
Abstract
Background
Candidates for metabolic bariatric surgery (MBS) experience significantly higher rates of mental disorders compared to the general population. While previous studies have primarily focused on a limited range of mental health conditions, this study expands the scope by studying a broader spectrum of psychopathological symptoms. Our aim was to map the psychopathological profile of candidates for MBS and to test whether individuals higher in general psychopathology exhibit a higher body mass index (BMI) and more severe eating disorder symptoms than those lower in general psychopathology.
Methods
A total of 222 candidates for MBS from the Dutch Obesity Clinic completed 16 questionnaires to generate a comprehensive psychopathological profile. Cluster analysis was applied to identify distinct groups based on general psychopathology. The clusters were compared on BMI and eating disorder psychopathology. A cross-sectional network approach was used to explore the complex interconnections between symptoms.
Results
Two clusters emerged: a high psychopathology profile (high PP; 29%) characterized by elevated scores on general psychopathology, and a low psychopathology profile (low PP; 71%) marked by healthier psychological functioning. The high PP cluster exhibited more severe eating disorder psychopathology than the low PP cluster, while the clusters did not differ in BMI. The symptom network revealed that general psychopathology is linked to eating disorder psychopathology through the bridge symptom ‘eating concerns.’
Conclusions
Approximately one-third of the individuals presenting for MBS exhibit elevated, transdiagnostic psychopathology with complex connections between symptoms. Notably, BMI was not associated with the severity of symptoms. The symptom network analysis highlights that ‘eating concerns’ serve as a crucial bridge linking eating disorder symptoms and symptoms of emotional disorders. Future research should focus on the transdiagnostic nature of psychopathology associated with obesity and investigate its potential impact on treatment outcomes, such as weight loss and quality of life.
Similar content being viewed by others


Introduction
Numbers of obesity and accompanying chronic diseases like diabetes, hypertension and cardiovascular diseases have been rising hand in hand to the point where 1 in 8 individuals worldwide are currently living with obesity [1, 2]. The probability of people with obesity achieving and maintaining a healthy body weight is low [3]. Lifestyle interventions for obesity are widely applied to bring about weight loss, however, weight loss is modest and the maintenance of lost weight is a huge challenge, with approximately 50% of patients returning to their initial weight 4–5 years after the intervention [4,5,6,7]. The rising prevalence of obesity paired with limited long-term success of current interventions has led to an increasing acceptance and utilization of metabolic bariatric surgery (MBS) for those with severe obesity. This surgical intervention shows to be considerably more effective in achieving long-term weight loss compared to non-surgical interventions and in reducing cardiovascular risk, hypertension, and increasing diabetes control or remission and quality of life [8,9,10,11].
It was documented that, next to medical comorbidities, candidates for MBS show significantly higher rates of mental problems than the general population [12, 13]. Prevalence rates of current mental disorders in candidates for MBS range from 21–56%: over 75% reports a history of any mental disorder (lifetime), which is considerably higher than the ~26% in the general population [12,13,14]. Specifically, depression (up to 31.5%) and anxiety (up to 24%) are frequently reported, followed by binge eating disorder (up to 23.3%), lifetime post-traumatic stress disorder (up to 11.8%), and lifetime substance abuse disorders (approximately 10%) [12,13,14,15,16,17,18,19,20,21,22].
These above-mentioned prevalence studies investigated the presence of mental disorders by using a diagnostic classification system such as the DSM, where mental disorders are conceptualized, measured and diagnosed as distinct constructs [23]. However, mental disorders are usually not present in isolation, at least 50% of the individuals with a mental disorder suffer from another comorbid mental disorder [24]. This indicates that symptoms of multiple mental disorders are present simultaneously, with complex interactions and interplay between the symptoms, e.g., a patient may report insomnia, leading to high levels of fatigue, followed by changes in appetite, evolving into a binge eating episode, which in its turn can lead to ruminating thoughts and feelings of guilt, eventually resulting in depression and dieting behaviors. Thus, mental disorders are not so clear-cut; a wide range of symptoms can interact with each other, activate, and maintain each other [24, 25]. Comorbidity of mental disorders also seems to be common in candidates for MBS [22, 26, 27].
In addition, studies investigating mental disorders in candidates for MBS usually assess a limited selection of disorders or symptoms (e.g., depressive disorder, binge eating disorder, body image) [28,29,30]. Because symptoms of obesity-related eating behaviors frequently co-occur with other forms of psychopathology, investigating transdiagnostic factors—such as loss of control over eating [31]—is essential to capture the role of comorbid symptoms. A more comprehensive approach in which a broad range of mental disorders and symptoms are analyzed may help embracing the complexity of mental health problems in a sample presenting for MBS. One way to investigate this complexity is to examine whether the sample can be divided into clusters based on psychological variables, which may help identify groups that share similar symptom profiles or levels of severity. These groups could then be monitored throughout their MBS trajectories, allowing for more targeted support in managing these difficulties, particularly given that the surgery itself might create a stressful period [32].
