
Abstract
Objectives
We aimed to profile the family impact, specifically parental health-related quality of life (HRQoL) and family functioning, of children discharged from a quaternary referral program with the most severe forms of bronchopulmonary dysplasia (BPD).
Study design
We collected cross-sectional data through telephone interviews with 282 families of children aged 18 months to 11 years who had been discharged from a BPD referral program.
Results
Parental HRQoL and family functioning were not associated with the child’s age, despite improvements in the children’s health and respiratory morbidity with age. Many medical issues negatively impacted parental HRQOL and family functioning. The health outcome most strongly associated with decreased parental HRQoL and family functioning was an autism diagnosis, followed by use of feeding tube.
Conclusions
Among families of children discharged from a quaternary BPD program, family impact was not associated with child age and was impacted by a wide range of health outcomes in their children.
Similar content being viewed by others

Introduction
Bronchopulmonary dysplasia (BPD) has a substantial impact on children’s families during the initial hospitalization and following discharge. One study conducted during children’s first two years of life showed that all domains of health-related quality of life (HRQoL) included in the PedsQL Family Impact Module were significantly, negatively affected by taking care of a child with BPD [1]. This impact is not surprising in light of the long-term sequelae and high rates of technology dependence in this population. Infants with BPD experience significantly increased healthcare needs, including supplemental oxygen, nutrition, therapies, specialist visits, and medications, compared to preterm infants without BPD and term controls [2, 3]. Approximately half of infants with BPD will be re-admitted to the hospital during childhood due to respiratory problems and most require more frequent outpatient visits [4, 5]. Infants with BPD experienced greater impacts on cognitive and motor development and are more likely to be enrolled in special education compared to controlled VLBW infants without BPD [6]. The effects of BPD on parental HRQoL and family functioning are found to be long-lasting. One study found that respiratory morbidity in premature children continues to affect the parent’s quality of life and family functioning beyond infancy in school aged children [7]. Yet, in a number of studies the negative impact of BPD on families is shown to decrease over time [1, 7,8,9].
Increasingly, patients with the most severe forms of BPD survive [10]. Our group recently reported on the outcomes of patients discharged from a referral BPD program who have among the most severe sequalae reported. Forty two percent of patients had a tracheostomy at some point. Ninety eight percent had individualized education plans (IEPs) in school, and thirteen percent had a diagnosis of autism [11]. The NICHD Neonatal Research Network found that rates of re-hospitalization, pulmonary medication use and incidence of poor outcomes requiring medical intervention increased with the severity of BPD [12]. In other diseases, severity of the illness correlates with its ramifications for families [13, 14]. For example, one study found that mild perinatal strokes had no impact on family quality of life, while strokes with severe medical sequelae impacted parental depression, marital satisfaction, quality of life and family functioning [15]. Severe BPD is expected to more negatively impact families’ quality of life and functioning due to the associated demands of caring for a child and need for medical technology. Yet, little is known about the specific nature of this impact or how impact varies between children of different ages.
As part of a larger cross-sectional study on the outcomes of children with severe BPD, we assessed the relationship between the specific health resource needs of the child and parental HRQoL, differences in parental HRQoL based on child’s age, and the subcategories within parental HRQoL that are particularly impacted. Additionally, we investigated how the parents’ HRQoL and family functioning differed for children with and without tracheostomies. A more complete understanding of how severe forms of BPD impact parental HRQoL and family functioning across childhood will help clinicians target support for families.
Methods
Participants and recruitment
We contacted parents or guardians of children who were cared for between May 2010 and November 2020 in the Neonatal Chronic Lung Disease (NeoCLD) Program at Children’s Hospital of Philadelphia (CHOP). This program treats patients who were referred from across the United States with the most severe forms of BPD. Seventy percent of transfers are from outside of the network of hospitals directly affiliated with CHOP. The CLD Program maintains a clinical registry of all program participants, which we used to identify eligible participants. Additional inclusion criteria for the current study were: the child was still alive and was 0–12 years old when the questionnaires were administered. There was no inclusion criteria based on BPD grade. We did not contact the families of deceased patients, but the age and cause of death were recorded from the electronic medical record. We used medical translators for non-English speaking participants to assist in completing the questionnaires. We contacted all eligible participants through phone calls. After three attempted phone calls without contact, we mailed a letter to the address on file. The CHOP Institutional Review Board deemed this study exempt (Category 2).
