
Abstract
Goal-directed behavior requires resolving both consciously and subconsciously induced response conflicts. Neuronal gain control, which enhances processing efficacy, is crucial for conflict resolution and can be increased through pharmacological or brain stimulation interventions, though it faces inherent physical limits. This study examined the effects of anodal transcranial direct current stimulation (atDCS) and methylphenidate (MPH) on conflict processing. Healthy adults (n = 105) performed a flanker task, with electroencephalography (EEG) used to assess alpha and theta band activity (ABA, TBA). Results showed that combining atDCS with MPH enhanced cognitive control and reduced response conflicts more effectively than atDCS alone, particularly when both conflict types co-occurred. Both atDCS and atDCS + MPH exhibited similar task-induced ABA and TBA modulations in the (pre)supplementary motor area, indicating heightened gain control. Overlapping neuroanatomical effects in mid-superior frontal areas suggest that atDCS and MPH share a common neuronal mechanism of gain control, especially in high-conflict/-demand situations.
Similar content being viewed by others
Introduction
Resolving response conflicts is influenced by the brain’s ability to effectively distinguish relevant input from intrinsic noise (including irrelevant stimulus features). This key component of goal-directed behavior and cognitive control particularly relies on the signal-to-noise ratio (SNR), which indicates the processing system’s sensitivity to important inputs versus neural noise1,2. Fine-tuning the SNR, namely sharpening the neuronal input/output function (the probability that varying strengths of presynaptic input will trigger a postsynaptic response), describes neuronal gain control mechanisms1,3. Enhanced neural gain control is linked to improved response control and overall cognitive, motor, and sensory performance4,5,6. Here, we investigated the effect of modulating gain control onto cognitive control processes, specifically the selection of appropriate actions by prioritizing relevant information over consciously and subliminally perceived cued distractions.
Research indicates that gain control mechanism can be modulated by various pharmacological and non-invasive brain stimulation (NIBS) techniques1,7,8,9, both of which may exhibit ceiling effects as there is a limit to how much gain control can be increased. Combining both approaches in a proof-of-concept study will provide crucial insights into their interactive effects. In the current study, we therefore combined a NIBS method and a psychostimulant, of which both have been shown to modulate the efficacy of gain control mechanisms. Specifically, we used transcranial direct current stimulation (tDCS), which through a low electric current applied to the scalp induces focal changes in cortical excitability (i.e., increase or decrease dependent on electrode polarity), which last about one hour10,11. Cortical excitability adjusts neuronal gain control9,12, i.e., anodal tDCS (atDCS) induced amplification of spontaneous neuronal firing, and cortical excitability has been associated with modulation of gain control efficacy12,13. We applied atDCS to the right inferior frontal gyrus (rIFG) a region critical for response conflict resolution, and action inhibition14,15,16. This region was targeted, as it was shown to reflect response conflict effects specific to the experimental task at hand6. Furthermore, the catecholaminergic system underlies effective neural information processing, in that appropriate levels of dopamine (DA) and norepinephrine (NE) are central to conflict processing and resolution17,18,19. Thus, we used methylphenidate (MPH), a psychostimulant that selectively blocks DA/NE reuptake, consequently increasing postsynaptic DA and NE levels20,21,22. Previously, MPH-induced modulations of cognitive control have been attributed to neuronal gain mechanisms and linked to fronto-striatal loops6,23. Importantly, the rIFG has been highlighted as a key site for reflecting the modulatory effects of MPH on cognitive control6, making it, together with its well-established role in cognitive control, a suitable stimulation target.
In the current literature, there is a notable lack of research combining tDCS with pharmacological interventions in the context of cognitive control. Few studies have explored how these two modulations might interact to influence neural plasticity and reorganization24,25,26,27,28,29, underlining the need for further investigations in this area. While both tDCS and MPH have been studied individually, their combined effects on behavioral accuracy and brain oscillations, particularly during cognitive tasks inducing conscious and subconscious conflicts, have not been investigated. However, both consciously and subconsciously processed information affect controlled behavior30,31,32,33. To investigate such response conflicts in the current study, we used a combination of a spatial flanker task with preceding subliminal primes6,34,35 (full details in the methods section). Gain control facilitates task-relevant processing and modulations via atDCS appear to facilitate the resolution of stimulus-response conflicts36. In contrast, MPH-induced increases in gain control were shown to benefit the resolution of subconsciously and consciously induced conflicts differentially6.
As a measure of neuronal mechanisms underlying task performance modulations, we focused on both theta and alpha band activity (TBA and ABA). TBA coordinates and integrates neuronal activity in complex networks, reflecting conflict monitoring and response conflicts37,38,39. Whereas, ABA has been implicated in interceding suppression of task-irrelevant information by regulating access to behaviorally relevant information40,41. Both ABA and TBA are associated with neuronal gain control mechanisms by facilitating selective noise inhibition and enhancing perceptual and response selection accuracies42,43,44,45. This dual focus on cognitive and neuronal gain control relevant TBA and ABA will likely provide a comprehensive understanding of the neuronal dynamics underlying gain control modulations via atDCS and MPH.
In this study, we set out to investigate the effects of gain control modulations via atDCS and atDCS + MPH on consciously and subconsciously triggered response conflicts. Presuming that atDCS over the rIFG and MPH administration enhances the SNR in cortical areas relevant to response conflict processing, we hypothesize that (1) consciously and subconsciously induced response conflicts will engage distinct functional neuroanatomical networks (2) behavioral effects will be accompanied by comparable ABA and TBA modulations (reflecting gain control modulations) in mid-superior and inferior-frontal areas6,29,39 (3) the combined effects of atDCS and MPH will surpass the individual effects of each technique29 (4) combining atDCS with MPH will result in additive effects (rather than doubling) of both stimulation methods29, given that the extent to which gain control may be increased underlies a physical limit. The goal was to investigate neuronal gain control as a common neuronal mechanism underlying atDCS and MPH effects. Our neurophysiological analyses were aimed at investigating the neural mechanisms driving behaviorally relevant effects, providing insight into the cortical dynamics that underpin cognitive and behavioral outcomes obtained in this study. Accordingly, functional-neuroanatomical networks underlying consciously and subconsciously induced response conflicts modulated with atDCS and MPH (separately and combined) were examined.
Results
Included participants
After initial data inspection, n = 12 participants were excluded from all subsequent analyses (behavioral and EEG data). Participants were excluded based on the following criteria: (1) incomplete data due to technical issues (e.g., equipment malfunctions), (2) failure to comply with task instructions (e.g., responding inconsistently or inaccurately beyond acceptable thresholds), and (3) inability to complete study both study appointments (e.g., withdrawal or scheduling conflicts). Additional details are provided in the supplement (section “Additional details on exclusion decisions and the composition of the final sample”).
This resulted in a final sample of n = 93 (mean age 25.11 ± 0.315 SEM; 44 females) participants included in all subsequent analyses. Specifically, there were n = 45 (mean age 25.20 ± 0.428 SEM; 21 females) participants in the placebo group and n = 48 (mean age 25.02 ± 0.465 SEM; 23 females) in the MPH group.
Behavioral data
Task effects
The typical task effects of prime compatibility and flanker congruency (i.e., higher accuracies in congruent/compatible than in incongruent/incompatible trials) were replicated6,34. There was an interaction of prime compatibility x flanker congruency (F(1,89) = 57.930; p < .001; η2p = 0.394). Post hoc t-tests revealed significant differences for all possible contrasts (all p ≤ .001). In line with previous results, the prime compatibility effect (i.e. compatible – incompatible) was larger in incongruent flankers (10.263% ± 1.167) than in congruent flankers (6.722% ± 0.771) (t(1,75) = −7.390; p < 001). Additionally, the flanker congruency effect (i.e. congruent – incongruent) was larger in incompatible primes (5.264% ± 0.553) than in compatible primes (1.754% ± 10.234) [t(1,92) = −7.346; p < 0.001 (one-sided p)].
