
Abstract
Lower extremity stenosis (LES) is a prevalent cardiovascular condition and a strong indicator of systemic arteriosclerosis. Existing diagnostic methods are invasive or operator-dependent and often unavailable at the primary care level. Here, we propose a non-invasive screening method based on morphological features extracted from multi-site PPG signals that were calculated from multi-site photoplethysmography measurements during a proof-of-concept clinical study at University Hospital Tübingen. Machine learning methods were used to classify 42 patients with 2 measurements each at four locations (i.e., a total of 84 measurements and 336 signals) into either the control or stenosis group. An overall classification accuracy of 82.6% (sensitivity: 0.750, specificity: 0.865) is achieved. This result is clinically relevant and shows that the selected features are effective for detecting stenosis and could be used as a screening method at the primary physician level.
Similar content being viewed by others
Introduction
Cardiovascular diseases are the leading causes of death and health impairments worldwide1. Lower extremity artery disease (LEAD) is the manifestation of arteriosclerosis in the pelvic and leg arteries and occurs in 3–10% of the population2. Prevalence of common iliac artery stenosis, on which we focus here, is up to 30% for patients with lower extremity artery disease3. Although LEAD is only responsible for 0.4% of cardiovascular deaths1, it causes chronic illness, loss of life quality, disability, increased health care costs, and it has been shown to be a strong indicator of systemic arteriosclerosis. Patients with LEAD have higher mortality compared to patients without this disease4. Moreover, LEAD can result in the need for amputations. An early non-invasive detection is therefore highly desirable.
Diagnosis of lower extremity artery occlusive disease classically relies on the patient history of a painfully limited walking distance and the clinical signs of unilaterally weakened pulse and tissue malperfusion5, even though only 5 to 10% of cases show the classical symptom of intermittent claudication6.
Actually, the ankle brachial index (ABI) is the first-line non-invasive test for screening and a diagnosis of LEAD: a blood pressure cuff is placed around the calf just above the angle, with a CW-Doppler-probe signal from the anterior or posterior tibial artery, a systolic blood pressure in the respective artery is measured and compared with the systolic blood-pressure from the brachial artery.
An ABI <0.9 is indicative of LEAD5, however, the ABI allows no conclusions about the localization of the stenosis and the underlying pathoanatomy. The latter, however, is a domain of cross-sectional imaging methods such as Doppler-sonography or CT- or MRI-angiography. Doppler-sonography allows the simultaneous examination of pathoanatomy and hemodynamics7, but its accuracy depends on the physiognomy of the patient and the skills of the examiner. CT- and MRI-angiography are costly, of limited availability, and come with the risks associated with X-ray exposure and intravenous contrast agents2.
Early diagnosis of lower extremity artery occlusive disease not only facilitates early interventional or surgical treatment, improves prognosis in terms of limb salvage and functional outcome8, but also enables a more comprehensive assessment of a patient’s individual cardiovascular risk profile, and therefore is desirable5. The early diagnosis of lower extremity artery occlusive disease, however, depends on the diagnostic skills of the general practitioner and his ability to differentiate arterial occlusive disease from other pathologies causing reduced walking distance and lower extremity pain. Based on his examination results, he indicates the specialized technical examinations mentioned above.
An objective, examiner-independent screening method with high sensitivity and good specificity for the identification of arterial occlusive disease would be a useful help in this process and a desirable extension of the diagnostic armamentarium in primary care medicine.
Thematically, non-invasive detection of stenosis can be considered a special case of the inverse hemodynamic problem, trying to ascertain details about the morphological structure of the cardiovascular system from the output of the system alone. The direct hemodynamic problem is the determination of blood pressure and flow at an arbitrary point of the body if the pulse waves at the heart and the morphological structure of the cardiovascular system are known. Pressure and flow waves can easily be calculated by suitable simulation software, e.g., ref. 9 (0D). There are many different approaches in different dimensions, as well as 0D, 1D10,11,12,13, 3D, as mixed dimensional models14,15,16.
The inverse problem, however, i.e., to deduce information on the morphological structure of the cardiovascular system from known blood pressure and/or pulse waves, may not have a unique solution17 and is much harder to solve in general. Nevertheless, there have been successful attempts to gain insights into the network structure of the arterial system and deduce information on, e.g., aneurysms and stenoses. For example, using peripheral in-vitro arterial blood pressure signals has been shown to be feasible for detecting both stenosis degree and location18. For more information on similar approaches see ref. 18 or ref. 19 and the references therein.
As already stated, there is a clear need for new non-invasive methods to detect LEAD. One attempt could be non-invasive continuous peripheral blood pressure measurements and solving the inverse problem of hemodynamics, but such suitable blood pressure measurements are not always easily achieved. Thus, it is worth considering other biosignals with high morphological similarity to the blood pressure waveforms. A common and simple method for non-invasively acquiring peripheral pulse signals with high morphological similarity to the blood pressure waveforms is photoplethysmography (PPG)20,21,22,23,24,25. PPG allows to measure changes in microvascular tissue perfusion caused by pressure changes via reflection or transmission of light impulses and contains valuable information about the cardiovascular system26,27,28. In the application context, it might therefore be a feasible alternative to invasive blood pressure measurements.
Previous approaches use in vivo PPG to detect stenosis, they include measuring the pulse rise time at the toes29, or deep learning based approaches on spectrograms created from PPGs30.
The shape of the measured PPG, including the pulse rise time, is, among other parameters, dependent on mean blood pressure, age and heart rate31,32. It might therefore give false results if not regarded in conjunction with the patients overall condition.
Instead of relying on the PPG wave shape alone, using a transfer kernel-based approach removes the dependence on boundary parameters, while retaining information about morphological differences (i.e., channel characteristics). A transfer function-based approach has previously been used for detecting aneurysms in ref. 19. The term “Transfer kernel features” is a technical term that refers to a method of modeling how blood flow changes between measurement sites. These transfer kernels are convolution kernels, allowing us to define the channel characteristics in a different form. The main advantage of this approach is the fact that one works in the time domain, and it is easier to estimate parameters in the time domain than in the frequency domain. Moreover, the quasi-periodic aspect of the pulse wave is considered correctly in the time domain, whereas, due to incorrect cutting, this is not the case in the frequency domain, because it introduces window bias effects.
