
Abstract
Background/Objectives
Glucagon-like peptide-1 receptor agonist medications (GLP-1s) are effective for weight loss, but when people discontinue them, they tend to regain weight. The present work sought to examine the stigma of losing and regaining weight after GLP-1 use and cessation.
Subjects/Methods
In two randomized, between-subjects experiments, participants evaluated a fictional target after reading a brief description of the target’s weight-related history, which varied by study condition. Study 1 (N = 607) aimed to understand stigma directed at individuals who lose weight using GLP-1s, so the target was described as either: having lost weight by using a GLP-1, having lost weight via diet and exercise, or not having lost weight. Study 2 (N = 706) examined stigma directed at people who regain weight after discontinuing GLP-1s, and the target was described as either: having regained weight after discontinuing a GLP-1, having regained weight after discontinuing a diet and exercise plan, not having lost weight, or having maintained weight loss. After reading, participants completed measures of weight-related stereotyping and willingness to affiliate with the target.
Results
In Study 1, the GLP-1 target was evaluated more negatively than the diet/exercise target and the no weight loss target. Participants’ willingness to affiliate differed significantly across groups (p < 0.001), with the GLP-1 target receiving significantly lower ratings compared to the diet/exercise target (Mean difference = 0.52, 95% CI [0.27, 0.76]) and the no weight loss target (Mean difference = 0.26, 95% CI [0.02, 0.51]). In Study 2, the GLP-1 and diet/exercise targets were evaluated similarly, and both were rated more negatively than the target who maintained weight loss (ps ≤ 0.001).
Conclusions
These findings suggest that people may face stigma across the cycle of losing and regaining weight after using a GLP-1, underscoring the need for stigma-reduction efforts in the context of weight management.
Similar content being viewed by others
An experimental investigation of the stigmatization of weight loss and regain from GLP-1 receptor agonist use and cessation
Glucagon-like peptide-1 receptor agonist medications, or GLP-1s, are a class of medications initially developed to treat diabetes. In 2021 and 2023, two GLP-1s, semaglutide and tirzepatide (a dual GLP-1/glucose-dependent insulinotropic polypeptide agonist), received FDA approval to treat obesity [1, 2], and they have since revolutionized the weight management field [3]. Evidence suggests that these new GLP-1s are effective for achieving clinically significant weight loss [4,5,6], although long-term follow-up studies are still needed [7]. Given the generally low, short-term efficacy of behavioral weight loss interventions [8,9,10] and the invasiveness of weight loss surgery [11], GLP-1s are an attractive treatment option for many higher-weightFootnote 1 patients.
A key drawback of GLP-1s is that when people stop taking them (e.g., due to side effects, changes in insurance coverage), they tend to regain a substantial amount of weight within a year [12, 13]. Widespread weight regain resulting from GLP-1 cessation is concerning, both because weight cycling (i.e., losing and regaining weight) is physiologically taxing [14] and because people may be stigmatized for regaining weight. It is critical to understand and mitigate stigma associated with GLP-1 cessation and weight regain, as it has the potential to undermine people’s well-being and discourage them from seeking healthcare [15, 16].
These issues are pressing, as GLP-1 discontinuation and subsequent weight regain are poised to become increasingly common in the United States. Soon, many Americans may be forced to discontinue GLP-1s as they reach time- and cost-based limits of their health insurance coverage [17] and as access to compounded versions of GLP-1s is restricted [18]. To contextualize stigma directed at people who regain weight after GLP-1 cessation, it is also important to understand how people are regarded for losing weight with a GLP-1.
Stigmatization of GLP-1 use and cessation
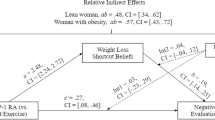
One narrative that has gained traction is that using GLP-1s to lose weight is “taking the easy way out” [19, 20], particularly as compared to behavioral weight loss methods. A similar narrative has been perpetuated about people who undergo bariatric (i.e., weight loss) surgery [21], a notion that is inherently stigmatizing, as it suggests that people who undergo surgery or use GLP-1s are lazy or undisciplined. Moreover, it reflects widespread bias against higher-weight people (i.e., weight stigma), which is unjust and harmful [15]. Indeed, there is a rich experimental literature about the stigma of having previously had obesity [22], with several studies finding that one’s method of weight loss (i.e., bariatric surgery vs. behavior change) can influence these judgments [23,24,25,26]. In general, this work finds that individuals who lose weight via bariatric surgery are regarded less highly than individuals who lose weight via behavior change. Some recent empirical work explored this phenomenon in the GLP-1 context [20], finding that a person who lost weight using a GLP-1 (i.e., a GLP-1 user) was evaluated more negatively than someone who lost weight via diet and exercise (i.e., a dieter). Consistent with the “taking the easy way out” narrative, this effect was mediated by the belief that using a GLP-1 was a “shortcut” to weight loss. Thus, GLP-1 users may be socially penalized. However, it is not clear how the magnitude of GLP-1-related stigma compares to more generalized stigma directed at higher-weight people. One potential benefit of losing weight might be reduced experiences of weight stigma, but this benefit may not be realized if people are stigmatized for doing so with a GLP-1.
