
Abstract
Background/objectives
We provide the rationale for and description of energy balance measures (i.e., energy intake and energy expenditure) in The Physiology Of the WEight Reduced State (POWERS) study which aims to understand the contribution of the many factors that influence weight regain following behavioral weight loss.
Methods
The primary dependent variable is weight regain over 1 year following a 7% or greater supervised weight loss. The balance between energy intake and expenditure is the primary determinant of weight regain. Healthy adults (target n = 205), aged 25- < 60 years, with body mass index (BMI) 30- < 40 kg/m2 are being recruited. Energy intake and expenditure phenotypes are measured prior to weight loss (baseline, BL), immediately following weight loss (T0), and then four (T4) and 12 months (T12) after weight loss. Weight stability is required before BL and T0 measurement periods. Weight change at T12 from T0 is the primary outcome variable. Energy intake is measured with serial doubly labeled water (DLW) measurements combined with dual x-ray absorptiometry (DXA) to assess changes in fat and lean mass; DLW is also used to measure twenty-four-hour energy expenditure (TEE). Components of TEE including resting energy expenditure (REE) and non-resting and activity energy expenditure (NREE and AEE), as well as skeletal muscle chemomechanical efficiency and grip strength are assessed. Self-reported dietary intake is assessed with interviewer-administered multiple-pass 24-hour food recalls.
Discussion
This manuscript describes the rationale for the methods chosen to assess energy balance and the analytical methods employed to normalize and express data in the setting of changes in body weight and composition immediately following behavioral weight loss and thereafter at 4- and 12-months post-weight loss.
Similar content being viewed by others

Introduction
The primary goal of the Physiology Of the WEight Reduced State (POWERS) study is to determine the physiological basis for the variability in weight regain among adults with obesity following clinically significant weight loss achieved in a behavioral weight loss (BWL) intervention including diet, exercise, and regular self-monitoring. The rationale for, and overall design of POWERS are provided elsewhere [1]. The physiological contributors to energy balance are examined to understand factors that differentiate those who maintain their reduced weight, continue to lose weight, or regain some or all their lost weight. Adaptive thermogenesis [declines in energy expenditure (EE) beyond those attributable to changes in body composition or time spent in physical activity (PA)] and increased energy intake (EI) reported to occur with BWL have been hypothesized to play a role, but have not been significantly correlated with subsequent weight [2,3,4]. No studies have examined the effects of early changes occurring in EI and EE during weight maintenance efforts following BWL.
Changes in weight, and in energy stores [sum of energy in changes in fat mass (FM) and fat-free mass (FFM)] over time must reflect differences between daily EI and EE (TEE) [5, 6], POWERS’ primary independent variables. These factors will be measured at four points: Baseline (BL, prior to a BWL intervention); T0 (directly following weight loss of >7% and 2 weeks of weight stability); T4 (4 months following T0), and T12 (12 months following T0). No intervention will be provided after T0. Data will be analyzed to examine the effects on daily EI and EE, both calculated as an average of 14 days (see below) and weight regain of weight loss of >7% of BL (changes from BL to T0), and the early phase (T0 to T4) and the later phase (T4 to T12) of weight change occurring without behavioral support from T0 to T12. The primary and secondary measures of dependent and independent variables related to energy balance are summarized in Table 1.
Average responses to BWL interventions are weight loss (approximately 4–9 months), then relative weight stability (approximately 5–9 months), then weight regain. POWERS will study the variability in these responses to understand the predictors and drivers of changes in body weight and energy stores after weight loss [7,8,9,10,11,12]. Weight stability will be required before BL and T0 study points to ensure these crucial measures are not influenced by acute effects of negative or positive energy balance. T4 was chosen to maximize the opportunity to examine detectable changes in EI and TEE in the early period following weight loss (when significant weight change from T0 is less likely) that may be premonitory of subsequent weight change. T12 measurements allow observation of EI and EE over time and study of temporal correlations of early and later measures after weight loss.
The relationship of body composition, EI and EE is complex. FFM is the primary determinant of TEE, especially resting energy expenditure (REE). Fat mass (FM) has a larger effect on activity energy expenditure (AEE) than REE due to the extra work involved in moving a total body mass when engaged in PA [13, 14]. Changes in energy balance (weight gain or loss) and energy stores (predominantly FM) affect these relationships.
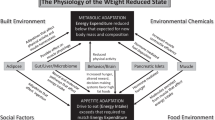
At usual weight, EI and TEE vary directly to contribute to maintenance of body weight despite wide daily fluctuations in diet and PA. This apparent “coupling” is consistent with the relative constancy of body weight in U.S. adults with average gain of 0.5 to 1.5 kg/year (about 4000 kcal, less than 0.5% of the average annual caloric intake) [15,16,17]. Attempts to lose weight (negative energy balance) and avoid regain (maintain energy balance) have been associated with varying degrees of increased appetite and decline in TEE [18,19,20] beyond those predicted by changes in body weight and energy stores (see Fig. 1). Data suggest EI may change in response to variation in TEE [21] more than EE responds to changes in EI. REE and AEE adjusted for age and body composition have been reported to account, respectively, for about 55% and 20% of the variation [22,23,24,25,26] in daily EI [27]; short-term changes in EI have much smaller effects on EE [28,29,30,31,32].

These systems act coordinately to increase energy intake (EI) and decrease energy expenditure (EE) in response to negative energy balance or reduced energy stores (predominantly fat). The degrees to which various afferent signals of energy stores (predominantly from adipose tissue) and efferent outputs affecting both EI and EE (predominantly originating in the central nervous system) are “engaged” during and following weight reduction are highly variable between individuals which contributes to the large inter-individual variability in weight regain over longer timeframes. In POWERS, interrogating this variability will advance understanding of the physiology of the weight-reduced state.
POWERS analyzes the nature and regulation of the relationship between EI and EE following weight loss (which are associated with different genotypes [33,34,35] and phenotypes [36,37,38,39,40,41,42,43,44], and treatment responses [45,46,47,48,49] than during weight loss). A key purpose of POWERS is to examine this variability under standardized conditions and determine to what extent changes in components of energy balance [50,51,52,53] occurring during weight loss and novel changes following weight loss, are associated with subsequent weight regain. This manuscript discusses the methods used to assess energy intake, utilization, stores, and expenditure.
