
Abstract
Introduction
To promote home phototherapy adoption, clearer insights are needed on current evidence and the population most likely to benefit.
Methods
Six online databases were searched until 20 January 2025. Studies were included that reported on (cost-)effectiveness, safety, and/or implementation barriers and facilitators of home phototherapy. Two reviewers independently extracted data and assessed bias using the Mixed Methods Appraisal Tool. Data were pooled via random-effects meta-analysis. Barriers and facilitators were analyzed using the Theoretical Domains Framework. GRADE was used to assess evidence quality.
Results
Thirty-one studies were included, representing 5059 neonates, 869 healthcare professionals, and 478 parents. Risk of bias was moderate. Hospital (re)admission following home phototherapy was 3.5% (95% CI, 2.2–5.3%). No difference was found in treatment duration (mean difference = +4.9 h, 95% CI –8.0 to +17.9) and daily decline in bilirubin (mean difference = +5.7 μmol/L, 95% CI −2.6 to +13.9). No studies evaluated cost-effectiveness. Key facilitators included eligibility screening and parental education, while key barriers included bilirubin measurement, healthcare professionals’ concerns about homecare consequences, and parental insecurity. Quality of evidence was rated low for all outcomes.
Conclusion
Evidence suggests home phototherapy can be an alternative to in-hospital treatment for hyperbilirubinemia in near-term neonates. Clinical recommendations are limited due to low-certainty evidence.
Impact
-
Home phototherapy can be a safe and effective alternative to in-hospital treatment for low-risk neonates with hyperbilirubinemia. Strength of this recommendation is low.
-
Our study is the first to systematically synthesize parent/caregiver and healthcare professional perspectives on home phototherapy using the Theoretical Domains Framework.
-
Key facilitators included eligibility screening and parental education, while key barriers included concerns about home care consequences by healthcare professionals and parental insecurity. Addressing these barriers through improved support and accurate monitoring is recommended.
Similar content being viewed by others

Introduction
Neonatal jaundice is caused by elevated levels of unconjugated bilirubin, affecting 60% of full term neonates and up to 80% of preterm neonates.1,2 Depending on screening practices and treatment thresholds, which vary in different guidelines, 4–9% of neonates born after 35 weeks of gestation will develop clinically significant hyperbilirubinemia.2,3,4 Phototherapy continues to be the primary treatment to decrease unconjugated serum bilirubin levels and is applied in-hospital in most settings.5 The light used during phototherapy treatment converts bilirubin into water-soluble compounds. It allows the neonate’s body to eliminate it through urine and stool. This process helps prevent bilirubin from reaching dangerously high levels, which could otherwise result in brain damage (kernicterus) if untreated.6,7
Currently, severe hyperbilirubinemia is a primary cause of hospitalization within the first week of the neonate’s life, accounting for up to 35% of hospital (re)admissions in high-resource settings.2 Home phototherapy has the potential to avoid hospital admissions, reduce associated costs, and promote parent-child bonding. Despite this, home phototherapy for neonatal hyperbilirubinemia is not commonplace. Barriers to implementation, such as the lack of a uniform protocol and concerns about potential consequences of home-based care, may arise at various levels.8,9 In the last decade, five systematic reviews including two meta-analyses have evaluated home phototherapy, each focusing on various outcomes or study types, with contradicting results.10,11,12,13,14 Moreover, international guidelines use different criteria for selecting neonates and parent(s)/caregiver(s) for home phototherapy.15 In order to facilitate widespread adoption of home phototherapy in a safe and effective manner, clearer insights are needed on the resulting recommendations arising from the current existing evidence and the population that home phototherapy may be best utilized. Thus, a clear overview is needed for presenting evidence summaries, using a systematic approach offered by the GRADE guideline.16,17
We therefore conducted an updated systematic review, including meta-analyses, to provide the most comprehensive synthesis to date on home phototherapy use for neonatal hyperbilirubinemia. This includes summarizing quantitative and qualitative evidence on (cost-)effectiveness, safety, inclusion criteria, and parental and health care professionals’ experiences. We assessed the certainty of the results for each outcome. This work will facilitate further consideration of home phototherapy in international guidelines on the management of hyperbilirubinemia in neonates.