Another important, underexplored aspect of GLP-1-related stigma is how GLP-1 users are regarded after discontinuing medication and regaining weight. Dieters who regain weight are judged harshly for “falling off the wagon” [27, 28], and similar judgments may be applied to GLP-1 users who regain weight. Moreover, GLP-1 users who regain weight may be accused of “squandering an opportunity” granted by these highly sought-after medications, similar to stigma directed at people who regain weight after bariatric surgery [29, 30]. To our knowledge, no empirical work has sought to understand the stigma of regaining weight after GLP-1 use.
GLP-1 users may also encounter judgment related to high medication costs. Insurance coverage for GLP-1s is limited, and out-of-pocket costs are extremely high (i.e., list prices ~$1200/month, or ~$700/month with manufacturer discounts) [31]. Thus, people may make assumptions about the socioeconomic status (SES) of individuals who use or discontinue GLP-1s. Indeed, some have pointed to the lack of GLP-1 affordability as a factor that could widen obesity-related health disparities [32, 33] and increase stigma at the intersection of class and body size [34]. For instance, if people perceive GLP-1 usage as a signal of high SES, someone who chooses not to use or discontinues the medication may be assumed to be unable to afford them, thereby layering classism on top of weight stigma. However, the more basic question of whether people make assumptions about SES based on GLP-1 use is not yet established.
The present work
Across two pre-registered, randomized experiments, we investigated the stigma of weight loss and regain resulting from GLP-1 use and cessation. We asked participants to evaluate a fictional target and assessed two measures of weight stigma (i.e., endorsement of weight-related stereotypes about the target, willingness to affiliate with the target) and perceptions of the target’s SES.
As the literature in this field is nascent, Study 1 was designed to examine the stigmatization of losing weight using a GLP-1, both by replicating the few existing studies [20, 35] and by extending them by examining whether losing weight with a GLP-1 is more or less stigmatized than maintaining a higher weight. Therefore, we sought to compare how people evaluated someone who lost weight using a GLP-1 versus someone who either lost weight via diet and exercise or did not attempt weight loss. We anticipated that higher-weight people would be more stigmatized than people who lost weight using a GLP-1, so we hypothesized that the target who did not attempt weight loss would receive the most unfavorable evaluations, followed by the target who lost weight using a GLP-1. We expected the target who lost weight via diet and exercise to receive the most favorable evaluations.
Study 2 was designed to understand the stigmatization of weight regain after GLP-1 cessation. Participants evaluated a target who had either regained weight after discontinuing a GLP-1, regained weight after discontinuing a diet and exercise program, did not attempt weight loss, or lost weight and maintained it. Based on some unexpected findings in Study 1 (i.e., the GLP-1 weight loss target was evaluated more unfavorably than the no weight loss target; see Study 1 Confirmatory Findings), we hypothesized that the target who regained weight after discontinuing a GLP-1 would be evaluated most unfavorably, followed by the target who did not attempt weight loss, and then by the target who regained weight after discontinuing a diet and exercise program. We expected the target who lost weight and maintained it to receive the most favorable evaluations, as they were the only target who succeeded at losing weight.
In both studies, we tested the exploratory hypothesis that ratings of the target’s SES would be higher for the GLP-1 target than for the diet+exercise target. We also explored whether participants’ explicit or internalized weight bias moderated the effects of study condition on willingness to affiliate with the target. These moderation tests were pre-registered, but we did not specify directional hypotheses.
Methods
Participants
Participants were recruited from Prolific, an online survey platform, in October 2024 (Study 1; N = 607) and February 2025 (Study 2; N = 706). To be eligible, participants needed to be 18 years or older, fluent in English, and reside in the United States. Study 1 participants were excluded from Study 2, and participant-facing study descriptions did not mention weight, dieting, or GLP-1s. Recruitment targets were determined a priori based on power analyses conducted using G*Power Version 3[36];. For one-way ANOVA models with power of 0.9 and an anticipated small-to-medium effect size (f = 0.15), a minimum of 567 (Study 1) and 636 participants (Study 2) were needed. We set recruitment targets slightly above these minimums to ensure sufficient power for exploratory tests. For sample demographics and sample size by condition, see Tables 1–3.
