
Abstract
Background
Immediate Kangaroo Mother Care (iKMC) after delivery and delayed cord clamping (DCC), both improve cardiorespiratory stability in newborns.
Methods
This prospective observational study included 96 moderate to late preterm (MLPT) neonates. Preductal pulse oximetry (SpO₂) and heart rate (HR) were recorded during the first 10 min after birth. Neonates who received iKMC and DCC were compared to those who did not receive iKMC.
Results
iKMC was performed in 64.6% of the infants. The iKMC group showed a non-significant trend toward higher SpO₂ levels. Mean SpO₂ was 76.06% in the iKMC group versus 70.98% in the non-iKMC group; at 420 s, it was 95.13% versus 93.77%. HR was significantly higher in the iKMC group at all time points, averaging 102.2 bpm at 120 s compared to 87.1 bpm in the non-iKMC group.
Conclusions
Combining iKMC with DCC improves hemodynamic stability and oxygenation in MLPT infants, with higher HR and earlier stabilization of SpO₂ levels.
Similar content being viewed by others


Introduction
Moderate to late preterm (MLPT) neonates, including infants born between 32+0 and 33+6 (moderate) and 340 to 36+6 (late) weeks of gestation, often require active resuscitation. Therefore, interventions that favor postnatal stabilization are of particular interest. In high-income countries (HIC), MLPT accounts for 71.8% of all preterm deliveries [1].
Kangaroo mother care (KMC) is defined as the direct interaction between the newborn and the naked torso of the mother after birth. KMC enhances infant’s temperature regulation, promotes breastfeeding, and fosters a strong bond between mother and child. It is prioritized in low- and middle-income countries (LMIC) as a key strategy to enhance neonatal health outcomes and increase survival rates, particularly for low birth-weight (LBW) infants [2, 3]. The physiological mechanism underlying KMC involves skin-to-skin contact that activates thermoregulatory and neuroendocrine pathways, including the release of oxytocin and modulation of the autonomic nervous system. These responses help stabilize vital parameters such as heart rate (HR) and oxygen saturation (SpO₂) in preterm and term newborns [4], and have been associated with reduced mortality at 28 days when implemented immediately after birth [3].
Delayed cord clamping (DCC), defined as delaying at least 60 s before clamping the umbilical cord, has been shown to facilitate cardiopulmonary transition at birth. Placental transfusion increases blood volume, enhances pulmonary gas exchange, and stabilizes HR during the immediate postnatal period [5,6,7].
We hypothesized that in MPLTs, the simultaneous combination of iKMC and DCC would enhance earlier stabilization of SpO2 and HR compared with those not receiving iKMC.
Population & methodos
Study design
Post-hoc analysis from an observational cohort study conducted at the Hospital Universitario y Politécnico La Fe (Valencia, Spain) [7].
SpO2, HR, time of DCC, and iKMC time during stabilization were recorded in MLPT infants born by vaginal delivery or cesarean section after an uncomplicated pregnancy that did not require stabilization maneuvers in the delivery room (DR). GA was defined according to the criteria of the Spanish Society of Obstetrics and Gynecology (SEGO) [8]. All neonates underwent skin stimulation to improve spontaneous breathing [9].
Ethics
The study was approved by the Medical Research Ethics Committee (ID = 2021-275-1). Parents/legal guardians signed the informed consent.
Population, study interventions, and monitoring
Inclusion criteria were MLPT (320–36⁶ weeks) born after uncomplicated pregnancies, who did not require stabilization maneuvers in the delivery room. Exclusion criteria included major congenital malformations, need for resuscitation, and/or maternal contraindications for iKMC. The comparison was made between infants who received iKMC and those who did not (non-iKMC), to assess early physiological adaptation. Mode of delivery (vaginal or cesarean) was considered one of the contextual factors influencing iKMC implementation according to institutional protocols.
Midwives and neonatal nurses handled all the infants in the DR. Preductal SpO2 and HR were retrieved for 10 min after fetal expulsion and stored [7]. Cord clamping was delayed for ≥ 60 s according to the Spanish guidelines [8]. iKMC was offered to clinically stable infants, following established criteria for stability (Apgar ≥8 at 1 min, no need for respiratory support). Cesarean deliveries were performed according to obstetric indications, independent of neonatal status, and the decision for iKMC followed standard clinical procedures. Infants requiring stabilization maneuvers were excluded from iKMC.
In vaginal deliveries, the newborn was placed on the mother’s lower abdomen or thighs, approximately at the level of the placenta, with the cord unclamped for ≥ 60 s and gentle tactile stimulation to encourage spontaneous breathing. In cesarean deliveries, the newborn was placed on the mother’s thighs, covered with pre-warmed cloths, maintaining the cord intact for the same period. After DCC, clinically stable newborns were transferred skin-to-skin to the mother’s chest to initiate iKMC.