Data collection
A multidisciplinary group including physicians, nurses, social workers, and physical therapists, all with a focus on the clinical care and research related to children with severe BPD, selected validated instruments and additional questions to administer to parents. The group selected instruments that are valid across a wide age range, in children with a wide range of abilities, and appropriate for telephone administration. The final list of instruments collected information about:
-
1.
Quality of life as reflected in the PedsQL Inventory
-
2.
PedsQL Family Impact Module (PedsQL FIM) [16]
-
3.
Respiratory symptoms as recorded by the International Study of Asthma and Allergies in Childhood (ISAAC) [17,18,19]
-
4.
Child’s development as reflected in the Adaptive Behavior Assessment System (ABAS), 3rd Edition [20]
The group also designed tailored questionnaires to collect family demographic characteristics and data on the child’s health since discharge. They included the question: “In general, how would you describe your child’s health?” which parents were asked to respond to on a 5-point Likert scale poor to excellent.
We gathered most data from parent report during the interview. The CHOP electronic medical record and the NeoCLD Program registry were used to obtain additional demographic information, baseline perinatal characteristics of the child, and information about inpatient hospitalizations and outpatient care. When discrepant, parent reports were trusted over medical records. For example, if a parent reported a diagnosis of autism from an outside provider, the child was marked as having autism even if not indicated in our medical record. Per the 2019 NRN definition, BPD grade was based on level of respiratory support at 36 weeks [19]. The PedsQL forms include items scored on a 0–100 scale, with higher scores designating better quality of life. The PedsQL FIM includes 36 questions in 8 domains focused on concerns or difficulties the parents or family may have had due to their child’s health within the last month. The total score is calculated by averaging the eight domains: physical, emotional, social, and cognitive functioning, communication, worry, daily activities, and family relationships. The parent HRQoL summary score is calculated by averaging the physical, emotional, social, and cognitive functioning scores. The family functioning summary score is calculated by averaging the daily activities and family relationships scores.
Statistical analysis
We collected all data in a REDCap database. Only the study team had access to the data and subjects were assigned a unique participant number to protect confidentiality. We exported de-identified data to STATA v16.1 (College Station, TX) for analysis. For all variables, we calculated the percentage of children affected, mean values, and standard deviations. We assessed normality before selecting statistical tests. We examined the correlations between PedsQL FIM and several pre-specified primary outcomes using Wilcoxon rank sum or Spearman’s rank correlation coefficient, as appropriate, to assess for significant relationships and then used regression analysis to assess the magnitude of the correlations. To show results in association with ages of the children, the cohort was split into two groups: aged younger than five years or aged five years and older. Selecting the age of five allowed the young and older cohort to be similar in size, as well as accounted for a significant change in the lives of many families as this is the typical age in which children begin school. We prospectively designated the following variables as primary outcomes: respiratory support (yes or no), tracheostomy (ever placed), current medicines (number), current respiratory medicines (number), wheezing (ever in past 12 months), rehospitalizations (lifetime number), hearing or vision impairment (yes or no), poor weight gain, walking alone, cerebral palsy (CP, yes or no), developmental delay, autism, outpatient therapies (number of services), and parent-reported child health. For parent-reported health, we re-scaled the Likert rating of overall health to a 100-point scale to parallel the HRQoL metric and assessed the correlations between parental-reported health and PedsQL summary scores. We used linear regression to evaluate correlations between PedsQL FIM and child’s current age. We compared patient characteristics between respondents and non-respondents using t-tests. We did not correct for multiple comparisons as these analyses are exploratory in nature.
