
Abstract
Tumor budding, a histological hallmark of epithelial–mesenchymal transition in colorectal cancer, is a parameter of tumor progression and according to the International Union Against Cancer/American Joint Committee on Cancer an ‘additional’ prognostic factor. The current definition of tumor budding is reserved for the invasive tumor front of colorectal cancer (so called peri-tumoral budding), but tumor buds can also be observed in small preoperative biopsy specimens. Whereas the prognostic value of peri-tumoral budding assessed in resection specimens has found wide acceptance, the value of budding in preoperative biopsies, which normally do not encompass the invasive tumor margin and hence can be called intra-tumoral budding, has not been systematically investigated yet. Therefore, the aim of this study is to assess the predictive value of intra-tumoral budding for lymph node and distant metastasis in preoperative biopsies. Preoperative biopsy samples and consecutive resection specimens from 72 patients with pathological information on TNM stage, vascular, lymphatic and perineural invasion, and tumor border configuration were used to evaluate intra-tumoral budding and peri-tumoral budding. Both parameters were scored semiquantitatively as ‘high’ (detectable at low power magnification × 2.5) and ‘low’ (occasional budding at intermediate magnification × 10, difficult to find or absent). In biopsy samples high intra-tumoral budding was observed in 12/72 patients (17%) and associated with high peri-tumoral budding in the corresponding resection specimens (P=0.008). Additionally, there was a correlation between high intra-tumoral budding and lymph node metastasis (P=0.034), distant metastasis (P=0.007) and higher tumor grade (P=0.025). Peri-tumoral budding was associated with higher N stage (P=0.004), vascular (P=0.046) and lymphatic invasion (P=0.019) as well as with an infiltrating tumor border (P<0.001), reflecting the predictive power of peri-tumoral budding for tumor progression. High intra-tumoral budding in preoperative biopsy samples of colorectal cancer patients predicts high peri-tumoral budding at the invasive margin and lymph node metastasis in the corresponding resection specimens as well as distant metastasis.
Similar content being viewed by others

Main
Colorectal cancer accounts for one of the most common malignancies in industrialized nations. Prognostication of newly diagnosed colorectal cancer predominantly relies on stage or anatomic extent of the disease based on the International Union Against Cancer (UICC-TNM)1 and the American Joint Committee on Cancer (AJCC)2 staging classifications.
Tumor infiltration depth, loco-regional lymph node involvement, venous and lymphatic invasion, tumor grade, tumor budding3 and tumor border configuration4 are histological features associated with worse patient outcome and can only be assessed in surgical tumor resection specimens.
Tumor budding, a histological hallmark of epithelial–mesenchymal transition, was comprehensively defined in 1987 by Jass et al4 and subsequently obtained wide acceptance among surgical pathologists. Peri-tumoral budding in colorectal cancer is associated with tumor progression and has been retained as an adverse feature of the primary tumor according to the World Health Organisation5 as well as an ‘additional’ prognostic factor according to the UICC/AJCC.6 Tumor budding is defined as isolated single cancer cells or clusters composed of fewer than five undifferentiated cancer cells at the invasive tumor margin (ie, peri-tumoral budding7).8 Tumor buds are believed to have the properties of tumor stem cells,9 including the potential for redifferentiation both locally and at the sites of metastasis.10 As the extent of tumor budding is an adverse feature of primary tumor, it is eligible to be reported in histopathology reports. Various elaborate systems for quantification of tumor budding in colorectal cancer have been described.3, 8, 11, 12, 13, 14, 15, 16, 17, 18, 19 All of these tumor budding grading systems share an association of high peri-tumoral budding with a worse outcome.
In daily practice, colorectal cancer is most often diagnosed on colonoscopy biopsy specimen obtained from superficial tumor areas by forceps biopsy technique, hence usually not encompassing the invasive tumor margin. These biopsies typically suffice to confirm the clinical suspicion of malignancy. It would be helpful to have a preoperative/pre-treatment biomarker to predict the stage of disease and particularly the lymph node status from the biopsy. Only sparse data exist on the role of tumor budding in biopsy specimens.11, 20 Morodomi et al11 described tumor buds in preoperative biopsy specimens in rectal cancer and hypothesized that tumor buds might have a predictive value for lymph node metastasis. Nevertheless, the value of tumor budding in preoperative biopsy specimens (intra-tumoral budding), located within the main tumor body away from the invasive border, has so far not been investigated systematically.
We have previously described that tumor buds are not only observed at the invasive border of a colorectal cancer, but that they may also be encountered within the tumor bulk. We thus implemented the terms of peri-tumoral budding for traditional tumor budding at the invasive tumor front and of intra-tumoral budding defined as budding located within the main tumor body, away from the invasive border. We further found that intra-tumoral budding is associated, in both DNA mismatch repair-proficient and -deficient cancers, with histological hallmarks of aggressive tumor behavior and worse tumor outcome.7
The aim of the present study was therefore to investigate the predictive value of intra-tumoral budding for lymph node and distant metastasis based on preoperative biopsy samples.
