
Abstract
Myeloproliferative neoplasms (MPN) are associated with a variety of symptoms that severely impact patients’ quality of life and ability to perform daily activities. Recent studies showed differences in the perception of physician- versus patient-reported symptom burden. However, studies directly comparing patient- and physician-reported ratings are lacking. Here, a retrospective analysis on symptom burden of 3979 MPN patients of the Bioregistry of the German Study Group for MPN was conducted to intra-individually compare physician and patient reports collected at the same time. Cohen’s kappa was calculated to assess the degree of agreement between patient and physician reports. Factors influencing baseline symptom severity were identified using linear regression and adjusted Cox models were calculated to investigate the effect of symptom burden on survival. MPN patients had a high symptom burden, which neither decreased over time nor upon cytoreductive therapy. All symptoms were more frequently reported by patients compared to physicians. Agreement remained low and only slightly improved when considering a higher threshold for patient symptom severity. Patients with severe symptom burden had inferior survival compared to patients with less severe symptoms. Assessment of symptom burden in MPN is therefore insufficient and patient-reported outcome tools need to be implemented into clinical routine.
Similar content being viewed by others

Introduction
Myeloproliferative neoplasms (MPN) are clonal, phenotypically inflammatory diseases [1] associated with a plethora of symptoms that severely impact patients’ quality of life and ability to perform daily activities. MPNs are characterized by high symptom prevalence and burden [2,3,4,5,6,7,8,9,10,11,12]. The most common symptoms reported in real life settings include fatigue, pruritus (itching), night sweats, (bone) pain, weight loss, and fever [13,14,15,16].
Symptom control is one of the main treatment goals in MPN serving as primary endpoint in most of the trials leading to approval of new compounds in MPN in the last decades [17, 18]. However, the true impact of symptoms on prognosis remains unclear. Nevertheless, impact of symptom burden on patients´ ability to work and follow their social life has been studied before. In a large cohort of MPN patients, up to 60% of patients with myelofibrosis (MF) had to reduce working hours [2]. Previous studies have shown that the perception of symptom burden and its impact differs between physician- and patient-reported documentation [3, 4, 15]. However, these analyses were conducted without matching patient and physician reports intra-individually. The MPN Landmark survey, which included 813 patients and 457 physicians treating MPN patients, found that physicians significantly underestimated the proportion of patients with symptomatic polycythemia vera (PV) or essential thrombocythemia (ET) at the time of diagnosis compared to patient reporting [4]. Similar findings have been reported for MPN patients in Asia [9]. It is unavoidable that there will be discrepancies in the recognition of symptoms, as the symptom is subjective in nature and experienced exclusively by the patient. It is possible to assess the physician’s ability to correctly report the patient’s perception of symptoms.
To date, little is known about the impact of symptom burden on overall survival in patients with MPN [11, 19]. Two studies that examined symptom burden found contrasting results on the association between symptom burden and patients´ survival [11, 19].
Data from a population-based registry that directly includes patient and physician reports of symptoms at the same point in time are suitable for investigating the intra-individual agreement between these. The aim of this analysis was to assess MPN symptoms in patients enrolled in the German Study Group for MPN (GSG-MPN) Bioregistry and to compare physicians’ and patients’ perceptions of symptom burden on an intra-individual basis. A particular focus of the study was the impact of symptom burden on overall survival of the patients.
Materials and methods
The German Study Group MPN Bioregistry (GSG-MPN Bioregistry) is an observational study of BCR::ABL1-negative MPN patients with over 70 participating centers, including university hospitals, community hospitals, and office-based hematologists/oncologists. Patients with a confirmed BCR::ABL1-negative MPN diagnosis according to the WHO classification of 2008 [20] or 2016 [21] or IWG-MRT criteria [22], who were 18 years of age or older were included in the bioregistry. Patients are being prospectively followed after enrollment into the registry, with annual recording of clinical data, patient-reported outcomes, and collection of biomaterial. Recruitment started in August 2012, and the present analysis is based on the data of 5198 patients from the first registration and annual follow-up up to 8 years, with a data cut-off date of September 5th, 2023.
Ethics approval and consent to participate
The study was performed in accordance with the Declaration of Helsinki. The bioregistry was approved by the Ethics Committees of the Medical Faculty of RWTH Aachen University (EK 127/12), University Hospital Ulm (100/13), as well as by each local ethics committee of the participating medical centers. All patients included in the bioregistry provided written informed consent prior to inclusion in the registry. Patients deemed unable to provide written informed consent due to neurological or psychological impairment and patients who did not agree to registration were not included in the bioregistry.
Symptom assessment
Patients’ symptom ratings were assessed using a modified version of the MPN-SAF-TSS form [6] on a scale from 0 (absent/as good as it can be) to 10 (worst-imaginable/as bad as it can be) for each symptom. A severity score of 7 or higher was considered severe, as seen in the literature [2]. Persistent severe symptoms were defined in this study as symptoms reported as severe at baseline and at the first follow-up visit. The physician’s statement of whether a symptom was present was assessed via a dichotomous question (yes or no, with a category for unknown) and obtained from the electronic case report form (eCRF) of the GSG-MPN registry. Six symptoms were reported by both physician and patient at different times during the course of the disease and included in the analysis: fatigue, pruritus (itching), fever, night sweats, weight loss and pain. The physician’s assessment of “pain” was approximated by “bone pain” as reported by the patients.
