
Abstract
Objective:
To characterize the delivery of genetic consultative services for adults, we examined the prevalence and organizational determinants of genetic consult availability and the organization of these services in the Veterans Health Administration.
Methods:
We conducted a Web-based survey of Veterans Health Administration clinical leaders. We summarized facility characteristics using descriptive statistics. Multivariate logistic regression assessed associations between organizational characteristics and consult availability.
Results:
We received 353 survey responses from key informants representing 141 Veterans Affairs Medical Centers. Clinicians could obtain genetic consults at 110 (78%) Veterans Affairs Medical Centers. Cancer genetic and neurogenetic consults were most common. Academic affiliation (odds ratio = 3.0; 95% confidence interval: 1.1–8.6) and provider education about genetics (odds ratio = 2.9; 95% confidence interval: 1.1–7.8) were significantly associated with consult availability. The traditional model of multidisciplinary specialty clinics or coordinated services between geneticists and other providers was most prevalent, although variability in the organization of these services was described, with consults available on-site, at another Veterans Affairs Medical Center, via telegenetics, or at non–Veterans Health Administration facilities. The emerging model of nongeneticists integrating genetics into their practices was also reported, with considerable variability by specialty.
Conclusion:
Both traditional and emerging models for genetic consultation are available in the Veterans Health Administration; however, there is variability in service organization that could influence quality of care.
Genet Med 16 8, 609–619.
Similar content being viewed by others


Main
Integration of genetic information into health care can improve health outcomes through improved diagnosis, risk assessment, prognosis, and treatment decisions. However, to fully realize the benefits of genetic information, it will be important to identify successful models of care,1 particularly for the field of adult genetics, which is growing due to increasing recognition of adults with genetic conditions and expanding genetic testing opportunities for adult-onset conditions.2
Delivery models for genetic consultative services were recently described in a systematic review of genetics in health3; they include (i) the traditional model of multidisciplinary specialist clinics or coordinated services between geneticists and other specialists—the latter is favored for adult-onset conditions—and (ii) the emerging model, in which genetic services are integrated directly within primary care and other specialties. The emerging model can be supported by information technology and software applications assisting in genetic risk assessment4,5 or by embedding genetic nurse coordinators or genetic counselors within clinics.6,7
The traditional model of multidisciplinary specialist clinics is generally organized as a regional genetic center, usually affiliated with an academic medical center, offering clinics for various patient-care needs (e.g., prenatal, cancer genetic, and pediatric genetic needs).3 These regional centers can provide expertise to smaller genetics clinics in the community, like a hub-and-spoke network.3 This can be achieved by the core (hub) facility accepting referrals from the peripheral clinics (spokes) or through the use of (i) “telegenetics,” which brings core genetic services into peripheral clinics via videoteleconferencing,8,9 and (ii) telephone genetic consultation, which provides core genetic services directly to patients.10,11
The health professionals providing clinical genetic consultative services are genetic specialists (medical geneticists, genetic counselors, and nurse geneticists) or non–genetics health-care professionals who are increasingly using genetics in routine care, including primary-care providers, other specialists, nurses, psychologists, and social workers.3 The lack of medical geneticists has been recognized as a serious problem compromising the delivery of genetic services with the traditional model,12 and the lack of training and awareness of genetics among non–genetics health-care providers is a challenge for the emerging model.13,14,15,16,17,18,19
The Veterans Health Administration (VHA) is the largest integrated health-care system in the United States, serving more than 8.3 million Veterans at 153 Veterans Affairs Medical Centers (VAMCs).20 The VAMCs are located within 21 Veterans Integrated Service Networks (VISNs) nationwide. Multiple VAMCs and their respective community-based outpatient clinics are connected within each network, and each network is connected to the central office in Washington, DC. Resources for health-care delivery are typically organized at the facility or network level. We conducted a Web-based survey of clinical leaders of various specialties in the VHA to determine the prevalence of the traditional and emerging models of genetic consultative service delivery, learn how these services are organized, and identify the health-care professionals who provide these services in the VHA.
At the time of the survey, we were aware of at least five VAMCs (Boston, MA; Houston, TX; Los Angeles, CA; Salt Lake City, UT; and Seattle, WA) that provide clinical genetic consultative services via medical geneticists on-site. In 2010, to expand genetic service delivery in the VHA, the agency launched the national Genomic Medicine Service based in Salt Lake City, UT, which staffs genetic counselors to provide telegenetic services to Veterans at VAMCs across the United States. Thus, given the variety of possible genetic consultative services, the VHA offers a unique opportunity to describe the organization of these services for adults.