Procedures
We conducted two between-subjects randomized experiments. In both studies, participants were randomly assigned to a condition (via a randomizer embedded in the survey) and then read a brief description of a fictional target. Across all conditions, the target (age 38, no gender specifiedFootnote 2, college-educated) was described as having had obesity since puberty, with a recent weight of around 220 pounds. These demographic details were designed after an average-aged, average-weight individual in the U.S. with a modal period of onset of obesity [39]. Further details about the target’s weight-related history varied by study condition.
In Study 1, we manipulated whether the target had lost weight (i.e., 35 pounds over the past year) by taking a GLP-1 medication (GLP-1 weight loss condition) or by going on a diet and exercising regularly (diet+exercise weight loss condition). In both weight loss conditions, we specified that the target was no longer in the “obese” BMI category to emphasize the results of the target’s weight loss efforts. In a third condition, the target description did not mention weight loss (no weight loss condition), indicating that the target currently had obesity.
In Study 2, we manipulated whether the target had lost weight with a GLP-1 medication and then regained it after stopping (GLP-1 regain condition), lost weight via diet and exercise and regained it after stopping (diet+exercise regain condition), never lost weight (no weight loss condition), or lost weight and maintained it, with the method of weight loss unspecified (maintained weight loss condition). In the maintained weight loss condition, the target was described as “no longer in the obese BMI category,” but for all other conditions, it was noted that the target had obesity.
Aside from condition-specific details, information about the target was identical across conditions (see Supporting Information for study manipulations). After reading the target description, participants completed questionnaires and received $1.60 ( ~ $15/hour).
Measures
Weight-related stereotyping
On a scale from 1 (not at all) to 7 (extremely), participants rated the target on a variety of traits related to stereotypes of higher-weight people [40,41,42]. The positive traits were: honest, generous, sociable, productive, organized, friendly, outgoing, intelligent, warm, and humorous. The negative traits were: lazy, undisciplined, self-indulgent, unclean, weak-willed, sloppy, insecure, and sluggish. Scores for positive and negative traits were averaged to form reliable composite scales (Study 1:αpositive = 0.91, αnegative = 0.92; Study 2:αpositive = 0.91, αnegative = 0.92). We also assessed participants’ ratings of the trait “unhealthy,” which we analyzed individually because it is conceptually different from the other traits (i.e., about the target’s physical health rather than their personality or current state).
Willingness to affiliate
Participants reported their willingness to affiliate with the target using six items adapted from the Interpersonal Attraction Questionnaire ([43]; see [44] for a similar adaptation). An example items is: “I think I would enjoy [target’s] company.” Response options ranged from 1 (strongly disagree) to 7 (strongly agree), and scores were averaged (αStudy 1 = 0.9, αStudy 2 = 0.89).
Explicit weight bias
Explicit weight bias was measured using the Empathy (7-item), Responsibility (6-item), and Socioeconomic Complexity (3-item) subscales of the Fat Attitudes Assessment Toolkit [45]. Subscale scores were averaged separately (αs > 0.89).
Internalized weight bias
Internalized weight bias was measured using the 11-item Weight Bias Internalization Scale-Modified [46]. Responses were averaged to create a composite score (both αs = 0.93).
Perceptions of the target’s SES
We measured perceptions of the target’s SES using the single-item MacArthur Scale of Subjective Social Status [47]. Participants viewed an image of a ladder and were told that the top represented people who were the best off in society (i.e., best jobs, most money), whereas the bottom represented people who were the worst off. They were asked to estimate where the target would fall on the ladder on a scale from 1 (bottom rung) to 10 (top rung).
Analytic plan
Confirmatory analyses
Study 1 and Study 2 employed similar analytic approaches, and all analyses were conducted in RStudio 4.3.1. After computing composite scales, we confirmed that they approximated a normal distribution. We tested our confirmatory hypotheses by conducting one-way ANOVAs to determine whether key outcomes differed by study condition. Whenever an overall model was significant, we used Tukey’s Honestly Significant Difference (HSD) tests. We set α = 0.05, and due to randomization, we did not use any covariates. Groups did not differ by age, self-reported gender, race/ethnicity, income, or education (all ps > 0.06).
