
Abstract
Off-label hypomethylating agents and venetoclax (HMA/VEN) are often used for relapsed and refractory (R/R) AML patients. However, predictors of outcome are elusive. The objective of the current retrospective observational multicenter study of 240 adult patients (median age 68.6 years) with R/R AML was to establish a prognostic risk score. Overall response was documented in 106 (44%) patients. With a median follow-up of 31.5 months, 179 deaths were recorded. Median overall survival (mOS) was 7.9 months. In multivariate analysis of the subgroup with molecular information (n = 174), risk factors for inferior survival included the presence of extramedullary disease, HMA pretreatment and mutations in NF1, PTPN11, FLT3, and TP53, whereas mutated SF3B1 was identified as favorable risk factor. These risk factors were subsequently applied to construct an HR-weighted risk model that allocated patients to one of three risk groups with significantly different survival outcomes: favorable (n = 46; mOS 21.4 months), intermediate (n = 75; mOS 7.5 months), and adverse (n = 53; mOS 4.6 months; p < 0.001). The model was validated in 189 AML patients treated with HMA/VEN in first line. This clinical-molecular, 3-tiered venetoclax prognostic risk score (VEN-PRS) for HMA/VEN treatment outcomes in R/R AML patients will support the selection of appropriate treatment options in this high-risk population.

Similar content being viewed by others

Introduction
Despite substantial progress in the development of new therapeutic strategies, relapsed and refractory (R/R) acute myeloid leukemia (AML) is associated with poor outcome and still represents an underserved medical condition [1]. The prognosis of R/R AML patients depends on many factors including age, prior therapy including allogeneic hematopoietic cell transplantation (alloHCT), timing of relapse, and the mutational as well as the cytogenetic profile of the disease at relapse [2]. According to the European LeukemiaNet (ELN) primary refractory disease is defined as failing to achieve complete remission (CR) after two cycles of intensive chemotherapy (including at least one cycle of intermediate dose cytarabine) [3]. Ferguson et al. additionally defined an insufficient response to the first induction – i.e. less than 50% reduction in blasts and the presence of more than 15% blasts – as primary refractory disease since it was shown that these patients have an equally poor prognosis as patients with primary refractory disease defined by ELN [4]. Primary refractory disease is reported in approximately 25–30% of patients and is associated with poor outcome due to limited salvage options with low response rates [5]. A retrospective study by Zeichner et al. reported a median overall survival (OS) of only 4 months in patients with R/R AML [6]. Risk factors associated with primary refractory AML include a complex or monosomal karyotype, advanced age, and an increased time to blast clearance in the bone marrow or peripheral blood [7,8,9]. In patients with hypomethylating agents, the current ESMO Clinical Practice Guideline suggests to assess response at the very least after four cycles of non-intensive therapy to diagnose refractory disease [10].
Relapse is diagnosed in patients who have achieved a CR or CR with incomplete hematologic recovery (CRi) but show a reappearance of blasts in the bone marrow ≥5%, reappearance of blasts in the blood in at least 2 peripheral blood samples at least one week apart, or the development of extramedullary AML [3]. In a large analysis of more than 3000 patients treated with intensive frontline chemotherapy, approximately 60% of patients suffered from relapse after a median of 7.2 months after achieving a CR [11].
In patients with relapsed AML treated with intensive chemotherapy, Breems et al. identified patient and disease characteristics to predict outcomes of patients in first relapse. Based on the parameters length of relapse-free interval after first CR, cytogenetics at diagnosis, age at relapse, and prior alloHCT, patients were stratified into favorable-, intermediate-, or poor-risk groups, with associated 5-year OS of 46%; 18% and 4%, respectively [12].
There is no standard salvage therapy in R/R AML, particularly in older patients [3, 10]. Feasible options include enrollment into clinical trials and use of targeted therapies such as gilteritinib for AML with FLT3 mutation [10, 13], combination of the BCL-2 inhibitor venetoclax (VEN) with HMA, or cytarabine-based salvage chemotherapy [14, 15]. Response to HMA/VEN salvage treatment is reported in 20–40% of R/R AML patients with a median OS of 3.3–11.2 months [16,17,18,19,20,21].
However, prognostic factors associated with outcome to venetoclax-based regimens remain sparse. Therefore, precise, robust and applicable prognostic models for predicting long-term survival, stratifying risk groups, and helping with therapeutic decision-making in R/R AML is still an unmet clinical need.
In the current study of 240 patients with R/R AML receiving HMA and VEN we aimed to (I) assess efficacy of HMA/VEN in a large cohort of R/R AML patients, (II) determine clinical and genetic predictors of response, event-free survival (EFS) and OS, and (III) develop an integrative response, EFS and OS model to support treatment decisions.