Methods
This review is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Supplementary Table S1).18,19 Our review was prospectively registered in PROSPERO, registration number: CRD42023386798.20
Study inclusion
We included primary quantitative, qualitative, and mixed-methods studies that assessed the effectiveness and/or safety of home phototherapy for neonatal hyperbilirubinemia, or that provided insight into parental or health care professionals’ experiences, or into barriers and/or facilitators to its implementation. The outcomes of interest are summarized below. Case reports, commentaries, reviews, study protocols, and conference abstracts were excluded. In-hospital phototherapy was considered the reference treatment. Studies evaluating neonates born after 35 weeks gestation, aged 0 to 28 days, were considered eligible.
Outcomes of interest
We divided the outcomes of interest into three groups: (1) effectiveness, (2) safety, (3) barriers and facilitators to implementation. First, effectiveness outcomes were defined as following: (1.1) hospital (re)admission rate, (1.2) treatment duration, (1.3) daily bilirubin reduction, (1.4) and health care costs. Second, safety outcomes included: (2.1) any adverse events of phototherapy treatment, (2.2) the need for exchange transfusion, (2.3) reported acute bilirubin encephalopathy (ABE), (2.4) and reported Kernicterus Spectrum Disorder (KSD). Finally, (3.1) the barriers and (3.2) facilitators to implementation according to parents and healthcare professionals.
Search strategy and selection criteria
The following six online databases were systematically searched for relevant studies: MEDLINE/PubMed, Embase, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Library, Web of Science and Google Scholar. We used a combination of Medical Subject Headings (MeSH) terms and free text to search for potentially eligible studies. A tailor-made search strategy for each database was designed in close collaboration with an experienced biomedical information specialist (Supplementary Table S2). There were no restrictions imposed on language, geographical location, publication date, or timeframe of the study. The search was updated on 20 January 2025 for all databases to include studies published since the initial search (8 June 2022). In addition, the reference lists of included studies and their citations (through Google Scholar) were screened to identify additional relevant studies that may have been missed. All records identified were downloaded into EndNote™ and duplicates were deleted. Two reviewers (JS and LEHW) independently screened titles and abstracts to select potentially relevant records. When a record was considered relevant or when the title/abstract was deemed insufficiently informative for deciding inclusion/exclusion, the full text was retrieved and evaluated. Discrepancies and uncertainties at any stage in this selection process were resolved through discussion with a third reviewer (JVB) until consensus was reached.
Data extraction
Data extraction was performed independently by two reviewers (JS and LEHW) using a standardized form specifically designed for this review (Supplementary Table S3). Subsequently, the reviewers shared their results and created a final extraction table. Any disagreement was discussed and resolved through consensus, if necessary with a third reviewer (JVB). The information extracted included characteristics of the study, methods, and study population, as well as the relevant outcomes (effectiveness, safety, and on barriers and facilitators to implementation according to healthcare professionals and parents). For the effectiveness and safety, numerical data were extracted. For the barriers and facilitators to implementation according to parents and healthcare professionals, themes, authors’ interpretations, and participants’ quotations of the qualitative studies, as well as data from quantitative studies were extracted. In case the data in the original publications were not sufficiently detailed or unclear, we contacted the authors for clarification and additional information.
Risk-of-bias assessment of included studies
Two reviewers independently (JS and LEHW) assessed risk of bias for each study using the Mixed Methods Appraisal Tool (MMAT).21 MMAT is designed for mixed-methods systematic reviews and appraises methodological aspects of five study designs: qualitative research, randomized studies, non-randomized studies, descriptive studies, and mixed methods studies. Any disagreement was resolved through discussion, and when necessary, by involving a third reviewer (JVB). Risk-of-bias assessment was not used to exclude any studies in this review and instead used to assess confidence in the evidence.
Grading the quality of evidence of outcomes of interest
Two reviewers independently (JS and LEHW) used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) to assess the certainty of the synthesized results for the outcomes of interest.16,17 We pre-selected the following outcomes for the GRADE assessment: (1) effectiveness: treatment duration, (2) effectiveness: daily bilirubin reduction, (3) effectiveness: hospital (re)admission rate, (4) effectiveness: healthcare costs, and (5) safety: any adverse events of phototherapy treatment.
