
Abstract
Background
Previous studies have not typically separated body mass index (BMI) slope and variability as distinct constructs when examining dementia risk. This study assessed the association between the slope-adjusted visit-to-visit BMI variability and dementia risk.
Subjects/methods
We conducted a retrospective cohort study using Japanese national health insurance data (2015–2023) of individuals aged 50–74 years who underwent five annual health checkups. BMI variability was assessed using the slope-adjusted standard deviation (SD) to account for underlying temporal trends. The proxy outcome for dementia was antidementia drug initiation, analyzed using Fine-Gray competing risk models, accounting for death as a competing risk.
Results
During the mean 2.17 ± 1.19 years of follow-up among 303,042 participants (mean age: 66.6 years, men: 38.6%), antidementia drugs (predominantly donepezil: 67.4%) were initiated in 665 and 2394 died. After adjusting for covariates including BMI at baseline and annual BMI change, the highest tertile of slope-adjusted BMI-SD (≥0.50 kg/m²) was significantly associated with increased dementia risk compared with the lowest tertile (≤0.31 kg/m²). Annual BMI change showed a U-shaped association with dementia risk, with pronounced elevation in the first tertile (BMI decline ≤−0.31%, hazard ratio: 1.60, 95% confidence interval: 1.32–1.93). In the basic model including baseline covariates except BMI at baseline, there was no significant difference in the C-statistics improvements when BMI at baseline or adding slope-adjusted BMI-SD (+0.0147 vs +0.0146) were added, while the greatest C-statistics improvement was observed when BMI decline ≤−0.31% was added. The association between the highest slope-adjusted BMI-SD tertile and dementia risk was stronger in females than males (P for interaction = 0.0039).
Conclusions
Slope-adjusted visit-to-visit BMI variability is independently associated with dementia risk, particularly among females, while BMI decline patterns are strong risk factors of dementia. Incorporating longitudinal monitoring of visit-to-visit BMI variability into routine dementia screening may be beneficial.

Similar content being viewed by others


Introduction
Dementia has rapidly become a global public health concern. The prevalence of dementia has been estimated to increase from 57 million in 2019 to 153 million by 2050 worldwide [1]. To mitigate its societal and economic burden, early prediction through timely behavioral and clinical intervention is crucial.
Body mass index (BMI), particularly low BMI, is associated with a high risk of dementia [2]. Since weight loss has also been reported as a risk factor for dementia [2,3,4,5,6,7,8,9,10,11], measuring long-term trends in BMI may be crucial for precise dementia risk prediction. Furthermore, within-person variability in weight or BMI has more recently been linked to cognitive decline and dementia risk [7, 12,13,14,15,16,17]. Worse glucose tolerance, inflammation, and metabolic factors are considered to be possible mediators contributing to this association [18,19,20,21,22]. However, traditional variability indices that rely on standard deviation (SD), including the coefficient of variation, have computational limitations. These metrics inherently produce higher variability estimates for individuals with steeper slopes, even if the trends are stable. This results in artificially elevated variability measures in individuals with pronounced slopes. The variability indices should preferably be adjusted by the corresponding slope to rigorously explore the effect of variability on differential risk. Despite this problem, previous studies have not considered slope in their analysis of variability measures [7, 12,13,14,15,16,17]. Another issue in these studies could be the number of measurement points because they mainly included individuals who underwent measurement only three times [7, 12,13,14,15,16,17]. With such a small number of observations, the calculated variability may largely reflect measurement error or random fluctuations rather than true biological variation, raising questions regarding the validity of these variability estimates.
Given these considerations, the present study aimed to assess the association between slope-adjusted visit-to-visit variability in BMI and the risk of dementia using annually measured data recorded at the five time points from Asian health check-up and claims data. By examining the predictive ability of other indices, including the latest BMI values and slopes, we explored whether measuring visit-to-visit BMI variability provided additional practical benefits for dementia prediction.
Methods
Study design and population
This retrospective cohort study used the data from 2015 to 2023 from insurer-based databases provided by DeSC Healthcare Inc. (Tokyo, Japan). The DeSC National Health Insurance (NHI) database includes health checkups and claims data from self-employed individuals, unemployed individuals, or farmers aged <75 years [23,24,25]. When individuals reach the age of 75 years, all insured individuals are forced to switch their insurance to the “Later-Stage Elderly Healthcare System” in Japan; the follow-up is discontinued at this point due to the change in insurance identification number. The claims database includes data on all inpatient, outpatient, and pharmacy claims received by the insurers. This study was approved by the Research Ethics Committee for Life Science and Medical Research of Tohoku Medical and Pharmaceutical University, and the requirement for informed consent was waived because all data were fully de-identified before analysis (approval ID: 2024-2-015) [26]. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [27] and were performed in accordance with the Declaration of Helsinki.