Primary dependent and independent variables related to energy balance
The primary outcome (dependent) variables of POWERS are percentage and absolute changes in body weight (kg) over 1 year following a > 7% weight loss. The fractional contributions of changes in FM and FFM to changes in body weight are influenced by many factors including, but not limited to, sex, age, energy balance, diet composition, and PA [54]. FM and FFM must be measured both during and after the weight loss phases to assess fuel partitioning and energy stores (FM and FFM) due to the roughly 9-fold differences in the caloric storage density of FM (9.3 kcal/gm) versus FFM (1.1 kcal/gm) [55]. Comparisons of EI and TEE, REE, AEE and various biomarkers, between participant groups (e.g., ethnicity/race) or within participants (e.g., temporal changes) must be “normalized” to body composition, which will be measured by dual energy x-ray absorptiometry (DXA) for accurate interpretation [56,57,58,59].
Energy expenditure
Total energy expenditure (TEE)
TEE includes REE, the thermic effect of feeding (TEF), NREE [total daily energy expenditure above resting which consists of (TEF) and AEE (energy expended in PA)] [13], with a variable degree of change observed in EE during and following weight loss [60,61,62].
The primary measure of TEE in POWERS will be by doubly labeled water (DLW) [63] which relies on the fact that the oxygen in metabolically produced CO2 quickly reaches isotopic exchange equilibrium with that in body water due to the action of carbonic anhydrase. CO2 production will be measured from the differential elimination rates of deuterium (eliminated only in water) and oxygen (18O—eliminated in both water and CO2). In the fasted state, a urine sample will be obtained to assess background isotope enrichment. Participants are weighed and given an accurately weighed dose of enriched water to drink with approximately 10 atom percent excess (APE) 18O (H218O) and 5 APE deuterium (D2O) and is calculated to result in an enrichment of about 200 ppm 18O excess above background levels and 100 ppm deuterium excess. The dose equilibrates in the body water for the next 3 h during which participants refrain from food or excessive water consumption; additional urine samples are obtained on-site. Participants then provide additional daily urine samples for another 14 days.
The isotope enrichments in urine are determined using off-axis laser spectroscopy [64] in parallel with simultaneously run laboratory and international standards and background enrichment values are subtracted from post-dose samples. The resultant excess enrichments are loge converted, and a linear relationship fitted to the derived values to estimate the elimination constants (ko and kd) (gradients) and back extrapolated to intercepts at the dosing time to estimate the dilution spaces of the two isotopes (No and Nd). The values of elimination constants and dilution spaces are then combined to estimate the CO2 production using a recently derived equation that performed best in retrospective validation studies [65]. The average accuracy across n = 61 simultaneous indirect chamber calorimetry trials for this equation was −0.4% and precision was 7.67%.
To calculate EE, the CO2 production must be converted using an estimate of the respiratory exchange ratio [RER the ratio of the volume of CO2 produced (VCO2) to the volume of O2 consumed (VO2)]. If the individual is in energy balance (weight stable) this can be derived from the “food quotient,” (FQ) from food intake records. During weight loss or gain this requires adjustment for the part of the expenditure derived from body fat. Similarly, if the individual is in energy balance the expenditure will be equivalent to the metabolizable energy intake but if not, the metabolizable energy intake estimate needs adjustment for the estimated weight change. The main advantage of DLW is that, unlike chamber calorimetry, it reflects TEE in a free-living participant over longer periods of time (usually 7-14 days). The disadvantages relate to imprecision in the conversion of CO2 production into EE which depend on the weight status of the participant and the accuracy of the FQ estimate.
Resting energy expenditure (REE)
Measurement of REE is required to determine NREE and AEE. REE will be measured at all four time points by indirect calorimetry using the same within site-specific equipment throughout the study to minimize error within and between participants. REE measurement is different between the two POWERS sites. Chamber calorimetry has the highest precision and accuracy for REE based on available methodologies [66], but was a resource available only at the Columbia University Irving Medical Center (CUIMC) site. It was decided to use the best REE methodology available at each site, recognizing that the different methodologies will be a limiting factor in interpreting REE data. We aim to collect all within-site and within-participant REE data on the same cart (Philadelphia) and in the same chamber (CUIMC) to maximize accuracy for data being collected within each site. During data analysis, using the sites’ merged data, site will be included as a covariate to ascertain whether differences related to REE instrument are apparent. Methodology by site is described below.
REE will be measured in the morning (approximately 6:30–8:00 a.m.) after an overnight inpatient stay to standardize fasting and other physiological conditions including PA. Prior to REE testing, participants are asked to maintain their usual dietary and activity behaviors during the 72 h prior to clinic visit, with no exercise during the 24-h before the overnight admission [67]. EI, sleep, PA, and menstrual phase (when relevant) are recorded. After a 10–12 overnight fast, the participant rests, but remains awake, on a recliner or in their hospital bed, in a thermoneutral noise-free environment for a measurement period of approximately 45–60 min.
REE at Columbia University Irving Medical Center (CUIMC)
Data collection will occur using a whole-room calorimeter consisting of an air-tight temperature-controlled room with pre-specified flow rate connected to a pull through calorimetry system (Sable Systems, Las Vegas NV). By flowing a known amount of fresh air through the room, respiratory gases from the study participant are sampled on the exhaust side of the system for measurement of O2 and CO2 using fuel cell oxygen and near infrared carbon dioxide sensors (Model GA-3m2, Sable Systems Intl, Las Vegas, NV) and analysis software for a SW-Promethium System is installed on a Sable Systems approved computer, with a Sable Systems Promethium Interface Module (Model IM-2). Data are recorded and processed on-line by the Sable software programs Caloscreen and Expedata. During the 60-min data collection period, the participant will be asked to remain motionless, awake, and relaxed. The first and last 10 min of data collection are discarded to allow for the room and sampling line air to reach steady state and eliminate anticipatory signaling from the participant that may artificially inflate EE. A more robust REE will be calculated from the expiratory gases collected in steady state during the remaining 40 min.
