
Abstract
Background
The purpose of this study was to compare behavioral, psychosocial, and neighborhood environmental factors of long-term weight loss maintainers in North America and Europe.
Methods
Participants were weight loss maintainers in WeightWatchers in North America (n = 3656) and Europe (n = 624) who had maintained a ≥ 9.1 kg (21.7 kg on average) weight loss for ≥1 year (5.3 years on average) and had a current mean BMI of 29.9 kg/m2. Validated surveys assessed behavioral (e.g., self-weighing, dietary strategies, restaurant eating, physical activity, sedentary time) psychological (e.g., habit strength, future focus, diet consistency, motivation, quality of life, body image, internalized weight bias), and neighborhood environment factors.
Results
Weight loss maintainers in North America vs. Europe had higher odds of weekly self-weighing (95% vs. 91%; OR = 1.7 [95% CI: 1.1, 2.5]), eating at fast food restaurants ≥weekly (11.6% vs. 2.6%; 7.7 [3.9, 14.3]; p < 0.001]), and other restaurants (29.7% vs 17.3%; OR = 1.47 [1.2, 2.1]; p < 0.001), more positive scores for body image (21.4 vs.20.7; ηp2 = 0.253; p < 0.001) and body satisfaction (28.7 vs 22.8; ηp2 = 0.248; p < 0.001), less weight bias internalization (3.0 vs 3.1; ηp2 = 0.320; p < 0.001), shape concerns (2.3 vs 2.4; ηp2 = 0.181; p < 0.001) and weight concerns (2.6 vs2.7; ηp2 = 0.176; p < 0.001), and higher quality of life (75.0 vs. 73.4; ηp2 = 0.154; p < 0.001), including general health perception (72.3 vs 68.1; ηp2 = 0.187; p < 0.00), and physical functioning (81.3 vs 79.2; ηp2 = 0.252; p < 0.001). In a multivariable regression, the variables that most strongly differentiated weight loss maintainers in North America and Europe were fast food consumption (OR = 10.8 [4.6, 25.5] p < 0.001) and self-weighing (OR = 1.9 [1.2,3.0]; p < 0.01).
Conclusions
Weight loss maintainers in North America and Europe differed in restaurant eating and self-weighing practices but otherwise reported similar behavioral, psychological, and environmental strategies.
Similar content being viewed by others


Introduction
National registries of weight loss maintainers have helped identify the factors that promote long-term weight loss maintenance [1]. At the forefront was the National Weight Control Registry that has identified, among North American weight loss maintainers, several factors that promote long-term weight loss maintenance, including high levels of physical activity, dietary restraint, self-monitoring, and diet consistency [2]. Also in North America, but in the context of a commercial weight management setting, the WeightWatchers (WW) Success Registry has identified other strategies, including reduced sitting time, maintaining a positive body image, and living in a healthier retail food environments [3,4,5].
The extent to which the weight maintenance strategies documented in North America populations extend to the European weight loss maintainers remains unclear. In Europe, registries in Portugal [6], Germany [7], Greece, and Finland [8, 9] have documented some behavioral and psychological characteristics of weight loss maintainers in Europe. A systematic review of the European and North American registries found that the most consistent strategy across all regions was high physical activity [1]. However, as noted in the review, comparisons across registries was limited because the registries use different inclusion criteria, procedures, and measures [1, 4, 6, 9,10,11,12,13]. No study to date has used a standardized methodology to comprehensively examine cross-cultural differences in behavioral, psychosocial, and environmental factors of weight loss maintainers in different regions and cultural settings [14, 15]. A deeper understanding of the factors that facilitate long-term weight loss maintenance in different cultural contexts is needed to inform culturally tailored guidance to promote weight loss maintenance in different global contexts.
The purpose of this study was to compare the behavioral, psychosocial, and environmental factors of long-term weight loss maintainers in WW in North America (Canada, US) and Europe (United Kingdom, Germany, France, Netherlands, Switzerland, Sweden). Hypotheses were that weight loss maintainers in both regions would report similar levels of physical activity, self-weighing, and practice of healthy dietary strategies [1, 4, 6, 9,10,11,12,13]. Differences were examined in other factors, including behavioral (sedentary time, active transportation, beverage intake, restaurant eating), psychological (habit strength, diet consistency, motivation, quality of life, body image), and environmental (neighborhood environment).
Materials/subjects and methods
The WW Success Registry-Global (WWSR-G) enrolled participants from locations where it operated in North America (i.e., Canada, US) and Europe (i.e., United Kingdom, Germany, France, Netherlands, Switzerland, Sweden) between October 2020 and February 2024. Survey measures were completed at study entry. The consent form, screening, and assessments were sent to participants electronically via Research Electronic Data Capture (REDCap).