The investigators were not involved in clinical decisions or interventions regarding the delivery and postnatal stabilization of the newborn. Monitor alarms were not silenced during resuscitation procedures. All infants requiring stabilization maneuvers were excluded from the study.
HR and preductal SpO₂ were continuously measured using a Masimo SET Masimo M-LNCS Neo sensor (Low Noise Cabled Sensor, Irvine, CA) placed on the right hand/wrist and connected to the Masimo Rad-97 Pulse CO-Oximeter®. The sensor was applied before connection to improve the reliability and speed of displayed data. Measurements were recorded at 2-second intervals with maximum sensitivity (HR sensitivity: 3 bpm for a 25–240 bpm range; SpO₂ sensitivity: 3% for a 60–80% range). All data were exported as .csv files for subsequent analysis, enabling precise assessment of neonatal physiological parameters during the first 10 min after birth.
Statistical analysis
The data were summarized as mean (standard deviation, SD) and median (first and third quartiles) for continuous variables, and as relative and absolute frequencies for categorical variables. The statistical analysis was divided into two parts:
First, SpO2 and HR percentiles were calculated using generalized least squares regression with the rms R package (v 5.4-1, R Foundation for Statistical Computing, Vienna, Austria) [10]. Relevant variables such as gestational age, sex, iKMC, and delivery mode (vaginal/C-section) were included in the model. Additionally, a within-group correlation structure was introduced to correct for non-independent observations. SpO2 values equal to 100 were changed to 99.9 and divided by 100 for a logit transformation. Nonlinear relationships between time (in minutes) and the response variables were modeled using natural splines. Percentiles were calculated using the quantile function for the standard normal distribution. Each model’s estimated residual standard error was multiplied by the corresponding value of a standard normal distribution for the required quantile and added to the predicted mean. Logit-transformed SpO2 percentile values were back-transformed to display the results.
Second, to compare percentiles based on whether iKMC had been performed, the skewness-median-coefficient of variation (LMS) method described by Cole et al. [11] was applied. Results were fitted using the gamlss R package (v 5.1-6). Statistical analyses were conducted using R statistical software (v 3.6.1).
Results
A total of 96 preterm neonates with a median gestational age of 35 weeks (34–36) and a mean birth weight of 2294.8 ± 397 g were included in the study. Table 1 provides clinical information on the mothers and neonates. The median DCC time was 70 s. Baseline sociodemographic and perinatal characteristics the iKMC and non-iKMC groups are shown in the Supplementary Table 1. No significant differences were assessed between the study groups.
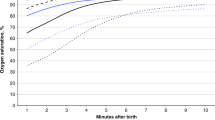
Table 2 shows the values of SpO2 for each time point. SpO₂ was 8% higher in the iKMC than in the non-iKMC group across all time points; however, this difference did not reach statistical significance (p = 0.082). At 120 s of life, neonates in the iKMC group had a mean SpO₂ of 76.3% (95% CI: 65.4–84.2) compared to 71% (95% CI: 63.2–77.7) in the non-iKMC group. This trend persisted in subsequent measurements, reaching a mean SpO₂ of 88.9 (95% CI: 87–92) at 300 s in the iKMC group, compared to 92% (95% CI: 87.5–95) in the non-iKMC groups. Figure 1 depicts the time-dependent progression of SpO₂ in both groups during the first minutes of life.

The x-axis represents time (minutes) and the y-axis oxygen saturation (%). Solid lines indicate median values, and dashed lines represent the 3rd, 50th, and 97th percentiles. Neonates with iKMC showed consistently higher SpO₂ values throughout this period.
Table 3 shows HR values at different time points. At 120 s after birth, the iKMC group had a mean HR of 102.2 bpm (95% CI: 88.9–117.5) compared to 90.1 bpm (95% CI: 87.7–98.5) in the non-iKMC group. At 300 s after birth, the iKMC group showed a mean HR of 135.2 bpm (95% CI: 120.7–149.7) compared to 120 bpm mean in the non-iKMC group (95% CI: 109–130.3). HR was consistently and significantly (p = 0.013) higher in the iKMC group throughout the study.
Figure 2 depicts evolving HR in the first minutes after birth. Statistically significant differences (p = 0.013) between iKMC and non-iKMC groups were assessed, with values approximately 14% higher in neonates who received iKMC.

The x-axis represents time (minutes) and the y-axis heart rate (beats per minute). Solid lines indicate median values, and dashed lines represent the 3rd, 50th, and 97th percentiles.