The study design is outlined in Supplementary Fig. S1. We used five annual health checkups (Visits 1–5) to define BMI variability. Visit 5, i.e., the last checkup, was defined as the baseline.
Participant selection
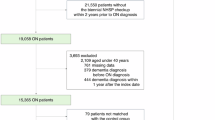
The participant selection process is illustrated in Fig. 1. Data were available for 1,638,474 individuals. To consider the outcome of death as a competing risk, 444,682 patients whose death information was not available were excluded. Additionally, 855,645 individuals without data from the five available annual health checkups to define visit-to-visit BMI variability were excluded. Of the remaining 338,147 individuals, individuals with intervals longer than eight years between the initial and final health examinations, those with a history of dementia-related diagnostic codes, those with a history of antidementia medication prescription, those with a history of cardiovascular diseases (from the health examination questionnaire) at baseline, and those with a follow-up period of less than 30 days were further excluded. To eliminate the effects of outliers, individuals with extreme BMI values outside the 0.1–99.9 percentile range were excluded. Finally, data from 303,042 individuals were analyzed. This observational study included all available eligible participants; no a priori sample size calculation was performed.

BMI body mass index.
Baseline data
All health checkups in Japan are encouraged to be performed under the guidelines of the Japanese Ministry of Health, Labour, and Welfare [28]. Body mass index was calculated as weight in kilograms divided by height in meters squared (kg/m²). Blood and urine samples were collected at the same time as the other examination. Blood pressure (BP), hemoglobin A1c (HbA1c) level, low-density lipoprotein cholesterol (LDL) level, and proteinuria by dipstick test, which are commonly measured for detecting metabolic syndrome in Japan, were used as covariates. Information on smoking status, alcohol consumption, and history of cardiovascular disease were collected using a questionnaire at each health checkup.
The use of lipid-lowering (World Health Organization Anatomical Therapeutic Chemical [WHO-ATC] code: C10), antidiabetic (ATC code: A10), and antihypertensive medications (ATC code: C02CA, C02A, C03AA, C03BA, C03CA01, C03DA, C03DB, C08CA, C08DB, C09, C07A, C02DB, G04CA03) was confirmed using claims data from within 365 days before the baseline (Detailed codes are shown elsewhere [29, 30]).
Visit-to-visit BMI variability indices
As the primary measure of visit-to-visit BMI variability, the slope-adjusted BMI-SD was calculated as the SD of residuals derived from individual linear regression analyses, eliminating the influence of underlying temporal trends from the variability estimates (Supplementary Fig. S2). This approach addresses the computational limitation in which traditional SD-based metrics artificially inflate the variability in individuals with steeper BMI trajectories. Additional variability indices included the coefficient of variation (CV), average real variability (ARV), and the maximum minus minimum difference (MMD). Visit-to-visit percentage changes were calculated as the percentage difference between consecutive measurement points (i.e., the relative change from one visit to the next immediate visit). As CV values are influenced by both positive and negative slope values, the absolute values of the annual BMI change (|BMI annual change|) were used for the slope analyses.
The variability indices had positively skewed distributions, and thus were naturally log (ln) transformed. To account for potential measurement errors and extreme outliers in the BMI variability indices, slope-adjusted BMI-SD, CV, ARV, and MMD values below the 0.1st percentile and above the 99.9th percentile were replaced with the 0.1st and 99.9th percentile values, respectively, in a process called winsorization.
Outcome definitions
The initial prescription of the following antidementia drugs (WHO-ATC code) was defined as a proxy for incident dementia: donepezil (N06DA02), rivastigmine (N06DA03), galantamine (N06DA04), ipidacrine (N06DA05), and memantine (N06DX01). We did not use the initial definitive diagnosis of dementia (ICD-10 codes F00–03 and G30–G31 [with the exception of G319]) recorded in the claims data because its reliability remains uncertain; the diagnosis documented in the claims data could be assigned so that various clinical examinations would be approved by insurance [23].
