The Government of India has launched key initiatives to address anaemia, including the National Nutritional Anaemia Control Programme (1970), the National Nutritional Policy (1993), and the National Iron+ Initiative (2013) (Department of Women and Child Development, 1993; Gupta et al. 2013). In 2018, the Anemia Mukt Bharat was launched to reduce anaemia among children, WRA, and adolescents (MoHFW, 2018a). Furthermore, the Indian government has implemented specific health and nutrition action plans across each state that has ADs, focusing on reducing anaemia among pregnant women (MoHFW, 2018b).
In examining the positive effect of ADP on anaemia prevalence among adolescent girls, our findings indicate mixed progress. Out of the 112 designated ADs, approximately 33% (37 ADs) have shown reductions in anaemia prevalence from NFHS-4 to NFHS-5. Notably, these reductions were observed across all ADs in Kerala (southern India), as well as in the northeastern states of Arunachal Pradesh, Sikkim, and Meghalaya, northern states of Himachal Pradesh and Uttarakhand, and seven of the eight ADs in Uttar Pradesh, excluding Fatehpur. This pattern is encouraging and suggests that ADP interventions may be having a positive impact in these regions. However, the prevalence of anaemia has increased in the majority of ADs, signaling persistent challenges and highlighting the need for intensified, region-specific strategies to strengthen the program’s efficacy in addressing anaemia among vulnerable populations. It is essential to develop specialized healthcare and nutrition programs tailored for adolescent girls, similar to those targeting anaemia in pregnant women in ADs. These programs should focus on formerly married girls, ST adolescent girls, and girls experiencing amenorrhoea, as these groups have been identified as being more likely to have anaemia. This approach will allow for the development of programs that not only improve access to vital health resources and nutritional education but also promote reproductive health in a supportive way. Focusing on these specific areas is crucial for effectively lowering anaemia rates.
This study highlights that adolescent girls in India’s ADs exhibit the highest anaemia rates among all age groups in the country, which stands as a significant strength of this study. Additionally, the research evaluates district-wise changes in anaemia prevalence among these girls from 2015 to 2021. These findings offer valuable insights that could guide policymakers in implementing targeted measures to mitigate anaemia in ADs. Despite these strengths, the study is constrained by its cross-sectional survey design and also limited by missing data on crucial variables like vitamin A intake and cultural beliefs, which were not available in the dataset. It is also important to acknowledge that the precise reasons for the rising anaemia rates among adolescent girls in ADs remain unclear. Future research should focus on integrating these variables to enhance the depth and precision of understanding regarding anaemia among adolescent girls in ADs of India.
Conclusion
Anaemia remains a pressing issue among adolescent girls in ADs. This study contributes valuable findings on the shifting patterns and underlying determinants of anaemia from 2015 to 2021. Our findings reveal that adolescent girls in ADs are particularly vulnerable, experiencing the highest anaemia rates across age groups, both within ADs and at the national level. Adolescent girls from lower-income families, the Muslim community, girls experiencing amenorrhoea, those with higher parity, and those belonging to ST were more likely to have anaemia. These findings emphasize the need for targeted, context-specific interventions in ADs, beyond the general programs currently in place. Additionally, it is essential to develop specialized healthcare and nutrition programs tailored for adolescent girls, similar to those targeting anaemia in pregnant women in ADs. This study not only contributes to the understanding of anaemia in adolescent girls but also underscores the necessity for district-level and state-level interventions, particularly in areas where anaemia rates have risen significantly. The research provides a strong foundation for policymakers to develop more refined, data-driven strategies aimed at reducing anaemia prevalence among adolescent girls in ADs.
Data availability
Our study utilizes data from the National Family Health Survey (NFHS) rounds 4 and 5. These datasets are publicly available and can be accessed upon submission of a formal request through the official website of the Demographic and Health Surveys (DHS) Program: https://dhsprogram.com/data/availabledatasets.cfm.
