
Abstract
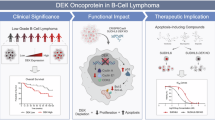
PELI is a family of E3 ubiquitin ligases that regulate protein activity through a post-translational modification, ubiquitination. While PELI1 has been found to play a pivotal role in inflammatory processes through the activation of Toll-like receptor signaling and the NF-kB pathway, the role of PELI1 in oncogenesis has not been the subject of much investigation. We aimed to explore PELI1 expression in various malignant lymphomas and identify clinicopathologic significance. Immunohistochemistry for PELI1 was performed on a total of 502 cases, including 406 B-cell, 76 T or NK-cell, and 20 Hodgkin lymphomas. High expression of PELI1 was found in high-grade B-cell lymphoma cases such as diffuse large B-cell lymphoma, Burkitt lymphoma, and plasmablastic lymphoma, whereas low-grade B-cell lymphoma, T/NK-cell lymphoma, and Hodgkin lymphoma cases showed very low levels of expression. In vitro cell line studies, the results of western blot, and RT-PCR were concordant with those of the immunohistochemical results; RL7, Pfeiffer, SUDHL-2, DOHH2, and Ramos cell lines showed high levels of PELI1 protein and mRNA expression. In 182 diffuse large B-cell lymphoma, PELI1 expression was positively correlated with the expression of MYC, BCL6, BCL2, and MUM1 (Spearman’s ρ=0.427, 0.507, 0.246, and 0.137, respectively; P<0.001, <0.001, 0.001, and 0.066, respectively). In diffuse large B-cell lymphoma, high expression of PELI1 was associated with frequent bone marrow involvement (P=0.013) and shorter relapse-free survival (P=0.002). Our results suggest that PELI1 might participate in B-cell maturation or oncogenic activation of aggressive B-cell lymphomas, both during and after germinal center stages.
Similar content being viewed by others


Main
PELI1 is a small regulatory molecule that functions as an E3 ubiquitin ligase and tags proteins that are subsequently activated, located, or degraded by the proteasome. Like other ubiquitin ligases, PELI1 takes part in intracellular enzymatic post-translational modification in animal cells.1 Among the three homologous forms of PELIs, PELI1 is known to play a pivotal role in inflammatory and autoimmune processes by mediating toll-like receptor signaling and regulating the transcription activities of nuclear factor kappa light chain enhancer of activated B-cells (NF-kB).1, 2, 3 In addition, there is growing evidence that PELI1 is linked to proliferation and activation of B and T lymphocytes based on some in vitro experiments.4, 5 However, the role of PELI1 in oncogenesis has not been fully elucidated.
Recently, Park et al4 found that PELI1 induced B-cell lymphomas in transgenic mice through the promotion of BCL6 stabilization.4 It is well known that lymphocytic development is a highly dynamic, genetically unstable process and that the biology of the lymphoma depends on the level of cell maturation at the corresponding stages of lymphocytic development. Although little is known about PELI in lymphomagenesis, apart from BCL6, we suspect PELI1 plays a cooperative role with other B-cell signaling molecules or other oncogenes in certain stage of lymphomagenesis.
As reported in this manuscript, we investigated PELI1 expression in 17 types of malignant lymphoma of B- or T-cell lineages and analyzed its clinical significance and correlation with MYC, BCL6, BCL2, and MUM1 expression in diffuse large B-cell lymphoma. We found that PELI1 was highly expressed with a strong correlation with MYC in aggressive B-cell lymphomas in addition to diffuse large B-cell lymphoma and that high levels of these proteins predict shorter relapse-free survival in diffuse large B-cell lymphoma.
Materials and methods
Patients
Samples were obtained from 495 patients diagnosed with malignant lymphoma at three university hospitals in Korea from 2005 to 2012. Diagnosis was confirmed by two experienced hematopathologists (JYC and JEK), according to the 2008 WHO classification.6 Clinical data were obtained from electronic medical records. This study was approved by the Institutional Review Board of Seoul National University Boramae Hospital (IRB No. 16-2013-38) on April 2013.