Death outcome was extracted from the information on loss of eligibility as an NHI-insured person and was used as a competing risk. Censoring was defined as the end of the database period or loss of eligibility for reasons other than death.
Statistical analysis
Differences among groups were compared by assessing standardized mean differences (SMDs) [31]. An SMD of |0.1| was set as the cutoff point to determine the group difference [31]. Unless otherwise specified, continuous variables are summarized as mean ± SD and categorical variables are expressed as percentages. The correlations between BMI variability indices and annual BMI changes were assessed to confirm the associations between the variability indices and annual changes.
The association between BMI indices and dementia risk was analyzed using Fine-Gray hazard models to account for the competing risk of death [32]. To consider the potential non-linear associations, the participants were categorized into tertiles or sextiles of annual BMI change or slope-adjusted BMI-SD. The group with the lowest risk was used as the reference. The hazard ratios were calculated using the model with both annual BMI change and slope-adjusted BMI-SD categories and were adjusted for sex and baseline characteristics, including age, smoking status, alcohol consumption, proteinuria, systolic BP, HbA1c, LDL, and the use of antihypertensive, antidiabetic, or lipid-lowering drugs, as identified from the claims data. Missing continuous variables for systolic BP (n = 5, 0.002%), diastolic BP (n = 6, 0.002%), HbA1c levels (n = 2145, 0.71%), LDL levels (n = 152, 0.05%), and high-density lipoprotein levels (n = 9, 0.003%) were interpolated from the regression slope of age after sex stratification. For participants with an unknown smoking (n = 9, 0.003%), alcohol consumption (n = 13,194, 4.35%), and proteinuria status (n = 441, 0.15%), the design variable was imputed to the sex-specific mean of the codes (0, 1).
Model fit was assessed using the Akaike Information Criterion (AIC), with lower values indicating better model fit [33]. The discriminative ability of each model was evaluated using the C-statistic calculated at two years, based on the time-dependent area under the receiver operating characteristic curve (AUC) for competing risk analysis. Confidence intervals for C-statistics were obtained using the DeLong method [34] as implemented in the pec package’s Score function. To evaluate the incremental predictive value of adding variables to the models, the AUC differences between the models were calculated using their corresponding 95% confidence intervals (CIs).
For sensitivity analyses, we examined alternative BMI variability indices other than slope-adjusted BMI-SD. In addition, visit-to-visit differences between adjacent time points were evaluated to determine their association with the risk of dementia. In addition, stratified analyses according to these baseline covariates as well as subgroup analyses based on a follow-up duration of two years (median) and median annual BMI change were performed. Interaction was tested using an interaction variable calculated as a stratification factor multiplied by the primary independent variable.
To calculate C-statistics and AIC with the cmprsk package for competing risk analysis, riskRegression package for model evaluation, and pec package for performance assessment R (Ver 4.4.1) was used. The Fine-Gray models were fitted using the FGR function from the riskRegression package. All other analyses were conducted using the SAS software (version 9.4 1M8; SAS Institute Inc., Cary, NC, USA). Statistical significance was set at α < 0.05, and all tests were two-sided. Continuous variables are presented as means ± standard deviations unless otherwise noted.
Results
Baseline characteristics
The baseline characteristics of the participants stratified by slope-adjusted BMI-SD tertiles are shown in Table 1. Compared with the lowest BMI variability tertile, participants in the highest tertile were younger, more likely to be prescribed antidiabetic or antihypertensive drugs, and had higher HbA1c levels (|SMD|≥0.1). As expected, BMI variability indices and BMI-related measures increased substantially across tertiles, with participants in higher tertiles having progressively higher mean BMI values and greater annual changes in absolute BMI.
The absolute value of annual BMI change was moderately to strongly correlated with ln BMI-CV, ln BMI-ARV, and ln BMI-MMD (r ≥ 0.43). The slope-adjusted BMI-SD exhibited the weakest correlation with the absolute value of annual BMI change (r = 0.25). Slope-adjusted BMI-SD strongly correlated with other variability indices (r ≥ 0.73) (Supplementary Table S1).
BMI variability or annual change and dementia risk
During a mean follow-up of 2.17 ± 1.19 (median 2.15 [interquartile range: 1.13–3.39]) years, antidementia drugs were initiated in 665 participants and 2394 died. Donepezil (N06DA02) was prescribed to 448 patients (67.4%), followed by galantamine (N06DA04) to 90 (13.5%), memantine (N06DX01) to 79 (11.9%), and rivastigmine (N06DA03) to 48 (7.2%).
