
Abstract
Objective
Compare Eat, Sleep, Console (ESC) and limited opioid treatment on birth length of stay (LOS), postnatal opioid exposure, and 30-day re-hospitalizations in opioid-exposed newborns (OENs) in two hospital systems.
Study design
Quality improvement teams supported change from scheduled methadone using Finnegan scores to standardized non-pharmacologic support using ESC. Intermittent morphine was used only if needed. Statistical process control charts examined changes over time.
Result
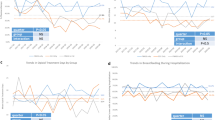
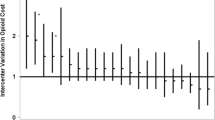
Between 2017 and 2019 we treated 280 OENs ≥35 weeks’ gestation, 101 and 179 per hospital. Post-ESC, LOS decreased 51.2% (16.8–8.2 days), postnatal opioid treatment decreased from 64.1 to 29.9%; percent decline in both hospitals was similar. 30-day re-hospitalizations were 5/103 (4.8%) pre-ESC, and 7/177 (4.0%) post-ESC (p = 0.72, NS). Multiple substance co-exposures were common (226/280, 80.7%).
Conclusion
ESC and as needed morphine decreased LOS and postnatal opioid exposure for OENs in two hospital systems without increasing 30-day readmissions. ESC appears effective in OENs with multiple co-exposures.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on SpringerLink
- Instant access to the full article PDF.
USD 39.95
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others

References
Haight SC, Ko JY, Tong VT, Bohm MK, Callaghan WM. Opioid use disorder documented at delivery hospitalization—United States, 1999–2014. MMWR Morb Mortal Wkly Rep. 2018;67:845–9. https://doi.org/10.15585/mmwr.mm6731a1.
Winkelman TNA, Villapiano N, Kozhimannil KB, Davis MM, Patrick SW. Incidence and costs of neonatal abstinence syndrome among infants with medicaid: 2004–2014. Pediatrics. 2018;141:e20173520.
Sanlorenzo LA, Stark AR, Patrick SW. Neonatal abstinence syndrome: an update. Curr Opin Pediatr. 2018;30:182–6.
Heroin Response Work Group. Heroin in Colorado 2018: Law Enforcement Public Health Treatment Data 2018;2011–6. http://www.corxconsortium.org/heroin-response-work-group.
Brown J. Colorado grapples with 80 percent jump in newborns going through opioid withdrawal: Pueblo hospital’s number of drug-addicted babies makes others “shudder.” Denver Post; November 29, 2017.
Strahan AE, Guy GP, Bohm M, Frey M, Ko JY. Neonatal abstinence syndrome incidence and health care costs in the United States, 2016. JAMA Pediatr. 2020;174:200–2. https://doi.org/10.1001/jamapediatrics.2019.4791.
Bogen DL, Whalen BL, Kair LR, Vining M, King BA. Wide variation found in care of opioid-exposed newborns. Acad Pediatr. 2017;17:374–80. https://doi.org/10.1016/j.acap.2016.10.003.
Wachman EM, Schiff DM, Silverstein M. Neonatal abstinence syndrome: advances in diagnosis and treatment. JAMA. 2018;319:1362–74. https://doi.org/10.1001/jama.2018.2640.
Clemans-Cope L, Holla N, Lee HC, Shufei Cong A, Castro R, Chyi L, et al. Neonatal abstinence syndrome management in California birth hospitals: results of a statewide survey. J Perinatol. 2020;40:463–72. https://doi.org/10.1038/s41372-019-0568-6.
Davis JM, Shenberger J, Terrin N, Breeze JL, Hudak M, Wachman EM, et al. Comparison of safety and efficacy of methadone vs morphine for treatment of neonatal abstinence syndrome: a randomized clinical trial. JAMA Pediatr. 2018;172:741–8. https://doi.org/10.1001/jamapediatrics.2018.1307.