Ethics approval and consent to participate
Approval was obtained from the Cal Poly Institutional Review Board (#2018-022-CO), and all methods were performed in accordance with guidelines for the United States and the European Union’s General Data Protection Regulation criteria. Informed consent was obtained from all participants.
Enrollment
Prospective WWSR-G participants were recruited through an email sent by WW to identify members who had reported a loss of ≥20 lb (9.1 kg) >12 months ago [3, 5]. The recruitment email was sent in the predominant language of each participant’s country. Interested individuals were referred to the WWSR-G study server (hosted by Cal Poly) for online screening, consent, and enrollment in the language of their choosing, including German, English, French, and Dutch. All materials were translated and back translated for accuracy following pre-established protocols and consistent with EORTC (European Organisation for Research and Treatment of Cancer) translation procedures [16]. To be eligible for enrollment, an individual must have lost ≥9.1 kg (20 lb) via the WW program (online or in-person meetings), be aged ≥18 at the start of the WW membership during which they lost ≥9.1 kg, currently be ≥9.1 kg below their weight at the start of the membership during which they lost ≥9.1 kg, have maintained a ≥9.1 kg loss from that membership weight for at least 12 months, and be able to read and write in German, English, French, and/or Dutch. Eligibility was based on criteria used in the WWSR for the US [3, 5] and based on self-reported weight, height, and weight change and duration. The 20 pound (9.1 kg) weight loss maintenance criterion was selected to approximate a clinically significant 10% weight loss, assuming a 200 pound (90 kg) starting weight among people entering WW and other weight loss programs [17]. Use of this absolute weight loss value was also used for comparability purposes with other established registries [3, 18].
Measures
WWSR-G participants were asked to complete a series of surveys administered online via REDCap. All participants were asked demographic information, including about their gender, sex at birth, age, and marital status. Race/ethnicity data were collected with the exception of participants in France and Germany where regulations restricted collecting these data. Annual total family income was assessed in the currency of the country of enrollment and converted into increments of US $5000 [3]. Education was assessed consistent with country and converted into the following categories: Less than primary education, primary education, secondary education (junior high school), post-secondary/non-tertiary education, short-cycle tertiary education, bachelor’s or equivalent level, master’s or equivalent level, doctoral or equivalent level [3]. All participants were asked to provide details about weight history (age of onset of overweight, maximum lifetime weight, weight at beginning of WW) and current weight and height [3].
Behavioral factors
The Weight Control Strategies Scale [19] was used to measure weight control behaviors and included a total score and the following subscales: Dietary Choices, Self-Monitoring Strategies, Physical Activity, and Psychological Coping. Self-weighing was assessed by the question, “Currently, how often do you weigh yourself?” with options ranging from several times/day, one time/day, several times/week, one time/week, less than 1 time/week, less than 1 time/month, and never [3]. Participants were asked to complete the Three Factor Eating Inventory9, which includes subscales for Cognitive Restraint (conscious control over food intake) and Disinhibition (periodic loss of control over eating). Participants were asked about frequency of eating fast food, and examples that were given included McDonald’s, Burger King, Taco Bell, KFC, Pizza Hut, or Domino’s. They were also asked about the frequency of eating from non-fast-food restaurants that were described as “sit-down, full-service restaurants that had ordering from a waiter/waitress.” Frequency of eating at fast food or other restaurants was over the past 30 days with the following response categories: Never or rarely, 1 time per month, 2–3 times per month, 1–2 times per week, 3–4 times per week, 5–6 times per week, 1 time per day, 2 times per day, 3 or more times per day [3]. Sugar sweetened beverage intake was measured using the Brief Questionnaire to Assess Habitual Beverage Intake [20]. The International Physical Activity Questionnaire (IPAQ) was used to measure various dimensions of physical activity, including the total metabolic equivalent (MET) minutes per week of vigorous physical activity, moderate physical activity and walking, where a MET-minute represents the amount of energy expended in one minute of physical activity, calculated as a multiple of the energy expenditure at rest, with walking assigned a value of 3.3 METs, moderate activity 4.0 METs, and vigorous activity 8.0 METs. Sedentary behavior was assessed using the Multi-Context Sitting Time Questionnaire [21] that captures time spent sedentary during work, transportation, and leisure time. A measure from the National Household Travel Survey [22] assessed active transportation and how people got from place to place (e.g., walk, bike, bus, car, taxi).