Physician assessments were available when patients entered the MPN Registry (baseline/registry inclusion) and at up to 8 annual follow-up visits. The following procedure was used to match patient-reported symptoms with physician-reported symptoms: For each physician assessment date, the date of the patient assessment was taken if the patient assessment was within a 3-month interval around the physician assessment date (physician date ±92 days). If there were multiple patient assessments, the one with the smallest time difference from the physician assessment was selected. Using this approach, the maximum time difference between patient and physician assessments was three months.
The prevalence of patient-reported symptoms was calculated using two different thresholds: Prevalence was defined as a symptom score >0 or ≥4.
Data
The following data were available for analysis: Demographic data such as year of birth, sex, date and type of diagnosis (coded as essential thrombocythemia (ET), polycythemia vera (PV), primary myelofibrosis (PMF), and other/unclassified MPN), history of thrombosis (yes/no), antithrombotic therapy (yes/no), cytoreductive therapy (with hydroxyurea, interferon alpha, JAK2 inhibitor and/or anagrelide, yes/no with start date), phlebotomy dependency (yes/no), concurrent medical conditions (with diagnosis, yes/no), mutation status (JAK2, CALR, MPL, yes/no). For dichotomous questions (yes or no), the eCRF also included a category for unknown. Age at enrollment and age at first MPN diagnosis were estimated by subtracting the year of birth from the year of enrollment and the year of first MPN diagnosis. As the exact date of birth was not available, both age variables could only be estimated as whole years. For age-specific analysis, age was categorized as follows: 18–35 as “30”, 36–45 as “40”, 46–55 as “50”, 56–65 as “60”, 66–75 as “70”, 76 and older as “80”. Disease duration was calculated as the time from diagnosis to the baseline visit. Physician demographics were not available.
Statistical analysis
Continuous demographic variables were summarized as mean and standard deviation (SD) or median and interquartile range (IQR), as appropriate. Fisher’s exact test was used to test for association between two or more categorical variables. The non-parametric Mann–Whitney U test was used to test for differences between two continuous variables (e.g., patient-reported symptom scores), because the normality assumption was not met. McNemar’s test was used to compare the prevalence of physician-reported symptoms and patient-reported symptoms. Cohen’s kappa (κ) [23] was calculated to assess the degree of agreement between patient-reported and physician-reported symptom prevalence and was interpreted as follows [24]: κ between 0 and 0.20 was interpreted as no agreement, κ between 0.21 and 0.39 as minimal agreement, κ between 0.40 and 0.59 as weak agreement, κ between 0.60 and 0.79 as moderate agreement, κ between 0.80 and 0.90 as strong agreement, and κ above 0.9 as almost perfect agreement.
Multiple linear regression analysis was performed to determine associations between baseline symptom severity (dependent variable) and the demographic factors of age, sex, history of thrombosis, anticoagulation therapy, cytoreductive therapy, phlebotomies, and diagnosis (independent variables). Models were adjusted for age and sex. An interaction term between age and sex was allowed. However, if the interaction term was not statistically significant, the models were run without it. Cox models for overall survival were estimated with adjustment for age, sex, and disease duration, and hazard ratios (HRs) were reported with their 95% confidence intervals (CIs). All tests were two-tailed without adjustment for multiple comparisons. P values < 0.05 were considered statistically significant. All statistical analyses and data visualization were performed with R software, version 4.3.2. [25]. The R codes are potentially available from the corresponding author upon reasonable request.
Results
Baseline characteristics
A total of 3979 patients (76.5% of all GSG-MPN registry patients at the time of data extraction) had at least one common patient-physician symptom assessment at baseline or any follow-up visit and were included in the analysis (see Fig. 1). The sample sizes for the calculations of the symptom prevalence and agreement (baseline) and the symptom prevalence (baseline to follow-up 8) are also shown.
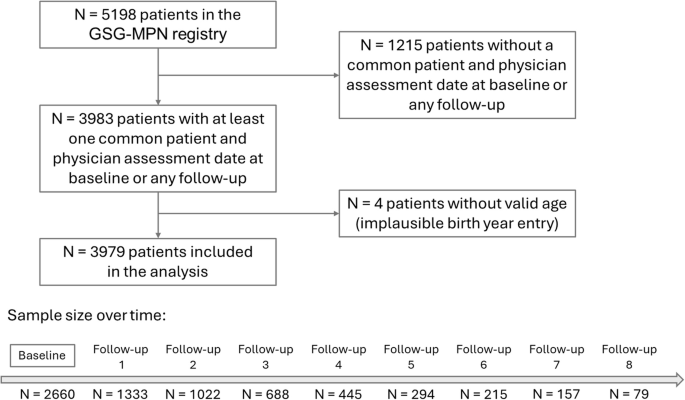
Of all 5198 patients in the registry, a total of 3979 had at least one common assessment date for both patient and physician and were included in the study. Sample size over time refers to the mean number of patients with available patient and physician symptom assessment reports. The exact sample size varies slightly between the six symptoms that were examined.
The median age of this cohort was 64 years (range: 18–96), identical to the total of 5198 patients included in the registry. The sample had a similar female-to-male ratio as the overall registry (both 53% female). The diagnosis spectrum was with 38% ET, 33% PV, 21% PMF, and 8% another/unclassified MPN also similar to the overall registry population (38% ET, 32% PV, 21% PMF, and 9% another/unclassified MPN). The characteristics of the included patients are shown in Table 1.
