
Abstract
Neonatal sepsis-induced cardiovascular dysfunction includes impaired myocardial function (which may be systolic and/or diastolic) and vasoregulatory failure (which may lead to vasodilation or vasoconstriction). The haemodynamic response in neonatal sepsis may therefore be hyperdynamic or hypodynamic, and the underlying pathophysiological mechanisms are heterogenous. The assessment of the neonate with sepsis and cardiovascular dysfunction is critical for targeted pathophysiology-based management. However, this assessment is challenging; it may include clinical features, echocardiography, electrocardiography and heart rate variability monitoring, non-invasive cardiac output monitoring (NICOM), near-infrared spectroscopy (NIRS) and biomarkers. Neonatologist performed echocardiography (NPE), in particular, can aid in the evaluation of the pathophysiological mechanism of cardiovascular dysfunction specific to each patient and further guide individualised management.
Impact: What does this article add to the existing literature?
-
This review provides an integrative overview of current methods for assessing cardiovascular dysfunction in neonatal sepsis, combining clinical evaluation with echocardiographic, electrocardiographic, non-invasive hemodynamic (NICOM, NIRS), and biomarker-based approaches to support early recognition and management.
Similar content being viewed by others


Introduction
A lack of a unified definition for neonatal sepsis leads to difficulties in determining its incidence. It is estimated to occur in 1.3 million neonates throughout the globe annually1, resulting in over 200,000 deaths2. The most common cause of death in sepsis is cardiovascular dysfunction3. However, due to heterogeneity in the definitions of both sepsis and cardiovascular dysfunction, as well as a lack of hemodynamic data in most studies, the true incidence of cardiovascular dysfunction complicating neonatal sepsis is unknown4.
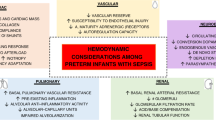
Sepsis may cause a hyperdynamic or hypodynamic cardiovascular response. The hyperdynamic response (‘warm shock’) is characterised by decreased systemic vascular resistance (SVR) and increased heart rate (HR) and cardiac output (CO), resulting in bounding pulses, hypotension and a brisk capillary refill time. The increase in CO is dependent on adequate pre-load and preserved myocardial function. A hypodynamic response (‘cold shock’) is characterised by decreased CO and increased SVR, clinically detectable as cool, pale peripheries, reduced volume pulses and prolonged capillary refill time. The neonatal CV response to sepsis is less well defined compared to that seen in adults (who typically demonstrate a biphasic response5) or in children (in whom the majority have a hypodynamic response6). From the available literature, neonates, in particular those born preterm, typically present with a hyperdynamic, warm shock phenotype. The vasoregulatory failure is compounded in preterm infants by relative adrenal insufficiency and immaturity of the autonomic nervous system7,8,9,10,11. However, both term and preterm infants can present with either warm or cold shock physiology, and furthermore there is evidence for pathogen-specific haemodynamic responses, with one study demonstrating a significantly higher cardiac output state in neonates with Gram-negative sepsis compared to those with Gram-positive sepsis12. Although a recent systematic review found the most common phenotype in neonates to be hyperdynamic, this is not the experience of many of the authors of this paper. This could be a reflection of the relatively small number of included studies and/or of the challenges in haemodynamic assessment. Pulmonary hypertension has been reported in up to 50% of septic neonates in studies including both term and preterm infants13,14,15. Notably, the incidence of reduced myocardial function in neonates with sepsis is unknown due to a lack of studies on neonatal sepsis with detailed echocardiographic evaluations. Considering the varied pathophysiological mechanisms at play, a rigorous assessment is vital in order to deliver targeted therapy, addressing each patient’s unique underlying pathophysiology. A full discussion of the underlying pathophysiological mechanisms is found in part one of this series describing neonatal sepsis and cardiovascular dysfunction4. Cardiopulmonary interactions in neonatal sepsis are summarised in Fig. 1.

Both sepsis and interventions (fluid boluses, inotropes, vasopressors, invasive mechanical ventilation) can have a profound influence on hemodynamics. Sepsis increases capillary leak and third spacing along with dilation of venous capacitance vessels resulting in pooling. Arteriolar dilation leads to decreased systemic vascular resistance (SVR). Poor myocardial function combined with low SVR leads to hypotension and hypoperfusion. Invasive mechanical ventilation increases intrathoracic pressure and decreases systemic venous return. However, mechanical ventilation has a variable effect on pulmonary vascular resistance (PVR). If there is parenchymal lung disease or atelectasis and ventilation increases lung volume to functional residual capacity (FRC), PVR decreases. However, if lung inflation exceeds FRC, PVR increases and can reduce left ventricular preload. Due to reduced left ventricular transmural pressure and due to enhancement of intrathoracic-to-extrathoracic pressure gradient, systemic blood flow may be enhanced by mechanical ventilation. The net hemodynamic effect is a result of the complex interplay of various factors. Copyright Satyan Lakshminrusimha, with permission.
The assessment and diagnosis of cardiovascular dysfunction in neonatal sepsis can be difficult due to the lack of reliability of subjective clinical signs. This may lead to late recognition of a hypoperfused state. The assessment is greatly improved with the incorporation of neonatologist performed echocardiography (NPE), which aids in the understanding of the specific pathophysiological mechanism of cardiovascular dysfunction in an individual patient16. In this way, therapeutic interventions can be targeted and a patient-specific approach adopted. There is a dearth of studies in the literature which have evaluated echocardiography in neonatal sepsis, however findings to date have demonstrated its utility and ability to change management17,18,19,20. NPE is likely most useful in cases of severe sepsis with evidence of organ dysfunction. Advanced imaging techniques, including tissue Doppler imaging and speckle tracking, may be more sensitive than traditional techniques, such as fractional shortening and ejection fraction, for detecting myocardial dysfunction in sepsis. However, these advanced techniques are not considered part of a basic haemodynamic assessment and may be limited to research settings.
Electrocardiography and, more recently, heart rate variability monitoring have shown promise in the early identification of sepsis; however, clinical evidence remains limited, and caution is warranted when interpreting these findings. Machine learning algorithms incorporating such parameters may, in future, become of critical importance in the neonatal unit. Near-infrared spectroscopy (NIRS) and non-invasive cardiac output monitoring (NICOM) allow continuous monitoring and are technically easy to perform, however they have yet to enter routine clinical practice. Lactate remains the most important and clinically useful biomarker in neonatal sepsis; it predicts severity and is used to guide resuscitation. The utility of cardiac biomarkers such as troponin and B-type natriuretic peptides (BNP) has been demonstrated in adult and paediatric patients, particularly for prognostication, but requires further study in the neonatal population. They may have a role in identifying patients who would benefit from closer monitoring and NPE.
Emphasis should be placed on the early recognition of cardiovascular dysfunction in sepsis with early initiation of goal-directed treatment. Management approaches for cardiovascular dysfunction, which are discussed further in the third part of this series, including fluid therapy, inotropic therapy, vasopressor or vasodilator therapy, should be individualised and targeted towards the underlying pathophysiological process for each patient.
Methods
A narrative review approach was used to synthesise current evidence on the assessment of cardiovascular function and haemodynamics in the setting of neonatal sepsis. Literature was identified through a structured search of PubMed, Embase and Google Scholar up to April, 2025. The search combined keywords and MeSH terms including “neonatal sepsis,” “myocardial dysfunction,” “haemodynamics,” “echocardiography,” “shock,” “NICOM,” and “NIRS.”
Original research articles, reviews, and relevant experimental studies were included if they focused on neonates or provided mechanistic insights applicable to neonatal physiology. Studies limited to older paediatric or adult populations were excluded unless they contributed important comparative or pathophysiological information. Only English-language publications were considered.
Key findings were extracted and synthesised narratively, with thematic organisation according to each form of assessment.
