
Abstract
Background
This study examined parental stress indicators during outpatient pediatric surgery and whether intraoperative text messaging could alleviate stress.
Methods
This randomized trial assigned parents of children aged 6 months to 6 years undergoing minor outpatient surgery to an intervention group, receiving standardized intraoperative text messages, or a control group without messages. Both groups received a postoperative phone call. Stress was assessed using salivary cortisol, heart rate, heart rate variability, and subjective ratings at multiple perioperative time points.
Results
Fifty-one families participated, predominantly mothers (71%). Cortisol and heart rate variability peaked preoperatively, while heart rate and subjective stress were elevated pre- and intraoperatively regardless of messaging. Fathers had lower cortisol at the end of surgery, heart rate pre- and postoperative and subjective stress at pre-treatment consultation compared to mothers, who exhibited lower heart rate variability the evening before surgery. Messaging reduced postoperative cortisol and intraoperative subjective stress among fathers but increased subjective stress at surgery onset within mothers and had no significant effect on stress indicators across the full cohort.
Conclusion
Intraoperative text messaging reduced stress in fathers but not in mothers or the full cohort. The preoperative period remained the most stressful. Future research should explore gender-specific strategies to improve perioperative parental support.
Impact
-
This study assessed parental stress during outpatient pediatric surgery and the impact of intraoperative text messaging as a supportive intervention.
-
Text messages reduced stress in fathers but showed minimal benefit and potential adverse effects in mothers, with increased subjective stress at surgery onset; no overall stress reduction was observed in the full cohort. The preoperative phase was identified as the most stressful for parents.
-
These findings inform pediatric surgical teams that text-based interventions may support fathers’ perioperative coping and postoperative compliance but may be ineffective or counterproductive for mothers, highlighting the need in future research for gender-sensitive stress-reduction strategies.
Similar content being viewed by others
Introduction
Pediatric surgical procedures are not only challenging for the child but also impose significant emotional and physical stress on accompanying parents. The physical stress experienced by parents can be measured using salivary cortisol levels, heart rate (HR), and heart rate variability (HRV), which reflect the activation of the hypothalamic-pituitary-adrenal (HPA) axis and the autonomic nervous system, respectively.1,2 Subjective stress is often characterized by feelings of nervousness, anxiety, and concern during their child’s surgery.3 Factors such as inadequate preparation, uncertainty about postoperative management, and concerns about complications amplify this stress.4
Efforts to reduce parental stress have included various interventions, such as written materials, preoperative programs, videos, and web-based tools, all of which have demonstrated some success in reducing anxiety.4,5,6,7 More recently, text messaging (TM) has emerged as a promising strategy to enhance communication and alleviate parental anxiety in the perioperative setting. A non-randomized study of periodic intraoperative TM during complex spinal surgeries in adolescents reported reduced anxiety among parents, particularly as they received updates during surgery.8 However, the impact of TM on parental stress, especially during shorter outpatient pediatric surgeries, remains unexplored.
Existing research has primarily focused on the pre- and postoperative periods, leaving a gap in understanding the parental stress response during the intraoperative phase. Furthermore, studies have rarely assessed physical stress markers, such as cortisol and HRV, alongside subjective stress measures. To address these gaps, this study investigates the effects of standardized intraoperative TM on parental physical and mental stress during outpatient pediatric surgery, utilizing a randomized controlled trial design.
This approach aims to provide a comprehensive evaluation of the intervention’s effectiveness and explore its potential for reducing parental burden during this critical period. The primary objectives are to assess the impact of intraoperative TM on parental physiological stress markers, including salivary cortisol, HR, and HRV, as well as on parental subjective stress levels. Additionally, the study seeks to explore potential gender differences in stress responses in order to gain a deeper understanding of gender-specific variations in parental anxiety and to examine the progression of parental physiological and subjective stress parameters throughout the perioperative period as secondary objectives.