Materials and Methods
Design
We conducted a cross-sectional, Web-based, structured key informant survey to ascertain organizational-level information about clinical genetic consultative services available at each VAMC. (Survey items are available upon request.) Informed by findings from qualitative, semistructured interviews with VHA clinical leaders from a variety of clinical specialties,21 we developed surveys for five clinical specialties: primary care, neurology, medical oncology, gastroenterology, and cardiology. The questions asked in each of the surveys were identical but were customized by referring to each specialty by name for specialty-specific items. Once the prototype survey was developed, we conducted cognitive pretesting with four primary-care clinicians, followed by review for content, language, and ease of use by a national VHA committee including chief medical officers and other clinical and administrative leaders. With this input, the survey was then finalized for each specialty. The Greater Los Angeles VAMC Institutional Review Board approved all study procedures.
Setting and participants
Survey responses from chiefs of primary care, neurology, medical oncology, cardiology, and gastroenterology at each VAMC were included in this study. Chiefs were identified through publicly available sources (e.g., facility websites) and by contacting the chief of Staff (i.e., medical director) of each VAMC. The primary-care chief was identified for most (142) of the 153 VAMCs. However, not all VAMCs have chiefs in other specialties. We were able to identify 110 neurology, 101 cardiology, 103 gastroenterology, and 103 medical oncology chiefs.
Data collection
Surveys for each specialty were in the field for 4–6 months. Before the launch of each specialty survey, an introductory e-mail was sent to eligible respondents from the national VHA director of each specialty and the national VHA director of genomic medicine. Up to six reminder e-mails were sent to nonresponders, followed by several phone calls, if necessary. Before the close of data collection, a final e-mail was sent from the national director encouraging participation from nonrespondents. Data collection across all specialty surveys occurred from November 2011 through September 2012.
Outcomes of interest
For this study, we focused on survey responses that described the availability and delivery of genetic consults, and we characterized facilities as having the traditional model or the emerging model for delivery of clinical genetic consults. We characterized genetic consultative services provided by medical geneticists with or without genetic counselors as the traditional model, and services provided by nongeneticists with or without genetic counselors were characterized as the emerging model.
We asked, “To the best of your knowledge, can clinicians at [name of VAMC] obtain a clinical genetic consult (either on- or off-site) for their Veteran patients?” If genetic consults were available, the chiefs were asked about the types offered, including consults in cancer genetics, neurogenetics, cardiovascular genetics, reproductive genetics, pharmacogenetics, and “other.” Facilities were characterized as having genetic consults available if at least one chief per facility reported their availability.
We also asked about the arrangements for each type of genetic consult; chiefs could select availability of consults on-site at their facility, at another VAMC, via telegenetics (telephone or videoteleconferencing), or at a non-VHA facility, or they could answer that they did not know. The VHA national Genomic Medicine Service based in Salt Lake City probably provided the telegenetic services because memoranda of understanding had been established with these facilities at the time of the survey (V. Venne, personal communication).
The facilities were then characterized according to a hierarchy regarding the type of arrangements reported, beginning with on-site consults available, followed by consults available at another VAMC, via telegenetics, and, finally, at a non-VHA facility. For example, if at least one type of consult was available on-site, then a facility was characterized as having on-site consults regardless of other reported arrangements. When a type of consult was available on-site, we asked about the types of clinicians providing the service. Response options included a specialist for the condition of concern (e.g., oncologist for cancer genetic consults, neurologist for neurogenetic consults), a medical geneticist, a genetic counselor, another type of physician, or another type of health-care provider. We did not ask about the types of clinicians providing the service at another VAMC or a non-VHA facility because we were advised that it would be unlikely that chiefs would be able to answer this question. One facility was excluded from analyses because the types of genetic consult arrangements were not described.
Because clinical services are organized at the facility or VISN level within the VHA, in order to characterize the model of genetic service delivery for VAMCs obtaining genetic consults from another VAMC we characterized these facilities as having the traditional model of genetic consultative service delivery if they were located within a VISN that had a medical geneticist at a VAMC providing genetic consults, whereas facilities located within a VISN that had a nongeneticist providing genetic consults were characterized as having the emerging model of genetic consultative service delivery.