Assessment of cardiovascular dysfunction in neonatal sepsis
End-organ perfusion is determined by systemic blood flow which is challenging to monitor. Although clinical signs such as HR, blood pressure (BP), urine output and capillary refill time are of critical importance, they have limited ability to accurately discern systemic blood flow and organ perfusion21. In particular, the use of BP as a surrogate marker for systemic blood flow is problematic22, illustrated by the poor correlation between BP and left ventricular output on the first day of life23. According to Poiseuille’s Law, CO is determined by the pressure gradient (arterial blood pressure minus right atrial pressure) divided by SVR24. This means that as long as the SVR is increased, the BP may remain normal or even high, despite a low cardiac output state. In addition, the arbitrary threshold of mean arterial pressure approximating the gestational age lacks scientific validation and is too simplified an approach to a complex issue. For example, birth weight, postnatal age, whether in asleep or awake state and method of measurement all play a role alongside gestational age25. Invasive arterial BP measurement is the gold standard for determining BP in a neonate, however invasive arterial lines carry a risk of morbidity. Multi-parametric monitoring, which collects data via central venous and/or arterial catheters can calculate cardiac output, stroke volume, systemic vascular resistance, stroke volume variation and pulse volume variation have been used in adults with sepsis26, for example to predict fluid responsiveness27, however these devices are less effective in neonates due to small vessel size, physiologically high heart rates and parameter variability. These limitations highlight the importance of integrating non-invasive monitoring techniques with functional echocardiography. The most common non-invasive method used in NICUs is automated BP measurement using oscillometric devices25. In both term and preterm infants, there may be significant differences in BP recordings when comparing invasive and non-invasive measurements28,29. In clinical practice and in research settings, the mean arterial blood pressure (MAP) is the most commonly used component of blood pressure measurement30. However all components of blood pressure should be taken into consideration during a haemodynamic assessment. The systolic component and the pulse pressure (the difference between the systolic and diastolic arterial blood pressure) correlate with left ventricular output and therefore reflect myocardial performance30; a narrow pulse pressure indicative of a lower left ventricular output. Meanwhile, the diastolic component is reflective of vasomotor tone 31.
In more recent years, there has been a paradigm shift to use NPE to assess cardiovascular status, identify the pathophysiology of each individual patient and to target treatment accordingly24. This is especially important when we consider the differences in cardiovascular physiology of neonates which render them particularly sensitive to changes in preload and afterload, and the fact that many NICU interventions may have adverse haemodynamic effects. These include invasive ventilation reducing venous return and RV preload, chronotropic effects of certain cardiovascular drugs (e.g. adrenaline and dobutamine) reducing diastolic filling time and thus left ventricle (LV) preload, and vasodilatory effects of drugs used for sedation and anaesthesia. Recent work has outlined how an integrated evaluation of haemodynamics, combining clinical features (BP, HR, pulse oximetry, haemoglobin), echocardiography and NIRS can be useful in the management of preterm infants with a compromised systemic circulation in whom it reduced the time to clinical recovery32,33. Figure 2 shows components of a hemodynamic assessment.

Pulse oximetry (oxygenation and perfusion assessments), near infrared spectroscopy (NIRS), electrocardiogram, bedside echocardiography, cardiorespiratory monitoring, and noninvasive cardiac output monitoring (NICOM) complement clinical tools such as heart rate, capillary refill, blood pressure, urine output and laboratory investigations such as blood gas and lactate.
Clinical features
Clinical features suggestive of cardiovascular dysfunction include tachycardia, hypotension, prolonged capillary refill time, reduced urine output, and failure to respond to or worsening clinical status with fluid therapy. However, many of these features are present in neonates with sepsis alone and, in general, the clinical assessment of hemodynamic state is subjective and imprecise, regardless of the clinician’s level of experience21. A meta-analysis evaluated prediction models for neonatal sepsis based on different combinations of clinical signs, biomarkers and risk factors and found that all the models lacked diagnostic accuracy34. The most predictive clinical signs for diagnosis of sepsis were lethargy and mottling for all neonates and/or bradycardia and reduced peripheral perfusion for very low birth weight infants.
Echocardiography features
NPE has become the standard of care for haemodynamic assessment in many neonatal units internationally. It is used to non-invasively assess real-time cardiovascular performance and systemic and pulmonary haemodynamics. It is, however, a skill which requires training, necessitates handling of often fragile infants, and currently not available in all institutions.
Serial echocardiography offers additional information regarding the physiology of cardiovascular compromise and its routine use in the neonatal unit leads to changes in management17,18,20, especially in situations of high illness severity, for example, in over 80% of cases of systemic hypoperfusion19. In adult patients with sepsis, the use of echocardiography has been shown to improve 28-day survival35; the impact on outcomes has yet to be proven in the neonatal population. As described in most recent guidelines, NPE provides patient-tailored, physiology-based haemodynamic monitoring16. The interpretation of hemodynamic data is dependent on image quality and hence operator-dependent. Challenges in neonates include the small size of preterm infants, hyperinflated lungs or air trapping which may obstruct the cardiac view, and the potential for clinical decompensation with handling. A baseline functional echocardiogram (Table 1) can include the evaluation of the heart using two-dimensional methods (2D), pulsed wave Doppler (PWD), continuous wave Doppler (CWD) and M-mode techniques. Right and left ventricular outputs (RVO, LVO) as well as SVC flow can be estimated from echocardiography. The description of how to perform these echocardiography techniques is outside the scope of this review, but has been outlined in recent guidelines16. More advanced imaging methods include tissue Doppler imaging (TDI) and speckle tracking (Table 2).
Traditional methods
Cardiac output
The most commonly used measurements for evaluation of central blood flow in neonates are right and left ventricular outputs. Normal RV and LV outputs are 150–300 mL/min/kg. There is a paucity of published literature evaluating these parameters in neonatal sepsis but the evidence to date suggests a hyperdynamic state is often seen with high RVO and LVO and reduced SVR10,11,12,14. There was no difference between term and preterm infants in one small study12. Interestingly, the RVO and LVO were significantly higher in patients with Gram-negative sepsis (mean value of 338 and 378 mL/kg/min respectively) than in patients with Gram-positive sepsis, in whom the values remained within the normal range (mean 225 and 240 mL/kg/min respectively), suggesting diverse host responses to assorted pathogens may lead to different haemodynamic states 12.
Systolic function
Fractional shortening (FS) can be measured by 2D or M-mode; normal neonatal values range from 30 to 45%16,22. However, fractional shortening is highly preload dependent. Furthermore, it does not take into consideration regional wall motion abnormalities and may over-estimate systolic function if, for example, there is preserved motion at the level of the M-mode cursor but impaired apical or basal function. Finally, high right-ventricular pressures secondary to pulmonary hypertension, seen in the early neonatal period or frequently in the setting of sepsis, may impair ventricular septal wall movement and thus reduce FS 36.
Ejection fraction (EF) can be estimated using the M-mode technique, and similar limitations apply as to those seen with fractional shortening. However, EF is more accurately calculated using the Simpson biplane technique, which is a volumetric appraisal of ventricular fibre shortening. Normal neonatal values range from 55 to 70% 16.
Qualitative assessment, i.e., visual estimation or “eye-balling” systolic function, is closely correlated with formal quantitative methods37. However, this requires significant operator experience in order to be accurate and also limits the ability to “trend” a patient’s function.
In paediatric and adult studies, FS and EF are reduced in more than half of septic patients38,39,40,41. However, these measurements have not been shown to correlate with mortality in adult or paediatric studies of sepsis38,39,42,43,44. The limited literature available regarding FS and EF in neonatal populations shows no significant difference between neonates with sepsis compared to control subjects in most studies14,15,45,46,47. One study showed that in septic neonates, LV-FS was significantly higher in the survivors compared to those who died15 and another demonstrated significantly reduced LV-EF in a group with sepsis and cardiovascular dysfunction compared to those with sepsis without cardiovascular dysfunction or controls 48.
