
Abstract
CDKN2A is a tumor suppressor located in chromosome 9p21 and frequently lost in Barrett’s esophagus (BE) and esophageal adenocarcinoma (EAC). How CDKN2A and other 9p21 gene co-deletions affect EAC evolution remains understudied. We explored the effects of 9p21 loss in EACs and cancer progressor and non-progressor BEs with matched genomic, transcriptomic and clinical data. Despite its cancer driver role, CDKN2A loss in BE prevents EAC initiation by counterselecting subsequent TP53 alterations. 9p21 gene co-deletions predict poor patient survival in EAC but not BE through context-dependent effects on cell cycle, oxidative phosphorylation and interferon response. Immune quantifications using bulk transcriptome, RNAscope and high-dimensional tissue imaging showed that IFNE loss reduces immune infiltration in BE, but not EAC. Mechanistically, CDKN2A loss suppresses the maintenance of squamous epithelium, contributing to a more aggressive phenotype. Our study demonstrates context-dependent roles of cancer genes during disease evolution, with consequences for cancer detection and patient management.
Similar content being viewed by others


Main
CDKN2A is among the most frequently damaged cancer genes, with loss of function (LoF) reported in at least 35 different tumor types across 12 organ systems1. CDKN2A acts as a tumor suppressor by inducing cell cycle arrest and cellular senescence2 as well as preventing angiogenesis3, oxidative stress4, and metastasis2. Additionally, CDKN2A LoF predicts poor patient survival5,6,7.
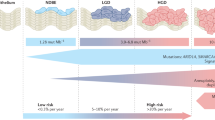
CDKN2A LoF may occur through damaging point mutations, small indels or large deletions of chromosome 9p21.3 locus (hereon 9p21), an event observed in around 15% of cancers8. Depending on their length, 9p21 deletions may involve up to 26 genes, including other cell cycle regulators (CDKN2B and KLHL9), a metabolic enzyme (MTAP) and a cluster of 16 type I interferons (Fig. 1a). Recently, the loss of the whole locus, rather than CDKN2A alone, has been associated with poor survival and resistance to immunotherapy, possibly through the onset of an immune-cold tumor microenvironment (TME)8.

a, Gene composition of chromosome 9p21 locus. b, Canonical EAC drivers damaged in at least 5% of EACs (n = 1,032 patients). All cell cycle regulators are reported in bold. c, Alterations in cell cycle regulators in BE and EAC. CDKN2A gene products (p14-ARF and p16-INK4a) regulate the cell cycle through the E2F genes93. p14-ARF blocks MDM2 and TP53 degradation, which induces CDKN1A transcription. CDKN1A in turn inhibits the CCNE1/CDK2 complex ultimately blocking cell cycle through E2F1 inhibition. p16-INK4a directly inhibits the CCND/CDK6/CDK4 complex preventing RB1 phosphorylation. Unphosphorylated RB1 can bind E2F1, leading to cell cycle arrest. CDKN2A LoF favors cell cycle progression resulting in uncontrolled cell proliferation. Values within the circle represent the proportion of EACs, P-BEs and NP-BEs with at least one damaged cell cycle regulator (except TP53). d, Canonical EAC drivers damaged in at least 5% of P-BEs (n = 257 patients). e, Paired BE-EACs (n = 66 patients) with CDKN2A LoF. Clonally related alterations refer to either identical CDKN2A alterations in both lesions or CDKN2A alterations in BE that could further evolve in EAC. f, Canonical drivers damaged in at least 5% of NP-BEs (n = 99 patients). Alteration frequency of EAC canonical drivers in b, d and f is indicated in brackets. The alteration frequency of all EAC drivers in the three cohorts is available in Supplementary Table 2. FHCRC, Fred Hutchinson Cancer Research Center; LoF, loss of function; MSKCC, Memorial Sloan Kettering Cancer Center; NP-BE, non-progressor Barrett’s esophagus; EAC, esophageal adenocarcinoma; P-BE, progressor Barrett’s esophagus; SNV, single-nucleotide variant; TCGA, The Cancer Genome Atlas; UoC, University of Cambridge.
Dissecting the consequences of individual 9p21 gene losses is not straightforward because of their co-occurrence. Recently, the induction of different 9p21 deletions in pancreatic cancer mouse models enabled observation of reduced CD8+ T cell infiltration only when the IFN cluster was co-deleted with CDKN2A, CDKN2B and MTAP9. IFNE, one of the 9p21 type-I interferons (Fig. 1a), is a tumor suppressor in ovarian cancer10, and IFNE treatment promotes CD8+ T cell activation while reducing T regulatory cells (Treg cells) and myeloid-derived suppressor cells (MDSCs)10. Also, MTAP can regulate CD8+ and CD4+ T cell infiltration in melanoma mouse models by controlling methylthioadenosine accumulation in their TME11. These studies started to unveil that at least some of the effects previously ascribed to CDKN2A LoF are in fact due to the loss of other 9p21 genes.
CDKN2A LoF has long been known as an early event in the evolution of esophageal adenocarcinoma (EAC), occurring already in its precursor, Barrett’s esophagus (BE)12,13,14,15,16. Consequently, CDKN2A LoF has been proposed to drive EAC initiation by favoring BE clonal selective sweeps and subsequent alterations of additional drivers, most frequently TP53 (refs. 17,18,19,20). Recently, this model has been replaced by an alternative one where early TP53 LoF would enable whole-genome doubling with consequent acquisition of additional drivers21,22. The role of CDKN2A LoF in EAC initiation remains controversial. Some studies reported higher frequency of CDKN2A LoF in BE cases progressing to EAC compared to BEs that did not progress23,24,25,26,27, implying that CDKN2A inactivation favors cancer initiation. Other studies found either no difference between progressor and non-progressor BEs22,28,29,30,31 or a higher frequency of CDKN2A LoF in non-progressor BEs15. This uncertainty raises questions on the role of CDKN2A in BE and EAC evolution. Moreover, very little is known about the function of the remaining 9p21 genes.
Here, we investigated how the loss of CDKN2A and other 9p21 genes affects EAC initiation and progression. We compared genomic, transcriptomic and survival data from large and clinically annotated cohorts of EAC and patients with BE who progressed or did not progress to cancer. We validated the results in vitro and studied the effect of 9p21 loss on BE and EAC TME by high-dimensional tissue profiling coupled with RNAscope. Finally, we rebuilt the causal gene regulatory networks linking CDKN2A gene loss to specific downstream functional effects. Our results suggested that the same genetic alterations of CDKN2A and other 9p21 genes have different effects in different contexts and stages of EAC evolution, with possible implications in patient management.
Results
CDKN2A LoF drives BE and EAC evolution, but not EAC initiation
We collected whole-genome sequencing (WGS), whole-exome sequencing (WES) and gene panel sequencing data for 1,032 EACs from the literature6,32,33,34,35,36,37,38 or sequenced de novo by the Esophageal Cancer Clinical and Molecular Stratification (OCCAMS) Consortium (Supplementary Table 1). Our cohort reflected EAC high male prevalence, with almost 9:1 male-to-female incidence ratio39 (Supplementary Table 1). To ensure consistency, we annotated damaging mutations and copy-number alterations in all datasets using the same approach (Methods and Extended Data Fig. 1a–e). Because CDKN2A can be silenced also via epigenetic modifications, we analyzed methylation data for a subset of EACs32,40 (Supplementary Table 1). We then identified the damaged drivers in each sample using a curated list of 54 known (canonical) EAC drivers (Supplementary Table 2). In agreement with previous studies29,32,41, CDKN2A was the second most frequently damaged EAC driver, with LoF in 25% of samples (Fig. 1b). More than 56% of EACs (90% considering also TP53) had damaging alterations in other cell cycle regulators (Fig. 1c and Supplementary Table 2), suggesting that cell cycle disruption is key in EAC evolution but does not always involve CDKN2A.
Next, we measured the frequency of CDKN2A LoF in 257 BEs that progressed to high-grade dysplasia or EAC (P-BEs), again sequenced for this study or gathered from published datasets15,40,42,43,44 (Supplementary Table 1 and Extended Data Fig. 1f–j). CDKN2A LoF occurred significantly more frequently in P-BE than EAC (P = 4 × 10−9, two-sided Fisher’s exact test; Fig. 1d), suggesting that EAC does not always originate from a CDKN2A-damaged BE. To further investigate this, we analyzed 66 matched EAC-BE pairs with CDKN2A LoF in BE or EAC (Supplementary Table 1). Only 15 matched lesions had either identical or clonally related CDKN2A alterations (Fig. 1e), confirming that CDKN2A LoF is not required for precancer to cancer transition. Interestingly, 28 EACs lost CDKN2A independently of the paired BEs (Fig. 1e), suggesting that either EAC developed from a different CDKN2A-damaged BE clone or CDKN2A LoF was acquired after transformation.
Finally, we analyzed 99 BEs that did not progress to high-grade dysplasia or EAC (NP-BEs)15,40,43,44 (Supplementary Table 1 and Extended Data Fig. 1f–j). The frequency of CDKN2A LoF in NP-BE was even higher than P-BE and EAC (P = 3 × 10−3 and P = 3 × 10−13, respectively, two-sided Fisher’s exact test, Fig. 1f). Moreover, although in EAC, the dysregulation of cell cycle could occur through alterations of other genes, CDKN2A was the only gene encoding a cell cycle regulator damaged in BE (Fig. 1d). Therefore, unlike EAC, only CDKN2A LoF is relevant for BE evolution.
As observed previously22,45, P-BEs had significantly more damaged drivers than NP-BEs (P = 7 × 10−6, two-sided Fisher’s exact test; Supplementary Table 2), indicating that EAC initiation requires several driver events, most frequently TP53 complete loss. Given its high recurrence, we used TP53 LoF to assess the role of CDKN2A LoF in EAC initiation calculating the odds of cancer progression based on the mutational status of CDKN2A and TP53 in BE. As expected, the odds of cancer progression in BE cases with TP53 LoF was 1 irrespective of CDKN2A status (Supplementary Table 3), confirming that TP53 is a strong driver of EAC initiation. However, the odds of cancer progression in BEs with CDKN2A LoF and wild-type TP53 was lower than those of BEs with both wild-type genes (0.58 and 0.72, respectively; Supplementary Table 3). This suggested that an early occurrence of CDKN2A LoF in BE may reduce the likelihood of EAC initiation. To test this further, we compared two logistic regression models, one assuming a role in EAC initiation only for TP53 LoF (model 1) and the other for both TP53 and CDKN2A LoFs (model 2; Methods). Model 2 was a significantly better predictor of EAC initiation than model 1 (P = 0.01, ANOVA test), with expected occurrences of P-BEs with any status of TP53 and CDKN2A perfectly matching the observed occurrences (Supplementary Table 3). The negative β coefficient of CDKN2A in model 2 further confirmed that CDKN2A LoF may reduce risk of cancer progression (Methods and Supplementary Table 3).