To assess the emerging model of integrating genetic services within primary care and other specialties, we asked about the availability of tools within the electronic health record (EHR) designed to assist with genetic risk assessment and ordering of genetic tests, and about clinical activities typically expected from these clinicians relating to genetic risk assessment, testing, and management. The survey described specific scenarios for evaluation of patients who have signs and symptoms of a hereditary condition (diagnostic evaluation), are asymptomatic and at risk for a genetic disorder due to family history or other characteristics (predisposition evaluation), have a genetic test to inform drug selection or dosing (pharmacogenetic testing), and reproductive decision-making by patients (carrier screening for a recessive disorder). For each scenario, the chiefs were asked if their clinicians were expected to perform the pre- and postanalytic steps in the genetic testing process described in Figure 1 .

This framework represents the total genetic testing process conceptualized by the Centers for Disease Control and Prevention to assess the quality of genetic testing services. The framework has three phases: preanalytic, analytic, and postanalytic. The pre- and postanalytic phases comprise the clinical activities that relate to delivery of typical genetic consultative services—the focus of our study. The preanalytic phase begins with recognition of a patient who may have an inherited genetic condition or risk, usually based on personal or family history (step 1). If genetic testing is available and indicated, a genetic testing strategy is developed to refine the initial risk assessment or differential diagnosis (step 2). Informed consent (step 3) typically follows with varying degrees of formality (e.g., verbal or written), including discussion of the benefits, risks, limitations, and alternatives to testing. If the patient agrees to genetic testing (step 4), the test is ordered (step 5), and a specimen is sent to a laboratory (step 6). If the patient declines genetic testing, then recommendations are based on personal and family history (step 12). For certain situations, the preanalytic steps may be curtailed if genetic testing occurs as part of routine protocol in the laboratory, such as testing on tumor tissues; these situations may not require genetic consultation. There may be additional steps as well, such as an approval process that occurs somewhere between steps 5 and 8. The analytic phase comprises genetic testing activities performed in the laboratory (steps 7 through 9). The postanalytic phase comprises activities relating to management specific to a genetic risk or diagnosis, which may or may not include results of genetic testing. If genetic testing is performed, the ordering clinician receives a report (step 10), who then discloses the implications of the test result to the patient (step 11), and recommendations for management are made (step 12). Reprinted from ref. 36.
Independent variables
Most independent variables were obtained from the survey responses. However, the Area Resource File (http://arf.hrsa.gov) served as the source describing the area surrounding each VAMC, including the population density, whether it was a primary-care-shortage area, the number of male and female veterans per 100,000 population, and the number of medical geneticists per 100,000 population. Academic affiliation (defined as an affiliation with a medical school or medical school training program for residents) was derived by examining national VHA organizational data, including lists of academic affiliations found at the Department of Veterans Affairs Office of Academic Affiliations website (http://www.va.gov/oaa), key informant organizational surveys, and local VHA website facility descriptions.
Statistical analysis
We computed descriptive statistics to summarize the characteristics of facilities. We used t-tests to compare means of quantitative variables and χ2 analyses for homogeneity to compare the frequency distributions of categorical variables. Multivariate logistic regression was used to assess associations between availability of genetic consults and organizational characteristics that were significantly different (P < 0.05) in frequency between VAMCs with and without genetic consults available. All statistical analyses were performed using SAS statistical software, version 12.0 (SAS Institute, Cary, NC).
Results
Overall, 353 chiefs (63.1%) responded to the survey. Response rates for each specialty were as follows: primary care, 77.5% (110/142); neurology, 68.2% (75/110); medical oncology, 58.3% (60/103); cardiology, 54.5% (55/101); and gastroenterology, 51.5% (53/103). These chiefs represented 141 (92.2%) of the 153 VAMCs, with an average of 2.5 (range: 1–5) chiefs responding per facility.