In this work, in vivo PPG measurements measured at both thumbs and toes from vascularly healthy patients, as well as patients with severe stenosis of the pelvic arteries, are used to calculate per-patient transfer function features based on convolution kernels. For every patient, exactly two measurements under identical conditions are recorded, such that more data is available, but every patient is equally weighted. The data of 42 patients was included in the analysis, i.e. 84 measurements composed by 336 singular signals. The second measurement was originally intended as a possible substitute in the event that the first measurement was unusable. As almost every measurement was usable, we always included two measurements per patient in the evaluation and classification.
A schematic overview on the signal path from the four raw signals of an exemplary patient to the four calculated kernels is given in Fig. 1. Note that all signals are treated in the same way and there are no differences between the different measurement sites. Note that four transfer kernels were computed per measurement, each comprising 500 samples. After applying median pooling, 50 features were extracted per kernel, resulting in a 200-dimensional input vector per measurement.

Column a shows the four raw signals of an exemplary patient with stenosis, whereas column b presents the four kernels, which are created at the end of the signal processing pipeline. (Original work by C. Teichert using Affinity Designer 2 and draw.io).
A random forest classifier was trained on those features and validated. To overcome the limitations of the small available in vivo dataset, the cross-validation splits in training and test sets are randomly repeated and the mean accuracy, sensitivity and specificity serve as measures for the performance of the proposed algorithm.
The proposed method is simple to use, cost-effective in comparison to imaging methods and the patient receives his results instantaneously. In contrast to ABI, the patient has no compression feeling and the localization of the stenosis may be obtained.
All numerical calculations were done using Python 3.11.4, Scipy33, Numpy34, Scikit-Learn35, and the open-source available lab-internal pyProcessingPipeline36, unless otherwise noted.
Results
Classification of control and stenosis group (Nc = 26 and Ns = 16, respectively) was performed by a random forest classifier37 trained on features extracted from multi-site PPG measurements, as described in sections “Feature extraction” and “Classification”.
Using the cross-validation scheme from “Cross-validation setup” for binary classification on unseen samples of both the control and stenosis group, a mean classification accuracy of 82.6% ± 2.31% was achieved. Figure 2 shows the distribution of the accuracies for every of the 400 runs in the “Cross-validation scheme”. According to the uneven distribution of patients between the control and double-sided stenosis group, this accuracy score is biased towards higher values.

Each run is a 10-fold cross-validation, and mean accuracy and standard deviation are built up from this distribution. The mentioned mean accuracy here is 0.1 % higher than in the main text. This is due to the random choice of different cross-validations and the resulting minimal differences in the distribution if the evaluation scheme is repeated.
Sensitivity was calculated as 0.750, while specificity yields 0.865 (both calculated from Table 1), assuming a positive outcome generated at the stenosis being diagnosed. Table 1 was generated by summing all true positives, true negatives, false positives and false negatives over every cross-validation fold and then normalizing it to the total number of measurements Nt = 84 (two per patient), resulting in a mean confusion matrix over all validation folds using unseen samples only.
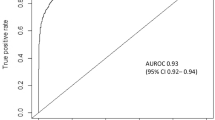
Figure 3 presents visually the performance of the classifier by a mean ROC curve that is calculated over the ROC curves for every of the 400 runs.

Here the mean ROC curve and its standard deviation are presented.
An overview of the kernel features calculated by, e.g., Table 1 is shown in Fig. 4.

Indices correspond to the pooled features, where 0 to 49, 50 to 99, 100 to 149, and 150 to 199 belong to hll, hrr, hlr, and hrl, respectively. The y-axis is given as arbitrary units, because relative comparison rather than absolute values is in focus. The data dimensions can be summarized as follows: (i) 42 patients comprising 2 measurements each, i.e., 84 measurement instances (ii) Each measurement ⇒ 4 transfer kernels (500 samples each) (iii) Median pooling ⇒ 50 features per kernel iv) Final input per instance ⇒ 200-dimensional feature vector.
Averaging the kernels for every body side instead of appending them as in Equations (9) and (10) (see Fig. 5) results in the classification as given in Table 2.

The classification accuracy over all repeated cross-validation folds for the averaged kernels was 80.1% ± 1.96%, with sensitivity of 0.719 and specificity of 0.846 (calculated from Table 2).
The absolute values of the differences between the median kernel features for both classes, i.e. control group and stenoses group, are presented in Fig. 6. The feature importance for the classifier is also shown here and show good congruence with the observed differences between the median kernel features.

Indices correspond to the pooled features, where 0 to 49, 50 to 99, 100 to 149, and 150 to 199 belong to hll, hrr, hlr, and hrl, respectively. Obviously, there is a good agreement between the absolute values of the feature differences and the feature importance.
Discussion
As mentioned in the introduction, the large number of cases of LEAD and simultaneously good prospects of disease improvement through risk factor modification emphasize the value of early detection. Ideally, this is done using a cost-effective procedure that is suitable for screening.
Previous PPG-based approaches, such as using the pulse rise time29 or spectrogram30 rely on the shape of the PPG measured at the lower body, typically the big toes.
These time domain features of the pulse wave are not suitable for robust analysis:
The main disadvantage of this approach is that the waveform differs from patient to patient and also shows different morphological characteristics simply due to differences in blood pressure and age-dependent vascular changes31,32. Additionally, local vascular changes such as aneurysms or stenoses alone have a relatively small influence on the pressure and flow waveform, and hence on the waveform of the PPG38 (Fig. 4).
Therefore it might be better to analyze the whole channel characteristics using a transfer kernel-based approach. Describing a system in this way usually entails measuring the response of the system to either a unit impulse or a unit step function. In practice, however, instead of externally disturbing the system, the heart’s central aortic pressure (CAP) waveform is used as a generator. Given a CAP and a peripheral pressure waveform18, could determine the location and degree of stenosis in vitro.
However, it is difficult to measure the CAP directly. Measurement of the CAP either requires invasive procedures (e.g., aortic catheterization), or depends on peripheral blood pressure recordings which are scaled or transformed to more closely resemble CAP39. Instead of measuring peripheral blood pressure and using some transfer function, the established morphological similarities between PPG and blood pressure20 should allow the PPG measured at the hand to be used as a surrogate input signal for the CAP.