Immunohistochemistry
Tissue microarray blocks were constructed with a pair of 2–5 mm wide core tissues from the most representative areas of paraffin-embedded blocks, and immunohistochemistry was performed using tissue microarray blocks. Immunohistochemistry for PELI1 (F-7; Santa Cruz Biotechnology, Santa Cruz, CA, USA; 1:50) was conducted on all 502 cases. Additional immunohistochemistry was performed in diffuse large B-cell lymphoma cases (N=182) with the following antibodies: MYC (Y69; Epitomics, Burlingame, CA, USA), BCL6 (LN22; Novocastra, Newcastle upon Tyne, UK), BCL2 (M0887; Dako, Carpinteria, CA, USA), CD3 (M7254; Dako), CD5 (M7194; Dako), CD10 (PA0270; Novocastra), MUM1 (M7259; Dako), and Ki-67 (MIB1; Dako). Epstein-Barr virus (EBV) in situ hybridization (ISH) was performed in diffuse large B-cell lymphoma, Hodgkin lymphoma and T- or NK-cell lymphomas using an EBV-encoded RNA (EBER) probe (INFORM EBER Probe; Ventana Medical Systems, Tucson, AZ, USA). Single immunohistochemistry for PELI1 and double immunohistochemistry for PELI1 and PAX5/CD3 were performed using the BOND-MAX autoimmunostainer (Leica Biosystems, Melbourne, Australia). Other immunohistochemistry and EBV ISH were conducted with the Bench Mark autoimmunostainer (Ventana Medical Systems) using validated protocols.
Evaluation of immunohistochemistry was quantitatively or semiquantitatively graded for each antibody. Nuclear proteins (MYC, BCL6, MUM1, and Ki-67) were measured as a percentage of positive tumor cells using automated image analysis software with a slide scanner (Aperio, Vista, CA, USA). The positivity of cytoplasmic or membranous staining with/without nuclear staining (PELI1, BCL2, and CD10) was manually calculated using H scores with 5-tiered intensity scores (0, absent; 0.1, faint; 1, weak; 2, moderate; 3, strong) multiplied by the frequency scores (0, <1%; 0.1, 1–10%; 0.5, 10–50%; 1, 50–100%) of positive tumor cells.
Western Blot Analysis for PELI1
Expression of PELI1 protein was investigated by western blot with the same antibody as immunohistochemistry in 14 lymphoma cell lines. Cell lines consisted of Ramos, RL7 (Burkitt lymphoma), Pfeiffer, DOHH2 (diffuse large B-cell lymphoma, germinal center B-cell), SUDHL-2 (diffuse large B-cell lymphoma, non-germinal center B-cell), SP53, REC (mantle cell lymphoma), IM-9 (multiple myeloma), Jurkat (T-cell lymphoma), Karpas299, SUDHL-1 (anaplastic large cell lymphoma), NK-YS (NK/T-cell lymphoma), L428, and KMH2 (Hodgkin lymphoma). Ramos, IM-9, and Jurkat cell lines were purchased from the Korean cell line bank (Seoul, Korea). DOHH2, SP53, Karpas299, L428, and KMH2 cell lines were kindly provided by Dr Francisco Vega-Vazquez (University of Miami, Coral Gables, FL, USA). REC and NK-YS were gifts from Dr Yoon Kyung Jeon (Seoul National University Hospital, Seoul, Korea). The other cell lines were obtained from American Type Culture Collection (ATCC, Manassas, VA, USA).
Western blot was performed as previously described.7 Briefly, cells in log-phase growth were prepared, and 20 μg of protein resolved in 10% sodium dodecyl sulfate-polyacrylamide gel electrophoresis was transferred to polyvinylidene difluoride membranes. The blot was incubated with primary antibodies against PELI1 (1:1000) in TBST (TBS containing 0.05% Tween 20) with 5% skim milk at 4 °C overnight. The membranes were subsequently incubated at room temperature for 1 h with horseradish peroxidase conjugated anti-mouse IgG (Thermo Fisher Scientific, Fremont, CA, USA).