Psychological Factors
Habit strength for exercise and healthy eating was measured using the Self-Report Habit Index [23]. Dietary and exercise consistency were measured with questions used in previous research [3, 24]. The Consideration of Future Consequences Scale [25] was used to measure the extent to which people consider the potential distant outcomes of their current behaviors and the extent to which they are influenced by these potential outcomes. The Treatment Self-Regulation Questionnaire [26] was used to measure the degree to which participants’ motivation for managing weight was autonomous (intrinsic), controlled (extrinsic) or lacking (amotivation). The Weight Bias Internalization Scale [27] was used to assess the degree to which a person applied societal weight biases to their own self-concept and behaviors. Quality of life was measured using the Short Form-20 Health Survey (SF-20) [28], including subscales of bodily pain, role functioning, general health perception, physical functioning, social functioning, and mental health. The Multidimensional Body-Self Ratings Questionnaire was used to measure body image, including the subscales of Body Areas Satisfaction and Appearance Evaluation [29]. The Eating Disorders Examination Questionnaire [30] was used to assess eating disorder symptoms and attitudes on a scale from 0 to 6, including restraint (avoidance of eating), shape concern (importance of body shape), eating concern (eating in secret), and weight concern (importance of body weight).
Neighborhood environment
Perceptions of the neighborhood physical environment was assessed using a modified version of the abbreviated Neighborhood Environment and Walking Scale [31]. The scale measures perception of neighborhood design features hypothesized to be related to physical activity. These include perceptions of neighborhood’s land use mix, street connectivity, density, cycling and walking infrastructure, neighborhood’s aesthetics, and traffic and crime safety. The measure is comprised of 5-point Likert-type scale items (1 = strongly disagree, 5 = strongly agree).
Statistics
Independent t-tests and chi square tests were used to compare differences between survey completers and non-completers in socioeconomic factors, including region (North America vs. Europe), age, income, education, marital status, race/ethnicity, body mass index (BMI), BMI at start of WW, lifetime maximum weight, weight loss since starting WW, and duration of ≥9 kg loss. Country level data were combined a priori into two regions (North America and Europe). Independent t-tests and chi square tests were used to compare differences in sociodemographic factors between weight loss maintainers in the two regions. Behavioral, psychological, and environmental factors were compared between the two regions using a general linear model (GLM), adjusting for age, duration of weight loss maintenance, employment, education, income, maximum lifetime weight, current weight and sex at birth. Among the set variables that differed between the regions in these initial univariate analyses, logistic regression was used to determine the strategies that most discriminated weight loss maintainers in North America vs. Europe (block 1 = sociodemographics; block 2 = the behavioral/psychological/environmental determinants). In selecting variables for the regression, variables within one domain (behavioral/ psychological/ environmental) that had high multicollinearity (Pearson correlation coefficients >0.80) were evaluated, and the variable with the strongest theoretical justification, highest internal validity, and biggest effect size in the univariate analyses was chosen for inclusion [32, 33]. To guard against type 1 error due to multiple analyses, statistical significance for all GLM models and the regression was set to p < 0.01 and significance only interpreted for group differences that resulted in partial eta square (ηp2) values ≥ 0.15 as done in prior work [3], and representing an effect size d ≥ 0.20 [32, 33]. A post-hoc, sensitivity analysis was done in which Propensity Score Matching was used to create matched pairs of participants from North America and Europe who were matched on age, income, education, marital status, employment, lifetime maximum weight, and BMI at study entry. We utilized nearest-neighbor matching with a caliper of <0.1 to ensure a high degree of similarity between matched cases from the two regions. From the matched dataset, a subset of pairs (n = 434 per group) was randomly selected for further analysis. The SPSS (23.0.0) statistical package was used for all analyses.
Results
A total of 44,246 prospective participants accessed the study link hosted by Cal Poly for online information, screening, consent, and enrollment. Of these, 5904 (13.3%) completed the screening and consented to study participation and, of these, 4280 (72.5%) completed the survey for the Weight Control Strategies Questionnaire and were included in this study. Completers vs non completers were slightly older (mean [SD] of 57.1 [12.1] vs 55.9 [12.8] years, respectively; p = 0.002), more likely to be married (68.6 vs 62.4%; p = 0.002) and less likely to be employed (58.5 vs 66.0%; p = 0.0003). Completers had a greater proportion who identified as White (vs. non-White; 93.0 vs 39.6%; p < 0.0001) and from North America (vs. Europe; 73.7% vs. 70.5%; p = 0.03). Completion vs non-completion rates didn’t significantly differ by language (Dutch, English, French, German, Swedish), income, education, gender identity, sex at birth, BMI at study entry, weight loss from WW start, weight loss from lifetime maximum weight, and duration of weight loss maintenance.