Methods
Study design and subjects
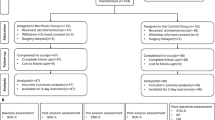
The study was conducted at our tertiary pediatric surgery center and approved by the Ethics Committee of the University of Leipzig (reference number 482/17-ek) in February 2018. It was registered in the German Clinical Trials Register (ID: DRKS00037953). Reporting followed the CONSORT checklist (Supplementary Table S5), and the study flow is illustrated in the CONSORT diagram (Supplementary Fig. S5). The full trial protocol, statistical analysis plan, and additional supplementary materials are available from the corresponding author upon request.
Parents of healthy children aged six months to six years that were scheduled for elective outpatient pediatric surgical interventions, were invited to participate in the study. Parents were recruited on the day their child was examined preoperatively in our outpatient department, which generally took place two days before surgery. The decision on which parent would accompany the child on the day of surgery and therefore would participate in the study, was made by the parents themselves. Surgical informed consent was completed by one of three senior surgeons as well as an anesthesiologist and written informed consent for study participation was always conducted by the study assistant (R.L.).
Eligible interventions were minor procedures such as excisions of dermal lesions or epi-/dermoid cysts, orchidopexy, inguinal herniorrhaphy, umbilical hernia repair, and circumcision. Children were excluded if they had already undergone any previous surgery or general anesthesia, had relevant diseases, or intraoperative complications. Parents were ineligible if suffering from affected cortisol levels due to renal failure, cirrhosis, obesity, psychiatric disorders, or use of exogenous synthetic corticosteroids, or were pregnant.
On the day of surgery, families arrived at the hospital two to three hours before the procedure and were randomized using simple randomization in one of two study groups: Parents of group one (intervention group) received three intraoperative TM. Just before surgery started, they received a mobile phone that was used exclusively for this study to ensure that messages were not sent to strangers. Prior to the beginning of the surgery a TM was sent to ensure that the mobile phone was working properly. Standardized intraoperative TM were sent at the beginning, halfway, and at the end of the surgery by RL, timed by the operating surgeon (Table 1). Parents of group two (control group) did neither get a mobile phone nor any intraoperative TM. Both groups received a phone call at the end of the surgery and were subsequently seen in the recovery room by their surgeon. The surgical and anesthetic protocols were the same for all participating families.
The sample size was determined based on previously published studies. Kwan et al. included 96 accompanying parents in their study and calculated a power of 0.95.8 To detect smaller effects between groups in the present study, we assumed a moderate effect size of 0.55. Based on an alpha level of 0.05, this resulted in a target sample size of n = 48 per group. To ensure robustness, the target sample size was rounded up to n = 50 per group, leading to a total of n = 100 study participants.
Study protocol and sample recruitment
The study protocol is summarized in Fig. 1. Salivary cortisol and subjective stress levels were assessed as such: (T0) two days before surgery at the outpatient department after informed consent to the study had been given; (T2) arrival to the hospital in the morning of surgery; (T3) start of surgery (equivalent to TM 1); (T4) halfway during surgery (TM 2); (T5) immediately after reception of the phone call by the surgeon, that the operation has been finished successfully; and (T6) one hour after reunion with the child at the recovery ward. Parents’ long-term electrocardiogram (ECG) was started the evening before surgery (T1). HR and HRV were analyzed between (T1) and (T6).

Parameters were measured at ‘X’ (T0–T6). TM text message, RM randomization, HR heart rate, HRV heart rate variability, Stress subjective stress level, ECG electrocardiogram.
Cortisol
Salivary cortisol was obtained using the Salivette™ Cortisol tube from Sarstedt (Nuembrecht, Germany). All parents were instructed by the same staff member (RL) how to utilize the Salivette™ correctly and collected the samples under supervision. As all surgeries were scheduled in the morning, samples were harvested at similar time periods. They were stored at 6 °C until surgery was completed; samples were then retained at –80 °C for further analysis at the University of Leipzig Medical Center’s central laboratory by liquid chromatography tandem mass spectrometry.