Data synthesis
Meta-analyses
Meta-analysis was possible for the following outcomes: hospital readmission rates, daily decline of bilirubin levels, and treatment duration. Heterogeneity of the findings was assessed using the I2 statistic. An I2 > 75% was considered as substantial heterogeneity. Random effects models were used to calculate pooled estimates and the corresponding 95% confidence intervals (CI). For hospital readmission rates, the standard continuity correction (adding ½ to the number of participants with and without an event) was applied in case a study group had zero events. In case included articles reported on the same study population, this study population was then considered only once to prevent duplication in the analyses. Furthermore, subgroup analyses were conducted to evaluate whether factors as bilirubin levels, term status, and age at phototherapy initiation impacted the readmission rate. For the daily decline of bilirubin levels and the treatment duration, only studies with a control group (in-hospital phototherapy) were included in the meta-analyses. Analyses were performed using R (version 4.3.1.) packages meta version 4.9-7 and metaphor 2.0-0. If necessary, we converted bilirubin levels from mg/dL to μmol/L by applying a conversion factor of 17.1.
Barriers and facilitators according to healthcare professionals and parents
To further explore barriers and facilitators to implementation of home phototherapy, both qualitative and quantitative findings were synthesized based on the Theoretical Domains Framework (TDF).22 TDF provides a theory-based approach to identify determinants. This framework consists of 14 domains that integrate constructs from multiple theories in relation to behavior change: 1) knowledge; 2) skills; 3) social/professional role and identity; 4) beliefs about capabilities; 5) optimism; 6) beliefs about consequences; 7) reinforcement; 8) intentions; 9) goals; 10) memory, attention, and decision processes; 11) environmental context and resources; 12) social influences; 13) emotion; and 14) behavioral regulation.22 Two reviewers (JS and LEHW) discussed the studies to reach consensus regarding the identification and coding of themes. Discrepancies were resolved by discussion with an implementation expert (EI) until consensus was reached.
Results
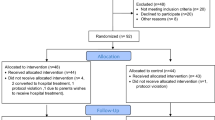
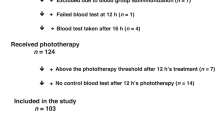
A flow diagram of the study selection process is presented in Fig. 1. We identified 857 records from database searches, and after removing duplicates, 510 studies were screened based on their titles and abstracts. Following this initial screening, 63 potentially relevant studies were retrieved for full text assessment. Additionally, one more relevant study was identified through reference searching. A total of 31 studies were included in this systematic review.

PRISMA flow diagram of the literature search and selection process.18
Study characteristics
Table 1 lists the main study characteristics of the 31 included studies, representing 5059 neonates, 869 health care professionals, and 478 parents. This compilation comprises five randomized controlled trials,23,24,25,26,27 10 non-randomized studies,28,29,30,31,32,33,34,35,36,37 13 quantitative descriptive studies,8,9,38,39,40,41,42,43,44,45,46,47,48 one mixed-methods study,49 and two qualitative studies.50,51 Five studies have examined data from two study populations, with one study population being explored in three papers,24,25,26 and the other in two papers respectively.23,27 Eleven studies were performed in North America,29,33,34,35,39,40,41,42,43,44,45 nine in Europe,9,24,25,26,28,32,47,48,51 eight in Asia,23,27,30,36,37,38,46,49 and three in Oceania.8,31,50 Studies were published between 1984 and 2024.
The home phototherapy programs in the included studies varied in several key characteristics, including different inclusion criteria for home phototherapy program. The most reported characteristics determining eligibility were gestational age and postnatal age at the initiation of phototherapy. Some studies included neonates with a gestational age from 35 weeks,4,28,31,32,48 others 36 weeks,24 and some 37 weeks.23,30,34,35,43 The lower bound of postnatal age at start of phototherapy varied between 24 h,29,30,40,43,46 48 h,24,32,35,37,46,47 and 72 h,23,27 as summarized in Table 1. Characteristics of the home phototherapy devices used in the included studies can be found in Supplementary Table S4.
Risk of bias of the studies
Detailed critical appraisals of included studies are available in Supplementary Table S5. In the five randomized controlled trials, multiple studies inadequately reported details regarding randomization and blinding. All quantitative non-randomized studies were rated as having a low risk of bias. Risk of bias of quantitative descriptive studies varied, often affected by factors such as the lack of reported statistical analysis techniques and unclear risks of nonresponse bias. In the mixed-methods study, the rationale for using the methodology, integration, and interpretation of the qualitative and quantitative data was missing. The qualitative studies were rated as moderate to low risk of bias. Overall, risk of bias of most studies was rated as moderate.
Primary outcome - effectiveness
Data on effectiveness of home phototherapy were available in eight (non)-randomized studies and in 13 single-arm studies (Supplementary Table S6).