Taleghani AA, Isemann BT, Rice WR, Ward LP, Wedig KE, Akinbi HT. Buprenorphine pharmacotherapy for the management of neonatal abstinence syndrome in methadone‐exposed neonates. Paediatr Neonatal Pain. 2019;1:33–8. https://doi.org/10.1002/pne2.12008.
Grossman MR, Berkwitt AK, Osborn RR, Xu Y, Esserman DA, Shapiro ED, et al. An initiative to improve the quality of care of infants with neonatal abstinence syndrome. Pediatrics. 2017;139:e20163360. https://doi.org/10.1542/peds.2016-3360.
Grossman MR, Lipshaw MJ, Osborn RR, Berwitt AK. A novel approach to assessing infants with neonatal abstinence syndrome. Hosp Pediatr. 2018;8:1–6. https://doi.org/10.1542/hpeds.2017-0128.
Colorado Health Institute report. Drug overdoses deaths in colorado increase. 2018. https://www.coloradohealthinstitute.org/research/death-drugs. Accessed 16 Apr 2020.
Hwang SS, Weikel B, Adams J, Bourque SL, Cabrera J, Griffith N. et al. The colorado 407 hospitals substance exposed newborn quality improvement collaborative:408 standardization of care for opioid-exposed newborns shortens length of stay and 409 reduces number of infants requiring opiate therapy.Hosp Pediatr. 2020;10:783–291. https://doi.org/10.1542/hpeds.2020-0032.
Colorado Hospital Substance Exposed Newborns Quality Improvement Collaborative, CHoSEN QIC. https://www.chosencollaborative.org. Accessed 16 June 2020.
Johnson MR, Nash DR, Laird MR, Kiley RC, Martinez MA. Development and implementation of a pharmacist-managed, neonatal and pediatric, opioid-weaning protocol. J Pediatr Pharm Ther. 2014;19:165–73. https://doi.org/10.5863/1551-6776-19.3.165.
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) – a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–81.
Provost LP, Murray SK. The health care data guide: learning from data for improvement. 1st ed. San Francisco, CA: Jossey-Bass; 2011.
Xiao F, Yan K, Zhou W. Methadone versus morphine treatment outcomes in neonatal abstinence syndrome: a meta-analysis. J Paediatr Child Health. 2019;55:1177–82. https://doi.org/10.1111/jpc.14609.
Czynski AJ, Davis JM, Dansereau LM, Engelhardt B, Marro P, Bogen DL, et al. Neurodevelopmental outcomes of neonates randomized to morphine or methadone for treatment of neonatal abstinence syndrome. J Pediatr. 2020;219:146–51.e1. https://doi.org/10.1016/j.jpeds.2019.12.018.
Acknowledgements
We would like to thank the staff and providers at both hospitals for their enthusiastic support of the project and excellent patient care, and the QI teams for their leadership, particularly Victoria Del Valle, RNC, CNS at Memorial and Stephanie Shaver, RNC at Parkview for their work on project implementation.
Funding
University of Colorado School of Medicine Upper Payment Limit Program; Custodial Funds from the Colorado Attorney General’s Office; The COPIC Foundation; The Caring for Colorado Foundation.
Author information
Authors and Affiliations
Contributions
SFT conceptualized and designed the study, analyzed and interpreted data, drafted the initial manuscript, and approved the final manuscript as submitted. CDH conceptualized and designed the study, analyzed and interpreted data, critically reviewed and edited the manuscript, and approved the final manuscript as submitted. BW carried out the analysis, interpreted the data, critically reviewed and edited the manuscript, and approved the final manuscript as submitted. SSH conceptualized and designed the study, supervised the data analysis and interpreted data, critically reviewed and edited the manuscript, and approved the final manuscript as submitted.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing financial interests or conflicts of interest. The Colorado Multiple Institutions Review Board (COMIRB) reviewed the study, and approved as exempt as a QI project. The study was performed in accordance with the Declaration of Helsinki.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Townsend, S.F., Hodapp, C.D., Weikel, B. et al. Shifting the care paradigm for opioid-exposed newborns in Southern Colorado. J Perinatol 41, 1372–1380 (2021). https://doi.org/10.1038/s41372-020-00900-y
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41372-020-00900-y