Heart rate and heart rate variability
A long-term ECG device (CardioMem™ CM 3000, Getemed, Teltow, Germany) was explained and handed out together with a written manual to the parents during recruitment. They were asked to start continuous recording at home the evening before surgery and proceed it for 24 h. For analysis, five minute intervals were defined at each time point T1 to T6 (Fig. 1) and HR as well as time and frequency dependent HRV were assessed using the software CardioDay™ (Getemed, Teltow, Germany; Supplement Table S2).9 Sex dependent normal values are summarized in Supplement Table S1.
Subjective stress assessment
Parents were asked to rate their subjective stress levels on a numeric rating scale (NRS) from zero (“no stress”) to ten (“highest imaginable stress”) to objectify their actual burden/stress at T0 and T2–T6. Subjective stress assessment by NRS had been shown to correlate well with the detailed State-Trait-Anxiety Inventory score that had been validated in preoperative children (correlation r = 0.42–0.64)10 and post-partum females (correlation r = 0.78–0.81).11
Statistical analysis
Data were analyzed using SPSS version 29 (IBM, Armonk, United States of America). Nominal variables are expressed as absolute numbers and percentages. Dichotomous data were compared using Fisher’s exact test or chi-square test. Continuous data are presented as mean ± standard deviation. Normal distribution was graphically confirmed by histograms. Continuous data between groups for each time point were analyzed using Student’s t test or Mann–Whitney U-test, respectively. Logarithmic transformation was applied to achieve normal distribution and to minimize variance and outliers for salivary cortisol levels and HRV. An analysis of variance (ANOVA) with repeated measures was used to evaluate changes over time for the overall cohort. An ANOVA with repeated measures was conducted to assess time-dependent differences between groups. When a significant main effect was observed, a post-hoc Welch’s t test was employed to examine intergroup differences at each time point. The level of significance for two-tailed testing was set at p < 0.05. As this study followed an exploratory design, adjustments for multiple testing were not undertaken.
Results
Study population
Sixty-two families, consisting of 44 boys and 18 girls accompanied by 45 mothers and 17 fathers, were recruited to participate in the study between May 2018 and February 2020. Of those, 11 families were excluded during the study period due to secondary withdrawal of consent (n = 7) or transition from outpatient to inpatient setting (n = 4). Consequently, 51 families were included in the final analysis, with 25 assigned to the intervention group and 26 to the control group.
The accompanying parent was predominantly female (71%), well educated (37%), and native Germans (88%), with a mean age of 33.5 years and a standard deviation of 6.2 years. Demographic characteristics of the parents showed only negligibly differences between study groups (Table 2). The participating children, with a mean age of 28.1 months and a standard deviation of 20.0 months, were primarily male (71%). No substantial differences in demographic characteristics, surgery duration (M = 41.4 min, SD = 23.1 min), or separation duration from parents (M = 94.7 min, SD = 33.3 min) were observed between groups (Table 3).
Impact of TM on physical and mental stress of parents
In the overall cohort, physical (salivary cortisol, HR, and HRV) and subjective psychological stress levels did not significantly differ between the intervention and control groups at any time point (T0-T6; Supplementary Table S3). An ANOVA with repeated measures also showed no significant changes over time and groups.
As a result, data were reanalyzed to assess changes in measured stress parameters over time across the entire cohort, irrespective of group assignment. Additionally, differences between mothers and fathers were examined within the overall cohort, regardless of group classification (Supplementary Table S4), as well as separately within mothers and fathers to compare intervention and control group.