TP53 loss reduces proliferation of CDKN2A LoF BE cells
Next, we set out to investigate how CDKN2A LoF in BE could prevent EAC initiation. As the proportion of BEs with both CDKN2A and TP53 LoF was significantly lower than that of BEs with CDKN2A LoF only (P = 0.05, two-sided Fisher’s exact test; Fig. 2a), we hypothesized that negative selection might act on BE cells losing both genes. To test this hypothesis, we compared CDKN2A and TP53 LoF clonality in 580 EACs with WGS or WES data, as clonality informs on when alterations are acquired during cancer evolution. Despite the well-known EAC intratumor heterogeneity14, CDKN2A or TP53 LoFs were clonal in almost 70% of EACs (397/580), confirming that both alterations are early events. However, EACs with fully clonal CDKN2A LoF were significantly fewer than those with fully clonal TP53 LoF (P = 0.001, two-sided Fisher’s exact test; Fig. 2b), suggesting that overallTP53 LoF tends to predate CDKN2A LoF. In support of this, CDKN2A LoF occurred before TP53 LoF in only 6% of the 47 EACs with LoF alterations in both genes as compared to 38% where TP53 LoF occurred before that of CDKN2A (Fig. 2c). This finding confirmed that the subsequent loss of TP53 in the presence of CDKN2A LoF is a rare event, suggesting that it might be selected against.

a, Frequency of CDKN2A LoF in 356 BEs (n = 257 P-BE and n = 99 NP-BE individuals, respectively) with or without TP53 LoF. Statistical significance was assessed using a two-sided Fisher’s exact test (P = 0.05). b, Frequency of EACs with clonal LoF alterations in CDKN2A and TP53 genes. For this analysis, n = 580/779 patients with EAC with WGS or WES data and LoF in these genes were considered. Statistical significance was assessed using a two-sided Fisher’s exact test (P = 0.001). c, Frequency of EACs with clonal and subclonal LoF alterations in CDKN2A and TP53 genes in n = 47 patients with WGS or WES data and damaging alterations in both genes. d, CDKN2A and TP53 gene expression levels quantified by RT–qPCR of RNA from TP53 wild-type CP-A cells (CP-A_TP53wt), three TP53 KO clones (CP-A_2c8, CP-A_3d2, CP-A_5f4) and control RNA relativized to ACTB expression. One biological replicate was performed with three technical replicates. e, TP53 gene structure in CP-A_TP53wt, CP-A_2c8, CP-A_3d2 and CP-A_5f4 cells. Exon-intron arrangement was derived from the UCSC genome browser (https://genome.ucsc.edu/) based on NM_000546 mRNA sequence (chr17:7,668,421-7,687,490, hg38 assembly). Dotted lines represent edited regions. f, Growth curves of CP-A_TP53wt, CP-A_2c8, CP-A_3d2 and CP-A_5f4 cells. Proliferation was assessed every 24 h and normalized to time zero. Mean values at 72 h were compared by two-tailed Student’s t-test (P = 1 × 10−4, 8 × 10−6 and 2 × 10−7, respectively). Error bars show standard deviation. Three biological replicates were performed, each in two to four technical replicates. ctrl, control; KO, knockout; P-BE, progressor Barrett’s esophagus; RLU, relative light unit; RT–qPCR, real-time quantitative PCR; RQ, relative quantification; UTR, untranslated region; wt, wild type.
Interestingly, BAR-T cells, derived from BE with constitutive loss of CDKN2A, increase cell doubling times upon TP53 knockdown46, supporting the hypothesis that the additional loss of TP53 reduces cell growth rate. To test this experimentally, we induced TP53 knockout (KO) in metaplastic BE CP-A cells derived from a male individual with CDKN2A LoF and wild-type TP53 (ref. 47). First, we confirmed that CP-A cells expressed TP53 but did not express CDKN2A (Fig. 2d). We then used CRISPR-Cas9 to edit TP53 (Supplementary Table 4) and performed single cell cloning to expand cell colonies. To control for off target effects and clonal differences, we selected three clones with a partial deletion of TP53 exons 5 and 6 (Fig. 2e), as assessed via amplicon sequencing (Supplementary Table 4). We confirmed that these clones did not express CDKN2A nor TP53 (Fig. 2d). The fact that we could isolate clones losing both genes implied that BE cells with CDKN2A LoF can survive subsequent TP53 loss. However, compared to TP53 wild-type CP-A cells, all three TP53 KO CP-A clones showed significantly slower growth rate that was already visible after 72 h (two-sided t-test test, Fig. 2f).
This finding was in line with the reported increase in cell doubling times of TP53 knockdown BAR-T cells46 and supported the tumor-preventive role of early CDKN2A inactivation due to the reduced fitness, defined as proliferative capacity, of cells additionally losing TP53.
LoF of 9p21 genes predicts poor survival in EAC, but not in BE
Because CDKN2A LoF has been associated with poor patient survival5,6,7, we investigated the survival effect of CDKN2A and other 9p21 gene LoF in our extended BE and EAC cohorts. Patients with EAC and CDKN2A LoF showed significantly worse survival than those with the wild-type gene (Fig. 3a). This difference held true even when patients with CDKN2A homozygous deletions (Fig. 3b) or damaging mutations (Fig. 3c) were considered separately. However, we did not observe lower survival in patients with CDKN2A heterozygous deletions only (Extended Data Fig. 2a), suggesting that CDKN2A complete loss is required to affect prognosis. Damaging alterations in TP53 or other cell cycle regulators had no effect on survival (Extended Data Fig. 2b–f) despite their frequent EAC alterations (Fig. 1c). Therefore, the survival effect of CDKN2A LoF does not depend on its function as cell cycle regulator. Moreover, CDKN2A LoF was not a predictor of worse survival in P-BE (Fig. 3d), again suggesting context-dependent consequences of its loss.

a–c, Kaplan–Meier survival curves of n = 1,032 patients with EAC with wild-type CDKN2A compared to those with all types of LoFs (P = 2 × 10−4) (a), only homozygous deletions (P = 6 × 10−3) (b) and only LoF mutations (P = 3 × 10−3) (c). d, Kaplan–Meier survival curves of n = 129 patients with P-BE with and without CDKN2A LoF. Log-rank method was used to estimate the P values. ns, not significant. e, Approach to test the effect of the co-damage in 9p21 genes on patient survival. Only n = 779 patients with EAC with WGS or WES data were used for the survival analysis, whereas n = 337 patients with RNA-seq data were used to measure 9p21 gene expression. Letters correspond to the 26 genes according to their order in the chromosomal locus. f, LoF frequency of 9p21 genes in n = 779 patients with EAC. g, Distribution of normalized expression values in the 9p21 genes in n = 337 patients with EAC. Boxplot shows first and third quartiles, whiskers extend to the lowest and highest value within the 1.5× interquartile range and the line indicates the median. h, Kaplan–Meier survival analysis of patients with EAC with co-alterations in the ten expressed 9p21 genes and n = 413 patients with EAC with a wild-type locus. Only groups with significantly poor survival (FDR < 0.1) are shown and genes of interest are outlined in black. All groups used in the analysis are listed in Supplementary Table 5. The minimum and maximum number and percent of damaged EACs in f and h are reported in the corresponding heatmap. HD, homozygous deletion; WES, whole-exome sequencing; WGS, whole-genome sequencing. Cartoon in (e) was created with BioRender.com.
We then investigated whether the co-occurring loss of other 9p21 genes could also contribute to poor survival, restricting the analysis to 779 EACs with WGS or WES data (Fig. 3e). Although CDKN2A was the most frequently occurring alteration in the locus, confirming that it is the event under positive selection, the other 25 genes were frequently co-lost with it (Fig. 3f). However, only ten 9p21 genes were expressed in EAC (Fig. 3g) or normal esophagus (Extended Data Fig. 3), suggesting that the loss of the remaining 16 genes likely had no functional consequences. We therefore tested the potential impact on survival of the ten 9p21 expressed genes by dividing patients with EAC in nine groups. Each of these groups represented at least 5% of the cohort and was composed of patients with the same 9p21 mutation and copy-number profile (Supplementary Table 5). Patients in all nine groups had worse survival than 413 patients with EAC with a wild-type 9p21 locus (FDR < 0.1; Fig. 3h and Supplementary Table 5). All patients lost KLHL9, IFNE, MTAP, CDKN2A, CDKN2B and DMRTA1 (Fig. 3h), suggesting that alterations in these genes may contribute to poor prognosis.
LoF of 9p21 genes has distinct consequences in BE and EAC
Our results suggested that the LoFs of CDKN2A and other 9p21 genes have functional and survival consequences that depend on time and context. Disentangling these variable effects is challenging because 9p21 genes are often co-damaged (Fig. 3f). To tease out the contribution of individual 9p21 genes, we divided 22 NP-BEs, 108 P-BEs and 337 EACs with matched genomic and transcriptomic data (Supplementary Table 1) into four groups (Fig. 4a). Each group had the same LoF profile of the six genes whose loss impacted survival (KLHL9, IFNE, MTAP, CDKN2A, CDKN2B and DMRTA1; Fig. 3h). Group 1 included all samples with CDKN2A LoF independently of the status of the other genes (Fig. 4b), closely resembling the cohorts tested in the survival analysis (Fig. 3a,d). The other three groups were subsets of group 1 with variable LoF frequency in the six genes (Fig. 4b).

a, Frequency of damaged 9p21 genes in the four groups estimated over n = 22 patients with NP-BE, n = 108 patients with P-BE and n = 337 patients with EAC with matched genomic and transcriptomic data. b, Proportions of samples with LoF in KLHL9 (N), IFNE (T), MTAP (U), and CDKN2B (W) and DMRTA1 (X) over samples with CDKN2A LoF (V) in each group of NP-BEs, P-BEs and EACs. The number of samples in each group and condition is reported. c, Relative proportion of dysregulated pathways in NP-BE, P-BE and EAC cohorts mapping to cell cycle regulation, metabolism, signal transduction, immune response and development. Numbers in brackets represent the number of unique pathways. d–f, Results of pre-ranked GSEA48 showing the normalized enrichment score (NES), FDR and gene ratio (number of leading-edge genes over the total expressed genes) of pathways dysregulated in each group of NP-BEs (d), P-BEs (e) and EACs (f). NES > 0 indicates pathway upregulation, whereas NES < 0 indicates downregulation. P values were estimated by permutation and corrected for multiple testing using the Benjamini–Hochberg method. g,h, Fold change of expression and correlation plot of the shared leading-edge (LE) genes of interferon gamma (g) and alpha (h) response pathways enriched in P-BE and EAC group 2 as compared to 9p21 wild-type samples. Coefficients and associated P values from two-sided Pearson’s correlation test are reported for both pathways. i, Overlap of leading-edge genes between interferon gamma and alpha response pathways enriched in P-BE and EAC group 2. The 19 shared genes are listed. FC, fold change.