Demographic characteristics of weight loss maintainers in North America and Europe are displayed in Table 1. Participants in North American region were from the United States (88.3%) and Canada (11.7%). Participants in the European region were from the United Kingdom (41.2%), Germany (22.6%), France (14.1%), the Netherlands (10.7%), Belgium (3.4%), and Switzerland (5.0%) and Sweden (3.0%). Participants in both regions identified mostly as female and non-Hispanic White. At the time of study enrollment and since initiating WW, weight loss maintainers in North America and Europe had lost substantial amounts of weight (22 and 20 kg, respectively) and had maintained ≥9.1 loss on average for 5 years (Table 1). Weight loss maintainers from North America (vs. Europe) were older (58 vs 53 years, respectively), had greater proportions with an annual income ≥$75,000 (64% vs 32%) and a college education or higher (70% vs 60%), and a lower proportion currently employed (56% vs72%), and had a higher lifetime maximum weight (110 vs 104 kg) and BMI at the start of WW (38 vs 36 kg/m2). These differences were adjusted for in subsequent analyses.
Univariate analyses of group differences
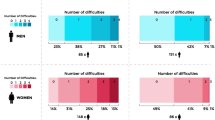
Table 2 shows the behavioral, psychological, and environmental factors of weight loss maintainers in North America and Europe. Examining behavioral factors, group differences that met the pre-specified effect size (ηp2 ≥ 0.15) threshold included a greater proportion of weight loss maintainers in North America than in Europe reporting weekly or more frequent consumption of fast food (11.6% vs 2.6%), and dining at a sit-down (non-fast food) restaurants (29.7% vs 17.3%; Fig. 1). The vast majority of weight loss maintainers in both regions reported weekly or more frequent self-weighing, but a greater proportion was reported among North American than among European weight loss maintainers (95% vs. 91%). Weight loss maintainers in both regions reported similar scores on the Weight Control Strategies total scale and subscales, including frequent practice of weight control strategies for healthy eating, self-monitoring, and psychological coping. Weight loss maintainers in both regions reported low consumption of sugar sweetened beverages (95.1% reporting never) and frequent engagement in moderate-to-vigorous physical activity, averaging 2484 MET-minutes (200 min) of moderate to vigorous activity per week. Weight loss maintainers in both regions also reported often walking for transportation and maintaining consistent eating and activity routines (Table 2).

A greater proportion (%) of weight loss maintainers in North America (shown in black) than in Europe (shown in gray) reporting weekly or more frequent consumption of fast food, and dining at a sit-down (non-fast food) restaurants. Odds ratios (OR) are also shown.
In adjusted analyses, weight loss maintainers in North America compared with Europe reported higher levels of satisfaction with their body weight, lower weight bias internalization, and less shape and weight concerns. Quality of life scores overall in both regions were good (scores of 60–79) to excellent (scores >80), but weight loss maintainers in North America reported higher quality of life scores overall and specifically in perceptions of general health and physical functioning (Table 2). Weight loss maintainers in both regions reported predominantly intrinsic (i.e., autonomous) motivation for maintaining long-term weight loss. There were no significant differences in the neighborhood environment variables reported among weight loss maintainers in North America vs. Europe, and scores suggested participants lived in generally safe, connected, and retail-accessible environments.
Logistic regression
Logistic regression analysis was conducted to determine, among subscale variables that differed between groups in univariate analyses, which variables most strongly predicted the weight loss maintainer group in North America vs. Europe. As shown in Table 3, after adjusting for sociodemographic factors, weekly or more frequent consumption of fast food was 10.8 times more likely among weight loss maintainers in North America compared with Europe. Weekly or more frequent self-weighing was 1.9 times more likely among North American than European weight loss maintainers. Other variables entered into the model (body satisfaction, and physical functioning) did not meet the pre-specified effect size threshold (ηp2 ≥ 0.15) for interpreting significance. Similar findings were observed in the post-hoc sensitivity analysis of matched pairs (Supplementary Tables 1–3).
Discussion
This is the first known study to compare the characteristics of weight loss maintainers in North America and Europe. Weight loss maintainers in each region reported similar weight loss and maintenance histories. Some different strategies were that those in Europe reported less restaurant eating, and those in North America reported more self-weighing, a more positive body image, and better physical functioning. However, similarities in both regions were more common. Weight loss maintainers in both regions reported frequent practice of healthy eating strategies, high levels of physical activity, frequent self-monitoring, high intrinsic motivation, a good quality of life, and living in supportive neighborhood environments.