Patient and physician perspectives on baseline symptom prevalence
Overall, 93% of patients of this cohort reported the presence of at least one symptom at baseline (ET: 93%, PV: 95%, PMF: 92%, other/unclassified MPN: 94%). Severe disease burden (i.e. any symptom score ≥7) was present in 38% of the patients (ET: 34%, PV: 42%, PMF: 37%, other/unclassified MPN: 44%). Baseline patient and physician symptom prevalence and mean symptom severity scores are shown in Fig. 2.

Patient-reported prevalence (A), physician-assessed prevalence (B), and mean patient-reported symptom severity (C) at baseline are shown. Prevalence was defined as a symptom score greater than or equal to 1 (patient) or “yes” (physician). ET essential thrombocythemia, PV polycythaemia vera, PMF primary myelofibrosis, other other/unclassified MPN.
Fatigue was the most common symptom reported by both patients and physicians. It was reported by 85%, 82%, 84%, and 82% of patients with ET, PV, PMF, and other/unclassified MPN, respectively. These differences between diagnostic groups were not statistically significant. Physician assessment of the same patients showed statistically significantly different prevalences ranging from 26% (ET and other/unclassified MPN) to 36% (PMF; p < 0.001). Night sweats, pain, and pruritus were the second most common symptoms, followed by weight loss and fever. Pruritus was reported by both patients and physicians as having the highest prevalence in patients with PV (60% and 27%, respectively). This difference between MPN entities was statistically significant for both patient and physician reporting (p < 0.001). Another statistically significant difference was seen for weight loss, the prevalence of which was the lowest in patients with ET and the highest in patients with unclassified/other MPN.
Physician and patient agreement on baseline symptom prevalence
Agreement on baseline symptom prevalence between physician and patients´ assessment was quite low. Even for symptoms which are objectively measurable, such as weight loss, reports on symptom frequency were discrepant (any (unintentional) weight loss in the past 6 months reported by 26% (706/2687) of patients, whereas physicians reported weight loss in only 6% (169/2687) of patients). Table 2 shows physician and patient ratings of weight loss at baseline for the 2687 patients for whom both physician and patient ratings were available.
In 44 cases the physician reported weight loss while the patient did not indicate burden from this symptom.
Similar cross-tabulations were used to calculate the prevalence of symptoms in patients with and without cytoreductive therapy, as well as the agreement κ between physician and patient assessment (see Table 3). In all but two cases, there was a statistically significant difference in agreement between physician and patient with p < 0.05, except for fever with a prevalence assumption of 4 or more points for both patients with and without cytoreductive therapy, where there was no statistically significant difference in agreement. For all symptoms, patients reported a higher prevalence of symptoms than physicians. Agreement was low and improved only slightly for symptoms with a severity score of ≥4. In addition, agreement was similar for patients with and without cytoreductive therapy.
Age and sex dependency of patient-physician agreement is shown in Fig. 3. No clear difference in agreement could be detected for fatigue, fever, and weight loss for age or between male and female patients. Regarding pruritus, night sweats, and pain, agreement decreased slightly with increasing age, similarly for both male and female patients. Overall, there is no clear difference between male and female MPN patients in agreement about the presence of symptoms as rated by both patients and physicians. Focusing on agreement analysis when patients reported symptom severity of 4 or more points did not provide any additional insight.

Agreement regarding symptom presence of fatigue (A), pruritus (B), fever (C), night sweats (D), weight loss (E) and pain (F). Kappa Cohen’s kappa, CI confidence interval. Agreement is shown for female and male MPN patients across age groups.
Factors influencing baseline symptom severity
Linear regression analyses for symptom severity (see Supplementary Table 1) showed some statistically significant associations with demographic variables, but most associations appeared rather subtle. Considering changes of approximately one score point as relevant associations, the following associations with pruritus remained: Pruritus was 0.92 (CI: 0.75, 1.22) points higher in PV patients than in ET patients, and 0.85 (CI: 0.63, 1.08) points higher in phlebotomy-dependent patients. In addition, with a decrease in fatigue of 0.23 points per 10 years of age, patients in their twenties had approximately 1.2 points higher fatigue scores than patients in their seventies. When combined with sex (women had a 0.51-point higher fatigue score than men), fatigue scores were the highest in young female patients.
Symptom prevalence over time
Symptom prevalence over time calculated from patients and physicians ratings is shown in Fig. 4. Patient-reported symptom prevalence was remarkably higher than the prevalence perceived by the physician. This was consistent for all symptoms. Symptom prevalence was not lower in patients who received cytoreductive therapy. There was no trend towards better physician symptom recognition over time. Of note, sample size for the later follow-up visits significantly decreased compared to baseline (see Fig. 1 for numbers).

Prevalence is shown for baseline (BL) and annual follow-up (FU) visits for fatigue (A), pruritus (B), fever (C), night sweats (D), weight loss (E) and pain (F). Black lines show prevalence calculated from patient-reported symptom severity, where prevalence was defined as a symptom score greater than or equal to 1. Brown lines show prevalence calculated from patient-reported symptom severity, where prevalence was defined as a symptom score greater than or equal to 4. Blue lines show physician-reported prevalence. Solid lines represent patients with cytoreductive therapy and dotted lines represent patients without cytoreductive therapy. For brevity, the legend uses the word “therapy” instead of cytoreductive therapy.