Pharmacological group and tDCS stimulation effects
The repeated measures ANOVA for accuracy revealed an interaction of tDCS x order of stimulation x prime compatibility x flanker congruency x pharmacological group (F(1,89) = 4.132; p = .045; η2p = 0.044). Next, the interaction effect was separately examined with post-hoc ANOVAs for real vs. sham tDCS appointments.
The post-hoc ANOVA for the active tDCS, but not for the sham tDCS appointment, revealed an interaction of order of stimulation x prime compatibility x flanker congruency x pharmacological group (F(1,89) = 9.535; p = .003; η2p = 0.097). To resolve this interaction, independent samples t-tests were conducted to compare the magnitudes of flanker and prime effects between the pharmacological groups when they received active tDCS. Of note, using those difference effects focusses the post-hoc analyses to the most relevant behavioral performance measures while simultaneously shortening subsequent analyses due to employing contrasts. These comparisons were made separately for participants who received active tDCS during their first appointment and those who received active tDCS during their second appointment. The results show that for participants who received active tDCS on the second appointment, the flanker congruency effect (i.e., congruent – incongruent trials) in case of incompatible primes was larger in the placebo group (7.737% ± 1.734) than in the MPH group (3.728% ± 1.001) [t(43) = 1.979; p = .027 (one-sided p)]. Moreover, the prime compatibility effect (i.e. compatible – incompatible trials) in case of incongruent flankers was also larger in the placebo group (9.165% ± 2.052) than in the MPH group (4.741% ± 1.372) [t(43) = 1.775; p = 0.041 (one-sided p)]. For participants who received active tDCS during their first appointment, no statistically significant differences in the contrasts of interest (flanker and prime effects) were observed between the pharmacological groups [all p > 0.051 (one-sided p)].
Taken together, significant differences between the pharmacological groups emerged exclusively when active tDCS was applied during the second appointment. This effect was observed only under high response conflict conditions – specifically, in scenarios where the respective other conflict was also present (i.e. when the flanker effect involved an incompatible prime, and the prime effect involved an incongruent flanker). In other words, when active tDCS was applied during the second appointment, the MPH group showed smaller flanker and prime effects compared to the placebo group. Figure 1 illustrates the most relevant behavioral accuracy results. The significance and magnitude of the overall learning/practice effects are reported in the supplementary material (section “Additional details on behavioral data: Learning/practice effects”).

Shown are the prime effects (in percent) for when the flankers were congruent (top row, left plot) and incongruent (top row, right plot), as well as the flanker effect (in percent) for when the primes were congruent (bottom row, left plot) and incongruent (bottom row, right plot). Green boxplots illustrate data for the placebo group and yellow boxplots for the MPH group. The “x” and the horizontal line inside the boxplots indicate the mean and median, respectively. Asterisks indicate significant differences at p < 0.05 and error bars represent the 95% confidence intervals. The raincloud plots illustrate the data distribution (above boxplot) and data points (below boxplot) of n = 93 participants.
Response times (RTs)
The repeated measures ANOVA for RTs showed a main effect of the pharmacological group (F(1,89) = 4.914; p = 0.029; η2p = 0.052), indicating overall faster response times of the MPH group (395.145 ms ± 4.852) as compared to the placebo group (410.583 ms ± 4.995). Importantly, there was an interaction of flanker congruency x pharmacological group (F(1,89) = 4.581; p = 0.035; η2p = 0.049). Post hoc independent samples t-tests show that overall the flanker effect (congruent minus incongruent trials) was larger (more negative) in the placebo group (−17.372 ms ± 1.306) than in the MPH group (−13.709 ms ± 0.933) [t(80.675) = −2.282; p = 0.013 (one-sided p)]. The relevant results are illustrated in Fig. 2.

Depicted is the flanker effect (congruent minus incongruent trials) for both pharmacological groups (MPH and placebo). Data is illustrated in green for the placebo group and in yellow for the MPH group. Asterisks indicate significant differences at p < 0.05 and error bars represent the 95% confidence intervals. The “x” and the horizontal line inside the boxplots indicate the mean and median, respectively. The raincloud plots illustrate the data distribution (above boxplot) and data points (below boxplot) of n = 93 participants.
Further main and interaction effects not involving the pharmacological group factor included the following: There was a main effect of the order of stimulation (F(1,89) = 4.557; p = .036; η2p = 0.049), showing overall faster response times for those who received active tDCS on the second appointment (-395.430 ms ± 4.995) as compared to those on the first appointment (-410.297 ms ± 4.852). Moreover, there was an interaction of tDCS x order of stimulation x flanker congruency (F(1,89) = 5.020; p = 0.028; η2p = 0.053). The interaction was examined with an independent samples t-test comparing the flanker effect after real and sham tDCS between those who received active tDCS on the first vs. those who received active tDCS on the second appointment. The results indicate smaller flanker congruency effects for those who received active stimulation on the second appointment (-9.978 ms ± 0.959) as compared to those who received active tDCS on the first appointment (-12.948 ms ± 0.869) [t(91) = -2.2300; p = .012 (one-sided p)]. There was no difference in the magnitude of the flanker effects on the sham tDCS appointment.
Neurophysiology
The behavioral differences between both pharmacological groups were only significant when participants received active tDCS stimulation on the second appointment. Based on this, subsequent neurophysiological analyses exclusively investigated differences between the MPH and placebo group when active tDCS was administered on the second appointment.
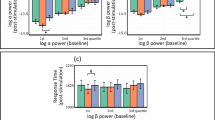
In the interval of 0−1000 ms relative to target onset, separate cluster-based permutation tests (CBPTs) were conducted for alpha and theta band activity (ABA and TBA respectively), and MPH and placebo groups. The results revealed significant negative differences in both ABA and TBA between compatible and incompatible primes trials when the flankers were incongruent, as well as between congruent and incongruent flanker trials when the prime was incompatible. Negative power differences indicate that alpha and theta band power were higher in incompatible prime trials compared to compatible ones, and in incongruent flanker trials compared to congruent ones, potentially highlighting greater difficulty, interference, or need for cognitive control effort in these conditions. Further details are provided in the supplement (section “Additional neurophysiological results for participants who received sham tDCS on the first appointment”). The significant electrode locations of the cluster-based permutation tests are visualized in Fig. 3, accompanied by the time-frequency representation (TFRs) of the power differences in the aforementioned contrasts.

a Alpha band time-frequency (TF) analysis and cluster-based permutation testing (CBPT) results. The TF plots display average power differences (0-1000 ms post-target arrow onset) for the prime effect (compatible MINUS incompatible trials) when flankers were incongruent, as well as for the flanker effect (congruent MINUS incongruent trials) when the prime was incompatible. Topographic plots highlight significant electrodes identified in the CBPTs, marked with red “x“s to indicate negative differences. These plots show average power in the significant timeframe (100 to ~600 ms) separately for both MPH and placebo groups, with conflict effects noted in corresponding titles. b Theta band time-frequency (TF) analysis and cluster-based permutation testing (CBPT) results. The TF plots display average power differences (0–1000 ms post-target arrow onset) for the prime effect (compatible MINUS incompatible trials) when flankers were incongruent, as well as for the flanker effect (congruent MINUS incongruent trials) when the prime was incompatible. Topographic plots highlight significant electrodes identified in the CBPTs, marked with red “x“s to indicate negative differences. These plots show average power in the significant timeframe (250 to ~750 ms) separately for both MPH and placebo groups, with conflict effects noted in corresponding titles.