Patients and methods
Patients aged 18 years or older with refractory or relapsed (R/R) acute myeloid leukemia (AML) as defined by the 2022 International Consensus Classification of Myeloid Neoplasms and Acute Leukemias (ICC) [22], who had been treated with VEN combined with HMA and had been reported to the venetoclax registry (venreg.org; ClinicalTrials.gov NCT03662724) were included in the analysis. The venetoclax registry is a multicenter, prospective, observational cohort study initiated in 2018, which allowed retrospective patient inclusion until 2017 [23]. In the current analysis patients were included from eight academic centers in Germany and Austria. Patients receiving low-dose cytarabine or other non-HMA combinations with VEN were excluded. Extramedullary disease was evaluated clinically and considered as reported by the investigators to the registry. All patients provided written informed consent to the off-label use of VEN, genetic analysis and use of clinical data according to the Declaration of Helsinki and institutional guidelines. Response and outcome data are reported for the entire cohort. The subgroup of patients with available molecular data (n = 174) constitute the molecular cohort for risk model construction. A cohort of 189 AML patients receiving HMA/VEN as first line treatment from the same registry served as an independent validation cohort. Details of the first line cohort will be reported separately. The registry was approved by the local Ethics Review Committee (ethical vote No.7972_BO_K_2018).
Treatment
All patients had received off-label VEN for relapsed or refractory disease in combination with either azacitidine 75 mg/m2 days 1–7 or 1–5 and 8 + 9 subcutaneously (n = 192) or decitabine 20 mg/m2 days 1–5 intravenously (n = 48). Patients had not received VEN in a prior line of therapy. Orally administered VEN doses ranged from 50 to 600 mg depending on concomitant CYP3A4 inhibitor use for antifungal prophylaxis. Additionally, patients received supportive care measures including transfusions, acid-reducing and antiemetic agents according to local practice. Timing of response evaluation was at the discretion of the treating physician, and bone marrow was obtained for response assessment after the completion of either one or two cycles in the majority of patients.
Details of cytogenetic, molecular and statistical analyses can be found in the Supplemental Materials.
Comprehensive risk model
Based on multivariate Cox regression a model was derived capable of predicting personalized outcomes. The OS prediction is performed by using N patient-dependent parameters \({{{\bf{X}}}}=({X}_{1},{X}_{2},\ldots ,\,{X}_{N})\) of the multivariate model in the Cox proportional hazards formula:
where \({h}_{0}\left(t\right)\) is a baseline hazard, a hazard for a patient with zero in every variable and βi are coefficients of the model for the parameter Xi, related to the respective hazard ratio as \({h}_{i}=\exp ({\beta }_{{{{\rm{i}}}}})\). The same formula was used for EFS with its own coefficients. The value of the sum \(S={{\sum }_{{{{\rm{i}}}}}\beta }_{{{{\rm{i}}}}}\cdot {X}_{{i}}\) is defined as venetoclax-prognostic risk score (VEN-PRS) for each patient. For OS/EFS the score value SOS/EFS < 0.25 corresponds to a favorable risk, 0.25 < SOS/EFS ≤ 0.75 to intermediate risk, and SOS/EFS > 0.75 to adverse risk. Further details are provided in the Supplemental Materials.
To evaluate calibration of the model, the patient population was divided into a training cohort comprising 100 patients and a validation cohort comprising 74 patients. Two hundred models were generated by randomly choosing 100 training patients and 74 test patients and the predicted and observed 10-month OS and EFS times were compared for three risk groups. The discrimination ability of the model was evaluated by area under the curve (AUC) values of receiver operating characteristic (ROC) curves for 10-month OS and EFS [24].
All statistical analyses were performed using the R computing language (version 4.2.2) and statistical software package SPSS 29.0.
Results
Patient characteristics
Two-hundred-and-forty R/R AML patients were treated with HMA and off-label VEN between January 2017 and April 2023 and were included in our analysis (entire cohort). Table 1 provides details on clinical characteristics at the time of treatment with HMA/VEN. The median age was 68.6 years (range, 20-88). A similar proportion of patients had relapsed (n = 110; 46%) or had refractory disease (n = 130; 54%). ELN 2022 risk was favorable, intermediate and adverse in 5%, 20%, and 57% of patients, respectively. Patients had a median of two prior treatment lines (range, 1–7), including 67% patients with intensive pretreatment and 36% with prior alloHCT. The majority of patients received azacitidine (80%) combined with VEN, while 20% received decitabine (Table 2). Median VEN dose after ramp-up was 100 mg (range, 50–600 mg) and 121 patients (50%) received VEN for 14 days.
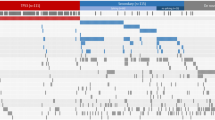
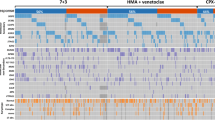
For 174 patients (73%) molecular data were available (molecular cohort, Supplementary Fig. S1).
Most commonly mutated genes included those associated with clonal hematopoiesis (TET2 20%, ASXL1 18%, DNMT3A 17%) besides RUNX1 (19%), and TP53 (18%), whereas 19 patients (11%) had no detectable mutation. Among those, three patients had a complex karyotype, three had KMT2A-rearranged AML and two had single cytogenetic aberrations, while the remaining 11 (6%) patients had no detectable cytogenetic aberration. Median variant allele frequencies (VAF) are depicted in Supplementary Fig. S2, indicating lower VAFs in genes that are involved in signaling pathways such as FLT3-ITD, NRAS and PTPN11, whereas higher VAFs were observed in splicing genes (SRSF2, ZRSR2) and transcription factors (RUNX1).