Some previous studies used cluster analysis based on psychological variables to discover subgroups in individuals with obesity (e.g., [26, 33,34,35,36]). Clusters based on personality were found, with one being more resilient and the other being more emotionally dysregulated [33]; clusters with high versus low severity of eating disorder symptoms [34]; clusters with high versus low psychological concerns [35]; and clusters with high versus low negative affect [36]. These studies help to recognize the interrelatedness of various psychopathological symptoms, but a broad assessment of transdiagnostic symptoms is still missing.
Another way to investigate this complexity is the use of network analyses. This type of analysis allows one to map out the connections between symptoms and to identify symptoms that play a central role in maintaining and exacerbating mental problems. To date, few network studies have been done in the context of MBS (e.g., [37,38,39]), making this a novel approach to studying psychological symptoms.
The current study examined a broad range of transdiagnostic and disorder-specific symptoms and traits in a sample presenting for MBS, to assess their comorbidity with obesity. To study the complex interplay between these symptoms, two types of analyses were performed. First, a cluster analysis revealed whether and how the sample could be divided into subgroups based on general psychopathology (i.e., self-esteem, depression, anxiety, stress, trauma, impulsivity, self-control, and dichotomous thinking). It was then studied whether these subgroups differ in body mass index (BMI) and eating disorder psychopathology (e.g., binge eating, body image, food addiction, emotional and external eating, dietary restraint). It is hypothesized that a cluster high in general psychopathology will be higher in BMI and eating disorder psychopathology, given the high rates of comorbidity among mental disorders. Secondly, it is hypothesized that symptoms of diverse mental disorders are connected with each other in a psychopathological profile. To study the connections between symptoms, we used a network analysis.
Methods
Participants and procedure
Participants (N = 222) were recruited in the Dutch Obesity Clinic South from March to October 2024. The clinic specializes in MBS combined with a comprehensive program of care before and after surgery performed by a multidisciplinary team. Those scheduled for the clinical screening to determine eligibility for surgery were invited by phone to participate in the current study. Participation took place before the clinical screening, meaning that candidates were not yet screened and selected for MBS. The sample therefore consists of candidates that still needed to be screened for surgery. Exclusion criteria were previous MBS and insufficient command of the Dutch language. After providing informed consent, the participants completed sixteen online questionnaires assessing general and eating disorder psychopathology. In addition, demographic information was collected, including age, gender, occupational situation, and the self-reported lifetime experience of mental disorders. BMI was retrieved from the electronic patient files of the obesity clinic. Ethical approval was received from the Ethics Review Committee Psychology and Neuroscience (ERCPN) of Maastricht University (OZL_245_156_11_2021_S1) and all methods were performed in accordance with the relevant guidelines and regulations. The study is pre-registered on AsPredicted (https://aspredicted.org/sftm-hzpc.pdf). Participants received a small monetary reward after completing the questionnaires. No formal sample size calculation was performed prior to the study. The sample size was determined by available participants.
Measures—psychopathological profile
An overview of the assessed symptoms and traits related to general psychopathology (i.e., self-esteem, anxiety, depression, stress, dichotomous thinking, trauma, impulsivity, and self-control) and eating disorder psychopathology (i.e., body image, food addiction, power of food, dietary restraint, emotional eating, external eating, night eating, loss of control over eating, large amount of food eaten, distress regarding binge eating, compensatory behaviors, eating-, weight-, and shape concerns, and global EDE-Q score) is shown in Table 1. Together, these variables comprise the psychopathological profile of the candidates. Higher scores refer to higher levels of the variable. The questionnaires were completed using the online platform Qualtrics (https://www.qualtrics.com). More information on the questionnaires is presented in Supplementary 1.
Statistical analyses
Descriptives
First, descriptive statistics were performed to describe the scores on all variables.
Cluster analysis
To test the first hypothesis, the cluster analysis was done with a pre-determined set of all variables related to general psychopathology, i.e., nine variables) (see overview in Table 1). Before performing the cluster analysis, the clustering tendency of the data was checked with a principal component analysis and the Hopkins statistic. Then, hierarchical K-means clustering was performed on the standardized scores of the variables to identify psychopathological profiles. This method was performed using the practical guide of Kassambara [40], with the factoextra package (version 1.0.7) [41] and the cluster package (version 2.1.4) [42]. A detailed description of the steps in this cluster analysis can be found in Supplementary 2. Finally, a two-cluster solution was chosen. To internally validate the two clusters, the mean levels of the cluster variables were compared, using Wilcoxon rank-sum tests with Bonferroni correction and Cliff Delta to demonstrate effect sizes. These tests were also used to test the hypothesis that a cluster high in general psychopathology has a higher BMI and more eating disorder psychopathology. A non-parametric version was used due to non-normality of the data and unequal variances between the clusters. For categorical variables Fisher’s Exact Test was used.