Describing the channel characteristics from hand-to-toe-PPG using a transfer kernel should still contain information about the presence of stenoses, independent of the patient-specific PPG waveform differences. The signal measured at the hand can be thought of as a convolution of the CAP with some unknown kernel harm as
with xCAP being the PPG signal that is induced by CAP, ⊗ being the convolution operation, and yhand being the measured PPG at the hand. Assuming there exists some inverse kernel \({h}_{arm}^{-1}\), we can multiply Equation (1) by this element and rewrite the CAP input signal as
Analogous the measured foot PPG yfoot can be written as
with hleg being the kernel that transforms the CAP PPG-signal into the measured signal. Substituting xCAP from Equation (2) gives
hence using a hand-signal as a surrogate for the CAP, we are actually calculating \(h={h}_{arm}^{-1}\otimes {h}_{leg}\) instead of h = hleg. This should be similar to first using a specific transfer function transforming the hand-PPG into the CAP. Assuming no severe angiopathy of the upper limbs, this should still allow us to assert some influence of the occlusive disease on the kernel.
In general, characterizing such a system would require a multi-dimensional, non-linear approach incorporating patient-specific parameters, such as the age, (non-stationary) heart rate, and viscoelastic non-linearities of the arteries. This is due to the fact that the cardiovascular system is a multi-dimensional non-linear system, with, amongst other things, arterial wall stiffness and pulse wave velocity being dependent on mean arterial pressure31, as well as pulse rise time (and therefore shape of the PPG) being dependent on age and heart rate32.
Typical possible approaches for characterizing these types of complex biological systems are e.g. the Volterra series or the Wiener series. Here, the output is based on a linear combination of 0d, 1d and higher dimensional convolutions with finite memory, where non-linearities can be approximated with an arbitrarily small error using finite amount of kernels40.
However, using those approaches is not feasible without additional information or assumptions on known functions that drive the system.
Therefore, these approaches can not be used in the present situation. Instead, since the measurement protocol during the clinical trial enforces a measurement at rest, the present non-linearities, such as the artery compliance, are assumed to be approximately linear over the given range of parameters. This steady-state assumption (e.g., with constant system parameters such as mean arterial pressure) eliminates the need for higher order integrals, so that the measured system output y(t) at time t can be written using a regular convolutional integral with some multi-dimensional kernel h and the measured input x(t) as
with h dependent on the (unknown) constant system parameters such as the mean pressure \(\overline{p}\) and the channel characteristics of the artery.
Taking into account the small sample size in the clinical trial, we decided to neglect patient-specific system parameters and use a simple 1d kernel h. While the inter-patient parameters are different (compare, e.g., the blood pressure in Table 3), assuming constant patient parameters is what enables us to compare the estimated kernels. All kernels calculated for the stenosis patients can be considered slices of some higher dimensional kernel \({h}_{stenosis}(\tau ,\overline{p},\ldots \,)\), likewise all control kernels can be considered slices of \({h}_{control}(\tau ,\overline{p},\ldots \,)\).
Classifying kernels based on some similarity measure requires the kernel space to be continuous, so that while intra-group kernels may differ based on their system parameters, comparison should obtain higher similarity scores than for inter-group kernels. Given the accuracy results in section “Results”, the assumption that the kernels between patients are comparable, at least along the parameter space given in Table 3, holds.
According to discrete measurements of the input and output signals, a discrete kernel estimation has to be applied.
Assuming a time-invariant linear system that does not depend on future values in time, the lower integration limit in Equation (5) is zero. As the measurement protocol ensures that the measurements are started in a resting state, we assume a system with steady-state conditions and application of the upper integration limit of t, leading to
where y(t) is the output of the system measured at the foot, while x(t) is the input measured at the hand at time t, respectively. Then h(τ) is the desired kernel estimate.
In discrete convolution, however, the integral is written as the sum
where y(n) and x(n) are the n-th measured output and input sample, respectively, while h(i) is the kernel estimate.
The motivation for this convolutional approach is the following:
The cardiovascular system can be described by ordinary differential equations (see e.g., refs. 9,41,42). These ordinary differential equations can be expressed as state-space models (see e.g., ref. 43). This description incorporates the transfer function approach in the frequency domain. It is well known that state-space models (e.g., of the cardiovascular system or in general) can be transformed into a convolutional form44.
Hence, the convolution kernels allow us to define the channel characteristics in a different form. The main advantage of this approach is the fact that one works in the time domain, as it is easier to estimate parameters in the time domain than in the frequency domain. Moreover, the quasi-periodic aspect of the pulse wave is considered correctly in the time domain, whereas due to incorrect cutting, this is not the case in the frequency domain, because it introduces window bias effects.
Scientifically, a transfer kernel represents the mathematical model that describes how input signals (thumb PPG) transform as they propagate through the cardiovascular system to output signals (toe PPG). It effectively characterizes the system’s response and can highlight abnormalities like stenosis by identifying disruptions in the signal path.
Similar approaches are known for the case of pressure waveforms instead of PPG where, e.g. ref. 45 explores how to obtain the aortic pressure waveform from multiple peripheral artery pressure waveforms.
Considering Equation (7) for discrete signal length n and rewriting it in matrix form leads to
where X is the non-symmetrical n × m Toeplitz matrix of the input and h is the unknown kernel. Since the system does not include any decaying samples where the input has stopped, we set n = dim(x) and m = dim(h), ensuring a full overlap of the kernel and signal.
According to these assumptions the estimate of the kernel is performed using the least squares solver.
As seen from Fig. 4, the stenosis kernels are quite noisy compared to the control kernels. As an alternative to concatenating all four kernels (as was done in Equation (11)), one might be inclined to simply average the kernels over all sides. Assuming correlated kernels and uncorrelated noise, this will improve the signal-to-noise ratio (SNR) significantly.
While the arterial system is not perfectly symmetrical, the path of the pressure wavefront from the heart to each arm and each leg can be decomposed into approximately symmetrical segments. Differences between the left and right arm are limited to a slightly longer distance from the ascending aorta for the left arm, and the split from the brachiocephalic artery for the right arm. Those differences are small in nature compared to the overall signal path from the heart to each hand. We can therefore assume both arm kernels to be approximately the same:
A similar argument holds for the signal path from the heart to both feet, which also allows us to assume both leg kernels to be approximately the same:
Based on these assumptions, the kernels are averaged, the median kernels over all patients for control and stenosis group, are shown in Fig. 5, leading to an improved SNR, meaning a smaller range of 5th/95th percentile values, compared to the kernels from Fig. 4, confirming the assumption that the measurement noise is uncorrelated.
However, during evaluation, we found that the averaged feature kernels result in a slightly worse classification score than simply concatenating the kernels. The feature importances in Fig. 6 indicate that not all kernels are considered equally important by the subsequent random forest classifier. Instead, features from hrr and hlr, which contain information about the right leg have a higher importance than those kernel features derived from the left leg.