Figure 2 shows the dementia risk according to the slope-adjusted BMI-SD and sextiles of annual BMI changes, which were included in the same model. Dementia risk did not differ across the 1st to 4th sextiles of slope-adjusted BMI-SD, whereas it was higher in the 5th and 6th sextile groups, i.e., the highest tertile group of slope-adjusted BMI-SD. The association between the annual BMI changes and dementia risk was U-shaped.

Hazard ratios for antidementia drug initiation across sextiles for annual BMI change from baseline (left panel) and slope-adjusted BMI-SD (right panel). Both BMI trends and variability measures were simultaneously included in the models with covariates to assess independent associations. The models were adjusted for age, sex, smoking status, alcohol consumption, proteinuria, systolic blood pressure, HbA1c and LDL cholesterol levels, medication use, and baseline BMI. The lowest risk group was used as the reference category. BMI body mass index, HbA1c hemoglobin A1c, LDL low-density lipoprotein, SD standard deviation.
Table 2 lists the incremental predictive values of the different BMI-related measures. When the model with baseline characteristics but without BMI (Model 1) was treated as the reference model, annual BMI change ≤−0.31% revealed the best predictive ability with the lowest AIC (Model 4), followed by BMI at baseline (Model 2), slope-adjusted BMI-SD (Model 6), mean BMI (Model 3), and annual BMI change ≥1.19% (6th sextile) (Model 5); there was no significant difference in the C-statistic improvements when BMI at baseline and slope-adjusted BMI-SD were added to Model 1 (Model 2 vs Model 6, −0.0001 [95% CI: −0.0007 to 0.0004]). Further addition of slope-adjusted BMI-SD to the model with baseline BMI and annual BMI change categories provided significant incremental improvements (Model 9).
Sensitivity analyses
Similar patterns were observed across all BMI variability indices, with the highest tertile consistently showing an increased risk compared to the reference groups (Supplementary Table S2). The associations between visit-to-visit differences from Visits 1 to 2, 2 to 3, 3 to 4, and 4 to 5 and dementia risk were not consistent (Supplementary Table S2).
The association between the highest slope-adjusted BMI-SD tertile and dementia risk was assessed after stratification according to age (<70/≥70 years), sex, smoking status, alcohol consumption, BP levels (<140/≥140 mmHg), HbA1c levels (<6.5%/≥6.5%), LDL levels (<140/≥140 mg/dL), medication use (antihypertensive, antidiabetic, and lipid-lowering drugs), baseline BMI (<25/≥25 kg/m²), follow-up duration (<2.0/≥2.0 years), and annual BMI change (≤0.14%/≥0.14%). Among these subgroup analyses, a significant interaction was observed only for sex (P for interaction = 0.0039) (Fig. 3). After stratification by sex, the association between slope-adjusted BMI-SD and dementia risk was clearer in females (Supplementary Fig. S3) than in males (Supplementary Fig. S4). Improvements in C-statistics when slope-adjusted BMI-SD was added were observed in females (Supplementary Table S3) but not in males (Supplementary Table S4).

Hazard ratios for antidementia drug initiation comparing low-to-moderate (tertiles 1–2: ≤0.50 kg/m²) vs high slope-adjusted BMI-SD (tertile 3: ≥0.50 kg/m²) across subgroups. The square marker size is proportional to the number of events. All models were adjusted for age, sex, smoking status, alcohol consumption, proteinuria, systolic blood pressure, HbA1c and LDL levels, medication use, and BMI category. BMI body mass index, LDL low-density lipoprotein, SBP systolic blood pressure, HbA1c hemoglobin A1c, SD standard deviation.
Discussion
This large-scale longitudinal study demonstrated that slope-adjusted BMI-SD is independently associated with an increased risk of dementia, which was assessed considering antidementia drug initiation as the proxy outcome. The predictive value of the slope-adjusted BMI-SD for dementia remained significant after adjusting for annual BMI changes. Slope-adjusted BMI-SD provided additional prognostic information, with more pronounced associations in females than males. Meanwhile, annual BMI decline by ≤−0.31% was consistently associated with the risk of dementia regardless of sex and was the strongest predictor of dementia among the BMI-related indices.