Network analysis
A transdiagnostic symptom network was created to visualize the partial correlations between symptoms. The symptoms in psychopathology networks are referred to as ‘nodes’ and the connections between them as ‘edges’—these edges (partial correlations) statistically control for connections with all other nodes in the network. In addition to theoretical considerations, the goldbricker function was used to reduce the number of nodes (networktools package, version 1.5.0) [43]. Goldbricker generates a list of node pairs that are colinear, meaning that they most likely measure the same underlying construct. The starting point were the 28 variables presented in Table 1 (excluding experienced burden of trauma and global EDE-Q score). The high and moderate redundancy pairs were reviewed and 11 nodes were removed, according to if they returned in multiple pairs. The goldbricker function was performed a second time on the remaining nodes, with only one redundant pair as output of which 1 node was removed. This resulted in 16 nodes, and 4 final nodes were removed based on theoretical considerations, i.e., nodes measuring the same construct (self-control and impulsivity, restraint measured by DEBQ and EDE-Q, body image avoidance and body image satisfaction) and compensatory behaviors because of the low prevalence. The network was then estimated with the remaining 12 nodes by a Gaussian graphical model (GGM) using the qgraph package (version 1.9.5) [44]. To control for spurious edges in the network, the EBICglasso argument in GGM was used [45]. To determine the importance of a node in the network, strength centrality was calculated using the centrality function in qgraph. More information on the accuracy and stability of the network is provided in Supplementary 2.
Results
Descriptive statistics of the sample
Participants (N = 222; n = 161 female, 73%) had a mean age of 44 years (SD = 13, min = 18, max = 80) and a mean BMI of 42.33 kg/m2 (SD = 5.65, min 32.50, max = 63.57). They had full time (n = 64; 29%), part time (n = 72; 33%), or no (n = 85; 38%) paid work. Of the whole sample, 22% reported to be diagnosed with a mental disorder ever in their life (n = 49). The mean (SD) scores on all variables included in the psychopathological profile can be found in Table 1 (Supplementary 1 provides information on scoring and cut-off/norm scores). Mean scores on general psychopathology (e.g., self-esteem, anxiety, depression, stress) were in the healthy range while mean scores on specific eating disorder psychopathology were high (e.g., weight and shape concerns, global EDE-Q score, and body image). See also Table S1 (Supplementary 3) for the frequencies of food addiction, binge eating, and bulimia nervosa.
Clustering based on general psychopathology
Psychopathological profiles
The hierarchical K-means cluster analysis revealed a two-cluster solution that fitted the data best, meaning the candidates could be divided in two different psychopathological profiles: a High Psychopathology Profile (high PP) and a Low Psychopathology Profile (low PP). The standardized means of the cluster variables for both clusters are shown in Fig. 1 (the non-standardized means and standard deviations can be found in Table 2). The high PP cluster (n = 64, 29%, red line) is characterized by relatively high scores on anxiety, depression (BDI and DASS), dichotomous thinking, impulsivity, stress and trauma, while their scores on self-control and self-esteem are low. The low PP cluster (n = 158, 71%, blue line) shows the opposite pattern. The high PP cluster is characterized by severe anxiety and depression scores, a low self-esteem, and moderate stress levels. The low PP cluster shows healthy scores. The self-reported lifetime prevalence of mental disorders was significantly higher in the high PP cluster (39%) than the low PP cluster (15%) (see Table S2 in Supplementary 3). The Wilcoxon rank-sum tests show that all cluster variables were significantly different between the two clusters (see Table 2), demonstrating high internal validity.

Cluster 1 = high PP (n = 64), Cluster 2 = low PP (n = 158).
Hypothesis testing: the high PP cluster is characterized by significantly more eating disorder psychopathology and a higher BMI
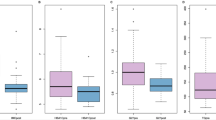
In line with the hypothesis, the high PP cluster showed significantly higher eating disorder psychopathology than the low PP cluster. More specifically the high PP cluster scored higher on body image dissatisfaction, weight and shape concerns, emotional and external eating, eating concerns, and the high PP cluster showed more symptoms of food addiction and binge eating (large amount of food eaten, loss of control over eating, distress regarding binge eating) than the low PP cluster (see Table 3). Binge eating (present if all three binge eating symptoms were scored with 2 or higher) and food addiction (present if two or more food addiction symptoms plus clinical significance was present) were also more present in the high PP cluster (respectively 50% and 39%) compared to the low PP cluster (respectively 16% and 7%) (see Table S2 in Supplementary 3). Interestingly, and contrary to our hypothesis, no differences in BMI were found between the high PP and low PP cluster (see Table 3). It should be noted that, though the high PP cluster showed significantly more eating disorder psychopathology than the low PP cluster, the low PP cluster was characterized by eating disorder psychopathology as well: in particular weight and shape concerns, external eating, and body image dissatisfaction were increased in the low PP cluster (see Table 3) compared to the norm scores (see Supplementary 1).