Right ventricular dysfunction is reported in 30–60% of adult sepsis patients40,49. FS and EF are not suitable for the assessment of the right ventricle due to the differences in RV geometry compared to the LV. In contrast to the left ventricle, qualitative assessment of the RV is imprecise50,51. Fractional area change (FAC) and tricuspid annular plane systolic excursion (TAPSE) have emerged as reliable techniques for systolic function assessment of the right ventricle. TAPSE has been validated, and normal neonatal reference ranges have been published50,51,52,53 in term and preterm infants52,54. It is a reliable marker of RV longitudinal function, correlating well with RV EF by cardiac MRI51, and is not influenced by heart rate, which is an advantage for preterm infants. There are limited data regarding the role of TAPSE in neonatal sepsis; one paediatric study reported a TAPSE Z score of <−2 (i.e., more than 2 standard deviations below an age- and size-matched population mean measurement) in 60% of patients with sepsis39 and another reported significantly reduced TAPSE in septic neonates compared to controls55. Fractional area change (FAC) is a quantitative measure of RV function which expresses the percentage change in RV area between end-diastole and end-systole. References ranges have been published for both term and pre-term neonates56. The roles of TAPSE and FAC in neonatal sepsis have not yet been evaluated in the literature.
Diastolic function
Conventional echocardiographic measurements of left and right ventricular diastolic function are based on mitral and tricuspid inflow patterns of the E wave (early diastolic filling) and A wave (late diastolic filling) (Fig. 3). However, because the inflow patterns reflect the gradient between the atrium and the ventricle, it is important to note that they are highly preload- and afterload-dependent. Parameters which are used include the peak E wave and the E/A ratio. Both are significantly lower, indicating diastolic dysfunction, in the LV of term and preterm neonates with sepsis compared to non-septic neonates 7,15,46.

Pulsed-wave Doppler measurement showing passive (E wave) and active (A wave) flow in a term neonate from the apical four-chamber view.
Pulmonary hemodynamics
Increased PVR leading to pulmonary hypertension occurs in 25–50% of cases of neonatal sepsis and carries important management implications as well as increasing mortality7,13,57. Pulmonary hemodynamic assessment is therefore critical. This may include transductal blood flow pattern, peak tricuspid regurgitation (TR) velocity, end-diastolic pulmonary regurgitation gradient and LV systolic eccentricity index (Table 3). LV systolic eccentricity index (EI) is a way to objectively measure septal flattening and therefore quantify RV pressure loading. Measurements for EI are done at end-systole in the parasternal short axis view at the level of the mitral valve papillary muscles. The EI is a ratio of the midseptum to posterior wall diameter to the perpendicular diameter, parallel to the ventricular septum (see Fig. 4). A description of these methods is detailed in recent guidelines 16.

Findings on an echocardiogram in a normal infant. The systemic vascular resistance (SVR) is higher than the pulmonary vascular resistance (PVR), and the interventricular septum bows to the right with a spherical left ventricle (LV) and a crescentic right ventricle (RV). The LV eccentricity index (LVEI) is the ratio of the two diameters of the LV and is close to 1.0 under normal circumstances. The shunt across the patent foramen ovale (PFO) and patent ductus arteriosus (PDA) is left-to-right. The tricuspid annular plane systolic excursion (TAPSE) is high, and the pulmonary arterial acceleration time to RV ejection time (PAAT/RVET) is long when the RV function is normal, and afterload is low. B In sepsis, SVR decreases and often falls below PVR, resulting in bidirectional or right-to-left shunt at PFO and PDA, decreased TAPSE and PAAT/RVET ratio and an increase in LVEI. The inset shows changes in Tei index and tissue Doppler imaging (see text for details). Copyright Satyan Lakshminrusimha, used with permission.
Advanced imaging techniques
Traditional echocardiographic indices of cardiac function, including EF and stroke volume, are affected by changes in heart rate, preload and afterload, and therefore reduced indices may not necessarily be indicative of true myocardial dysfunction or conversely, compensatory mechanisms may mean that early myocardial dysfunction is missed. For example, tachycardia and peripheral vasodilation leading to changes in cardiac loading conditions are common in patients with neonatal sepsis, and in this context, conventional echocardiography parameters may not detect early myocardial dysfunction45.
The Tei index or myocardial performance index (MPI) is a Doppler index of combined systolic and diastolic function, calculated as isovolumetric relaxation time plus isovolumetric contraction time divided by ejection time. One neonatal study, which included 30 septic neonates, both preterm and term, demonstrated that non-survivors had a statistically significantly higher Tei index (a higher number correlates with worse global function)46; another neonatal study demonstrated a significantly higher Tei index in the group with sepsis who also had cardiovascular dysfunction compared to those who did not48.
TDI is an echocardiographic technique that provides quantitative information about myocardial wall motion velocity with high temporal and spatial resolution. TDI can be performed using colour-Doppler or pulsed-wave modes. Pulsed-wave TDI (PW-TDI) is used to measure peak myocardial velocities. For example, PW-TDI of systolic myocardial velocity (s’) at the lateral mitral valve annulus is a measure of longitudinal LV systolic function and correlates with LV ejection fraction58. Similarly, PW-TDI s’ at the lateral tricuspid valve annulus is a measure of longitudinal RV systolic function. A recent study demonstrated a third of adult patients with severe sepsis to have RV dysfunction based on PW-TDI s’ and this appeared to carry prognostic impact59.
Regarding diastolic assessment, PW-TDI of the lateral mitral valve annulus demonstrates an e’ wave, which reflects the velocity of early myocardial relaxation as the mitral valve annulus descends rapidly during early diastolic filling, and an a’ wave, which reflects the later velocity of myocardial relaxation during late diastolic filling. Septal e’ and a’ velocities can also be measured and are usually lower than lateral e’ velocities due to intrinsic differences in myocardial fibre orientation60. E/e’ and e’/a’ can also be measured as parameters of diastolic function. The same measurements can be performed at the tricuspid valve annulus. Normal reference range values exist for term and preterm neonates54,61,62,63. In studies evaluating the use of TDI in term infants with LOS, the atrioventricular annular systolic velocities were significantly lower (indicating reduced longitudinal systolic RV and LV function) in the septic group compared to the healthy controls45,47. Of note, conventional echocardiography parameters of CO, FS and atrioventricular inflow velocity patterns showed no significant difference in the septic patients, suggesting that TDI parameters are more sensitive to detect early myocardial damage in neonatal sepsis. In adult sepsis studies, diastolic dysfunction by TDI is common and is associated with higher mortality49,64,65. This has yet to be elucidated in neonatal studies. Limitations of TDI include the influence of ventricular loading on the velocity, the fact Doppler is angle-dependent, and the inability to distinguish between active (myocardial fibre shortening or lengthening) and passive myocardial tissue movements (secondary to tethering to adjacent myocardium).
Myocardial deformation imaging by speckle tracking echocardiography (STE), including strain and strain rate, is increasingly used to assess biventricular function. Strain is a measure of absolute tissue deformation during systole and is expressed as a percentage change from baseline; a negative figure for shortening in longitudinal and circumferential planes and a positive figure for thickening in the radial plane66. Preload increases wall strain, and afterload reduces wall strain67. Strain rate (SR) measures the time course of deformation (velocity of shortening/time), i.e., the rate at which the deformation occurs. It is thought to be less dependent on loading conditions than strain68. Strain has improved sensitivity for early cardiac dysfunction compared to conventional function measurements69,70,71, including in patients with sepsis72 in whom reduced indices of strain correlate with disease severity73,74 and mortality75. One neonatal sepsis study to date demonstrated significantly worse strain values in septic patients versus controls47 and of note, there are published neonatal reference ranges 76.