This indicates that, in contrast to the initial assumption, the asymmetry of the human cardiovascular system is significant.
We note that the degree of stenosis in the double-sided stenosis patient cohort is slightly higher on the right side (75% to 100%) compared to the left side (50% to 100%) as described in “Statistical analysis of patient cohort”. This also explains the decreased performance in the case of the side-averaged kernel features.
The transfer kernel models were calculated for every set of simultaneous measurements, and there were exactly two such sets for each patient. The fact that the modeling was done on a per-patient basis ensures personalized detection of stenosis characteristics.
Furthermore, the choice of a random forest classifier for the classification task is reasonable. The random forest is chosen as it is conceptually easy to understand while still being one of the more powerful classification algorithms in use today46,47. Using both the random subspace method and bootstrap aggregation, it is generally robust against overfitting37,46, which promotes generalization for unseen samples even for small datasets. Additionally, the way in which each feature influences the decision purity allows for estimating feature importance from the trained random forest, aiding in subsequent analysis.
The estimated values for the feature importance support the claim that the presented method is robust, i.e., it is not affected by noise, which is partly present, and the decision of the classifier does not rely on noise or artifacts.
Other classical machine learning models such as SVM and KNN have been considered also, but delivered poorer results. Besides their already mentioned robustness, random forest classifiers can describe as well linear as non-linear boundaries47,48. Moreover, due to the small dataset deep learning methods are not applicable, but may be applied for large datasets in future, if they are once available.
Another important point is the multiple k-fold cross-validation that is applied. The validation scheme presented in “Cross-validation setup” is suggested in ref. 19 and allows to mitigate some of the problems of the k-fold cross-validation arising for small datasets, where a simple permutation of validation folds would produce vastly different performance values. Averaging the accuracy over multiple cross-validations leads to a mean accuracy on unseen data, while smoothing out the high variability between multiple validation runs. Resulting averages are smaller than peak accuracies, but in contrast, are better measures for practical applications. In particular, these thoughts also justify the choice of k-fold cross-validation instead of leave-one-out.
The discussion of the results and the study presented here is concluded by a comparison with other diagnostic procedures and a discussion of the applicability in medical practice and the limitations of the study. The new diagnostic method for LEAD presented here is complementary to existing diagnostic tools. ABI, Doppler, and CT angiography are all well-established diagnostic tools, but are not suitable for a low-cost screening method that is available at the primary care level and can give a first indication for LEAD. If the method described here indicates LEAD, we encourage you to use further diagnostics to confirm this diagnosis.
Actually, the ABI is the first-line non-invasive test for screening and diagnosis of LEAD. However, the ABI allows no conclusions about the localization of the stenosis and the underlying pathoanatomy, and it could be inconvenient for the patient. Doppler sonography allows the simultaneous examination of pathoanatomy and hemodynamics, but its accuracy depends on the physiognomy of the patient and the skills of the examiner. Moreover, it is not always available on the primary care level. CT angiography, finally, is costly, of limited availability, and therefore not suitable for a comprehensive screening.
Our method is less expensive, non-invasive, has no known risks, and can be applied as a screening method at the primary care level. That means that it might be included in regular checkup examinations starting at a certain age or for patients with risk factors. If this method diagnoses LEAD, the patient is encouraged to perform further diagnostic tools, such as image-based methods. The method complements the existing diagnostic tools. This could be a significant improvement in the early detection of LEAD and therefore maintain the quality of life or even the life of many patients.
As the methods presented here are based on a proof-of-concept study, some limitations remain before clinical application. A sample size of the clinical study makes it obligatory to ignore patient-specific system parameters in the kernel estimation. The influence of, e.g., heart rate variations, weight, age, and other patient-specific parameters is incorporated using bigger datasets. More data is therefore needed to finally validate the results, e.g., from a multi-center study.
Table 3 and Supplementary Table 1 provide only information on the demographics of the dataset. However, no metadata are included in the classification process. The SOP of the study ensures, moreover, that we can expect that the dataset is relatively homogenous and therefore there are no important differences within the dataset caused by demographic factors. However, it is true that demographic aspects can influence PPG signals and it is a limitation of the study that this could not be analyzed further. It would thus be interesting to analyze these factors in future research. As already stated, more data is needed to do this.
The CAP surrogate signals measured at the hands introduce errors in the estimated kernels. However, due to its proximity to the aorta, the carotid artery is frequently used instead, but as for the ABI, getting reasonable measurements at the carotid is highly operator-dependent, leading to large variations and consequently making it an impractical screening method39.
As reliable methods for PPG measurements at the carotid are established, future clinical studies incorporating these signals might improve the classification scores further than simply increasing the size of the dataset.
In conclusion, the new diagnostic method for LEAD shows promising results, but, due to the small size of the dataset, it has to be validated on much larger datasets that are collected from a multi-center study. These new datasets would also enable us to improve our method further, incorporate demographical information, and evaluate other machine and deep learning methods.
Methods
Dataset and design of the clinical study
The proposed diagnostic method is based on a dataset obtained in a clinical study performed at the University Hospital Tübingen (study no. 136/2018801) in which 78 patients were included. The patients were divided into three groups:
-
i.
control group (CG)
-
ii.
aneurysm (A)
-
iii.
iliac artery stenosis (S)
The control and aneurysm group includes 55 patients already described in ref. 19; however, the stenoses group was not considered for classification purposes yet.
In this article, we propose a reasonable method to classifying the control and stenosis group. The results are based on diagnoses obtained by the gold standard, the computed tomography angiography (CTA).
The study was approved by the ethics committee of the Medical Faculty, University Tübingen (study no. 136/2018801)19. Patients gave their written informed consent prior to entering the study. All patients were treated as intended due to their illness, no medical decisions were influenced by the study protocol, no additional diagnostic procedures, particularly no imaging studies involving radiation, were triggered by the study protocol. All patients treated at the Department of Thoracic and Cardiovascular Surgery, University Medical Center Tübingen, between August 2018 and June 2019 were screened for eligibility in this study. All patients suffered from diseases such as pulmonary masses, aneurysms, and iliac artery stenoses.
According to their diseases, the 78 patients were divided into study groups based on the available CTA datasets, each group containing 27 (group i) and 28 (group ii), and 23 (group iii), respectively, patients:
-
i.
Control group (CG): Vascularly healthy subjects. No stenoses in the aorta or the pelvic arteries, diameter of the aorta in the entire thoracic and abdominal course 40 mm (except aortic sinus).