REE at Drexel-Dartmouth-Tufts-Penn (DTP)
REE will be measured via indirect calorimetry using a ventilated hood system (Parvo TrueOne 2400, http://www.parvo.com/trueone-2400/). Participants are asked to remain supine in bed, motionless, awake, and relaxed for the 45-min test. The first 15 min of test data are discarded. Calculations of O2 consumption (V̇O2) and CO2 production (V̇CO2) for the subsequent 30 min are generated from continuous measurements of gas exchange and used to calculate rate of REE. The calorimeter will be calibrated before each measurement with standardized gases and room air, and measurements of V̇O, V̇CO and respiratory quotient (RQ) are required to be within 2% of calibration values.
REE at both sites will be calculated using the Weir formula [68] to convert the steady state concentrations of collected respiratory gases (V̇O2 L/min and V̇CO2 L/min)) to EE in kilocalories per min (kcal/min) [REE, kcal/min = 3.941(V̇O2) + 1.106(V̇CO2). The coefficient of variation for REE is 2.8% ± 2.0% kcal/h, 3.1% ± 2.0% L/min for V̇O2 and 4.1% ± 1.7% L/min for V̇CO2.
NREE and AEE reflect, respectively, all energy expended above resting and all energy expended in PA. They are calculated as:
TEF (thermic effect of feeding), calculated as a percentage (10%) of EI derived from DLW, constitutes a small fraction of TEE and, and has not been shown to be affected by weight loss [69]. The inter-individual TEF variability is anticipated to result in a much greater variation in AEE compared to NREE even corrected for body composition and time spent in PA [70] which is measured by actigraphy during the DLW period (see below).
Adaptive thermogenesis
Adaptive thermogenesis is defined as the decline in TEE and its components occurring during and/or following weight loss [19] that is independent of body weight and composition [71] and not accounted for by changes in total PA. At any single point EE is often expressed per unit of FFM (TEE and REE), or weight (NREE and AEE). These ratios are not appropriate for longitudinal studies such as POWERS because the regression lines of EE measures to FFM or weight have non-zero intercepts, partially due to varying energy requirements of different FFM components. This issue is addressed by calculating the difference (residual) between predicted and actual EE for participants at each time-period, calculated as the measured EE values minus the predicted value for each participant based on regression of all EE values (TEE, REE, or AEE) against all relevant weight and body composition values (i.e., FFM and FM) in the same cohort measured at BL [4]. This will allow for temporal measurement of adaptive thermogenesis due to BWL, and duration of that adaptation up to a year (see Table 2).
Controlled in-patient studies with prescribed PA show that skeletal muscle chemomechanical contractile efficiency (MCME) is significantly associated with adaptive thermogenesis in NREE [72, 73]. There is, on the average, a significant increase in the amount of time spent in PA during and following BWL which is even greater if the weight loss intervention includes exercise as in the present study [74]. Changes in time spent in PA during the study are potential confounders of calculations of adaptative thermogenesis in TEE, NREE, and AEE. To minimize confounding effects of time spent in PA (behavioral), but not spontaneous or isometric PA, on assessments of physiological changes in thermogenesis, calculating changes in TEE, NREE and AEE will include the time spent in PA, which is expected to be light to moderate intensity, measured by accelerometry as a covariate. In addition to time spent in PA, there may also be BWL effects on energy expenditure arising from spontaneous physical activity, such as fidgeting and maintaining posture, and resting muscle physical activity to maintain body temperature, which may also contribute to adaptive thermogenesis but are not assessed in this study [75].
Energy intake (EI)
EI is a core variable and is defined as consumed metabolizable energy, assuming standard coefficients for the ratio of metabolizable energy to gross energy content [76]. Dietary quality with respect to macronutrients, micronutrients, dietary fiber, food form, energy density, portion size, and glycemic load will also be analyzed for additional contributions to energy balance. Assessments of components of EI, such as hunger, satiety, nausea, food cravings, disinhibition, and restraint are measured during various eating tasks, described elsewhere [77].
The primary measure of EI in POWERS will be based on changes in body energy stores over the 14 days when TEE is measured by DLW [55]. DXA measurements are performed on Day 1, immediately following ingestion of DLW isotopes, and again on Day 15, the final urine collection day. Changes in energy stores (ES) from DXA are calculated as follows:
EI over the 14-day period will be calculated as the sum of TEE and the change in energy stores. We plan to average EI during T0–T12 by integrating TEE over that period from DLW data and summing TEE with changes in body energy stores, which will reduce errors associated with short-term measurements.
Secondary independent variables in POWERS
Body composition
DXA measures FM, FFM and bone mineral content (BMC), where FFM represents the sum of lean mass (LM) and BMC at whole-body and regional (trunk, arms, legs, android, gynoid) levels [78,79,80]. At each study site, measures are collected on the same whole-body scanner (iDXA, GE Healthcare, Madison, WI; Encore software v16 at CUIMC and Horizon model, Hologic Inc., Marlborough, MA; software 13.5.3.1:3 at DTP). Eight DXA scans within 18 months are well within acceptable radiation safety limits. A DXA study identifies aggregate FFM which will be treated as a single variable in subsequent analyses but does not allow assessment of the contributions of individual components of FFM (muscle, liver, brain, etc.) which have significantly different metabolic rates [81, 82]. It should also be noted that the relative contributions of individual components of FFM to energy expenditure, as well as the hydration status of these components, may be affected by changes in body weight [83] and thereby influence interpretation of DXA data as it affects calculation of EE (reflecting changes in assessment of body composition) and EI (reflecting changes in both body composition and the energy density of FM and FFM).
Participant's maximum body width will be measured to confirm that all body parts fit within the DXA field-of-view, and all individuals of child-bearing potential must have a negative urine pregnancy test before each scan. Participants wear a hospital gown and are positioned with legs fully extended and flat, with hips and shoulders level, the spine straight, and the chin line above the shoulders. Arms are extended with hands turned in with thumbs facing up. Heels are separated by 6-10 inches and the legs inwardly rotated with toes touching. A short X-ray transparent Velcro strap (or masking tape) may encircle the top of the feet for proper positioning.