The slope-adjusted BMI-SD significantly predicted future dementia risk. Only the third tertile exhibited a significantly elevated dementia risk, implying a nonlinear association between BMI variability and dementia risk. This index also achieved a C-statistic improvement comparable to that of the baseline BMI, suggesting its potential value for long-term dementia risk assessment if sufficient longitudinal data are available.
The present study focused specifically on evaluating whether slope-independent variability predicts dementia risk, rather than comprehensively comparing all available BMI variability indices. Although conventional variability indices such as BMI-CV, BMI-MMD, and BMI-ARV were also significantly associated with a higher risk of dementia, they were highly correlated with absolute annual BMI change, indicating potential confounding. In contrast, slope-adjusted BMI-SD may offer a more valid and independent measure of intra-individual BMI variability, minimizing the influence of secular trends such as annual BMI change. Notably, BMI changes between consecutive visits (e.g., change in BMI from Visit 4 to Visit 5) showed inconsistent associations and did not improve risk prediction, highlighting the importance of multiple repeated measurements over time to capture meaningful variability. The statistically significant improvement suggests slope-adjusted variability captures complementary information independent of directional weight change. However, the improvement in C-statistics achieved by adding slope-adjusted BMI-SD to the model accounting for baseline BMI, BMI change, and all other risk factors was modest (+0.0094). Future studies employing more sophisticated analytical approaches, including machine learning algorithms and decision curve analysis, are warranted to determine the optimal BMI variability index for dementia prediction.
Although the direct mechanisms underlying our findings remain unclear, repeated weight cycling in obese mice has been reported to cause glucose intolerance [18]. Brain insulin resistance can occur in patients with Alzheimer’s disease [19], which may be caused by weight variability. Weight fluctuations are closely linked to central nervous system regulation via hormonal signals such as leptin, insulin, and gut-derived peptides [22], and impairment of this complex regulatory system may mediate our findings. Furthermore, body weight variability has been associated with inflammation and cardiovascular risk [20, 21, 35, 36], which may also contribute to dementia risk through vascular mechanisms. Meanwhile, the association between slope-adjusted BMI-SD and dementia risk was significant only in females but not in males. Although the exact reasons for the sex-specific discrepancies remain uncertain, females experience steep estrogen decline during menopause, losing estrogen’s protective effects against amyloid β-protein accumulation suddenly [37,38,39]. Additionally, the APOE ε4 allele confers disproportionately greater dementia risk in females compared to males [40, 41], and genetic polymorphisms including APOE variants influence both Alzheimer’s disease susceptibility and BMI regulation [42]. This convergence of hormonal changes, genetic predisposition, and metabolic dysregulation may explain why BMI variability serves as a particularly sensitive marker of dementia risk in females. Another possible reason for sex differences may be lifestyle factors. In Japan, women, particularly the older generations, have traditionally been primarily responsible for preparing household meals. Therefore, cognitive decline in women may directly influence BMI variability through changes in dietary patterns and food preparation. However, sex differences in the association between body weight variability and the risk of dementia remain controversial. Some studies reported stronger associations in females [7, 16, 43], while others found stronger associations in males [14, 17] and several studies reported no significant sex interactions [11, 15]. Further studies are needed to clarify this issue.
Despite the significant predictive value of the slope-adjusted BMI-SD, the AIC values and C-statistics improvement analysis revealed that BMI decline by ≤−0.31% annually demonstrated the greatest improvement in predictive performance among the BMI related indices. This improvement achieved by adding the annual BMI decline to the prediction model exceeded that achieved by adding the baseline BMI or mean BMI, highlighting the critical importance of detecting BMI decline patterns in dementia risk assessment. In longitudinal studies with over 20 years of follow-up, BMI decline demonstrated an onset approximately 10 years prior to dementia diagnosis and exhibited a linear decrease during the past 5 years [9, 10]. In contrast, the contribution of annual BMI increase to model improvement was limited. This could be because the definition of antidementia drug initiation in the present study strongly reflects the incidence of nonvascular diseases. A previous meta-analysis revealed that ≥0.5% weight gain per year tended to be associated with vascular dementia but not with non-vascular dementia [2]. A recent study demonstrated that weight loss or gain during 1 year was significantly associated with the incidence of functional disability and all-cause mortality in older adults [44]. Therefore, weight change is not a negligible factor considered when assessing future general health status in older adults.