Organizational characteristics associated with genetic consultative services
The ability to obtain genetic consults within the VHA or at a non-VHA facility was reported for 110 (78.0%) of the 141 VAMCs. Table 1 reviews the characteristics of the VAMCs according to consult availability. There were no significant differences in the proportions of chiefs responding from VAMCs with or without genetic consultative services made available within the VHA or at a non-VHA facility, and no significant differences were observed according to their regional location in the United States. There were only 10 on-site genetics experts (defined as providers with any formal genetics training, such as a master’s or PhD degree in human genetics or board certification in medical genetics or genetic counseling), and there were no significant differences in frequency of these experts at VAMCs with genetic consultative services compared with those without these services. However, availability of a local genetics champion (defined as someone who takes a leadership role in developing and/or promoting genetic services at his or her VAMC) was more frequent at VAMCs with genetic consultative services available compared with VAMCs without these services (31.2 vs. 9.7%; P = 0.017). Academic medical center affiliation was more commonly reported for VAMCs with genetic consultative services (89.0 vs. 65.5%; P = 0.002), and the number of medical geneticists per 100,000 population was more than twice that for VAMCs with genetic consultative services compared with VAMCs without these services (0.27 vs. 0.12; P = 0.046). Templates for comprehensive family-history documentation or decision support for ordering genetic tests were not available in the EHR at a majority of VAMCs, and they were neither more nor less frequent at facilities with genetic consultative services. Provider education on genetic topics was significantly more frequent at VAMCs with genetic consultative services (90.1 vs. 9.9%; P < 0.001).
In a logistic regression analysis including the four variables that were significantly more frequent at VAMCs with consultative services (i.e., genetics champion on-site, number of geneticists per 100,000 population, academic affiliation, and genetics education for providers), we found only academic affiliation (odds ratio = 3.0; 95% confidence interval: 1.1–8.6) and provider education on genetic topics (odds ratio = 2.9; 95% confidence interval: 1.1–7.8) to be significantly associated with genetic consultative services available within the VHA or at a non-VHA facility.
Types of genetic consults available
Chiefs from 70.2% (99/141) of the VAMCs reported the ability to refer Veterans for cancer genetic consults, followed by neurogenetic, 51.8% (73/141); reproductive genetic, 41.8% (59/141); cardiovascular genetic, 33.3% (47/141); and pharmacogenetic consults, 29.1% (41/141). Another 19.9% (28/141) of facilities also had “other” genetic consults available, which were usually described as consultative services for polyposis, thrombophilia, or general genetic concerns. Among the 110 VAMCs that could refer Veterans for genetic consults, 48.2% (53/110) had only one or two types of consults available, and these were usually cancer genetic and/or neurogenetic consults, and 41.8% (46/110) of the VAMCs had four or more types of consults available.
Organization of genetic consultative services
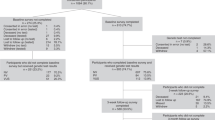
There was considerable variability in how genetic consultative services were made available at VHA facilities ( Figure 2 ). Among the 110 VAMCs that could refer a Veteran for a genetic consult, only 15.5% reported availability of a genetic consult within the VHA system (either on-site, at another VAMC, and/or via telegenetics). More than half (56.4%) had genetic consultative services available only at non-VHA facilities, and most of these (83.9%, 52/62) were through arrangements with academic medical centers. The remaining 27.3% of VAMCs obtain genetic consults from non-VHA facilities in combination with VHA-based care (i.e., genetic consults available on-site, at another VAMC, or through telegenetics) for the same and/or different types of consults. One facility with genetic consultative services did not describe its arrangements.

There were 31 Veterans Administration Medical Centers (VAMCs) without available genetic consults, and 110 VAMCs had genetic consults available. There were 21 VAMCs with on-site consults available, including six with on-site consults only, 10 with on-site consults and consults at non-VHA facilities, one with on-site and telegenetic consults; three with on-site, telegenetic, and non-VHA consults; and one with on-site consults and consults available at another VAMC. There were 19 VAMCs with consults available at another VAMC, including two with consults also available via telegenetics, and 13 with genetic consults also available at a non-VHA facility. There were three VAMCs that had only telegenetic consults available and four VAMCs that had both telegenetic consults and genetic consults available at a non-VHA facility. There were 62 VAMCs with consults only available at non-VHA facilities. VHA, Veterans Health Administration.
Availability of on-site genetic consultative services
Among the 21 VAMCs that provided on-site genetic consultation, only four reported having a breadth of services, i.e., with at least four types of consults available ( Table 2 ). These facilities had a medical geneticist on-site providing these comprehensive services, and for certain types of consults, non–genetic specialists were also involved, consistent with the traditional model of genetic service delivery involving multidisciplinary specialist clinics and coordination between genetics and other specialists. These four sites were among those already known to have on-site services before the survey. We did not identify any other VAMCs with an on-site, traditional delivery model. VAMCs with on-site medical geneticists generally did not obtain genetic consults through other arrangements, such as a non-VHA facility, via telegenetics, or another VAMC.