References
Abate TW, Getahun B, Birhan MM, Aknaw GM, Belay SA, Demeke D, Abie DD, Alemu AM, Mengiste Y (2021) The urban–rural differential in the association between household wealth index and anemia among women in reproductive age in Ethiopia, 2016. BMC Women’s Health 21(1):1–8. https://doi.org/10.1186/s12905-021-01461-8
Ahankari AS, Myles PR, Fogarty AW, Dixit JV, Tata LJ (2017) Prevalence of iron-deficiency anaemia and risk factors in 1010 adolescent girls from rural Maharashtra, India: a cross-sectional survey. Public Health 142:159–166. https://doi.org/10.1016/j.puhe.2016.07.010
Aikawa R, Khan NC, Sasaki S, Binns CW (2006) Risk factors for iron-deficiency anaemia among pregnant women living in rural Vietnam. Public Health Nutr 9(4):443–448. https://doi.org/10.1079/phn2005851
Al-farsi YM, Brooks DR, Werler MM, Cabral HJ, Al-shafei MA (2011) Effect of high parity on occurrence of anemia in pregnancy: a cohort study. BMC Pregnancy and Childbirth. https://doi.org/10.1186/1471-2393-11-7
Apouey BH (2013) Health policies and the relationships between socioeconomic status, access to health care, and health. Isr J Health Policy Res 2(1):1–2. https://doi.org/10.1186/2045-4015-2-50
Arabyat R, Arabyat G, Al-Taani G (2019) Prevalence and risk factors of anaemia among ever-married women in Jordan. East Mediterr Health J 25(8):543–552. https://doi.org/10.26719/emhj.18.074
Armah-Ansah EK (2023) Determinants of anemia among women of childbearing age: analysis of the 2018 Mali demographic and health survey. Arch Public Health 81(1):1–13. https://doi.org/10.1186/s13690-023-01023-4
Armo-Annor D, Colecraft EK, Adu-Afarwuah S, Christian AK, Jones AD (2021) Risk of anaemia among women engaged in biomass-based fish smoking as their primary livelihood in the central region of Ghana: a comparative cross-sectional study. BMC Nutr 7(1):1–11. https://doi.org/10.1186/s40795-021-00456-w
Arpey NC, Gaglioti AH, Rosenbaum ME (2017) How socioeconomic status affects patient perceptions of health care: a qualitative study. J Prim Care Community Health 8(3):169–175. https://doi.org/10.1177/2150131917697439
Balarajan, YS, Fawzi, WW, Subramanian, SV (2013) Changing patterns of social inequalities in anaemia among women in India: cross-sectional study using nationally representative data. BMJ Open, 3(3). https://doi.org/10.1136/bmjopen-2012-002233
Casey BJ, Duhoux S, Cohen MM (2010) Adolescence: What do transmission, transition, and translation have to do with it? Neuron 67(5):749–760. https://doi.org/10.1016/j.neuron.2010.08.033
Centre for Social and Behaviour Change, A. U. (2022) Stories of change: from India’s aspirational districts. https://www.niti.gov.in/sites/default/files/2022-04/Stories_of_Change_2022_1.pdf
Chakrabarty M, Singh A, Singh S, Chowdhury S (2023) Is the burden of anaemia among Indian adolescent women increasing? Evidence from Indian Demographic and Health Surveys (2015–21). PLOS Glob Public Health 3(9):e0002117. https://doi.org/10.1371/journal.pgph.0002117
Chauhan S, Kumar P, Marbaniang SP, Srivastava S, Patel R (2022) Prevalence and predictors of anaemia among adolescents in Bihar and Uttar Pradesh, India. Sci Rep. 12(1):1–9. https://doi.org/10.1038/s41598-022-12258-6
Chen Y-T, & Chen MC (2010) Using chi square. expert systems with applications. https://doi.org/10.1016/j.eswa.2010.08.100
De M, Halder A, Podder S, Sen R, Chakrabarty S, Sengupta B, Chakraborty T, Das U, Talukder G (2006) Anemia and hemoglobinopathies in tribal population of Eastern and North-eastern India. Hematology 11(5–6):371–373. https://doi.org/10.1080/10245330600840180
Department of Women and Child Development. (1993) National Nutrition Policy. In Ministry of Human Resource Development. https://doi.org/10.5005/jp/books/13071_4
Dwumoh D, Essuman EE, Afagbedzi SK (2014) Determinant of factors associated with child health outcomes and service utilization in Ghana: multiple indicator cluster survey conducted in 2011. Arch Public Health 72(1):1–10. https://doi.org/10.1186/2049-3258-72-42
Elder L, & Ransom E (2003) Nutrition of Women and Adolescent Girls: Why It Matters. https://www.prb.org/resources/nutrition-of-women-and-adolescent-girls-why-it-matters/