Patients and methods
Patient and Specimen Characteristics
One hundred and thirty-five patients with colorectal cancer treated at the Cantonal Hospital of Aarau, Switzerland between 1990 and 2008 were entered in the study. Patients with rectal tumors as well as patients who received neo-adjuvant therapy were excluded from the cohort. According to the clinical data files none of the patients was known to have a hereditary colorectal cancer syndrome (familial adenomatous polyposis or hereditary non-polyposis colorectal cancer). Permission to perform the study was granted by the Swiss federal health office; individual patient consent from surviving patients was obtained. For all 135 patients, histological slides of colorectal cancer resections were retrieved from the archives of the Department of Pathology, Cantonal Hospital Aarau, Switzerland. In addition, for 72 patients, the histological slides of preoperative biopsy specimens were also available. Histological work-up included TNM stage, tumor grade, presence of vascular, lymphoid, and perineural invasion. Tumor border configuration was assessed according to Jass et al.21 Patient and specimen characteristics are summarized in Table 1.
Assay Methods
Tissue samples were fixed in buffered formalin and paraffin embedded according to the standard protocols. Approximately 4-μm tissue slices were mounted on glass slides and were stained with H&E according to the standard protocols. All colorectal cancer-containing slides were reviewed for peri-tumoral budding quantification (OG). All biopsies had three levels separated by 20–50 μm. For resection specimen, all tumor-containing slides (average of five slides per tumor, range 2–14 slides per tumor; median 4 tissue slides) were reviewed.
Peri-tumoral budding was scored in analogy to the method proposed by Nakamura et al.22 Tumor budding at the invasive tumor front in the resection specimen, namely peri-tumoral budding, was designated as ‘high peri-tumoral budding’ when at least one focus of high tumor budding was detected at the entire invasive front at low magnification ( × 2.5 objective, 10 × 20 mm field of view eye piece, Zeiss Axioscope, Germany) and ‘low’ budding, ie, cases where tumor budding was not detected at low power magnification, with occasional budding at intermediate magnification × 10, difficult to find or absent. For intra-tumoral budding in the biopsy specimens, the same criteria were applied as for peri-tumoral budding, ie, being obvious at low power and being confirmed at intermediate power magnification. Tumor budding is illustrated in Figures 1 and 2. Thirty-nine resection specimens and 14 biopsy cases were evaluated by a second pathologist (SC) to assess the inter-observer agreement of the scoring method blinded to other data.

Peri-tumoral budding quantification on resection specimen with H&E staining in the top row and the extracted epithelial component from immunohistochemical staining for cytokeratin for the purpose of illustration in the bottom row. Invasive margin in analogy to Jass et al;4 (a) expanding border: tumor budding low; (b) expanding border: tumor budding high; (c) infiltrating border: tumor budding high.

Biopsy specimen with high intra-tumoral budding in H&E staining (top); extracted epithelial component from immunohistochemical staining for cytokeratin for the purpose of illustration (bottom).
Statistical Analysis
The associations between intra-tumoral budding or peri-tumoral budding and clinicopathological features were evaluated using the χ2 or Fisher's exact test where appropriate. Sensitivity, specificity, negative and positive predictive values were calculated. Adjustment for multiple testing was not performed.23 The inter-observer reproducibility of the scoring method was assessed using the kappa statistic. P-values <0.05 were considered statistically significant. All statistical analyses were carried out using SAS V9.1 (The SAS Institute, Cary, NC, USA).
Results
Frequency and Inter-Observer Agreement of Intra-Tumoral Budding and Peri-Tumoral Budding
In biopsy specimens, high intra-tumoral budding was seen in 17% (12/72) whereas no or sparse tumor budding, detectable only at high power magnification, was seen in 83% (60/72). Within the resection specimen of patients with an available preoperative biopsy, high peri-tumoral budding was seen in 57% (41/72) whereas low peri-tumoral budding was seen in 43% (31/72). A strong inter-observer concordance was detected for peri-tumoral budding scoring in resection specimen (k=0.68, percent-concordance 85%) and intra-tumoral budding scoring in biopsy samples (k=0.65, percent concordance 86%).
Association of Peri-Tumoral Budding, Intra-Tumoral Budding and the Histomorphological Parameters
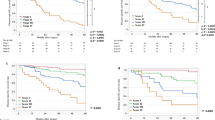
High peri-tumoral budding in resection specimen was associated with an infiltrating tumor border configuration (P<0.001), vascular (P=0.046) and lymphatic invasion (P=0.019), and lymph node metastasis (P=0.004). There was no association with pT classification (P=0.33) distant metastasis (P=0.49) and with tumor grade (P=0.78) (Table 2).