Hospital readmission rates following home phototherapy
Data from 17 studies were included in this meta-analysis.8,24,27,28,29,31,32,33,35,37,38,39,40,42,43,45,48 The mean hospital (re)admission rate across these studies was 3.5% (95% CI) 2.2–5.3; I2 = 67%; 4010 participants) (Fig. 2). Reasons for readmission included: reduced exposure duration to phototherapy due to language and cultural barriers, non-compliance with the treatment protocol, parental anxiety, and clinical concerns for the neonate, such as temperature instability.

CI confidence interval.
A subgroup analysis was conducted on studies that included only neonates with bilirubin levels above the phototherapy threshold at initiation of treatment, showing a readmission rate of 3.7% (95% CI = 2.3–5.8; 1389 participants). Similarly, a subgroup analysis of studies that included only term neonates showed a readmission rate of 4.8% (95% CI = 2.5–12.7; 101 participants). For studies including only neonates above 48 h of postnatal age at initiation of phototherapy, the readmission rate was 4.4% (95% CI = 2.4–7.9; 254 participants).
Treatment duration in home versus in-hospital phototherapy
Data on treatment duration of home phototherapy compared to in-hospital phototherapy were available in seven studies.24,27,29,32,34,35,37 There was no statistically significant difference in treatment duration between home phototherapy and in-hospital phototherapy (mean difference (MD) = +4.9 h, 95% CI = –8.0 to +17.9; I2 = 91%; 620 participants) (Fig. 3a).

a Treatment duration in home phototherapy versus in-hospital phototherapy. b Daily serum bilirubin reduction in treatment with home phototherapy versus in-hospital phototherapy. CI confidence interval, SD standard deviation, PT phototherapy.
Serum bilirubin reduction in home versus in-hospital phototherapy
Data retrieved from six studies were included in this meta-analysis.29,32,34,35,36,37 No statistically significant difference was found in daily serum bilirubin reduction between home phototherapy and in-hospital phototherapy (MD = +5.7 μmol/L, 95% CI = −2.6 to +13.9; I2 = 80%; 459 participants) (Fig. 3b).
Primary outcome - health care costs
Health care costs data were available in 12 studies.8,26,29,30,31,35,37,40,41,42,43,47 Due to the heterogeneity of study designs and the diversity in cost measurements, we could not perform a meta-analysis. Five studies included a control group, of which all five showed that home phototherapy was less expensive than in-hospital phototherapy (savings ranging from US$70-US$982 per patient per day).26,30,31,37,40 The cost savings in each individual study are detailed in Supplementary Table S7. No studies conducted formal cost-effectiveness analyses.
Primary outcome - safety
No severe adverse events were reported among 688 neonates treated with home phototherapy from eight studies24,27,29,35,37,42,46,47 (Supplementary Table S8). There were no neonates that needed exchange transfusions.24 In a few studies, mild adverse events were reported such as vomiting, hyperthermia, restlessness or dehydration.29,46 Within individual studies with a control group, no statistically significant differences were found in the occurrence of mild adverse events such as skin rashes, hyperthermia, diarrhea, vomiting, weakness and restlessness between home phototherapy and in-hospital phototherapy.27,37 None of the readmitted neonates needed exchange transfusion, or developed ABE or KSD.
Primary outcome - barriers and facilitators according to parents and health care professionals
Seventeen studies explored perspectives of parents and health care professionals.8,9,31,32,35,37,40,41,42,43,44,45,47,48,49,50,51 Fourteen studies were quantitative studies, two qualitative studies, and one was a mixed-methods study. Three studies primarily focused on health care professionals’ attitudes and experiences,9,44,50 six studies evaluated parental experiences,35,37,45,47,48,51 and the remaining eight studies evaluated both parental and health care professionals’ experiences.8,31,32,40,41,42,43,49
A summary of barriers and facilitators according to the TDF domain is provided in Table 2. The most important factors were related to the following domains: knowledge, skills, social/professional role, beliefs about consequences, goals, environmental context and resources, and emotion, and are described below.