Patient-reported severe symptom burden and overall survival
No statistically significant difference in the presence of severe symptom burden at baseline between patients receiving cytoreductive therapy and those without could be detected (Supplementary Table 2). Likewise, the persistence of severe symptoms did not differ between patients with and without cytoreductive therapy. The presence of any severe symptom at baseline (Fig. 5A) was associated with a higher hazard of death in a multivariable model adjusted for age, sex, and disease duration (adjusted HR = 1.5 (CI: 1.2, 1.9), p < 0.001). Among the six symptoms, severe fatigue at baseline (Fig. 5C) and severe weight loss at baseline (Fig. 5E) were both associated with increased hazard of dying, with adjusted HR = 1.8 (CI: 1.4, 2.3), p < 0.001 and adjusted HR = 3.5 (CI: 2.4, 5.0), p < 0.001, respectively. Considering symptom persistence resulted in a non-significant hazard of death (Fig. 5B). Persistent fatigue (Fig. 5E) did not result in a significantly higher hazard ratio. Despite low numbers of patients with persistent weight loss, a higher risk could be confirmed (Fig. 5F, adjusted HR = 6.3 (CI: 2.3, 17.0), p < 0.001).
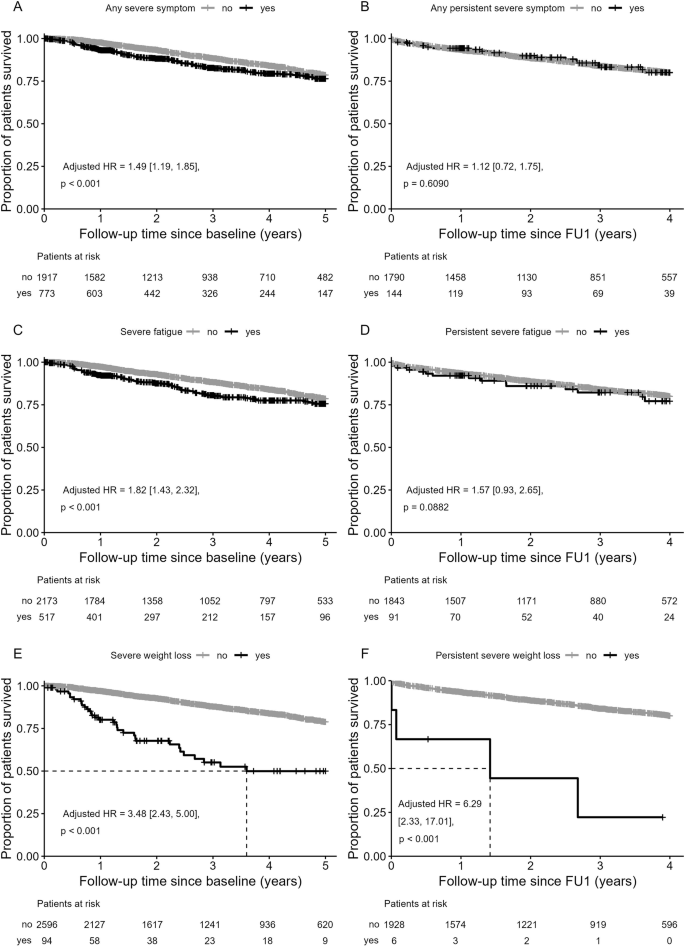
Overall survival by the presence of at least one severe symptom at baseline (A), at least one persistent severe symptom (B), severe fatigue at baseline (C), persistent severe fatigue (D), severe weight loss at baseline (E), and persistent severe weight loss (F). Persistent severe symptoms were symptoms reported as severe at baseline and at the first follow-up visit (FU1). Graphs on the right exclude patients who died or were censored between the baseline and FU1 visit.
In order to exclude the possibility that the cause of death may influence the correlation, a subgroup of 195 patients was analyzed in which the cause of death was reported. Notably, symptom presence and burden did not differ between patients who died due to MPN and those who died due to unrelated causes (Supplementary Table 3).
Discussion
The present study retrospectively analyzed the symptom burden of patients with Myeloproliferative Neoplasms (MPN), specifically Essential Thrombocythemia (ET), Polycythemia vera (PV), Primary Myelofibrosis (PMF), and other/unclassified MPNs, focusing on six key symptoms. At baseline, 93% of the patients were symptomatic, consistent with other studies reporting similarly high symptom prevalence [2,3,4,5,6,7,8,9,10,11,12]. Severe symptom burden, defined as a score of 7–10 in at least one symptom, was present in 38% of patients. The median disease duration at baseline was 3.3 years. Fatigue was the most frequently reported symptom by both patients and physicians, followed by night sweats, pain, pruritus, weight loss, and fever, mirroring patterns seen in other studies [2, 5, 6, 8,9,10,11]. Pruritus was particularly prevalent in PV patients, reported by both patients (60%) and physicians (27%).
In terms of symptom burden, PMF patients did not exhibit an increased burden compared to those with ET, PV, and other/unclassified MPNs, which aligns with previous studies [10, 12, 26]. The only exception was pain showing a slightly higher prevalence in PMF patients (53%), compared to the other entities (ET: 50%, PV: 52%, other/unclassified MPN: 49%). Overall, the disease burden in PMF patients in our cohort appeared lower compared to other published cohorts.