Physical stress
Salivary cortisol
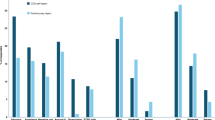
Parental salivary cortisol peaked significantly preoperatively (T2), upon families’ arrival at the hospital, and declined steadily until one hour after reuniting with the child (T6; Fig. 2). This overall trend was comparable in mothers and fathers. However, fathers exhibited a steeper decline of salivary cortisol from the preoperative peak (T2) until the end of surgery (T5) as compared to mothers (Fig. 2). Parents in the intervention group showed slightly lower salivary cortisol levels at T2–T6 (Fig. 3). Fathers in the intervention group experienced a decrease in salivary cortisol levels both intraoperatively (T3–T5) and a significant drop postoperatively (T6) compared to those in the control group (Fig. 3).

a Salivary cortisol levels in parents showed a significant peak preoperatively upon the families’ arrival at the hospital (T2, p < 0.001), followed by a continuous decline until the postoperative time point (T6). Both mothers and fathers demonstrated this overall trend over time. However, fathers exhibited a greater decrease in salivary cortisol levels after the peak at T2, with a significant difference observed at T5 (p = 0.049; °) compared to mothers. b Parental HR were significantly elevated on the day of surgery (T2-T5; p < 0.001, T6 p = 0.031, peaking at the beginning of surgery (T3) compared to the baseline values measured the evening prior (T1). Fathers exhibited a smaller increase in heart rate on the day of surgery (T2–T6), with significant differences compared to mothers’ HR preoperatively (T2, p = 0.009; *) and postoperatively (T6, p = 0.026; #).

a No significant differences in salivary cortisol levels were found between the intervention and control group. Mothers also showed no significant differences between groups. However, fathers in the intervention group had insignificantly lower salivary cortisol levels intraoperatively (T3–T5) and significantly lower cortisol levels postoperatively (T6, p = 0.032; *) compared to those in the control group. b HR showed no significant differences between the two groups for the overall cohort, as well as between groups for mothers or fathers.
Heart rate
Parental HR was significantly higher at the day of surgery (T2–T6) as compared to baseline levels recorded the evening before (T1), with a peak at the start of surgery (T3; Fig. 2). Although fathers’ HR was significantly lower than mothers’ HR at the day of surgery pre- (T2) and postoperatively (T6), particularly at T2, with a mean HR difference exceeding 10 bpm (Fig. 2). Additionally, fathers exhibited a smaller increase in HR perioperatively compared to baseline the evening before (T1; Fig. 2). There were no significant differences in HR between the intervention and the control groups for either mothers or fathers (Fig. 3).
Heart rate variability
Frequency-based (LF nu, HF nu, LF/HF ratio; Supplementary Table S2) and time-based (SDNN, RMSSD, pNN50; Supplementary Table S2) HRV parameters suggested sympathetic activation and parasympathetic inhibition on the day of surgery, regardless of parents’ sex and intervention (Supplementary Figs. S1–S4). LF nu and LF/HF-ratio peaked significantly preoperatively (T2) relative to baseline (T1) and then declined significantly to a steady state from T3 to T6. In contrast, HF nu was significantly lowest preoperatively (T2) compared to baseline (T1) and increased significantly, reaching a steady state from T3 to T6 (Supplementary Fig. S2). RMSSD (T2, T5) and pNN50 (T3) decreased significantly pre- or intraoperatively compared to baseline (T1, Supplementary Fig. S1). At baseline (T1), mothers had significantly lower LF nu and LF/HF-ratio and significantly higher HF nu compared to fathers (Supplementary Fig. S2). Fathers tended to have slightly lower pNN50 values at the beginning of surgery (T3) and lower RMSSD intraoperatively (T3–T5) than mothers (Supplementary Fig. S1).
The LF/HF-ratio values for fathers in the intervention group were marginally higher intra- and postoperatively (T3–T6) than those for fathers in the control group (Supplementary Fig. S4). Fathers in the intervention group exhibited lower pNN50 values throughout the day of surgery and lower RMSSD preoperatively and at the beginning of surgery (T2–T3) compared to fathers in the control group. In contrast, mothers in the intervention group showed slightly higher RMSSD values intra- and postoperative (T3–T6) compared to mothers in the control group (Supplementary Fig. S3). However, these differences between the intervention and control groups, within mothers or fathers, were not statistically significant.
