
Abstract
Background
Infants with congenital diaphragmatic hernia (CDH) remain at high risk for ECMO and mortality. We previously reported improved outcomes after implementing new CDH care guidelines. This study reassesses ECMO rates, survival, and guideline adherence to determine if improvements persisted.
Methods
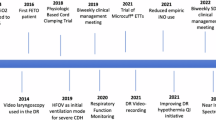
Retrospective review of all neonatal CDH cases at a single center during pre-guideline (2003–2015, n = 229) and post-guideline (2016–2024, n = 160) periods, with post-guideline subdivided into two epochs: post-1 (2016–2019, n = 70) and post-2 (2020–2024, n = 90).
Results
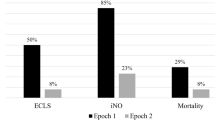
Survival without ECMO improved (pre-53%; post-1 74%; post-2 82%; p < 0.001), as did overall survival (72% vs. 83% vs. 86%; p = 0.006). ECMO use decreased (31% vs. 14% vs. 6%; p < 0.001). Inhaled nitric oxide use remained low, and vasoactive medication use dropped significantly in post-2.
Conclusion
Sustained survival improvement and reduced ECMO use followed guideline changes emphasizing minimal stimulation, gentle ventilation, delayed transfer, pre-ductal saturation monitoring, and limited vasoactive therapy.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on SpringerLink
- Instant access to the full article PDF.
USD 39.95
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others

Data availability
The data that support the findings of this study are not publicly available due to privacy and ethical restrictions but are available from the corresponding author upon reasonable request.
References
Ameis D, Khoshgoo N, Keijzer R. Abnormal lung development in congenital diaphragmatic hernia. Semin Pediatr Surg. 2017;26:123–8.
Chandrasekharan PK, Rawat M, Madappa R, Rothstein DH, Lakshminrusimha S. Congenital diaphragmatic hernia - a review. Matern Health Neonatol Perinatol. 2017;11:6.
Mohseni-Bod H, Bohn D. Pulmonary hypertension in congenital diaphragmatic hernia. Sem Pediatr Surg. 2007;16:126–33.
Gupta VS, Harting MT, Lally PA, Miller CC, Hirschl RB, Davis CF, et al. Congenital Diaphragmatic Hernia Study Group. Mortality in congenital diaphragmatic hernia: a multicenter registry study of over 5000 patients over 25 years. Ann Surg. 2023;277:520–7.
Wild KT, Hedrick HL, Ades AM, Fraga MV, Avitabile CM, Gebb JS, et al. Update on management and outcomes of congenital diaphragmatic hernia. J Intensive Care Med. 2024;39:1175–93.
van den Hout L, Schaible T, Cohen-Overbeek TE, Hop W, Siemer J, van de Ven K, et al. Actual outcome in infants with congenital diaphragmatic hernia: the role of a standardized postnatal treatment protocol. Fetal Diagn Ther. 2011;29:55–63.
Dimmer A, Stark R, Skarsgard ED, Puligandla PS. The promises and pitfalls of care standardization in congenital diaphragmatic hernia. Sem Pediatr Surg. 2024;33:151445.
Puligandla P, Skarsgard E, Baird R, Guadagno E, Dimmer A, Ganescu O, et al. Canadian Congenital Diaphragmatic Hernia Collaborative. Diagnosis and management of congenital diaphragmatic hernia: a 2023 update from the Canadian Congenital Diaphragmatic Hernia Collaborative. Arch Dis Child Fetal Neonatal Ed. 2024;109:239–52.
Puligandla PS, Grabowski J, Austin M, Hedrick H, Renaud E, Arnold M, et al. Management of congenital diaphragmatic hernia: a systematic review from the APSA outcomes and evidence based practice committee. J Pediatr Surg. 2015;50:1958–70.
Snoek KG, Reiss IK, Greenough A, Capolupo I, Urlesberger B, Wessel L, et al. CDH EURO Consortium. Standardized postnatal management of infants with congenital diaphragmatic hernia in Europe: the CDH EURO consortium consensus - 2015 update. Neonatology. 2016;110:66–74.
Ito M, Terui K, Nagata K, Yamoto M, Shiraishi M, Okuyama H, et al. Clinical guidelines for the treatment of congenital diaphragmatic hernia. Pediatr Int. 2021;63:371–90.
Jancelewicz T, Brindle ME, Guner YS, Lally PA, Lally KP, Harting MT, et al. Toward standardized management of congenital diaphragmatic hernia: an analysis of practice guidelines. J Surg Res. 2019;243:229–35.
Yang MJ, Fenton S, Russell K, Yost CC, Yoder BA. Left-sided congenital diaphragmatic hernia: can we improve survival while decreasing ECMO?. J Perinatol. 2020;40:935–42.