Exploratory analyses
We tested our moderation hypotheses by mean-centering each proposed moderator and testing the interaction between the moderator and study condition in a multiple linear regression model. For these tests, we focused on pairwise comparisons containing GLP-1 conditions. To test our hypotheses about perceptions of the target’s SES, we used two-tailed independent samples t-tests to compare scores from participants in the GLP-1 and diet+exercise conditions.
Results
Study 1
Confirmatory findings
Participants’ endorsement of weight-related stereotypes differed significantly by study condition (all ps < 0.001; see Table 2). Consistent with hypotheses, those seeing the GLP-1 weight loss target rated the individual as significantly lower in positive traits, higher in negative traits, and more unhealthy than those seeing the diet+exercise weight loss target did (Tukey HSD ps < 0.001). However, an unexpected pattern emerged for the no weight loss condition. We hypothesized that those seeing the no weight loss target would rate the individual less favorably than would those seeing either weight loss target. Instead, we found that they rated the target higher in positive traits and no different in negative traits or unhealthiness compared to the GLP-1 weight loss target (ppositive = 0.003; pnegative = 0.26; punhealthy = 0.26).
Another unexpected pattern emerged for participants’ willingness to affiliate. Willingness differed significantly by condition (F(2, 603) = 12.54, ηp2 = 0.04, p < 0.001), and all group means were significantly different from each other (ps < 0.04). Participants seeing the diet+exercise weight loss target were most willing to affiliate with the individual (M = 5.51, SD = 0.92), followed by those seeing the no weight loss target (M = 5.25, SD = 1.08), and then those seeing the GLP-1 weight loss target (M = 4.99, SD = 1.1). For a visual representation of these results, see Fig. 1.

Mean endorsement of outcome measures by study condition. Error bars represent standard errors. Level of significance for follow-up Tukey’s HSD tests denoted by ***p ≤ 0.001, **p ≤ 0.01, *p ≤ 0.05, +p ≤ 0.1.
Exploratory findings
There were no significant differences in ratings of the target’s SES between those viewing the GLP-1 weight loss individual (M = 5.95, SD = 1.27) and the diet+exercise weight loss individual (M = 5.82, SD = 1.42; t(399) = 0.99, p = 0.32). Moreover, effects were generally not moderated by participants’ levels of explicit or internalized weight bias (see Tables S1 and S2 and Supporting Information). However, two significant moderation effects emerged in models comparing the GLP-1 weight loss and diet+exercise weight loss conditions. Specifically, willingness to affiliate with the target was especially low among participants who viewed the GLP-1 weight loss target and had low empathy (p = 0.04) or high responsibility beliefs (p < 0.001), both of which represent greater weight bias.
Study 2
Confirmatory findings
Weight-related stereotyping of the target differed significantly by study condition (ps < 0.008; see Table 3) but not as hypothesized (see Fig. 2). In general, we found that participants seeing the GLP-1 regain target and those seeing the diet+exercise regain target had similar responses; there were no differences in their ratings of the target’s positive traits, negative traits, or unhealthiness (Tukey’s HSD ps > 0.55). However, we observed differences between the two regain groups and the other groups. For instance, participants seeing the no weight loss target endorsed more positive traits for the individual than did those seeing the GLP-1 regain target (p = 0.01), but ratings of negative traits and unhealthiness were similar across the two groups (p > 0.06). In addition, those who viewed the maintained weight loss target rated the individual as significantly lower in negative traits (ps < 0.001) and less unhealthy (ps < 0.001) than did participants who viewed the GLP-1 regain target or diet+exercise regain target.

Mean endorsement of outcome measures by study condition. Error bars represent standard errors. Level of significance for follow-up Tukey’s HSD tests denoted by ***p ≤ 0.001, ** p ≤ 0.01, *p ≤ 0.05, +p ≤ 0.1.
Participants’ willingness to affiliate with the target differed across groups (F(3, 702) = 3.51, ηp2 = 0.01, p = 0.02). A follow-up test revealed that those seeing the GLP-1 regain target (M = 5.02, SD = 1.1) were significantly less willing to affiliate with the individual than those seeing the maintained weight loss target (M = 5.33, SD = 0.97).
Exploratory findings
Ratings of the target’s SES did not differ between those viewing the GLP-1 regain target (M = 5.75, SD = 1.5) and those viewing the diet+exercise regain target (M = 5.77, SD = 1.25; t(341) = –0.18, p = 0.85). Moreover, no relationships between study condition and willingness to affiliate were moderated by explicit or internalized weight bias (ps > 0.08; see Tables S3-S5).