Results
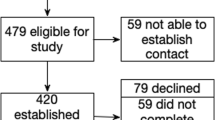
Between June 2021 and July 2022, our team collected information via phone interview on 568 children who were cared for by the NeoCLD Program at CHOP and survived to discharge. Eighty-nine of these children (16%) died after NICU discharge and were excluded from the study. We contacted 479 families, of whom 282 participated in the study (59% overall, 67% of those with whom we established contact). Birthweight, gestational age, gestational age at discharge, and child age at the time of attempted contact did not differ between respondents and nonrespondents (Supplementary Table 1). At the time of follow-up, the mean age in our cohort was 5.7 years (Table 1, SD 2.9). Our group previously published data that demonstrated children’s respiratory and developmental morbidities for this cohort were worse than any previously reported in the literature in terms of respiratory and developmental status [11].
The mean total score for PedsQL Family Impact Module (FIM) in the entire cohort was 76.7 (SD 22.3). Worry and daily activities were the lowest-scoring subsections. The highest-scoring subsections were cognitive functioning and family relationships (Table 2). The lowest scoring (highest concern) questions amongst all subsections were: I worry about my child’s future, I feel that others do not understand my family’s situation, it’s hard to find time for social activities, and I feel tired in the morning and throughout the day (Table 3). The questions with the highest scores (least concern) amongst all subsections were: I feel sick to my stomach, I feel physically weak, it is hard for me to tell doctors and nurses how I feel, I feel helpless or hopeless, and I feel angry.
The average summary scores and the respective subsections of the PedsQL did not change with the age of the child. Additionally, most of the ten lowest scoring questions (highest concern) remained consistent between parents of toddlers aged younger than five years old, and parents of children aged five years of age or older (Table 4). However, parents with children under the age of five years more often reported having difficulty finding time to finish household tasks and feeling too tired to finish household tasks. Parents of children older than five years more often reported worrying about how others will react to their child’s condition and feeling frustrated.
In regression analysis, the following child medical and developmental characteristics and outcomes were associated with worse PedsQL FIM score (ordered from greatest to least impact): Autism, tube feeds in the past year, wheezing in the past year, developmental delay, need for baseline respiratory support, not walking, parent-reported health, having had a tracheostomy, number of respiratory medications, number of total medications, number of outpatient therapies, and number of rehospitalizations (Fig. 1). Autism, tube feeds, and history of recent wheezing were associated with 11.3, 11.1, and 10.4 point reductions in PedsQL FIM score, respectively (Remainder of correlation coefficients provided in Supplementary Table 2). A diagnosis of CP, poor weight gain, vision and hearing impairment were not associated with PedsQL FIM.

Line thickness represents strength of correlation.
Discussion
We present parental HRQoL and family function outcomes for a referral cohort of children with BPD, the most severe cohort reported on a number of respiratory and developmental outcomes [11]. Compared to previous studies of families impacted by BPD that used the PedsQL FIM, parental HRQoL and family functioning were lower in all sub-scores in this more severe cohort [1, 7]. Scores were similar to one other study in a severe cohort [21]. HRQoL and family functioning scores were not higher in parents of older children, despite improvements in children’s physical health, including the decreased respiratory morbidity and more positive parental assessments of the child’s overall health, that we have previously reported [11]. A diagnosis of autism, a feeding tube, and having wheezed in the past year were most strongly correlated with HRQoL total scores, though many other respiratory and developmental outcomes also had important impacts on the family. Three elements of our findings warrant further discussion.
First, parents of older children did not report improved parental HRQoL and family functioning compared to parents of younger children, as would be consistent with studies in less severe BPD cohorts [1, 7,8,9]. This finding suggests that adaptation and improved respiratory symptoms seem insufficient to better family life. A plausible explanation is that although physical health of the children improves, the neurodevelopmental sequalae weigh more heavily on parents as the child ages. Nearly half of our participants were told by a doctor that their child had developmental delay and almost all of the children required an IEP for school [11]. Autism and developmental delay were also some of the most strongly associated outcomes with both parental QoL and child QoL in our cohort [11]. Problems with development may also lead parents to worry about future academic success and their children’s’ potential to gain independence, further impacting QoL. The shifts in the specific questionnaire items that were most problematic suggest a shift from difficulty with household tasks to concerns about how their child will engage with society and how others will react to their child’s disabilities. The severity of disease in this cohort likely explains the discrepancy between our reported stagnation of family outcomes, and other studies reported improvement. The impact on parents of school-age children with such severe BPD sequelae has not previously been reported.