-
ii.
Aneurysm group (A): detection of a thoracic or abdominal aortic aneurysm with a diameter of 45 mm.
-
iii.
Stenoses group (S): high-grade vascular stenoses with degree of stenosis larger than 70%, occlusions of the pelvic arteries (aa. iliacae com., and/or aa. iliacae externae) clinically at least Fontaine stage IIb.
Patients, who for any reason, e.g. diameters between 40–45 mm between the sinotubular junction and the aortic bifurcation, could not be assigned to one of the above-mentioned groups, were excluded from the study. For the exact inclusion and exclusion criteria see the Supplementary Note 1.
Measurement device and study protocol
The measurement device was previously described in ref. 19; the measurement followed the study protocol described there.
The PPG device +5 V (PPG, TMSi, Ref 95-05800-0001-0) has been developed by the own laboratory and has been approved as a medical device by Applied Biosignal (Weener, Germany) and TMSi (Oldenzaal, The Netherlands). It uses light of 660 nm wavelength and provides pure raw signals, i.e., there is neither phase shift nor phase distortion by signal processing.
In comparison, standard transducers have strong influence on signals by phase-shifting filtering and use strong intensity correction to produce a “clean” PPG curve. These common changes could have more impact than the information that we want to deduce from the signals.
In this article, we consider four different PPG-signals recorded simultaneously at multiple sites of every patient:
-
i.
PPG probe placed at the right thumb
-
ii.
PPG probe placed at the left thumb
-
iii.
PPG probe placed at the right toe
-
iv.
PPG probe placed at the left toe
These measurement locations were selected following the subsequent considerations: In49, optimal measurement locations for the detection of stenosis were determined. In the clinical study at the University Hospital Tübingen, similar, but more easily accessible locations were selected. Besides thumbs and toes, additional measurements were done at both temples. Moreover, the signals measured at both thumbs and toes have shown promising results in the analysis of the classification problem of aortic aneurysms in refs. 19,50, which is similar to the classification problem of stenoses.
As stated in ref. 19, the PPG-signals were recorded over 60 s at a sampling frequency of 2048 Hz. To remove artifacts by the placing and removal of the sensors, the first five and last five seconds of each measurement are excluded, such that signals of 50 s length remain. The remaining pre-processing is the same as in ref. 19 and explained in section “Feature extraction” et seqq.
Computed tomography angiography
As stated in ref. 19, all computed tomography angiography (CTA) studies were performed prior to the study-enrollment during regular medical care with the aim to diagnose the primary illness of the patient. The process of image acquisition, processing, and analysis has been described elsewhere before in ref. 19 and in ref. 51. For all patients in the study, curved multiplanar reformats (CPR) were produced by manually defining the aortic central line with a 3D-Bezier-path (see Fig. 7, which is a reprint of ref. 19 (Fig. 2).

1: lateral (sagittal) view of the aorta and its anatomical relations (thick slab view), 2: curved multiplanar reformation (CPR), displaying the aortic diameter- and length measurement, 3: true-short axis views of the aorta at the respective landmark for determination of the diameter; for the definition of D1, …, D11, L1,…, L6 see19. Their definitions adhere to the guidelines57,58,59 except where otherwise noted in Appendix B. of ref. 19. This Figure is reprinted with permission from [ref. 19, Fig. 2]. (The figure was published by the authors in [ref. 19, Fig. 2] under the CC BY-NC-ND license.) For more details on the used CT scanner and software package, see ref. 19.
From these CPR, aortic length values and diameter values at defined landmarks were measured. See [ref. 19, section 2.1.3] for further explanation of the determination of the length and diameter values and the choice of the corresponding landmarks. See also the Supplementary Note 1 and Supplementary Table 1.
Statistical analysis of patient cohort
The clinical study consists of data from 78 patients, thereof 27 are in the control group, 28 are in the group with aneurysms, and 23 are in the group with stenoses. In this article, we consider only the data from the control group and the group of stenoses, whereas the data from the aneurysm group are already described in previous articles (ref. 19 and ref. 50). More general statistics are collected in Table 3. Similar to the description in ref. 19 and ref. 50, further statistical analysis of the anatomical average can be found in Supplementary Table 1.
Moreover, there are 19 patients with stenoses on the right side of length 4.665 ± 3.738 cm and degree 75−100%, whereas there are 20 patients with stenoses on the left side with 3.548 ± 1.789 cm and degree of 50−100%. In particular, there are 16 patients with double-sided stenoses.
Feature extraction
This and the following subsections are dedicated to the description of the signal processing and feature extraction.
Algorithm 1
Pseudocode for feature extraction using raw multi-site PPG signals. Detailed descriptions of all processing steps are given in the sections to the right.
for all x ∈ PPGs do
x ← x[5 s : 55 s] ⊳ (4.6)
x ← Highpass (x, cutoff = 0.5 Hz)
x ← Lowpass (x, cutoff = 30 Hz)
imfs ← EMD (x) ⊳ (4.7)
x ← Sum (imfs[1: 4])
x ← Downsample (x) ⊳ (4.8)
x ← normalize (x) ⊳ (4.9)
ifx ∈ lower body then
x ← Delay (x) ⊳ (4.10)
end if
end for
hll ← Kernel (xlefthand, xleftfoot) ⊳ (4.10)
hrr ← Kernel (xrighthand, xrightfoot)
hlr ← Kernel (xlefthand, xrightfoot)
hrl ← Kernel (xrighthand, xleftfoot)
return Pooling ([hll, hrr, hlr, hrl]) ⊳ (4.11)
In order to realize an operator-independent screening method for stenosis, we firstly propose a classification method based on data of the control group and double-sided stenosis group. Features were calculated via a convolution kernel from peripheral PPG measurements.
The database was confined to patient measurements containing at least two measurements. To maintain the similarity of the data, only two measurements per patient were used in case of three or more available measurements per patient. This truncation prevents over- or underrepresentation of patients, which could otherwise skew the results by overfitting to these patients' specific features. After preselection, the control and double-sided stenosis groups now consist of 26 and 16 patients, respectively.
The proposed method consists of both a feature engineering and a classification part, as described in “Classification” (see Algorithm 1). The pseudocode of the feature engineering is also depicted as a processing pipeline in Fig. 8. Features are based on the transfer kernel approach, based on assumptions from the section “Discussion”.