Real-Time Polymerase Chain Reaction (PCR) for PELI1
PELI1 mRNA levels were detected with real-time PCR in the same series of lymphoma cell lines. Total RNA was isolated using a TRIzol reagent (Thermo), and cDNAs were synthesized using the Maxima First Strand cDNA Synthesis Kit (Thermo). Real-time PCR was performed with LightCycler 480 SYBR I Master (Roche, Basel, Switzerland) using primers specific for the PELI1 (199 bp; forward, 5′-TGTAGTAACTGACACGGTTCCT-3′ and reverse, 5′-TCCATCTGATGTCTTCCATTTGG-3′) and GAPDH (452 bp; forward, 5′-ACCACAGTCCATGCCATCAC-3′ and reverse, 5′-TCCACCACCCTGTTGCTGTA-3′) genes.
Fluorescence In Situ Hybridization (FISH) for IgH/MYC Translocation and MYC Amplification
FISH was performed on tissue microarray block sections and whole slides according to the manufacturer’s protocols. A Vysis LSI MYC dual-color, break-apart rearrangement probe (Abbott Molecular, Abbott Park, IL, USA) was used to detect MYC translocation, and a Vysis MYC 8q24 probe mixed with a CEP8 probe (Abbott) was used for amplification. At least 100 cells from each case were assessed for split signals to identify MYC translocation and MYC gene copy numbers.
Statistical Analysis
Spearman’s ρ was used to assess the correlation between protein expression levels. Mann–Whitney U-test and Fisher's exact test were performed to compare immunohistochemistry results according to the clinicopathologic variants. Overall survival was calculated from the date of diagnosis to the date of death. Relapse-free survival was calculated from the date of diagnosis to the date of relapse after complete or partial remission or death. Progression-free survival was calculated from the date of diagnosis to the date of disease progression or death. Univariable Kaplan–Meier survival functions with log rank tests were estimated to compare binary groups based on protein expression levels. Multivariable survival analysis using the Cox multiple regression model was performed to identify independent prognostic markers. The results were considered statistically significant with a two-tailed P-value of <0.05. All data were analyzed with SPSS software, version 22.0 (SPSS Inc., IBM, NY, USA).
Results
Expression of PELI1 in Reactive Lymphoid Tissue
The cellular localization of PELI1 staining was nuclear and/or diffuse cytoplasmic pattern without membranous or Golgi pattern. In reactive lymph nodes and spleen, PELI1 was selectively positive in lymphocytes of the germinal centers and of the marginal zone and negative in the mantle zone. In the paracortical area in lymph nodes, PELI1 was mostly negative in small lymphocytes but weakly positive in a few stromal cells, such as endothelial cells. Double immunohistochemistry with PELI1 and PAX5 or CD3 revealed that PELI-positive cells were mainly PAX5-positive B-cells but not CD3-positive T-cells. In thymus, PELI1 was negative in T lymphoblasts (Figure 1).

Immunohistochemical expression of PELI1 in reactive lymphoid tissue. (a, b) PELI1 expression was localized in germinal center, but rarely found outside follicles. (c) In double immunohistochemical staining with PELI1 (brown) and PAX5 (red), PELI1-positive cells were revealed as PAX5-positive B-cells in germinal centers. (d) In double immunohistochemical staining with PELI1 (brown) and CD3 (red), PELI1-positive cells were rarely overlapped with CD3-positive T-cells. (e) In thymus, T lymphoblast did not show PELI1 expression. (f) In spleen, germinal center cells and the marginal zone B-cells were positive for PELI1, but the mantle zone B-cells were negative for PELI1.
Expression of PELI1 in Various Malignant Lymphomas
In tissues, PELI1 expression varied according to the type of lymphoma. Overall, PELI1 expression was higher in B-cell type lymphomas (mean±s.d., 0.92±0.85) than in T- or NK-cell lymphomas (0.25±0.39) or Hodgkin lymphoma (0.06±0.06) (P<0.001). Among all types of lymphomas, diffuse large B-cell lymphoma, Burkitt lymphoma, and plasmablastic lymphoma showed the highest levels of PELI1 expression. Other B-cell lymphomas, including follicular lymphoma, mantle cell lymphoma, small lymphocytic lymphoma, lymphoplasmacytic lymphoma, and nodal/extranodal marginal zone lymphoma, showed low levels of PELI1 expression. Among 33 follicular lymphomas in our study, 20 cases (61%) were low grade (grade 1 or 2) and 13 cases (39%) were high grade (grade 3). The levels of PELI1 expression were not significantly different according to histologic grade, although high-grade lesions revealed slightly higher expression (mean H-score ±s.d.: 0.51±0.42 in high grade vs 0.40±0.28 in low grade; P-value=0.36).