Second, we found that many medical factors negatively impacted parental HRQoL and family functioning, presumably by increasing the burden of caring for children with severe BPD. Our findings that the severity of respiratory disease correlates with parental HRQoL and family functioning are consistent with prior work done in more mildly affected populations [1, 7]. However, our data suggest that respiratory morbidities do not convey the whole story, as autism and other developmental sequelae which are far more common in patients with severe BPD also have a major impact on families. While tracheostomies have often been used as an indicator of severe disease, they are no more correlated with parental HRQoL than the ability to walk or developmental delay. Surprisingly, however, tracheostomies were correlated more strongly with parents’ report of their own HRQoL than parent-reported child HRQoL. This is consistent with some prior work and further supports the hypothesis that while the parent’s perceived impact of the tracheostomy on the child was minimal, parents themselves were overwhelmed by the pressure of caregiving, were experiencing adverse effects on their sleep, and were worried about their child’s health after tracheostomy [22]. We were surprised to find that CP, poor weight gain, vision and hearing impairment were not associated with PedsQL FIM. Perhaps conditions that are stagnant rather than progressive or episodic better allow for parental adaptation. Overall, our findings suggest researchers should measure a wide variety of outcomes—rather than rely on respiratory morbidity— to capture the effect of severe BPD on families. Additionally, these results demonstrate the importance of clinicians understanding and addressing the many ways that a child’s clinical trajectory impacts parents over time.
Third, many of the issues cited as most problematic to family HRQoL are modifiable with additional support, particularly financial support. These issues include feeling tired, feeling like people don’t understand their situation, and lacking time for chores and social activities. Providing additional resources for families, such as access to respite care, home nursing, medical daycare, support groups and counseling has the potential to substantially improve the experiences of parents of children with BPD. Past studies have found that parental income in families of chronically ill children predicts positive quality of life and that peer support groups are helpful in reducing distress [23, 24]. Additionally, home nursing is highly valued by these families [25, 26]. Increasing access to resources like financial support and nursing for families of children with severe BPD would likely improve familial HRQoL and functioning. Several studies have demonstrated that increased family functioning leads to improved adherence to medical regimens and control of symptoms in children with chronic conditions [27,28,29].
Our study design has strengths and limitations. First, our cohort consists of children referred to a specialized program at a single center. However, this is also a strength because given the severity of BPD required for referral to the NeoCLD program at CHOP, our patient cohort provided an opportunity to study parental HRQoL for a common condition in its most severe form. This data is applicable to other centers that care for patients with severe disease. Second, our data collection overlapped with the beginning of the Coronavirus-19 pandemic, which could have led to further challenges for the families. However, our data largely represents outcomes prior to this period. Another limitation is that our data on post-discharge diagnoses are gathered through parental report rather than medical records. Still, it would be unlikely for parents to misremember important diagnoses, especially to overestimate. Another limitation is that our study was cross sectional rather than longitudinal, so age-related differences may in part reflect changes in standard care over time. Additionally, given that we interviewed each family at one moment in their lives, the circumstances outside of their child’s health status at that time may have influenced their responses. Finally, our response rate was relatively high for a follow up study [7, 30], and the baseline similarities between responders and non-responders are reassuring against sampling bias (Supplementary Table 1).
Conclusion
The present study captures the impact of severe BPD on parental HRQoL and family functioning. While the physical health of these children improves with age, and the nature of families’ concerns shift, parental HRQoL and family functioning are not improved in families with older children. This highlights the importance of evaluating and addressing not just respiratory morbidity in this population, but also the neurodevelopmental outcomes and healthcare utilization needs that continue well into childhood. Despite past evidence that parental HRQoL of children with BPD improves over time, our results demonstrate that families with particularly severe disease and significant neurodevelopmental sequalae experience continued impact throughout childhood. Additionally, these results suggest that families have different concerns and reasons for decreased HRQoL depending on the age of their children. Many of the parents’ specific concerns and struggles were modifiable. The data collected in this study can be used by physicians to identify the specific sequalae of BPD that have the largest impact on families and target those families for additional support. That concerns vary by age suggests that the most effective interventions may also vary by age and longitudinal follow up by expert providers in how severe BPD evolves over time is of the utmost importance. An enduring question is which interventions will most effectively target parental quality of life in these patients and what indicators can be used to predict the most effective interventions.