At the 17 other facilities with on-site genetic consults, only one or two types of consults were available, provided by non–genetic specialists, consistent with the emerging model of genetic consultative services delivery; one facility had a genetic counselor and oncologist providing cancer genetic consults. Unlike the VAMCs with on-site medical geneticists, facilities with non–genetics specialists providing genetic consultative services typically obtained the same or different types of consults from a non-VHA facility, via telegenetics, or from another VAMC.
Consults available at another VHA facility
Chiefs of 19 facilities indicated that genetic consults were available at another VAMC and not on-site, and at all but four of these facilities there were other arrangements for genetic consults with non-VHA facilities (13) or via telegenetics (2). One VAMC had cancer genetic consults on-site but also obtained these consults, as well as neurogenetic and reproductive genetic consults, from another VAMC.
The four VAMCs with a medical geneticist providing genetic consults on-site were located in four different VISNs, and 11 VAMCs reported obtaining genetic consultative services from another VAMC located in these four VISNs. Of the remaining VAMCs that obtained genetic consults from another VAMC, five were located within five different VISNs, each of which had a facility with a non–genetics specialist providing genetic consultative services, and four were located within three other VISNs; however, no chiefs reported availability of genetic consultative services at a facility in those VISNs.
Consults available via telegenetics
There were 13 VAMCs that obtained genetic consults via telegenetics. Two VAMCs obtained five or more types of genetic consultative services via telegenetics; however, both also obtained these consults on-site or at a non-VHA facility. One VAMC obtained cancer genetic and neurogenetic consults via telegenetics, yet both were also available at another VAMC. Ten facilities obtained only one type of consult via telegenetics (cancer genetic, 7; neurogenetic, 2; and “other” genetic, 1), and at six of these VAMCs these services were also available at a non-VHA facility (4), on-site (1), or at another VAMC (1).
Clinical genetic activities of non–genetics providers: the emerging model of genetic services delivery
Integration of genetic consultative services within primary care and other nongenetic specialties was assessed by asking the chiefs about activities relating to genetic risk assessment, testing, and management for a patient with signs and symptoms of a genetic condition (diagnostic evaluation); for a patient with a family history of a common disorder (predisposition evaluation); for selection of a genetic test to inform drug selection or dosing (pharmacogenetic testing); and for reproductive decision-making by a patient; Figure 3 ). The chiefs reported that their clinicians were involved in activities relating to a diagnostic genetic evaluation (averages ranging from 28.3 to 52.8%) and a predisposition evaluation (averages ranging from 21.4 to 43.4%) more often than in activities relating to carrier testing (averages ranging from 13.4 to 25.2%) or pharmacogenetic testing (averages ranging from 12.3 to 21.2%). Most chiefs expected their clinicians to recognize patients who may benefit from genetic testing (averages ranging from 21.2 to 52.8%), followed by ordering tests and recommending management based on genetic test results. Fewer expected their clinicians to discuss familial implications of genetic test results or to obtain informed consent for genetic tests. In general, across all the indications for testing, a greater percentage of neurology, oncology, and gastroenterology chiefs indicated that their clinicians were expected to perform the activities listed compared with the primary-care and cardiology chiefs.

Integration of genetic services within primary care and other non-genetic specialties was assessed by asking the chiefs about activities relating to genetic risk assessment, testing, and management for a patient with signs and symptoms of a genetic condition (diagnostic testing); for a patient with a family history of a common disorder (predisposition testing); for selection of a genetic test to inform drug selection or dosing (pharmacogenetic testing); and for reproductive decision-making by patients (carrier testing for a recessive disorder). N/A, not applicable.
Discussion
Both the traditional and emerging models of genetic consultative service delivery exist within the VHA health-care system. Cancer genetic and neurogenetic consults were most common, with reproductive, cardiovascular genetic, and pharmacogenetic consults available less often. The traditional model of multidisciplinary specialist clinics or coordinated services between geneticists and other specialists was most prevalent, although considerable variability in the arrangements for these services was described, which may translate to differences in the quality of care provided.