Discussion
The present work demonstrates that both losing weight with a GLP-1 and regaining weight after discontinuing a GLP-1 can result in stigma. In Study 1, we found that participants evaluated an individual who lost weight with a GLP-1 more harshly than an individual who lost weight via diet and exercise (i.e., higher in negative traits, lower in positive traits, more unhealthy, less willing to affiliate). Moreover, they evaluated an individual who lost weight with a GLP-1 even more harshly (i.e., lower in positive traits, less willing to affiliate) than a higher-weight individual who had not attempted weight loss. Study 2 tested whether regaining weight after discontinuing a GLP-1 is stigmatized, and hypotheses were partially confirmed. Participants stigmatized an individual who had regained weight after using a GLP-1, rating them less favorably than an individual who had lost weight and maintained it (i.e., higher in negative traits, lower in positive traits, more unhealthy, less willing to affiliate) and less favorably, again, than even an individual who had not attempted weight loss (i.e., lower in positive traits). However, the weight loss method prior to regain did not seem to influence stigma; there were no significant differences in weight-related stereotyping or willingness to affiliate across the GLP-1 and diet+exercise groups. Notably, the target who lost weight and maintained it was rated more favorably (i.e., higher in positive traits, lower in negative traits, less unhealthy) than all three of the targets who currently had obesity (i.e., targets from the GLP-1 regain, diet+exercise regain, and no weight loss conditions), suggesting that having a higher weight is harshly stigmatized regardless of a person’s prior weight loss attempts.
Our findings conceptually replicate the work of Post and Persky [20], who also found that participants evaluated a GLP-1 user more negatively than a dieter. We found that a similar pattern exists for people’s willingness to affiliate with someone who lost weight – participants reported greater interest in spending time with the dieter than the GLP-1 user. In addition, our findings extend the field’s understanding of the full cycle of GLP-1-related stigma by demonstrating that GLP-1 users and dieters face similar levels of stigma after regaining weight. Given that weight regain is the likely outcome of these weight loss methods [10, 12, 13], and that widespread weight regain after GLP-1 cessation may become increasingly common, it is crucial to understand the social consequences of weight regain.
Another key extension of this work is that it directly compares the stigma directed at GLP-1 users with the stigma directed at higher-weight people. Without this comparison, one cannot discern whether stigma directed at GLP-1 users represents a decrease from the status quo (i.e., lower than the amount of stigma endured at a higher weight). After significant weight loss, one might expect that a GLP-1 user could “escape” weight stigma. However, our findings suggest the opposite: that people may experience more stigma for losing weight with a GLP-1 than for remaining at a higher weight. These findings contrast those of a similar study of bariatric surgery stigma, which found that higher-weight targets without a stated weight loss history were stigmatized more (i.e., rated as less desirable mates) than normal-weight targets who had undergone bariatric surgery [26]. Moreover, the apparent inevitability of stigma for GLP-1 users is concerning, particularly given that a desire to escape weight stigma has been conceptualized as a driver of unhealthy weight control behaviors (e.g., purging, skipping meals) and social isolation [48, 49].
Finally, we found relatively little support for our exploratory hypotheses. We found some evidence of moderation by empathy and responsibility beliefs in Study 1, suggesting that people with high explicit weight bias may penalize GLP-1 users (vs. dieters) especially harshly. However, we did not find similar effects in Study 2, and we found no differences in perceptions of the target’s SES in either study. To avoid demand characteristics, we did not provide information about GLP-1 costs in the study manipulations, so our hypotheses relied on participants’ existing knowledge of GLP-1s. Thus, one explanation for the lack of differences observed in perceptions of the target’s SES is that the high costs of GLP-1s may not have been widely known among our participants. However, we also note that we did not specify whether the target had insurance coverage, so even if participants were familiar with the costs of GLP-1s, they may not have felt able to make SES-related judgments about the target.
Strengths, limitations, and future directions
This work presents novel evidence about the stigma of weight loss and regain following GLP-1 use and cessation. It is the first study, to our knowledge, to investigate how stigma directed at GLP-1 users compares to stigma directed at higher-weight people, and it offers a timely examination of the stigma associated with regaining weight after discontinuing a GLP-1. Mapping the stigma GLP-1 users face across the weight loss/regain cycle is crucial to designing future bias-reduction efforts.