The finding of less restaurant eating among European compared with North American weight loss maintainers is consistent with spending data, which suggest that people from Europe spent about 30% of their food budget on eating out while people in America spent about 50% of their food budget on eating out [34, 35]. Some European registries have indicated that reducing the frequency of eating out was a critical strategy among successful weight loss maintainers. In the Finnish registry, 80% of weight loss maintainers reported limiting fast food intake as part of their weight loss maintenance [13]. In the Portuguese registry, 25% of participants reported this as an important approach during weight loss maintenance [6]. By contrast, in the German registry, frequency of eating out (3.7 times per week) was the same among weight loss maintainers and a general population [10]. Reducing restaurant eating may be a more culturally acceptable and feasible strategy for weight loss maintainers in European contexts that prioritize home cooking and potentially less practiced in cultures, including North American, that have a greater emphasis on fast food and eating for convenience [36].
It is unclear how North American weight loss maintainers, relative to Europeans, were able to maintain the same magnitude of long-term weight loss yet report eating out at fast food and other restaurants more frequently. North American maintainers might have been strategic in their consumption at fast food and other restaurants, opting for smaller portions or compensating with reduced caloric intake at other meals to offset the caloric load from restaurants. We did not assess takeout food or ready-prepared meals from restaurants; thus, regional differences in these practices remains unknown. Prior data from the WW registry has found that increases in restaurant eating were related to greater weight regain among weight loss maintainers in North America [37]. Whether the greater restaurant eating among weight loss maintainers in North American (vs Europe) would predict greater weight regain over time is an area for future research.
General population data have suggested that Europeans typically incorporate more physical activity into their daily routine, including walking or cycling, as compared to North Americans who live in a more car-dependent environments [36]. However, in the current study, weight loss maintainers in both regions engaged in similarly high levels of physical activity, averaging 2484 MET-minutes (200 min) of moderate-to-vigorous physical activity per week, consistent with other studies of weight loss maintainers [4, 6, 9,10,11,12,13]. In the current study, walking as a means of transportation was slightly more frequent in Europe, averaging at least a few times per week, as compared with North America, averaging a few times per month. While few prior studies of weight loss maintainers have examined walking for transportation, the Portuguese registry identified walking for transportation (driving/taking public transit) as a key characteristic of weight loss maintainers [6]. Nevertheless, in the current study, weight loss maintainers in both North America and Europe reported that cars were the most frequent mode of transportation.
The vast majority (>90%) of weight loss maintainers in both North America and Europe reported self-weighing on at least a weekly basis, which is consistent with other studies of weight loss maintainers [4, 6, 9,10,11,12,13]. However, proportions of weekly self-weighing were modestly higher in North America than in Europe. The WW program worldwide encourages weekly self-weighing because it has consistently been related to successful weight loss maintenance [38]. However, there may be different cultural attitudes toward self-weighing. North America and Europe have different recommendations for self-weighing during pregnancy, for example. In Europe, prenatal guidelines discourage self-weighing during pregnancy and cite a lack of data to support routine weighing [39], but in the US and Canada prenatal guidelines encourage routine weighing based on the available evidence [40].
In both regions, weight loss maintainers reported moderate satisfaction with their body’s appearance, after losing an average of 22 kg of body weight. However, weight loss maintainers in North America consistently reported more positive body image satisfaction, more positive evaluations of their appearance, less shape and weight concerns, and lower internalized weight bias scores, even after adjusting for weight, age, and other sociodemographic differences. Prior studies of weight loss maintainers have reported that appearance concerns were a major motivator for weight loss and maintenance in both North American [4, 5, 18] and European [9, 10, 13] weight loss maintainers. In one North America-based study, participants described profound embarrassment while shopping for clothes and being unable to fit into clothes, and the ability to fit into clothes was reported as one of the most important things that changed after weight loss [4]. The persistence of appearance-based concerns as a motivator for weight maintenance in both Europe and North America may reflect sociocultural environments that continue to tie appearance with self-concept, discriminate against people with obesity, and promote an arbitrary definition of beauty based on a Westernized thin ideal [41]. Future weight-maintenance interventions in both Europe and North America should include empirically validated approaches for separating weight from body image [42, 43].
The dietary strategies of weight loss maintainers in North America and Europe included frequent self-monitoring of dietary intake, avoiding soft drinks, maintaining dietary restraint and consistency in their diet over the holidays and weekends. A systematic review of European and North American registries similarly reported that weight loss maintainers commonly engaged in healthy diet strategies, such as having healthy foods available at home and decreasing sugary foods [1], and prior work in WW in North America has shown that weight loss maintainers sustain high diet quality while living in a diversity of food environments [44]. For diet consistency, prior research has suggested that diet consistency over weekends and holidays was characteristic among North American weight loss maintainers [3, 24] and was protective against later weight regain among weight loss maintainers in Portugal [11]. However, diet consistency was not a distinguishing characteristic between weight loss maintainers and a general population in Germany [10].