This study has several limitations. First, our outcome definition was based on antidementia drug initiation, which may have overlooked patients who received non-pharmacological interventions for cognitive impairment. This precludes accurate estimation of dementia incidence rates or risk differences and reduces statistical power. However, antidementia drugs are rarely prescribed for individuals without cognitive impairment, suggesting the high specificity of our definition, leading to accurate relative risk estimation [23]. Second, we were unable to examine actual dementia subtypes separately, such as Alzheimer’s disease, dementia with Lewy bodies, or other specific forms of dementia. Furthermore, data on the cognitive scales used to evaluate the severity or progression of cognitive decline were lacking. Third, the study population was restricted to participants who attended all five annual health checkups, which likely introduced a healthy selection bias and may limit the generalizability of our findings to a broader population. Fourth, the relatively short mean observation period of two years may not have captured the full spectrum of cognitive decline. Given that the progression from subjective cognitive impairment to amnestic mild cognitive impairment can span approximately a decade [45], the observed BMI variability may have been influenced by an underlying cognitive impairment that had not yet reached the threshold for antidementia drug prescription. Finally, other confounding factors such as education level and economic status that could not be captured in the present database may have influenced our findings.
In conclusion, high BMI variability, indicated by slope-adjusted BMI-SD, provided additional prognostic information, with associations that were particularly pronounced in females. Use of the slope-adjusted variability index enhanced the plausibility of the observed association between long-term visit-to-visit BMI variability and dementia risk. Meanwhile, annual BMI decline emerged as a strong predictor, regardless of sex, outperforming baseline BMI measures in predictive performance. These findings support the integration of not only a single BMI point but also longitudinal BMI monitoring into routine dementia risk assessment strategies. Future research with long-term follow-up is needed to establish causality and to explore optimal intervention strategies for individuals with different BMI patterns.
Data availability
The data in this study are not authorized for use by third parties under a contract with DeSC Healthcare, Inc. The authors can provide additional analyses upon request. The DeSC database is available to anyone who purchases it from DeSC Healthcare Inc.
Code availability
Available from the first author upon request.
References
G. B. D. Dementia Forecasting Collaborators. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: an analysis for the Global Burden of Disease Study 2019. Lancet Public Health. 2022;7:e105–e125.
Lee CM, Woodward M, Batty GD, Beiser AS, Bell S, Berr C, et al. Association of anthropometry and weight change with risk of dementia and its major subtypes: a meta-analysis consisting 2.8 million adults with 57 294 cases of dementia. Obes Rev. 2020;21:e12989.
Backman K, Joas E, Waern M, Ostling S, Guo X, Blennow K, et al. 37 years of body mass index and dementia: effect modification by the APOE genotype: observations from the prospective population study of Women in Gothenburg, Sweden. J Alzheimers Dis. 2015;48:1119–27.
Li J, Liu C, Ang TFA, Au R. BMI decline patterns and relation to dementia risk across four decades of follow-up in the Framingham Study. Alzheimers Dement. 2023;19:2520–7.
Guo J, Marseglia A, Shang Y, Dove A, Grande G, Fratiglioni L, et al. Association between late-life weight change and dementia: a population-based cohort study. J Gerontol A Biol Sci Med Sci. 2023;78:143–50.
Tashiro M, Yasuda N, Inoue M, Yamagishi K, Tsugane S, Sawada N. Body mass index, weight change in midlife, and dementia incidence: the Japan Public Health Center-based Prospective Study. Alzheimers Dement (Amst. 2023;15:e12507
Wu Z, Owen A, Woods RL, Cribb L, Alharbi T, Zhou Z, et al. Associations of body habitus and its changes with incident dementia in older adults. J Am Geriatr Soc. 2024;72:1023–34.
Cannon EJ, Windham BG, Griswold M, Palta P, Knopman DS, Sedaghat S, et al. Association of body mass index in late life, and change from midlife to late life, with incident dementia in the ARIC study participants. Neurology. 2025;104:e213534.
Singh-Manoux A, Dugravot A, Shipley M, Brunner EJ, Elbaz A, Sabia S, et al. Obesity trajectories and risk of dementia: 28 years of follow-up in the Whitehall II Study. Alzheimers Dement. 2018;14:178–86.