Schematic overview of the processing pipeline explained in Algorithm 1, using four PPG measurement locations as input (a), a time delay to postpone the foot signals (b), the kernel estimation (c) and the resulting kernels (d) with subsequent feature vector after median pooling (e). A more detailed overview of the filtering and normalization is shown in (f).
Pre-processing
Prior feature extraction, each signal was truncated between 5 s and 55 s to both (i) remove artefacts stemming from initial sensor placement and (ii) obtain similar signal length. Baseline drift and high-frequency noise were reduced using a zero phase highpass- (fc = 0.5 Hz) and subsequent lowpass-filter (fc = 30 Hz), as suggested in ref. 19.
Empirical mode decomposition
Empirical mode decomposition (EMD) is a method that allows for decomposing a signal into its orthogonal oscillatory components, the so-called IMFs52.
EMD is used to improve the results of the digital filters, by discarding the IMFs containing remaining high-frequency noise and baseline drift. The masked sifting approach from ref. 53 is used to generate the IMFs, forcing specific frequency components to end up in the same indexed IMF every time54. This allows us to automate the cleanup process without having to manually select IMFs to discard for every patient.
EMD was performed using the mask_sift functionality from the emd python package55, with masking frequencies of 20, 10, 5, 2.5, 1.25, and 0.625 Hz, resulting in 6 IMFs, of which the first and last are dropped, removing the remaining high-frequency noise and baseline drift, respectively.
Downsampling
Computation time for the subsequent steps, such as kernel estimation, is reduced by downsampling from fs = 2048 Hz to 1024 Hz. This reduction by a factor of two is reasonable because the high-frequency components were previously filtered, i.e., no aliasing will occur. However, due to the time-domain approach, we note that further reduction will lead to reduced time resolution of the kernels and thus to unfavorable binning of time events in the kernel.
Normalization
Overall absolute amplitude of the PPG differs from patient to patient, and may also vary based on external conditions such as ambient light, or internal conditions such as autonomic nervous system activity56. Without normalization, these differences will introduce errors during kernel estimation and classification, especially if the beat-to-beat amplitude variation from the foot waveform differs from the variation in the hand waveform. Therefore, signal normalization is required.
Applied normalization scheme is based on both a frequency- and time-domain approach. Firstly, a Fourier transform of the signal is calculated, and the amplitude of the fundamental frequency is determined using the absolute value in the frequency domain. Each signal is normalized so that the amplitude of this base frequency is equal to 1. This preparation step allows the use of the same minimum height parameters for the peak finding in the time domain throughout all patients.
Subsequently, peak-to-peak indices for local maxima and minima, one for each cardiac cycle, are found using a peak-finding method in the time domain. Piecewise linear interpolation is applied to create a lower envelope using the minima, which is subtracted from each signal.
Likewise, the upper envelope is calculated using local, which is finally used for point-wise division of the signal.
Kernel estimation
A linear time-invariant system is characterized by its input impedance, i.e., the response to a unit impulse. Since it is not feasible to generate an infinitely short unit impulse as an input signal for the arterial tree, the method is based on the heart as a driving mechanism. As opposed to the unit impulse, the CAP does not contain all possible frequencies. Therefore, application to characterize the system kernel for specific frequency contents as given by the CAP does not allow the calculation of the output for any given input signal. It contains sufficient information to quantify stenosis effects in the observed arterial pathway.
According to above assumption, the kernels for each patient are calculated as:
-
i.
left hand to left foot (hll),
-
ii.
left hand to right foot (hlr),
-
iii.
right hand to right foot (hrr) and
-
iv.
right hand to left foot (hrl).
The kernel length was chosen to be 1024 Samples (1 second). Making sure that the output follows after the input, therefore enforcing causality, is done by adding a delay of 200 ms to both the left and right foot signal of each patient.
Only the first 500 samples from each kernel are kept, as the remaining samples between control and stenosis kernels are almost equal. Keeping all samples did not improve classification accuracy compared to the cut kernels.
Finally, all kernels are concatenated, creating a single feature kernel h from all four subkernels:
where n = 500.
Median pooling
Because of residual noise in the estimated kernels, we utilize a pooling step to both reduce the dimensionality of the kernels as well as improve the signal-to-noise ratio. This dimensionality reduction is feasible because the estimated kernels are oversampled, meaning this should improve the noise robustness without losing information. The n-th feature pool y(n) of h is calculated as
where med is the median and m is the number of samples per pool. The pooled feature kernels can be seen in Fig. 4.
Classification
Binary classification between the control and stenosis group is performed on the median pooled kernel features using Scikit-Learn’s RandomForestClassifier35. Before training, the diagnoses of either the control group or the stenosis group are encoded using a LabelEncoder35.
Cross-validation setup
Validation was performed using multiple k-fold cross-validation with 10 folds each.
The small sample size of the underlying clinical trial means that using a 10-fold cross-validation may result in vastly different accuracy scores per fold. To mitigate this, multiple k-fold cross-validations with randomized folds are performed as explained in refs. 19,50, and the accuracy, confusion matrix, and feature importance are calculated for each fold. At the end, a mean accuracy and standard deviation, as well as a mean confusion matrix and mean feature importance, are calculated over all results.
During fold randomization, measurements from the same patient only end up in either the train or the test set, but not in both. This ensures that only unseen patients are used during testing.
Data availability
The data originates from a clinical study at the University Hospital of Tübingen (study no. 136/2018801). Unfortunately, we are unable to share these data due to the consent signed by the study participants, which did not include information on public data sharing. Our methods can be applied to most in vivo datasets of PPG signals at thumbs and toes, which contain vascular healthy patients and patients with lower extremity stenosis.
Code availability
Processing steps used in this study are available in the pyProcessingPipeline gitlab repository36.
References
Roth, G. A. et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J. Am. Coll. Cardiol. 76, 2982–3021 (2020).
Huppert, P., Tacke, J. & Lawall, H. S3 guidelines for diagnostics and treatment of peripheral arterial occlusive disease. Der Radiol. 50, 7–15 (2010).
Maca, T., Taheri, S., Pfleger, W., Zier, G. & Ingerle, E. Beckenarterien-pta bei dysgenetischer beckenniere. Z. f.ür. GefäßMed. 4, 24–26 (2007).
Diehm, C. et al. Association of low ankle brachial index with high mortality in primary care. Eur. Heart J. 27, 1743–1749 (2006).
Aboyans, V. et al. Editor’s Choice–2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in Collaboration with the European Society for Vascular Surgery (ESVS). Eur. J. Vasc. Endovasc. Surg. 55, 305–368 (2018).