Treatment response and outcome in the entire cohort
Patients received a median of 2 treatment cycles (range 1-34) of HMA/VEN. CR and CRi rates were 25% and 14%, respectively. The overall response rate (ORR) was 44%, including 39% of patients with CR/CRi and 5% of patients with MLFS (Table 3). Partial remission was achieved in one patient, while 45% of patients (n = 108) did not respond to HMA/VEN. Twenty-five patients (10%) died before response assessment was performed (Table 3). CR/CRi rates were higher in patients with white blood cell (WBC) count ≤5 × 109/L (46% vs 25%; p = 0.002) and platelet count >30 × 109/L (46% vs 30%; p = 0.01), while all other characteristics did not associate with response (Supplementary Table S1).
After a median follow-up of 31.5 months, median OS was 7.9 months (95% CI, 6.4–10.2 months) and median EFS was 5.1 months (95% CI, 4.4–6.3 months) in the entire cohort. In CR/CRi patients median RFS was 12.9 months (95% CI, 10.2 months to not reached) (Fig. 1A–C).

A Kaplan–Meier estimates for overall survival. B Kaplan–Meier estimates for event-free survival. C Kaplan–Meier estimates for relapse-free survival in CR/CRi patients.
Clinical and molecular signatures of response
One-hundred-seventy-four patients with molecular data were evaluated for clinical and molecular predictors of response. In univariate analysis, CR/CRi was more likely to occur in patients with WBC count ≤5 × 109/L (46% vs 20%; p = 0.02) and platelet count >30 × 109/L (41% vs 29%; p = 0.05) (Supplementary Table S2).
Molecular predictors of inferior response included mutated PTPN11 (mutated vs wildtype (wt) CR/CRi 0% vs 38%; p = 0.06). Mutated NF1 and TP53 were numerically associated with inferior response (NF1 mutated vs wt CR/CRi 14% vs 37%; p = 0.2; TP53 mutated vs wt CR/CRi 29% vs 38%; p = 0.36), whereas mutated IDH2 (mutated vs wt CR/CRi 46% vs 34%; p = 0.2) or STAG2 (mutated vs wt CR/CRi 53% vs 34%; p = 0.13) status were numerically associated with a higher rate of CR/CRi (Supplementary Table S3).
Predictors of overall and event-free survival
We next evaluated clinical and molecular markers for associations with OS and EFS. In univariate analysis of pretreatment variables, predictors of inferior OS included age >70 years (HR 1.38 95% CI 1.0-1.98; p = 0.064), the presence of extramedullary disease (HR 2.06, 95% CI 1.33–3.2; p = 0.001), HMA pretreatment (HR 1.63, 95% CI 1.15–2.3; p = 0.006), higher WBC count (HR 1.38 95% CI 0.92–1.94; p = 0.12) and complex karyotype (HR 1.33, 95% CI 0.91-1.94; p = 0.14) (Supplementary Fig. S3, Supplementary Table S4). Predictors for inferior EFS further included the type of combination partner (decitabine vs. azacitidine: HR 1.48, 95% CI 1.02–2.13; p = 0.038). Molecular predictors of inferior OS included mutations in NF1 (HR 2.53, 95% CI 1.2–5.4; p = 0.015), PTPN11 (HR 2.26, 95% CI 1.5–3.4; p < 0.001), TP53 (HR 1.5, 95% CI 0.96–2.3; p = 0.073), and FLT3 (any FLT3 mutation, HR 1.64, 95% CI 1.00–2.7; p = 0.05) (Supplementary Fig. S4, Supplementary Table S5). The number of prior treatment lines was not a significant parameter in univariate analysis for OS and EFS (Supplementary Table S5; Supplementary Fig. S5) and was not further considered. In multivariate analysis extramedullary disease (HR 2.46, 95% CI 1.5–4.0; p = <0.001), HMA pretreatment (HR 1.9, 95% CI 1.3-2.8; p < 0.001), presence of PTPN11 (HR 2.2, 95% CI 1.3–4.0; p = 0.006), and NF1 (HR 2.26, 95% CI 1.5–3.4; p < 0.001) mutations were identified as independent risk factors for inferior OS, whereas presence of SF3B1 mutations (HR 0.38, 95% CI 0.2–0.8; p = 0.01) remained as independent risk factor for superior OS (Table 4). Independent risk factors for inferior EFS were similar to those for OS and included extramedullary disease (HR 1.76, 95% CI 1.1–2.8; p = 0.02), HMA pretreatment (HR 1.57, 95% CI 1.1–2.2; p = 0.014), and presence of mutations in PTPN11 (HR 2.1, 95% CI 1.1–4.03; p = 0.03), and FLT3 (HR 1.82, 95% CI 1.1–3.04; p = 0.02). Presence of a SF3B1 mutation was associated with superior EFS (HR 0.42, 95% CI 0.2–0.8; p = 0.01) (Table 4).
Subsequently, a three-tiered risk stratification model was developed for OS and EFS based on HR-weighted scoring. For OS the following variables were included in the model: extramedullary AML, HMA pretreatment, mutated PTPN11, FLT3, TP53, NF1, and SF3B1. Each variable was weighted by calculating the hazard coefficient, which is the natural logarithm of the hazard ratio of the variable (Table 4). The individual score for each patient was calculated by adding up the coefficients of variables that apply for each individual patient. Based on the individual score, patients were stratified into three risk groups: patients with a VEN-PRS of <0.25 were assigned to the favorable risk group, patients with a VEN-PRS between 0.25 and 0.75 to the intermediate risk group, and patients with VEN-PRS > 0.75 to the adverse risk group (Supplementary Fig. S6A). When applying the newly developed VEN-PRS, it allocated 46 (26%), 75 (43%), and 53 patients (31%) into the favorable-, intermediate-, and adverse risk groups, respectively with significant differences in OS (median OS, 95% CI in favorable vs intermediate vs adverse risk groups: 14.2 months (10.2–31.1) vs 7.0 months (5.0–13.2) vs 3.1 months (1.5–6.7); p < 0.001) (Fig. 2).