High intra-tumoral budding in biopsies was associated with lymph node (P=0.034) and distant metastasis at the time of diagnosis (P=0.007) and with a higher tumor grade (P=0.025). There was no association with pT stage (P=0.619), vascular (P=1.0) and lymphatic invasion (P=1.0), perineural invasion (P=0.114) and tumor border configuration (P=0.114; Table 3).
Association of Intra-Tumoral Budding (in Biopsies) for Lymph Node and Distant Metastasis
The specificity of intra-tumoral budding in biopsies for lymph node involvement and for distant metastasis was 94%, with positive predictive value for loco-regional lymph node involvement of 83% and 82%, respectively. This contrasts with lower sensitivities (24% for lymph node involvement and 33% for distant metastasis) as well as lower negative predictive value (48% for lymph node involvement and 65% for distant metastasis).
Concordance of Intra-Tumoral Budding in the Biopsy Samples and Peri-Tumoral Budding in the Corresponding Resection Specimens
The association of high intra-tumoral budding in biopsies with high peri-tumoral budding in the corresponding resection specimens was statistically highly significant (P=0.008), showing a sensitivity of 27% (11/41), a specificity of 97% (30/31), a positive predictive value of 91% (11/12) and a negative predictive value of 50% (30/60; Table 4).
Discussion
In this study the value of intra-tumoral budding was systematically assessed in preoperative biopsy samples of non-rectal colon cancers. On the basis of H&E-stained tissue slides from a total of 135 colorectal cancer resection specimens and 72 corresponding preoperative biopsy samples, we were able to assess intra-tumoral budding in biopsy specimens and correlate this feature with peri-tumoral budding in the resection specimens. High intra-tumoral budding in biopsies predicts lymph node and systemic metastasis. Additionally, the association of high intra-tumoral budding with high peri-tumoral budding was significant (P=0.008), showing a positive predictive value of 91%, zconfirming the strength of the assessment of intra-tumoral budding for predicting more aggressive tumor behavior in preoperative biopsy samples.
Peri-tumoral budding and intra-tumoral budding were scored in analogy to the method proposed by Nakamura et al.22 This method was selected for several reasons. First, in contrast to other methods such as those proposed by Ueno et al8, 24 or Wang et al,25 the method proposed by Nakamura is not limited to the size of the tumor or choice of microscope. Second, though it is a subjective assessment of tumor budding, it still shows a significant reproducibility between different observers. Third, it avoids the requirement of counting individual tumor buds, an exercise that can be challenging particularly in small or fragmented biopsy samples.
Our findings are comparable to previous studies that used more complex and elaborate tumor budding quantification systems.8, 11 The results of this study are also in agreement with previous work from our group using tissue microarrays, where we observed an association of intra-tumoral budding with advanced tumor stage and lymph node metastasis (even in the absence of peri-tumoral budding), vascular invasion, infiltrating tumor border configuration and shorter survival time.7
The identification of a histological hallmark for tumor aggressiveness in superficial tumor biopsy samples not encompassing the deep infiltration border of colorectal cancer raises a question regarding the future of tumor budding assessment in general. The survey of intra-tumoral budding may allow risk stratification for patients with worse prognosis already at the time point of the initial biopsy, and, if confirmed in prospective studies, intra-tumoral budding can be proposed as a histomorphological marker for daily practice that is applicable in preoperative biopsies and may assist the decision-making for a neo-adjuvant therapy approach.
References
Leslie Sobin MG, Wittekind C . TNM Classification of Malignant Tumors. 7th edn. Wiley Blackwell: Chichester, West Sussex, UK, 2009, pp 100–105.
Edge SB, Compton CC, Fritz AG, et al. (eds). AJCC Cancer Staging Manual 7th edn. Springer: New York, USA, 2009, pp 143–164.
Hase K, Shatney C, Johnson D, et al. Prognostic value of tumor ‘budding’ in patients with colorectal cancer. Dis Colon Rectum 1993;36:627–635.
Jass JR, Love SB, Northover JM . A new prognostic classification of rectal cancer. Lancet 1987;1:1303–1306.
Bosman FT, Carneiro F, Hruban RH, Theise ND, (eds). WHO Classification of Tumours of the Digestive System. IARC: Lyon, 2010, pp 146.
Compton CC, Gospodarowicz MK, O'Sullivan B, Sobin LH (eds). Prognostic Factors in Cancer 3rd edn. Wiley Liss: Hoboken, NJ, USA, 2006, pp 133–137.