Subjective stress
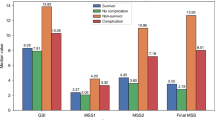
Parental mental stress levels increased perioperatively (T2-T5), with significant increases at T2–T4, peaking at the beginning of surgery (T3) compared to recruitment (T0) and postoperatively (T6, Fig. 4). Fathers had a significantly lower subjective stress level than mothers at T0 and showed a tendency toward lower subjective stress pre- and intraoperatively, yet without reaching statistical significance (Fig. 4). The intervention did not alter subjective stress levels significantly (Fig. 5). However, mothers in the intervention group had significantly higher subjective stress compared to those in the control group at the start of surgery (T3, Fig. 5). In contrast, fathers in the intervention group reported significantly lower subjective stress at the end of surgery (T5) compared to fathers in the control group.

Parental subjective stress levels increased significantly during the perioperative period (T2-T5), reaching a peak at the start of surgery (T3) compared to the recruitment (T0, p < 0.005) and the postoperative phase (T6, p < 0.001). Fathers had significantly lower subjective stress levels at recruitment than mothers (T0, p = 0.019; *) and tended to report lower subjective stress levels pre- and intraoperatively, although this difference did not reach statistical significance.

In the overall cohort, parents showed no significant differences between the two groups at any time point. However, mothers in the intervention group exhibited slightly higher subjective stress levels intraoperatively, particularly at the start of the surgery (T3, p = 0.016; *). In contrast, fathers in the intervention group reported lower intraoperative subjective stress levels (T3–T5) than those in the control group, with a significant difference at the end of the surgery (T5, p = 0.006;#).
Discussion
This randomized controlled trial evaluated the physical and mental stress levels of parents accompanying their children for elective outpatient pediatric surgery and examined the effectiveness of regular intraoperative text messages as a simple, cost-effective method for providing real-time updates to parents in the intervention group.
Preoperative stress responses: cortisol peaks and sympathetic activation
Parental salivary cortisol levels peaked upon arriving at the hospital on the day of surgery (T2), typically in the morning, before gradually declining (mean sample times: T2 8:38 a.m., T3 10:11 a.m., T4 10:37 a.m., T5 10:59 a.m. and T6 12:06 p.m.). This indicates that the preoperative period, particularly the time leading up to the separation from their child, is the most stressful for parents. However, this cortisol peak might also partially reflect the natural circadian rhythm, which reaches its maximum after awakening and decreases throughout the day.2 Supporting this, we also observed a preoperative (T2) increase in frequency-based HRV parameters (LF nu, HF nu, and LF/HF-ratio), indicative of sympathetic activation. These findings align with previous studies, such as Arai et al., who noted elevated LF/HF-ratios in mothers after arousal on the day of surgery.12 Similarly, Angelhoff et al. found that parents staying overnight in the hospital exhibited reduced morning cortisol levels the following day, likely due to stress experienced during admission, coupled with feelings of powerlessness and uncertainty.1 These observations highlight the strong connection between the HPA axis and emotional states. The stress parents experience may stem from managing their own emotions, responding to their child’s reactions, and navigating the unfamiliar preoperative environment—all contributing to this heightened physical stress.
Parental mental stress: risk factors and the impact of perioperative anxiety
Parents reported heightened mental stress levels both preoperatively (T2) and intraoperatively (T3–T5), with the peak occurring at the start of surgery (T3). This aligns with previous studies documenting significant increases in preoperative anxiety among parents.13 Pediatric surgical procedures are inherently stressful for both children and their parents. Key risk factors for heightened parental anxiety include younger children, first-time surgeries, more severe procedures, younger parental age, maternal status, socioeconomic challenges, higher trait anxiety, and language barriers.14,15,16 Additionally, preoperative fasting requirements for the child can exacerbate parental distress.3
The elevated mental stress levels observed in this cohort may be attributed to uncertainties about surgical outcomes, the expected duration of the procedure, feelings of powerlessness, and the transfer of responsibility for their child to medical professionals. These concerns are especially pronounced during the perioperative waiting period and may explain the reduction in physical stress without a corresponding decrease in subjective stress levels. Although the intraoperative TM in this study aimed to address concerns about surgery duration and complications, they were insufficient to significantly alleviate parental mental stress.