Data availability
All data is available upon request, which should be submitted to the corresponding author.
References
McGrath-Morrow SA, Ryan T, Riekert K, Lefton-Greif MA, Eakin M, Collaco JM. The impact of bronchopulmonary dysplasia on caregiver health related quality of life during the first 2 years of life. Pediatr Pulmonol. 2013;48:579–86.
Greenough A. Preschool healthcare utilisation related to home oxygen status. Arch Dis Child Fetal Neonatal Ed. 2006;91:F337–41.
Homan TD, Nayak RP. Short- and long-term complications of bronchopulmonary dysplasia. Respir Care. 2021;66:1618–29.
Smith VC, Zupancic JAF, McCormick MC, Croen LA, Greene J, Escobar GJ, et al. Rehospitalization in the first year of life among infants with bronchopulmonary dysplasia. J Pediatr. 2004;144:799–803.
Greenough A. Health care utilisation of infants with chronic lung disease, related to hospitalisation for RSV infection. Arch Dis Child. 2001;85:463–8.
Short EJ, Klein NK, Lewis BA, Fulton S, Eisengart S, Kercsmar C, et al. Cognitive and academic consequences of bronchopulmonary dysplasia and very low birth weight: 8-year-old outcomes. Pediatrics. 2003;112:e359.
Peralta GP, Piatti R, Haile SR, Adams M, Bassler D, Moeller A, et al. Respiratory morbidity in preschool and school-age children born very preterm and its association with parents’ health-related quality of life and family functioning. Eur J Pediatr. 2023;182:1201–10.
Berlin KEK, Scott W, Dawson S, Brousseau D, Lagatta JM. Health-related quality of life for parents of infants with bronchopulmonary dysplasia. J Pediatr. 2024;264:113773.
Lee DMX, Tan AKS, Ng YPM, Amin Z. Quality of life of patients and caregivers affected by bronchopulmonary dysplasia: a systematic review. Qual Life Res. 2023;32:1859–69.
Jobe AH. The new bronchopulmonary dysplasia. Curr Opin Pediatr. 2011;23:167–72.
Callahan KP, Farrell K, Gibbs K, Kielt MJ, Morris H, Nilan K, et al. Childhood outcomes following discharge from a referral bronchopulmonary dysplasia program. J Perinatol. 2024. https://www.nature.com/articles/s41372-024-02035-w.
Ehrenkranz RA, Walsh MC, Vohr BR, Jobe AH, Wright LL, Fanaroff AA, et al. Validation of the national institutes of health consensus definition of bronchopulmonary dysplasia. Pediatrics. 2005;116:1353–60.
Fairfax A, Brehaut J, Colman I, Sikora L, Kazakova A, Canadian Inherited Metabolic Diseases Research Network, et al. A systematic review of the association between coping strategies and quality of life among caregivers of children with chronic illness and/or disability. BMC Pediatr. 2019;19:215.
Stelmach I, Podlecka D, Smejda K, Majak P, Jerzyńska J, Stelmach R, et al. Pediatric Asthma Caregiver’s Quality of Life Questionnaire is a useful tool for monitoring asthma in children. Qual Life Res. 2012;21:1639–42.
Bemister TB, Brooks BL, Dyck RH, Kirton A. Parent and family impact of raising a child with perinatal stroke. BMC Pediatr. 2014;14:182.
Varni JW, Sherman SA, Burwinkle TM, Dickinson PE, Dixon P. The PedsQLTM Family Impact Module: preliminary reliability and validity. Health Qual Life Outcomes Health Qual Life Outcomes. 2004;2:55.
AsherWeiland. The International Study of Asthma and Allergies in Childhood (ISAAC). Clin Exp Allergy. 1998;28:52–66.
Asher M, Keil U, Anderson H, Beasley R, Crane J, Martinez F, et al. International Study of Asthma and Allergies in Childhood (ISAAC): rationale and methods. Eur Respir J. 1995;8:483–91.