Knowledge about home phototherapy was seen as an important facilitator by parents, which included demonstration on how to use the phototherapy equipment32,50 and the availability of (written) information about phototherapy.40,41,50,51 Lack of information, such as missing information about the expected duration of home phototherapy treatment, was mentioned as a barrier.51 Effectively informing all health care professionals about the home phototherapy program proved to be challenging. Additionally, health care professionals had reservations about the community’s ability to provide the appropriate care.8 Knowledge about careful screening and selection of potentially eligible patients for home phototherapy was reported as a facilitator.41,44,50
In the ‘skills’ domain, parents reported barriers to properly administering home phototherapy, including difficulties with the equipment, such as placing the neonate’s eye mask on correctly.32,35,48,51 However, ‘the equipment was easy to use’ was reported as a facilitator in several studies, specifically when using the BiliCocoon Bag (NeoMedLight, Villeurbanne, France) or the BiliSoft blanket (GE Healthcare, Chicago, Illinois).32,34,51
In the domain ‘social/professional role and identity’, parents viewed the involvement of different health care professionals, such as daily contact with nurses and/or support from midwives, as a key facilitator.8,31,32,40,41,43,49 The ability to contact the hospital for advice if parents had concerns was also regarded as a facilitator.8,51
Beliefs about the potential adverse consequences of home-based care was seen as an important barrier, including concerns about parental compliance and the safety of the neonate due to insufficient monitoring.8,42,44,50 However, positive consequences were also reported by health care professionals, including decreased health care expenditure42,44,50 and a decreased workload.49,50
In the domain ‘goals’, multiple facilitators were identified. The most commonly mentioned goals of home phototherapy, according to both health care professionals and parents, were family centered care,8,32,50 improved parent-child bonding,8,32,35,42,51 and discharging otherwise healthy babies from the hospital.44,50
In the ‘environmental context and resources’ domain, we found significant barriers, including the travel distance from parental home to the hospital for check-ups,35,50 difficulties with blood draws,31,40,44 and issues with insurance reimbursement.44,45 The most frequently mentioned facilitator in this domain was the benefit of being in one’s own environment.32,45,47,51 Furthermore, parents mentioned freedom and the ability to maintain routines at home as facilitators.32,51 Health care professionals cited flexibility in their schedules as a facilitator.31,41
Important facilitators and barriers were found in the ‘emotional’ domain. (Concern of) parental anxiety was mentioned as a barrier from both parents’ and health care professionals’ perspectives.44,45,51 Furthermore, health care professionals mentioned apprehensiveness about parental non-compliance with phototherapy44,50 and fears of overheating or dehydration44 as barriers. Facilitators included the perception that hospitalization is more traumatic,51 and a perceived reduction in parental stress.23,51
Certainty of evidence
The quality of the evidence included in the systematic review was rated using GRADE. For each of the included studies, the evidence-level was determined. The results of these assessment are summarized in Supplementary Table S9. All outcomes were considered to be of low or very low quality.
Discussion
This comprehensive mixed-methods systematic review and meta-analysis provides a synthesized framework on the best available evidence of home phototherapy use for neonatal hyperbilirubinemia. By pooling data from over four thousand (near) term neonates treated with home phototherapy, we found a mean hospital readmission rate of 3.5%. This did not vary substantially according to the eligibility criteria for home phototherapy used in individual studies. Daily serum bilirubin reduction and treatment duration were similar between home phototherapy and in-hospital phototherapy, and no severe adverse events were reported. All studies that included a control group showed that home phototherapy was less expensive than in-hospital phototherapy. However, formal cost-effectiveness assessments were lacking. These findings suggest that home phototherapy for neonatal hyperbilirubinemia can be an effective and safe alternative to in-hospital phototherapy in a selected low-risk patient group (e.g. gestational age ≥ 35 weeks, postnatal age ≥24 h). Still, the quality of evidence is of low certainty.
To successfully implement home phototherapy, the following considerations should be taken into account, based on insights from 869 health care professionals and 478 parents. First, it is important to thoroughly screen neonates and their parents to determine their suitability for home phototherapy. Second, providing comprehensive education to parents about jaundice, phototherapy, the phototherapy device, and about the process and benefits of home phototherapy is necessary. Finally, maintaining good communication and documentation regarding the treatment and providing a designated contact person for parents or caregivers are essential. Several key barriers must also be addressed. Challenges in home bilirubin quantification need to be mitigated. Concerns from health care professionals about the potential adverse consequences of home-based care can be alleviated through clear (inter-)national guidelines and support structures, such as home visits by (maternity care) nurses or community midwives. Additionally, reducing parental insecurity via offering adequate information, documentation and home support is crucial.
Previous systematic reviews and meta-analyses had contradicting findings and therefore different clinical recommendations.10,11,12,13,14 To our knowledge, this study represents the most comprehensive assessment to date regarding home phototherapy for neonatal hyperbilirubinemia. We conducted a highly comprehensive search strategy, covering several electronic databases, reference searches, and citation searches. One of the strengths of this study is that we included all studies designs reporting data on home phototherapy for hyperbilirubinemia in (near) term neonates, including qualitative and mixed-methods studies. Moreover, our study is the first to systematically synthesize the perspectives from both parent(s)/caregiver(s) and health care professionals on home phototherapy based on the Theoretical Domains Framework, providing a broad scope of analysis. We incorporated the GRADE guideline which provided a clear overview of the existing certainty of evidence.