NPE in clinical practice
Putting this into clinical practice, not all infants with suspected sepsis require an echocardiogram. However, NPE often changes management and can be used to guide fluid and cardiovascular drug use. A basic functional echocardiogram (Table 1) can (and should) be carried out in a matter of minutes by experienced operators. Assessment of ductal patency, shunt direction and pressure gradient should also be included to assess for pulmonary hypertension. It is therefore the opinion of this group that all neonates with suspected sepsis and evidence of end-organ failure and/or hemodynamic instability have a NPE within 12 hours of onset which should include ventricular outputs, biventricular systolic (FS, EF, TAPSE, FAC) and diastolic (E and A waves, E/A) performance and pulmonary hemodynamic assessment (directionality and gradient of PDA shunt, peak TR velocity, end-diastolic pulmonary regurgitation gradient). Figure 4 summarises echocardiographic changes in neonatal sepsis.
Electrocardiogram (ECG) and heart rate variability
There are no ECG changes which are specific for cardiovascular dysfunction in neonatal sepsis although sinus tachycardia is a classic feature. Signs of strain may be seen in cases when there is myocardial involvement, such as T wave inversion (in the inferior and lateral leads) or ST segment changes.
The significance of reduced HR variability and transient decelerations in HR is increasingly recognised77 and therefore, HR monitoring has emerged as a diagnostic tool in sepsis. Although the precise mechanisms are incompletely understood, this is hypothesised to be due to vagal activation via the cholinergic anti-inflammatory pathway in response to infection78,79. Variability monitoring evaluates fluctuations in HR, and many different metrics based on this have emerged80. A randomised control trial (RCT) in very low birth weight infants demonstrated reduced sepsis-associated mortality with HR characteristics monitoring, which identified reduced HR variability and transient decelerations79,81. Subsequent trials have used sophisticated machine learning techniques based on continuous electrocardiogram and monitoring data, to enhance earlier detection of sepsis in preterm infants82,83,84, with one study demonstrating predictive potential as early as 42 h before antibiotics had been started85. However, it must be noted that these studies are limited by biases in how the infants were managed. Future physiology monitoring in NICUs will likely incorporate machine learning algorithms which include patient-specific risk factors with real-time data, including HR variability to alert clinicians to patients at high risk of sepsis. It must be noted that these tools do not predict cardiovascular dysfunction in sepsis but may be useful as an early warning sign to assess for sepsis.
Non-invasive continuous monitoring
Near-infrared spectroscopy (NIRS) offers a non-invasive, objective and continuous alternative to assess cerebral and peripheral oxygenation and oxygen extraction. It is, however, an indirect measurement. Cerebral oxygenation measured by NIRS can be used as a correlate for cerebral perfusion and suggested as a surrogate marker for cardiovascular function, but this is complicated by cerebrovascular reactivity and autoregulation. Cerebral oxygenation may be reduced for a variety of reasons other than perfusion, including changes in cerebral arterial oxygen saturation, arterial partial carbon dioxide pressure, haemoglobin concentration, fractional-inspired oxygen and tissue oxygen diffusivity. Neonatal reference values exist86,87, but the trend is more important than the absolute value, and there is more evidence for its use in term than in preterm infants. NIRS monitoring has been shown to reduce cerebral hypoxic burden in preterm neonates88, to predict cardiac arrest in children with congenital heart disease89, and to identify low cardiac output state in neonates peri-operatively90,91. There is a paucity of data regarding the clinical applicability of NIRS for haemodynamic monitoring of septic infants. One study correlated echocardiography estimates of CO with NIRS monitoring in preterm neonates with sepsis and found that CO was negatively associated with intestinal tissue oxygen extraction but not with renal or cerebral tissue oxygen extraction suggesting that gut perfusion was most at risk92. Another study of preterm infants demonstrated those with infection/inflammation had significantly lower venous oxygen saturation in peripheral muscle tissue compared to the control group93. Preterm infants with sepsis compared to controls were shown to have lower cerebral oxygenation by NIRS, which was associated with reduced neurodevelopmental scores in childhood in one study94 but not another95. A potential model could use NIRS to predict cardiovascular collapse in neonates with sepsis, allowing earlier intervention by physicians, but ultimately we should aim to be diagnosing haemodynamic instability before cerebral perfusion is significantly affected. Multiple hurdles have yet to be overcome in the clinical applicability of NIRS, as have been recently highlighted96. Although identifying autoregulatory failure to the brain should theoretically allow us to target interventions and improve outcomes, this has not been demonstrated. In a large multi-centre RCT of extremely premature infants, treatment guided by NIRS monitoring for the first 72 h of life was not associated with lower mortality or severe brain injury97.
Non-invasive cardiac output monitoring (NICOM) provides continuous estimation of CO via easily applicable surface electrodes which can apply and detect a high-frequency, low-magnitude electrical current across the body. There are two broad categories to consider in electrical biosensing technologies: bioimpedance (BI) and bioreactance (BR). The electrical current is mainly distributed to the blood, and an increase in compartmental blood volume, blood flow velocity, and alignment of red blood cells during systole will cause a reduction in electrical impedance98. These fluctuations in impedance are assumed to be proportional to stroke volume in BI. BR estimates CO by measuring the phase shift of an oscillating current as it traverses the thorax based on the theory that blood flow changes cause variation in impedance, but also in capacitance and inductance99. It is important to note that due to technical and practical elements, BI and BR NICOM techniques are not interchangeable.
The use of NICOM has been validated in adult populations where values correlate with invasive measures of CO100,101,102. In neonatal studies, it has been shown to correlate with echocardiographic estimates of left ventricular CO103,104, but notably, a systematic review highlighted wide limits of agreement with most studies having a percentage error >30%105 and therefore NICOM’s role was thought to be as a trending tool. However, studies assessing this are scarce, and those that have been performed are not encouraging105. Overall, NICOM should be used with caution in the neonatal population as its benefit has not been proven.
Biomarkers
Lactate is an easy to measure indirect marker of tissue hypoperfusion. Higher serum levels are associated with increased mortality and morbidity in neonates106, including in sepsis107. However there have been no published studies which the authors could identify evaluating whether lactate was predictive of cardiovascular dysfunction specifically. The importance of lactate in sepsis is underlined by the fact it is included in the Sepsis-3 definition of septic shock in adults as those requiring a vasopressor to maintain a mean arterial blood pressure of 65 mmHg or greater and serum lactate greater than 2 mmol/L in the absence of hypovolaemia108. Unfortunately, no consensus definition for septic shock has been established in the neonatal population to date. Serum lactate is clearly an important prognostic biomarker in the management of neonatal sepsis and is also used to guide resuscitation as recommended in most recent guidelines109. The value of lactate is underlined in recent work, which determined lactate levels to exhibit the strongest individual significance in predicting mortality amongst a cohort of preterm neonates with late-onset sepsis110. Although a higher lactate level is associated with sepsis, it is not reliably diagnostic due to a low sensitivity111. Elevated levels are not specific for hypoperfusion and may also be raised due excessive adrenaline stimulation (including in the context of an adrenaline infusion), liver or kidney dysfunction107. However, in neonatal sepsis, elevated levels are predictive of mortality and therefore aid in the identification of the infants who may require more intensive monitoring and more aggressive support.
Troponin is a protein complex of the cardiac sarcomere with three distinct sub-units, Troponin T, C and I. In sepsis, troponin may be released secondary to cytokine-induced cardiomyocyte apoptosis or due to inflammation-induced increased cell permeability112. In adults, elevated troponin confers a poorer prognosis and is predictive of mortality in sepsis113,114, while in pediatric sepsis studies, it correlates with decreased LV ejection fraction and peak inotrope requirements 115.
The cardiac troponins are also useful markers of myocardial damage in neonatal cohorts116. Cardiovascular dysfunction occurs frequently as part of multi-organ dysfunction following a perinatal hypoxic-ischaemic event. Troponins T and I are significantly higher in asphyxiated neonates compared to controls, and they predict mortality117,118 and neurodevelopmental outcomes at age one year119. There have been mixed results in the limited studies published to date assessing the relationship between troponin and cardiac dysfunction in neonatal sepsis, with some studies demonstrating a significant association between increased levels of Troponin T and reduced cardiac function45,47,120,121, inotropic support45, or mortality45,121, while others have shown no association122,123. Therefore, in both sepsis and hypoxia, raised troponins reflect myocardial dysfunction and may serve as proxies for severity. There is, however, still no accepted physiological reference range in the neonatal period, and this limits its use 124,125.