Complex connections between symptoms in the network
The symptom network with its unique connections between symptoms is shown in Fig. 2. Strength centrality indices are plotted in Fig. 3. The network shows general psychopathology nodes (depression, anxiety, traumatic experiences, self-esteem) connected to eating disorder psychopathology nodes (emotional eating, external eating, loss of control over eating) and self-control. The general psychopathology and eating disorder pathology nodes are connected to each other via the central node eating concerns (strength centrality = 1.08). So, eating concerns function as a bridge symptom between specific eating disorder psychopathology and general psychopathology in this network. Besides eating concerns, depression (strength centrality = 1.48) and loss of control over eating (strength centrality = 1.04) are also central in the network: they have the most direct connections with other nodes and in particular depression is strongly connected to other nodes in the network. The weights of edges (Table S3, Supplementary 3) show the strength of connections; emotional eating and external eating have the highest edge weight (r = 0.44), followed by depression and anxiety (r = 0.39), depression and self-esteem (r = −0.33), weight concerns and eating concerns (r = 0.29), and loss of control over eating and eating concerns (r = 0.29). These nodes are most strongly connected to each other. Results on the accuracy and stability of the network are shown in Figs. S1–S4 in Supplementary 3. Overall, the edge estimates were quite accurate (rather wide distributions) and strength centrality remained quite stable while dropping a large proportion of people from the dataset.

The figure shows the LASSO-regularized partial correlation network with a minimum edge weight of 0.15. Blue edges indicate positive partial correlations and red edges indicate negative partial correlations. Thicker edges reflect stronger partial correlations between the nodes. Tra traumatic experiences (TEC), Dep depression (BDI), Anx anxiety (DASS), SE self-esteem (RSE), EC eating concerns (EDE-Q), LOC loss of control over eating (SED), EE emotional eating (DEBQ), EX external eating (DEBQ), SC self-control (BSCS), Res dietary restraint (DEBQ), WC weight concerns (EDE-Q), BI body image satisfaction (BISS).

Values towards the right reflect higher strength centrality.
Discussion
The present study investigated a diverse range of transdiagnostic psychopathological symptoms in candidates for MBS, more specifically it was tested if symptom severity clusters could be distinguished and how symptoms are uniquely connected to each other. While the average scores on general psychopathology scales for the whole group are rather healthy, one-third of the candidates for MBS experiences clinically relevant psychopathology in multiple areas. The high PP subgroup (29%) is characterized by significantly more general psychopathology and significantly more eating disorder psychopathology than the low PP subgroup (71%). Thus, if the focus is on the group average, as is usually the case, it goes unnoticed that a significant proportion of the group is characterized by clinically relevant psychopathology; they exhibit not only eating disorder symptoms but a wide range of psychological complaints and symptoms. Furthermore, transdiagnostic symptoms were characterized by complex connections. In the network, general psychopathology symptoms were bridged to eating disorder psychopathology via eating concerns. The combination of these two methods provides both understanding of the profiles (cluster analysis) picturing how symptoms co-occur within individuals, as well as insight into the connections between symptoms (network analysis) that clarifies whether symptoms are associated with other symptoms.
Our hypothesis that the cluster high in general psychopathology would show more eating disorder psychopathology was confirmed. Nevertheless, despite being clustered as low psychopathology and showing significantly less eating disorder psychopathology than the high PP cluster, the low PP cluster scored above healthy norm scores on eating disorder psychopathology. Thus, the entire sample shows elevated levels of eating disorder psychopathology, while eating disorder psychopathology is more severe in one-third of the sample and this subsample also shows significantly more symptoms of general psychopathology. Interestingly, BMI did not differ between the two clusters. This is in line with two other studies finding no BMI differences between clusters based on psychological constructs [35, 36]. While BMI did not differ between the clusters, body-related worrying was found to be significantly stronger in a high negative affect cluster compared to a low negative affect cluster [36], and another study also did not find BMI differences between three clusters (a low and a high psychological concerns cluster, and a cluster high in bodily concerns) [35]. So although the clusters had similar BMIs, their concerns about weight, shape, and eating differed significantly. These findings show that psychopathological symptoms in people with obesity are not associated with a person’s actual body weight, but rather with how badly a person feels about their weight.
The finding that symptoms of multiple mental disorders were present in this sample is also reflected by the complex connections between the nodes in the cross-sectional network. Here, worrying about eating and food served as a bridge to general psychopathology, thereby demonstrating that different domains of psychopathology are not totally different disorders or loosely coupled systems, but are all interconnected.