The most common arrangement for the traditional model was referral to non-VHA facilities—usually academic medical centers—and we observed a significant association between academic affiliation and ability to obtain a genetic consult. Academic medical centers are the typical setting for the traditional genetic service model;3,12 thus, medical geneticists and other specialists with genetics expertise are likely providing these services. Although the quality of genetic care provided at non-VHA facilities may be superb, off-site consultations threaten to compromise coordination of care, a measure of quality.22 Patients who switch providers will experience at least temporary discontinuity of care, which may adversely affect health outcomes and overall health-care costs.23,24,25
Only four VAMCs reported having services consistent with a core genetic center with a medical geneticist, often working together with genetic counselors and other specialists to provide consultative services for a breadth of genetic conditions, including cancer genetic, neurogenetic, cardiovascular genetic, and reproductive genetic consults. About 20% of VAMCs obtain genetic consultative services from another VAMC, and, given the network structure of the VHA, it appears likely that at least half of these VAMCs receive these services from one of the four VAMCs that have a medical geneticist on-site. Thus, although few in number, medical geneticists in the VHA can have a relatively large impact on delivery of genetic consultative services.
Telegenetics is another arrangement that enables expansion of the traditional model within the VHA. Telegenetics increases access to genetics professionals,9 and generally patients and providers are satisfied with telegenetics services.26,27 It is likely that the 13 VAMCs reporting the ability to obtain genetic consults via telegenetics had arrangements with the VHA national Genomic Medicine Service staffed by genetics counselors based at the Salt Lake City VAMC. However, our findings suggest that telegenetics alone may not suffice because most facilities with telegenetics also had other arrangements for the same types of consults (i.e., genetic consults provided by on-site clinicians or at another VAMC or a non-VHA facility). It may be that in-person consults are preferred for some patients or by certain referring clinicians, or telegenetic services may have limited capacity to accommodate all referrals. Clarifying these referral patterns is important to understanding the role of telegenetics for genetic consultation.
The emerging model of genetic consultative service delivery was also reported within the VHA, although there was considerable variability by specialty. Neurology, oncology, and gastroenterology chiefs consistently described higher expectations for their clinicians with respect to genetic risk assessment, testing, and management compared with cardiology and primary-care chiefs; this is probably due to increased knowledge and confidence regarding genetics among these specialists28,29 and increased awareness about genetics through marketing to specialists.30 Activities related to diagnostic and predisposition testing were more often performed by a non–genetic specialist than was pharmacogenetic testing or carrier screening. Tools supporting the emerging model that assist with genetic risk assessment and testing were rarely available within the EHR of VAMCs surveyed, although a recent study showed that a clinical reminder in the EHR can improve primary care clinicians’ recognition and appropriate referral of veterans at risk for hereditary cancer at the greater Los Angeles VAMC.4
Nongeneticists also provided genetic consults at VAMCs with on-site services available. However, our findings suggest that the types of consults were limited (e.g., neurologists only provided neurogenetic consults and oncologists only provided cancer genetic consults), and other arrangements for these consultative services, such as referral to another VAMC or a non-VHA facility, were typical, suggesting limited capacity of the nongeneticists to provide genetic consultative services even within their specialty. For example, a neurologist might have expertise with hereditary movement disorders but not hereditary neuropathies or hereditary forms of dementia; therefore, the latter would require referral elsewhere.
Clinicians with greater genetics knowledge have higher levels of confidence in assessing genetic risk and are more comfortable with identifying patients who may benefit from genetic services.31,32 In addition, awareness of available genetic services is associated with referral.31,33,34 Provider education on genetic topics was a key factor associated with ability to obtain a genetic consult within the VHA. Our results suggest that facilities that make consults available are more likely to offer provider education on genetic topics to ensure appropriate utilization of these services or clinicians educated about genetics may drive the availability of genetic consultative services at their facilities.
Several limitations of our study deserve mention. Although the VHA is the largest integrated health-care system in the United States,20 our findings may not be relevant to other settings, particularly solo or small group practices. The VHA, however, is an example of an existing accountable care organization that provides systems-based care using a patient-centered medical home model supported by a world-class EHR system. As such, what we have described for the VHA regarding delivery of genetic consultative services may become important as providers transition to practice within such organizations as promoted by the Patient Protection and Affordable Care Act.35 However, with our survey results, we can describe only the existing arrangements for genetic care models and make inferences about the quality of care provided.
In conclusion, both the traditional and emerging models of genetic consultative service delivery are available to Veterans receiving care at VAMCs. There is considerable variability in the organization of the traditional model, and the breadth of services available within the VHA depends on the type of clinician providing these services, with medical geneticists providing a greater breadth of services than nongeneticists. There is also variability within the emerging model, with specialists more likely to integrate genetics activities into their practice, particularly for diagnostic and predisposition genetic testing. This variability in both the traditional and emerging models could compromise the quality of the genetic care provided. Future studies are needed to more directly assess the quality of care delivered according to the organization of the service delivery for the available genetic care models in the VHA.