Gardner WM, Razo C, McHugh TA, Hagins H, Vilchis-Tella VM, Hennessy C, Taylor HJ, Perumal N, Fuller K, Cercy KM, Zoeckler LZ, Chen CS, Lim SS, Aravkin AY, Arndt MB, Bishai JD, Burkart K, Chung E, Dai X, Moradi M (2023) Prevalence, years lived with disability, and trends in anaemia burden by severity and cause, 1990–2021: findings from the Global Burden of Disease Study 2021. Lancet Haematol 10(9):e713–e734. https://doi.org/10.1016/S2352-3026(23)00160-6
Ghosh P (2023a) Corrigendum to “Determinants and transition of anaemia among under-five children from different social groups in India from 2005-06 to 2015–16” [Soc. Sci. Med. 320 (2022) 115702] (Social Science & Medicine (2023) 320, (S0277953623000576), (10.1016/j.socsc. Social Science and Medicine 323(March):115842 https://doi.org/10.1016/j.socscimed.2023.115842
Ghosh P (2023b) Undernutrition among the children from different social groups in India: prevalence, determinants, and transition over time (2005–2006 to 2019–2021). J Racial Ethn Health Disparities, 0123456789. https://doi.org/10.1007/s40615-023-01796-y
Ghosh P, Bose K, & Rohatgi P (2023) Prevalence and determinants of anaemia among under‑five children in West Bengal: an insight from the national family health survey 2015–2016. Global Soc Welfare, 1–13. https://doi.org/10.1007/s40609-023-00299-2
Ghosh P, Rohatgi P, Bose K (2022) Determinants of time-trends in exclusivity and continuation of breastfeeding in India: an investigation from the National Family Health Survey. Soc Sci Med 292(September 2021):114604. https://doi.org/10.1016/j.socscimed.2021.114604
Gupta A, Kumar R, Salhotra VS, Mohan A, & Rahi S (2013) National iron plus initiative-towards infinite potential in an anaemia free India. In National Rural Health Mission
Hakizimana D, Nisingizwe MP, Logan J, Wong R (2019) Identifying risk factors of anemia among women of reproductive age in Rwanda - A cross-sectional study using secondary data from the Rwanda demographic and health survey 2014/2015. BMC Public Health 19(1):1–11. https://doi.org/10.1186/s12889-019-8019-z
Hosmer DW, & Stanley L (2007) Goodness of fit tests for the multiple logistic regression model. Communications in Statistics—Theory and Methods, 1043–1069. https://www.tandfonline.com/doi/abs/10.1080/03610928008827941
IIPS and ICF. (2017). National Family Health Survey (NFHS-4), 2015-16: India. Mumbai: IIPS
IIPS and ICF. (2019). National Family Health Survey (NFHS-5), 2019-21: India. Mumbai: IIPS
Let S, Tiwari S, Singh A (2025) Contextualising Anaemia Among Reproductive Women in West Bengal: Trends, Patterns, and Predictors. In P. Chouhan, A Roy, N Kapasia, J Das, & M Rahaman (Eds.), Sexual and Reproductive Health of Women (1st ed., pp. 41–57). Springer Singapore. https://doi.org/10.1007/978-981-97-8418-9_4
Let S, Tiwari S, Singh A, Chakrabarty M (2024) Prevalence and determinants of anaemia among women of reproductive age in Aspirational Districts of India: an analysis of NFHS 4 and NFHS 5 data. BMC Public Health, 1–19. https://doi.org/10.1186/s12889-024-17789-3
Mawani M, Aziz Ali S (2016) Iron deficiency anemia among women of reproductive age, an important public health problem: situation analysis. Reprod Syst Sex Disord 5(3):1–6. https://doi.org/10.4172/2161-038x.1000187
McLean E, Cogswell M, Egli I, Wojdyla D, De Benoist B (2009) Worldwide prevalence of anaemia, WHO vitamin and mineral nutrition information system, 1993-2005. Public Health Nutr 12(4):444–454. https://doi.org/10.1017/S1368980008002401
Mertler CA, Vannatta RA, & LaVenia KN (2021) Binary Logistic Regression. In Advanced and Multivariate Statistical Methods. https://doi.org/10.4324/9781003047223-10
Midi H, Sarkar SK, Rana S (2010) Collinearity diagnostics of binary logistic regression model. J Interdiscip Math 13(3):253–267. https://doi.org/10.1080/09720502.2010.10700699
Mistry SK, Jhohura FT, Khanam F, Akter F, Khan S, Yunus FM, Hossain MB, Afsana K, Haque MR, Rahman M (2017) An outline of anemia among adolescent girls in Bangladesh: Findings from a cross-sectional study. BMC Hematol 17(1):1–8. https://doi.org/10.1186/s12878-017-0084-x
Mog M, Neogi D, Pratim Bharadwaz M, Kumar Panda B, & Sil A (2023) Prevalence and factors associated with anaemia in married women of reproductive age group: evidence from North East India. J Biosoc Sci 425–437. https://doi.org/10.1017/S0021932022000177
MoHFW. (2018a). Anemia Mukt Bharat: Intensified National Iron Plus Initiative (I-NIPI). https://anemiamuktbharat.info/resource/amb-operational-guidelines-english/