For both studies, we employed a randomized, between-subjects experiment in which participants were asked to evaluate a fictional target. Although this approach maximized internal validity and allowed for causal inference via precise study manipulations, it may have felt somewhat artificial to participants. To remedy this, future work could employ more immersive, realistic manipulations (e.g., lab-based interactions, virtual reality). Another limitation is that our study manipulations provided people with information they may not usually have when making social judgments. In everyday life, people only have access to others’ weight-related history if the information has been shared with them directly or if they make an assumption. Moreover, it is not possible to tell if a stranger has recently lost (or regained) weight after dieting or using a GLP-1. Therefore, it will be necessary for future work to examine GLP-1 users’ experiences of stigma in everyday life to quantify the frequency and intensity with which it is experienced. This work is also limited by the demographics of our participants, who were predominantly white, tended to be young, and had high income and educational attainment. To ensure that findings are generalizable, key next steps will be to replicate and extend this work with variations of the target (e.g., gender, race/ethnicity, prior attempts at weight loss, cost paid for medication) and diverse groups of participants, both in terms of participant demographics and preexisting knowledge of GLP-1s (e.g., general population, eligible patients, healthcare professionals). Finally, we note that many GLP-1 users also engage in lifestyle changes to lose weight. Future research should examine whether sharing about one’s concurrent lifestyle change efforts can buffer stigma faced by GLP-1 users.
Conclusion
As GLP-1s have gained popularity, people have begun to stigmatize those who lose weight using GLP-1s. Moreover, people stigmatize those who have regained weight after discontinuing a GLP-1, demonstrating that GLP-1 users may find it difficult to escape weight stigma and its deleterious social, health, and economic consequences [50]. Thus, individuals pursuing these treatments can become mired in a “damned if you do, damned if you don’t” situation, wherein remaining at a higher weight means enduring weight stigma, but losing (and potentially regaining) weight after using a GLP-1 also makes them vulnerable to judgment and discrimination. There is, therefore, a clear need for interventions that address the stigma associated with using GLP-1s for weight loss. Furthermore, it will be crucial for stigma-reduction efforts to be wide-reaching and designed for a variety of audiences (e.g., public health campaigns for the general population, specialized training for healthcare professionals, educational materials for patients to combat self-stigma), particularly as GLP-1s continue to grow in popularity.
Data availability
Materials used to conduct this work (e.g., study manipulations, measures) and de-identified datasets are available in a public archive: https://doi.org/10.17605/OSF.IO/7FM2R.
References
FDA. FDA Approves New Drug Treatment for Chronic Weight Management, First Since 2014 [Internet]. US Food and Drug Administration; 2021 June. (FDA News Release). Available from: https://www.fda.gov/news-events/press-announcements/fda-approves-new-drug-treatment-chronic-weight-management-first-2014.
FDA. FDA Approves New Medication for Chronic Weight Management [Internet]. US Food and Drug Administration; 2023 Nov. (FDA News Release). Available from: https://www.fda.gov/news-events/press-announcements/fda-approves-new-medication-chronic-weight-management.
Roomy MA, Hussain K, Behbehani HM, Abu-Farha J, Al-Harris R, Ambi AM, et al. Therapeutic advances in obesity management: an overview of the therapeutic interventions. Front Endocrinol. 2024;15:1364503.
American College of Cardiology/American Heart Association Task Force on Practice Guidelines, Obesity Expert Panel, 2013. Executive summary: Guidelines (2013) for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Obesity Society published by the Obesity Society and American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Based on a systematic review from the The Obesity Expert Panel, 2013. Obes Silver Spring Md. 2014;22:S5–39.
Wilding JPH, Batterham RL, Calanna S, Davies M, Gaal LFV, Lingvay I, et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384:989–1002.
Jastreboff AM, Aronne LJ, Ahmad NN, Wharton S, Connery L, Alves B, et al. Tirzepatide once weekly for the treatment of obesity. N Engl J Med. 2022;387:205–16.
Shah MY, Mohammad A, Bashir Ahmed Samejo R, Rana S, Singla S, Aurangzeb RI, et al. Weight loss that lasts: reviewing the long-term impact of GLP-1 receptor agonists. Cureus. 2025;17:e88334.
Elmaleh-Sachs A, Schwartz JL, Bramante CT, Nicklas JM, Gudzune KA, Jay M. Obesity management in adults: a review. JAMA. 2023;330:2000–15.
Ge L, Sadeghirad B, Ball GDC, da Costa BR, Hitchcock CL, Svendrovski A, et al. Comparison of dietary macronutrient patterns of 14 popular named dietary programmes for weight and cardiovascular risk factor reduction in adults: systematic review and network meta-analysis of randomised trials. BMJ. 2020;369:m696 .