We identified the dysregulated biological processes in each group as compared to the corresponding 9p21 wild-type samples by performing a pre-ranked gene set enrichment analysis (GSEA)48 in NP-BEs, P-BEs and EAC separately. Overall, we detected 72, 62 and 28 unique pathways significantly dysregulated (FDR ≤ 0.01) in NP-BE, P-BE and EAC, respectively (Supplementary Table 6). Almost 80% of these pathways mapped to only five biological processes, namely cell cycle regulation, metabolism, immune response, signal transduction, and development. Overall NP-BE and P-BE showed a higher fraction of dysregulated pathways than EAC (Fig. 4c), suggesting that 9p21 LoF had higher impact in premalignant conditions.
As expected, given CDKN2A, CDKN2B and KLHL9 role in cell cycle regulation role, we found cell cycle dysregulation across groups and conditions except group 4 (CDKN2A LoF only; Fig. 4d–f and Supplementary Table 6), suggesting that the co-deletion of KLHL9, CDKN2A and CDKN2B maximizes the effect.
CDKN2A LoF alone might not be sufficient also to trigger metabolic or immune dysregulation (Fig. 4d–f and Supplementary Table 6). In this case MTAP and IFNE LoF could play a role given their functions in metabolic reprogramming49,50 and activation of immune response through metabolic regulation51, respectively. Interestingly, oxidative phosphorylation was consistently downregulated in NP-BE, upregulated in P-BE, and showed no difference in EAC (Fig. 4d–f and Supplementary Table 6). This once again suggested that the same genetic alterations may trigger different functional responses depending on the context. Similarly, the disruption of immune pathways differed between BE and EAC (Fig. 4d–f and Supplementary Table 6). Although interferon alpha and gamma responses were consistently downregulated in NP-BE and P-BE, both were upregulated in EAC, particularly in group 2 (Fig. 4b). Consistently, we observed a significant inverse correlation between expression fold changes of interferon gamma (Fig. 4g) and alpha (Fig. 4h) genes in BE and EAC groups 2 compared to 9p21 wild-type samples. Moreover, there was substantial overlap between altered genes in the two pathways (Fig. 4i), suggesting a comprehensive transcriptional reprogramming of interferon response. The most likely candidates for this reprogramming were again MTAP, given its recently reported ability to regulate the TME11, and IFNE, a type-1 interferon expressed in adult epithelia. Since the effect was most visible in group 2, which had LoF in both genes, and not in group 3, which had MTAP LoF and IFNE wild-type (Fig. 4a,b), the effect on interferon response might be due to IFNE loss.
CDKN2A LoF alone might instead be enough for the pervasive downregulation of keratinization genes given that these pathways were consistently dysregulated also in group 4 (Supplementary Table 6 and Fig. 4d–f).
Loss of IFNE reduces immune infiltration in BE, but not in EAC
To further investigate the opposite effect of IFNE on interferon alpha and gamma response in BE and EAC (Fig. 4g,h), we quantified the infiltration of 18 immune cell populations in NP-BEs, P-BEs and EACs from their bulk transcriptomic data. We then compared the abundance of immune infiltrates between each of the four 9p21 LoF groups (Fig. 4a) and the corresponding 9p21 wild-type samples.
Immune infiltrates were depleted in NP-BE groups 1 to 3 (Fig. 5a and Supplementary Table 7) and P-BE groups 1 and 2 as compared to 9p21 wild-type samples (Fig. 5b and Supplementary Table 7), where the impact of IFNE LoF was more appreciable. This again suggested that the immune depletion is a consequence of IFNE loss consistent with recent observations of a cold TME when IFNE10 or the whole IFN locus9 are lost in melanoma ovarian, or pancreatic cancers (Supplementary Table 8). However, the same studies also reported an increased infiltration of Treg cells, MDSCs and B cells (Supplementary Table 9) that we did not observe (Fig. 5a,b). The TME of group 4 (CDKN2A LoF only) was not significantly different to that of 9p21 wild-type samples in both NP-BE and P-BE, confirming that CDKN2A LoF does not directly interfere with the immune system.

a–c, Comparison of NESs of 18 immune populations between 9p21 LoF and wild-type samples in n = 22 patients with NP-BE (a), n = 108 patients with P-BE (b) and n = 337 patients with EAC (c), respectively. NES distributions were compared using a two-sided Wilcoxon’s rank sum test and corrected for multiple testing using the Benjamini–Hochberg method. Numbers of samples are reported in brackets. Immune populations with significant differences (FDR < 0.1) are outlined in red. d–f, Representative IMC images from group 2 (n = 4 patients, d), group 4 (n = 3 patients, e) and 9p21 wild-type (n = 3 patients, f) EACs showing the expression of 9p21 targeted proteins and mRNAs. Cadherin-1 and pan-keratin denote tumor. Arrows indicate examples of epithelial staining. Scale bar: 200 μm. g, Relative abundance of immune cells over all cells in 9p21 LoF and wild-type EACs. Samples in groups 2 and 4 were pooled together to form group 1 (n = 7 patients). Distributions were compared using a two-sided Wilcoxon rank sum test. h, Relative abundance of CD4+ cells over all CD3+ cells in 9p21 LoF and wild-type EACs. Distributions were compared using a two-sided Wilcoxon rank sum test. i, Median marker intensity across the T cell clusters at a clustering resolution of 0.5. j, UMAP map of 9750 T cells in n = 10 patients with EAC. Cells were grouped in 12 clusters based on the expression of six markers and colored according to the mean intensities of CD3 and CD4. The cluster enriched in group 1 is circled. Boxplots in g and h show first and third quartiles, whiskers extend to the lowest and highest value within the 1.5X interquartile range and the line indicates the median. Samples in groups 2 (n = 4 patients) and 4 (n = 3 patients) were pooled together to form group 1 (n = 7 patients). For 9p21 wt groups n = 3 patients are shown for all populations, except NK and dendritic cells where samples with no staining were removed. DCs, dendritic cells; TAMs, tumour-associated macrophages.
Unlike other cancer types (Supplementary Table 8) and BE (Fig. 5a,b), we did not observe any significant TME difference between 9p21 LoF and wild-type EACs (Fig. 5c and Supplementary Table 7). To investigate this at higher resolution, we performed high-dimensional imaging mass cytometry (IMC) on tissue sections representative of group 1, group 2, group 4 and 9p21 wild-type EACs (Supplementary Table 9). We used a panel of 26 antibodies targeting structural, immune and 9p21-encoded proteins as well as RNAscope probes against IFNE and IFNB1 mRNAs to increase the detection signal (Supplementary Table 10). We confirmed that group 2 lost the expression of all 9p21-encoded proteins in the tumor, whereas group 4 lost CDKN2A only compared to 9p21 wild-type EACs (Fig. 5d–f). Moreover, IFNE was the only interferon clearly expressed in EAC epithelium (Fig. 5d–f).
We performed single-cell segmentation of the IMC images to quantify T cells, NK cells, macrophages, dendritic cells, monocytic (M) and granulocytic (G) MDSCs, and neutrophils (Methods). We then compared the relative abundance of each immune population over all cells in each slide across EAC groups. We confirmed no significant difference in immune infiltration between 9p21 LoF and wild-type EACs, except for a borderline significant enrichment in dendritic cells in groups 1 and 2 (Fig. 5g). We further applied unsupervised clustering to T cells and macrophages, for which we had multiple markers (Supplementary Table 10), to test whether there was any difference in specific subpopulations. Again, we detected no major differences in any subpopulations of macrophages or T cells, except a borderline significant depletion of CD4+ T cells in groups 1 and 2 compared to 9p21 wild-type EAC (Fig. 5h–j). These results confirmed that, unlike BE, the loss of IFNE or any other 9p21 genes does not lead to any major difference in the TME of EAC.
CDKN2A LoF favors squamous to columnar epithelium transition
We observed a pervasive downregulation of processes responsible for terminal differentiation of keratinocytes, such as keratinization and formation of the cornified envelope, across all 9p21 LoF groups (Fig. 4d–f). In particular, P-BE and EAC groups 4 were associated with the downregulation of keratinization, suggesting that CD2KNA LoF alone was sufficient for triggering this process. To gain further mechanistic insights, we rebuilt the gene regulatory network linking CD2KNA LoF to keratinization in P-BE and EAC group 4 (Fig. 6a).

a, Gene regulatory network linking CDKN2A LoF to the downregulation of keratinization genes through TF deregulations. b–d, Distributions of gene expression values of SOX15 in n = 17 patients with P-BE (P = 0.002) (b) and SOX15 (P = 0.04) (c) and TP63 (d) in n = 26 patients with EAC of group 4 and 9p21 wild type (31 P-BE and 184 patients with EAC, respectively). Distributions were compared using two-sided Wilcoxon’s rank sum test. FC and FDR from the differential gene expression analysis with DESeq2 (ref. 77) are also shown. Boxplot shows first and third quartiles, whiskers extend to the lowest and highest value within the 1.5× interquartile range and the line indicates the median. e, Overlap between keratinization genes targeted by SOX15 and TP63 in P-BE and EAC. f,g, Preranked GSEA plots using as signature keratinization genes targeted by SOX15 in P-BE (f) and by SOX15 and TP63 in EAC (g). Genes were ranked from the most upregulated to the most downregulated in group 4 compared to 9p21 wild-type samples. For EAC, only the top 2,000 downregulated genes are shown. h–j, Correlation plots between keratinization GSEA NES and the gene expression values of SOX15 in P-BE (h) and SOX15 (i) and TP63 (j) in EAC. Coefficients and associated P values from two-sided Spearman’s correlation test are reported. k–n, Preranked GSEA plots using gene signatures for quiescent basal cells (k), proliferating basal cells (l), early suprabasal cells (m) and late suprabasal cells (n) in P-BE and EAC group 4. P values in (e–g and k–n) were estimated by permutation. ES, enrichment score; TF, transcription factor; GSEA, gene set enrichment analysis.