Lugli A, Vlajnic T, Giger O, et al. Intratumoral budding as a potential parameter of tumor progression in mismatch repair-proficient and mismatch repair-deficient colorectal cancer patients. Hum Pathol 2011;42:1833–1840.
Ueno H, Murphy J, Jass JR, et al. Tumour ‘budding’ as an index to estimate the potential of aggressiveness in rectal cancer. Histopathology 2002;40:127–132.
O'Brien CA, Pollett A, Gallinger S, et al. A human colon cancer cell capable of initiating tumour growth in immunodeficient mice. Nature 2007;445:106–110.
Prall F . Tumour budding in colorectal carcinoma. Histopathology 2007;50:151–162.
Morodomi T, Isomoto H, Shirouzu K, et al. An index for estimating the probability of lymph node metastasis in rectal cancers. Lymph node metastasis and the histopathology of actively invasive regions of cancer. Cancer 1989;63:539–543.
Goldstein NS, Hart J . Histologic features associated with lymph node metastasis in stage T1 and superficial T2 rectal adenocarcinomas in abdominoperineal resection specimens. Identifying a subset of patients for whom treatment with adjuvant therapy or completion abdominoperineal resection should be considered after local excision. Am J Clin Pathol 1999;111:51–58.
Park KJ, Choi HJ, Roh MS, et al. Intensity of tumor budding and its prognostic implications in invasive colon carcinoma. Dis Colon Rectum 2005;48:1597–1602.
Masaki T, Sugiyama M, Matsuoka H, et al. Coexpression of matrilysin and laminin-5 gamma2 chain may contribute to tumor cell migration in colorectal carcinomas. Dig Dis Sci 2003;48:1262–1267.
Hori H, Fujimori T, Fujii S, et al. Evaluation of tumor cell dissociation as a predictive marker of lymph node metastasis in submucosal invasive colorectal carcinoma. Dis Colon Rectum 2005;48:938–945.
Horkko TT, Klintrup K, Makinen JM, et al. Budding invasive margin and prognosis in colorectal cancer--no direct association with beta-catenin expression. Eur J Cancer 2006;42:964–971.
Masaki T, Matsuoka H, Sugiyama M, et al. Tumor budding and evidence-based treatment of T2 rectal carcinomas. J Surg Oncol 2005;92:59–63.
Kanazawa H, Mitomi H, Nishiyama Y, et al. Tumour budding at invasive margins and outcome in colorectal cancer. Colorectal Dis 2008;10:41–47.
Yamauchi H, Togashi K, Kawamura YJ, et al. Pathological predictors for lymph node metastasis in T1 colorectal cancer. Surg Today 2008;38:905–910.
Stewart FW, Spies JW . Biopsy histology in the grading of rectal carcinoma. Am J Pathol 1929;5:109–169.
Jass JR, Atkin WS, Cuzick J, et al. The grading of rectal cancer: historical perspectives and a multivariate analysis of 447 cases. Histopathology 1986;10:437–459.
Nakamura T, Mitomi H, Kikuchi S, et al. Evaluation of the usefulness of tumor budding on the prediction of metastasis to the lung and liver after curative excision of colorectal cancer. Hepatogastroenterology 2005;52:1432–1435.
Perneger TV . What's wrong with Bonferroni adjustments. BMJ 1998;316:1236–1238.
Ueno H, Mochizuki H, Hashiguchi Y, et al. Risk factors for an adverse outcome in early invasive colorectal carcinoma. Gastroenterology 2004;127:385–394.
Wang LM, Kevans D, Mulcahy H, et al. Tumor budding is a strong and reproducible prognostic marker in T3N0 colorectal cancer. Am J Surg Pathol 2009;33:134–141.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Giger, O., Comtesse, S., Lugli, A. et al. Intra-tumoral budding in preoperative biopsy specimens predicts lymph node and distant metastasis in patients with colorectal cancer. Mod Pathol 25, 1048–1053 (2012). https://doi.org/10.1038/modpathol.2012.56
Received:
Revised:
Accepted:
Published:
Issue date:
DOI: https://doi.org/10.1038/modpathol.2012.56
Keywords
This article is cited by
-
Tumor Budding Assessment with Cytokeratin and Its Significance in Laryngeal Squamous Cell Carcinomas
Indian Journal of Otolaryngology and Head & Neck Surgery (2022)
-
Tumour budding in solid cancers
Nature Reviews Clinical Oncology (2021)
-
Tumor budding in colorectal cancer revisited: results of a multicenter interobserver study
Virchows Archiv (2015)
-
Prognostic value of poorly differentiated clusters in invasive breast cancer
World Journal of Surgical Oncology (2014)
-
CD8/CD45RO T-cell infiltration in endoscopic biopsies of colorectal cancer predicts nodal metastasis and survival
Journal of Translational Medicine (2014)