Gao S, Nguyen JT, Hendrie HC, Unverzagt FW, Hake A, Smith-Gamble V, et al. Accelerated weight loss and incident dementia in an elderly African-American cohort. J Am Geriatr Soc. 2011;59:18–25.
Beeri MS, Tirosh A, Lin HM, Golan S, Boccara E, Sano M, et al. Stability in BMI over time is associated with a better cognitive trajectory in older adults. Alzheimers Dement. 2022;18:2131–9.
Ravona-Springer R, Schnaider-Beeri M, Goldbourt U. Body weight variability in midlife and risk for dementia in old age. Neurology. 2013;80:1677–83.
Lee SH, Han K, Cho H, Park YM, Kwon HS, Kang G, et al. Variability in metabolic parameters and risk of dementia: a nationwide population-based study. Alzheimers Res Ther. 2018;10:110.
Park KY, Nam GE, Han K, Hwang HS. Body weight variability and the risk of dementia in patients with type 2 diabetes mellitus: a nationwide cohort study in Korea. Diab Res Clin Pr. 2022;190:110015.
Roh E, Hwang SY, Kim JA, Lee YB, Hong SH, Kim NH, et al. Body weight variability increases dementia risk among older adults: a nationwide population-based cohort study. Front Endocrinol. 2020;11:291.
Kang SY, Kim YJ, Jang W, Son KY, Park HS, Kim YS. Body mass index trajectories and the risk for Alzheimer’s disease among older adults. Sci Rep. 2021;11:3087.
Ha J, Kwon Y, Kwon YJ, Kim D, Han K, Jang M, et al. Variability in body weight precedes diagnosis in dementia: a nationwide cohort study. Brain Behav. 2020;10:e01811.
Simonds SE, Pryor JT, Cowley MA. Repeated weight cycling in obese mice causes increased appetite and glucose intolerance. Physiol Behav. 2018;194:184–90.
Kellar D, Craft S. Brain insulin resistance in Alzheimer’s disease and related disorders: mechanisms and therapeutic approaches. Lancet Neurol. 2020;19:758–66.
Prattichizzo F, Frige C, La Grotta R, Ceriello A. Weight variability and diabetes complications. Diab Res Clin Pr. 2023;199:110646.
Li W, Chen W. Weight cycling based on altered immune microenvironment as a result of metaflammation. Nutr Metab. 2023;20:13.
Morton GJ, Cummings DE, Baskin DG, Barsh GS, Schwartz MW. Central nervous system control of food intake and body weight. Nature. 2006;443:289–95.
Satoh M, Nakayama S, Toyama M, Hashimoto H, Murakami T, Metoki H. Usefulness and caveats of real-world data for research on hypertension and its association with cardiovascular or renal disease in Japan. Hypertens Res. 2024;47:3099–113.
Satoh M, Murakami T, Obara T, Metoki H. Time-series analysis of blood pressure changes after the guideline update in 2019 and the coronavirus disease pandemic in 2020 using Japanese longitudinal data. Hypertens Res. 2022;45:1408–17.
The Ministry of Health Labour and Welfare. Overview of Medical Service Regime in Japan. https://www.mhlw.go.jp/bunya/iryouhoken/iryouhoken01/dl/01_eng.pdf. Access date: 10 Mar 2026.
Eba J, Nakamura K. Overview of the ethical guidelines for medical and biological research involving human subjects in Japan. Jpn J Clin Oncol. 2022;52:539–44.
von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370:1453–7.
The Ministry of Health Labour and Welfare. Standard health checkup and health guidance programs. 2018. https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000194155_00001.html. Access 10 Mar 2026.
Satoh M, Muroya T, Murakami T, Obara T, Asayama K, Ohkubo T, et al. The impact of clinical inertia on uncontrolled blood pressure in treated hypertension: real-world, longitudinal data from Japan. Hypertens Res. 2024;47:598–607.
Satoh M, Hirose T, Satoh H, Nakayama S, Obara T, Murakami T, et al. Actual impact of angiotensin II receptor blocker or calcium channel blocker monotherapy on renal function in real-world patients. J Hypertens. 2022;40:1564–76.
Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. 2009;28:3083–107.
Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc. 1999;94:496–509.
Akaike H. A new look at the statistical model identification. IEEE Trans Autom Control. 1974;19:716–23.
DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988;44:837–45.
Massey RJ, Siddiqui MK, Pearson ER, Dawed AY. Weight variability and cardiovascular outcomes: a systematic review and meta-analysis. Cardiovasc Diabetol. 2023;22:5.