Using a three-step protocol (Extended Data Fig. 4a–c and Methods), we identified 8 and 14 causal models in P-BE and EAC, respectively, linking CDKN2A LoF directly to keratinization gene downregulation through the perturbation of two TFs (SOX15 and TP63; Supplementary Table 11). We further confirmed that these TFs were significantly downregulated in P-BE (Fig. 6b) and EAC (Fig. 6c,d) groups 4 as compared to 9p21 wild-type samples. Overall, the gene modules controlled by SOX15 and TP63 included 45 keratinization genes (Supplementary Table 11), 16 (36%) of which were shared across all gene modules and 30 were shared between SOX15 and TP63 (Fig. 6e). Therefore, the downregulation of these two TFs in CDKN2A LoF samples led to a comprehensive downregulation of the keratinization transcriptional program, as confirmed by a pre-ranked GSEA48 using keratinization gene-derived signatures in P-BE (Fig. 6f) and EAC (Fig. 6g). Moreover, SOX15 and TP63 gene expressions were positively correlated with the enrichment score of the keratinization genes (Fig. 6h–j), again confirming that the two TFs control their expression.
SOX15 regulates transcription of a large number of genes specific to esophageal epithelium52, and TP63 is essential for development and maintenance of all stratified epithelia53. The transition from esophageal squamous epithelium to intestinal columnar epithelium is a key feature in the initiation of BE and EAC54. Our data suggest that CDKN2A LoF leads to a downregulation of the transcriptional program responsible for the maintenance of the squamous epithelium more robust and persistent than in CDKN2A wild-type samples. Although this did not prove a direct causative role of CDKN2A LoF, it shows correlation between the two events. To further test the link between CDKN2A LoF and suppression of squamous epithelium, we performed preranked GSEA48 using four independent gene signatures characteristic of cells composing the esophageal epithelium, namely quiescent basal cells, proliferating basal cells, early suprabasal cells and late suprabasal cells55. We observed global downregulation of all four signatures in EAC and quiescent basal cells and late suprabasal cells in P-BE (Fig. 6k–n). These results supported our hypothesis that CDKN2A LoF exacerbates a phenotype typical of EAC and that this may contribute to more aggressive tumors.
Discussion
In this study, we dissected the role of CDKN2A and other 9p21 genes in EAC evolution, from the transformation of premalignant BE to the impact on patient survival.
Despite being an EAC driver, the early loss of CDKN2A has a tumor-suppressive role supported by its higher occurrence in NP-BE than P-BE and EAC. This is consistent with other drivers whose alterations are more frequent in normal tissues than cancer, including ERBB2, ERBB3, KRAS and NOTCH1 (ref. 56). The anti-tumorigenic function of NOTCH1 is exerted through an increased fitness of NOTCH1 mutant cells that outcompete early tumors57. For CDKN2A we propose a different mechanism whereby TP53 mutations reduce the proliferative capacity of CDKN2A mutant BE cells that are therefore counter-selected. As TP53 loss is a strong driver of EAC initiation, the decrease of its occurrence induced by CDKN2A LoF also decreases tumor initiation. Recent studies observed tumor formation upon induction of TP53 and CDKN2A double KO in mouse or human gastroesophageal organoids58,59,60. However, in these studies, TP53 and CDKN2A inactivation was induced concomitantly, that is targeting both genes at the same time. However, in real precancer conditions, such as BE, mutations are acquired over time and cells with different genetic makeup and fitness coexist and compete for nutrient and space. Our results confirm that the order of mutations is key to decide the fate of mutant cells in the initial phases of tumor evolution56.
It is tempting to speculate that the tumor-preventive role of early CDKN2A LoF could be further developed as a marker of favorable prognosis in nondysplastic BE. Endoscopic surveillance of BE is an integral component of the current EAC prevention paradigm, but the rate of progression to EAC is only 0.54/100 patient-years61. Identifying BE cases with a lower risk of progression could substantially improve patient management, decreasing the burden of endoscopy for patients who have low chances to develop cancer.
CDKN2A LoF is the most frequent event in 9p21 locus, implying that the co-occurring loss of other 9p21 genes is due to genetic hitchhiking, with variable effects on cell cycle, oxidative phosphorylation, and interferon response depending on the stage and context of BE and EAC evolution. Most notably, IFNE exerts a tumor-suppressive role in BE, but not in EAC, by reducing IFN response and inducing a cold immune microenvironment. Despite several reports of a lower infiltration of immune cells in cancers with reduced CDKN2A expression62,63, CDKN2A LoF alone does not change the immune composition of BE or EAC TME. This may be due to tumor-specific effects or to the fact that at least some cancer-promoting roles previously attributed to CDKN2A LoF are in fact triggered by the loss of other 9p21 genes.
The association of CDKN2A LoF with bad prognosis is also context dependent and detectable only in patients with EAC. It appears unrelated to the role of CDKN2A in cell cycle since alterations in other cell cycle regulators can drive EAC without affecting survival. A contribution towards a more aggressive EAC phenotype is likely due to a combination of effects, including the pervasive suppression of transcriptional programs responsible for the maintenance of squamous epithelium. Although this is a common feature of BE and EAC54, it is significantly more pronounced when CDKN2A is lost and is achieved through TP63 and SOX15 downregulation. This could be an indirect effect of CDKN2A LoF on the E2F transcriptional program, as iASPP, which controls TP63 expression64, is a target of E2F1 (ref. 65) and SOX15, in turn, is a target of TP63 (ref. 66).
Our study introduces the intriguing concept that the functional consequences of alterations in cancer genes may change during the evolution of disease, from preventing cancer transformation in the premalignant setting to favoring a more aggressive disease at later stages. This fits the emerging scenario whereby the functional consequences of cancer alterations and the fitness provided to the mutant cell are not invariable but depend on the cell genetic background67, neighborhood57 or order of events as we showed here. If proven of general applicability, this may lead to a paradigm shift with consequences on the understanding and treatment of cancer.
Methods
Ethical approval
Written consent was obtained from all patients with BE or EAC from the University of Cambridge (UoC) whose samples were sequenced for this study (REC: 10/H0305/1 & IRAS:15757). Samples were collected at endoscopy, staging laparoscopy, endoscopic mucosal resection or surgical resection and then snap frozen in liquid nitrogen. Samples were then embedded in optimal cutting temperature media for cutting of 1 × 3 µM slide to be H&E stained and reviewed by a pathologist. Only tumor samples of >50% cellularity and BE samples with high intestinal metaplasia content proceeded to sequencing.
Sample collection
Single-nucleotide variants (SNVs), indels and copy-number data for 1,032 primary EACs were collected from published studies and de novo sequenced samples (Supplementary Table 1). In particular, WGS from 706 EACs was performed at UoC (EGAD00001011191 and EGAD00001006083, https://ega-archive.org/). WES data for 73 TCGA EACs were downloaded from the Genomic Data Commons portal (https://portal.gdc.cancer.gov/). Damaged genes for 253 Memorial Sloan Kettering Cancer Center (MSKCC) EACs that underwent targeted re-sequencing of 528 (ref. 37), 477 (ref. 6) and 970 (ref. 38) genes were downloaded from the cBioPortal (https://www.cbioportal.org/). In cases of multiple samples per patient, the sample with CDKN2A LoF was retained. Clinical data for the TCGA and MSKCC cohorts were obtained from the same sources. For the UoC cohort, clinical data were derived from LabKey (https://occams.cs.ox.ac.uk/labkey). Bulk RNA-seq data were available for 337 EACs, all of which had matched WGS or WES (Supplementary Table 1). Of these, 264 were sequenced at the UoC (EGAD00001011190) and 73 were derived from TCGA. Methylation data were available for 256 EACs (EGAD00010001822 (ref. 40) and TCGA32; Supplementary Table 1).
WGS, WES and clinical data for 356 BEs were obtained from UoC (EGAD00001011191 and EGAD00001011189, which also includes samples from Katz-Summercorn et al.43 and Killcoyne et al.44) and from the Fred Hutchinson Cancer Research Center (FHCRC)15,42 (Supplementary Table 1). As for EAC, in cases of multiple samples per patient, the sample with CDKN2A LoF was retained. BE cases were classified as progressors (P-BE, 257) or non-progressors (NP-BE, 99) based on whether patients progressed or not to high-grade dysplasia or EAC in a follow-up period of up to 17 years (Supplementary Table 1).
Paired WGS BE and EAC data were available for 86 cases (EGAD00001011191 and EGAD00001006083, which also include samples from Noorani et al.34, Ross-Innes et al.35and Katz-Summercorn et al.43). Methylation data for 57 BE cases were derived from UoC (EGAD00010001838 (ref. 40) and EGAD00010001972 (ref. 43)). Bulk RNA-seq data for 108 P-BEs and 22 NP-BEs were sequenced at the UoC (EGAD00001011190, including samples from Katz-Summercorn et al.43) (Supplementary Table 1).
DNA and RNA extraction, library preparation and variant calling
DNA and RNA were extracted using Qiagen AllPrep Mini kits, using a Precellys for tissue dissociation after all excess OCT was removed. Extracted nucleic acids were quantified by Qubit. Libraries were then prepared using Illumina PCR Free methods and sequenced on HiSeq 4000 or NovaSeq platforms. Paired-end whole-genome sequencing at 50× target depth for EACs, P-BEs and NP-BEs and 30× target depth for matched normal (blood) was performed by Illumina, the Sanger Institute, or the CRUK Cambridge Institute on Illumina platforms. Quality checks were performed using FastQC (http://www.bioinformatics.babraham.ac.uk/projects/fastqc/). For mutation calling, sequencing reads were aligned against the reference genome (hg19/GRCh37) using BWA-MEM68. Aligned reads were then sorted into genome coordinate order and duplicate reads were flagged using Picard MarkDuplicates (http://broadinstitute.github.io/picard). Strelka69 2.0.15 was used for calling single nucleotide variants and indels. Sample purity and ploidy values were estimated using ASCAT-NGS 2.170. Copy-number alterations (CNAs) after correction for estimated normal-cell contamination were inferred using ASCAT from read counts at germline heterozygous positions estimated by GATK 3.2-2 HaplotypeCaller71. Shallow WGS data for 75 BE cases44 were processed with the QDNAseq package using 50-kb bins including GC-bias correction, segmentation and generation of copy-number calls and used to identify homozygously deleted and amplified genes. Because the read depth was only 0.4×, mutation calls could not be performed.