Immature T- or B-cell lymphomas also had low levels of PELI1 expression. T- or NK-cell lymphomas and all Hodgkin lymphoma showed very low levels of PELI1 protein. Anaplastic large cell lymphomas included 22 ALK negative and 14 ALK positive cases. Among 20 cases of Hodgkin lymphoma, 2 cases were nodular lymphocyte predominant type and 18 cases were classical type including 9 nodular sclerosis, 7 mixed cellularity, and 1 lymphocyte-depleted type (Figures 2,3, and Table 1).

Representative figures of PELI1 expression by immunohistochemistry in various types of malignant lymphomas. (a) Diffuse large B-cell lymphoma, (b) Burkitt lymphoma, and (c) plasmablastic lymphoma showed the highest levels of PELI1 expression. Other low-grade B-cell lymphoma, including (d) follicular lymphoma, (e) mantle cell lymphoma, and (f) small lymphocytic lymphoma showed very low level of PELI1 expression. T/NK-cell lymphomas such as (g) extranodal NK/T-cell lymphoma and (h) angioimmunoblastic lymphoma or (i) Hodgkin lymphoma showed negative or very low level of PELI1 expression.

Immunohistochemical expression of PELI1 in various types of malignant lymphomas. PELI1 expression was variable according to types and cell lineages of malignant lymphomas. Some high-grade B-cell lymphomas showed high levels of PELI1 expression whereas low-grade B-cell lymphomas, T/NK-cell lymphomas, and Hodgkin lymphomas showed relatively low level of expression. PELI1 expression was semiquantatively measured using H-score, which was calculated as intensity scores (0, 0.1, 1, 2, 3) multiplied by frequency scores (0, 0.1, 0.5, 1) of positive tumor cells. (A circle or an asterisk is representative for an outlier greater than 1.5 or 3 times the interquartile ranges, respectively; AITL, angioimmunoblastic T-cell lymphoma; ALCL, anaplastic large cell lymphoma; B-LBL, B-lymphoblastic lymphoma; BL, Burkitt lymphoma; DLBCL, diffuse large B-cell lymphoma; EMZL, extranodal marginal zone lymphoma of MALT; FL, follicular lymphoma; HL, Hodgkin lymphoma; LPL, lymphoplasmacytic lymphoma; MCL, mantle cell lymphoma; MM, multiple myeloma; NKTL, extranodal NK/T-cell lymphoma; NMZL, nodal marginal zone lymphoma; PBL, plasmablastic lymphoma; PTCL, peripheral T-cell lymphoma; SLL/CLL; small cell lymphoma/chronic lymphocytic leukemia; T-LBL, T-lymphoblastic lymphoma.)
These immunohistochemistry results were concordant with the results of western blot (Figure 4a) and real-time PCR (Figure 4b). B-cell lymphoma cell lines showed high levels of PELI1 mRNA expression. Burkitt lymphoma (Ramos, RL7), diffuse large B-cell lymphoma (Pfeiffer, SUDHL-2 and DOHH2), and multiple myeloma cells (IM-9) showed very high levels of PELI1 protein and mRNA. Mantle cell lymphoma cell lines (Sp53 and REC) showed intermediate levels of PELI1 protein and mRNA. In contrast, lymphoma cell lines of T or NK lineages (Jurkat, Karpas299, SUDHL-1, NK-YS) and Hodgkin lymphoma cell lines (L428 and KMH2) showed very low levels of PELI1 protein and mRNA.