Symptom burden, as reported by both patients and physicians, did not decrease over time, consistent with findings from other studies [9, 19, 27]. Patients receiving cytoreductive therapy reported similar symptom burdens to those not receiving such therapy. Cytoreductive treatments included commonly used drugs such as hydroxycarbamide, anagrelide, interferon and JAK inhibitors, as well as less frequently used drugs like busulfan or experimental treatments. Unfortunately, the registry did not provide detailed treatment information to perform subgroup analysis. Unexpectedly, symptom burden, with or without treatment, remained unchanged over time. Physicians also reported no difference in symptom burden between patients with and without cytoreductive treatment. Similar findings, or even deterioration of symptoms following cytoreductive treatment, have been reported in other studies [9, 12, 19]. In recent reports on ET and PV patients, improvement in symptom burden was mainly observed in those with high symptom burden at initial diagnosis, while worsening was noted in patients with low baseline symptom burden following cytoreductive treatment [28]. Due to the lack of detailed treatment information, we can only hypothesize that the beneficial effects of symptom-oriented treatment, especially JAK inhibitors, might have been obscured due to the small sample size in our cohort.
Patient-physician consensus on the presence of symptoms was low, improving only slightly for symptoms with a severity score of ≥4. Fever in patients not receiving cytoreductive therapy exhibited the highest patient-physician consensus, although this agreement was still weak. We found only one study with data on simultaneous patient-physician symptom assessment in MPN patients, which similarly showed that patients reported higher symptom presence than physicians [9]. The MPN Landmark survey indicated that physicians underestimated the proportion of patients with symptomatic PV or ET at diagnosis compared to patient reports [4]. However, physician and patient responses were not matched in that survey. Comparable findings have been observed in metastatic breast cancer patients, where physicians significantly underreported symptoms compared to patients [29], and in multiple myeloma patients, where there was poor to fair agreement between patients and physicians in reporting treatment side effects [30]. Furthermore, the discrepancies in symptom perception between patients and physicians did not diminish over time, which is consistent with the literature [31].
Our results confirm that physicians tend to underestimate the presence of symptoms in their patients compared to patient reports. Several factors could contribute to this discrepancy: Patients might prefer to report symptoms via questionnaires rather than during visits, possibly omitting symptoms they consider less relevant in the communication with their physicians. Physicians may also fail to recognize symptoms that are not easily measurable. The patient and physician may also record the patient’s symptoms for different reasons: The patient is encouraged to record the symptoms so that the physician using the questionnaire is properly informed about the patient’s condition. The physician records symptoms as a useful decision-making tool for prognostic stratification of the patient. A systematic review comparing patient-reported and clinician-observed symptoms in cancer patients found that physician assessments were more aligned with clinical outcomes, whereas patients reported symptoms impacting their daily activities and quality of life [31]. The MPN Landmark survey also found that only 26% of participating physicians used a validated symptom assessment form, with nearly half using their own rating methods [3].
Most notably, we found a significant association between overall survival and the presence of severe symptoms, primarily due to severe fatigue and severe weight loss. After considering persistent severe symptom burden (patient-reported score of 7 or higher at baseline and first follow-up), the hazard of death decreased. These results suggest that severe symptoms may serve as a predictor of short-term survival in MPN patients. However, we still observed a significant effect of persistent severe weight loss on overall survival despite the small number of patients with persistent severe weight loss.
In a study on Thai MPN patients, symptom burden was not associated with inferior overall survival [11], although it included a lower number (n = 80) of patients and identified only the strongest predictors as significantly associated with survival. Conversely, a recent study including approximately 800 participants from a Canadian MPN registry found a significantly higher risk of death in patients with higher symptom burden, defined as >20 points on the MPN-SAF Total Symptom Score [19]. Therefore, the impact of symptom burden on patient survival warrants further investigation in future studies.
The presence of constitutional symptoms is included in prognostic scores for MF, such as IPSS [32], DIPSS [33], DIPPS+ [34] and MIPSS70 [35], but to our knowledge not in prognostic scores for ET or PV. Given our findings on the effect of severe symptom burden on overall survival, the introduction of new prognostic scores incorporating a symptom component may be justified in the future.
The main strength of the study is the availability of both patient and physician reports, documented at approximately the same point in time. Despite patients reporting on a scale of 0–10 and physicians reporting as yes or no, we were able to examine the agreement on the presence of symptoms from both perspectives. Furthermore, this study benefits from its large sample size with data from a population-based registry of 3979 MPN patients. The longitudinal design allowed us to examine symptom burden over time. Our analysis included 77% of all patients enrolled in the GSG-MPN Bioregistry, and our cohort´s characteristics are similar to those of the overall registry population, excluding a selection bias. Moreover, the GSG-MPN Bioregistry is representative of the German MPN patient population.
A major limitation of the study is related to the sample size: although high numbers were available for baseline, lower numbers were available for the follow-up visits (with only 80 patients at the final data point). Within the Bioregistry of the German MPN Study Group more than 6000 MPN patients have been registered so far. Missing patient questionnaires were the main reason for not including all patients in our analysis. At baseline, physician assessments were missing in 3.2% (166/5198) of cases. In order to include as many data points as possible, we also incorporated partially completed questionnaires and assessments. A second limitation of our study was the interval of assessments: within the registry documentation is scheduled in yearly intervals. Therefore, short-term changes in symptom burden and/or severity could not be assessed at higher temporal granularity. However, when considering the complete cohort, symptom prevalence appeared to be rather stable over time. In general, symptom burden in MPN patients was high and did not decrease over time. Discrepancy in symptom recognition between patients and physicians was evident, with physicians underestimating symptom burden as reported by their patients. Of note, patient-reported symptom burden was not lower in those on cytoreductive therapy, and physicians did not report symptoms differently when their patient was receiving cytoreductive treatment. A third limitation of our study was the fact that physicians did not rate symptoms on the same questionnaire as the patients, but, for physicians´ assessments, the mere presence or absence of a symptom was documented from the medical record.