Annotation of damaged genes and EAC drivers and clonality analysis
For WGS (UoC, FHCRC) and WES (TCGA) data, SNV, indel and copy-number calls were taken from the original publications or derived as described above. ANNOVAR72 (April 2018) and dbNSFP73 v3. 0 were used to annotate the effect of mutations and indels. Only SNVs and indels with damaging effects on the proteins as previously described1 were further retained. Briefly, these included (1) truncating (stopgain, stoploss, frameshift) mutations; (2) missense mutations predicted by at least seven methods1.
CNA segments from ASCAT were intersected with the exonic coordinates of 19,641 unique human genes1, and a gene was considered amplified, homozygously or heterozygously deleted if at least 25% of its length overlapped with an amplified (CNA > twice sample ploidy) or homozygously (CNA = 0) or heterozygously deleted (CNA = 1) segment, respectively. Genes with at least one damaging SNV or indel as well as amplified and homozygously deleted genes were considered damaged. Genes with heterozygous deletion of one allele and at least a damaging SNV or indel in the other (double hit), were also considered damaged. Genes with only heterozygous deletions were not considered damaged. For CDKN2A only, CDKN2A silencing via methylation was also considered. Raw methylation data were processed with the minfi package and normalized with the BETA mixture model BMIQ of the ChAMP package. CDKN2A was considered epigenetically silenced if the cg12840719 probe located within 1,500 bp from its transcription start site40 had a methylation β value ≥ 0.3 and its CDKN2A value was comparable to samples with homozygously deleted CDKN2A. The distribution of damaged genes across EAC and BE cohorts is shown in Extended Data Fig. 1. Mutated, amplified and homozygously deleted genes for the MSKCC cohort6,37,38 were downloaded from the cBioPortal.
Five hundred eighty out of 779 EACs with WGS or WES data (Supplementary Table 1) had damaging alterations in TP53 or CDKN2A and were further analyzed to measure mutation clonality as described previously74. Briefly, the probability of each damaging mutation to have a cancer cell fraction (CCF) from 0.01 to 1 incremented by 0.01 was calculated given the observed variant allele frequency (VAF), gene copy-number status in the cancer and normal sample and sample purity. Then, the clonal probability of a TP53 or CDKN2A mutation was calculated as the cumulative probability of CCF being >0.95. A damaging mutation was considered clonal if its clonal probability was >50%.
A list of 40 EAC canonical drivers was obtained from the Network of Cancer Genes (NCG7.1, http://www.network-cancer-genes.org)1. Additionally, 34 EAC drivers that undergo CNA were collected through manual curation of the literature. Only 54 of the resulting 74 EAC drivers were present also in the gene panel used in the MSKCC studies and these were considered for further analysis (Supplementary Table 2).
Cell lines and gene expression quantification
In vitro experiments were carried out using the CP-A (KR-42421) BE cells from the Francis Crick Institute cell service facility (ATCC catalog number CRL-4027). Cells were grown at 37 °C and 5% CO2 in keratinocyte serum-free medium supplemented with 50 µg ml−1 bovine pituitary extract and 5 ng/ml recombinant human EGF (Thermo Fisher). Total RNA was extracted from CP-A wild-type cells and TP53 KO clones using the Direct-zol RNA miniprep kit (ZymoResearch) and reverse transcribed using the High-capacity cDNA reverse transcription kit (Thermo Fisher). Predesigned Taqman gene expression assays for CDKN2A and TP53 were used (Life Technologies; Supplementary Table 4), whereas gene-specific primers and probe were designed for ACTB (Merck; Supplementary Table 4). Real-time quantitative PCR (rt-qPCR) was performed in duplicate using QuantiTect probe PCR mastermix (Qiagen) and repeated three times. Gene relative expression was calculated using the 2−ΔΔCt method and ACTB as endogenous control. A pool of human RNA was used as a positive control.
TP53 gene editing and cell proliferation assay
To induce TP53 KO via CRISPR-Cas9 gene editing, 3.5 × 105 CP-A cells were co-transfected with two TP53-specific gRNAs (Supplementary Table 4) and Alt-R S.p.Cas9-Nuclease V3 (IDT) by nucleofection using the P3 Primary Cell 4D-NucleofectorTM X Kit S (Lonza) on a 4D-Nucleofector (Lonza). After nucleofection, single cells were plated in individual wells to form clonal colonies. Genomic DNA of nucleofected colonies was extracted using PureLink Genomic DNA mini kit (Invitrogen) and regions surrounding the targeted sites were amplified from genomic DNA of nucleofected colonies using HotStartTaq Plus DNA polymerase (Qiagen) and primers including Illumina adapters (Supplementary Table 4). Amplicons were sequenced on Illumina Novaseq using the paired-end protocol to confirm editing (BAM files: 10.5281/zenodo.12918301).
Cell proliferation of TP53 KO and wild-type CP-A cells was measured every 24 h for 3 days, starting 3 h after seeding the cells using CellTiter-Glo Luminescent Cell Viability Assay (Promega). Briefly, 2 × 103 cells per well were seeded on 96-well plates in a final volume of 100 μl per well. At each time point, 100 μl of the CellTiter-Glo reagent was added to the wells and luminescence was measured after 30 minutes using the Infinite F200 Pro plate reader (Tecan). For all proliferation assays, two or four technical replicates per condition were measured at each time point and each measure was normalized to the average time zero measure for each condition. Each experiment was repeated three independent times. Conditions were compared using the two-sided Student’s t-test.
Logistic regression and survival analysis
Logistic regression with Firth bias correction75 was used to test the difference between two models of EAC initiation in the entire BE (P-BE and NP-BE) cohort. The first model assumed TP53 LoF as the only driver (model 1), whereas the second model assumed that both TP53 and CDKN2A LoF impacted on EAC initiation (model 2). The models were developed using the package logistf v1.25.0 and compared using the anova function in R. The two models were used to estimate the numbers of expected BE cases that progressed to EAC according to corresponding genomic status of TP53 and CDKN2A. The β coefficients for TP53 and CDKN2A LoF were obtained from the regression models and the p-values were calculated using the chi-squared test. Negative or positive β coefficient values indicated cancer-protective or cancer-promoting roles, respectively. The β coefficient (β) of CDKN2A LoF in model 2 was used to estimate the odds of progression as:
The results of the whole analysis are reported in Supplementary Table 3.
Kaplan-Meier survival analysis was performed with survminer v.0.4.9 using the log-rank method. The analysis of the survival effect of CDKN2A co-damage with other 9p21 genes was performed only on 779 patients with EAC with WGS or WES data as the information on the genomic alteration of all 9p21 genes was not available in the targeted re-sequencing studies. Log-rank method was used to estimate P values, which were then corrected for multiple hypothesis testing using the Benjamini–Hochberg method, when needed.
RNA-seq, gene set enrichment and immune infiltration
Paired-end RNA-seq for EAC, P-BE and NP-BE from UoC was performed at the CRUK Cambridge Institute on Illumina platforms and quality checks were performed using FastQC. Reads were aligned using STAR with ENSEMBL gene annotation. Reads per gene were quantified using the summariseOverlaps function from the GenomicRanges package. Raw read counts of 18,846 human genes shared between the UoC and TCGA cohorts were extracted from the corresponding BE and EAC RNA-seq datasets. SMIXnorm v0.0.0.9 (ref. 76) was used to estimate the probability of expression of these genes across all samples. Genes with a probability of expression below 0.9 were filtered out, resulting in 16,901 retained genes in EAC, 15,134 in P-BE and 15,866 in NP-BE, respectively.
Twenty-two NP-BEs, 108 P-BEs and 337 EACs with matched genomic and transcriptomic data (Supplementary Table 1) were divided into four groups depending on the mutation and copy-number profiles of the six 9p21 genes (KLHL9, IFNE, MTAP, CDKN2A, CDKN2B and DMRTA1) with impact on survival. Differential gene expression analysis was performed between each of these groups and the corresponding 9p21 wild-type EACs (184), P-BEs (31) and NP-BEs (6) using DESeq2 v1.38.3 (ref. 77) after correction for the batch effect with DESeqDataSetFromMatrix. Genes were ordered according to log2 fold-change values and used for preranked GSEA using fgsea v1.24.0 (ref. 48) against 50 gene sets from MSigDB v7.5.1 (ref. 78) and 1,303 level 2-8 pathways from Reactome v.72 (ref. 79) containing between 10 and 500 expressed genes and excluding the disease hierarchical level. The resulting P values were corrected for multiple testing in each analysis separately using the Benjamini–Hochberg method. Pathway redundancy was removed accounting for the extent of overlap between leading-edge genes; that is, the genes that contributed the most to the enrichment. If the number of unique leading-edge genes in a pathway was higher than the shared and the unique leading-edge genes in the other pathway, the latter was removed. If the number of shared leading-edge genes between two pathways was higher than the unique leading-edge genes in both, the pathway with the higher FDR was removed. Retained processes are reported in Supplementary Table 6.
To estimate the abundance of immune cell populations from bulk RNA-seq data, raw read counts of the expressed genes from 22 NP-BEs, 108 P-BEs and 337 EACs were normalized to transcripts per million values after batch correction with ComBat-seq80. Resulting transcripts per million were used as input for ConsensusTME v0.0.1 (ref. 81) as implemented in immunedeconv v2.1.0 to estimate the NES using 16 esophageal carcinoma immune signatures. To further estimate the abundance of MDSCs, two M-MDSC and G-MDSC signatures82 were used in ConsensusTME custom mode.
RNAScope and imaging mass cytometry
A panel of 26 antibodies targeting structural markers, immune markers, three 9p21 proteins and three RNAScope probes against IFNE, IFNB1 and PPIB mRNAs was assembled (Supplementary Table 10). RNAScope staining was detected using metal-tagged antibodies as previously described83. Sixteen of these antibodies were already metal-tagged (Standard Biotools), whereas eleven were carrier-free and tagged using the Maxpar X8 metal conjugation kit (Standard Biotools). The whole panel was tested in EAC FFPE sections using three dilutions ranging from 1:100 to 1:3,500 and the dilution giving the highest signal-to-noise ratio was chosen for each antibody (Supplementary Table 10).