The statistical analysis included key variables such as gestational age, type of delivery, sex, umbilical artery pH at birth, neonatal weight and adjustments made in the SpO2 analysis. These methodological controls aimed to ensure that the physiological differences between groups could be attributed to the intervention and not to the baseline characteristics of delivery-related factors.
Table 4 informs on the body temperature in both groups at different timings. At 2–3 min of life, the iKMC group had a significantly higher mean temperature (36.1 ± 1 °C) compared with the non-iKMC group (35.8 ± 1 °C; p = 0.041). This difference increased at 5 min after birth (iKMC vs. non-iKMC: 36.4 ± 0.60 °C vs. 36.1 ± 0.7 °C; p = 0.018), and reach a peak at 10 min after birth (36.6 ± 0.5 °C vs. 36.3 ± 0.7 °C; p = 0.003). At the time of protocol entry or termination, the iKMC-exposed group maintained a significant thermal advantage (36.6 ± 0.5 °C vs. 36.3 ± 0.5 °C; p = 0.009).
Discussion
MLPT infants subjected to DCC plus iKMC achieved physiologic HR and SpO2 earlier than those with delayed KMC (non-iKMC group). These findings suggest that the combination of iKMC and DCC contributes to improved cardiovascular and respiratory adaptation in the transition to extrauterine life, in line with previous studies that have documented the physiological benefits of these interventions in vulnerable neonates [3, 12, 13].
Although our results showed a 14% higher heart rate (HR) in neonates receiving iKMC, this finding should be interpreted within the hemodynamic context of birth transition. In the third trimester, fetal HR typically ranges between 120 and 160 bpm, reflecting the high sympathetic tone of intrauterine life. From this perspective, the increased HR observed in the iKMC group may indicate a more physiologic transition from fetal to extrauterine circulation. iKMC contact may contribute to this process by reducing external stressors and mimicking the uterine thermal, tactile, and olfactory environment. Further studies, including autonomic markers such as HR variability or stress-related biomarkers, are needed to validate this interpretation.
The autonomic nervous system plays a key role in the fetal-to-neonatal transition, influencing HR regulation and oxygenation. Previous research has shown that iKMC modulates autonomic activity, promoting greater sympathetic-parasympathetic balance and reducing physiological stress in the neonate [14, 15]. In addition, KMC has been documented to enhance central nervous system maturation, which promotes HR regulation and cardiorespiratory stability in preterm and low birth weight neonates [16, 17]. An observational study showed that iKMC significantly reduced SpO2 and HR variability, compared to incubator care. In addition, KMC accelerates the maturation of vagal tone and improves state organization, suggesting faster maturation of the autonomic system [18].
DCC optimizes placental transfusion, increasing blood volume and improving oxygenation during the first minutes of life. A recent study by Padilla et al. (2021) [5] demonstrated that DCC is associated with higher SpO₂ levels and faster stabilization of HR, reducing episodes of bradycardia and tachycardia in term neonates.
Our data align with previous findings by Ashish et al. in neonates ≥33 weeks, where DCC was associated with higher SpO₂ values during early postnatal life [19]. In our cohort, a trend toward improved oxygenation was observed in iKMC + DCC infants although it didn’t reach statistical significance
iKMC contact improves thermoregulation and reduces temperature variability in preterm neonates [17, 19,20,21]. In our cohort, neonates exposed to iKMC showed significantly higher temperatures at all measured intervals, with the most pronounced difference observed at 10 min postpartum (+0.32 °C, *p* = 0.003).
The study has several limitations. HR during the fetal-to-neonatal transition was measured using pulse oximetry, a technique widely used in clinical practice because of its availability and ease of application. However, several studies have highlighted the limitations of this method, especially in the first minutes of life when it can experience delays in obtaining a stable signal and tends to underestimate the actual HR [22, 23]. In contrast, electrocardiography (EKG) provides a more accurate and faster HR signal, crucial for timely clinical decision-making during neonatal resuscitation [24, 25]. Recent literature supports the superiority of EKG over pulse oximetry for detecting bradycardia, particularly in preterm neonates [22], and suggests that using both technologies together significantly improves accuracy in hemodynamic monitoring [24, 25]. Consistent with these recommendations, phase II of the study has incorporated EKG monitoring to assess HR during neonatal transition, aiming to align the methodology with the latest scientific evidence and improve the accuracy of cardiovascular monitoring. Additionally, the generalizability of our findings is limited because infants who required resuscitation or advanced stabilization at birth were excluded [26,27,28]. Therefore, our results apply specifically to clinically stable moderate and late preterm neonates born after uncomplicated pregnancies. Future studies should include a broader spectrum of MLPT infants, including those requiring stabilization, to better assess the effects of iKMC and delayed cord clamping across the full range of clinical presentations.