Mann T, Tomiyama AJ, Westling E, Lew AM, Samuels B, Chatman J. Medicare’s search for effective obesity treatments: diets are not the answer. Am Psychol. 2007;62:220–33.
Alalwan AA, Friedman J, Park H, Segal R, Brumback BA, Hartzema AG. US national trends in bariatric surgery: a decade of study. Surgery. 2021;170:13–7.
Rubino D, Abrahamsson N, Davies M, Hesse D, Greenway FL, Jensen C, et al. Effect of continued weekly subcutaneous semaglutide vs placebo on weight loss maintenance in adults with overweight or obesity: the STEP 4 randomized clinical trial. JAMA. 2021;325:1414–25.
Aronne LJ, Sattar N, Horn DB, Bays HE, Wharton S, Lin WY, et al. Continued treatment with tirzepatide for maintenance of weight reduction in adults with obesity: the SURMOUNT-4 randomized clinical trial. JAMA. 2024;331:38–48.
Gaesser GA, Angadi SS. Obesity treatment: Weight loss versus increasing fitness and physical activity for reducing health risks. iScience. 2021;24:102995.
Tomiyama AJ, Carr D, Granberg EM, Major B, Robinson E, Sutin AR, et al. How and why weight stigma drives the obesity ‘epidemic’ and harms health. BMC Med. 2018;16:123.
Phelan SM, Bauer KW, Bradley D, Bradley SM, Haller IV, Mundi MS, et al. A model of weight-based stigma in health care and utilization outcomes: Evidence from the learning health systems network. Obes Sci Pract. 2021;8:139–46.
Klein H. Rising costs lead insurers to drop weight loss drug coverage, further increasing patient burden. Am J Manag Care. 2024;30:SP781–2.
Robbins R, Blum D. Patients cut off from cheaper obesity drugs as the F.D.A. Halts Sales of Copycats. The New York Times [Internet]. 2025; Available from: https://www.nytimes.com/2025/04/16/health/obesity-drugs-fda-compounding-wegovy-zepbound.html.
Bernstein E On Ozempic, and Feeling Judged for Taking the ‘Easy Way Out.’ Wall Street Journal [Internet]. 2023 July 7; Available from: https://www.wsj.com/health/wellness/ozempic-weight-loss-drugs-strains-relationships-327ab217.
Post SM, Persky S. The effect of GLP-1 receptor agonist use on negative evaluations of women with higher and lower body weight. Int J Obes. 2024;48:1019–26.
Himmelstein MS, Knepp KA, Phelan SM. The role of weight stigma in weight regain in bariatric surgery. Front Endocrinol. 2022;13:1076696.
Latner JD, Ebneter DS, O’Brien KS. Residual obesity stigma: an experimental investigation of bias against obese and lean targets differing in weight-loss history. Obesity. 2012;20:2035–8.
Vartanian LR, Fardouly J. The stigma of obesity surgery: negative evaluations based on weight loss history. Obes Surg. 2013;23:1545–50.
Fardouly J, Vartanian LR. Changes in weight bias following weight loss: the impact of weight-loss method. Int J Obes 2005. 2012;36:314–9.
Carels RA, Rossi J, Borushok J, Taylor MB, Kiefner-Burmeister A, Cross N, et al. Changes in weight bias and perceived employability following weight loss and gain. Obes Surg. 2015;25:568–70.
Carels RA, Rossi J, Solar C, Selensky JC. Changes in perceived mate value and weight bias associated with former obesity status. Stigma Health. 2018;3:338–47.
Romo L, Earl S, Mueller KA, Obiol M. A qualitative model of weight cycling. Qual Health Res. 2024;34:798–814.
Bombak AE, Monaghan LF. Obesity, bodily change and health identities: a qualitative study of Canadian women. Socio Health Illn. 2017;39:923–40.
Jones L, Cleator J, Yorke J. Maintaining weight loss after bariatric surgery: when the spectator role is no longer enough. Clin Obes. 2016;6:249–58.
Ulian MD, Unsain RF, Franco RR, Santo MA, Brewis A, Trainer S, et al. Weight stigma after bariatric surgery: A qualitative study with Brazilian women. PLOS ONE. 2023;18:e0287822 .
Hernandez I, Sullivan SD. Net prices of new antiobesity medications. Obesity. 2024;32:472–5.
Ryan N, Savulescu J. The Ethics of Ozempic and Wegovy. J Med Ethics. 2026;52:185–193.