While health status wasn’t directly assessed in the current study, weight loss maintainers in both regions reported positive perceptions of their health and a good, overall quality of life. This aligns with prior research in North America that showed quality of life scores were higher among weight loss maintainers compared to weight-stable individuals with obesity [3]. Improved quality of life may serve as a motivator for weight loss maintainers to continue to practice healthy eating, activity, and other weight loss maintenance strategies [45]. Given the average of participants was 57 years, and that chronic health conditions become more common with age, it is possible that health benefits served as particularly strong motivator for the weight maintenance among study participants [4]. Future research should explore whether and how health status influences weight loss maintenance strategies in different cultural contexts.
The study has several strengths, including being among the first to examine cross-cultural differences in weight loss maintenance [1]. While the International Weight Control Registry [14, 15] has enrolled from international settings, cross-cultural comparisons have not yet been reported. The current study used a comprehensive array of validated instruments in multiple languages and applied the same eligibility criteria and procedures across regions, filling in a major literature gap [1]. While differences in some sociodemographic characteristics were observed across regions, the study adjusted for these differences, and a sensitivity analysis of randomly selected matched pairs yielded consistent findings.
The study also has some limitations. Participants were predominantly female, White, higher income, and with higher education, yet people who have lower income, less education, and who come from historically marginalized populations have the greatest risk of obesity and related co-morbidities [46,47,48,49,50]. The study was cross sectional, and future prospective research is needed to identify whether predictors of weight loss maintenance differ between North American and European weight loss maintainers. This study focused on individual level and neighborhood environment determinants of weight and health, but weight management is influenced by multiple determinants functioning at multiple levels, with important interactions between levels [51, 52]. The study was not powered to examine differences at the country level, and instead a priori grouped countries with different cultures into one of two regions. “Culture” encompasses a wide range of elements, including language, traditions, customs, values, beliefs, and social norms, which can differ significantly with and across countries and geographic areas. Other unmeasured factors, such as the cost of living, price levels, and purchasing power, can differ widely within and across countries. The delineation of North America and Europe aligns with the World Health Organization definitions [53], but findings may not generalize to specific countries within each region.
In conclusion, weight loss maintainers in North America and Europe differed mainly in self-weighing and restaurant eating practices but otherwise practiced similar behavioral, psychological, and environmental strategies. Global interventions for weight loss maintenance should emphasize common strategies while accommodating for cultural differences.
Data availability
The datasets generated and analyzed during this study are not publicly available in accordance with the study’s informed consent but can be obtained from the corresponding author upon reasonable request.
References
Paixao C, Dias CM, Jorge R, Carraca EV, Yannakoulia M, de Zwaan M, et al. Successful weight loss maintenance: A systematic review of weight control registries. Obes Rev. 2020;21:e13003.
Thomas JG, Bond DS, Phelan S, Hill JO, Wing RR. Weight-loss maintenance for 10 years in the National Weight Control Registry. Am J Prev Med. 2014;46:17–23.
Phelan S, Halfman T, Pinto AM, Foster GD. Behavioral and Psychological Strategies of Long-Term Weight Loss Maintainers in a Widely Available Weight Management Program. Obesity. 2020;28:421–8.
Phelan S, Roake J, Alarcon N, Ng SM, Glanz H, Cardel MI, et al. In their own words: Topic analysis of the motivations and strategies of over 6000 long-term weight-loss maintainers. Obesity. 2022;30:751–61.
Phelan S, Cardel MI, Lee AM, Alarcon N, Foster GD. Behavioral, psychological, and environmental predictors of weight regain in a group of successful weight losers in a widely available weight-management program. Obesity. 2023;31:2709–19.
Santos I, Vieira PN, Silva MN, Sardinha LB, Teixeira PJ. Weight control behaviors of highly successful weight loss maintainers: the Portuguese Weight Control Registry. J Behav Med. 2017;40:366–71.
Neumann M, Holzapfel C, Muller A, Hilbert A, Crosby RD, de Zwaan M. Features and trajectories of eating behavior in weight-loss maintenance: Results from the German Weight Control Registry. Obesity. 2018;26:1501–8.
Soini S, Mustajoki P, Eriksson J, Lahti J. Personality traits associated with weight maintenance among successful weight losers. Am J Health Beh. 2018;42:78–84.
Soini S, Mustajoki P, Eriksson JG. Long-term weight maintenance after successful weight loss: Motivational factors, support, difficulties, and success Factors. Am J Health Behav. 2018;42:77–84.
Feller S, Muller A, Mayr A, Engeli S, Hilbert A, de Zwaan M. What distinguishes weight loss maintainers of the German Weight Control Registry from the general population? Obesity. 2015;23:1112–8.