Conclusions
Combining iKMC and DCC promotes hemodynamic stability during fetal-to-neonatal transition in MPLT infants. In our cohort, iKMC was associated with a significantly higher HR and earlies achievement of a stable SpO2 in the first minutes after birth. These findings underscore potential short-term physiological benefits of applying both interventions simultaneously. Further research is necessary to evaluate their long-term clinical effects and applicability in different delivery settings. applicability to neonates requiring stabilization maneuvers.
Data availability
The datasets generated and/or analyzed during the current study are not publicly available due to privacy and ethical restrictions but are available from the corresponding author on reasonable request.
References
Boyle EM, Johnson S, Manktelow B, Seaton SE, Draper ES, Smith LK, et al. Neonatal outcomes and delivery of care for infants born late preterm or moderately preterm: a prospective population-based study. Arch Dis Child Fetal Neonatal Ed. 2015;100:F479–85.
Ahmed S, Mitra SN, Chowdhury AM, Jamil K, Baqui AH, Black RE, et al. Community Kangaroo Mother Care: Implementation and potential for neonatal survival and health in very low-income settings. J Perinatol. 2011;31:361–7.
Arya S, Naburi H, Kawaza K, Newton S, Anyabolu CH, Bergman N, et al. Immediate “Kangaroo Mother Care” and Survival of Infants with Low Birth Weight. N Engl J Med. 2021;384:2028–38.
Sehgal A, Nitzan I, Jayawickreme N, Menahem S. Impact of Skin-to-Skin Parent-Infant Care on Preterm Circulatory Physiology. J Pediatr. 2020;222:91–97.e2.
Padilla-Sánchez C, Baixauli-Alacreu S, Cañada-Martínez AJ, Lara-Cantón I, Parra-Llorca A, Torres B, et al. Delayed vs Immediate Cord Clamping Changes Oxygen Saturation and Heart Rate Patterns in the First Minutes After Birth. J Pediatr. 2020;227:149–56.
Lara-Cantón I, Badurdeen S, Dekker J, Castañar-Pérez C, Álvarez-Palacios B, García-Muñoz Rodrigo F, et al. Oxygen Saturation and Heart Rate in Healthy Term and Late Preterm Infants With Delayed Cord Clamping. Pediatr Res. 2024;96:604–9.
Valles-Murcia N, Solaz-García Á, Pinilla-González A, Torrejón-Rodriguez L, Gormaz M, Escrig-Fernández R, et al. Reference ranges for preductal oxygen saturation and heart rate in moderate and late preterm infants with deferred cord clamping. Neonatology. 2025;122:161–70.
Sociedad Española de Ginecología y Obstetricia (SEGO). Control prenatal del embarazo normal. Progresos de Obstetricia y Ginecología. 2018;61. (Online). Available: https://sego.es/documentos/progresos/v61-2018/n5/GAP_Control%20prenatal%20del%20embarazo%20normal_6105.pdf
Wyckoff MH, Wyllie J, Aziz K, de Almeida MF, Fabres J, Fawke J, et al. Neonatal Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2020;142:S185–S221.
Harrell FE Jr rms: Regression Modeling Strategies. In: R Package Version 5.1-4. Vienna, Austria: R Foundation for Statistical Computing; 2019.
Cole TJ, Green PJ. Smoothing reference centile curves: The LMS method and penalized likelihood. Stat Med. 1992;11:1305–19.
Solaz-García Á, Lara-Cantón I, Pinilla-González A, Montejano-Lozoya R, Gimeno-Navarro A, Sánchez-Illana Á, et al. Impact of Kangaroo Care on Premature Infants’ Oxygenation: Systematic Review. Neonatology. 2022;119:537–46.
Medvedev MM, Tumukunde V, Kirabo-Nagemi C, Greco G, Mambule I, Katumba K, et al. Process and costs for readiness to safely implement immediate kangaroo mother care: a mixed methods evaluation from the OMWaNA trial at five hospitals in Uganda. BMC Health Serv Res. 2023;23:613.
Zengin H, Suzan OK, Hur G, Kolukısa T, Eroglu A, Cinar N. The effects of kangaroo mother care on physiological parameters of premature neonates in neonatal intensive care unit: A systematic review. J Pediatr Nurs. 2023;71:e18–e27.
Tian Y, Inocencio IM, Sehgal A, Wong FY. Impact of Kangaroo mother care on autonomic cardiovascular control in foetal-growth-restricted preterm infants. Pediatr Res. 2025;97:1983–8.