BNP is a secretory granule stored in the ventricular myocardium. BNP and its inactive by-product, N-terminal pro-BNP (NTpBNP), are released by the stressed ventricular myocardium in response to either pressure- or volume-loading126. In adult septic patients, raised BNP or NTpBNP confers a significantly increased mortality risk127,128, while in paediatric sepsis cohorts, raised BNP levels are associated with myocardial dysfunction, inotropic requirement and mortality112,129. Increased BNP level is associated with LV systolic dysfunction in septic patients130, although it can also be increased in those with preserved left ventricular ejection fraction131, including in the setting of catecholamine therapy, renal failure, CNS disease as well as pro-inflammatory cytokine up-regulation131,132,133. BNP is therefore less specific than troponin for cardiac dysfunction in sepsis. In one study of neonates with sepsis, those with clinically determined cardiovascular dysfunction had significantly higher NT-Pro-BNP levels on admission to the NICU. Using a cut-off level of 12,291.5 pg/L, NT-Pro-BNP levels on admission acted as an early predictive marker of cardiovascular dysfunction with a sensitivity and specificity of 80% and 79%, respectively48.
Plasma levels of NTpBNP in preterm infants correlate with echocardiographic measurements of LV systolic and diastolic function120,134. However, the extrapolation of adult and pediatric data regarding raised BNP or NTpBNP in the setting of sepsis is complicated in neonates. Firstly, there is a paucity of data of normative values and reference ranges quoted in the literature vary according to gestation at birth, timing of test and the testing kit used135. Secondly, co-morbidities which are commonly seen in sick neonates, such as respiratory distress syndrome and patent ductus arteriosus, are associated with raised NTpBNP levels120,136,137. Finally, due to the stiff non-compliant state of the preterm heart, it is more vulnerable to many issues commonly seen in babies in NICU, including mechanical ventilation, anaemia and hypoxia138. This may explain why raised NTpBNP is more common in premature infants particularly137. Furthermore, NTpBNP may be raised in neonatal pulmonary hypertension139 with or without sepsis.
As both troponin and BNP/NTpBNP tests are easily accessible, cheap, and appear to offer diagnostic and prognostic value, serial testing could be considered in neonatal sepsis, with increased levels prompting more intensive monitoring and/or an echocardiogram. The BNPs are less specific than troponin, and renal dysfunction may affect levels as they are primarily excreted by the kidneys. However, considering these limitations, further exploration for more useful markers of cardiovascular dysfunction in neonatal sepsis is required. Artificial intelligence has great potential to advance biomarker discovery in sepsis due to its ability to analyse high volume complex data and to identify complex multiparametric patient trajectories 140.
Conclusion
Cardiovascular dysfunction in neonatal sepsis is a frequent, harmful complication that significantly contributes to morbidity and mortality. Septic neonates often demonstrate pulmonary hypertension and LV diastolic dysfunction, though they may present with either warm or cold shock physiology. Accurate cardiovascular assessment of these neonates is critical to tailor therapies to an individual’s specific pathophysiology in order to improve outcomes. While observation of subjective clinical signs is imprecise, objective parameters are currently lacking. NPE, increasingly adopted in neonatal units, provides real-time assessment of cardiovascular performance, pulmonary and systemic hemodynamics, and may guide volume therapy and choice of vasoactive agents. Advanced imaging techniques, including TDIs and strain, show promise for early detection of myocardial dysfunction and correlation with mortality, however, they extend beyond the scope of a first-line NPE assessment and may remain primarily research tools. Diastolic dysfunction could be more prognostically significant than systolic dysfunction, but research on NPE in neonatal sepsis is limited, and further studies are needed to validate its diagnostic, therapeutic, and prognostic utility. Specifically, future work should evaluate whether NPE integration improves clinical outcomes.
Although lactate remains the key biomarker in neonatal sepsis, additional studies are needed to clarify the roles of serum troponin and BNP. Alternatively, the future may lie in broader exploration of metabolomic, transcriptomic and proteomic data of septic neonates to identify novel biomarkers with greater prognostic and therapeutic value. Similarly, while NICOM or NIRS has not yet demonstrated clear benefits in neonatal sepsis management, this could evolve with emerging evidence. In summary, based on the available evidence, it is the opinion of this group that all neonates with suspected sepsis and evidence of end-organ dysfunction and/or hemodynamic compromise should have a basic hemodynamic assessment by NPE within 12 h of symptom onset in order to guide targeted therapy. Future research should focus on whether incorporation of NPE improves outcomes.
References
James, S. L. et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 392, 1789–1858 (2018).
Roth, G. A. et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 392, 1736–1788 (2018).
Weiss, S. L. et al. The Epidemiology of hospital death following pediatric severe sepsis: when, why, and how children with sepsis die. Pediatr. Crit. Care Med. 18, 823–830 (2017).
Duignan, S. M. et al. Neonatal sepsis and cardiovascular dysfunction I: mechanisms and pathophysiology. Pediatr Res. https://doi.org/10.1038/s41390-023-02926-2 (2023).
Groeneveld, A. B., Nauta, J. J. & Thijs, L. G. Peripheral vascular resistance in septic shock: its relation to outcome. Intensive Care Med. 14, 141–147 (1988).
Ceneviva, G., Paschall, J. A., Maffei, F. & Carcillo, J. A. Hemodynamic support in fluid-refractory pediatric septic shock. Pediatrics 102, e19 (1998).
Pugnaloni, F. et al. Assessment of hemodynamic dysfunction in septic newborns by functional echocardiography: a systematic review. Pediatr. Res. 95, 1422–1431 (2024).
Cerritelli, F. et al. A review on the vagus nerve and autonomic nervous system during fetal development: searching for critical windows. Front. Neurosci. 15, (2021).
Galland, B. C., Taylor, B. J., Bolton, D. P. G. & Sayers, R. M. Heart rate variability and cardiac reflexes in small for gestational age infants. J. Appl. Physiol. 100, 933–939 (2006).
de Waal, K. & Evans, N. Hemodynamics in Preterm Infants with Late-Onset Sepsis. J. Pediatr. 156, 918–922.e1 (2010).
Saini, S. S., Kumar, P. & Kumar, R. M. Hemodynamic changes in preterm neonates with septic shock: a prospective observational study*. Pediatr. Crit. Care Med. 15, 443–450 (2014).
Deshpande, S., Suryawanshi, P., Chaudhary, N. & Maheshwari, R. Cardiac output in late onset neonatal sepsis. JCDR https://doi.org/10.7860/JCDR/2017/30312.10871 (2017).
Deshpande, S. et al. Pulmonary hypertension in late onset neonatal sepsis using functional echocardiography: a prospective study. J. Ultrasound 25, 233–239 (2022).
Yengkhom, R. et al. Point of care neonatal ultrasound in late-onset neonatal sepsis. J. Neonatol. 35, 59–63 (2021).
Fahmey, S. S., Hodeib, M., Refaat, K. & Mohammed, W. Evaluation of myocardial function in neonatal sepsis using tissue Doppler imaging. J. Matern. Fetal Neonatal Med. 33, 3752–3756 (2020).
McNamara, P. J. et al. Guidelines and recommendations for targeted neonatal echocardiography and cardiac point-of-care ultrasound in the neonatal intensive care unit: an update from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 37, 171–215 (2024).
Moss, S. Evaluation of echocardiography on the neonatal unit. Arch. Dis. Child. Fetal Neonatal Ed. 88, 287F–291F (2003).
Sehgal, A. & McNamara, P. J. Does point-of-care functional echocardiography enhance cardiovascular care in the NICU? J. Perinatol. 28, 729–735 (2008).
Papadhima, I. et al. Targeted neonatal echocardiography (TNE) consult service in a large tertiary perinatal center in Canada. J. Perinatol. 38, 1039–1045 (2018).