Ceriello A, Lucisano G, Prattichizzo F, Eliasson B, Franzen S, Svensson AM, et al. Variability in body weight and the risk of cardiovascular complications in type 2 diabetes: results from the Swedish National Diabetes Register. Cardiovasc Diabetol. 2021;20:173.
Xu H, Gouras GK, Greenfield JP, Vincent B, Naslund J, Mazzarelli L, et al. Estrogen reduces neuronal generation of Alzheimer beta-amyloid peptides. Nat Med. 1998;4:447–51.
Galea LA, Wainwright SR, Roes MM, Duarte-Guterman P, Chow C, Hamson DK. Sex, hormones and neurogenesis in the hippocampus: hormonal modulation of neurogenesis and potential functional implications. J Neuroendocrinol. 2013;25:1039–61.
Long J, He P, Shen Y, Li R. New evidence of mitochondria dysfunction in the female Alzheimer’s disease brain: deficiency of estrogen receptor-beta. J Alzheimers Dis. 2012;30:545–58.
Barker W, Harwood D, Duara R, Mullan M, Fallin D, Hyslop PS, et al. The APOE-epsilon4 allele and Alzheimer disease among African Americans, Hispanics, and whites. JAMA. 1998;280:1661–2. author reply 1663.
Altmann A, Tian L, Henderson VW, Greicius MD. Alzheimer’s Disease Neuroimaging Initiative I. Sex modifies the APOE-related risk of developing Alzheimer disease. Ann Neurol. 2014;75:563–73.
Goni L, Garcia-Granero M, Milagro FI, Cuervo M, Martinez JA. Phenotype and genotype predictors of BMI variability among European adults. Nutr Diab. 2018;8:27.
Crane BM, Nichols E, Carlson MC, Deal JA, Gross AL. Body mass index and cognition: associations across mid- to late life and gender differences. J Gerontol A Biol Sci Med Sci. 2023;78:988–96.
Tabara Y, Shoji-Asahina A, Sato Y. Association of body weight changes over 1 year with the incidence of functional disability and all-cause mortality in older adults: the Shizuoka Kokuho Database Study. J Am Med Dir Assoc. 2025;26:105904.
Kim KW, Woo SY, Kim S, Jang H, Kim Y, Cho SH, et al. Disease progression modeling of Alzheimer’s disease according to education level. Sci Rep. 2020;10:16808.
Acknowledgements
The manuscript was comprehensively edited by Editage (Cactus Communications). Additional language refinement was conducted using DeepL, Claude, Grammarly, and ChatGPT.
Funding
This study was supported by Grants-in-Aid for Scientific Research (KAKENHI) from the Japan Society for the Promotion of Science (JSPS) (Grant Numbers JP21K10478 and JP25K02854); academic support from Bayer Yakuhin Co., Ltd.; and a grant from the Daiwa Securities Foundation.
Author information
Authors and Affiliations
Contributions
Author Contributions: MS contributed to conceptualization, data curation, formal analysis, funding acquisition, resources, methodology, project administration, visualization, and writing of the original draft. HN contributed to conceptualization, methodology, visualization, validation, review, and editing. TY, YI, SI, TaM, YS, MT, SN, ToM, and JF contributed to conceptualization, methodology, validation, review, and editing. HM contributed to conceptualization, formal analysis, funding acquisition, methodology, project administration, supervision, validation, visualization, review, and editing. All authors contributed to this scientific work and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
MS received a scholarship donation (academic support program) from Bayer Yakuhin Co., Ltd. The Division of Public Health, Hygiene, and Epidemiology received scholarship donations from Pfizer Japan Inc., Bayer Academic Support, Takeda Research Support, Astellas Research Support, and J&J Medical Research Grant, as well as scholarship donations from Chugai Pharmaceutical Co., Ltd., Daiichi Sankyo Co., Ltd., and Otsuka Pharmaceutical Co., Ltd. HM concurrently hold the position of Director of the Tohoku Institute for the Management of Blood Pressure, supported by Omron Healthcare Co., Ltd.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Satoh, M., Nobayashi, H., Yagihashi, T. et al. The impact of slope-adjusted visit-to-visit body mass index variability on early dementia risk prediction. Int J Obes (2026). https://doi.org/10.1038/s41366-026-02052-z
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41366-026-02052-z