Although half of the candidates in the high PP cluster reported binge eating (16% in low PP), 39% reported food addiction (7% in low PP), and 39% reported lifetime mental disorders (15% in low PP), it is not clear whether pre-surgery psychopathology will affect surgery outcomes. Several meta-analyses did not find pre-surgery mental or behavioral predictors for weight loss [46,47,48]. Apart from weight loss, it seems beneficial to monitor candidates’ psychopathology symptoms on the long term. It was shown that anxiety, depression and eating disorder symptoms that were present before surgery tend to reduce shortly after surgery, but these symptoms may recur over time [32, 49]. So, it seems wise to make mental health services available throughout the remainder of the candidate’s trajectory. More intensive psychological assessment and monitoring throughout the trajectory could be particularly important for the high PP cluster, as this cluster experiences difficulties in multiple psychological areas [50, 51].
The current transdiagnostic consideration of the psychopathological profiles of candidates for MBS shows complex interactions between symptoms in the symptom network. Such networks are useful to show the unique connections between certain symptoms of different mental disorders, presented in one transdiagnostic framework. The connections in the cross-sectional network are unique because they are partial correlations and they are robust because the used regularization techniques while estimating the network, i.e., graphical LASSO in the current study, limits the number of very weak connections [52]. The presented network thus only shows robust unique connections, in line with the few previous studies that have estimated cross-sectional networks in samples of patients undergoing MBS [37,38,39]. These studies likewise link eating behaviors to psychological symptoms. For example, one study showed that emotion dysregulation plays an important role in the link between pathological eating styles and psychopathological traits [37], comparable to the central role of eating concerns in the current study. The network approach to psychopathology is a recent development in clinical psychology that does not have the disadvantages of diagnostic classification systems and does justice to the high prevalence of comorbidity [24]. Its core assumption is that the complex system of symptoms constitutes the mental disorder, which contrasts the common view of these symptoms being indicative of underlying disorder(s) [25]. By investigating a broad set of relevant symptoms and traits, relevant to the individual, symptom networks of people with obesity can precisely map a person’s mental problems, which can then lead to personalized network-informed treatment. This study represents a first step in mapping a broad psychopathological profile of candidates for MBS, exploring connections between symptoms through cluster and network analyses, with the aim of informing which patients may benefit from additional treatment and monitoring throughout the MBS trajectory. Future research may consider ecological momentary assessments (EMA) to also map the dynamics of complex symptom interactions within the transdiagnostic networks. EMA means that the person assesses a set of questions several times throughout the day at random times and during several weeks. EMA data enable the construction of idiosyncratic dynamic networks and inferences on causality between symptoms. Such an understanding of individual networks paves the way for new personalized network-based interventions (see [24]).
A limitation in the current study and in many other studies on psychopathology in candidates for MBS, is the assessment of psychopathology using questionnaires. Even when questionnaires are well validated and reliable self-reports, they are insufficient to diagnose. Good mental disorder diagnostics require valid diagnostic interviews. Diagnostic interviews conducted by professional experts can also reduce the risk of ‘faking good’, which is a strategy to underreport pre-operative psychopathological symptoms during the clinical screening, to increase the chance of being accepted for surgery (e.g., [53]). Moreover, while the current study already includes a broad set of symptoms, other important domains such as substance use and behavioral addictions could be relevant as well and may be considered in future research.
To conclude, the present findings indicate that one-third of the people presenting for MBS shows elevated psychopathology in several domains. Their psychopathological profile is complex; the symptoms are transdiagnostic, meaning that they not only suffer from elevated eating disorder psychopathology but also from emotional disorders like depression, anxiety and post-traumatic stress. Interestingly, BMI was not associated with transdiagnostic symptom severity. The network analysis shows that the symptoms are connected in a complex way, and that elevated eating concerns function as a bridge between eating disorder symptoms and emotional disorder symptoms. The transdiagnostic and dynamic nature of symptoms deserves more research in the future to better map the complexity of the psychopathological profile, as well as whether the presence of these psychopathological symptoms influences weight loss and quality of life after surgery.
Data availability
The dataset generated during and/or analyzed during the current study is available from the NSMD management team after completion of the entire project and on reasonable request.
Code availability
No custom computer code was used to generate the results. All analyses were performed in R (version 2024.04.2 + 764) [54] using the publicly available packages following published tutorials, mentioned above.
References
Boutari C, Mantzoros CS. A 2022 update on the epidemiology of obesity and a call to action: as its twin COVID-19 pandemic appears to be receding, the obesity and dysmetabolism pandemic continues to rage on. Metabolism. 2022;133:155217. https://doi.org/10.1016/j.metabol.2022.155217.
World Health Organization. Obesity and overweight. World Health Organization; 2024. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
Fildes A, Charlton J, Rudisill C, Littlejohns P, Prevost AT, Gulliford MC. Probability of an obese person attaining normal body weight: cohort study using electronic health records. Am J Public Health. 2015;105:e54–9. https://doi.org/10.2105/ajph.2015.302773.