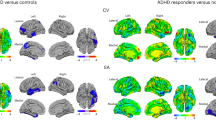
On the source level, the DBSCAN algorithm on the Prime and Flanker effect ratio identified several negative clusters in both alpha and theta bands for both MPH and placebo groups. Negative clusters (i.e., negative power ratios) indicate that ABA and TBA were higher in incompatible prime trials compared to compatible ones, and in incongruent flanker trials compared to congruent ones. The negative ratio reflects the directionality of this difference and suggests that the incompatible prime/incongruent flanker is influencing the processing system more prominently than the compatible prime/congruent flanker under these specific circumstances. An overview of all resulting clusters is provided in Fig. 4.

The color of the cluster represents the power ratio of the prime effect (when flankers are incongruent) and of the flanker effect (when the prime is incompatible). a Clusters identified in the alpha band. b Clusters identified in the theta band.
Discussion
This study investigated alterations in the functional neuroanatomical sources associated with subconsciously and consciously evoked response conflicts when gain control was experimentally increased. Assuming that atDCS and MPH share a common neuronal mechanism (i.e., gain control), we investigated the modulatory effects of atDCS, MPH, and atDCS + MPH via their effects on interference control and corresponding alpha and theta band oscillations (reflecting gain control). Compared to those who only received tDCS, participants who received both stimulations (i.e., atDCS + MPH) on the second appointment showed lower interference conflict effects, especially when subliminal and conscious conflicts were combined. Using an EEG beamforming approach, we identified the functional neuroanatomical correlates of atDCS-induced, and atDCS + MPH-induced modulations in ABA and TBA, respectively. Across both frequency bands, our results show overlapping neuroanatomical sources when atDCS and atDCS + MPH were applied. Consistent with the assumption that tDCS and MPH share a common underlying neural mechanism [most likely gain control, 4], we show that tDCS separately and combined with MPH modulates TBA in cognitive control-relevant mid-superior-frontal areas. Importantly, we extend these findings by showing similar modulatory effects in the ABA, highlighting the widespread influence of these interventions on cognitive control processes.
The behavioral data indicate clear differences between the pharmacological groups on the active atDCS appointment but not on the sham tDCS appointment. Specifically, when participants received atDCS on their second appointment (i.e., in the presence of learning/practice effects), both the flanker congruency effect and prime compatibility effect were significantly larger in the placebo group compared to the MPH group under high interference conflict conditions (i.e., in the presence of the respective other conflict, i.e., incompatible prime or incongruent flanker trials). While we did not have an a priori hypothesis expecting such learning/practice or order effects, this observation aligns with some of our previous MPH stimulation studies that demonstrated cognitive control-enhancing MPH effects46,47, but also hampered behavioral adaptation48, and sometimes even a reduction of MPH effects on simple response inhibition and perception-action integration49,50,51,52 in case of repeated measurements (i.e., after the task had already been performed once without MPH before). Given that the effectiveness of MPH modulation does generally not only depend on the dose, but also on task difficulty and prior learning/practice, it would have been unscientific to have postulated a clear direction of effects a priori. This does however not mean that the obtained effect cannot be interpreted: Given that the participants showed a small, but significant overall improvement in behavioral performance from the first to the second appointment (by 0.9% ± 0.3 and 11 ms ± 25; see supplement for details), it can be assumed that their improvement in accuracy and speed is likely due to learning/practice effects and/or response automatization. Given that we found no significant MPH differences in prime and flanker effects on the first appointment, it is unlikely that MPH produced out data pattern by hampering the initial learning of the task to a relevant degree. Instead, it seems that MPH only made a difference, once a relevant degree of learning / training had taken place (and tDCS stimulation was present, but this will be discussed in further details below). Given that the MPH effects were specific to high-conflict/demand situations, it seems plausible to assume that the combined effects of MPH and tDCS are most pronounced in a situation where easy responses have been extensively trained / automatized, which might potentially make it harder to switch into a cognitive control mode when needed (i.e., when a high-conflict trial pops up). Neurobiologically, the modulatory impact of elevated catecholamine levels on gain control processes may have been further strengthened by increasing cortical excitability via atDCS13,26,29, leading to optimal performance. No significant differences were found when atDCS was applied on the first appointment. Our results corroborate previous findings on the effects of MPH [19–22 etc.] and underscore the significant impact of the intricate interplay between atDCS, catecholaminergic stimulation, and the order of tDCS administration onto behavioral outcomes, particularly under challenging conditions (i.e. when the mental effort needed to perform well is high). In the following, we will separately discuss the functional neuroanatomical sources reflecting the prime and flanker effects when gain was modulated (via atDCS) on the second appointment.
Prime effect
In both frequency bands and pharmacological groups, the prime effect (in incongruent flanker trials) was associated with negative clusters in the (pre)SMA. Agreeing with previous results, TBA in the SMA is elevated when information conflicts and the need for cognitive control is high29,37,53. Moreover, TBA in mid-superior frontal regions is essential for cognitive control processes during response control, selection, and execution29,37,54,55. This is likely because TBA in these regions is particularly well-suited for integrating sensory information with motor commands37.
Notably, ABA is crucial for TBA-associated cognitive control processes and information-gating56, and their interplay is central for goal-directed action control. Increased ABA in the SMA likely reflects active engagement in attentional modulation/weighting and cognitive control56,57,58. The combined atDCS and MPH-induced amplification of the signal-to-noise ratio was sufficient to better suppress the processing of distracting information59, leading to improved/optimal interference and cognitive control. Mid-superior frontal ABA thus likely reflects the suppression of task-irrelevant information40,41. Our results show that after modulation of gain control via atDCS, but not when atDCS and MPH stimulation were combined, ABA additionally increases in an occipito-temporal cluster when the response conflict is high. The occipito-temporal areas have been linked to guiding (visual) attentional selection processes60,61. This pattern suggests that participants in the placebo group who experienced higher behavioral interference demonstrated enhanced visual processing of the prime stimulus and subsequently needed higher suppression of distracting information within occipito-temporal regions implemented by ABA. This likely reflects a gain-induced compensatory mechanism to manage increased cognitive load and mental effort to perform well. Our current results support the role of ABA in the temporal lobe as a critical element in moderating interference through selective (visual) attention and filtering out irrelevant or distracting stimuli40,59, especially when the cognitive load is high.
Flanker effect
Similar to the prime effect, the flanker effect (in incompatible prime trials) was associated with negative clusters spanning mid-superior-frontal areas62, across both frequency bands and pharmacological groups. When atDCS and MPH were combined, an additional cluster of ABA was detected in the left inferior frontal gyrus (left IFG). This aligns with a recent study29, suggesting that the additive effect of both modulations on neuronal gain control likely pushed the mid-superior frontal regions beyond their optimal functioning level, leading to the compensatory recruitment of higher processing capacities (i.e., the left IFG). Activity in the left IFG highlights its essential function in detecting and resolving conflicts at both the response and motor response levels63,64 and response control65.