Favorable risk: SOS < 0.25; intermediate risk: 0.25 ≤ SOS ≤ 0.75; adverse risk: SOS > 0.75.
For EFS the following variables were included to the model: extramedullary AML, HMA pretreatment, mutated PTPN11, FLT3, NF1, and SF3B1. Based on the individual scores patients were stratified into three risk groups for EFS analogous to OS (Supplementary Fig. S6B). The VEN-PRS model allowed to allocate patients into three risk groups with significantly different EFS (median EFS, 95% CI in favorable vs intermediate vs adverse risk group: 8.8 months (6.3–18.43) vs 4.1 months (3.33–6.2) vs 1.8 months (1.03–3.03); p < 0.001) (Fig. 3). One-, two-, and three-year OS and EFS are provided in Supplementary Table S6. Supplementary Table S7 provides the VEN-PRS calculator for estimating patient’s individual risk.

Favorable risk: SEFS < 0.25; intermediate risk: 0.25 ≤ SEFS ≤ 0.75; adverse risk: SEFS > 0.75.
The VEN-PRS was evaluated separately in the relapsed and refractory cohorts and was similarly prognostic in these subgroups (Supplementary Figs. S7 and S8). The VEN-PRS was also prognostic in patients treated with HMA/VEN after one prior line of treatment for OS, but not EFS (Supplementary Fig. S9), and it was prognostic in patients treated with HMA/VEN after more than one prior line of treatment for both OS and EFS (Supplementary Fig. S10).
Calibration analysis showed that the predicted 10-month survival correlated well with the observed survival for the three risk groups, where EFS in the adverse risk group is somewhat underestimated, confirming that the model is well calibrated (Supplementary Fig. S11). In discrimination analysis, the AUC was 0.67 for OS and 0.68 for EFS, corresponding to a moderate discrimination (Supplementary Fig. S12).
As we did not have access to a second R/R AML cohort treated with venetoclax for external validation, we evaluated our score in patients treated with HMA/VEN at first diagnosis (n = 189). There were less patients in the adverse risk group since a significantly lower number of patients in the first-line cohort had prior HMA treatment (first-line n = 22; R/R AML n = 99) and extramedullary manifestation (first-line n = 4; R/R AML n = 17) (Supplementary Table S8), but the model showed significantly different risks for the favorable, intermediate and adverse risk groups for OS and for the favorable and intermediate risk groups for EFS, thus independently validating the VEN-PRS (Supplementary Figs. S13A and S13B). AIC differences are negative with -6.14 for OS and -6.94 for EFS, showing that our variable selection is suitable for modeling an independent cohort.
Taken together, our analyses suggest HMA pretreatment, extramedullary disease and the mutation status of NF1, PTPN11, FLT3, TP53 and SF3B1 as clinically relevant predictors of survival in patients treated with HMA/VEN for R/R AML.
Comparison of VEN-PRS to other AML risk models
We first compared our prognostic score model with the prognostic index proposed by Breems and colleagues [12], which was developed to estimate the outcome of AML patients in first relapse. The prognostic index showed no significant fit to our data. The AIC difference between the prognostic index by Breems et al. and the null model was 3.72 and 3.97 for OS and EFS, respectively, whereas the AIC difference between our proposed model and the null model was −26.67 and −20.11 for OS and EFS, respectively. As a more negative AIC difference indicates less prognostic information loss, our model clearly outperforms the prognostic index by Breems (Supplementary Fig. S14).
We next evaluated the ELN2022 risk classification, which was developed for newly diagnosed AML patients undergoing intensive chemotherapy and thus is not expected to be prognostic in R/R patients [3]. CR/CRi rates were 42%, 44%, and 33% in favorable, intermediate, and adverse ELN2022 risk patients, respectively (p = 0.44). Overall survival in the context of ELN2022 in the favorable, intermediate, and adverse risk groups was 11.1 months, 8.4 months, and 9.3 months, respectively (p = 0.9). The AIC difference between the ELN2022 classification and the null model was 3.8 and 3.91 for OS and EFS, respectively.
We then evaluated the VIALE A prognostic score proposed by Döhner and colleagues [25], which stratified newly diagnosed HMA/VEN treated patients into three risk groups based on the mutational status of four genes (favorable: TP53 wt, no FLT3-ITD, K/NRAS wt; intermediate FLT3-ITD or K/NRAS mutated; adverse TP53 mutated) [24]. Median OS rates in favorable, intermediate, and adverse risk groups were 7.6 months, 12 months, and 8.2 months (p = 0.18), respectively, when applying the VIALE A prognostic score on our cohort of R/R AML patients (Supplementary Fig. S15). The AIC difference between the proposed VIALE A prognostic score and the null model was 0.90 and 0.32 for OS and EFS, respectively.