Negreiros Figueira, S. et al. Echocardiography performed by the neonatologist: the impact on the clinical management. Pediatr. Res. 94, 724–729 (2023).
de Boode, W.-P. Clinical monitoring of systemic hemodynamics in critically ill newborns. Early Hum. Dev. 86, 137–141 (2010).
El-Khuffash, A. F. & McNamara, P. J. Neonatologist-performed functional echocardiography in the neonatal intensive care unit. Semin. Fetal Neonatal Med. 16, 50–60 (2011).
Kluckow, M. & Evans, N. Relationship between blood pressure and cardiac output in preterm infants requiring mechanical ventilation. J. Pediatr. 129, 506–512 (1996).
de Boode, W. P. Individualized hemodynamic management in newborns. Front. Pediatr. 8, 580470 (2020).
Pejovic, B., Peco-Antic, A. & Marinkovic-Eric, J. Blood pressure in non-critically ill preterm and full-term neonates. Pediatr. Nephrol. 22, 249–257 (2007).
Sangkum, L. et al. Minimally invasive or noninvasive cardiac output measurement: an update. J. Anesth. 30, 461–480 (2016).
Khwannimit, B. & Bhurayanontachai, R. Prediction of fluid responsiveness in septic shock patients: comparing stroke volume variation by FloTrac/Vigileo and automated pulse pressure variation. Eur. J. Anaesthesiol. 29, 64–69 (2012).
Shah, S., Kaul, A., Khandare, J. & Dhalait, S. Comparison of invasive arterial blood pressure monitoring vs. non-invasive blood pressure monitoring in preterm infants < 37 weeks in the neonatal intensive care unit— a prospective observational study. J. Trop Pediatr. 67, fmab109 (2021).
Zhou, J., Elkhateeb, O. & Lee, K.-S. Comparison of non-invasive vs invasive blood pressure measurement in neonates undergoing therapeutic hypothermia for hypoxic ischemic encephalopathy. J. Perinatol. 36, 381–385 (2016).
Kharrat, A. et al. The Relationship between blood pressure parameters and left ventricular output in neonates. J. Perinatol. 39, 619–625 (2019).
Lee, E.-P. et al. Diastolic blood pressure impact on pediatric refractory septic shock outcomes. Pediatr. Neonatol. 65, 222–228 (2024).
Elsayed, Y. N., Amer, R. & Seshia, M. M. The impact of integrated evaluation of hemodynamics using targeted neonatal echocardiography with indices of tissue oxygenation: a new approach. J. Perinatol. 37, 527–535 (2017).
Elsayed, Y. N. et al. Integrated evaluation of hemodynamics: a novel approach for the assessment and management of preterm infants with compromised systemic circulation. J. Perinatol. 38, 1337–1343 (2018).
Verstraete, E. H., Blot, K., Mahieu, L., Vogelaers, D. & Blot, S. Prediction models for neonatal health care–associated sepsis: a meta-analysis. Pediatrics 135, e1002–e1014 (2015).
Feng, M. et al. Transthoracic echocardiography and mortality in sepsis: analysis of the MIMIC-III database. Intensive Care Med. 44, 884–892 (2018).
Gill, A. B. & Weindling, A. M. Echocardiographic assessment of cardiac function in shocked very low birthweight infants. Arch. Dis. Child. 68, 17–21 (1993).
Gudmundsson, P., Rydberg, E., Winter, R. & Willenheimer, R. Visually estimated left ventricular ejection fraction by echocardiography is closely correlated with formal quantitative methods. Int. J. Cardiol. 101, 209–212 (2005).
Li, J. et al. The prognostic value of left ventricular systolic function and cardiac biomarkers in pediatric severe sepsis. Medicine 98, e15070 (2019).
Williams, F. Z., Sachdeva, R., Travers, C. D., Walson, K. H. & Hebbar, K. B. Characterization of myocardial dysfunction in fluid- and catecholamine-refractory pediatric septic shock and its clinical significance. J. Intensive Care Med. 34, 17–25 (2019).
Pulido, J. N. et al. Clinical spectrum, frequency, and significance of myocardial dysfunction in severe sepsis and septic shock. Mayo Clin. Proc. 87, 620–628 (2012).
Vieillard-Baron, A., Prin, S., Chergui, K., Dubourg, O. & Jardin, F. Hemodynamic instability in sepsis: bedside assessment by Doppler echocardiography. Am. J. Respir. Crit. Care Med. 168, 1270–1276 (2003).
Gunjan, K., Modi, M., Thakur, A., Soni, A. & Saluja, S. Echocardiographic characteristics in neonates with septic shock. Eur. J. Pediatr. 183, 1849–1855 (2024).
Huang, S. J., Nalos, M. & McLean, A. S. Is early ventricular dysfunction or dilatation associated with lower mortality rate in adult severe sepsis and septic shock? A meta-analysis. Crit. Care 17, R96 (2013).
Raj, S., Killinger, J. S., Gonzalez, J. A. & Lopez, L. Myocardial dysfunction in pediatric septic shock. J. Pediatr. 164, 72–77.e2 (2014).
Abdel-Hady, H. E., Matter, M. K. & El-Arman, M. M. Myocardial dysfunction in neonatal sepsis: a tissue Doppler imaging study*. Pediatr. Crit. Care Med. 13, 318–323 (2012).
Tomerak, R. H., El-Badawy, A. A., Hussein, G., Kamel, N. R. M. & Razak, A. R. A. Echocardiogram done early in neonatal sepsis: what does it add? J. Investig. Med 60, 680–684 (2012).
A Al-Biltagi, M. Cardiac functions by tissue doppler and speckle tracking echocardiography in neonatal sepsis and its correlation with sepsis markers and cardiac troponin-T. J. Pediatr. Neonatal Care 5, 00184 (2016).
Yang, C. et al. NT-Pro-BNP and echocardiography for the early assessment of cardiovascular dysfunction in neonates with sepsis. Medicine 101, e30439 (2022).
Landesberg, G. et al. Diastolic dysfunction and mortality in severe sepsis and septic shock. Eur. Heart J. 33, 895–903 (2012).
Smith, A. et al. Accuracy and reliability of qualitative echocardiography assessment of right ventricular size and function in neonates. Echocardiography 36, 1346–1352 (2019).
Tissot, C., Singh, Y. & Sekarski, N. Echocardiographic evaluation of ventricular function-for the neonatologist and pediatric intensivist. Front. Pediatr. 6, 79 (2018).
Koestenberger, M. et al. Systolic right ventricular function in preterm and term neonates: reference values of the Tricuspid Annular Plane Systolic Excursion (TAPSE) in 258 patients and calculation of Z-score values. Neonatology 100, 85–92 (2011).
Koestenberger, M. et al. Right ventricular function in infants, children and adolescents: reference values of the Tricuspid Annular Plane Systolic Excursion (TAPSE) in 640 healthy patients and calculation of Z-score values. J. Am. Soc. Echocardiogr. 22, 715–719 (2009).
Jain, A. et al. A comprehensive echocardiographic protocol for assessing neonatal right ventricular dimensions and function in the transitional period: normative data and Z- scores. J. Am. Soc. Echocardiogr. 27, 1293–1304 (2014).
Alzahrani, A. K. Cardiac function affection in infants with neonatal sepsis. J. Clin. Trial 7, 329 (2017).
Levy, P. T. et al. Right ventricular function in preterm and term neonates: reference values for right ventricle areas and fractional area of change. J. Am. Soc. Echocardiogr. 28, 559–569 (2015).
Ahmed, T., Abqari, S., Firdaus, U., Shahab, T. & Ali, S. M. Status of pulmonary artery pressures on echocardiography among high-risk newborns. J. Clin. Neonatol. 9, 235 (2020).
Galiuto, L., Ignone, G. & DeMaria, A. N. Contraction and relaxation velocities of the normal left ventricle using pulsed-wave tissue doppler echocardiography. Am. J. Cardiol. 81, 609–614 (1998).