In contrast to the prime effect, the flanker effect and associated interference conflict appear to engage a more distributed functional neuroanatomical network, particularly in the theta band. When modulating gain control with atDCS the flanker effect was additionally associated with TBA clusters spanning the right anterior and medial-temporal lobes. Medial temporal lobe (MTL) structures support memory functions and have been implicated in interference control66,67. Increased TBA in the most challenging trials likely indicates the involvement of the MTL in proactive interference control and successfully resolving the possibly detrimental effects of subliminal distractors66. Furthermore, the flanker effect following both atDCS and atDCS + MPH was associated with TBA in the right and left temporal pole (TP) respectively. When interference resolution is required, the right TP (i.e. a high-level visual cortical area) has been associated with object concept categorization based on their visual features68,69. Generally, the TP has been ascribed a role in receiving and integrating sensory modalities including visual inputs and participation in the ventral visual stream70. Ultimately, our results support the notion that in effortful situations the interaction of (mid-superior) frontal areas with MTL structures becomes more important71.
Shared conflict effects
Overall, in high-conflict scenarios, both response conflicts were reflected in gain-induced ABA and TBA modulations in similar, yet critically distinct, neuroanatomical regions. Consistent with our hypothesis, subconsciously and consciously evoked conflicts (in the presence of the respective other conflict) were associated with activity modulations in the (pre)SMA in both frequency bands, likely reflecting gain control29,72. Mid-superior frontal cognitive control-related brain activity29,37,54), likely reflects goal shielding processes essential for stabilizing goal representations amidst distracting input73,74. Here, the presence of both conflicts likely potentiated the conflict effects given a certain threshold was surpassed34. When modulating gain control with atDCS, ABA and TBA were increased in conflicting, as compared to non-conflicting trials37,54,62, irrespective of catecholaminergic stimulation. This indicates enhanced gain control, where neuronal gain is adjusted to prioritize relevant information and effortfully suppress distractions. These gain control increases were reflected in negative clusters for both response conflicts, pharmacological groups, and frequency bands.
Limitations
The observed results support the assumption that tDCS not solely affects the targeted cortical region, but also indirectly influences remote areas through interconnected cortical networks75,76. Given the evident cortical network-level impact of tDCS, this study further highlights the importance of interpreting tDCS effects within the context of broader neural interactions. A potential limitation of our study might have been that we did not assess whether participants could discern whether they were in the placebo or MPH group, nor which session involved active versus sham tDCS. It will further remain somewhat unclear whether the observed order effects are due to task learning, automatization, or both.
Conclusions
In summary, we dissociated the modulatory effect of gain control stimulated with atDCS and atDCS + MPH on subliminally and consciously induced response conflicts. Combining catecholaminergic enhancement with atDCS resulted in greater gain-induced cognitive control and lower response conflicts for both subconscious and consciously induced conflicts compared to atDCS alone, especially when both conflict types were present. Following active atDCS (irrespective of MPH stimulation), both response conflicts were associated with larger conflict-induced ABA and TBA modulations (reflecting gain control) spanning mid-superior-frontal areas. Activity modulations in the SMA likely indicate the need to correct cued response tendencies by generating internal (correct) responses that overwrite stimulus-triggered movements. Gain control modulation (via atDCS and atDCS +MPH), induced similar neuronal gain task requirement-specific allocations of ABA and TBA. The overlapping modulatory pattern in the same cortical network subserving response conflict resolution substantiates the theoretical assumption that atDCS and MPH exert their effects through a shared underlying mechanism, specifically neuronal gain control29,72.
Methods
Participants
An a priori estimation of the required sample size using G*Power software77,78 assuming a within-inbetween interaction in a 4 × 8 ANOVA design (for details on the factors, please refer to the section on behavioral statistics) with α = 5%, 1-β = 95%, a correlation of 5, the assumption of non-sphericity and an effect size of 2% (i.e., \({\eta }_{p}^{2}=.02\), or f = 0.14285) yielded a required total sample size of n = 100. Of note, this sample size is comparable to another publication of ours investigating the combined effects of tDCS and (a higher dose of) MPH on response inhibition, where the smallest significant pharmacological effect explained around 4% of variance (i.e., twice as much as assumed for the a priori sample size estimation)29. N = 105 healthy adults (mean age 25.06 ± 0.288 SEM; 54 females) voluntarily participated in this study. All participants were 20-31 years old, had normal or corrected-to-normal vision, had no current/reported history of psychiatric, neurologic, or developmental disorders, and reported no CNS-affecting medication use. Participants provided written informed consent and received course credits or financial compensation. The study was approved by the ethics committee of TU Dresden (EK 420092015) and conducted following the Declaration of Helsinki and its later amendments. All ethical regulations relevant to human research participants were followed.
Experimental design and methylphenidate administration
The study employed a mixed design with anodal tDCS (real vs. sham) and experimental conditions as within-subject factors, and pharmacological group (placebo vs. MPH) and order of stimulation (active tDCS on the first vs. second appointment) as between-subject factors. Pseudorandomization ensured equal numbers in each subgroup, defined by pharmacological group and order of stimulation. Group assignment was otherwise random and double-blind.
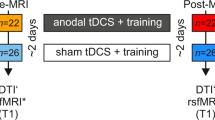
Participants attended two experimental sessions, spaced seven days apart. Depending on their randomly assigned pharmacological group, participants received either their respective MPH dose (0.50 mg per kg body weight) or a placebo (lactose) on both study appointments in a double-blind manner. Participants were instructed to abstain from caffeine and smoking for a minimum of two hours before testing. The experimental task on both appointments started roughly 120 min after drug administration, as this is when MPH plasma levels peak (MPH plasma levels peak around 1–3 h, with maximum drug concentration at about 2 h after oral administration79,80). A visual summary is provided in Fig. 5.

Illustrated is a visual summary of all methods and analyses applied in the current study. The top part depicts the timeline of an experimental session, showing the sequence and duration of key interventions. The horizontal axis marks time in minutes. Each session began with administering either a dose of MPH or a placebo, depending on the participants’ subgroup. Before starting the experimental task and EEG recording, participants received active/real tDCS on one appointment, and sham tDCS on the other (for details see methods section). Behavioral and neurophysiological data collection started 120 min post MPH/placebo administration and lasted approximately 15 min for the task reported in this study. Of note, this was followed by another task (duration ~20 min) that is not reported here. All details are provided in the methods section. The bottom part summarizes the analyses applied from the sensor to the source level. Abbreviations: tDCS (transcranial direct current stimulation), MPH (methylphenidate).
tDCS stimulation
Before the experiment and EEG recording, participants received 20 min of either anodal tDCS or sham stimulation targeting the right inferior frontal gyrus (rIFG), as shown in Fig. 5. Following previous studies29,81,82, the rIFG was identified as the midpoint between electrodes FC4 and F8, corresponding to the midpoint of the anode in our setup. The cathode (reference electrode) was positioned contralaterally between the neck and deltoid muscle. Anodal and sham stimulation were administered via two 5 × 5 cm² rubber electrodes (NeuroConn, Ilmenau, Germany) using a NeuroConn DC-Stimulator Plus device (NeuroConn, Ilmenaum Germany). Ten20 conductive paste (0.5 mm thick, customized casing4) ensured optimal conductivity and kept impedances below 5 kΩ. The current was ramped up and down over 15 sec to minimize possible discomfort, with active stimulation lasting 1200 s (20 min) at 2 mA. For the sham condition, a 2-mA current was applied for 15 s and then tapered off for 15 s to mimic the initial tingling of active tDCS. Both the tDCS protocols included identical waiting and preparation periods preceding the experiment. While the administration of MPH/placebo was double-blind, the experimenter could not be blinded to the tDCS manipulation, as they had to manually start the active or sham stimulation on the tDCS device. This detail was not disclosed to the participants to minimize potential biases. The electrical potential induced by the tDCS using the specified electrode configuration was calculated using the MATLAB toolbox “COMETS2”83 and is depicted in Fig. 6.