Expressions of PELI1 protein and mRNA in cell lines of various malignant lymphomas. PELI1 expression levels by (a) western blot were concordant with PELI1 mRNA expression by (b) real-time PCR. Both PELI1 protein and mRNA expression levels were high in high-grade B-cell lymphoma cell lines but low in T/NK-cell lymphoma and Hodgkin lymphoma cell lines. (cell lines: Ramos: Burkitt lymphoma; RL7: high-grade B-cell lymphoma; Pfeiffer, SUDHL-2, DOHH2: diffuse large B-cell lymphoma; Sp53, REC: mantle cell lymphoma; IM-9: multiple myeloma; Jurkat: T-cell lymphoma; Karpas299, SUDHL-1: anaplastic large cell lymphoma; NK-YS: NK/T-cell lymphoma; L428, KMH2: Hodgkin lymphoma).
Clinicopathologic Correlation of PELI1 in Diffuse Large B-cell Lymphoma Patients
To assess the clinical significance of expression of PELI1 protein, we analyzed the clinicopathologic correlation in diffuse large B-cell lymphoma cases, which showed distinctively high PELI1 levels among the various lymphoma types. Detailed profiles of 182 diffuse large B-cell lymphoma patients are presented in Table 2. The median follow-up of the patients was 42.6 months (range 0–261); remission, either complete or partial, was achieved in 133/145 patients (92%) with 18 cases (12%) resulting in death and 42 (32%) recurrent cases.
Patients with higher PELI1 expression levels showed frequent bone marrow involvement (P=0.013) in diffuse large B-cell lymphoma. Otherwise, there was no significant association between PELI1 expression and other clinical parameters, including age, International Prognostic Index score, Ann Arbor stage, and ECOG performance status. Additionally, PELI1 expression was not significantly associated with Hans classification, CD5 positivity, or EBV positivity.
Correlation of PELI1 and Other Proteins in Diffuse Large B-cell Lymphoma
Additional immunohistochemistry for MYC, BCL6, BCL2, MUM1, CD10, CD5, CyclinD1, and Ki-67 was performed in diffuse large B-cell lymphoma patients. PELI1 expression was significantly correlated with the expression of MYC, BCL6, and BCL2 (r=0.427, 0.507, 0.246, respectively, all P≤0.001) and also marginally correlated with MUM1 expression (r=0.137, P=0.066). The proliferation index of Ki-67 was not correlated with PELI1 expression (Table 3).
FISH for MYC Rearrangement and MYC Amplification in Diffuse Large B-cell Lymphoma and Plasmablastic Lymphoma Patients
Rearrangement of MYC was tested by FISH in 89 cases of diffuse large B-cell lymphoma and 6 plasmablastic lymphoma cases; 3 of 89 diffuse large B-cell lymphomas and 1 of 6 plasmablastic lymphomas showed MYC rearrangement (Figure 5). Copy number analysis of MYC was also tested by FISH in 81 diffuse large B-cell lymphoma and 6 plasmablastic lymphoma; MYC amplification (MYC gene copy number>4) was found in 4 of 81 diffuse large B-cell lymphoma but in none of 6 plasmablastic lymphoma. Low polysomy or trisomy of the MYC gene (MYC gene copy number <4) was also detected in two and one cases of diffuse large B-cell lymphoma, respectively. There was no case harboring concurrent MYC rearrangement and MYC copy number alteration.

Fluorescence in situ hybridization of MYC gene alteration in diffuse large B-cell lymphoma. (a) Splitted red and green signals were shown in MYC gene translocation cases by break-apart probe. (b) Amplified red (MYC) signals compared with green (CEP8) signals were shown in MYC gene amplification cases.
In diffuse large B-cell lymphoma and plasmablastic lymphoma, the expression levels of MYC were similar between the cases with MYC translocation or amplification and the cases without MYC gene alteration. Tendency of positive correlation between expression of PELI1 and MYC was sustained not only in the diffuse large B-cell lymphoma cases with MYC gene alteration but also in the diffuse large B-cell lymphoma without MYC gene alteration (r=0.253, P=0.056 vs r=0.268, P=0.052), although statistical significance was lowered due to decreasing sample size.