Butryn ML, Webb V, Wadden TA. Behavioral treatment of obesity. Psychiatr Clin North Am. 2011;34:841–59. https://doi.org/10.1016/j.psc.2011.08.006.
Fothergill E, Guo J, Howard L, Kerns JC, Knuth ND, Brychta R, et al. Persistent metabolic adaptation 6 years after “The Biggest Loser” competition. Obesity. 2016;24:1612–9. https://doi.org/10.1002/oby.21538.
Kheniser K, Saxon DR, Kashyap SR. Long-term weight loss strategies for obesity. J Clin Endocrinol Metab. 2021;106:1854–66. https://doi.org/10.1210/clinem/dgab091.
Webb VL, Wadden TA. Intensive lifestyle intervention for obesity: principles, practices, and results. Gastroenterology. 2017;152:1752–64. https://doi.org/10.1053/j.gastro.2017.01.045.
Pipek LZ, Moraes WAF, Nobetani RM, Cortez VS, Condi AS, Taba JV, et al. Surgery is associated with better long-term outcomes than pharmacological treatment for obesity: a systematic review and meta-analysis. Sci Rep. 2024;14. https://doi.org/10.1038/s41598-024-57724-5.
Abhishek F, Ogunkoya GD, Gugnani JS, Kaur H, Muskawad S, Singh M, et al. Comparative analysis of bariatric surgery and non-surgical therapies: impact on obesity-related comorbidities. Cureus. 2024;16. https://doi.org/10.7759/cureus.69653.
Zhou X, Zeng C. Diabetes remission of bariatric surgery and nonsurgical treatments in type 2 diabetes patients who failure to meet the criteria for surgery: a systematic review and meta-analysis. BMC Endocr Disord. 2023;23. https://doi.org/10.1186/s12902-023-01283-9.
Konttinen H, Sjöholm K, Carlsson LMS, Peltonen M, Svensson PA. Fifteen-year changes in health-related quality of life after bariatric surgery and non-surgical obesity treatment. Int J Obes. 2024;48:1447–56. https://doi.org/10.1038/s41366-024-01572-w.
Malik S, Mitchell JE, Engel S, Crosby R, Wonderlich S. Psychopathology in bariatric surgery candidates: a review of studies using structured diagnostic interviews. Compr Psychiatry. 2014;55:248–59. https://doi.org/10.1016/j.comppsych.2013.08.021.
Sarwer DB, Heinberg LJ. A review of the psychosocial aspects of clinically severe obesity and bariatric surgery. Am Psychol. 2020;75:252–64. https://doi.org/10.1037/amp0000550.
Sarwer DB, Wadden TA, Ashare RL, Spitzer JC, McCuen-Wurst C, LaGrotte C, et al. Psychopathology, disordered eating, and impulsivity in patients seeking bariatric surgery. Surg Obes Relat Dis. 2021;17:516–24. https://doi.org/10.1016/j.soard.2020.11.005.
Barbuti M, Brancati GE, Calderone A, Fierabracci P, Salvetti G, Weiss F, et al. Prevalence of mood, panic and eating disorders in obese patients referred to bariatric surgery: patterns of comorbidity and relationship with body mass index. Eat Weight Disord. 2021;27:1021–7. https://doi.org/10.1007/s40519-021-01236-y.
Bianciardi E, Gentileschi P, Niolu C, Innamorati M, Fabbricatore M, Contini LM, et al. Assessing psychopathology in bariatric surgery candidates: discriminant validity of the SCL-90-R and SCL-K-9 in a large sample of patients. Eat Weight Disord. 2020;26:2211–8. https://doi.org/10.1007/s40519-020-01068-2.
Duarte-Guerra LS, Coêlho BM, Santo MA, Wang Y. Psychiatric disorders among obese patients seeking bariatric surgery: results of structured clinical interviews. Obes Surg. 2014;25:830–7. https://doi.org/10.1007/s11695-014-1464-y.
Kalarchian MA, Marcus MD, Levine MD, Soulakova JN, Courcoulas AP, Wisinski MS. Relationship of psychiatric disorders to 6-month outcomes after gastric bypass. Surg Obes Relat Dis. 2008;4:544–9. https://doi.org/10.1016/j.soard.2008.03.003.
Mauri M, Rucci P, Calderone A, Santini F, Oppo A, Romano A, et al. Axis I and II disorders and quality of life in bariatric surgery candidates. J Clin Psychiatry. 2008;69:295–301. https://doi.org/10.4088/jcp.v69n0216.
Mitchell JE, Selzer F, Kalarchian MA, Devlin MJ, Strain GW, Elder KA, et al. Psychopathology before surgery in the Longitudinal Assessment of Bariatric Surgery-3 (LABS-3) Psychosocial Study. Surg Obes Relat Dis. 2012;8:533–41. https://doi.org/10.1016/j.soard.2012.07.001.