Importantly, higher parental anxiety has been linked to lower compliance with postoperative care instructions.14 This is critical in the outpatient pediatric surgery setting, where parents must manage postoperative pain and potential complications at home. Enhancing parental confidence and well-being during the perioperative period is, therefore, essential for improving outcomes for both children and their parents.
Gender differences in stress responses and coping strategies
Fathers exhibited significantly lower HR responses upon arrival at the hospital (T2) and postoperatively (T6), as well as lower salivary cortisol levels at the end of surgery (T5) and reduced mental stress at recruitment (T0) compared to mothers. Conversely, fathers demonstrated higher frequency-based HRV values (LF nu and LF/HF-ratio) and lower HF nu at baseline (T1), reflecting greater sympathetic activation and lower parasympathetic tone. These findings align with previous research showing that men generally have higher HRV parameters, while women exhibit greater vagal modulation.17,18,19 No other significant differences in HR or HRV between fathers and mothers were observed.
While cortisol levels did not differ between fathers and mothers at baseline (T0) or during the preoperative peak (T2), fathers showed a steeper decrease from peak cortisol levels (T2) to the end of surgery (T5). This is consistent with studies suggesting no baseline sex differences in cortisol responses to physical stressors,20,21 though stronger responses to psychosocial stressors have been reported in men.22 Other previous studies have also shown that men exhibit a more pronounced cortisol response to acute psychological stressors, whereas women’s cortisol levels may fluctuate due to influences of the menstrual cycle and the intake of estrogen or oral contraceptives.23,24 Mothers’ higher reported anxiety and concern scores pre- and postoperatively25,26 may reflect greater baseline trait anxiety and their primary caregiving role, which often leads to deeper emotional involvement.16
These findings highlight the importance of considering gender-specific coping strategies when analyzing and addressing parental stress during pediatric surgery.
Effectiveness of intraoperative text messages: insights and contextual factors
In our study, intraoperative TM had no significant effect on physical and mental stress levels in the overall cohort but did show a notable impact on fathers when comparing both groups. Fathers who received TM exhibited significantly lower salivary cortisol levels postoperatively (T6) and reduced mental stress at the end of surgery (T5) compared to those who did not receive TM. Conversely, mothers receiving TM reported higher subjective stress intraoperatively (T3) than mothers without TM.
At first glance, these findings may seem to contradict those of Kwan et al., who reported that intraoperative TM reduced anxiety in both mothers and fathers.8 However, their study involved more frequent TMs (10 vs. 3) during longer surgeries (188.7 vs. 41.4 minutes) and included both parents, who could support one another. Additionally, their cohort focused on adolescents undergoing major idiopathic scoliosis surgery, whereas our study involved younger children (6 months to 6 years) undergoing minor procedures. Parents of younger children tend to experience greater anxiety,14,27 and the severity of surgery further influences stress levels.16 Factors such as the presence of siblings, prior surgical experiences, and family dynamics may also contribute to individual stress responses.
These findings suggest that intraoperative TM may be more effective in reducing parental stress during major surgeries, where heightened anticipation and anxiety related to surgical complexity play a greater role than general parental worry.
Limitations
An interim analysis conducted after the inclusion of 50 participants indicated that reaching the target sample size of 100 would not yield a significantly greater effect on the results. Consequently, the recruitment phase was terminated. Detecting smaller effects would likely require a substantially larger sample size.