Lastly, we further compared our prognostic model with the recently published score by Gangat and colleagues, which stratified newly diagnosed patients undergoing HMA/VEN treatment into three risk groups based on HR-weighted scoring of the following parameters: failure to achieve CR/CRi, adverse karyotype, TP53 mutation, and absence of IDH2 mutation. Reported mOS were 28.9, 9.6, and 3.1 months for the low, intermediate and high-risk groups, respectively for AML patients treated with frontline HMA/VEN [26]. Applying the score on our R/R AML cohort, survival estimates in favorable, intermediate, and adverse risk groups were 24.1 months, 6.7 months, and 4.6 months (p < 0.001), respectively (Supplementary Fig. S16). While this model provided good separation in the R/R setting, the AIC difference between the proposed score by Gangat et al. classification and the null model was −16.03 for OS and thus performed less well compared to the proposed VEN-PRS model.
In summary, previously published risk scores and classifications showed significantly lower accuracy in predicting outcomes of R/R AML patients treated with HMA/VEN compared to our proposed risk model, suggesting that other risk factors than the previously established pre-treatment characteristics determine efficacy of HMA/VEN in R/R AML patients.
Discussion
With HMA/VEN being increasingly used in relapsed/refractory AML patients, the evaluation of genetic and clinical signatures of response and survival is essential to support treatment selection for R/R AML patients. In this study, we analyzed a large cohort of relapsed or refractory AML patients treated with HMA/VEN and propose a novel prognostic risk score (VEN-PRS) derived from clinical and molecular parameters. When applying the VEN-PRS to R/R AML patients treated with HMA/VEN, patients were stratified into favorable (26%), intermediate (43%), and adverse risk (31%) groups. Outcome analysis demonstrated that the proposed VEN-PRS performed well, stratifying three different cohorts of patients with significant differences in overall and event-free survival, both in relapsed and refractory patients and patients with one or more than one prior lines of treatment.
This risk score identified extramedullary AML and HMA pretreatment as significant clinical variables and mutations in NF1, PTPN11, FLT3, TP53, and SF3B1 as significant molecular markers for OS. Significant prognostic parameters for EFS included the aforementioned clinical and molecular variables except for TP53, which was not prognostic for EFS.
The approval of HMA/VEN marked a substantial improvement in the treatment landscape of elderly/unfit patients with newly diagnosed AML providing a new standard of care. However, long-term outcomes of this combination regimen remain to be determined, and with a third of patients being primary refractory and the majority of patients eventually relapsing, treatment is primarily of palliative intention [27, 28].
In our analysis a lower WBC count and a higher platelet count were associated with a higher CR/CRi rate, while mutations in PTPN11, NF1, and TP53 were associated with a lower rate and mutations in IDH2 and STAG2 with a higher rate of CR/CRi. Molecular predictors of response to frontline HMA/VEN therapy include NPM1, IDH1/2, and DNMT3A mutations, whereas mutations in signaling genes (i.e. FLT3-ITD, KRAS, NRAS, PTPN11, CBL, KIT) and TP53 were associated with secondary resistance and shorter survival [29]. Other molecular markers that are associated with response outcomes include mutations in CEBPA, SRSF2 and ASXL1 [19, 30]. Shimony et al. recently reported on the clinical impact of molecular ontogeny in a large cohort of newly diagnosed AML patients who were treated with either HMA and venetoclax or HMA monotherapy. In patients with TP53 mutated AML, mOS and response rates were similar in patients treated with HMA/VEN vs HMA monotherapy. Patients with secondary ontogeny, defined by the presence of mutations in ASXL1, BCOR, EZH2, SF3B1, SRSF2, STAG2, U2AF1, or ZRSR2, showed prolonged OS and better response to HMA/VEN as compared to HMA monotherapy. However, in our study, OS for patients with secondary ontogeny was similar to what was observed for patients with de novo disease [31]. In line with our results, another study demonstrated that the addition of VEN to low intensity chemotherapy abrogated the adverse risk of splicing mutations [32]. Stahl et al. reported higher response rates in NPM1 mutated R/R AML patients and adverse cytogenetics. Mutations in TP53, KRAS/NRAS, and SF3B1 were associated with worse OS [16]. However, in other reports by Morsia et al. and Piccini et al., abnormal cytogenetics did not predict response or survival in HMA/VEN treated R/R AML patients [17, 18]. In another retrospective analysis by Aldoss et al. mutations in TET2 and ASXL1 were associated with improved response while responses were similar in TP53 and FLT3 wt and mutated patients [19]. Real-world data from the French Auraml Group demonstrated response rates of up to 63% in IDH mutated R/R AML patients [20].