Furian, T. et al. Ventricular dysfunction and dilation in severe sepsis and septic shock: Relation to endothelial function and mortality. J. Crit. Care 27, 319.e9–319.e15 (2012).
Ho, C. Y. & Solomon, S. D. A clinician’s guide to tissue Doppler imaging. Circulation 113, e396–8 (2006).
James, A. T. et al. Assessment of myocardial performance in preterm infants less than 29 weeks gestation during the transitional period. Early Hum. Dev. 90, 829–835 (2014).
Murase, M., Morisawa, T. & Ishida, A. Serial assessment of left-ventricular function using tissue doppler imaging in premature infants within 7 days of life. Pediatr. Cardiol. 34, 1491–1498 (2013).
Murase, M., Morisawa, T. & Ishida, A. Serial assessment of right ventricular function using tissue Doppler imaging in preterm infants within 7 days of life. Early Hum. Dev. 91, 125–130 (2015).
Sanfilippo, F. et al. Tissue Doppler assessment of diastolic function and relationship with mortality in critically ill septic patients: a systematic review and meta-analysis. Br. J. Anaesth. 119, 583–594 (2017).
Sanfilippo, F. et al. Diastolic dysfunction and mortality in septic patients: a systematic review and meta-analysis. Intensive Care Med. 41, 1004–1013 (2015).
Breatnach, C. R., Levy, P. T., James, A. T., Franklin, O. & El-Khuffash, A. Novel echocardiography methods in the functional assessment of the newborn heart. Neonatology 110, 248–260 (2016).
EL-Khuffash, A. F., Jain, A., Weisz, D., Mertens, L. & McNamara, P. J. Assessment and treatment of post patent ductus arteriosus ligation syndrome. J. Pediatr. 165, 46–52.e1 (2014).
Sutherland, G. R., Di Salvo, G., Claus, P., D’hooge, J. & Bijnens, B. Strain and strain rate imaging: a new clinical approach to quantifying regional myocardial function. J. Am. Soc. Echocardiogr. 17, 788–802 (2004).
Abraham, T. P., Dimaano, V. L. & Liang, H.-Y. Role of tissue doppler and strain echocardiography in current clinical practice. Circulation 116, 2597–2609 (2007).
Nesbitt, G. C., Mankad, S. & Oh, J. K. Strain imaging in echocardiography: methods and clinical applications. Int J. Cardiovasc. Imaging 25, 9–22 (2009).
Stanton, T., Leano, R. & Marwick, T. H. Prediction of all-cause mortality from global longitudinal speckle strain: comparison with ejection fraction and wall motion scoring. Circ. Cardiovasc. Imaging 2, 356–364 (2009).
Basu, S. et al. Two-dimensional speckle tracking imaging detects impaired myocardial performance in children with septic shock, not recognized by conventional echocardiography*. Pediatr. Crit. Care Med. 13, 259–264 (2012).
Haileselassie, B. et al. Strain echocardiography parameters correlate with disease severity in children and infants with sepsis*. Pediatr. Crit. Care Med. 17, 383–390 (2016).
Patel, M. D. et al. Cardiac dysfunction identified by strain echocardiography is associated with illness severity in pediatric sepsis. Pediatr. Crit. Care Med. 21, e192–e199 (2020).
Sanfilippo, F. et al. Left ventricular systolic function evaluated by strain echocardiography and relationship with mortality in patients with severe sepsis or septic shock: a systematic review and meta-analysis. Crit. Care 22, 183 (2018).
El-Khuffash, A. et al. Deformation imaging and rotational mechanics in neonates: a guide to image acquisition, measurement, interpretation, and reference values. Pediatr. Res. 84, 30–45 (2018).
Griffin, M. P. & Moorman, J. R. Toward the early diagnosis of neonatal sepsis and sepsis-like illness using novel heart rate analysis. Pediatrics 107, 97–104 (2001).
Fairchild, K. D., Srinivasan, V., Randall Moorman, J., Gaykema, R. P. A. & Goehler, L. E. Pathogen-induced heart rate changes associated with cholinergic nervous system activation. Am. J. Physiol. Regul. Integr. Comp. Physiol. 300, R330–R339 (2011).
Moorman, J. R. et al. Mortality reduction by heart rate characteristic monitoring in very low birth weight neonates: a randomized trial. J. Pediatr. 159, 900–906.e1 (2011).
Chiera, M. et al. Heart rate variability in the perinatal period: a critical and conceptual review. Front. Neurosci. 14, 561186 (2020).
Fairchild, K. D. et al. Septicemia mortality reduction in neonates in a heart rate characteristics monitoring trial. Pediatr. Res. 74, 570–575 (2013).
Meeus, M. et al. Clinical decision support for improved neonatal care: the development of a machine learning model for the prediction of late-onset sepsis and necrotizing enterocolitis. J. Pediatr. 266, 113869 (2024).
Cabrera-Quiros, L. et al. Prediction of late-onset sepsis in preterm infants using monitoring signals and machine learning. Crit. Care Explor. 3, e0302 (2021).
Kausch, S. L. et al. Cardiorespiratory signature of neonatal sepsis: development and validation of prediction models in 3 NICUs. Pediatr. Res. 93, 1913–1921 (2023).
Leon, C., Carrault, G., Pladys, P. & Beuchee, A. Early detection of late onset sepsis in premature infants using visibility graph analysis of heart rate variability. IEEE J. Biomed. Health Inform. 25, 1006–1017 (2021).
Alderliesten, T. et al. Reference values of regional cerebral oxygen saturation during the first 3 days of life in preterm neonates. Pediatr. Res. 79, 55–64 (2016).
Bruckner, M. et al. Normal regional tissue oxygen saturation in neonates: a systematic qualitative review. Pediatr Res. https://doi.org/10.1038/s41390-021-01786-y (2021).
Hyttel-Sorensen, S. et al. Cerebral near infrared spectroscopy oximetry in extremely preterm infants: phase II randomised clinical trial. BMJ 350, g7635 (2015).
Yu, P. et al. Early changes in near-infrared spectroscopy are associated with cardiac arrest in children with congenital heart disease. Front. Pediatr. 10, 894125 (2022).
Hickok, R. L., Spaeder, M. C., Berger, J. T., Schuette, J. J. & Klugman, D. Postoperative abdominal NIRS values predict low cardiac output syndrome in neonates. World J. Pediatr. Congenit. Heart Surg. 7, 180–184 (2016).
Levy, P. T. et al. Near-infrared spectroscopy for perioperative assessment and neonatal interventions. Pediatr. Res. https://doi.org/10.1038/s41390-021-01791-1 (2021).
van der Laan, M. E. et al. Multisite tissue oxygenation monitoring indicates organ-specific flow distribution and oxygen delivery related to low cardiac output in preterm infants with clinical sepsis. Pediatr. Crit. Care Med. 17, 764–771 (2016).
Mileder, L. P. et al. Non-invasively measured venous oxygen saturation as early marker of impaired oxygen delivery in preterm neonates. Front. Pediatr. 10, 834045 (2022).
Rallis, D. et al. The association of the cerebral oxygenation during neonatal sepsis with the Bayley-III Scale of Infant and Toddler Development index scores at 18–24 months of age. Early Hum. Dev. 136, 49–53 (2019).
Zonnenberg, I. A., van Dijk, J., van den Dungen, F. A. M., Vermeulen, R. J. & van Weissenbruch, M. M. The prognostic value of NIRS in preterm infants with (suspected) late-onset sepsis in relation to long term outcome: a pilot study. PLoS ONE 14, e0220044 (2019).
Martini, S. et al. Near-infrared spectroscopy monitoring of neonatal cerebrovascular reactivity: Where are we now? Pediatr Res. https://doi.org/10.1038/s41390-023-02574-6 (2023).