Feldman R, Eidelman AI. Skin-to-skin contact (Kangaroo Care) accelerates autonomic and neurobehavioural maturation in preterm infants. Dev Med Child Neurol. 2003;45:274–81.
Hucklenbruch-Rother E, Vohlen C, Mehdiani N, Keller T, Roth B, Kribs A, et al. Delivery room skin-to-skin contact in preterm infants affects long-term expression of stress response genes. Psychoneuroendocrinology. 2020;122:104883.
Sehgal A, Yeomans EJ, Nixon GM. Kangaroo mother care improves cardiorespiratory physiology in preterm infants: an observational study. Arch Dis Child Fetal Neonatal Ed. 2024;109:628–33.
Durmaz A, Sezici E, Akkaya DD. The effect of kangaroo mother care or skin-to-skin contact on infant vital signs: A systematic review and meta-analysis. Midwifery. 2023;125:103771.
Kardum D, Bell EF, Grčić BF, Müller A. Duration of skin-to-skin care and rectal temperatures in late preterm and term infants. BMC Pregnancy Childbirth. 2022;22:655.
Lode-Kolz K, Hermansson C, Linnér A, Klemming S, Hetland HB, Bergman N, et al. Immediate skin-to-skin contact after birth ensures stable thermoregulation in very preterm infants in high-resource settings. Acta Paediatr. 2023;112:934–41.
van Vonderen JJ, Hooper SB, Kroese JK, Roest AA, Narayen IC, van Zwet EW, et al. Pulse oximetry measures a lower heart rate at birth compared with electrocardiography. J Pediatr. 2015;166:49–53.
Khoury R, Klinger G, Shir Y, Osovsky M, Bromiker R. Monitoring oxygen saturation and heart rate during neonatal transition. comparison between two different pulse oximeters and electrocardiography. J Perinatol. 2021;41:885–90.
Katheria A, Rich W, Finer N. Electrocardiogram provides a continuous heart rate faster than oximetry during neonatal resuscitation. Pediatrics. 2012;130:e1177–81.
Gulati R, Zayek M, Eyal F. Presetting ECG electrodes for earlier heart rate detection in the delivery room. Resuscitation. 2018;128:83–7.
Tas Arslan F, Akkoyun S, Küçükoğlu S, Kocoglu-Tanyer D, Konak M, Soylu H. Effect of kangaroo mother care on cerebral oxygenation, physiological parameters, and comfort levels in late-premature infants: A randomized controlled trial. Midwifery. 2024;137:104096.
Solaz-García Á, Sánchez-Illana Á, Lara-Cantón I, Montejano-Lozoya R, Gimeno-Navarro A, Pinilla-González A, et al. Analysis of Fractional Cerebral Oxygen Extraction in Preterm Infants during the Kangaroo Care. Neonatology. 2023;120:508–16.
Popat H, Galea C, Evans N, Lingwood B, Colditz PB, Halliday R, et al. Effect of Delayed Cord Clamping on Cerebral Oxygenation in Very Preterm Infants. Neonatology. 2019;115:13–20.
Acknowledgements
We want to express our gratitude to the neonates and their families whose participation was indispensable for the development of this study. We would also like to extend our gratitude to the obstetrics and perinatology team of the University and Polytechnic Hospital La Fe (HULAFE) for their involvement in this project.
Author information
Authors and Affiliations
Contributions
N.V.-M., M.A., M.V., and Á.S.-G. conceived and designed the study. N.V.-M., A.P.-G., L.T.-R., A.C.-H., P.S.-G., and R.E.-F. contributed to patient recruitment and data collection. A.G.-T., L.C.-G.,M.C.; N.V.-M. and Á.S.-G., contributed to data curation and statistical analysis. N.V.-M. and Á.S.-G., drafted the initial version of the manuscript. M.A., M.V., Á.S.-G., and M.C. critically revised the manuscript for important intellectual content. All authors contributed to the interpretation of the results, reviewed the manuscript, and approved the final version for publication.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
ETHICAL STATEMENT
This study protocol was reviewed and approved the Comité de Ética e Investigación Médica of the University and Polytechnic Hospital La Fe (Valencia) with the approval number: # 2021-275-1. Parents/guardians signed the informed consent. This study was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Valles-Murcia, N., Aguar, M., Pinilla-González, A. et al. “Impact of delayed cord clamping and immediate kangaroo mother care on oxygen saturation and heart rate in moderate and late preterm infants”. J Perinatol (2026). https://doi.org/10.1038/s41372-026-02652-7
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41372-026-02652-7