Bauersachs, R. et al. A targeted literature review of the disease burden in patients with symptomatic peripheral artery disease. Angiology 71, 303–314 (2020).
Kim, E. S. et al. Interpretation of peripheral arterial and venous doppler waveforms: a consensus statement from the Society for Vascular Medicine and Society for Vascular Ultrasound. Vasc. Med. 25, 484–506 (2020).
Paisley, M. J., Adkar, S., Sheehan, B. M. & Stern, J. R. Aortoiliac occlusive disease. Semin. Vasc. Surg. 35, 162–171 (2022).
Huttary, R., Goubergrits, L., Schütte, C. & Bernhard, S. Simulation, identification and statistical variation in cardiovascular analysis (sisca)—a software framework for multi-compartment lumped modeling. Comput. Biol. Med. 87, 104–123 (2017).
Hughes, T. J. R. & Lubliner, J. On the one-dimensional theory of blood flow in the larger vessels. Math. BioSci. 18, 161–170 (1973).
Formaggia, L., Nobile, F. & Quarteroni, A. A One Dimensional Model for Blood Flow: Application to Vascular Prosthesis. In Mathematical Modeling and Numerical Simulation in Continuum Mechanics. Lecture Notes in Computational Science and Engineering (eds Babuška, I. et al.) Vol. 19 (Springer, Berlin, Heidelberg, 2002). https://doi.org/10.1007/978-3-642-56288-4_10.
Formaggia, L., Lamponi, D. & Quarteroni, A. One-dimensional models for blood flow in arteries. J. Eng. Math. 47, 251–276 (2003).
Alastruey, J., Parker, K., Peiro, J. & Sherwin, S. J. Lumped parameter outflow models for 1-d blood flow simulations: Effect on pulse waves and parameter estimation. Commun. Comput. Phys. 4, 317–336 (2008).
Formaggia, L., Gerbeau, J.-F., Nobile, F. & Quarteroni, A. On the coupling of 3d and 1D Navier–Stokes equations for flow problems in compliant vessels. Comput. Methods Appl. Mech. Engng. 6-7, 561–582 (2001).
Blanco, P. J., Pivello, M. R., Urquiza, S. & Feijóo, R. On the potentialities of 3D-1D coupled models in hemodynamics simulations. J. Biomech. 42, 919–930 (2009).
Fritz, M. et al. A 1D–0D–3D coupled model for simulating blood flow and transport processes in breast tissue. Int. J. Numer. Meth. Biomed. Engng. 38, e3612 (2022).
Quick, C. M., Young, W. L. & Noordergraaf, A. Infinite number of solutions to the hemodynamic inverse problem. Am. J. Physiol. Heart Circ. Physiol. 280, H1472–H1479 (2001).
Mair, A., Wisotzki, M. & Bernhard, S. Classification and regression of stenosis using an in-vitro pulse wave data set: Dependence on heart rate, waveform and location. Comput. Biol. Med. 151, 106224 (2022).
Hackstein, U. et al. Early diagnosis of aortic aneurysms based on the classification of transfer function parameters estimated from two photoplethysmographic signals. Inform. Med. Unlocked 25, 100652 (2021).
Martínez, G. et al. Can photoplethysmography replace arterial blood pressure in the assessment of blood pressure? J. Clin. Med. 7, 316 (2018).
Schukraft, S., Boukhayma, A., Cook, S. & Caizzone, A. Remote blood pressure monitoring with a wearable photoplethysmographic device (Senbiosys): protocol for a single-center prospective clinical trial. JMIR Res. Protoc. 10, e30051 (2021).
Aguirre, N., Grall-Maës, E., Cymberknop, L. J. & Armentano, R. L. Blood pressure morphology assessment from photoplethysmogram and demographic information using deep learning with attention mechanism. Sensors 21, 2167 (2021).
Tang, Q., Chen, Z., Ward, R., Menon, C. & Elgendi, M. Subject-based model for reconstructing arterial blood pressure from photoplethysmogram. Bioengineering 9, 402 (2022).
Joung, J. et al. Continuous cuffless blood pressure monitoring using photoplethysmography-based PPG2BP-Net for high intrasubject blood pressure variations. Sci. Rep. 13, 8605 (2023).
González, S., Hsieh, W.-T. & Chen, T. P.-C. A benchmark for machine-learning based non-invasive blood pressure estimation using photoplethysmogram. Sci. Data 10, 149 (2023).
Allen, J. Photoplethysmography and its application in clinical physiological measurement. Physiol. Meas. 28, R1 (2007).
Kyriacou, P. & Allen, J. (eds.) Photoplethysmography (Academic Press, 2021). https://shop.elsevier.com/books/photoplethysmography/kyriacou/978-0-12-823374-0.
Kaisti, M. et al. Hemodynamic bedside monitoring instrument with pressure and optical sensors: validation and modality comparison. Adv. Sci. 11, 2307718 (2024).
Allen, J. & Hedley, S. Simple photoplethysmography pulse encoding technique for communicating the detection of peripheral arterial disease—a proof of concept study. Physiol. Meas. 40, 08NT01 (2019).
Allen, J., Liu, H., Iqbal, S., Zheng, D. & Stansby, G. Deep learning-based photoplethysmography classification for peripheral arterial disease detection: a proof-of-concept study. Physiol. Meas. 42, 054002 (2021).
Cox, R. H. Pressure dependence of the mechanical properties of arteries in vivo. Am. J. Physiol.-Leg. Content 229, 1371–1375 (1975).
Allen, J., O’Sullivan, J., Stansby, G. & Murray, A. Age-related changes in pulse risetime measured by multi-site photoplethysmography. Physiol. Meas. 41, 074001 (2020).
Virtanen, P. et al. SciPy 1.0: Fundamental algorithms for scientific computing in Python. Nat. Methods 17, 261–272 (2020).
Harris, C. R. et al. Array programming with NumPy. Nature 585, 357–362 (2020).
Pedregosa, F. et al. Scikit-learn: machine learning in Python. J. Mach. Learn. Res. 12, 2825–2830 (2011).
Teichert, C., Mair, A., Haub, M., Hackstein, U. & Bernhard, S. Pyprocessingpipeline. online (2023). https://gitlab.com/agbernhard.lse.thm/agb_public/pyProcessingPipeline.
Ho, T. K. Random decision forests. In: Proceedings of 3rd International Conference on Document Analysis and Recognition. Vol. 1, 278–282 (IEEE, 1995).