The EP induced by anodal tDCS with the described electrode configuration was computed using the “COMETS2” toolbox83. The anode (5 × 5 cm) was positioned above the rIFG, centered between electrodes FC4 and F8 (red patch in the right image). The reference electrode was positioned contralaterally between the neck and deltoid muscle. The input current was 2 mA, with colors denoting simulated electrical potential. Abbreviations: tDCS (transcranial direct current stimulation), rIFG (right inferior frontal gyrus), mA (milliampere).
Experimental task
The task design and structure are described and depicted in Fig. 7. The experimental task was adapted from Boy et al.35 and is identical to the paradigm utilized in previous studies6,34,47. This task allows for the examination of subconsciously and consciously evoked conflicts in response selection by combining the target stimulus with subliminal prime and flankers, respectively.

Illustrated is an exemplary trial configuration. Each trial began with a fixation cross displayed for 100 ms. This was followed by a prime (central arrow) for 30 ms and a mask (randomly allocated lines) for 30 ms. The target (central arrow) and flankers were presented for 100 ms, after which the screen turned black. Primes aligning with the target arrow were labeled compatible, while those in the opposite direction were incompatible. Similarly, flankers matching the target arrows’ direction were classified as congruent, and those pointing in opposite directions as incongruent.
Participants were seated approximately 60 cm from a 24-inch CRT monitor, which displayed stimuli against a black background. Manual responses were collected using the “Ctrl” buttons on a standard QWERTZ keyboard. “Presentation” software (Version 18.3 by Neurobehavioral Systems, Inc.) managed stimulus presentation, response recording, and EEG synchronization. Each trial began with a central white fixation cross for 100 ms, followed by a subliminal prime (a white arrow pointing left or right) displayed centrally for 30 ms. Immediately after the prime, a mask stimulus (randomly distributed white lines) was shown for 30 ms. This resulted in a stimulus onset asynchrony (SOA) of 60 ms between the onsets of the subliminal prime and the target arrow. Subsequently, the target (a central white arrow pointing either left or right) and two flankers (white arrows positioned above and below the target arrow) were presented simultaneously for 100 ms. Participants were instructed to focus on the central target arrow and ignore the flankers. They were then asked to indicate the direction of the central target arrow by pressing the left “Ctrl” button with their left index finger for a left-pointing target arrow, or the right “Ctrl” button with their right index finger for a right-pointing target arrow. Each trial ended with the participant’s first response or 2000 ms after target onset. If no response was recorded within this time frame, the trial was marked as a “miss”. The response-stimulus interval (RSI) between the participant’s first response and the onset of the following trial varied randomly between 1000 and 1200 ms. Trials were categorized based on the direction of both the prime and target arrows. When the prime and target arrows pointed in the same direction, the trial was labeled as “compatible”. Conversely, if they pointed in opposite directions, the trial was labeled “incompatible”. Additionally, trials were classified as “congruent” when the flanker and target arrow pointed in the same direction, and as “incongruent” when they pointed in opposite directions. This classification resulted in four conditions: compatible-congruent, incompatible-congruent, compatible-incongruent, and incompatible-incongruent.
Each participant completed 384 trials, equally distributed across four blocks (96 trials per block). Within each block, all possible combinations of prime compatibility, flanker congruency, and target direction were randomized and presented at equal frequencies. At the first appointment, participants completed a practice run of 16 trials to familiarize themselves with the task immediately after MPH/placebo administration (i.e., before the potential onset of full MPH drug effects). Participants were instructed to respond as quickly and precisely as possible. After each block (96 trials), participants could take a self-timed break (i.e., to rest their eyes), and resume via button press. The experiment took on average approximately 15 min to complete.
EEG recording and analysis
EEG signals were recorded from 60 Ag/AgCl electrodes in equidistant positions, as in previously published publications54,84. The EEG preprocessing was performed using the Automagic toolbox85 and the EEGLAB toolbox86 in Matlab 2020a (The MathWorks Corp.):
The participants’ EEG signals were recorded from 60 Ag/AgCl electrodes in equidistant positions with a “QuickAmp” amplifier (Brain Products GmbH, Gilching, Germany) and the “BrainVision Recorder” software (Version 2.2), as in previous publications from our research group54,84. For this, 60 Ag/AgCl electrodes in equidistant positions were used. The ground electrode was positioned at the coordinates θ = 58, φ = 78, and the reference at Fpz (θ = 90, φ = 90). EEG signals were initially recorded at a sampling rate of 500 Hz, while electrode impedances were kept below 10 kΩ. First, EEG data were down-sampled to 256 Hz, and flat channels were removed (i.e., channels that showed activity below 5 µV for more than 5 sec). The remaining channels were then re-referenced to an average reference. Subsequently, the PREP preprocessing pipeline87 was applied, which removes line noise (for data recorded in Europe: 50 Hz) using a multi-taper algorithm. After removing contaminations by noisy/bad channels (using high and minimum variance criterion), a robust common average reference was applied. EOG artifacts were removed using a subtraction method, i.e., EOG Regression88. Subsequently, the EEGLABs pop_eegfiltnew() pipeline was used to apply a high pass filter (cutoff frequency: 0.5 Hz) and low pass filter (cutoff frequency: 40 Hz); the filter order was estimated by default. Remaining artifactual source components in the data were detected by applying the Multiple Artifact Rejection Algorithm (MARA89), which automatizes independent component analyses (ICA). For the ICA, the data was temporarily high pass filtered with 1 Hz, but this option was not applied to the final pre-processed data. In the final step, removed/missing channels were interpolated using a spherical method.
After visually inspecting each dataset, the preprocessed data was imported into the FieldTrip toolbox90 for further analysis. The EEG data was segmented in a target-locked manner into the four trial conditions: compatible prime - congruent flanker, incompatible prime - congruent flanker, compatible prime - incongruent flanker, and incompatible prime - incongruent flanker. Only correct trials were considered for the subsequent analyses.
To examine alpha-band (8–12 Hz) and theta-band (4–7 Hz) activity during these conditions, time-frequency (TF) decomposition was performed using Morlet wavelets (with a width parameter of 5). The average power in the alpha and theta frequency bands was computed for each electrode and time point. Only significant and most relevant behavioral effects were further investigated at the neurophysiological level. For this approach, cluster-based permutation tests (CBPTs) were conducted to identify clusters of electrodes with significant differences between congruent and incongruent flanker trials in case of incompatible primes, as well as to identify significant differences between compatible and incompatible prime trials in case of incongruent flankers. The CBPTs were performed separately for each frequency band within 0-1000 ms following target arrow stimulus onset using 1000 Monte Carlo randomizations and a cluster-alpha level of p = .05 (two-tailed). Analyses were conducted separately for placebo and MPH groups for the active tDCS appointment.
Source estimation and beamforming analysis
The neuroanatomical sources that reflect the prime effect (i.e., compatible minus incompatible) with incongruent flankers and the flanker effect (i.e., the congruent minus incongruent) with incompatible primes in the alpha and theta band were reconstructed following a previously established beamforming procedure39. First, a Dynamic Imaging of Coherent Sources (DICS) beamformer91 was used to identify neuroanatomical sources of substantial differences between conditions of interest in alpha and theta band activity. The source localization results were projected onto an equally spaced 0.5 cm grid created from the forward model template provided by the FieldTrip toolbox, based on the standard MNI (Montreal Neurological Institute) space. Power in the alpha and theta bands were extracted for the period following the presentation onset of the target stimulus. For both alpha and theta source power differences, corresponding contrasts were calculated and normalized on the total power of the two conditions as a ratio55:
Next, clusters of both frequency bands were identified by applying the density-based spatial clustering of applications with noise (DBSCAN92) algorithm as employed in MATLAB, comparable to previous studies39,93. The DICS beamforming results were restricted to negative ratios, indicating that alpha and theta power were higher in incompatible > compatible and incongruent > congruent trials. The negative top 2% of the power distribution in the prime and flanker effect ratio within labeled regions on the automated anatomical labeling atlas94 were submitted to the DBSCAN, restricting the analysis to the voxels with the largest negative differences. An epsilon of 1.5 the edge length of each voxel was used to detect neighboring voxels. The resulting clusters (minimum five voxels) were visually inspected.