Prognostic Significance of PELI1 and MYC in Diffuse Large B-cell Lymphoma Patients
A receiver operating characteristic curve was drawn to identify the most sensitive and specific cutoff points for patient survival based on the expression of PELI1 and MYC protein. Cases were dichotomized into two groups based on the expression levels of each protein as follows: ‘PELI1 high’ (>2 by H-score) and ‘PELI1 low’ (≤2 by H-score); and 'MYC high' (>20%) and ‘MYC low’ (≤20%).
Following univariable analysis, we found patients with high PELI1 expression levels had shorter relapse-free survival but not overall survival when compared with low PELI1 expression levels (P=0.002). Additionally, patients having high MYC expressing tumors had shorter overall survival and relapse-free survival than those with low MYC expressing tumors (P=0.003, P=0.036, respectively) (Figure 6). The cases with MYC translocation or MYC amplification showed no differences in overall survival or relapse-free survival.

Survival analyses of diffuse large B-cell lymphoma patients with PELI1 and MYC expression levels. (a, b) Patients with high PELI1 expression (≥2, H-score) showed significantly worse prognosis in relapse-free survival, but not in overall survival. (c, d) Patients with high MYC expression (≥20%) showed worse prognosis in both overall survival and relapse-free survival.
Multivariable Cox regression analysis was performed with integration of protein expression along with several parameters including patients’ age, Ann Arbor stage, performance status, therapeutic modalities, and transformed disease that were significant prognostic indicators or possible confounding factors in univariable survival analysis. Expression of PELI1 or MYC was analyzed in separate sets because of the strong correlation between them. As a result, overexpression of PELI1 and MYC was not independent prognostic factors of patients’ overall survival and relapse-free survival (Table 4).
Discussion
This study revealed that PELI1 was frequently expressed at high levels in high-grade B-cell lymphomas, including diffuse large B-cell lymphoma, and high levels of PELI1 protein, along with MYC expression, were a negative predictor of patients’ outcome. A previous study suggested that PELI1 induces constitutive activation of B-cell signal transduction through upregulation of BCL6,4 and the present study provides an additional clue as to the pivotal role of PELI1, especially in high-grade B-cell lymphomas.
Our working hypothesis was that PELI1 works differently in the normal development and neoplastic processes of B-cells. In reactive lymph node, PELI1 protein expression was restricted in the germinal center B-cells, confirming the close relationship of PELI1 with BCL6. However, in the B-cell lymphomas, PELI1 expression was not restricted in germial center B-cell type lymphomas and was not present in all germinal center B-cell type lymphomas. In our series, Burkitt lymphoma, one of the germinal center B-cell type lymphomas, revealed very high levels of PELI1 expression, whereas follicular lymphoma, another germinal center B-cell type lymphoma, displayed relatively low levels of PELI1. Additionally, PELI1 expression was not significantly different between germinal center B-cell type and non-germinal center B-cell type diffuse large B-cell lymphomas based on the Hans classifier.8 These findings indicate that not all lymphomas of germinal center B-cell origin resulted in PELI1 gene activation.
B-cell lymphomas originated from pre-germinal center stages, such as small lymphocytic lymphoma and mantle cell lymphoma, showed extremely low PELI1 expression levels. In post-germinal center stage lymphoma, marginal zone B-cell lymphoma and multiple myeloma showed low level of PELI1 expression in contrast to plasmablastic lymphoma. Plasmablastic lymphoma is known to have frequent MYC deregulation and showed very high levels of PELI1. Taken together, these findings suggest that activation of PELI1 starts in the germinal centers but can persist through post-germinal center stages and that the programmed tuning of PELI1 functions might be disrupted with the cooperation of other oncogenic pathways, such as pathways linked to MYC or B-cell signaling factors, including BCL6.
In T- or NK-cell lymphomas, expression of PELI1 protein or mRNA was uniformly low, even in angioimmunoblastic T-cell lymphoma, a lymphoma originated from germinal center-T cells often expressing BCL6. In a previous report, PELI1 mRNA expression was abundant in splenic T-cells of mice.5 Additionally PELI1 was shown to negatively regulate T-cell activation and maintain T-cell tolerance, which is the inverse of T-cell function activating B-cells.5 Therefore, it is possible that PELI1 targets different signaling factors according to the type of immune cell and that BCL6 is not involved in the activity of PELI1 in T-cell lymphomas.