MoHFW. (2018b) Health Atlas of Aspirational Districts (Issue April)
NITI Aayog. (2018) Transformation of Aspirational District A New India by 2022
Ntenda PAM, Nkoka O, Bass P, Senghore T (2018) Maternal anemia is a potential risk factor for anemia in children aged 6-59 months in Southern Africa: a multilevel analysis. BMC Public Health 18(1):1–13. https://doi.org/10.1186/s12889-018-5568-5
Opitasari C, Andayasari L (2015) Young mothers, parity and the risks of anemia in the third trimester of pregnancy. Health Sci J Indones 6(1):7–11
Porter ME, Stern S, Green M, Dr Kapoor A (2018) An assessment of aspirational districts programme. https://www.niti.gov.in/sites/default/files/2023-03/An-Assessment-Of-Aspirational-Districts-Programme.pdf
Puri N (2020) A review of the aspirational districts program of the National Institute of Transforming India, Government of India. SSRN Electron J, August, 1–21. https://doi.org/10.2139/ssrn.3511027
Räisänen S, Kancherla V, Gissler M, Kramer MR, Heinonen S (2014) Adverse perinatal outcomes associated with moderate or severe maternal anaemia based on parity in Finland during 2006-10. Paediatr Perinat Epidemiol 28(5):372–380. https://doi.org/10.1111/ppe.12134
Rose-Clarke K, Pradhan H, Rath S, Rath S, Samal S, Gagrai S, Nair N, Tripathy P, Prost A (2019) Adolescent girls ’ health, nutrition and wellbeing in rural eastern India: a based study. BMC Public Health 19(673):1–11. https://doi.org/10.1186/s12889-019-7053-1
Sachdev HS, Porwal A, Acharya R, Ashraf S, Ramesh S, Khan N, Kapil U, Kurpad AV, Sarna A (2021) Haemoglobin thresholds to define anaemia in a national sample of healthy children and adolescents aged 1–19 years in India: a population-based study. Lancet Glob Health 9(6):e822–e831. https://doi.org/10.1016/S2214-109X(21)00077-2
Saha S, Pandya A, Kandre Y, Raval D, Saxena D (2021) Cross-sectional analysis of nutritional status, knowledge and uptake of nutritional services among adolescent girls in Western India. Adolesc Health Med Ther 12:117–125. https://doi.org/10.2147/AHMT.S336071
Scott S, Lahiri A, Sethi V, de Wagt A, Menon P, Yadav K, Varghese M, Joe W, Vir SC, Nguyen PH (2022) Anaemia in Indians aged 10–19 years: Prevalence, burden and associated factors at national and regional levels. Matern Child Nutr 18(4). https://doi.org/10.1111/mcn.13391
Sharif N, Das B, Alam A (2023) Prevalence of anemia among reproductive women in different social group in India: cross-sectional study using nationally representative data. PLoS ONE 18(2 February):1–22. https://doi.org/10.1371/journal.pone.0281015
Sharma H, Singh SK, & Srivastava S (2018) Major correlates of anemia among women (age 15-49) in india and spatial variation, evidence from national family health survey-4. J Women’s Health Care, 07(04). https://doi.org/10.4172/2167-0420.1000440
Sharma H, Singh SK, Srivastava S (2020) Socio-economic inequality and spatial heterogeneity in anaemia among children in India: evidence from NFHS-4 (2015–16). Clin Epidemiol Glob Health 8(4):1158–1171. https://doi.org/10.1016/j.cegh.2020.04.009
Soofi S, Khan GN, Sadiq K, Ariff S, Habib A, Kureishy S, Hussain I, Umer M, Suhag Z, Rizvi A, Bhutta Z (2017) Prevalence and possible factors associated with anaemia, and Vitamin B 12 and folate deficiencies in women of reproductive age in Pakistan: analysis of national-level secondary survey data. BMJ Open, 7(12). https://doi.org/10.1136/bmjopen-2017-018007
Srivastava S, Kumar P, Paul R, Debnath P (2022) Effect of change in individual and household level characteristics on anemia prevalence among adolescent boys and girls in India. BMC Public Health 22(1):1–10. https://doi.org/10.1186/s12889-022-13863-w
StataCorp. (2017) Stata Survey Data Reference Manual—Introduction to survey commands. https://www.stata.com/manuals/svy.pdf
Sunuwar DR, Singh DR, Pradhan PMS, Shrestha V, Rai P, Shah SK, Adhikari B (2023) Factors associated with anemia among children in South and Southeast Asia: a multilevel analysis. BMC Public Health 23(1):1–17. https://doi.org/10.1186/s12889-023-15265-y
United Nations Development Program. (2020). Aspirational Districts Programme: An appraisal. https://www.niti.gov.in/sites/default/files/2023-03/Aspirational-Districts-Programme-An-Appraisal.pdf