Mühlhans B, Horbach T, De Zwaan M. Psychiatric disorders in bariatric surgery candidates: a review of the literature and results of a German prebariatric surgery sample. Gen Hosp Psychiatry. 2009;31:414–21. https://doi.org/10.1016/j.genhosppsych.2009.05.004.
Rosenberger PH, Henderson KE, Grilo CM. Psychiatric disorder comorbidity and association with eating disorders in bariatric surgery patients: a cross-sectional study using structured interview-based diagnosis. J Clin Psychiatry. 2006;67:1080–5. https://doi.org/10.4088/jcp.v67n0710.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Washington, DC: American Psychiatric Association Publishing; 2013; https://psychiatryonline.org/doi/book/10.1176/appi.books.9780890425596.
Roefs A, Fried EI, Kindt M, Martijn C, Elzinga B, Evers AW, et al. A new science of mental disorders: using personalised, transdiagnostic, dynamical systems to understand, model, diagnose and treat psychopathology. Behav Res Ther. 2022;153:104096. https://doi.org/10.1016/j.brat.2022.104096.
Borsboom D. A network theory of mental disorders. World Psychiatry. 2017;16:5–13. https://doi.org/10.1002/wps.20375.
Da Silva VB, Da Silva RB, Prud’homme A, Campan P, Azorin JM, Belzeaux R. Association between binge eating disorder and psychiatric comorbidity profiles in patients with obesity seeking bariatric surgery. Compr Psychiatry. 2018;87:79–83. https://doi.org/10.1016/j.comppsych.2018.09.004.
Jones-Comeille LR, Wadden TA, Sarwer DB, Faulconbridge LF, Fabricatore AN, Stack RM, et al. Axis I psychopathology in bariatric surgery candidates with and without binge eating disorder. Results of structured clinical interviews. Obes Surg. 2012;22:389–97. https://doi.org/10.1007/s11695-010-0322-9.
Fabrig A, Schmidt R, Mansfeld T, Sander J, Seyfried F, Kaiser S, et al. Depressive symptoms among bariatric surgery candidates: associations with stigmatization and weight and shape concern. Nutrients. 2024;16:510. https://doi.org/10.3390/nu16040510.
Gaudrat B, Andrieux S, Florent V, Rousseau A. Psychological characteristics of patients seeking bariatric treatment versus those seeking medical treatment for obesity: is bariatric surgery a last best hope? Eat Weight Disord. 2020;26:949–61. https://doi.org/10.1007/s40519-020-00934-3.
Geller S, Levy S, Hyman O, Jenkins PL, Abu-Abeid S, Goldzweig G. Body image, emotional eating and psychological distress among bariatric surgery candidates in Israel and the United States. Nutrients. 2020;12:490. https://doi.org/10.3390/nu12020490.
Catania J, Spirou D, Gascoigne M, Raman J. Loss of control as a transdiagnostic feature in obesity-related eating behaviours: a systematic review. Eur Eat Disord Rev. 2022;31:24–45. https://doi.org/10.1002/erv.2936.
Spirou D, Raman J, Smith E. Psychological outcomes following surgical and endoscopic bariatric procedures: a systematic review. Obes Rev. 2020;21:1–24. https://doi.org/10.1111/obr.12998.
Claes L, Vandereycken W, Vandeputte A, Braet C. Personality subtypes in female pre-bariatric obese patients: do they differ in eating disorder symptoms, psychological complaints and coping behaviour? Eur Eat Disord Rev. 2012;21:72–7. https://doi.org/10.1002/erv.2188.
Rodolico A, La Rosa VL, Romaniello C, Concerto C, Meo V, Saitta G, et al. Personality dimensions, depression, and eating behavior in individuals seeking bariatric surgery, a cluster analysis. Front Nutr. 2024;11:1429906. https://doi.org/10.3389/fnut.2024.1429906.
Plasonja N, Brytek-Matera A, Décamps G. Psychological profiles of treatment-seeking adults with overweight and obesity: a cluster analysis approach. J Clin Med. 2022;11:1952. https://doi.org/10.3390/jcm11071952.
Jansen A, Havermans R, Nederkoorn C, Roefs A. Jolly fat or sad fat?. Appetite. 2011;57:635–40. https://doi.org/10.1016/j.appet.2008.05.055.
Belloli A, Saccaro LF, Landi P, Spera M, Zappa MA, Dell’Osso B, et al. Emotion dysregulation links pathological eating styles and psychopathological traits in bariatric surgery candidates. Front Psychiatry. 2024;15. https://doi.org/10.3389/fpsyt.2024.1369720.
Monteleone AM, Cascino G, Solmi M, Pirozzi R, Tolone S, Terracciano G, et al. A network analysis of psychological, personality and eating characteristics of people seeking bariatric surgery: Identification of key variables and their prognostic value. J Psychosom Res. 2019;120:81–9. https://doi.org/10.1016/j.jpsychores.2019.03.010.