Taken together, this analysis in a large cohort of MPN patients suggests significant discrepancies in symptom recognition in an intra-individual assessment between patient-reported and physician-reported data. Physicians reported a much lower symptom presence than patients. Severe patient-reported symptoms were found to be an independent risk factor for short-term death and should be carefully assessed in routine clinical practice. These findings highlight the need to include patient-reported outcome tools, such as validated symptom questionnaires, into both clinical routine and the drug development process in clinical trials [36].
Data availability
The datasets generated during and/or analyzed during the current study are potentially available from the corresponding author on reasonable request.
References
Perner F, Perner C, Ernst T, Heidel FH. Roles of JAK2 in Aging, Inflammation, Hematopoiesis and Malignant Transformation. Cells. 2019;8:854.
Mesa R, Miller CB, Thyne M, Mangan J, Goldberger S, Fazal S, et al. Myeloproliferative neoplasms (MPNs) have a significant impact on patients’ overall health and productivity: the MPN Landmark survey. BMC Cancer. 2016;16:167–2.
Harrison CN, Koschmieder S, Foltz L, Guglielmelli P, Flindt T, Koehler M, et al. The impact of myeloproliferative neoplasms (MPNs) on patient quality of life and productivity: results from the international MPN Landmark survey. Ann Hematol. 2017;96:1653–65.
Mesa RA, Miller CB, Thyne M, Mangan J, Goldberger S, Fazal S, et al. Differences in treatment goals and perception of symptom burden between patients with myeloproliferative neoplasms (MPNs) and hematologists/oncologists in the United States: Findings from the MPN Landmark survey. Cancer. 2017;123:449–58.
Mesa RA, Niblack J, Wadleigh M, Verstovsek S, Camoriano J, Barnes S, et al. The burden of fatigue and quality of life in myeloproliferative disorders (MPDs): an international Internet-based survey of 1179 MPD patients. Cancer. 2007;109:68–76.
Emanuel RM, Dueck AC, Geyer HL, Kiladjian J, Slot S, Zweegman S, et al. Myeloproliferative neoplasm (MPN) symptom assessment form total symptom score: prospective international assessment of an abbreviated symptom burden scoring system among patients with MPNs. J Clin Oncol. 2012;30:4098–103.
Johansson P, Mesa R, Scherber R, Abelsson J, Samuelsson J, Birgegård G, et al. Association between quality of life and clinical parameters in patients with myeloproliferative neoplasms. Leuk Lymphoma. 2012;53:441–4.
Anderson LA, James G, Duncombe AS, Mesa R, Scherber R, Dueck AC, et al. Myeloproliferative neoplasm patient symptom burden and quality of life: evidence of significant impairment compared to controls. Am J Hematol. 2015;90:864–70.
Yassin MA, Taher A, Mathews V, Hou H, Shamsi T, Tuğlular TF, et al. MERGE: A Multinational, Multicenter Observational Registry for Myeloproliferative Neoplasms in Asia, including Middle East, Turkey, and Algeria. Cancer Med. 2020;9:4512–26.
Brochmann N, Flachs EM, Christensen AI, Bak M, Andersen CL, Juel K, et al. Health-Related Quality of Life in Patients with Philadelphia-Negative Myeloproliferative Neoplasms: A Nationwide Population-Based Survey in Denmark. Cancers. 2020;12:3565.
Cherdchoo N, Polprasert C, Rojnuckarin P, Kongkiatkamon S. Clinical characteristics and symptom burden of Thai myeloproliferative neoplasm patients. Hematology. 2023;28:2280731.
Eppingbroek AAM, Lechner L, Bakker EC, Nijkamp MD, de Witte MA, Bolman CAW. The personal impact of living with a myeloproliferative neoplasm. Psychooncology. 2024;33:e6338.
Schmidt A, Bernhardt C, Burkle D, Fries S, Hannig CV, Jentsch-Ullrich K, et al. Diagnosis and treatment of MPN in real life: exploratory and retrospective chart review including 960 MPN patients diagnosed with ET or MF in Germany. J Cancer Res Clin Oncol. 2023;149:7197–206.
Crodel CC, Jentsch-Ullrich K, Reiser M, Jacobasch L, Sauer A, Tesch H, et al. Cytoreductive treatment in real life: a chart review analysis on 1440 patients with polycythemia vera. J Cancer Res Clin Oncol. 2022;148:2693–705.
Jentsch-Ullrich K, Eberhardt J, Zeremski V, Koehler M, Wolleschak D, Heidel FH. Characteristics and treatment of polycythemia vera patients in clinical practice: a multicenter chart review on 1476 individuals in Germany. J Cancer Res Clin Oncol. 2016;142:2041–9.
Palandri F, Palumbo GA, Iurlo A, Polverelli N, Benevolo G, Breccia M, et al. Differences in presenting features, outcome and prognostic models in patients with primary myelofibrosis and post-polycythemia vera and/or post-essential thrombocythemia myelofibrosis treated with ruxolitinib. New perspective of the MYSEC-PM in a large multicenter study(⁎). Semin Hematol. 2018;55:248–55.
Verstovsek S, Mesa RA, Gotlib J, Levy RS, Gupta V, DiPersio JF, et al. A double-blind, placebo-controlled trial of ruxolitinib for myelofibrosis. N Engl J Med. 2012;366:799–807.