Inherent to a systematic review, our work is limited by the amount and quality of the underlying evidence. Specifically, we were unable to obtain full access to some potentially relevant - but mostly older - studies, despite efforts to mitigate this issue by using available abstracts and contacting authors and journals for access. This may have led to an incomplete representation of the current evidence base. Furthermore, the moderate risk of bias in the included studies and the absence of a control group in most studies needs to be considered when interpreting the results. Between-study heterogeneity in methodology, differences in inclusion criteria for home phototherapy, in phototherapy devices (including variation in irradiance), and in phototherapy treatment thresholds should also be taken into consideration. As most studies included in this review were conducted in high- or upper-middle-income countries, generalizability of the findings to low- or middle-income countries is unclear and likely limited.
Conclusion
In conclusion, our findings indicate that home phototherapy can be a safe and effective alternative to in-hospital phototherapy for treating hyperbilirubinemia in low-risk (near) term neonates, although the strength of this recommendation is low. Careful eligibility screening and adequate parental education facilitated home phototherapy, while barriers included challenges in healthcare professionals’ concerns, and parental insecurity. Hence, addressing these and other barriers including via enhanced support and accurate home monitoring is recommended. Such aspects should be considered when formulating much-needed guidelines for safe and effective implementation of home phototherapy programs.
Data availability
All data generated or analysed during this study are included in this published article [and its supplementary information files].
References
Olusanya, B. O., Kaplan, M. & Hansen, T. W. R. Neonatal hyperbilirubinaemia: a global perspective. Lancet Child Adolesc. Health 2, 610–620 (2018).
Battersby, C., Michaelides, S., Upton, M. & Rennie, J. M. Term admissions to neonatal units in England: a role for transitional care? A retrospective cohort study. BMJ Open 7, e016050 (2017).
Kuzniewicz, M. W., Escobar, G. J. & Newman, T. B. Impact of universal bilirubin screening on severe hyperbilirubinemia and phototherapy use. Pediatrics 124, 1031–1039 (2009).
Chang, P. W., Kuzniewicz, M. W., McCulloch, C. E. & Newman, T. B. A clinical prediction rule for rebound hyperbilirubinemia following inpatient phototherapy. Pediatrics 139, e20162896 (2017).
Kumar, P., Chawla, D. & Deorari, A. Light-emitting diode phototherapy for unconjugated hyperbilirubinaemia in neonates. Cochrane Database Syst. Rev. 2011, CD007969 (2011).
Vidavalur, R. & Devapatla, S. Trends in hospitalizations of newborns with hyperbilirubinemia and kernicterus in United States: an epidemiological study. J. Matern Fetal Neonatal Med 35, 7701–7706 (2022).
Bhutani, V. K., Committee on Fetus and Newborn; American Academy of Pediatrics. Phototherapy to prevent severe neonatal hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics 128, e1046–e1052 (2011).
Jackson, C. L., Tudehope, D., Willis, L., Law, T. & Venz, J. Home phototherapy for neonatal jaundice-technology and teamwork meeting consumer and service need. Aust. Health Rev. 23, 162–168 (2000).
Cnossen, M. C. et al. Home phototherapy for neonatal hyperbilirubinemia: current practices and attitudes. Pediatr. Res. https://doi.org/10.1038/s41390-024-03754-8 (2024).
Malwade, U. S. & Jardine, L. A. Home- versus hospital-based phototherapy for the treatment of non-haemolytic jaundice in infants at more than 37 weeks’ gestation. Cochrane Database Syst. Rev. 2014, CD010212 (2014).
Li, R. et al. Efficacy of home phototherapy versus inpatient phototherapy for neonatal hyperbilirubinemia: a systematic review and meta-analysis. Ital. J. Pediatr. 50, 37 (2024).
Chu, L., Qiao, J. & Xu, C. Home-based phototherapy versus hospital-based phototherapy for treatment of neonatal hyperbilirubinemia: a systematic review and meta-analysis. Clin. Pediatr.59, 588–595 (2020).
Snook, J. Is home phototherapy in the term neonate with physiological jaundice a feasible practice? A systematic literature review. J. Neonatal Nurs. 13, 28–39 (2017).