Reproducibility of DXA in adults is ±3.4% for FM and ±1.2% for FFM [84,85,86]. Scan modes are age and body weight/size-appropriate based on the manufacturer’s recommendations. All scans will be analyzed using the same software version at study completion. For quality control, an anthropomorphic spine phantom made of calcium hydroxyapatite embedded in a 17.5 × 15 × 17.5 cm block will be scanned each morning prior to study, and before and after all DXA system maintenance visits. A protocol for calibration between sites will be established.
Waist circumference
Waist circumference is a secondary independent variable in POWERS because of its relationship to other secondary outcome variables including hypertension, fatty liver disease, and insulin resistance. It will be also used as a “proxy” for abdominal fat and measured at all time points (BL, T0, T4 and T12) using a spring-loaded Gulick II Measuring Tape (to allow consistent tension) at a marked point mid-way between the iliac crest and lowermost rib on bare skin. Participants will be instructed to breathe normally while staff take the measurement twice, with confirmation that the tape remained horizontal. If the measurements are within 0.5 cm, they are averaged. If not, a third will be taken. If all three are discrepant by >0.5 cm, the participant will be remeasured by another trained staff member.
Skeletal muscle chemomechanical efficiency (MCME)
Activity energy expenditure (AEE) is the compartment of EE proposed to account for most of the variability in changes in EE after weight loss [87], most likely due to an approximately 20% increase in MCME at low levels of exercise (commensurate with activities of daily living) which is significantly correlated with the residual in NREE [72, 73, 88, 89] independent of changes in time spent in PA [90]. MCME is defined as the amount of power (watts) above resting generated per volume of oxygen consumed during pedaling on a bicycle ergometer at incremental levels of resistance [73, 87].
Comparison of MCME at BL to T0 provides information regarding the relationship of MCME to energy expended in PA, which may affect subsequent weight regain and changes in MCME after weight loss. Comparisons of MCME from T0 to T4 allow investigation of whether changes in MCME during the early months of unsupervised weight maintenance correlate with weight regain from T0 to T4 and from T0 to T12. Comparisons of MCME from T0 and T4 to T12, respectively, allow investigation of whether the changes in MCME from BL to T0 or T0 to T4 are predictive of changes in later weight regain. Using all time points, the relationship of changes in MCME to energy expended in PA will be investigated, as weight changes.
MCME will be evaluated by standardized incremental graded cycle ergometry an electronically braked cycle ergometer (Lode Corival). Using indirect calorimetry (Parvo Medics TrueOne 2400 metabolic cart), O2 consumption and CO2 production values are collected during rest while seated on the cycle ergometer (4 min); thereafter, during exercise performed at specific incremental intensities: 10 Watts (4 min), 25 W (4 min) and 50 Watts (4 min). Based on existing data [72, 73, 87, 91], most effects of weight loss on MCME should be evident at 10 and 25 W. The MCME at 50 W serves to ascertain whether the measurable effects of weight loss on MCME have been detected at the lower levels of work. A final stage at 75 W (2 min) will be performed to allow estimation of cardio-respiratory fitness. Heart rate will be measured throughout the test.
Skeletal muscle contractile efficiency reflects skeletal muscle gene expression and biochemistry [73, 87, 91] as well as mitochondrial function. These will be assessed in skeletal muscle samples taken by needle biopsy at T0 and T4 [92], and will provide insights into how weight regain affects the relationship between MCME and skeletal molecular physiology.
Isometric hand grip strength
Hand grip strength is a commonly used measure of upper body skeletal muscle function [93, 94] and has been reported to decrease following weight reduction [95]. It is not known to what degree changes in grip strength reflect changes in muscle composition MCME [91]. Grip strength in both hands will be measured as according to the Lifestyle for Independence in Elders trial (LIFE) [96] using a JAMAR handheld hydraulic dynamometer (Patterson Medical) at all study periods (BL, T0, T4, T12). This test will be performed in duplicate in a seated position, arm resting on a table with the elbow bent. The participant will be instructed to squeeze as hard as they can, allowing 10 seconds between each measurement. This tests the potential change in grip strength with weight loss and across the maintenance phase and associations between change in grip strength and change in appendicular lean mass (measured by DXA).
Total daily energy intake and diet composition
The primary assessment of EI described above estimates caloric intake but not diet composition. The multiple pass 24-h recall method [97] assesses average total daily food intake (both quantity and quality) in a more naturalistic setting and permits assessment of the possible effects of the differences in perceived vs. actual intake on subsequent weight regain [98].
Four 24-h dietary recalls over a 2-week period are conducted at BL, T0, T4, and T12. One is conducted the day before REE measures, to provide information on dietary intake in the immediate period before REE. The other three recall timepoints are selected at random, with the goal of obtaining two on weekdays and one on weekends, capturing potential variability in dietary intake and quality [99]. Additional 3-day dietary assessments are collected monthly during the T0 to T12 period.
The recalls are analyzed using the latest version of Nutrition Data System for Research (NDSR, Nutrition Coordinating Center (NCC), University of Minnesota, Minneapolis, MN). Output data include daily reported EI, macronutrient (fat, protein, carbohydrate) intakes, daily time interval for eating, number of meals and snacks, food groups, diet quality, diet variety, and dietary supplement use. The 24-h recall data are also used to calculate a Healthy Eating Index score using algorithms and SAS code provided by the University of Minnesota NCC and the National Cancer Institute. Direct observation of energy intake during a single meal and energy intake in the absence of hunger are being collected at T0 and T4 and are described elsewhere [77].
Conclusions
The methods of assessing energy intake, stores, and expenditure being employed in POWERS reflect the application of state-of-the-art methodology to studies of energy balance in community-dwelling participants. The physiological, genetic, environmental, behavioral, cognitive, and other –omics that affect these variables are discussed in other papers in this issue. Both the changes in EI and EE that occur with weight loss (baseline to T0) and during the early post-weight loss phase (T0 to T4) are examined in POWERS and related to the multiple mechanistic and behavioral variables discussed in other papers in this issue, to create a systems model of body weight regulation that can be leveraged to optimize interventions to promote weight loss maintenance and prevent weight regain.
References
Belle SH, Gallagher D, Roberts SB, Laughlin MR, Das SK, Whyte KJ, et al. The Physiology Of the WEight Reduced State (POWERS) study: overview and study design. Int. J Obes., in press.