Harrison C, Kiladjian J, Al-Ali HK, Gisslinger H, Waltzman R, Stalbovskaya V, et al. JAK inhibition with ruxolitinib versus best available therapy for myelofibrosis. N Engl J Med. 2012;366:787–98.
Poullet A, Busque L, Sirhan S, Delage R, Cournoyer G, Chamakhi I, et al. Prospective Symptom Burden Analysis in 784 Patients with Myeloproliferative Neoplasms: High Burden Correlates with Inflammatory/Genetic Biomarkers and Reduced Survival. Blood. 2023;142:917.
Vardiman JW, Thiele J, Arber DA, Brunning RD, Borowitz MJ, Porwit A, et al. The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes. Blood. 2009;114:937–51.
Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, Le Beau MM, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127:2391–405.
Barosi G, Mesa RA, Thiele J, Cervantes F, Campbell PJ, Verstovsek S, et al. Proposed criteria for the diagnosis of post-polycythemia vera and post-essential thrombocythemia myelofibrosis: a consensus statement from the International Working Group for Myelofibrosis Research and Treatment. Leukemia. 2008;22:437–8.
Cohen J. A Coefficient of Agreement for Nominal Scales. Educational Psychological Measur. 1960;20:37–46.
McHugh ML. Interrater reliability: the kappa statistic. Biochem Med. 2012;22:276–82.
R Core Team R. R Core Team R: a language and environment for statistical computing. R Core Team: Vienna, Austria 2020.
Abelsson J, Andréasson B, Samuelsson J, Hultcrantz M, Ejerblad E, Johansson B, et al. Patients with polycythemia vera have worst impairment of quality of life among patients with newly diagnosed myeloproliferative neoplasms. Leuk Lymphoma. 2013;54:2226–30.
Scherber RM, Geyer H, Harrison CN, Kosiorek HE, Dueck AC, Kiladjian J, et al. Impact of Disease Duration upon Symptom Burden Amongst Patients with Myeloproliferative Neoplasms (MPNs). Blood. 2015;126:4073.
Mazza GL, Mead-Harvey C, Mascarenhas J, Yacoub A, Kosiorek HE, Hoffman R, et al. Symptom burden and quality of life in patients with high-risk essential thrombocythaemia and polycythaemia vera receiving hydroxyurea or pegylated interferon alfa-2a: a post-hoc analysis of the MPN-RC 111 and 112 trials. Lancet Haematol. 2022;9:e38–48.
Umashankar S, Basu A, Esserman L, Van’t VeerL, Melisko ME. Concordance between patient-reported and physician-documented comorbidities and symptoms among Stage 4 breast cancer patients. Cancer Med. 2023;12:20906–17.
Ribbands A, Boytsov N, Bailey A, Gorsh B, Luke E, Lambert A. Real-world patient-reported outcomes and concordance between patient and physician reporting of side effects across lines of therapy in multiple myeloma within the USA. Support Care Cancer. 2023;31:371–x.
Xiao C, Polomano R, Bruner DW. Comparison Between Patient-Reported and Clinician-Observed Symptoms in Oncology. Cancer Nurs. 2013;36:E1–E16.
Cervantes F, Dupriez B, Pereira A, Passamonti F, Reilly JT, Morra E, et al. New prognostic scoring system for primary myelofibrosis based on a study of the International Working Group for Myelofibrosis Research and Treatment. Blood. 2009;113:2895–901.
Passamonti F, Cervantes F, Vannucchi AM, Morra E, Rumi E, Pereira A, et al. A dynamic prognostic model to predict survival in primary myelofibrosis: a study by the IWG-MRT (International Working Group for Myeloproliferative Neoplasms Research and Treatment). Blood. 2010;115:1703–8.
Gangat N, Caramazza D, Vaidya R, George G, Begna K, Schwager S, et al. DIPSS Plus: A Refined Dynamic International Prognostic Scoring System for Primary Myelofibrosis That Incorporates Prognostic Information From Karyotype, Platelet Count, and Transfusion Status. JCO. 2010;29:392–7.
Guglielmelli P, Lasho TL, Rotunno G, Mudireddy M, Mannarelli C, Nicolosi M, et al. MIPSS70: Mutation-Enhanced International Prognostic Score System for Transplantation-Age Patients With Primary Myelofibrosis. JCO. 2018;36:310–8.
Efficace F, Buckstein R, Abel GA, Giesinger JM, Fenaux P, Bewersdorf JP, et al. Toward a more patient-centered drug development process in clinical trials for patients with myelodysplastic syndromes/neoplasms (MDS): Practical considerations from the International Consortium for MDS (icMDS). Hemasphere. 2024;8:e69.