This study was exploratory and included a small sample size, limiting generalizability and precluding statistical adjustments for multiple comparisons. Fathers were underrepresented (29%), which may have inflated the observed gender-specific effects, though this reflects the common tendency for mothers to accompany children to the hospital.3
Salivary cortisol, used to measure stress, is a non-invasive and well-established method, but results are influenced by the natural circadian rhythm, which peaks in the morning.2 HRV was assessed over a 24-hour period without controlled rest or standardized stress conditions, which could have provided more precise insights.
The intervention (TM) was initiated after parents arrived at the hospital, missing the preoperative period, which showed the highest stress levels. Earlier interventions may have been more effective in reducing parental stress. These limitations highlight areas for refinement in future studies.
Conclusion
This study highlights the significant physical and mental stress experienced by parents during outpatient pediatric surgery, particularly in the preoperative and intraoperative periods. While intraoperative TM showed no overall impact on the cohort, they effectively reduced stress in fathers, demonstrating the potential for targeted interventions. Nevertheless, considering the lower proportion of fathers accompanying their children and the partially elevated subjective stress levels reported by mothers receiving intraoperative TM, it is plausible that such interventions may induce adverse stress responses. The limited beneficial effect observed among mothers underscores the necessity for more comprehensive, gender-sensitive approaches to mitigating parental stress during pediatric surgical procedures. The preoperative period, identified as the most stressful, presents an opportunity for earlier interventions to better support parents and improve outcomes for both families and patients. Future research should explore tailored, multidimensional approaches to parental stress reduction, particularly in diverse and larger populations.
Data availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
References
Angelhoff, C., Edéll-Gustafsson, U. & Mörelius, E. The cortisol response in parents staying with a sick child at hospital. Nurs. Open 6, 620–625 (2019).
Blair, J., Adaway, J., Keevil, B. & Ross, R. Salivary cortisol and cortisone in the clinical setting. Curr. Opin. Endocrinol. Diab, Obes. 24, 161–168 (2017).
Velhote, A. B., Bohomol, E. & Velhote, M. C. P. Caregivers’ reactions to preoperative procedures in outpatient pediatric surgery. Einstein 14, 403–407 (2016).
Hug, M., Tönz, M. & Kaiser, G. Parental stress in paediatric day-case surgery. Pediatr. Surg. Int. 21, 94–99 (2005).
Fortier, M. A. et al. Web-based tailored intervention for preparation of parents and children for outpatient surgery (WebTIPS): Formative evaluation and randomized controlled trial. Anesth. Analg. 120, 915–922 (2015).
Jenkins, B. N. et al. Changing healthcare provider and parent behaviors in the pediatric post-anesthesia-care-unit to reduce child pain: Nurse and parent training in postoperative stress. Pediatr. Anaesth. 29, 730–737 (2019).
Santapuram, P., Stone, A. L., Walden, R. L. & Alexander, L. Interventions for parental anxiety in preparation for pediatric surgery: A narrative review. Children 8, 1069 (2021).
Kwan, M. K., Chiu, C. K., Gan, C. C. & Chan, C. Y. W. Can Intraoperative text messages reduce parental anxiety of children undergoing posterior spinal fusion surgery for adolescent idiopathic scoliosis?. Spine 41, E225–E230 (2016).
Malik, M. et al. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 17, 354–381 (1996).
Crandall, M., Lammers, C., Senders, C., Savedra, M. & Braun, J. V. Initial validation of a numeric zero to ten scale to measure children’s state anxiety. Anesth. Analg. 105, 1250–3, table of contents (2007).
Prokopowicz, A., Stanczykiewicz, B. & Uchmanowicz, I. Validation of the Numerical Anxiety Rating Scale in postpartum females: a prospective observational study. Ginekologia Pol. 93, 686–694 (2022).
Arai, Y.-C. P. et al. Maternal heart rate variability just before surgery significantly correlated with emergence behavior of children undergoing general anesthesia. Pediatr. Anaesth. 18, 167–171 (2008).