Jorge R, Santos I, Teixeira VH, Teixeira PJ. Does diet strictness level during weekends and holiday periods influence 1-year follow-up weight loss maintenance? Evidence from the Portuguese Weight Control Registry. Nutr J. 2019;18:3.
Phelan S, Liu T, Gorin A, Lowe M, Hogan J, Fava J, et al. What distinguishes weight-loss maintainers from the treatment-seeking obese? Analysis of environmental, behavioral, and psychosocial variables in diverse populations. Ann Behav Med. 2009;38:94–104.
Soini S, Mustajoki P, Eriksson JG. Weight loss methods and changes in eating habits among successful weight losers. Ann Med. 2016;48:76–82.
Roberts SB, Das SK, Sayer RD, Caldwell AE, Wyatt HR, Mehta TS, et al. Technical report: an online international weight control registry to inform precision approaches to healthy weight management. Int J Obes. 2022;46:1728–33.
Clina JG, Sayer D, Gorczyca AM, Das SK, Friedman JE, Chui TK, et al. Weight history of individuals with and without physical disability in the International Weight Control Registry. Obesity Sci Pract. 2023;10:e733.
Cull A, Sprangers MAG, Bjordal K, Aaronson NK, West K, Bottomley A et al. EORTC Quality of Life Group Publication. Brussels: Quality of Life Group Publication: EORTC Brussels; 2002.
Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018;71:e127–e248.
Klem ML, Wing RR, McGuire MT, Seagle HM, Hill JO. A descriptive study of individuals successful at long-term maintenance of substantial weight loss. Am J Clin Nutr. 1997;66:239–46.
Pinto AM, Fava JL, Raynor HA, LaRose JG, Wing RR. Development and validation of the weight control strategies scale. Obesity. 2013;21:2429–36.
Hedrick VE, Savla J, Comber DL, Flack KD, Estabrooks PA, Nsiah-Kumi PA, et al. Development of a brief questionnaire to assess habitual beverage intake (BEVQ-15): Sugar-sweetened beverages and total beverage energy intake. J Acad Nutr Diet. 2012;112:840–9.
Clark BK, Lynch BM, Winkler EAH, Gardiner PA, Healy GN, Dunstan DW, et al. Validity of a multi-context sitting questionnaire across demographically diverse population groups: AusDiab3. Int J Behav Nutr Phys Act. 2015;12:148.
U.S. Department of Transportation Federal Highway Administration. Summary of Travel Trends: 2009 National Household Travel Survey In. 2011.
Verplanken B, Orbell S. Reflections on past behavior: A self-report index of habit strength. J Appl Soc Psychol. 2003;33:1313–30.
Gorin AA, Phelan S, Wing RR, Hill JO. Promoting long-term weight control: does dieting consistency matter? Int J Obes Relat Metab Disord. 2004;28:278–81.
Strathman A, Gleicher F, Boninger DS, Edwards CS. The consideration of future consequences: Weighing immediate and distant outcomes of behavior. J Pers Soc Psychol. 1994;66:742–52.
Williams GC, Grow VM, Freedman ZR, Ryan RM, Deci EL. Motivational predictors of weight loss and weight-loss maintenance. J Pers Soc Psychol. 1996;70:115–26.
Durso LE, Latner JD. Understanding self-directed stigma: development of the weight bias internalization scale. Obesity. 2008;16:S80–6.
Stewart AL, Hays RD, Ware JE Jr. The MOS short-form general health survey. Reliability and validity in a patient population. Med Care. 1988;26:724–35.
Cash TF. Multidimensional Body-Self Relations Questionnaire (MBSRQ, BSRQ): APA PsycTests. APA; 1990. Washington, DC. https://doi.org/10.1037/t03798-000
Faapprurn CG, Beglin SJ. Assessment of eating disorders: interview or self-report questionnaire? Int J Eat Disord. 1994;16:363–70.
Cerin E, Saelens BE, Sallis JF, Frank LD. Neighborhood environment walkability scale: Validity and development of a short form. Med Sci Sport Exer. 2006;38:1682–91.
Vatcheva KP, Lee M, McCormick JB, Rahbar MH. Multicollinearity in regression analyses conducted in epidemiologic studies. Epidemiology. 2016;6:227.
Kim JH. Multicollinearity and misleading statistical results. Korean J Anesthesiol. 2019;72:558–69.
USDA Economic Research Service. Food Expenditures. 2021. Retrieved from https://www.ers.usda.gov/topics/food-markets-prices/food-expenditures/.
Eurostat. Household consumption expenditure: Summary findings Household Consumption Expenditure. European Commission, 2021. Retrieved from https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Household_consumption_expenditure.