Five-micrometer-thick sections were obtained from FFPE blocks of ten patients with EAC selected based on their 9p21 gene profile (Supplementary Table 9). Slides were incubated for 1 h at 60 °C, loaded on a Leica Bond autostainer (Leica Biosystems) and processed using the RNASCope LS Multiplex Fluorescent Assay following manufacturer’s instructions and IFNE, IFNB1 and PPIB probes at a 1:50 dilution. C2 oligos were developed with TSA-digoxinenin, C3 oligos with TSA-biotin and C1 oligos with TSA-FITC (diluted 1:200 in TSA buffer). Slides were blocked for 2 h at room temperature in a Sequenza rack (Thermo Fisher Scientific). Slides were incubated overnight at 4 °C with the mix of metal-conjugated antibodies, washed, and incubated with the DNA intercalator Cell-ID Intercalator-Ir (Standard Biotools). Slides were removed from the Sequenza rack, air-dried and loaded into the Hyperion Imaging System (Standard Biotools). Regions of interest were manually selected to contain areas with tumor and immune cells by a certified pathologist (M.R.J). Regions of about 1.44 mm2 were laser-ablated within the preselected regions of interest at 1 μm pixel−1 resolution and 400 Hz frequency.
IMC image analysis was performed using SIMPLI84. TIFF images for each metal-tagged antibody and DNA intercalator were obtained from the raw.txt files of the ablated regions. Pixel intensities for each channel were normalized to the 99th percentile of the intensity distribution. Background pixels of the normalized images were removed with CellProfiler4 (ref. 85) using global thresholding and processed images were verified by an expert histologist (J.S.). Single-cell segmentation was performed using CellProfiler4 (ref. 85) to identify cell nucleus (DNA1 channel) and membrane (cadherin-1, pan-keratin, CD3, CD8, CD4, CD11b, CD11c, NCAM1, CD68, CD27, CD163, CD16, CD15 and CD14). Obtained cells were phenotyped based on at least 10% overlap with the masks of individual cell types in the following order: (1) CD15+ and CD16+ for neutrophils; (2) NCAM1+ for NK cells; (3) CD11c+ for dendritic cells; (4) CD68+ for macrophages; (5) CD14+ for M-MDSCs; (6) CD15+ for G-MDSCs; (7) CD3+ for T cells; (8) cadherin-1 and pan-keratin for tumor cells and (9) vimentin for stromal cells. Cells with <10% overlap with any mask were left unassigned.
Unsupervised clustering was performed separately on CD3+ T cells and CD68+ macrophages using Seurat v.2.4 (ref. 86), with random seed = 123 and 0.3, 0.5, 0.7 and 0.9 cluster resolutions. Markers used for clustering were CD3, CD4, CD8, FOXP3, GzMB and Ki67 for T cells, and CD68, CD11c, HLA-DR/DP/DQ and CD163, CD11b and Ki67 for macrophages. Silhouette score of each cluster was calculated using v.2.1.6 package. The resolution with the highest median silhouette score was identified as the best clustering resolution for each cell type.
Keratinization causal regulatory network analysis
Causal networks linking CDKN2A LoF to the downregulation of keratinization were inferred using a three-step protocol modified from87, separately for P-BE and EAC (Extended Data Fig. 4a–c). In the first step, co-regulated gene modules were identified using cMonkey2 (ref. 88) based on gene co-expression, proximity in the protein-protein interaction network (PPIN) and enrichment in transcription factor (TF) targets. Co-expressed genes were identified from the top 50% most variably expressed genes in P-BE and EAC after converting read counts into z-scores using DESeq2 v1.38.3 (ref. 77). Proximity in the PPIN was measured using the human weighted PPIN from STRING v11.5 (ref. 89). GO:0006355 term of Gene Ontology (release 2022-05) was used to identify 1,471 TFs. These were in turn used as input for ARACNE-AP90 together with P-BE and EAC gene expression data to identify TF-target pairs. cMonkey2 was run with a fixed number of iterations (n = 2,000) and seed value (n = 123) for the initialization step to ensure reproducibility. The number of gene modules (k) was determined as:
where nAG was the number of analyzed genes, nBpG was the maximum number of gene modules each gene could appear in (fixed to 2), and nGpB was the average number of genes per gene module (fixed to 30). Identified gene modules were then filtered based on (i) co-expression quality according to the first principal component (FDR ≤ 0.1 and variance explained ≥0.32 for P-BE and ≥0.25 for EAC), (ii) functional enrichment in keratinization-related genes (two-sided Fisher’s test P ≤ 0.01), (iii) enrichment in TF target genes (two-sided Fisher’s test P value ≤ 0.01), and (iv) correlation of TFs with gene module eigengenes, that is genes that explain the maximum expression variance. In the second step, the single.marker.analysis function of the Network Edge Orienting87 method was used to infer causal models where CDKN2A LoF causally affected the expression of specific TFs, which, in turn, altered keratinization gene modules. To assess statistical significance, the next best single marker score was defined as the log10 probability of the causal model divided by the log10 probability of the next best fitting alternative model91 and causal models with next best single marker score ≥0.5 were considered significant. In the third step, significant causal models were further retained if (1) TFs were differentially expressed (FDR < 0.1) in group 4 as compared to 9p21 wild-type P-BEs and EACs and (2) there was significant positive correlation (R > 0.5 and FDR < 0.1) between TF expression and the GSEA NES score of the predicted targets in P-BEs and EACs. Finally, only TFs contributing to ≥ 30% of the significant causal models were retained. The final list of significant causal models and associated TFs is reported in Supplementary Table 11.
Statistical analysis and reproducibility
All statistical tests were performed in R v.4.3.1 and results were plotted using ggplot2 v.3.4.4 and ggpubr v.0.6.0. All distributions were compared using two-sided Wilcoxon rank-sum test. Growth curves were compared using two-sided Student’s t-test. Two-sided Fisher’s exact test was used to compare categorical variables. Kaplan–Meier analysis with a log-rank test was performed for survival analysis. P value estimation for pre-ranked GSEA was based on an adaptive multilevel split Monte-Carlo scheme. Pearson’s correlation test and Spearman’s rank correlation test were used to assess correlation significance. Benjamini–Hochberg method was used to account for multiple testing when needed and false discovery rate <0.1 was considered as significant. No statistical method was used to predetermine sample size, as sample sizes were as large as possible considering available data. No data were excluded from any analysis. Data normalization was performed before analysis, but this was not formally tested, Experiments were not randomized, and the investigators were not blinded to allocation during experiments and outcome assessment. To ensure results reproducibility, all experiments were conducted in replicates as specified in the corresponding methods. Further information on research design is available in the Nature Research Reporting Summary linked to this article.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
DNA and RNA sequence data for the UoC cohort were deposited at the European Genome-phenome Archive with the following accession IDs: WGS (EGAD00001011191, EGAD00001006083), shallow WGS (EGAD00001011189), bulk RNA sequencing (EGAD00001011190). WES for 73 TCGA EACs were downloaded from the Genomic Data Commons portal (https://portal.gdc.cancer.gov/). Mutated genes for 253 Memorial Sloan Kettering Cancer Center (MSKCC) EACs that underwent targeted re-sequencing were downloaded from the cBioPortal (https://www.cbioportal.org/). Methylation data for EACs were derived from UoC (EGAD00010001822) and TCGA (https://portal.gdc.cancer.gov/). Methylation data for BE were derived from UoC (EGAD00010001838 and EGAD00010001972). BAM files of wild-type and TP53 edited CP-A cells were deposited at Zenodo (https://doi.org/10.5281/zenodo.12918301) (ref. 92). UoC WGS, sWGS, RNA-seq and methylation data of the human patients are under controlled access by ICGC (International Cancer Genome Consortium) due to privacy and security protection of personal data. The reasons and conditions for controlled access are described here (https://www.icgc-argo.org/page/132/data-access-and-data-use-policies-and-guidelines). The data can be accessed via the ICGC portal upon request to the ICGC Data Access Compliance Office here: https://docs.icgc-argo.org/docs/data-access/daco/applying. Source data for Figs. 1–6 and Extended Data Figs. 1–3 have been provided as Source Data files. All other data supporting the findings of this study are available from the corresponding author on reasonable request. Source data are provided with this paper.
Code availability
No unique or custom code was developed for this study.
References
Dressler, L. et al. Comparative assessment of genes driving cancer and somatic evolution in non-cancer tissues: an update of the Network of Cancer Genes (NCG) resource. Genome Biol. 23, 35 (2022).
Zhao, R., Choi, B. Y., Lee, M. H., Bode, A. M. & Dong, Z. Implications of genetic and epigenetic alterations of CDKN2A (p16(INK4a)) in cancer. EBioMedicine 8, 30–39 (2016).
Baruah, P. et al. Impact of p16 status on pro- and anti-angiogenesis factors in head and neck cancers. Br. J. Cancer 113, 653–659 (2015).
Jenkins, N. C. et al. The p16(INK4A) tumor suppressor regulates cellular oxidative stress. Oncogene 30, 265–274 (2011).
Izadi, F. et al. Genomic analysis of response to neoadjuvant chemotherapy in esophageal adenocarcinoma. Cancers 13, 3394 (2021).
Sihag, S. et al. Next-generation sequencing of 487 esophageal adenocarcinomas reveals independently prognostic genomic driver alterations and pathways. Clin. Cancer Res. 27, 3491–3498 (2021).
Gutiontov, S. I. et al. CDKN2A loss-of-function predicts immunotherapy resistance in non-small cell lung cancer. Sci. Rep. 11, 20059 (2021).
Han, G. et al. 9p21 loss confers a cold tumor immune microenvironment and primary resistance to immune checkpoint therapy. Nat. Commun. 12, 5606 (2021).
Barriga, F. M. et al. MACHETE identifies interferon-encompassing chromosome 9p21.3 deletions as mediators of immune evasion and metastasis. Nat. Cancer 3, 1367–1385 (2022).
Marks, Z. R. C. et al. Interferon-epsilon is a tumour suppressor and restricts ovarian cancer. Nature 620, 1063–1070 (2023).
Gjuka, D. et al. Enzyme-mediated depletion of methylthioadenosine restores T cell function in MTAP-deficient tumors and reverses immunotherapy resistance. Cancer Cell 41, 1774–1787.e9 (2023).
Barrett, M. T. et al. Allelic loss of 9p21 and mutation of the CDKN2/p16 gene develop as early lesions during neoplastic proression in Barrett’s esophagus. Oncogene 13, 1867–1873 (1996).
Weaver, J. M. J. et al. Ordering of mutations in preinvasive disease stages of esophageal carcinogenesis. Nat. Genet. 46, 837–843 (2014).
Killcoyne, S. & Fitzgerald, R. C. Evolution and progression of Barrett’s oesophagus to oesophageal cancer. Nat. Rev. Cancer 21, 731–741 (2021).
Paulson, T. G. et al. Somatic whole genome dynamics of precancer in Barrett’s esophagus reveals features associated with disease progression. Nat. Commun. 13, 2300 (2022).