In this manuscript, we showed a significant correlation between PELI1 and MYC levels and other oncogenic proteins that are important in developing malignant lymphomas. Stabilization of BCL6 by PELI1 was already demonstrated in a previous study.4 However, the relationship of PELI1 with MYC or BCL2 has not been elucidated. It is well known that PELI exerts its immunoregulatory functions via ubiquitination of some important transcription factors and that the MYC gene could be one substrate of PELI1. Because MYC is a protein with a short half-life and with several binding sites for ubiquitin ligases, the stability of MYC can be partly controlled by the ubiquitination system.9, 10 In the development of Burkitt lymphoma, constant upregulation of MYC is driven by the strong transcriptional control of the immunoglobulin heavy chain, and additional mutation of the ubiquitin system binding sites contributes to the stability of MYC via decreased proteasomal degradation.11 Therefore, similar to the relationship between PELI1 and BCL6, deregulation of PELI1 might induce prolongation of MYC activity by preventing MYC degradation. However, MYC stabilization by PELI1 ubiquitination was not proven directly, and further study will be needed to verify this hypothesis.
When examining the correlation between PELI1 and MYC, one needs to keep in mind that a reverse mechanism of action is also possible, that is, activation of MYC could bring about PELI1 overexpression. As MYC is known as a driver oncogene, MYC seems to be more likely to cause PELI1 overexpression rather than the reverse. However, in our study, positive correlation between PELI1 and MYC was maintained in the diffuse large B-cell lymphoma cases without MYC translocation or amplification, where the source of MYC overexpression is not obvious. Alternative or indirect mechanisms of MYC deregulation might work in those cases, and PELI1 ubiquitination is a possible candidate controlling MYC activity.
Our study also studied the correlation between PELI1 and BCL2. BCL2 works as an antiapoptotic protein and is thus considered an oncogene in B-cell lymphoma. Recently, BCL2 overexpression with MYC was found to contribute to the poor prognosis in diffuse large B-cell lymphoma patients.12, 13 However, little is known about BCL2 stabilization by the ubiquitination system. Although nothing can be confirmed from this cross-sectional aspect of PELI1 and BCL2 correlation, we suggest that MYC alteration could be a causal factor of BCL2 deregulation. One piece of support for this suggestion is based on the MYC-induced repression of some microRNAs targeting BCL2, such as miR15a/16-1, which results in increased BCL2 expression.14
Additionally, a tendency of correlation between PELI1 and MUM1 was noted in this study. A previous study also confirmed MUM1 expression in a small group of lymphomas in PELI1 transgenic mice,4 but no further investigations were published. MUM1 is a transcription factor that is necessary for development and activation of B lymphocytes. In reactive lymphoid tissue, MUM1 expression is mutually exclusive with BCL6 expression and appears at the later stages of germinal center in B-cell differentiation, after diminution of CD10 and BCL6 expression, and at the post-germinal center lymphocytes and plasma cells. In physiologic conditions, MUM1 with BLIMP1 represses both BCL6 and MYC and results in B-cell differentiation into plasma cells. However, in MYC-deregulated tumors, such as plasmablastic lymphoma, MYC is thought to overcome the repressive activity of MUM1.14 This phenomenon supports a mechanism for the positive interactions of PELI1–MYC–MUM1.
The regulatory mechanism of PELI1 is currently poorly understood. PELI1 E3 ligase activity and stability can be modified by phosphorylation and autoubiquitination by IRAK or sumoylation.2 In a previous study, miR21 was reported to target PELI1 and regulate cell proliferation in liver cell generation via NF-kB signaling.15 Further studies of PELI1 will be needed to fully elucidate the genetic and epigenetic aspects.
Whether PELI1 deregulation is an initiative event or a concomitant incident was not proven in this study; however, high expression of PELI1 protein showed worse relapse-free survival in diffuse large B-cell lymphoma patients. Further studies with a larger, uniformly treated group of diffuse large B-cell lymphoma cases will be needed to clarify prognostic significance of PELI1.