Two recently published communications from the Mayo Clinic and MD Anderson Cancer Center proposed genetic based risk scores to predict response and survival outcomes in newly-diagnosed patients treated with upfront HMA/VEN therapy [26, 33]. The 4-gene molecular prognostic risk signature from MD Anderson Cancer Center uses N/KRAS, FLT3-ITD and TP53 mutations to stratify patients into three risk groups [33], whereas the score proposed by Gangat et al. integrates ELN2022 adverse karyotype and failure to achieve CR/CRi in addition to molecular markers in their score [26]. Our findings of the differential benefit of HMA/VEN in R/R AML by molecular subgroups correspond with the aforementioned studies, which identified TP53, PTPN11 and FLT3 as adverse prognostic risk markers. Further, SF3B1 was identified as a favorable risk parameter, whereas other secondary ontogeny markers were not considered as adverse risk. While TP53 was found to be prognostically relevant for OS in our analysis, it was not prognostic for EFS. Our observation is supported by subgroup analyses from the VIALE A trial and other studies of upfront HMA/VEN treatment, which show that TP53 mutated patients respond quite well to HMA/VEN but do not derive long-term benefit from addition of VEN [27, 34, 35]. However, the TP53 mutation is found to be one of the main molecular denominators of secondary resistance and relapse resulting in a general dismal prognosis in TP53 mutated AML irrespective of treatment modality [36, 37]. Importantly, the VEN-PRS is applicable at the time of relapse and refractoriness and does not rely on response to salvage treatment.
Widely applied risk scores including the ELN2022 classification are effective in stratifying intensively treated patients according to molecular and cytogenetic risk at diagnosis. As the ELN2022 classification is derived from data of patients who were treated with intensive, mostly anthracycline based therapies, it is not expected to predict prognosis of patients treated with HMA/VEN and other lower-intensity regimens.
The VEN-PRS requires a medical history, physical examination and possibly imaging to detect extramedullary disease, and molecular profiling at time of relapse or refractoriness. We provide an easily applicable calculator for estimating patients’ individual risk based on globally accessible parameters that can support therapeutic decision-making regarding HMA/VEN versus alternative treatment options (VEN-PRS calculator). More and more frequently patients with R/R AML have several treatment options such as inhibitors of FLT3, IDH1/2, or menin, in addition to HMA/VEN, especially for relapse after alloHCT. Choosing among treatment options is difficult in this setting as no comparative studies are available. Prognostic risk scores like the one proposed here will therefore help to estimate prognosis under HMA/VEN treatment, and will facilitate the discussion with patients to meet an informed treatment decision.
Limitations of the current study include its design as a registry, which does not control for a selection bias, and a limited number of patients, which limit the evaluation of genetic markers to the more frequently mutated subgroups.
In conclusion, the current study identifies predictors of survival to HMA/VEN in R/R AML and proposes a clinical-molecular survival model, which is practically relevant and allows a clear stratification of patients into three risk groups with significantly different OS and EFS outcomes. Our proposed VEN-PRS is an efficiently designed prognostic tool to support informed therapeutic decision in this difficult-to-treat population.
Data availability
Individual patient data will not be made available in order to maintain health information privacy. De-identified mutation information will be shared upon reasonable request to the corresponding author.
References
Thol F, Döhner H, Ganser A. How I treat refractory and relapsed acute myeloid leukemia. Blood. 2024;143:11–20.
Thol F, Heuser M. Treatment for Relapsed/Refractory Acute Myeloid Leukemia. Hemasphere. 2021;5:e572.
Döhner H, Wei AH, Appelbaum FR, Craddock C, DiNardo CD, Dombret H, et al. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood. 2022;140:1345–77.
Ferguson P, Hills RK, Grech A, Betteridge S, Kjeldsen L, Dennis M, et al. An operational definition of primary refractory acute myeloid leukemia allowing early identification of patients who may benefit from allogeneic stem cell transplantation. Haematologica. 2016;101:1351–8.
Roloff GW, Odenike O, Bajel A, Wei AH, Foley N, Uy GL. Contemporary Approach to Acute Myeloid Leukemia Therapy in 2022. Am Soc Clin Oncol Educ Book. 2022;42:1–16.
Zeichner SB, Gleason S, Antun AG, Langston A, Heffner LT Jr., Kota VK, et al. Survival of Patients Diagnosed with Primary Refractory and Relapsed Acute Myeloid Leukemia from 2008-2012: A Single Institution Experience. Blood. 2015;126:4955.
Walter RB, Othus M, Burnett AK, Löwenberg B, Kantarjian HM, Ossenkoppele GJ, et al. Resistance prediction in AML: analysis of 4601 patients from MRC/NCRI, HOVON/SAKK, SWOG and MD Anderson Cancer Center. Leukemia. 2015;29:312–20.
Breems DA, Van Putten WL, De Greef GE, Van Zelderen-Bhola SL, Gerssen-Schoorl KB, Mellink CH, et al. Monosomal karyotype in acute myeloid leukemia: a better indicator of poor prognosis than a complex karyotype. J Clin Oncol. 2008;26:4791–7.
Byrd JC, Mrózek K, Dodge RK, Carroll AJ, Edwards CG, Arthur DC, et al. Pretreatment cytogenetic abnormalities are predictive of induction success, cumulative incidence of relapse, and overall survival in adult patients with de novo acute myeloid leukemia: results from Cancer and Leukemia Group B (CALGB 8461). Blood. 2002;100:4325–36.
Heuser M, Ofran Y, Boissel N, Brunet Mauri S, Craddock C, Janssen J, et al. Acute myeloid leukaemia in adult patients: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2020;31:697–712.
Ganzel C, Sun Z, Cripe LD, Fernandez HF, Douer D, Rowe JM, et al. Very poor long-term survival in past and more recent studies for relapsed AML patients: The ECOG-ACRIN experience. Am J Hematol. 2018;93:1074–81.