Statistics and reproducibility
We provide a power analysis justifying the recruited sample size (see section on participants for details). The behavioral data (i.e., response accuracy and reaction times) was analyzed using repeated measured ANOVAs using SPSS version 29.0.0.0 (IBM Corp., Armonk, N.Y., USA). As within-subject factors, the “tDCS” (active tDCS vs. sham), “prime compatibility” (compatible vs. incompatible), and “flanker congruency” (congruent vs. incongruent) were used. The between-subject factors were “pharmacological group” (placebo vs. MPH) and “order of stimulation” (active tDCS on the first appointment vs. active tDCS on the second appointment). Significant main or interaction effects were examined with post hoc ANOVAs and post-hoc t-tests. Given that post hoc tests were only conducted when a justifying significant interaction had been obtained in the ANOVA, post hoc tests were not corrected for multiple testing. Only correct trials, with response times (RTs) between min. 100 ms and max. 1000 ms after the target arrow onset, were included in the subsequent analyses. When a participant’s behavioral accuracy was below chance level (<50%) in two or more task conditions, or average response times were <100 ms/>1000 ms, that case was marked as an outlier, and no longer considered for all subsequent analyses of the behavioral and neurophysiological data. Descriptive data are given as mean and standard error of the mean (SEM). We used cluster-based permutation tests for the EEG data analysis (see section on EEG recording and analysis). The tDCS approach was based on prior research and a modeling of the tDCS current. EEG-beamforming analysis was only performed for contrasts for the cluster-based permutation testing revealed robust effects and according to previously published protocols.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
All data from this study are publicly accessible at the following link: https://osf.io/wexgu/95. For any additional inquiries, please contact Anna Helin Koyun (AnnaHelin.Koyun@ukdd.de).
Code availability
The custom scripts used for EEG data processing are available for download at: https://osf.io/wexgu/.
References
Servan-Schreiber, D., Printz, H. & Cohen, J. D. A network model of catecholamine effects: gain, signal-to-noise ratio, and behavior. Science 249, 892–895 (1990).
Yousif, N. et al. Dopamine activation preserves visual motion perception despite noise interference of human V5/MT. J. Neurosci. 36, 9303–9312 (2016).
Li, S. C., Lindenberger, U. & Sikström, S. Aging cognition: from neuromodulation to representation. Trends Cogn. Sci. 5, 479–486 (2001).
Adelhöfer, N., Mückschel, M., Teufert, B., Ziemssen, T. & Beste, C. Anodal tDCS affects neuromodulatory effects of the norepinephrine system on superior frontal theta activity during response inhibition. Brain Struct. Funct. 224, 1291–1300 (2019).
Adelhöfer, N. et al. The system-neurophysiological basis for how methylphenidate modulates perceptual–attentional conflicts during auditory processing. Hum. Brain Mapp. 39, 5050–5061 (2018).
Bensmann, W., Roessner, V., Stock, A. K. & Beste, C. Catecholaminergic modulation of conflict control depends on the source of conflicts. Int. J. Neuropsychopharmacol. 21, 901–909 (2018).
Molaee-Ardekani, B. et al. Effects of transcranial Direct Current Stimulation (tDCS) on cortical activity: a computational modeling study. Brain Stimul. 6, 25–39 (2013).
Hay, E. & Segev, I. Dendritic excitability and gain control in recurrent cortical microcircuits. Cereb. Cortex 25, 3561–3571 (2015).
Li, S. C. & Rieckmann, A. Neuromodulation and aging: implications of aging neuronal gain control on cognition. Curr. Opin. Neurobiol. 29, 148–158 (2014).
Kuo, M. F. & Nitsche, M. A. Exploring prefrontal cortex functions in healthy humans by transcranial electrical stimulation. Neurosci. Bull. 31, 198–206 (2015).
Nitsche, M. A. & Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J. Physiol. 527, 633–639 (2000).
Lafon, B., Rahman, A., Bikson, M. & Parra, L. C. Direct current stimulation alters neuronal input/output function. Brain Stimul. 10, 36–45 (2017).
Yamada, Y. & Sumiyoshi, T. Neurobiological mechanisms of transcranial direct current stimulation for psychiatric disorders; neurophysiological, chemical, and anatomical considerations. Front Hum. Neurosci. 15, 631838 (2021).
Kemmotsu, N., Villalobos, M. E., Gaffrey, M. S., Courchesne, E. & Müller, R. A. Activity and functional connectivity of inferior frontal cortex associated with response conflict. Cogn. Brain Res. 24, 335–342 (2005).
Sheu, Y. S. & Courtney, S. M. A neural mechanism of cognitive control for resolving conflict between abstract task rules. Cortex 85, 13–24 (2016).
Hampshire, A., Chamberlain, S. R., Monti, M. M., Duncan, J. & Owen, A. M. The role of the right inferior frontal gyrus: inhibition and attentional control. NeuroImage 50, 1313–1319 (2010).
Botvinick, M. M. Conflict monitoring and decision making: Reconciling two perspectives on anterior cingulate function. Cogn., Affect., Behav. Neurosci. 7, 356–366 (2007).
Willemssen, R., Falkenstein, M., Schwarz, M., Müller, T. & Beste, C. Effects of aging, Parkinson’s disease, and dopaminergic medication on response selection and control. Neurobiol. Aging 32, 327–335 (2011).
Beste, C., Willemssen, R., Saft, C. & Falkenstein, M. Response inhibition subprocesses and dopaminergic pathways: Basal ganglia disease effects. Neuropsychologia 48, 366–373 (2010).
Dipasquale, O. et al. Unravelling the effects of methylphenidate on the dopaminergic and noradrenergic functional circuits. Neuropsychopharmacol 45, 1482–1489 (2020).
Faraone, S. V. The pharmacology of amphetamine and methylphenidate: Relevance to the neurobiology of attention-deficit/hyperactivity disorder and other psychiatric comorbidities. Neurosci. Biobehav. Rev. 87, 255–270 (2018).
Kuczenski, R. & Segal, D. S. Effects of Methylphenidate on Extracellular Dopamine, Serotonin, and Norepinephrine: Comparison with Amphetamine. J. Neurochem. 68, 2032–2037 (1997).
Beste, C. et al. Dopamine modulates the efficiency of sensory evidence accumulation during perceptual decision making. Int. J. Neuropsychopharmacol. 21, 649–655 (2018).
Kuo, M. F., Paulus, W. & Nitsche, M. A. Boosting focally-induced brain plasticity by Dopamine. Cereb. Cortex 18, 648–651 (2008).
Monte-Silva, K., Liebetanz, D., Grundey, J., Paulus, W. & Nitsche, M. A. Dosage-dependent non-linear effect of l-dopa on human motor cortex plasticity. J. Physiol. 588, 3415–3424 (2010).
Nitsche, M. A. et al. Catecholaminergic consolidation of motor cortical neuroplasticity in humans. Cereb. Cortex 14, 1240–1245 (2004).