Acknowledgements
The authors would like to thank registry teams in Aachen and Ulm for support of study conduct. The authors would also like to thank the registry investigators and patients for their participation in this registry. FHH was supported by grants of the German Research Council (DFG): HE6233/15-1, project number 517204983 and HE 6233/16-1, project number 517204983.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Consortia
Contributions
KM analyzed the data, interpreted the results, wrote the first draft, and approved the final manuscript. FHH interpreted the results, wrote the first draft, contributed to acquiring data, reviewing the final manuscript, and approved the final manuscript. SK, RS, JL, FS, MG, MK, CC, AH, HS, JRG, HA-A, HB, AR, GB, KK, THB, WH and KD contributed to acquiring data, reviewing the final manuscript, and approved the final manuscript. SI designed the study, interpreted the results, wrote the first draft, contributed to acquiring data, reviewing the final manuscript, and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
KM reports no conflicts of interest. FHH reports research funding from Novartis, BMS/Celgene, CTI and Consultancy for Novartis, BMS/Celgene, AOP Pharma, Janssen, GSK, Abbvie, Kartos, Sierra Oncology. SK reports research funding from Novartis, Bristol-Myers Squibb, AOP Pharma, Janssen, Geron, Imago Biosciences; advisory board honoraria and/or consulting fees from Pfizer, Incyte, Ariad, Novartis, AOP Pharma, BMS, Celgene, Geron, Janssen, CTI, Roche, Baxalta, Sanofi, Sierra Oncology, GSK, Abbvie; patent for BET inhibitor at RWTH Aachen University; honoraria from Novartis, BMS, Celgene, Geron, Janssen, Pfizer, Incyte, Ariad, Shire, Roche, AOP Pharma, GSK, Abbvie, iOMEDICO, MPN Hub; and other financial support (e.g. travel support) from Alexion, Novartis, BMS, Incyte, Ariad, AOP Pharma, Baxalta, CTI, Pfizer, Sanofi, Celgene, Shire, Janssen, Geron, Abbvie, Kartos, Sierra Oncology, Imago Bioscience, GSK, Abbvie, MSD, iOMEDICO. RS reports no conflict of interest. JL reports no conflict of interest. FS reports advisory board and/or speaker honoraria from Abbvie, BMS/Celgene, GSK, Incyte, MorphoSys, Novartis, and Pfizer. MG reports consultancy for AOP Orphan, Novartis, BMS, AbbVie, Pfizer, Roche, Janssen, Gilead, AstraZeneca, Sierra, Lilly, GSK and honoraria from AOP Orphan, Novartis, BMS, AbbVie, Pfizer, Roche, Janssen, Gilead, AstraZeneca, Sierra, Lilly, GSK. MK reports no conflicts of interest. CC reports advisory board honoraria from GSK, BMS, BeiGene and AstraZeneca, honoraria from GSK, Novartis, BMS, Synlab, AOP Orphan and AstraZeneca; and other financial support (e.g. travel support) from Novartis. AH reports research support from Novartis, BMS, Incyte, Pfizer, Terns, Enliven; honoraria from Novartis and Incyte; Editor-in-Chief, Leukemia. HS reports no conflicts of interest. JRG reports honoraria from Bristol-Myers Squibb, Pfizer, Novartis, GlaxoSmithKline, Blueprint Medicines, AOP Orphan Pharmaceuticals, pharma&, Incyte; advisory board participation: Imago BioSciences, Proteros biostructures, CTI Biopharma, Bristol-Myers Squibb, Pfizer, Novartis, AbbVie, GlaxoSmithKline, Blueprint Medicines, AOP Orphan Pharmaceuticals, Incyte and travel support from Bristol-Myers Squibb, Novartis, AOP Orphan Pharmaceuticals, Incyte. HA reports consultancy for BMS, Novartis, Abbvie, AOP, GSK, Otsuka, and has received honoraria from BMS, Novartis, Abbvie, AOP, GSK, Blueprint, Stemline, MSD, Otsuka and membership on board of directors/ advisory committees from BMS, Novartis, Abbvie, AOP, and GSK, and other financial support (travel grants) from Alexion and Abbvie. HB reports honoraria from Abbvie, BMS, GSK, Lilly, MSD, Novartis, Pierre Fabre Pharma, and Servier. AR reports advisory boards and honoraria from AOP, Blueprint, Cogent, Novartis and GSK. GB reports no conflicts of interest. KK reports no conflicts of interest. THB has been a consultant for Gilead, Janssen, Merck, Novartis, and Pfizer, and has received research support from RepeatDx, Novartis and Pfizer. WH reports honoraria from Pfizer. KD reports financial relationsships or affiliations with Novartis, AOP Health, Celgene/BMS, JAZZ, Astellas, Agios, Abbvie, GSK, and MSD. SI reports advisory board honoraria from GSK, Silence Therapeutics, Pfizer, Incyte, and Novartis, honoraria from GSK, Novartis, BMS, Pfizer, Incyte, AOP Orphan; and other financial support (e.g. travel support) from Alexion, Novartis, Pfizer, Mundipharma, Roche, Hexal and AOP Orphan.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Manz, K., Heidel, F.H., Koschmieder, S. et al. Comparison of recognition of symptom burden in MPN between patient- and physician-reported assessment – an intraindividual analysis by the German Study Group for MPN (GSG-MPN). Leukemia 39, 864–875 (2025). https://doi.org/10.1038/s41375-025-02524-7
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41375-025-02524-7
This article is cited by
-
Assessing myelofibrosis burden on QoL and productivity from healthcare personnel and patient perspectives in India
BMC Cancer (2025)
-
Response to the commentary by Xu et al. on the PV-AIM study
Leukemia (2025)
-
Challenges in predicting hydroxyurea resistance and reducing thrombotic risk in polycythemia vera patients: unmasking the limits of its machine learning study
Leukemia (2025)
-
Prediction of resistance to hydroxyurea therapy in patients with polycythemia vera: a machine learning study (PV-AIM) validated in a prospective interventional phase IV trial (HU-F-AIM)
Leukemia (2025)
-
From symptom scales to regulatory endpoints: the evolution and clinical impact of patient-reported outcome measures in myeloproliferative neoplasms
Clinical and Experimental Medicine (2025)