Breems DA, Van Putten WL, Huijgens PC, Ossenkoppele GJ, Verhoef GE, Verdonck LF, et al. Prognostic index for adult patients with acute myeloid leukemia in first relapse. J Clin Oncol. 2005;23:1969–78.
Perl AE, Martinelli G, Cortes JE, Neubauer A, Berman E, Paolini S, et al. Gilteritinib or Chemotherapy for Relapsed or Refractory FLT3-Mutated AML. N. Engl J Med. 2019;381:1728–40.
Shahswar R, Beutel G, Gabdoulline R, Schwarzer A, Kloos A, Koenecke C, et al. Fludarabine, cytarabine, and idarubicin with or without venetoclax in patients with relapsed/refractory acute myeloid leukemia. Haematologica. 2024;109:72–83.
Thol F, Schlenk RF, Heuser M, Ganser A. How I treat refractory and early relapsed acute myeloid leukemia. Blood. 2015;126:319–27.
Stahl M, Menghrajani K, Derkach A, Chan A, Xiao W, Glass J, et al. Clinical and molecular predictors of response and survival following venetoclax therapy in relapsed/refractory AML. Blood Adv. 2021;5:1552–64.
Morsia E, McCullough K, Joshi M, Cook J, Alkhateeb HB, Al-Kali A, et al. Venetoclax and hypomethylating agents in acute myeloid leukemia: Mayo Clinic series on 86 patients. Am J Hematol. 2020;95:1511–21.
Piccini M, Pilerci S, Merlini M, Grieco P, Scappini B, Bencini S, et al. Venetoclax-Based Regimens for Relapsed/Refractory Acute Myeloid Leukemia in a Real-Life Setting: A Retrospective Single-Center Experience. J Clin Med. 2021;10:1684.
Aldoss I, Yang D, Pillai R, Sanchez JF, Mei M, Aribi A, et al. Association of leukemia genetics with response to venetoclax and hypomethylating agents in relapsed/refractory acute myeloid leukemia. Am J Hematol. 2019;94:E253–e5.
Gross Z, Tauveron-Jalenques U, Aspas Requena G, Carre M, Meunier M, Tavernier E, et al. Real World Use of Azacitidine and Venetoclax in Acute Myeloid Leukemia in Frontline and Relapse/Refractory Settings: A Multicentric Study from French Auraml Group. Blood. 2023;142:590.
Braitsch K, Schmalbrock LK, Jung P, Bumeder I, Kiewe P, Hecker JS, et al. Genotype and Intensive Pretreatment Influence Outcome of Acute Myeloid Leukemia Patients Treated With Venetoclax in Combination With Hypomethylating Agents or Low-dose Cytarabine: “Real World” Data From Germany. Hemasphere. 2022;6:e759.
Arber DA, Hasserjian RP, Orazi A, Mathews V, Roberts AW, Schiffer CA, et al. Classification of myeloid neoplasms/acute leukemia: Global perspectives and the international consensus classification approach. Am J Hematol. 2022;97:514–8.
Shahswar R, Beutel G, Klement P, Rehberg A, Gabdoulline R, Koenecke C, et al. FLA-IDA salvage chemotherapy combined with a seven-day course of venetoclax (FLAVIDA) in patients with relapsed/refractory acute leukaemia. Br J Haematol. 2020;188:e11–e5.
Heagerty PJ, Lumley T, Pepe MS. Time-dependent ROC curves for censored survival data and a diagnostic marker. Biometrics. 2000;56:337–44.
Döhner H, Pratz KW, DiNardo CD, Jonas BA, Pullarkat VA, Thirman MJ, et al. ELN Risk Stratification Is Not Predictive of Outcomes for Treatment-Naïve Patients with Acute Myeloid Leukemia Treated with Venetoclax and Azacitidine. Blood. 2022;140:1441–4.
Gangat N, Karrar O, Iftikhar M, McCullough K, Johnson IM, Abdelmagid M, et al. Venetoclax and hypomethylating agent combination therapy in newly diagnosed acute myeloid leukemia: Genotype signatures for response and survival among 301 consecutive patients. Am J Hematol. 2024;99:193–202.
DiNardo CD, Jonas BA, Pullarkat V, Thirman MJ, Garcia JS, Wei AH, et al. Azacitidine and Venetoclax in Previously Untreated Acute Myeloid Leukemia. N. Engl J Med. 2020;383:617–29.
Pratz KW, Jonas BA, Pullarkat V, Thirman MJ, Garcia JS, Döhner H, et al. Long-term follow-up of VIALE-A: Venetoclax and azacitidine in chemotherapy-ineligible untreated acute myeloid leukemia. Am J Hematol. 2024;99:615–24.
Chyla B, Daver N, Doyle K, McKeegan E, Huang X, Ruvolo V, et al. Genetic Biomarkers Of Sensitivity and Resistance to Venetoclax Monotherapy in Patients With Relapsed Acute Myeloid Leukemia. Am J Hematol. 2018;93:E202–5.
Gangat N, Ilyas R, McCullough K, Begna KH, Al-Kali A, Patnaik MM, et al. Predictors of response to venetoclax plus hypomethylating agent therapy and survival in blastphase myeloproliferative neoplasm. Haematologica. 2023;108:1423–8.