Anderson, C. M., Kandasamy, Y. & Kilcullen, M. The efficacy of home phototherapy for physiological and non-physiological neonatal jaundice: a systematic review. J. Neonatal Nurs. 28, 312–326 (2022).
Kemper, A. R. et al. Clinical practice guideline revision: management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics 150, e2022058859 (2022).
Schunemann, H. J. et al. The development methods of official GRADE articles and requirements for claiming the use of GRADE - a statement by the GRADE guidance group. J. Clin. Epidemiol. 159, 79–84 (2023).
Guyatt, G. H. et al. What is “quality of evidence” and why is it important to clinicians?. BMJ 336, 995–998 (2008).
Page, M. J. et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71 (2021).
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G. & Group, P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339, b2535 (2009).
Stewart, L., Moher, D. & Shekelle, P. Why prospective registration of systematic reviews makes sense. Syst. Rev. 1, 7 (2012).
Hong, Q. N., Gonzalez-Reyes, A. & Pluye, P. Improving the usefulness of a tool for appraising the quality of qualitative, quantitative and mixed methods studies, the Mixed Methods Appraisal Tool (MMAT). J. Eval. Clin. Pr. 24, 459–467 (2018).
Atkins, L. et al. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implement Sci. 12, 77 (2017).
Namnabati, M., Mohammadizadeh, M. & Sardari, S. The effect of home-based phototherapy on parental stress in mothers of infants with neonatal jaundice. J. Neonatal Nurs. 25, 37–40 (2019).
Pettersson, M., Eriksson, M., Albinsson, E. & Ohlin, A. Home phototherapy for hyperbilirubinemia in term neonates-an unblinded multicentre randomized controlled trial. Eur. J. Pediatr. 180, 1603–1610 (2021).
Pettersson, M., Eriksson, M., Odlind, A. & Ohlin, A. Home phototherapy of term neonates improves parental bonding and stress: findings from a randomised controlled trial. Acta Paediatr. Int. J. Paediatr. 111, 760–766 (2022).
Pettersson, M., Ryen, L., Eriksson, M. & Ohlin, A. The cost-effectiveness of home phototherapy for hyperbilirubinemia in neonates: results from a randomized controlled trial. Sci. Rep. 13, 10727 (2023).
Sardari, S., Mohammedizadeh, M., Namnabati, M. Efficacy of home phototherapy in neonatal jaundice. J. Compr. Pediatr. 10 https://doi.org/10.5812/compreped.82630 (2019).
Coquery, S. S. et al. Discharge of newborns with risk factors of severe hyperbilirubinemia: description of a hospital at home-based care monitoring and phototherapy. Eur. J. Pediatr. 181, 3075–3084 (2022).
Eggert, L. D., Pollary, R. A., Folland, D. S. & Jung, A. L. Home phototherapy treatment of neonatal jaundice. Pediatrics 76, 579–584 (1985).
Kavosi, Z., Mozafari, M., Rezaee, M., Keshavarz, K. Cost effectiveness analysis of home-based phototherapy versus hospital-based phototherapy for treatment of neonatal Hyperbilirubinemia in shiraz, Iran. Res. Sq. https://doi.org/10.21203/rs.3.rs-1452573/v1 (2022).
Khajehei, M., Gidaszewski, B., Maheshwari, R. & McGee, T. M. Clinical outcomes and cost-effectiveness of large-scale midwifery-led, paediatrician-overseen home phototherapy and neonatal jaundice surveillance: a retrospective cohort study. J. Paediatr. Child Health 58, 1159–1167 (2022).
Noureldein, M., Mupanemunda, G., McDermott, H., Pettit, K. & Mupanemunda, R. Home phototherapy for neonatal jaundice in the UK: a single-centre retrospective service evaluation and parental survey. BMJ Paediatr. Open 5, e001027 (2021).
Orringer, K. et al. Biliblanket utilization for outpatient treatment of newborn jaundice. Clin. Pediatr.62, 725–732 (2023).
Schuman, A. J. & Karush, G. Fiberoptic vs conventional home phototherapy for neonatal hyperbilirubinemia. Clin. Pediatr. 31, 345–352 (1992).
Slater, L. & Brewer, M. F. Home versus hospital phototherapy for term infants with hyperbilirubinemia: a comparative study. Pediatrics 73, 515–519 (1984).
Yilmaz, A., Ozkiraz, S., Akcan, A. B. & Canpolat, M. Low-cost home-use light-emitting-diode phototherapy as an alternative to conventional methods. J. Trop. Pediatr. 61, 113–118 (2015).