Martins C, Gower G, Hill J, Hunter G. Metabolic adaptation is not a major barrier to weight-loss maintenance. Am J Clin Nutr. 2020;112:558–65.
Turicchi J, O’Driscoll R, Finlayson G, Duarte C, Hopkins M, Martins N, et al. Associations between the proportion of fat-free mass loss during weight loss, changes in appetite, and subsequent weight change: results from a randomized 2-stage dietary intervention trial. Am J Clin Nutr. 2020;111:536–44.
Thom G, Dombrowski S, Brosnahan N, Algindan Y, Lopez-Gonzalez M, Roditi G, et al. The role of appetite-related hormones, adaptive thermogenesis, perceived hunger and stress in long-term weight-loss maintenance: a mixed-methods study. Eur J Clin Nutr. 2020;74:622–32.
Clausius R. On the moving force of heat and the laws of heat which may be deduced therefrom. Phil Mag J Sci. 1851;2:102–19.
Fine E, Feinman R. Thermodynamics of weight loss diets. Nutr Metab. 2004;1:15.
Wadden T, Berkowitz R, Womble L, Sarwer D, Phelan S, Cato R, et al. Randomized trial of lifestyle modification and pharmacotherapy for obesity. N Eng J Med. 2005;353:2111–20.
Wadden T, Neiberg R, Wing R, Clark J, Delahanty L, Hill J, et al. Four-year weight losses in the Look AHEAD study: factors associated with long-term success. Obesity. 2011;19:1987–98.
Dansinger M, Tasioni S, Wong J, Chung M, Balk E. Meta-analysis: The effect of dietary counseling for weight loss. Ann Intern Med. 2007;147:41–50.
Das S, GIlhooly C, Golden J, Pittas A, Fuss P, Cheatham R, et al. Long-term effects of 2 energy-restricted diets differing in glycemic load on dietary adherence, body composition, and metabolism in CALERIE: a 1-y randomized controlled trial. Am J Clin Nutr. 2007;85:1023–30.
Foster G, Wyatt H, Hill J, Makris A, Rosenbaum D, Brill C, et al. Weight and metabolic outcomes after 2 years on a low-carbohydrate versus low-fat diet: a randomized trial. Ann Int Med. 2010;153:147–57.
Sacks F, Bray G, Carey V, Smith S, Ryan D, Anton S, et al. Comparison of weight-loss diets with different compositions of fat, protein, and carbohydrates. N Eng J Med. 2009;360:859–73.
Hills A, Mokhtar N, Byrne N. Assessment of physical activity and energy expenditure: an overview of objective measures. Front Nutr. 2014;1:5.
Schutz Y, Weinsier R, Hunter G. Assessment of free-living physical activity in humans: an overview of currently available and proposed new measures. Obes Res. 2001;9:368–79.
Center for Disease Control. Anthropometric Reference Data for Children and Adults: United States, 2007–2010.
Tucker L, Parker K. 10-year weight gain in 13,802 US adults: the role of age, sex, and race. J Obes. 2022;2022:7652408.
Centers for Disease Control and Prevention (CDC). QuickStats: average daily intake of kilocalories, by sex and age group, for adults aged ≥20 years—National Health and Nutrition Examination Survey, United States, 2007–2008. MMWR. 2011;60:280.
Busetto L, Bettini S, Makaronidis J, Roberts C, Halford J, Batterham R. Mechanisms of weight regain. Eur J Int Med. 2021;93:3–7.
Nunes C, Casanova N, Francicso R, Bosy-Westphal A, Hopkins M, Sardinha L, et al. Does adaptive thermogenesis occur after weight loss in adults? A systematic review. Br J Nutr. 2022;127:45–69.
Foster-Shubert K, Cummings D. Emergying therapuetic strategies for obesity. Endocrin Rev. 2006;27:779–93.
Blundell J, Gibbons C, Beaulieu K, Casanova N, Duarte C, Finlayson G, et al. The drive to eat in homo sapiens: energy expenditure drives energy intake. Physiol Behav. 2020;219:112846.
Rumpler W, Seale J, Moe P. Repeatability of 24-h energy expenditure measurements in humans by indirect calorimetry. Am J Clin Nutr. 1990;51:147–52.
Champagne C, Han H, Bajpeyi S, Rood J, Johnson W, Lammi-Keefe C, et al. Day-to-day variation in food intake and energy expenditure in healthy women: the Dietitian II study. J Acad Nutr Diet. 2013;113:1532–38.
Champagne C, Han H, Bajpeyi S, Lammi-Keefe C, Flatt J, Bray G. Day-to-day variation in food intake and energy expenditure in health women: the dietitian II study. J Acad Nutr Diet. 2013 P1532-58.
Blundell J, Gibbons C, Beaulieu K, Casanova N, Duarte C, Finlayson G, et al. The drive to eat in homo sapiens: Energy expenditure drives energy intake. Physiol Behav. 2022;219:112846.
Schoeller D, Hnilcka J. Reliability of the doubly labeled water method for the measurement of total daily energy expenditure in free-living subjects. J Nutr. 1996;126:348S–54S.
Blundell J, Gibbons C, Caudwell P, Finlayson G, Hopkins M. Appetite control and energy balance: Impact of exercise. Obes. 2015;16:67–76.
Martins C, Morgan L, Bloom S, Robertson M. Effects of exercise on gut peptides, energy intake, and appetite. J Endocrinol. 2007;193:251–58.
Martins C, Morgan L, Truby H. A review of the effects of exercise on appetite regulation: an obesity perspective. Int J Obes. 2008;32:1337–47.
Hubert P, King N, Blundell J. Uncoupling the effects of energy expenditure and energy intake: appetite response to short-term energy deficit induced by meal omission and physical activity. Appetite. 1998;31:9–19.
Joosen A, Westerterp K. Energy expenditure during overfeeding. Nutr Metab. 2006;12:25.
Maughan R, Fallah J, Coyle E. The effects of fasting on metabolism and performance. Br J Sports Med. 2010;44:490–44.