Sproesser G, Ruby MB, Arbit N, Akotia CS, Alvarenga MDS, Bhangaokar R, et al. Understanding traditional and modern eating: the TEP10 framework. BMC Public Health. 2019;19:1606.
Phelan S, Wyatt HR, Hill JO, Wing RR. Are the eating and exercise habits of successful weight losers changing? Obesity. 2006;14:710–6.
Vanwormer JJ, French SA, Pereira MA, Welsh EM. The impact of regular self-weighing on weight management: a systematic literature review. Int J Behav Nutr Phys Act. 2008;5:54.
National Institute for Clinical Excellence. Weight management before, during and after pregnancy: Public health guidance scope. London: NICE; 2010.
Institute of Medicine National Research Council Committee to Reexamine IOM Pregnancy Weight Guidelines. The National Academies Collection: Reports funded by National Institutes of Health. In: Rasmussen KM, Yaktine AL, editors. Weight Gain During Pregnancy: Reexamining the Guidelines. National Academies Press (US) National Academy of Sciences: Washington (DC); 2009.
Puhl RM, Lessard LM, Himmelstein MS, Foster GD. The roles of experienced and internalized weight stigma in healthcare experiences: Perspectives of adults engaged in weight management across six countries. PLoS One. 2021;16:e0251566.
Cash TF. The Body Image Workbook: An eight-step program for learning to like your looks, 2nd edn. Oakland, CA: New Harbinger Publications; 2008.
Foster GD. The shift : 7 powerful mindset changes for lasting weight loss, 1st ed. St. New York: Martin’s Press; 2021.
Clynes S, Moran A, Cardel M, Foster G, Phelan S. Weight loss maintainers sustain high diet quality in diverse residential retail food =environments. J Acad Nutr Diet. 2024;124:957–963 e3.
Brantley PJ, Stewart DW, Myers VH, Matthews-Ewald MR, Ard JD, Coughlin JW, et al. Psychosocial predictors of weight regain in the weight loss maintenance trial. J Behav Med. 2014;37:1155–68.
World Health Organization Regional Office for Europe. WHO European Regional Obesity Report. WHO; 2022.
Fagerberg P, Langlet B, Oravsky A, Sandborg J, Lof M, Ioakimidis I. Ultra-processed food advertisements dominate the food advertising landscape in two Stockholm areas with low vs high socioeconomic status. Is it time for regulatory action? BMC Public Health. 2019;19:1717.
Molenberg FJM, Mackenbach JD, Poelman MP, Santos S, Burdorf A, van Lenthe FJ. Socioeconomic inequalities in the food environment and body composition among school-aged children: a fixed-effects analysis. Int J Obes. 2021;45:2554–61.
Hoffimann E, Barros H, Ribeiro AI. Socioeconomic inequalities in green space quality and accessibility-Evidence from a Southern European City. Int J Environ Res Public Health. 2017;14:916.
Gelormino E, Melis G, Marietta C, Costa G. From built environment to health inequalities: An explanatory framework based on evidence. Prev Med Rep. 2015;2:737–45.
Finegood DT. The importance of systems thinking to address obesity. Nestle Nutr Inst Workshop Ser. 2012;73:123–37.
Lakerveld J, Mackenbach J. The Upstream Determinants of Adult Obesity. Obes Facts. 2017;10:216–22.
WHO CVD Risk Chart Working Group. World Health Organization cardiovascular disease risk charts: revised models to estimate risk in 21 global regions. Lancet Glob Health. 2019;7:e1332–e1345.
Acknowledgements
This research was supported by a grant from WeightWatchers, International, Inc.
Author information
Authors and Affiliations
Contributions
SP was responsible for designing the study, writing the manuscript, analyzing data, creating tables, and interpreting results. GDF, MIC, AML were responsible for designing the study. They contributed to writing the manuscript. NA was responsible for screening potentially eligible participants, collecting data, and providing feedback on the manuscript. MT contributed to the literature review, data analysis and table creation. NAA contributed to extracting and analyzing data and creating tables and provided feedback on the final manuscript.
Corresponding author
Ethics declarations
Competing interests
SP reports receiving a research grant for this study from WeightWatchers, International, Inc. MIC is an employee of WeightWatchers, International, AML, GDF were employees of WeightWatchers, International. MIC, AML, GDF are shareholders of WeightWatchers, International.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Phelan, S., Cardel, M.I., Lee, A.M. et al. Cross-cultural differences in weight loss maintenance: a comparison between North America and Europe. Int J Obes 49, 1297–1306 (2025). https://doi.org/10.1038/s41366-025-01770-0
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41366-025-01770-0