Monteleone AM, Globus I, Cascino G, Klomek AB, Latzer Y. Psychopathology predicts mental but not physical bariatric surgery outcome at 3-year follow-up: a network analysis study. Eat Weight Disord. 2022;27:3331–40. https://doi.org/10.1007/s40519-022-01463-x.
Kassambara A. Practical guide to cluster analysis in R: unsupervised machine learning. STHDA. 2017:1–187. https://xsliulab.github.io/Workshop/2021/week10/r-cluster-book.pdf.
Kassambara A, Mundt F. factoextra: extract and visualize the results of multivariate data analyses [R package version 1.0.7]. 2020. https://cran.r-project.org/web/packages/factoextra/index.html.
Maechler M, Rousseeuw P, Struyf A, Hubert M, Hornik K. cluster: cluster analysis basics and extensions [R package version 2.1.4]. 2022. https://cran.r-project.org/web/packages/cluster/index.html.
Jones P. networktools: tools for identifying important nodes in networks [R package version 1.5.0]. 2022. https://CRAN.R-project.org/package=networktools.
Epskamp S, Cramer AOJ, Waldorp LJ, Schmittmann VD, Borsboom D. qgraph: network visualizations of relationships in psychometric data. J Stat Softw. 2012;48. https://doi.org/10.18637/jss.v048.i04.
Friedman J, Hastie T, Tibshirani R. glasso: graphical lasso: estimation of Gaussian graphical models [R package]. 2022. https://doi.org/10.32614/cran.package.glasso.
Jacobs A, Monpellier VM, Torensma B, Antoniou EE, Janssen IMC, Tollenaar RAEM, et al. Influence of mental and behavioral factors on weight loss after bariatric surgery: a systematic review and meta-analysis. Obes Rev. 2024;25. https://doi.org/10.1111/obr.13729.
Livhits M, Mercado C, Yermilov L, Parikh JA, Dutson E, Mehran A, et al. Preoperative predictors of weight loss following bariatric surgery. Obes Surg. 2012;22:951–8. https://doi.org/10.1007/s11695-011-0472-4.
Mauro MFF, Papelbaum M, Brasil MAA, Carneiro JR, Coutinho ESFC, Coutinho W, et al. Is weight regain after bariatric surgery associated with psychiatric comorbidity? A systematic review and meta-analysis. Obes Rev. 2019;20:1413–25. https://doi.org/10.1111/obr.12907.
Freire CC, Zanella MT, Segal A, Arasaki CH, Matos MIR, Carneiro G. Associations between binge eating, depressive symptoms and anxiety and weight regain after Roux-en-Y gastric bypass surgery. Eat Weight Disord. 2020;26:191–9. https://doi.org/10.1007/s40519-019-00839-w.
Rutledge T, Ellison JK, Phillips AS. Revising the bariatric psychological evaluation to improve clinical and research utility. J Behav Med. 2020;43:660–5. https://doi.org/10.1007/s10865-019-00060-1.
Sogg S, Lauretti J, West-Smith L. Recommendations for the presurgical psychosocial evaluation of bariatric surgery patients. Surg Obes Relat Dis. 2016;12:731–49. https://doi.org/10.1016/j.soard.2016.02.008.
Epskamp S, Fried EI. A tutorial on regularized partial correlation networks. Psychol Methods. 2018;23:617–34. https://eiko-fried.com/wp-content/uploads/Epskamp-Fried-2018-Tutorial-partial-corr.pdf.
Butt M, Wagner A, Rigby A. Associations of social desirability on psychological assessment outcomes for surgical weight loss patients. J Clin Psychol Med Settings. 2020;28:384–93. https://doi.org/10.1007/s10880-020-09725-5.
R Core Team. R: a language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; 2016. https://www.r-project.org/.
Acknowledgements
This study is part of the project ‘New Science of Mental Disorders’ (www.nsmd.eu), supported by the Dutch Research Council and the Dutch Ministry of Education, Culture and Science (NWO gravitation grant number 024.004.016). In addition, the study is financially supported by the Dutch Obesity Clinic. We would like to thank the Dutch Obesity Clinic in Heerlen for their support and the student assistant Aline Schellekens for her contributions to the recruitment of the participants.
Author information
Authors and Affiliations
Contributions
MD and AJ initially designed the study with contributions from EB. MD conducted the data collection and analysis, with contributions from JB for the network analysis. MD and AJ contributed to the interpretation of the findings. MD drafted the manuscript with contributions and revisions from AJ. EB, LL, CM, JB, MD, and AJ revised the final manuscript. MD and AJ had full access to the dataset. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Dix, M.H.C., Boerma, EJ.G., Martijn, C. et al. The psychopathological profile of candidates for metabolic bariatric surgery: a transdiagnostic and network approach. Int J Obes 50, 907–915 (2026). https://doi.org/10.1038/s41366-026-02023-4
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41366-026-02023-4