Delahanty L, Pan Q, Jablonski K, Watson K, McCaffery J, Shuldiner A, et al. Genetic predictors of weight loss and weight regain after intensive lifestyle modification, metformin treatment, or standard care in the Diabetes Prevention Program. Diab Care. 2012;35:363–66.
McCaffery J, Papandonagtos G, Huggins G, Peter I, Kahn S, Knowler W, et al. FTO predicts weight regain in the Look AHEAD clinical trial. Int J Obes. 2013;37:1545–52.
Papandonatos G, Pan Q, Pajewski N, Delahanty L, Peter I, Erar B, et al. Genetic predisposition to weight loss and regain with lifestyle intervention: analyses from the Diabetes Prevention Program and the Look AHEAD randomized controlled trials. Diabetes. 2015;64:4312–21.
Batra P, Das S, Robinson I, Saltzman E, Scott T, Pittas A, et al. Eating behaviors as predictors of weight loss in a 6 month weight loss intervention. Obesity. 2013;21:2256–63.
Womble L, Williamson D, Greenway F, Redmann S. Psychological and behavioral predictors of weight loss during drug treatment for obesity. Int J Obes. 2001;25:340–45.
Vogels N, Diepvens K, Westerterp-Plantenga M. Predictors of long-term weight maintenance. Obes Res. 2005;13:2162–68.
Hansen D, Astrup A, Toubro S, Finer N, Kopelman P, Hilsted J, et al. Predictors of weight loss and maintenance during 2 years of treatment by sibutramine in obesity. Results from the European multi-centre STORM trial. Sibutramine Trial of Obesity Reduction and Maintenance. Int J Obes. 2001;25:496–501.
Foster G, Wadden T, Swain R, Stunkard A, Platte P, Vogt R. The Eating Inventory in obese women: clinical correlates and relationship to weight loss. Int J Obes. 1998;22:778–85.
Munro I, Bore M, Nunro D, Garg M. Using personality as a predictor of diet induced weight loss and weight management. Int J Behav Nutr Phys Act. 2011;8:129.
Price D, Ma Y, Rubin R, Perreault L, Marrero D, Knowler W, et al. Depression as a predictor of weight regain among successful weight losers in the diabetes prevention program. Diab Care. 2013;36:216–21.
Wolters B, Lass N, Reinehr T. TSH and free triiodothyronine concentrations are associated with weight loss in a lifestyle intervention and weight regain afterwards in obese children. Eur J Endocrinol. 2013;168:323–29.
Stunkard A, Fernstrom M, Ptice R, Buss E, Frank E, Kupfer D. Weight change in depression: influence of “disinhibition” is mediated by body mass and other variables. Psychiatr Res. 1991;38:197–200.
Rosenbaum M, Leibel R. 20 years of leptin: role of leptin in energy homeostasis in humans. J Endocrinol. 2014;223:T83–96.
Rosenbaum M, Hirsch J, Murphy E, Leibel R. The effects of changes in body weight on carbohydrate metabolism, catecholamine excretion, and thyroid function. Am J Clin Nutr. 2000;71:1421–32.
Sumithran P, Proietto J. The defence of body weight: a physiological basis for weight regain after weight loss. Clin Sci. 2013;124:231–41.
Sumithran P, Prendergast L, Delbridge E, Purcell K, Shulkes A, Kriketos A, et al. Long-term persistance of hormonal adaptations to weight loss. N Eng J Med. 2011;365:1597–604.
Salem V, Demetriou L, Behary P, Alexiadou K, Scholtz S, Tharakan G, et al. Weight loss by low-calorie diet versus gastric bypass surgery in people with diabetes results in divergent brain activation patterns: a functional MRI study. Diab Care. 2021;44:1842–51.
Dent R, McPherson R, Happer M. Factors affecting weight loss variability in obesity. Metabolism. 2020;113:154388.
Bussetto L, Bettini S, Roberts C, Halford J, Batterham R. Mechanisms of weight regain. Eur J Int Med. 2021;93:3–7.
Mcneil J, Liepert M, Brenner D, Courneya K, Friedenreich C. Behavioral preedictors of weight regain in posmenopausal women: exploratory results from the breast cancer and exercise trial in Alberta. Obesity. 2019;27:1451–63.
Nymo S, Coutinho S, Rehfeld J, Truby H, Kulseng B, Martins C. Physiological predictors of weight regain at 1-year follow-up in weight-reduced adults with obesity. Obes. 2019;27:925–31.
Forbes GB. Lean body mass-body fat interrelationships in humans. Nutr Rev. 1987;45:225–31.
Racette S, Das S, Bhapkar M, Hadley E, Roberts S, Ravussin E, et al. Approaches for quantifying energy intake and %calorie restriction during calorie restriction interventions in humans: the multicenter CALERIE study. Am J Physiol Endocrinol Metab. 2012;302:E441–48.
Ravussin E, Lillioja S, Anderson T, Christin L, Bogardus C. Determinants of 24-hour energy expenditure in man. Methods and results using a respiratory chamber. J Clin Investig. 1986;78:1568–78.
Rosenbaum M, Agurs-Collins T, Bray M, Hall K, Hopkins M, Laughlin M, et al. The Accumulating Data to Optimally Predict Obesity Treatment (ADOPT): Recommendations from the biological domain. Obesity. 2018;26.
Rosenbaum M, Nicolson M, Hirsch J, Heymsfield S, Gallagher D, Chu F, et al. Effects of gender, body composition, and menopause on plasma concentrations of leptin. J Clin Endocrinol Metab. 1996;81:3424–27.
Rosenbaum M, Nicolson M, Hirsch J, Murphy E, Chu F, Leibel R. Effects of weight change on plasma leptin concentrations and energy expenditure. J Clin Endocrinol Metab. 1997;82:3647–54.
Egan A, Collins A. Dynamic changes in energy expenditure in response to underfeeding: a review. Proc Nutr Sci. 2022;81:199–212.
Rosenbaum M, Hirsch J, Gallagher D, Leibel R. Long-term persistence of adaptive thermogenesis in subjects who have maintained a reduced body weight. Am J Clin Nutr. 2008;88:906–12.
Rosenbaum M, Leibel R. Adaptive thermogenesis in humans. Int J Obes. 2010;34:S47–55.