Lichtsinn K, Waltz PK, Azzuqa A, Church J, Graham J, Troutman J, et al. Impact of a standardized management guideline for infants with CDH: a single-center experience. J Pediatr Surg. 2023;58:389–96.
Wild KT, Hedrick HL, Rintoul NE, Ades AM, Gebb JS, et al. Golden hour management of infants with congenital diaphragmatic hernia: 15 year experience at a high-volume center. J Perinatol. 2025;45:1247–54.
Bromiker R, Sokolover N, Ben-Hemo I, Idelson A, Gielchinsky Y, Almog A, et al. Congenital diaphragmatic hernia: quality improvement using a maximum lung protection strategy and early surgery improved survival. Eur J Pediatr. 2024;183:697–705.
Mesas Burgos C, Gatzinsky V, Nord P, Gustafson E, Stenstrom P, Winberg H, et al. Impact of centralization of care for patients with congenital diaphragmatic hernia in Sweden. J Pediatr Surg. 2025;60:162314.
Cox KJ, Fenton SJ, Yang ML, Russell KW, Yost CC, Yoder BA. Operative repair in congenital diaphragmatic hernia: how long do we really need to wait?. J Pediatr Surg. 2022;57:17–23.
Gebb J, Flohr S, Mathew L, Oliver ER, Barr K, Gallagher T, et al. Observed/expected lung-to-head ratio and total lung volumes that identify fetuses with severe congenital diaphragmatic hernia in a North American fetal center. Prenat Diagn. 2025;45:676–85.
Kahan AM, Glasgow SL, Yoder BA, Yang M, Yost CC, Peterson K, et al. Less is more: ECMO utilization and outcomes in congenital diaphragmatic hernia. J Pediatr Surg. 2025:162571. https://doi.org/10.1016/j.jpedsurg.2025.162571.
Shekelle PG, Ortiz E, Rhodes S, Morton SC, Eccles MP, Grimshaw JM, et al. Validity of the Agency for Healthcare Research and Quality clinical practice guidelines: how quickly do guidelines become outdated?. JAMA. 2001;286:1461–7.
Yang MJ, Carpenter R, Russell KW, Fenton SJ, Yost CC, Yoder BA. Are early, frequent echocardiograms necessary to improve outcomes of neonates with congenital diaphragmatic hernia?. J Pediatr. 2025;280:114510.
Byrd C, Nogee J, Gilmore MM, Baschat A, Keiser A, Organ J, et al. Clinical outcomes after implementation of a physiologic pre-operative management strategy in neonates with congenital diaphragmatic hernia. J Perinatol. 2025;45:1240–6.
Gallot D, Boda C, Ughetto S, Perthus I, Robert-Gnansia E, Francannet C, et al. Prenatal detection and outcome of congenital diaphragmatic hernia: a French registry-based study. Ultrasound Obstet Gynecol. 2007;29:276–83.
Stringer MD, Goldstein RB, Filly RA, Howell LJ, Sola A, Adzick NS, et al. Fetal diaphragmatic hernia without visceral herniation. J Pediatr Surg. 1995;30:1264–6.
Bronshitein M, Lewit N, Sujov PO, Makhoul IR, Blazer S. Prenatal diagnosis of congenital diaphragmatic hernia: timing of visceral herniation and outcome. Prenat Diagn. 1995;15:695–8.
Shanmugam H, Brunelli L, Botto LD, Krikov S, Feldkamp ML. Epidemiology and prognosis of congenital diaphragmatic hernia: a population-based cohort study in Utah. Birth Defects Res. 2017;109:1451–9.
Carmichael SL, Ma C, Lee HC, Shaw GM, Sylvester KG, et al. Survival of infants with congenital diaphragmatic hernia in California: impact of hospital, clinical, and sociodemographic factors. J Perinatol. 2020;40:943–51.
Author information
Authors and Affiliations
Contributions
Drs. Yang and Yoder participated in study design, data analysis, and manuscript writing. Drs. Carpenter, Yost, Kahan, Russell, and Fenton participated in manuscript writing. All authors agree with the final draft of this manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
All study methods were performed in accordance with the relevant guidelines and regulations, including institutional, national, and international research standards. Approval for this study was obtained from the University of Utah/Primary Children’s Hospital IRBs, under protocol IRB_00182610, which was determined to be exempt from full review. As part of this exempt determination, the Institutional Review Board granted a waiver of informed consent.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Yang, M.J., Carpenter, R.J., Yost, C.C. et al. Congenital diaphragmatic hernia: are improvements in ECMO & survival sustainable over time?. J Perinatol (2026). https://doi.org/10.1038/s41372-026-02605-0
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41372-026-02605-0