Disclosure
The authors declare no conflict of interest.
References
Manolio TA, Chisholm RL, Ozenberger B, et al. Implementing genomic medicine in the clinic: the future is here. Genet Med 2013;15:258–267.
Taylor MR, Edwards JG, Ku L . Lost in transition: challenges in the expanding field of adult genetics. Am J Med Genet C Semin Med Genet 2006;142C:294–303.
Battista RN, Blancquaert I, Laberge AM, van Schendel N, Leduc N . Genetics in health care: an overview of current and emerging models. Public Health Genomics 2012;15:34–45.
Scheuner MT, Hamilton AB, Peredo J, et al. A cancer genetics toolkit improves access to genetic services through documentation and use of the family history by primary-care clinicians. Genet Med 2014; 16:60–69.
Emery J, Morris H, Goodchild R, et al. The GRAIDS Trial: a cluster randomised controlled trial of computer decision support for the management of familial cancer risk in primary care. Br J Cancer 2007;97:486–493.
Wilson BJ, Torrance N, Mollison J, et al. Improving the referral process for familial breast cancer genetic counselling: findings of three randomised controlled trials of two interventions. Health Technol Assess 2005;9:iii–iv, 1.
Westwood G, Pickering RM, Latter S, Lucassen A, Little P, Karen Temple I . Feasibility and acceptability of providing nurse counsellor genetics clinics in primary care. J Adv Nurs 2006;53:591–604.
Zilliacus EM, Meiser B, Lobb EA, et al. Are videoconferenced consultations as effective as face-to-face consultations for hereditary breast and ovarian cancer genetic counseling? Genet Med 2011;13:933–941.
Hilgart JS, Hayward JA, Coles B, Iredale R . Telegenetics: a systematic review of telemedicine in genetics services. Genet Med 2012;14:765–776.
Platten U, Rantala J, Lindblom A, Brandberg Y, Lindgren G, Arver B . The use of telephone in genetic counseling versus in-person counseling: a randomized study on counselees’ outcome. Fam Cancer 2012;11:371–379.
Cohen SA, Marvin ML, Riley BD, Vig HS, Rousseau JA, Gustafson SL . Identification of genetic counseling service delivery models in practice: a report from the NSGC Service Delivery Model Task Force. J Genet Couns 2013;22:411–421.
Cooksey JA, Forte G, Benkendorf J, Blitzer MG . The state of the medical geneticist workforce: findings of the 2003 survey of American Board of Medical Genetics certified geneticists. Genet Med 2005;7:439–443.
Scheuner MT, Sieverding P, Shekelle PG . Delivery of genomic medicine for common chronic adult diseases: a systematic review. JAMA 2008;299:1320–1334.
Martin G, Currie G, Finn R . Bringing genetics into primary care: findings from a national evaluation of pilots in England. J Health Serv Res Policy 2009;14:204–211.
Burke W, Culver J, Pinsky L, et al. Genetic assessment of breast cancer risk in primary care practice. Am J Med Genet A 2009;149A:349–356.
Brierley KL, Campfield D, Ducaine W, et al. Errors in delivery of cancer genetics services: implications for practice. Conn Med 2010;74:413–423.
Dhar SU, Cooper HP, Wang T, et al. Significant differences among physician specialties in management recommendations of BRCA1 mutation carriers. Breast Cancer Res Treat 2011;129:221–227.
Plon SE, Cooper HP, Parks B, et al. Genetic testing and cancer risk management recommendations by physicians for at-risk relatives. Genet Med 2011;13:148–154.
Bensend TA, Veach PM, Niendorf KB . What’s the harm? Genetic counselor perceptions of adverse effects of genetics service provision by non-genetics professionals. J Genet Couns 2013; e-pub ahead of print 12 June 2013.
US Department of Veterans Affairs. Veterans Health Administration. http://www.va.gov/health/default.asp. Accessed 26 May 2013.
Hamilton AB, Oishi S, Yano EM, Gammage CE, Marshall NJ, Scheuner MT . Factors influencing organizational adoption and implementation of clinical genetic services. Genet Med 2013; e-pub ahead of print 15 August 2013.
Horak BJ, Welton W, Shortell S . Crossing the quality chasm: implications for health services administration education. J Health Adm Educ 2004;21:15–38.