Bian, Y. S., Osterheld, M. C., Fontolliet, C., Bosman, F. T. & Benhattar, J. p16 inactivation by methylation of the CDKN2A promoter occurs early during neoplastic progression in Barrett’s esophagus. Gastroenterology 122, 1113–1121 (2002).
Galipeau, P. C., Prevo, L. J., Sanchez, C. A., Longton, G. M. & Reid, B. J. Clonal expansion and loss of heterozygosity at chromosomes 9p and 17p in premalignant esophageal (Barrett’s) tissue. J. Natl Cancer Inst. 91, 2087–2095 (1999).
Barrett, M. T. et al. Evolution of neoplastic cell lineages in Barrett oesophagus. Nat. Genet. 22, 106–109 (1999).
Maley, C. C. et al. Genetic clonal diversity predicts progression to esophageal adenocarcinoma. Nat. Genet. 38, 468–473 (2006).
Maley, C. C. et al. Selectively advantageous mutations and hitchhikers in neoplasms: p16 lesions are selected in Barrett’s esophagus. Cancer Res. 64, 3414–3427 (2004).
Nones, K. et al. Genomic catastrophes frequently arise in esophageal adenocarcinoma and drive tumorigenesis. Nat. Commun. 5, 5224 (2014).
Stachler, M. D. et al. Detection of mutations in Barrett’s esophagus before progression to high-grade dysplasia or adenocarcinoma. Gastroenterology 155, 156–167 (2018).
Sepulveda, J. L. et al. High-resolution genomic alterations in Barrett’s metaplasia of patients who progress to esophageal dysplasia and adenocarcinoma. Int. J. Cancer 145, 2754–2766 (2019).
Wang, J. S. et al. DNA promoter hypermethylation of p16 and APC predicts neoplastic progression in Barrett’s esophagus. Am. J. Gastroenterol. 104, 2153–2160 (2009).
Schulmann, K. et al. Inactivation of p16, RUNX3, and HPP1 occurs early in Barrett’s-associated neoplastic progression and predicts progression risk. Oncogene 24, 4138–4148 (2005).
Jin, Z. et al. A multicenter, double-blinded validation study of methylation biomarkers for progression prediction in Barrett’s esophagus. Cancer Res. 69, 4112–4115 (2009).
Timmer, M. R. et al. Derivation of genetic biomarkers for cancer risk stratification in Barrett’s oesophagus: a prospective cohort study. Gut 65, 1602–1610 (2016).
Paulson, T. G. et al. p16 mutation spectrum in the premalignant condition Barrett’s esophagus. PLoS ONE 3, e3809 (2008).
Stachler, M. D. et al. Paired exome analysis of Barrett’s esophagus and adenocarcinoma. Nat. Genet. 47, 1047–1055 (2015).
Galipeau, P. C. et al. NSAIDs modulate CDKN2A, TP53, and DNA content risk for progression to esophageal adenocarcinoma. PLoS Med. 4, e67 (2007).
Clement, G., Braunschweig, R., Pasquier, N., Bosman, F. T. & Benhattar, J. Methylation of APC, TIMP3, and TERT: a new predictive marker to distinguish Barrett’s oesophagus patients at risk for malignant transformation. J. Pathol. 208, 100–107 (2006).
Cancer Genome Atlas Research Network et al. Integrated genomic characterization of oesophageal carcinoma. Nature 541, 169–175 (2017).
Frankell, A. M. et al. The landscape of selection in 551 esophageal adenocarcinomas defines genomic biomarkers for the clinic. Nat. Genet. 51, 506–516 (2019).
Noorani, A. et al. Genomic evidence supports a clonal diaspora model for metastases of esophageal adenocarcinoma. Nat. Genet. 52, 74–83 (2020).
Ross-Innes, C. S. et al. Whole-genome sequencing provides new insights into the clonal architecture of Barrett’s esophagus and esophageal adenocarcinoma. Nat. Genet. 47, 1038–1046 (2015).
Ng, A. W. T. et al. Rearrangement processes and structural variations show evidence of selection in oesophageal adenocarcinomas. Commun Biol. 5, 335 (2022).
Janjigian, Y. Y. et al. Genetic predictors of response to systemic therapy in esophagogastric cancer. Cancer Discov. 8, 49–58 (2018).
Samstein, R. M. et al. Tumor mutational load predicts survival after immunotherapy across multiple cancer types. Nat. Genet. 51, 202–206 (2019).
Xie, S.-H. & Lagergren, J. The male predominance in esophageal adenocarcinoma. Clin. Gastroenterol. Hepatol. 14, 338–347.e1 (2016).
Jammula, S. et al. Identification of subtypes of Barrett’s esophagus and esophageal adenocarcinoma based on DNA methylation profiles and integration of transcriptome and genome data. Gastroenterology 158, 1682–1697.e1 (2020).
Dulak, A. M. et al. Gastrointestinal adenocarcinomas of the esophagus, stomach, and colon exhibit distinct patterns of genome instability and oncogenesis. Cancer Res. 72, 4383–4393 (2012).
Galipeau, P. C. et al. NSAID use and somatic exomic mutations in Barrett’s esophagus. Genome Med. 10, 17 (2018).
Katz-Summercorn, A. C. et al. Multi-omic cross-sectional cohort study of pre-malignant Barrett’s esophagus reveals early structural variation and retrotransposon activity. Nat. Commun. 13, 1407 (2022).
Killcoyne, S. et al. Genomic copy number predicts esophageal cancer years before transformation. Nat. Med. 26, 1726–1732 (2020).
Reid, B. J. et al. Predictors of progression in Barrett’s esophagus II: baseline 17p (p53) loss of heterozygosity identifies a patient subset at increased risk for neoplastic progression. Am. J. Gastroenterol. 96, 2839–2848 (2001).
Zhang, X. et al. Malignant transformation of non-neoplastic Barrett’s epithelial cells through well-defined genetic manipulations. PLoS ONE 5, e13093 (2010).
Palanca-Wessels, M. C. et al. Extended lifespan of Barrett’s esophagus epithelium transduced with the human telomerase catalytic subunit: a useful in vitro model. Carcinogenesis 24, 1183–1190 (2003).
Korotkevich, G. et al. Fast gene set enrichment analysis. Preprint at bioRxiv https://doi.org/10.1101/060012 (2021).
Shihab, H. A. et al. Predicting the functional, molecular, and phenotypic consequences of amino acid substitutions using hidden Markov models. Hum. Mutat. 34, 57–65 (2013).
Hu, Q. et al. MTAP deficiency-induced metabolic reprogramming creates a vulnerability to cotargeting de novo purine synthesis and glycolysis in pancreatic cancer. Cancer Res. 81, 4964–4980 (2021).
Shi, L. Z. & Bonner, J. A. Bridging radiotherapy to immunotherapy: the IFN-JAK-STAT axis. Int. J. Mol. Sci. 22, 12295 (2021).
Sulahian, R. et al. SOX15 governs transcription in human stratified epithelia and a subset of esophageal adenocarcinomas. Cell. Mol. Gastroenterol. Hepatol. 1, 598–609.e6 (2015).
Thompson, C. A., DeLaForest, A. & Battle, M. A. Patterning the gastrointestinal epithelium to confer regional-specific functions. Dev. Biol. 435, 97–108 (2018).
Nowicki-Osuch, K. et al. Molecular phenotyping reveals the identity of Barrett’s esophagus and its malignant transition. Science 373, 760–767 (2021).
Busslinger, G. A. et al. Human gastrointestinal epithelia of the esophagus, stomach, and duodenum resolved at single-cell resolution. Cell Rep. 34, 108819 (2021).
Acha-Sagredo, A., Ganguli, P. & Ciccarelli, F. D. Somatic variation in normal tissues: friend or foe of cancer early detection? Ann. Oncol. 33, 1239–1249 (2022).
Colom, B. et al. Spatial competition shapes the dynamic mutational landscape of normal esophageal epithelium. Nat. Genet. 52, 604–614 (2020).
Wu, Z. et al. Reprogramming of the esophageal squamous carcinoma epigenome by SOX2 promotes ADAR1 dependence. Nat. Genet. 53, 881–894 (2021).
Ko, K. P. et al. Key genetic determinants driving esophageal squamous cell carcinoma initiation and immune evasion. Gastroenterology 165, 613–628.e20 (2023).
Zhao, H. et al. Generation and multiomic profiling of a TP53/CDKN2A double-knockout gastroesophageal junction organoid model. Sci. Transl. Med. 14, eabq6146 (2022).
Iyer, P. G. & Chak, A. Surveillance in Barrett’s esophagus: challenges, progress, and possibilities. Gastroenterology 164, 707–718 (2023).
Chen, Z. et al. Comprehensive analysis revealed that CDKN2A is a biomarker for immune infiltrates in multiple cancers. Front. Cell Dev. Biol. 9, 808208 (2021).
Cheng, T. et al. CDKN2A-mediated molecular subtypes characterize the hallmarks of tumor microenvironment and guide precision medicine in triple-negative breast cancer. Front. Immunol. 13, 970950 (2022).
Chikh, A. et al. iASPP/p63 autoregulatory feedback loop is required for the homeostasis of stratified epithelia. EMBO J. 30, 4261–4273 (2011).
Pandolfi, S., Montagnani, V., Lapucci, A. & Stecca, B. HEDGEHOG/GLI-E2F1 axis modulates iASPP expression and function and regulates melanoma cell growth. Cell Death Differ. 22, 2006–2019 (2015).
Sethi, I. et al. A global analysis of the complex landscape of isoforms and regulatory networks of p63 in human cells and tissues. BMC Genomics 16, 584 (2015).
Blair, L. M. et al. Oncogenic context shapes the fitness landscape of tumor suppression. Nat. Commun. 14, 6422 (2023).
Li, H. & Durbin, R. Fast and accurate short read alignment with Burrows-Wheeler transform. Bioinformatics 25, 1754–1760 (2009).
Saunders, C. T. et al. Strelka: accurate somatic small-variant calling from sequenced tumor-normal sample pairs. Bioinformatics 28, 1811–1817 (2012).
Van Loo, P. et al. Allele-specific copy number analysis of tumors. Proc. Natl Acad. Sci. USA 107, 16910–16915 (2010).
McKenna, A. et al. The Genome Analysis Toolkit: a MapReduce framework for analyzing next-generation DNA sequencing data. Genome Res. 20, 1297–1303 (2010).
Wang, K., Li, M. & Hakonarson, H. ANNOVAR: functional annotation of genetic variants from high-throughput sequencing data. Nucleic Acids Res. 38, e164 (2010).
Liu, X., Wu, C., Li, C. & Boerwinkle, E. dbNSFP v3.0: a one-stop database of functional predictions and annotations for human nonsynonymous and splice-site SNVs. Hum. Mutat. 37, 235–241 (2016).