Shimony S, Garcia JS, Keating J, Chen EC, Luskin MR, Stahl M, et al. Molecular ontogeny underlies the benefit of adding venetoclax to hypomethylating agents in newly diagnosed AML patients. Leukemia. 2024;38:1494–500.
Senapati J, Urrutia S, Loghavi S, Short NJ, Issa GC, Maiti A, et al. Venetoclax abrogates the prognostic impact of splicing factor gene mutations in newly diagnosed acute myeloid leukemia. Blood. 2023;142:1647–57.
Bataller A, Bazinet A, DiNardo CD, Maiti A, Borthakur G, Daver NG, et al. Prognostic risk signature in patients with acute myeloid leukemia treated with hypomethylating agents and venetoclax. Blood Adv. 2024;8:927–35.
DiNardo CD, Tiong IS, Quaglieri A, MacRaild S, Loghavi S, Brown FC, et al. Molecular patterns of response and treatment failure after frontline venetoclax combinations in older patients with AML. Blood. 2020;135:791–803.
Kim K, Maiti A, Loghavi S, Pourebrahim R, Kadia TM, Rausch CR, et al. Outcomes of TP53-mutant acute myeloid leukemia with decitabine and venetoclax. Cancer. 2021;127:3772–81.
Zhang Q, Riley-Gillis B, Han L, Jia Y, Lodi A, Zhang H, et al. Activation of RAS/MAPK pathway confers MCL-1 mediated acquired resistance to BCL-2 inhibitor venetoclax in acute myeloid leukemia. Signal Transduct Target Ther. 2022;7:51.
Nechiporuk T, Kurtz SE, Nikolova O, Liu T, Jones CL, D’Alessandro A, et al. The TP53 Apoptotic Network Is a Primary Mediator of Resistance to BCL2 Inhibition in AML Cells. Cancer Discov. 2019;9:910–25.
Acknowledgements
The authors thank all patients, centers and participating physicians of the venetoclax registry (venreg), who entered their patients into the registry and shared clinical and molecular data.
Funding
This study was supported by grants HE 5240/6-1, HE 5240/6-2 to MH from the German Research Foundation (DFG), grant 16 R/2021 to MH from DJCLS, and grants 70114189, 70114478 and 70115044 to MH from Deutsche Krebshilfe. AbbVie supported the data analysis. The registry design; data collection and interpretation of data were independent of AbbVie. AbbVie did not participate in writing, reviewing, and approval of the manuscript. RS received a grant from PRACTIS (DFG funded, grant No. 3696/3). AKB received funding from the DFG with grant No. BE6555/1-1 and BE6555/2-1. Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
RS and MH designed the study; RS, MH, and GB controlled the database. KK, MW, KB, LS, FM, SR, contributed to the collection of clinical and biological data. RG, KK, MW, KSG, KB, MM, LS, LB, FM, WF, JK, SK, SR, AV, YB, AKB, EK, GB, FT and FH contributed to the analysis of clinical and biological data. RS, RG, and MH performed the statistical analysis. RS and MH interpreted the data and wrote the manuscript. All authors read and agreed to the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
MH declares honoraria from Abbvie, Eurocept, Jazz Pharmaceuticals, Janssen, Novartis, Takeda, paid consultancy for Abbvie, Agios, BMS, Daiichi Sankyo, Glycostem, Jazz Pharmaceuticals, Kura Oncology, Novartis, Pfizer, PinotBio, Roche, Tolremo, and research funding to his institution from Abbvie, Agios, Astellas, Bayer Pharma AG, BergenBio, Daiichi Sankyo, Glycostem, Jazz Pharmaceuticals, Loxo Oncology, Novartis, Pfizer, PinotBio, Roche. RS declares support for meeting attendance from AbbVie. EK declares honoraria and/or travel support from Abbvie, JAZZ, BMS, Otsuka, Servier. WF declares honoraria from Jazz Pharmaceuticals, Pfizer, Amgen, Abbvie, Celgene, MorphoSys, Ariad/Incyte, Stemline Therapeutics, Clinigen, Daiichi Sankyo, Otsuka and Servier outside the submitted work; in addition, research support from Apis; patent issued with Amgen; support for medical writing for Amgen, Pfizer, and AbbVie. KSG declares honoraria from BMS and Abbvie. FM declares support for meeting attendance from Servier, AbbVie, Incyte, Gilead, Jazz Pharmaceuticals, Novartis, Teva, Pfizer, and Amgen, support for medical writing from Servier, and Springer Verlag, research support from Apis Technologies, and Daiichi Sankyo, honoraria from Servier, Jazz Pharmaceuticals, and AbbVie. The other authors declare no conflict of interest.
Ethics approval
The registry was approved by the local Ethics Review Committee (ethical vote No.7972_BO_K_2018).
Informed consent
All patients had given written informed consent to the off-label use of venetoclax, genetic analysis and use of clinical data according to the Declaration of Helsinki and institutional guidelines.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shahswar, R., Gabdoulline, R., Krueger, K. et al. A novel prognostic risk model for patients with refractory/relapsed acute myeloid leukemia receiving venetoclax plus hypomethylating agents. Leukemia 39, 614–622 (2025). https://doi.org/10.1038/s41375-024-02501-6
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41375-024-02501-6