Jensen EA, Dysart K, Gantz MG, McDonald S, Bamat NA, Keszler M, et al. The diagnosis of bronchopulmonary dysplasia in very preterm infants. an evidence-based approach. Am J Respir Crit Care Med. 2019;200:751–9.
Harrison P, Oakland T ABAS-3. 2021. Available from: https://www.pearsonassessments.com/store/usassessments/en/Store/Professional-Assessments/Behavior/Adaptive-Behavior-Assessment-System-%7C-Third-Edition/p/100001262.html.
Brady JM, Zhang H, Kirpalani H, DeMauro SB. Living with severe bronchopulmonary dysplasia—parental views of their child’s quality of life. J Pediatr. 2019;207:117–22.
Hopkins C, Whetstone S, Foster T, Blaney S, Morrison G. The impact of paediatric tracheostomy on both patient and parent. Int J Pediatr Otorhinolaryngol. 2009;73:15–20.
Toledano-Toledano F, Moral De La Rubia J, Nabors LA, Domínguez-Guedea MT, Salinas Escudero G, Rocha Pérez E, et al. Predictors of quality of life among parents of children with chronic diseases: a cross-sectional study. Healthcare. 2020;8:456.
Lancaster K, Bhopti A, Kern ML, Taylor R, Janson A, Harding K. Effectiveness of peer support programmes for improving well-being and quality of life in parents/carers of children with disability or chronic illness: a systematic review. Child Care Health Dev. 2023;49:485–96.
Baumgardner DJ, Burtea ED. Quality-of-life in technology-dependent children receiving home care, and their families-a qualitative study. WMJ Publ State Med Soc Wis. 1998;97:51–5.
Hatzmann J, Peek N, Heymans H, Maurice-Stam H, Grootenhuis M. Consequences of caring for a child with a chronic disease: employment and leisure time of parents. J Child Health Care. 2014;18:346–57.
Leeman J, Crandell JL, Lee A, Bai J, Sandelowski M, Knafl K. Family functioning and the well-being of children with chronic conditions: a meta-analysis. Res Nurs Health. 2016;39:229–43.
Psihogios AM, Fellmeth H, Schwartz LA, Barakat LP. Family functioning and medical adherence across children and adolescents with chronic health conditions: a meta-analysis. J Pediatr Psychol. 2019;44:84–97.
Cano-Garcinuño A, Mora-Gandarillas I, Bercedo-Sanz A, Callén-Blecua MT, Castillo-Laita JA, Casares-Alonso I, et al. Looking beyond patients: can parents’ quality of life predict asthma control in children?: Parents’ Quality of Life and Asthma Control. Pediatr Pulmonol. 2016;51:670–7.
Peacock JL, Lo JW, D’Costa W, Calvert S, Marlow N, Greenough A. Respiratory morbidity at follow-up of small-for-gestational-age infants born very prematurely. Pediatr Res. 2013;73:457–63.
Acknowledgements
We would like to thank Yasmin Broomand, Khoshbacht PT DPT PCS, Sarah Thomas, and Jennifer Strebel OTR/L for their help collecting data.
Funding
This work was supported by K01 Career Development Award Grant No. HG013114 from the National Human Genome Research Institute (KPC).
Author information
Authors and Affiliations
Contributions
KF collected data, analyzed the data, drafted the initial manuscript, and reviewed and revised the manuscript. KPC assisted in designing the study, analyzed the data, and reviewed and revised the manuscript. SBD conceptualized and designed the study, selected the study instruments, and reviewed and revised the manuscript. HM and KN collected the data and reviewed and revised the manuscript. KG assisted in designing the study and reviewed and revised the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study received institutional review board approval from Children’s Hospital of Philadelphia (Reference Number: 20-017548), and all parents included provided informed consent. This study was conducted in Accordance with the Declaration of Helsinki.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Farrell, K., DeMauro, S.B., Gibbs, K. et al. Health-related quality of life among families of children with severe bronchopulmonary dysplasia. J Perinatol 46, 200–205 (2026). https://doi.org/10.1038/s41372-025-02468-x
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41372-025-02468-x