Fortier, M. A. & Kain, Z. N. Treating perioperative anxiety and pain in children: a tailored and innovative approach. Pediatr. Anaesth. 25, 27–35 (2015).
Chahal, N. et al. Association between parental anxiety and compliance with preoperative requirements for pediatric outpatient surgery. J. Pediatr. Health Care 23, 372–377 (2009).
Charana, A. et al. Preoperative anxiety in greek children and their parents when presenting for routine surgery. Anesthesiol. Res. Pract. 2018, 5135203 (2018).
Scrimin, S., Haynes, M., Altoè, G., Bornstein, M. H. & Axia, G. Anxiety and stress in mothers and fathers in the 24 h after their child’s surgery. Child. Care Health Dev. 35, 227–233 (2009).
Agelink, M. W. et al. Standardized tests of heart rate variability: normal ranges obtained from 309 healthy humans, and effects of age, gender, and heart rate. Clin. Autonomic Res. 11, 99–108 (2001).
Geovanini, G. R. et al. Age and sex differences in heart rate variability and vagal specific patterns - Baependi Heart Study. Glob. heart 15, 71 (2020).
Nunan, D., Sandercock, G. R. H. & Brodie, D. A. A quantitative systematic review of normal values for short-term heart rate variability in healthy adults. Pacing Clin. Electrophysiol. 33, 1407–1417 (2010).
Kudielka, B. M., Hellhammer, D. H. & Wüst, S. Why do we respond so differently? Reviewing determinants of human salivary cortisol responses to challenge. Psychoneuroendocrinology 34, 2–18 (2009).
Nicolson, N., Storms, C., Ponds, R. & Sulon, J. Salivary cortisol levels and stress reactivity in human aging. J Gerontol A Biol Sci Med Sci. 52, M68–M75 (1997).
Kirschbaum, C., Wüst, S. & Hellhammer, D. Consistent sex differences in cortisol responses to psychological stress. Psychosom. Med. 54, 648–657 (1992).
Kudielka, B. M. & Kirschbaum, C. Sex differences in HPA axis responses to stress: a review. Biol. Psychol. 69, 113–132 (2005).
Hellhammer, D. H., Wüst, S. & Kudielka, B. M. Salivary cortisol as a biomarker in stress research. Psychoneuroendocrinology 34, 163–171 (2009).
Ayenew, N. T., Endalew, N. S., Agegnehu, A. F. & Bizuneh, Y. B. Prevalence and factors associated with preoperative parental anxiety among parents of children undergoing anesthesia and surgery: A cross-sectional study. Int. J. Surg. Open 24, 18–26 (2020).
Pomicino, L., Maccacari, E. & Buchini, S. Levels of anxiety in parents in the 24 h before and after their child’s surgery: A descriptive study. J. Clin. Nurs. 27, 278–287 (2018).
Hoetzenecker, W. et al. Parental anxiety and concern for children undergoing dermatological surgery. J. Dermatol. Treat. 25, 367–370 (2014).
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
Substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data: R.L., S.M., A.S., J.T., C.H., U.L., R.W., J.T., M.M., R.P., M.L., J.-H.G. Drafting the article or revising it critically for important intellectual content: R.L., S.M., M.M., J.-H.G., A.S., J.T. Final approval of the version to be published: R.L., J.-H.G.
Corresponding author
Ethics declarations
Competing interests
The authors have no conflicts of interest to declare. All co-authors have seen and agree with the contents of the manuscript and there is no financial interest to report. We certify that the submission is original work and is not under review at any other publication.
Consent statement
Patient/Participant consent was conducted by using written informed consent for study participation, surgical and anesthesiologic procedures.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Linke, R., Mayer, S., Suttkus, A. et al. Intraoperative text messaging to reduce parental stress during outpatient pediatric surgery: a randomized trial. Pediatr Res (2026). https://doi.org/10.1038/s41390-026-04816-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41390-026-04816-9