Speakman J. Doubly-labelled water: theory and practice: Springer New York (1997).
Berman E, Forston S, Snaith S, Gupta M, Baer D, Chery I, et al. Direct analysis of δ2H and δ18O in natural and enriched human urine using laser-based, off-axis integrated cavity output spectroscopy. Anal Chem. 2012;84:9768–73.
Speakman J, Yamada Y, Sagatyama H, Berman E, Ainslee P, Andersen L, et al. A standard calculation methodology for human doubly labeled water studies. Cell Rep Med. 2021;2:10023.
Rising R, Whyte K, Albu J, Pi-Sunyer X. Evaluation of a new whole room indirect calorimeter specific for measurement of resting metabolic rate. Nutr Metab. 2015;12:46.
Chen K, Smith S, Ravussin E, Krakoff J, Plasqui G, Tanaka S, et al. Room Indirect Calorimetry operating and reporting standards (RICORS 1.0). A guide to conducting and reporting human wWhole-room calorimeter studies. Obesity. 2020;28:1613–25.
Weir J. New methods for calulating metabolic rate with special reference to protein metabolism. Nutrition. 1990;6:212–21.
Leibel R, Rosenbaum M, Hirsch J. Changes in energy expenditure resulting from altered body weight. N Eng J Med. 1995;332:621–28.
Speakman J, Pontzer H. Quantifying physical activity energy expenditure based on doubly labelled water and basal metabolism calorimetry: what are we actually measuring? Curr Opin Clin Nutr Metab Care. 2023;26:401–08.
Muller M. Bpst-Westphal A. Adaptive thermogenesis with weight loss in humans. Obesity. 2013;21:218–21.
Rosenbaum M, Vandenborne K, Goldsmith R, Simoneau J, Heymsfield S, Joanisse D, et al. Effects of experimental weight perturbation on skeletal muscle work efficiency in human subjects. Am J Physiol Endocrinol Metab. 2003;285:R183–92.
Goldsmith R, Joanisse D, Gallagher D, Pavlovich K, Shamoon E, Leibel R, et al. Effects of experimental weight perturbation on skeletal muscle work efficiency, fuel utilization, and biochemistry in human subjects. Am J Physiol. 2010;298:R79–88.
Jakicic J, Rogers R, Lang W, Gibbs B, Yuan N, Friedman Y, et al. Impact of weight loss with diet or diet plus physical activity on cardiac magnetic resonance imaging and cardiovascular disease risk factors: Heart Health Study randomized trial. Obesity. 2022;30:1039–56.
Dulloo A, Miles-Chan J, Montani J, Schutz Y. Isometric thermogenesis at rest and during movement: a neglected variable in energy expenditure and obesity predisposition. Obes Rev. 2017;2017:56–64.
Sánchez-Peña M, Márquez-Sandoval F, Ramírez-Anguiano A, Velasco-Ramírez S, Macedo-Ojeda BM, Gonzalez-Ortiz L. Calculating the metabolizable energy of macronutrients: a critical review of Atwater’s results. Nutr Rev. 2017;75:37–48.
Mayer LES, Lowe M, Allison KC, Ashby-Thompson M, Benasi G, Burger KS, et al. The Physiology Of the WEight Reduced State (POWERS) study: design and rationale for assessment of food intake, physical activity and other behavioral constructs. Int J Obes., in press.
Hull H, HE Q, Thornton J, Javed F, Allen L, Wang J, et al. iDXA, Prodigy, and DPXL dual-energy X-ray absorptiometry whole-body scans: a cross-calibration study. J Clin Denisitom. 2009;12:95–102.
Gallagher D, Visser M, Wang Z, Harris T, Pierson RNJ, Heymsfield S. Metabolically active component of fat-free body mass: influences of age, adiposity, and gender. Metabolsim. 1996;45:992–97.
Bergman R, Stefanovski D, Buchanan T, Sumner A, Reynolds J, Sebring N, et al. A better index of body adiposity. Obes. 2011;19:1083–89.
Gallagher D, Elia M. Body composition, organ mass, and resting energy expenditure. In: SB SH, Lohman T, Wang Z, Going S, editors. Human body composition. 2nd Edition. Champaign, IL: Human Kinetics; 2005. p. 219–39.
Bosy-Westphal A, Schautz B, Lagerpusch M, Pourhassan M, Braun W, Goele K, et al. Effect of weight loss and regain on adipose tissue distribution, composition of lean mass and resting energy expenditure in young overweight and obese adults. Int J Obes. 2013;37:1371–77.
Heymsfield S, Ludwig D, Wong J, McCarthy C, Heo M, Shepherd J, et al. Are methods of estimating fat-free mass loss with energy-restricted diets accurate?. Eur J Appl Physiol. 2023;77:525–31.
Gallagher D, Kovera A, Clay-Williams G, Aglin D, Leone P, Albu J, et al. Weight loss in post-menopausal women: no adverse alterations in body composition and protein metabolism. Am J Physiol Endocrinol Metab. 2000;279:124–31.
Ma K, Kotler D, Wang J, Thronton J, Ma R, RN Pierson J. Reliability of in vivo neutron activation analysis for measuring body composition: comparisons with tracer dilution and dual-energy X-ray absorptiometry. J Lab Clin Med. 1996;5:420–27.
Wu C-H, Heshka S, Wang J, Pierson RNJ, Heymsfield S, Laferrère B, et al. Truncal fat in relation to total body fat: influences of age, sex, ethnicity and fatness. Int J Obes. 2007;31:1384–91.
Rosenbaum M, Heaner M, Goldsmith R, Schultze P, Shukla A, Shen W, et al. Resistance training reduces skeletal muscle chemomechanical efficiency in weight-reduced and non-weight reduced subjects. Obesity. 2018;26:1576–83.
Emerenziani G, Ferrari D, Migliaccio S, Lenzi A, Greco E, Marocco C, et al. Effects of body weight loss program on parameters of muscle performance in female obese adults. J Sports Med Phys Fitness. 2019;59:624–31.
Hames K, Coes P, King W, Anthony S, Stefanovic-Racic M, Toledo F, et al. Resting and exercise energy metabolism in weight-reduced adults with severe obesity. Obes. 2016;24:1290–98.