Jin, W. & Alastruey, J. Arterial pulse wave propagation across stenoses and aneurysms: assessment of one-dimensional simulations against three-dimensional simulations and in vitro measurements. J. R. Soc. Interface 18, 20200881 (2021).
McEniery, C. M., Cockcroft, J. R., Roman, M. J., Franklin, S. S. & Wilkinson, I. B. Central blood pressure: current evidence and clinical importance. Eur. Heart J. 35, 1719–1725 (2014).
Korenberg, M. J. & Hunter, I. W. The identification of nonlinear biological systems: Volterra kernel approaches. Ann. Biomed. Eng. 24, 250–268 (1996).
Ottesen, J. T. Modelling of the baroreflex-feedback mechanism with time-delay. J. Math. Biol. 36, 41–63 (1997).
Olufsen, M. S. & Nadim, A. On deriving lumped models for blood flow and pressure in the systemic arteries. Math. Biosci. Eng. 1, 61–80 (2004).
Monzon, J. E., Pisarello, M. I., Picaza, C. A. & Veglia, J. I. Dynamic modeling of the vascular system in the state-space. Int Conf. IEEE Eng. Med Biol. Soc. 2010, 2612–2615 (2010).
Gu, A. Modeling sequences with structured state spaces. Ph.D. Thesis, Stanford University (2023).
Swamy, G., Ling, Q., Li, T. & Mukkamala, R. Blind identification of the aortic pressure waveform from multiple peripheral artery pressure waveforms. Am. J. Physiol.-Heart Circ. Physiol. 292, H2257–2264 (2007).
Géron, A. Hands-on machine learning with Scikit-Learn, Keras, and TensorFlow (O’Reilly Media, Inc., 2022).
Breiman, L. Random forests. Mach. Learn. 45, 5–32 (2001).
Auret, L. & Aldrich, C. Interpretation of nonlinear relationships between process variables by use of random forests. Miner. Eng. 35, 27–42 (2012).
Gul, R. & Bernhard, S. Optimal measurement locations for diagnosis of aortic abnormalities in a lumped-parameter model of the systemic circulation using sensitivity analysis. Int. J. Biomath. 10, 1750116 (2017).
Hackstein, U. & Bernhard, S. Comparison of machine learning techniques in the early detection of abdominal aortic aneurysms from in-vivo photoplethysmography data. Inform. Med. Unlocked 35, 101123 (2022).
Krüger, T. et al. Aortic elongation and the risk for dissection: the tübingen aortic pathoanatomy (TAIPAN) project. Eur. J. Cardio-Thorac. Surg. 51, 1119–1126 (2017).
Huang, N. E. et al. The empirical mode decomposition and the Hilbert spectrum for nonlinear and non-stationary time series analysis. Proc. R. Soc. Lond. Ser. A Math. Phys. Eng. Sci. 454, 903–995 (1998).
Deering, R. & Kaiser, J. F. The use of a masking signal to improve empirical mode decomposition. In Proceedings (ICASSP’05). IEEE International Conference on Acoustics, Speech, and Signal Processing, 2005., vol. 4, iv–485 (IEEE, 2005).
Rilling, G. & Flandrin, P. One or two frequencies? The empirical mode decomposition answers. IEEE Trans. Signal Process. 56, 85–95 (2007).
Quinn, A. J., Lopes-dos Santos, V., Dupret, D., Nobre, A. C. & Woolrich, M. W. EMD: Empirical mode decomposition and Hilbert-Huang spectral analyses in Python. J. Open Source Softw. 6, 2977 (2021).
Park, J., Seok, H. S., Kim, S.-S. & Shin, H. Photoplethysmogram analysis and applications: an integrative review. Front. Physiol. 12, 808451 (2022).
Erbel, R. et al. 2014 ESC Guidelines on the Diagnosis and Treatment of Aortic Diseases: Document Covering Acute and Chronic Aortic Diseases of the Thoracic and Abdominal Aorta of the Adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur. heart J. 35, 2873–2926 (2014).
Goldstein, S. A. et al. Multimodality Imaging of Diseases of the Thoracic Aorta in Adults: from the American Society of Echocardiography and the European Association of Cardiovascular Imaging: endorsed by the Society of Cardiovascular Computed Tomography and Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. 28, 119–182 (2015).
Hiratzka, L. F. et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the Diagnosis and Management of Patients with Thoracic Aortic Disease: A Report of the American College of Cardiology Foundation/american Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation 121, e266–e369 (2010).
Acknowledgements
The authors express their gratitude to Charlotte Degünther and Tobias Krüger and his team at University Hospital Tübingen, who performed the clinical study and measured the in vivo data analyzed in this article. We thank the Klinik für Thorax-, Herz- und Gefäßchirurgie of University Hospital Tübingen and its head Christian Schlensak for the opportunity to perform the clinical study and constant support. Moreover, we thank Charlotte Degünther, who monitored the clinical study together with Tobias Krüger. The clinical study was supported by the German Federal Ministry of Education and Research (BMBF) within the project CardioInBaMed (grant number FKZ: 13GW0204B, no involvement). Urs Hackstein was partially financed through the EU-project Qumphy. The project (22HLT01 QUMPHY) has received funding from the European Partnership on Metrology, co-financed from the European Union's Horizon Europe Research and Innovation Program and by the Participating States. The authors thank the handling editor, Mohamed Elgendi, and the two anonymous reviewers for critically reviewing our manuscript and their very helpful comments.
Author information
Authors and Affiliations
Contributions
S.B. conceived of the study idea and design. C.T. was responsible for improving the model design, training, and testing, and wrote the major parts of the initial manuscript. U.H. and S.B. supervised his work, and all authors participated in writing. U.H. was responsible for the statistical analyses, whereas T.K. performed the clinical study at University Hospital Tübingen. All authors critically reviewed the paper, all authors have a clear understanding of the content, results, and conclusions of the study, and agree to submit this manuscript for publication.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study was approved by the Ethics Committee of the Medical Faculty of the University of Tübingen (study no. 136/2018801).
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Teichert, C., Hackstein, U., Krüger, T. et al. Noninvasive detection of lower extremity artery disease using multi-site photoplethysmographic signals and machine learning. npj Biosensing 2, 25 (2025). https://doi.org/10.1038/s44328-025-00044-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s44328-025-00044-z
This article is cited by
-
Injectable ultrasonic metagels for intracranial monitoring
npj Biosensing (2025)