Nitsche, M. A. et al. Dopaminergic modulation of long-lasting direct current-induced cortical excitability changes in the human motor cortex. Eur. J. Neurosci. 23, 1651–1657 (2006).
Fonteneau, C. et al. Frontal Transcranial Direct Current Stimulation Induces Dopamine Release in the Ventral Striatum in Human. Cereb. Cortex 28, 2636–2646 (2018).
Koyun A. H., Wendiggensen P., Roessner V., Beste C., Stock A. K. Effects of catecholaminergic and transcranial direct current stimulation on response inhibition. International Journal of Neuropsychopharmacology. Published online May 14, 2024:pyae023. https://doi.org/10.1093/ijnp/pyae023.
Diamond, A. Executive functions. Annu. Rev. Psychol. 64, 135–168 (2013).
Parkinson, J. & Haggard, P. Subliminal priming of intentional inhibition. Cognition 130, 255–265 (2014).
Mcbride J., Boy F., Husain M., Sumner P. Automatic motor activation in the executive control of action. Front. Hum. Neurosci. 2012;6. https://doi.org/10.3389/fnhum.2012.00082.
Schlaghecken, F. & Eimer, M. Masked prime stimuli can bias quot;freequot; choices between response alternatives. Psychon. Bull. Rev. 11, 463–468 (2004).
Stock, A. K., Friedrich, J. & Beste, C. Subliminally and consciously induced cognitive conflicts interact at several processing levels. Cortex 85, 75–89 (2016).
Boy, F., Husain, M. & Sumner, P. Unconscious inhibition separates two forms of cognitive control. Proc. Natl Acad. Sci. 107, 11134–11139 (2010).
Adelhöfer, N., Stock, A. K. & Beste, C. Anodal tDCS modulates specific processing codes during conflict monitoring associated with superior and middle frontal cortices. Brain Struct. Funct. 226, 1335–1351 (2021).
Cavanagh, J. F. & Frank, M. J. Frontal theta as a mechanism for cognitive control. Trends Cogn. Sci. 18, 414–421 (2014).
Cohen, M. X. & Donner, T. H. Midfrontal conflict-related theta-band power reflects neural oscillations that predict behavior. J. Neurophysiol. 110, 2752–2763 (2013).
Wendiggensen, P., Ghin, F., Koyun, A. H., Stock, A. K. & Beste, C. Pretrial Theta band activity affects context-dependent modulation of response inhibition. J. Cogn. Neurosci. 34, 605–617 (2022).
Klimesch, W. Alpha-band oscillations, attention, and controlled access to stored information. Trends Cogn. Sci. 16, 606–617 (2012).
Klimesch, W. Evoked alpha and early access to the knowledge system: The P1 inhibition timing hypothesis. Brain Res. 1408, 52–71 (2011).
Van Diepen, R. M., Foxe, J. J. & Mazaheri, A. The functional role of alpha-band activity in attentional processing: the current zeitgeist and future outlook. Curr. Opin. Psychol. 29, 229–238 (2019).
Jensen O. & Mazaheri A. Shaping functional architecture by oscillatory alpha activity: gating by inhibition. Front. Hum. Neurosci. 2010;4. https://doi.org/10.3389/fnhum.2010.00186.
Zhou, Y. J., Iemi, L., Schoffelen, J. M., de Lange, F. P. & Haegens, S. Alpha oscillations shape sensory representation and perceptual sensitivity. J. Neurosci. 41, 9581–9592 (2021).
Pertermann, M., Mückschel, M., Adelhöfer, N., Ziemssen, T. & Beste, C. On the interrelation of 1/ f neural noise and norepinephrine system activity during motor response inhibition. J. Neurophysiol. 121, 1633–1643 (2019).
Bluschke, A., Friedrich, J., Schreiter, M. L., Roessner, V. & Beste, C. A comparative study on the neurophysiological mechanisms underlying effects of methylphenidate and neurofeedback on inhibitory control in attention deficit hyperactivity disorder. Neuroimage Clin. 20, 1191–1203 (2018).
Bensmann, W., Zink, N., Roessner, V., Stock, A. K. & Beste, C. Catecholaminergic effects on inhibitory control depend on the interplay of prior task experience and working memory demands. J. Psychopharmacol. 33, 678–687 (2019).
Mückschel, M., Eggert, E., Prochnow, A. & Beste, C. Learning experience reverses catecholaminergic effects on adaptive behavior. Int. J. Neuropsychopharmacol. 23, 12–19 (2020).
Mückschel, M., Roessner, V. & Beste, C. Task experience eliminates catecholaminergic effects on inhibitory control – A randomized, double-blind cross-over neurophysiological study. Eur. Neuropsychopharmacol. 35, 89–99 (2020).
Eggert, E. et al. Perception-action integration is modulated by the catecholaminergic system depending on learning experience. Int. J. Neuropsychopharmacol. 24, 592–600 (2021).
Nikolin, S., Martin, D., Loo, C. K. & Boonstra, T. W. Effects of TDCS dosage on working memory in healthy participants. Brain Stimulation 11, 518–527 (2018).
Röhner F. et al. Modulation of working memory using transcranial electrical stimulation: a direct comparison between TACS and TDCS. Front Neurosci. 2018;12. https://doi.org/10.3389/fnins.2018.00761.
Cohen, M. X. A neural microcircuit for cognitive conflict detection and signaling. Trends Neurosci. 37, 480–490 (2014).
Koyun A. H. et al. Interactions of Catecholamines and GABA+ in Cognitive Control: Insights from EEG and 1H-MRS. NeuroImage. Published online April 26, 2024:120619. https://doi.org/10.1016/j.neuroimage.2024.120619.
Mückschel, M., Stock, A. K., Dippel, G., Chmielewski, W. & Beste, C. Interacting sources of interference during sensorimotor integration processes. NeuroImage 125, 342–349 (2016).
Beste, C., Münchau, A. & Frings, C. Towards a systematization of brain oscillatory activity in actions. Commun. Biol. 6, 1–11 (2023).
Lobier, M., Palva, J. M. & Palva, S. High-alpha band synchronization across frontal, parietal and visual cortex mediates behavioral and neuronal effects of visuospatial attention. NeuroImage 165, 222–237 (2018).
Sadaghiani, S. & Kleinschmidt, A. Brain Networks and α-Oscillations: Structural and Functional Foundations of Cognitive Control. Trends Cogn. Sci. 20, 805–817 (2016).
Bonnefond, M. & Jensen, O. The role of gamma and alpha oscillations for blocking out distraction. Commun. Integr. Biol. 6, e22702 (2013).
Moreau, Q., Candidi, M., Era, V., Tieri, G. & Aglioti, S. M. Midline frontal and occipito-temporal activity during error monitoring in dyadic motor interactions. Cortex 127, 131–149 (2020).
Ramezanpour, H. & Fallah, M. The role of temporal cortex in the control of attention. Curr. Res. Neurobiol. 3, 100038 (2022).
Bensmann, W., Zink, N., Mückschel, M., Beste, C. & Stock, A. K. Neuronal networks underlying the conjoint modulation of response selection by subliminal and consciously induced cognitive conflicts. Brain Struct. Funct. 224, 1697–1709 (2019).
Moss, H. E. et al. Selecting among competing alternatives: selection and retrieval in the left inferior frontal Gyrus. Cereb. Cortex 15, 1723–1735 (2005).
Zhang, J. X., Feng, C. M., Fox, P. T., Gao, J. H. & Tan, L. H. Is left inferior frontal gyrus a general mechanism for selection? NeuroImage 23, 596–603 (2004).
Swick, D., Ashley, V. & Turken, A. U. Left inferior frontal gyrus is critical for response inhibition. BMC Neurosci. 9, 102 (2008).