Hamilton AB, Frayne SM, Cordasco KM, Washington DL . Factors related to attrition from VA healthcare use: findings from the National Survey of Women Veterans. J Gen Intern Med 2013;28(suppl 2):S510–S516.
Saultz JW, Lochner J . Interpersonal continuity of care and care outcomes: a critical review. Ann Fam Med 2005;3:159–166.
McLeod J, McMurray J, Walker JD, Heckman GA, Stolee P . Care transitions for older patients with musculoskeletal disorders: continuity from the providers’ perspective. Int J Integr Care 2011;11:e014.
Zilliacus EM, Meiser B, Lobb EA, Kirk J, Warwick L, Tucker K . Women’s experience of telehealth cancer genetic counseling. J Genet Couns 2010;19:463–472.
Zilliacus E, Meiser B, Lobb E, Dudding TE, Barlow-Stewart K, Tucker K . The virtual consultation: practitioners’ experiences of genetic counseling by videoconferencing in Australia. Telemed J E Health 2010;16:350–357.
Freedman AN, Wideroff L, Olson L, et al. US physicians’ attitudes toward genetic testing for cancer susceptibility. Am J Med Genet A 2003;120A:63–71.
Wideroff L, Vadaparampil ST, Greene MH, Taplin S, Olson L, Freedman AN . Hereditary breast/ovarian and colorectal cancer genetics knowledge in a national sample of US physicians. J Med Genet 2005;42:749–755.
Vadaparampil ST, Wideroff L, Olson L, Viswanath K, Freedman AN . Physician exposure to and attitudes toward advertisements for genetic tests for inherited cancer susceptibility. Am J Med Genet A 2005;135:41–46.
Carroll JC, Cappelli M, Miller F, et al. Genetic services for hereditary breast/ovarian and colorectal cancers - physicians’ awareness, use and satisfaction. Community Genet 2008;11:43–51.
Kelly KM, Love MM, Pearce KA, Porter K, Barron MA, Andrykowski M . Cancer risk assessment by rural and Appalachian family medicine physicians. J Rural Health 2009;25:372–377.
Wideroff L, Freedman AN, Olson L, et al. Physician use of genetic testing for cancer susceptibility: results of a national survey. Cancer Epidemiol Biomarkers Prev 2003;12:295–303.
Koil CE, Everett JN, Hoechstetter L, Ricer RE, Huelsman KM . Differences in physician referral practices and attitudes regarding hereditary breast cancer by clinical practice location. Genet Med 2003;5:364–369.
Correia EW . Accountable care organizations: the proposed regulations and the prospects for success. Am J Manag Care 2011;17:560–568.
Hilborne LH, Lubin IM, Scheuner MT . The beginning of the second decade of the era of patient safety: implications and roles for the clinical laboratory and laboratory professionals. Clin Chim Acta 2009;404(1):24–27.
Acknowledgements
This publication was supported by a Department of Veteran Affairs Health Services and Research & Development (HSR&D) Investigator Initiated Research award (IBD 09-101). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Veterans Health Administration. At the time of the study, A.B.H. was an investigator with the Implementation Research Institute, at the George Warren Brown School of Social Work, Washington University, St Louis, through an award from the National Institute of Mental Health (R25 MH080916-01A2) and VA HSR&D QUERI. E.M.Y.’s effort was supported by a VA HSR&D Senior Research Career Scientist Award (RCS 05-195). M.T.S. had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. We thank Brian Mittman for his input into study design; Barbara Simon and Alissa Simon for their input into survey design and development; and Zebada Brown, Cynthia Gammage, and Ismelda Canelo for their contributions to survey development, sample development, and data collection. Each provided these services in his or her role as an employee of the Department of Veteran Affairs Greater Los Angeles Healthcare System.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Scheuner, M., Marshall, N., Lanto, A. et al. Delivery of clinical genetic consultative services in the Veterans Health Administration. Genet Med 16, 609–619 (2014). https://doi.org/10.1038/gim.2013.202
Received:
Accepted:
Published:
Issue date:
DOI: https://doi.org/10.1038/gim.2013.202
Keywords
This article is cited by
-
Underutilization of Lynch Syndrome Screening at Two Large Veterans Affairs Medical Centers
Digestive Diseases and Sciences (2020)
-
General Practitioners’ knowledge and use of genetic counselling in managing patients with genetic cardiac disease in non-specialised settings
Journal of Community Genetics (2015)