Rodriguez PJ, Zhang V, Gratzl S, Do D, Goodwin Cartwright B, Baker C, et al. Discontinuation and reinitiation of dual-labeled GLP-1 receptor agonists among US adults with overweight or obesity. JAMA Netw Open. 2025;8:e2457349.
Tomiyama AJ. Behavioral medicine in the GLP-1 era. Ann Behav Med. 2025;59:kaae069.
Post SM, Stock ML, Persky S. Comparing the impact of GLP-1 agonists vs. lifestyle interventions and weight controllability information on stigma and weight-related cognitions. Int. J Behav Med. 2025;32:528–40.
Faul F, Erdfelder E, Lang A, Buchner AG. Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39:175–91.
Himmelstein MS, Puhl RM, Quinn DM. Intersectionality: an understudied framework for addressing weight stigma. Am J Prev Med. 2017;53:421–31.
Crawford D, Campbell K. Lay definitions of ideal weight and overweight. Int J Obes Relat Metab Disord J Int Assoc Study Obes. 1999;23:738–45.
Gordon-Larsen P, Adair LS, Nelson MC, Popkin BM. Five-year obesity incidence in the transition period between adolescence and adulthood: the National Longitudinal Study of Adolescent Health. Am J Clin Nutr. 2004;80:569–75.
Foster GD, Wadden TA, Makris AP, Davidson D, Sanderson RS, Allison DB, et al. Primary care physicians’ attitudes about obesity and its treatment. Obes Res. 2003;11:1168–77.
Puhl RM, Schwartz MB, Brownell KD. Impact of perceived consensus on stereotypes about obese people: a new approach for reducing bias. Health Psychol. 2005;24:517–25.
Puhl RM, Brownell KD. Bias, discrimination, and obesity. Obes Res. 2001;9:788–805.
Montoya RM, Horton RS. A two-dimensional model for the study of interpersonal attraction. Personal Soc Psychol Rev J Soc Personal Soc Psychol Inc. 2014;18:59–86.
De Groeve B, Rosenfeld DL, Bleys B, Hudders L. Moralistic stereotyping of vegans: the role of dietary motivation and advocacy status. Appetite. 2022;174:106006.
Cain P, Donaghue N, Ditchburn G. Development and validation of the Fat Attitudes Assessment Toolkit (FAAT): a multidimensional nonstigmatizing measure of contemporary attitudes toward fatness and fat people. J Appl Soc Psychol. 2022;52:1121–45.
Pearl RL, Puhl RM. Measuring internalized weight attitudes across body weight categories: Validation of the Modified Weight Bias Internalization Scale. Body Image. 2014;11:89–92.
Adler NE, Epel ES, Castellazzo G, Ickovics JR. Relationship of subjective and objective social status with psychological and physiological functioning: preliminary data in healthy white women. Health Psychol J Div Health Psychol Am Psychol Assoc. 2000;19:586–92.
Hunger JM, Major B, Blodorn A, Miller CT. Weighed down by stigma: How weight-based social identity threat contributes to weight gain and poor health. Soc Personal Psychol Compass. 2015;9:255–68.
Major B, Rathbone JA, Blodorn A, Hunger JM. The countervailing effects of weight stigma on weight-loss motivation and perceived capacity for weight control. Pers Soc Psychol Bull. 2020;46:1–13.
Puhl RM, Heuer CA. Obesity stigma: important considerations for public health. Am J Public Health. 2010;100:1019–28.
Funding
NIH R01DK128575; NIH R01HL158555; NSF BCS2220295.
Author information
Authors and Affiliations
Contributions
ECS: Conceptualization, Methodology, Investigation, Formal Analysis, Data Curation, Writing—original draft, Writing—review and editing. SMP: Conceptualization, Methodology, Supervision, Writing—review and editing. AJT: Conceptualization, Methodology, Funding Acquisition, Supervision, Writing—review and editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This work was conducted in accordance with the ethical principles of the Declaration of Helsinki and the Institutional Review Board at the University of California, Los Angeles approved all study procedures (#24-000917). All participants provided informed consent. Study hypotheses and analytic plans were pre-registered via the Open Science Framework prior to data collection and can be found on our project page (https://doi.org/10.17605/OSF.IO/7FM2R).
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Standen, E.C., Phelan, S.M. & Tomiyama, A.J. An experimental investigation of the stigmatization of weight loss and regain from GLP-1 receptor agonist use and cessation. Int J Obes (2026). https://doi.org/10.1038/s41366-026-02061-y
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41366-026-02061-y