Oztekin, I., Curtis, C. E. & McElree, B. The medial temporal lobe and the left inferior prefrontal cortex jointly support interference resolution in verbal working memory. J. Cogn. Neurosci. 21, 1967–1979 (2009).
Winocur, G., Moscovitch, M. & Bruni, J. Heightened Interference on Implicit, but Not Explicit, Tests of Negative Transfer: Evidence from Patients with Unilateral Temporal Lobe Lesions and Normal Old People. Brain Cogn. 30, 44–58 (1996).
Herlin, B., Navarro, V. & Dupont, S. The temporal pole: From anatomy to function—A literature appraisal. J. Chem. Neuroanat. 113, 101925 (2021).
Martin, C. B. et al. Resolving cross-modal semantic interference among object concepts requires medial temporal Lobe Cortex. J. Cogn. Neurosci. 35, 869–884 (2023).
Cortese, F. et al. Anodal transcranial direct current stimulation over the left temporal pole restores normal visual evoked potential habituation in interictal migraineurs. J. Headache Pain. 18, 70 (2017).
Simons, J. S. & Spiers, H. J. Prefrontal and medial temporal lobe interactions in long-term memory. Nat. Rev. Neurosci. 4, 637–648 (2003).
Rahman, A., Lafon, B., Parra, L. C. & Bikson, M. Direct current stimulation boosts synaptic gain and cooperativity in vitro. J. Physiol. 595, 3535–3547 (2017).
Beste C. et al. The basal ganglia striosomes affect the modulation of conflicts by subliminal Information - evidence from X-linked dystonia parkinsonism. Cerebral Cortex. 2017;28. https://doi.org/10.1093/cercor/bhx125.
Goschke, T. & Bolte, A. Emotional modulation of control dilemmas: The role of positive affect, reward, and dopamine in cognitive stability and flexibility. Neuropsychologia 62, 403–423 (2014).
Jamil, A. & Nitsche, M. A. What effect does tDCS have on the brain? Basic physiology of tDCS. Curr. Behav. Neurosci. Rep. 4, 331–340 (2017).
Kuo M. F., Polanía R. & Nitsche M. Physiology of Transcranial Direct and Alternating Current Stimulation. In: Brunoni A., Nitsche M., Loo C., eds. Transcranial Direct Current Stimulation in Neuropsychiatric Disorders: Clinical Principles and Management. Springer International Publishing; 2016:29-46. https://doi.org/10.1007/978-3-319-33967-2_3.
Faul, F., Erdfelder, E., Lang, A. G. & Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 39, 175–191 (2007).
Faul, F., Erdfelder, E., Buchner, A. & Lang, A. G. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav. Res Methods 41, 1149–1160 (2009).
Challman, T. D. & Lipsky, J. J. Methylphenidate: Its pharmacology and uses. Mayo Clin. Proc. 75, 711–721 (2000).
Kimko, H. C., Cross, J. T. & Abernethy, D. R. Pharmacokinetics and Clinical Effectiveness of Methylphenidate. Clin. Pharmacokinet. 37, 457–470 (1999).
Jacobson, L., Javitt, D. C. & Lavidor, M. Activation of inhibition: diminishing impulsive behavior by direct current stimulation over the inferior frontal gyrus. J. Cogn. Neurosci. 23, 3380–3387 (2011).
Stramaccia, D. F., Penolazzi, B., Altoè, G. & Galfano, G. TDCS over the right inferior frontal gyrus disrupts control of interference in memory: A retrieval-induced forgetting study. Neurobiol. Learn Mem. 144, 114–130 (2017).
Lee, C., Jung, Y. J., Lee, S. J. & Im, C. H. COMETS2: An advanced MATLAB toolbox for the numerical analysis of electric fields generated by transcranial direct current stimulation. J. Neurosci. Methods 277, 56–62 (2017).
Koyun, A. H., Stock, A. K. & Beste, C. Neurophysiological mechanisms underlying the differential effect of reward prospect on response selection and inhibition. Sci. Rep. 13, 10903 (2023).
Pedroni A., Bahreini A. & Langer N. Automagic: Standardized Preprocessing of Big EEG Data. Published online June 18, 2019:460469. https://doi.org/10.1101/460469.
Delorme, A. & Makeig, S. EEGLAB: an open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J. Neurosci. Methods 134, 9–21 (2004).
Bigdely-Shamlo, N., Mullen, T., Kothe, C., Su, K. M. & Robbins, K. A. The PREP pipeline: standardized preprocessing for large-scale EEG analysis. Front Neuroinform. 9, 16 (2015).
Parra, L. C., Spence, C. D., Gerson, A. D. & Sajda, P. Recipes for the linear analysis of EEG. NeuroImage 28, 326–341 (2005).
Winkler, I., Haufe, S. & Tangermann, M. Automatic classification of artifactual ICA-components for artifact removal in EEG signals. Behav. Brain Funct. 7, 30 (2011).
Oostenveld, R., Fries, P., Maris, E. & Schoffelen, J. M. FieldTrip: Open Source Software for Advanced Analysis of MEG, EEG, and Invasive Electrophysiological Data. Comput. Intell. Neurosci. 2011, 156869 (2011).
Gross, J. et al. Dynamic imaging of coherent sources: Studying neural interactions in the human brain. Proc. Natl Acad. Sci. 98, 694–699 (2001).
Ester M., Kriegel H. P., Sander J. & Xu X. A. Density-Based Algorithm for Discovering Clusters in Large Spatial Databases with Noise. 96:226–231 (1996).
Adelhöfer, N. & Beste, C. Pre-trial theta band activity in the ventromedial prefrontal cortex correlates with inhibition-related theta band activity in the right inferior frontal cortex. NeuroImage 219, 117052 (2020).
Tzourio-Mazoyer, N. et al. Automated Anatomical Labeling of Activations in SPM Using a Macroscopic Anatomical Parcellation of the MNI MRI Single-Subject Brain. NeuroImage 15, 273–289 (2002).
Koyun, A. H. & Stock A. K. Neurophysiological Insights into Catecholamine-Dependent tDCS Modulation of Cognitive Control [Data set]. Open Science Frameworf: https://doi.org/10.17605/OSF.IO/WEXGU.
Acknowledgements
This work was supported by a grant from the Deutsche Forschungsgemeinschaft (DFG) SFB 940 project B8 and by a Grant from the Federal Ministry of Education and Research (Bundesministerium für Bildung und Forschung, BMBF) as part of the German Center for Child and Adolescent Health (DZKJ) under the funding code 01GL2405B.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
Anna Helin Koyun: Data collection; Formal analysis; Methodology; Visualization; Writing—Original draft. Paul Wendiggensen: Methodology. Veit Roessner: Conceptualization; Funding acquisition. Christian Beste: Conceptualization; Funding acquisition; Project administration; Supervision. Ann-Kathrin Stock: Conceptualization; Data curation; Funding acquisition; Project administration; Supervision; Writing—Original draft.
Corresponding author
Ethics declarations
Competing interests
Christian Beste is an Editorial Board Member for Communications Biology, but was not involved in the editorial review of, nor the decision to publish this article. All other authors have nothing to disclose.
Peer review
Peer review information
Communications Biology thanks Miles Wischnewski and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary Handling Editor: Jasmine Pan.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Koyun, A.H., Wendiggensen, P., Roessner, V. et al. Neurophysiological insights into catecholamine-dependent tDCS modulation of cognitive control. Commun Biol 8, 375 (2025). https://doi.org/10.1038/s42003-025-07805-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s42003-025-07805-6