Zainab, K. & Adlina, S. Effectiveness of home versus hospital phototherapy for term infants with uncomplicated hyperbilirubinemia: a pilot study in Pahang, Malaysia. Med. J. Malays. 59, 395–401 (2004).
Adlina, S., Ambigga, D., Narimah, A. H. H. & Ridha, A. Use of home phototherapy for neonatal jaundice. Malays. J. Public Health Med. 7, 49–52 (2007).
Chang, P. W. & Waite, W. M. Evaluation of home phototherapy for neonatal hyperbilirubinemia. J. Pediatr. 220, 80–85 (2020).
Dortch, E. & Spottiswoode, P. New light on phototherapy: home use. Neonatal Netw. 4, 30–34 (1986).
Ellis, J. Home phototherapy for newborn jaundice. Birth 12, 15–17 (1985).
Grabert, B. E., Wardwell, C. & Harburg, S. K. Home phototherapy. An alternative to prolonged hospitalization of the full-term, well newborn. Clin. Pediatr. 25, 291–294 (1986).
Hamelin, K. & Seshia, M. Home phototherapy for uncomplicated neonatal jaundice. Can. Nurse 94, 39–40 (1998).
Meropol, S. B., Luberti, A. A., De Jong, A. R. & Weiss, J. C. Home phototherapy: use and attitudes among community pediatricians. Pediatrics 91, 97–100 (1993).
Rogerson, A. G., Grossman, E. R. & Gruber, H. S. 14 Years of experience with home phototherapy. CLIN PEDIATR 25, 296–299 (1986).
Saeid, M. E., Dehgan, K. & Fakoor, Z. The effect of home phototherapy in jaundice and bilirubin levels of neonates in Urmia City. J. Chem. Health Risks 13, 241–247 (2023).
Thakkar, D., Verma, A. & Malgorzata, R. Phototherapy at home for the treatment of neonatal jaundice: an innovative, patient centered pilot project. Arch. Dis. Child Fetal Neonatal Ed. 15, 104 (2019).
Zanardo, V. et al. Pilot study of home phototherapy for neonatal jaundice monitored in maternity ward during the enforced Italy-wide COVID-19 national lockdown. Eur. J. Pediatr. 181, 3523–3529 (2022).
Jahan, F. et al. Evaluation of community health worker’s performance at home-based newborn assessment supported by mHealth in rural Bangladesh. BMC Pediatr. 22, 218 (2022).
Anderson, C. M., Kandasamy, Y. & Kilcullen, M. Neonatal healthcare providers’ perceptions of the feasibility of home phototherapy in neonatal jaundice. J. Neonat. Nurs. 29, 568–574 (2023).
Pettersson, M., Eriksson, M. & Blomberg, K. Parental experiences of home phototherapy for neonatal hyperbilirubinemia. J. Child Heal Care https://doi.org/10.1177/13674935221082404 (2022).
Acknowledgements
The authors thank Elise Krabbendam (University Library, Erasmus MC Rotterdam) for help with the search strategy. This work was supported by grant 05430052110003 from the Netherlands Organization of Health Research and Development (ZonMw; PI: J.V.B.). The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
Drs. Spaan and Drs. Westenberg conceptualized and designed the study, drafted the initial manuscript, and had full access to all of data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Dr Been. conceptualized and designed the study, coordinated and supervised data collection, and critically reviewed and revised the manuscript for important intellectual content. Furthermore, Dr Been is responsible for the obtained funding. Dr. Hulzebos and Dr. Ista conceptualized and designed the study, coordinated and supervised data collection, and critically reviewed and revised the manuscript for important intellectual content. Dr. Willemsen carried out the initial analyses and critically reviewed and revised the manuscript. Dr. van der Geest and Prof Reiss critically reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Spaan, J., Westenberg, L.E.H., Ista, E. et al. Home phototherapy for neonatal hyperbilirubinemia: a mixed methods systematic review and meta-analysis. Pediatr Res (2025). https://doi.org/10.1038/s41390-025-04313-5
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41390-025-04313-5
This article is cited by
-
Design and Photometric Optimization of a Low-Cost Phototherapy Bed for Neonatal Jaundice
Annals of Biomedical Engineering (2026)
-
Neonatal home phototherapy: need for standardized curriculum
Pediatric Research (2025)
-
Opinions on the cost-effectiveness of home phototherapy
Pediatric Research (2025)