Nunes C, Jesus F, Rosa G, Marianito M, Francisco R, Bosy-Westphal A, et al. Interindividual variability in energy intake and expenditure during a weight loss intervention. Appetite. 2024;193:107162.
Baldwin K, Joanisse D, Haddad F, Goldsmith R, Gallagher D, Pavlovich K, et al. Effects of weight loss and leptin on skeletal muscle in human subjects. Am J Physiol Endocrinol Metab. 2011;301:R1259–66.
Rosenbaum M, Allison KC, Laughlin MR, Kelley SS, Nunez-Matos J, Rickels M, et al. The Physiology Of the WEight Reduced State (POWERS) Study: strategies for the analysis of biological specimens. Int J Obes., in press.
Rantanen T, Guralnik J, Foley D, Masaki K, Leveille S, Curb J, et al. Midlife hand grip strength as a predictor of old age disability. JAMA. 1999;281:558–60.
Rantanen T, Harris T, Leveille S, Visser M, Foley D, Masaki L, et al. Muscle strength and body mass index as long-term predictors of mortality in initially healthy men. J Gerontol A Biol Sci Med. 2000;55:M168–73.
Zibellini J, Seimon R, Lee C, Gibson A, Hsu M, Sainsbury A. Effect of diet-induced weight loss on muscle strength in adults with overweight or obesity—a systematic review and meta-analysis of clinical trials. Obes Rev. 2016;17:647–63.
Fielding R, Rejeski S, Blair S, Church T, Espeland M, Gill T, et al. The lifestyle interventions and independence for elders study: design and methods. J Gerntol A Biol Med Sci. 2011;66A:1226–37.
Lytle L, Nicastro H, Roberts S, Evans M, Jakicic J, Laposky A, et al. Accumulating Data to Optimally Predict Obesity Treatment (ADOPT) core measures: behavioral domain. Obesity. 2018;26:S16–24.
Moshfegh A, RHodes D, Baer D, Murayi R, Clemens J, Rumpler W, et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am J Clin Nutr. 2008;88:324–32.
Jahns L, Conrad Z, Johnson L, Scheet A, Stote K, Raatz S. iet quality is lower and energy intake is higher on weekends compared with weekdays in midlife women: a 1-year cohort study. J Acad Nutr Diet. 2017;117:1080–86.
Acknowledgements
POWERS was funded as a Cooperative Agreement between the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), the NIH Offices of Disease Prevention (ODP), Behavior and Social Science Research (OBSSR), and Nutrition Research (ONR) to the following investigators: RLL [Contact], DG, LM, MR (UH3-DK128302); MRL [Contact], KCA, MRH, SBR (UH3-DK128298); and SHB (U24-DK128125). Additional funding to support this study was provided to PVB (R01 HL159805), RLL, MD (P30 DK026687 Human Phenotyping Core, Molecular Biology Molecular Genetics Core), MR, MBBCh, MSCE (UL1TR001873 Clinical Research Resource; Bionutrition Unit), DG (T32 DK007559 in support of Giada Benasi, PhD and K26 DK138418), and AWF (Hunter Eastman Fellowship in Translational Research in support of Maxine Ashby-Thompson, EdD). RAF, PhD was partially supported by the US Department of Agriculture (USDA), under agreement No. 58-8050-9-004, by NIH Boston Claude D. Pepper Center (OAIC; 1P30AG031679) and SKD was supported by the USDA Agricultural Research Service Cooperative Agreement # 58-8050-9-004 and # 1950-51000-071-01S. Any opinions, findings, conclusions, or recommendations expressed in this publication are those of the authors and do not necessarily reflect the view of the USDA. The project described was supported by the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant 5-UL1-TR-001878-09. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Additional support was provided by the Robard Corporation, Mt Laurel, New Jersey, which supplied Numetra meal replacement products.
Author information
Authors and Affiliations
Consortia
Contributions
All authors (MR, KCA, MRL, KW, JMJ, LESM, MAT, MRH, JS, RLL, SKD, DG, SRB) participated in designing the protocol. MR and KCA were responsible for designing and preparing the manuscript and critically reviewing it prior to submission. Other authors (MRL, KW, JMJ, LESM, MAT, MRH, JS, RLL, SKD, DG, SRB) were responsible for reviewing the manuscript and providing edits.
Corresponding author
Ethics declarations
Competing interests
Any opinions, findings, conclusions, or recommendations expressed in this publication are those of the authors and are not to be construed as reflecting the views of the National Institutes of Health, Department of Health and Human Services or United States Department of Agriculture. MR has funding from Eli Lilly & Co. and is a paid consultant for Scholar Rock. KCA receives research funding from Novo Nordisk, which was not used in support of this work. ESM receives research funding from Eli Lilly & Co. KW reports partial funding from Eli Lilly & Company. JMJ is on the Scientific Advisory Board for Wondr Health, Inc. and his institution received research funding from Epitomee Medical, Inc. MRH receives research funding from Boehringer Ingelheim, Eli Lilly & Co., Gila Therapeutics, Pfizer Inc., and Novo Nordisk which was not used in support of these studies. RLL is a consultant to Coronation Bio, MBX Biosciences, and Eli Lilly & Co. SKD is supported by the USDA Agricultural Research Service Cooperative Agreement # 58-8050-9-004. SBR is a Board member of Danone and the founder of www.theidiet.com. MA-T, DG, MRL, and JS have no competing interests.
Ethics approval and consent to participate
The protocol and informed consent forms were approved by the single Institutional Review Board at the University of Pittsburgh (CR21120046-021). All participants will undergo informed consent prior to enrolling in the study described in this manuscript, and all methods will be performed in accordance with the Declaration of Helsinki.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rosenbaum, M., Allison, K.C., Laughlin, M.R. et al. The Physiology Of the WEight Reduced State (POWERS) study: assessing energy balance. Int J Obes (2025). https://doi.org/10.1038/s41366-025-01935-x
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41366-025-01935-x
This article is cited by
-
The Physiology Of the WEight Reduced State (POWERS) study: design and rationale for assessment of food intake, physical activity and other behavioral constructs
International Journal of Obesity (2026)