Van Thuy P, Berger J, Davidsson L, Khan NC, Lam NT, Cook JD, Hurrell RF, Khoi HH (2003) Regular consumption of NaFeEDTA-fortified fish sauce improves iron status and reduces the prevalence of anemia in anemic Vietnamese women. Am J Clin Nutr 78(2):284–290. https://doi.org/10.1093/ajcn/78.2.284
Vart P, Jaglan A, Shafique K (2015) Caste-based social inequalities and childhood anemia in India: results from the National Family Health Survey (NFHS) 2005-2006 Chronic Disease epidemiology. BMC Public Health 15(1):1–8. https://doi.org/10.1186/s12889-015-1881-4
Weiß M, & Markus G (2011) Molecular phylogenetic reconstruction: akaike information criterion. In The Yeasts (Fifth Edition) (pp. 159–174). https://www.sciencedirect.com/topics/pharmacology-toxicology-and-pharmaceutical-science/akaike-information-criterion
Werner ER, Arnold CD, Caswell BL, Iannotti LL, Maleta KM, Stewart CP (2024) Associations of fish and meat intake with iron and anaemia in Malawian children. Matern Child Nutr 20(2):1–13. https://doi.org/10.1111/mcn.13622
WHO. (2018). Technical Handbook on Anaemia in Adolescents. 1–14
Wiafe MA, Ayenu J, & Eli-Cophie D (2023) A review of the risk factors for iron deficiency anaemia among adolescents in developing countries. Anemia, 2023. https://doi.org/10.1155/2023/6406286
Worku MG, Alamneh TS, Teshale AB, Yeshaw Y, Alem AZ, Ayalew HG, Liyew AM, Tessema ZT, Tesema GA (2022) Multilevel analysis of determinants of anemia among young women (15-24) in sub-Sahara Africa. PLoS ONE 17(5 May):1–16. https://doi.org/10.1371/journal.pone.0268129
World Health Organization. (2016). Obesity and overweight. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
World Health Organization. (2017). Prevention of iron deficiency anaemia in adolescents: role of weekly iron and folic acid supplementation. In World Health Organization. http://www.searo.who.int/entity/child_adolescent/documents/sea_cah_2/en/
Yang J, Li Q, Feng Y, Zeng Y (2023) Iron deficiency and iron deficiency anemia: potential risk factors in bone loss. Int J Mol Sci, 24(8). https://doi.org/10.3390/ijms24086891
Acknowledgements
Subhojit Let (Ref. No: 200510160983) and Mahashweta Chakrabarty (Ref. No: 200510082749) acknowledge the support of the Junior Research Fellowship provided by the University Grants Commission, India.
Funding
No particular grant was given to this research by any funding organizations in the public, private, or nonprofit sectors.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study. Subhojit Let was responsible for data curation, formal analysis, methodology, and visualization, and contributed to both the drafting and critical revision of the manuscript. Mahashweta Chakrabarty contributed to validation, and visualization, as well as drafting and revising the manuscript. Seema Tiwari was involved in the investigation, ensured validation, and supervised the research process. All authors read and approved the final draft.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
This study is based on secondary data from the National Family Health Survey (NFHS-4 and NFHS-5), conducted by the International Institute for Population Sciences (IIPS) under the Ministry of Health and Family Welfare, Government of India. Ethical approval for the surveys was obtained by IIPS from an independent ethics review committee before data collection. As this study uses publicly available, de-identified data, no additional ethical approval was required. The datasets can be accessed upon request via the DHS website: https://dhsprogram.com/data/new-user-registration.cfm.
Informed consent
The authors of this study did not collect any primary data or conduct any survey. Informed consent was obtained by the NFHS survey administrators before data collection. As per NFHS protocols, written and/or verbal informed consent was secured from all participants or their legal guardians before participation in the survey.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Let, S., Chakrabarty, M. & Tiwari, S. Investigating anaemia vulnerability: determinants and changes in prevalence among adolescent girls in aspirational districts of India. Humanit Soc Sci Commun 12, 268 (2025). https://doi.org/10.1057/s41599-025-04573-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1057/s41599-025-04573-w