In conclusion, deregulation of PELI1 may be associated with the pathogenesis of a subset of aggressive B-cell lymphomas. A correlation of PELI1 expression with other transcription factors such as MYC, BCL6, BCL2, or MUM1 supported the notion that PELI1 is involved in germinal center and post-germinal center stage B-cell maturation and lymphomagenesis.
References
Jin W, Chang M, Sun SC . Peli: a family of signal-responsive E3 ubiquitin ligases mediating TLR signaling and T-cell tolerance. Cell Mol Immunol 2012;9:113–122.
Humphries F, Moynagh PN . Molecular and physiological roles of Pellino E3 ubiquitin ligases in immunity. Immunol Rev 2015;266:93–108.
Medvedev AE, Murphy M, Zhou H et al, E3 ubiquitin ligases Pellinos as regulators of pattern recognition receptor signaling and immune responses. Immunol Rev 2015;266:109–122.
Park HY, Go H, Song HR et al, Pellino 1 promotes lymphomagenesis by deregulating BCL6 polyubiquitination. J Clin Invest 2014;124:4976–4988.
Chang M, Jin W, Chang JH et al, The ubiquitin ligase Peli1 negatively regulates T cell activation and prevents autoimmunity. Nat Immunol 2011;12:1002–1009.
Steven HS, Elias C, Nancy LH et al, (eds). WHO classification of Tumours of Haematopoietic and Lymphoid Tissues, 4th edn. IARC: Lyon, 2008.
Choe JY, Yun JY, Jeon YK et al, Sonic hedgehog signalling proteins are frequently expressed in retinoblastoma and are associated with aggressive clinicopathological features. J Clin Pathol 2015;68:6–11.
Hans CP, Weisenburger DD, Greiner TC et al, Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood 2004;103:275–282.
Tu WB, Helander S, Pilstal R et al, Myc and its interactors take shape. Biochim Biophys Acta 2015;1849:469–483.
Sun XX, He X, Yin L et al, The nucleolar ubiquitin-specific protease USP36 deubiquitinates and stabilizes c-Myc. Proc Natl Acad Sci USA 2015;112:3734–3739.
Bahram F, von der Lehr N, Cetinkaya C et al, c-Myc hot spot mutations in lymphomas result in inefficient ubiquitination and decreased proteasome-mediated turnover. Blood 2000;95:2104–2110.
Johnson NA, Slack GW, Savage KJ et al, Concurrent expression of MYC and BCL2 in diffuse large B-cell lymphoma treated with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone. J Clin Oncol 2012;30:3452–3459.
Hu S, Xu-Monette ZY, Tzankov A et al, MYC/BCL2 protein coexpression contributes to the inferior survival of activated B-cell subtype of diffuse large B-cell lymphoma and demonstrates high-risk gene expression signatures: a report from The International DLBCL Rituximab-CHOP Consortium Program. Blood 2013;121:4021–4031; quiz 250.
Ott G, Rosenwald A, Campo E . Understanding MYC-driven aggressive B-cell lymphomas: pathogenesis and classification. Blood 2013;122:3884–3891.
Marquez RT, Wendlandt E, Galle CS et al, MicroRNA-21 is upregulated during the proliferative phase of liver regeneration, targets Pellino-1, and inhibits NF-kappaB signaling. Am J Physiol Gastrointest Liver Physiol 2010;298:G535–G541.
Acknowledgements
This work was supported from the Seoul National University Bundang Hospital (SNUBH) Research Fund (grant number 14-2015-019) and a clinical research grant-in-aid from the Seoul Metropolitan Government Seoul National University (SMG-SNU) Boramae Medical Center (03-2016-4).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Choe, JY., Park, M., Yun, J. et al. PELI1 expression is correlated with MYC and BCL6 expression and associated with poor prognosis in diffuse large B-cell lymphoma. Mod Pathol 29, 1313–1323 (2016). https://doi.org/10.1038/modpathol.2016.128
Received:
Revised:
Accepted:
Published:
Issue date:
DOI: https://doi.org/10.1038/modpathol.2016.128