Goh, G., McGranahan, N. & Wilson, G. A. Computational methods for analysis of tumor clonality and evolutionary history. Methods Mol. Biol. 1878, 217–226 (2019).
Heinze, G. & Schemper, M. A solution to the problem of separation in logistic regression. Stat. Med. 21, 2409–2419 (2002).
Yin, S. et al. SMIXnorm: fast and accurate RNA-seq data normalization for formalin-fixed paraffin-embedded samples. Front. Genet. 12, 650795 (2021).
Love, M. I., Huber, W. & Anders, S. Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biol. 15, 550 (2014).
Liberzon, A. et al. The Molecular Signatures Database (MSigDB) hallmark gene set collection. Cell Syst. 1, 417–425 (2015).
Jassal, B. et al. The reactome pathway knowledgebase. Nucleic Acids Res. 48, D498–D503 (2020).
Zhang, Y., Parmigiani, G. & Johnson, W. E. ComBat-seq: batch effect adjustment for RNA-seq count data. NAR Genom. Bioinform. 2, lqaa078 (2020).
Jimenez-Sanchez, A., Cast, O. & Miller, M. L. Comprehensive benchmarking and integration of tumor microenvironment cell estimation methods. Cancer Res. 79, 6238–6246 (2019).
Alshetaiwi, H. et al. Defining the emergence of myeloid-derived suppressor cells in breast cancer using single-cell transcriptomics. Sci. Immunol. 5, eaay6017 (2020).
Montorsi, L. et al. Double-negative B cells and DNASE1L3 colocalise with microbiota in gut-associated lymphoid tissue. Nat. Commun. 15, 4051 (2024).
Bortolomeazzi, M. et al. A SIMPLI (Single-cell Identification from MultiPLexed Images) approach for spatially-resolved tissue phenotyping at single-cell resolution. Nat. Commun. 13, 781 (2022).
McQuin, C. et al. CellProfiler 3.0: next-generation image processing for biology. PLoS Biol. 16, e2005970 (2018).
Butler, A., Hoffman, P., Smibert, P., Papalexi, E. & Satija, R. Integrating single-cell transcriptomic data across different conditions, technologies, and species. Nat. Biotechnol. 36, 411–420 (2018).
Plaisier, C. L. et al. Causal mechanistic regulatory network for glioblastoma deciphered using systems genetics network analysis. Cell Syst. 3, 172–186 (2016).
Reiss, D. J., Plaisier, C. L., Wu, W. J. & Baliga, N. S. cMonkey2: Automated, systematic, integrated detection of co-regulated gene modules for any organism. Nucleic Acids Res. 43, e87 (2015).
Szklarczyk, D. et al. The STRING database in 2021: customizable protein-protein networks, and functional characterization of user-uploaded gene/measurement sets. Nucleic Acids Res. 49, D605–D612 (2021).
Lachmann, A., Giorgi, F. M., Lopez, G. & Califano, A. ARACNe-AP: gene network reverse engineering through adaptive partitioning inference of mutual information. Bioinformatics 32, 2233–2235 (2016).
Aten, J. E., Fuller, T. F., Lusis, A. J. & Horvath, S. Using genetic markers to orient the edges in quantitative trait networks: the NEO software. BMC Syst. Biol. 2, 34 (2008).
Ganguli, P., Acha-Sagredo, A., Misetic, H. & Ciccarelli, F. BAM files of wild-type CP-A cells and the TP53 KO CP-A clones. Zenodo https://doi.org/10.5281/zenodo.12918301 (2024).
Sherr, C. J. The INK4a/ARF network in tumour suppression. Nat. Rev. Mol. Cell Biol. 2, 731–737 (2001).
Acknowledgements
We thank P.C. Galipeau (Fred Hutchinson Cancer Research Center) for sharing somatic variant call files for the BE samples and M. Bortolomeazzi (Deutsches Krebsforschungszentrum), M. Pitcher and L. Montorsi (King’s College London) for help with the IMC analysis. This work was supported by Cancer Research UK (C43634/A25487 and EDDPJT-Nov21\100010 to F.D.C.), the Cancer Research UK City of London Centre (C7893/A26233 to F.D.C.), Barts Charity and the Francis Crick Institute, which receives its core funding from Cancer Research UK (FC001002), the UK Medical Research Council (FC001002) and the Wellcome Trust (FC001002). P.B. and A.B. were supported by The Rosetrees Trust (CF2\100014). For the purpose of Open Access, the author has applied a CC BY public copyright license to any Author Accepted Manuscript version arising from this submission.
Author information
Authors and Affiliations
Consortia
Contributions
F.D.C. conceived and directed the study with the support of P.G.; R.C.F. recruited participants and led the OCCAMS Consortium; P.G., C.C.B., M.A., A.M., A.Z., H.M., G.D. and F.D.C. analyzed the data; A.A.S. performed the experiments; A.B. and P.B. provided some reagents and helped with cell cultures; G.D. constructed and managed the sequencing alignment and variant-calling pipelines. G.K. guided the statistical analysis. A.F. coordinated and carried out the processing of patient samples. A.F. and P.G. screened histopathological reports and identified samples; M.A., A.A.S., M.G. and E.N. performed the IMC experiments; M.R.J. and J.S. assessed tissue sections. P.G. and F.D.C. wrote the paper with contributions from C.C.B., M.A., A.M., A.Z., H.M., G.D. and A.F. All authors approved the paper.
Corresponding author
Ethics declarations
Competing interests
R.C.F. is named on patents related to Cytosponge and related assays which have been licensed by the Medical Research Council to Covidien GI Solutions (now Medtronic) and is a co-founder and shareholder (<3%) of CYTED Ltd. The Fitzgerald lab also has an ongoing collaboration with AstraZeneca. The other authors declare no competing interests.
Peer review
Peer review information
Nature Cancer thanks Stephen Meltzer and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Extended Data Fig. 1 Distribution of damaged genes in BE and EAC.
Damaged genes per sample in EAC WGS/WES cohorts (n = 779 patients) with any type of damaging alterations (A), homozygous deletions (B), gene amplifications (C), double hits (D) and damaging SNVs and indels (E). Number of damaged genes per sample in P-BE (n = 218 patients) and NP-BE (n = 63 patients) with any type of damaging alterations (F), homozygous deletions (G), gene amplifications (H), double hits (I) and damaging SNVs and indels (J). FHCRC, Fred Hutchinson Cancer Research Center; NP-BE, non-progressor Barrett’s esophagus; EAC, esophageal adenocarcinoma; P-BE, progressor Barrett’s esophagus; SNVs, single nucleotide variants; TCGA, The Cancer Genome Atlas; UoC, University of Cambridge. All boxplots show first and third quartiles, whiskers extend to 1.5X the interquartile lower and upper range and the line indicates the median.
Extended Data Fig. 2 Effect of alterations in cell cycle regulators on EAC survival.
A. Kaplan-Meier survival curves of patients with EAC with wild type CDKN2A compared to those with heterozygous loss of CDKN2A. Heterozygous deletions could be inferred only in n = 779 patients with EAC with WGS or WES data. Kaplan-Meier survival curves of patients with EAC with alterations in CCND1 (p-value = 0.01) (B), TP53 (C), CDKN1A (D), CCNE1 (E) and MDM2 (F) compared to the corresponding wild type samples. Survival curves B-F were done using the whole cohort of 1032 EACs. GoF, gain-of-function; LoF, loss-of-function; EAC, esophageal adenocarcinoma; Het, Heterozygous deletions. Log-rank method was used to estimate the p-values.
Extended Data Fig. 3 Expression of 9p21 genes in normal esophagus.
Transcript Per Million (TPM) expression values of the 26 9p21 genes in esophagus samples from n = 139 healthy individuals. Data were derived from the Genotype-Tissue Expression (GTEx) repository (https://gtexportal.org/).
Extended Data Fig. 4 Workflow of causal gene network analysis.
The workflow to infer the causal gene network linking CDKN2A LoF to the downregulation of keratinization was divided into three steps: (A) identification and filtering of the keratinization-related gene modules and associated transcription factors (TFs) using cMonkey288 and ARACNE-AP90 (Step 1); (B) prediction of the causal models that link CDKN2A LoF to the dysregulation of keratinization genes through specific TFs using the network edge orienting (NEO) method87,91 (Step 2); and (C) retention of the causal models with differential expression (FDR < 0.1) of TFs in group 4 compared to 9p21 wild type samples assessed using DESeq277 and significant positive correlation (R > 0.5 and FDR < 0.1) between TF expression and the GSEA NES score of the predicted targets in P-BEs and EACs (Step 3).
Supplementary information
Supplementary Tables 1–11
Supplementary Table 1: Samples used in the study. Supplementary Table 2: Curated list of EAC canonical drivers. Supplementary Table 3: Results of logistic regression analysis. Supplementary Table 4: Oligos used in the study. Supplementary Table 5: Survival analysis of patients with 9p21 co-damaged genes. Supplementary Table 6: Dysregulated pathways in 9p21 LoF samples. Supplementary Table 7: Immune infiltration in 9p21 LoF and wild-type samples. Supplementary Table 8: Literature support for the effect of 9p21 gene LoF on immune infiltration. Supplementary Table 9: EACs used for RNAScope-Imaging mass cytometry. Supplementary Table 10: Markers used for RNAScope-Imaging mass cytometry. Supplementary Table 11: Causal models associated with decreased keratinization.
Source data
Source Data Fig. 1
Numerical source data.
Source Data Fig. 2
Numerical source data.
Source Data Fig. 3
Numerical source data.
Source Data Fig. 4
Numerical source data.
Source Data Fig. 5
Numerical source data.
Source Data Fig. 5
IMC images.
Source Data Fig. 6
Numerical source data.
Source Data Extended Data Fig. 1
Numerical source data.
Source Data Extended Data Fig. 2
Numerical source data.
Source Data Extended Data Fig. 3
Numerical source data.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ganguli, P., Basanta, C.C., Acha-Sagredo, A. et al. Context-dependent effects of CDKN2A and other 9p21 gene losses during the evolution of esophageal cancer. Nat Cancer 6, 158–174 (2025). https://doi.org/10.1038/s43018-024-00876-0
Received:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s43018-024-00876-0
This article is cited by
-
The biology and therapeutic implications of heterogeneity in Barrett oesophagus and oesophageal adenocarcinoma
Nature Reviews Clinical Oncology (2026)
-
Epigenomic landscape of nasopharyngeal carcinoma
Medical Oncology (2025)