Hansen, M. L. et al. Cerebral oximetry monitoring in extremely preterm infants. N. Engl. J. Med. 388, 1501–1511 (2023).
de Boode, W.-P. Advanced hemodynamic monitoring in the neonatal intensive care unit. Clin. Perinatol. 47, 423–434 (2020).
Murphy, E., Healy, D. B., Chioma, R. & Dempsey, E. M. Evaluation of the hypotensive preterm infant: evidence-based practice at the bedside? Children 10, 519 (2023).
Marqué, S., Cariou, A., Chiche, J.-D. & Squara, P. Comparison between Flotrac-Vigileo and Bioreactance, a totally noninvasive method for cardiac output monitoring. Crit. Care 13, R73 (2009).
Raval, N. Y. et al. Multicenter evaluation of noninvasive cardiac output measurement by bioreactance technique. J. Clin. Monit. Comput. 22, 113–119 (2008).
Squara, P. et al. Noninvasive cardiac output monitoring (NICOM): a clinical validation. Intensive Care Med. 33, 1191–1194 (2007).
Weisz, D. E., Jain, A., McNamara, P. J. & EL-Khuffash, A. Non-invasive cardiac output monitoring in neonates using bioreactance: a comparison with echocardiography. NEO 102, 61–67 (2012).
Weisz, D. E., Jain, A., Ting, J., McNamara, P. J. & EL-Khuffash, A. Non-invasive cardiac output monitoring in preterm infants undergoing patent ductus arteriosus ligation: a comparison with echocardiography. NEO 106, 330–336 (2014).
Van Wyk, L., Gupta, S., Lawrenson, J. & de Boode, W.-P. Accuracy and trending ability of electrical biosensing technology for non-invasive cardiac output monitoring in neonates: a systematic qualitative review. Front. Pediatr. 10, 851850 (2022).
Matsushita, F. Y., Krebs, V. L. J. & De Carvalho, W. B. Association between serum lactate and morbidity and mortality in neonates: a systematic review and meta-analysis. Children 10, 1796 (2023).
Song, Y., Wang, N., Xie, X., Tian, Y. & Wang, Y. Relationship between lactate levels and 28-day mortality in pediatric sepsis: results from the pediatric intensive care database. BMC Pediatr. 24, 712 (2024).
Shankar-Hari, M. et al. Developing a new definition and assessing new clinical criteria for septic shock: for the third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 315, 775–787 (2016).
Weiss, S. L. et al. Surviving sepsis campaign international guidelines for the management of septic shock and sepsis-associated organ dysfunction in children. Pediatr. Crit. Care Med. 21, e52 (2020).
Miselli, F. et al. Outcome prediction for late-onset sepsis after premature birth. Pediatr. Res. 1–7 https://doi.org/10.1038/s41390-025-03814-7 (2025).
Yilmaz, A. et al. Evaluating of neonatal early onset sepsis through lactate and base excess monitoring. Sci. Rep. 13, 14837 (2023).
Wu, A. H. B. Increased troponin in patients with sepsis and septic shock: myocardial necrosis or reversible myocardial depression? Intensive Care Med. 27, 959–961 (2001).
Bessière, F., Khenifer, S., Dubourg, J., Durieu, I. & Lega, J.-C. Prognostic value of troponins in sepsis: a meta-analysis. Intensive Care Med. 39, 1181–1189 (2013).
Sheyin, O., Davies, O., Duan, W. & Perez, X. The prognostic significance of troponin elevation in patients with sepsis: a meta-analysis. Heart Lung 44, 75–81 (2015).
Thiru, Y., Pathan, N., Bignall, S., Habibi, P. & Levin, M. A myocardial cytotoxic process is involved in the cardiac dysfunction of meningococcal septic shock. Crit. Care Med. 28, 2979–2983 (2000).
Correale, M. et al. Troponin in newborns and pediatric patients. Cardiovasc. Hematol. Agents Med. Chem. 7, 270–278 (2009).
Sweetman, D., Armstrong, K., Murphy, J. & Molloy, E. Cardiac biomarkers in neonatal hypoxic ischaemia: cardiac biomarkers in neonatal hypoxic ischaemia. Acta Paediatr. 101, 338–343 (2012).
Armstrong, K., Franklin, O., Sweetman, D. & Molloy, E. J. Cardiovascular dysfunction in infants with neonatal encephalopathy. Arch. Dis. Child 97, 372–375 (2012).
Lee, I.-C., Yu, C.-S., Wong, S.-H. & Lue, K.-H. Troponin I levels in neonatal hypoxic–ischemic encephalopathy are related to cardiopulmonary comorbidity and neurodevelopmental outcomes. JCM 10, 4010 (2021).
EL-Khuffash, A., Davis, P. G., Walsh, K. & Molloy, E. J. Cardiac troponin T and N-terminal-pro-B type natriuretic peptide reflect myocardial function in preterm infants. J. Perinatol. 28, 482–486 (2008).
Ramadhina, N. et al. Ventricular function and high-sensitivity cardiac troponin T in preterm infants with neonatal sepsis. PI 55, 203 (2015).
Cruz, M. A. et al. Cardiac troponin T and cardiac dysfunction in extremely low-birth-weight infants. Pediatr. Cardiol. 27, 396–401 (2006).
Perugu, S., Rehan, V. K., Chow, S. L. & Baylen, B. Plasma biomarkers and echocardiographic indices of left ventricular function in very low birth weight infants. J. Neonatal Perinat. Med. 7, 213–222 (2014).
Karlén, J., Karlsson, M., Eliasson, H., Bonamy, A.-K. E. & Halvorsen, C. P. Cardiac troponin T in healthy full-term infants. Pediatr. Cardiol. 40, 1645–1654 (2019).
Tarkowska, A. & Furmaga-Jabłońska, W. The evaluation of cardiac troponin T in newborns. Biomed. Hub. 2, 1–7 (2017).
El-Khuffash, A. & Molloy, E. J. Are B-type natriuretic peptide (BNP) and N-terminal-pro-BNP useful in neonates? Arch. Dis. Child. Fetal Neonatal Ed. 92, F320–F324 (2007).
Khoury, J. et al. The prognostic value of brain natriuretic peptide (BNP) in non-cardiac patients with sepsis, ultra-long follow-up. J. Crit. Care 42, 117–122 (2017).
Wang, F. et al. Brain natriuretic peptide for prediction of mortality in patients with sepsis: a systematic review and meta-analysis. Crit. Care 16, R74 (2012).
Domico, M., Liao, P., Anas, N. & Mink, R. B. Elevation of brain natriuretic peptide levels in children with septic shock*. Pediatr. Crit. Care Med. 9, 478–483 (2008).
Klouche, K. et al. Plasma brain natriuretic peptide and troponin levels in severe sepsis and septic shock: relationships with systolic myocardial dysfunction and intensive care unit mortality. J. Intensive Care Med. 29, 229–237 (2014).
Maeder, M., Ammann, P., Kiowski, W. & Rickli, H. B-type natriuretic peptide in patients with sepsis and preserved left ventricular ejection fraction. Eur. J. Heart Fail. 7, 1164–1167 (2005).
He, Q. & LaPointe, M. C. Interleukin-1β regulation of the human brain natriuretic peptide promoter involves Ras-, Rac-, and p38 kinase–dependent pathways in cardiac myocytes. Hypertension 33, 283–289 (1999).
Tomaru, K. et al. Transcriptional activation of the BNP gene by lipopolysaccharide is mediated through GATA elements in neonatal rat cardiac myocytes. J. Mol. Cell. Cardiol. 34, 649–659 (2002).
Zafra-Rodríguez, P., Méndez-Abad, P., Lubián-López, S. P. & Benavente-Fernández, I. NT-proBNP as an early marker of diastolic ventricular dysfunction in very-low-birth-weight infants. Pediatr. Cardiol. 40, 1165–1170 (2019).
Nir, A. et al. NT-Pro-B-type natriuretic peptide in infants and children: reference values based on combined data from four studies. Pediatr. Cardiol. 30, 3–8 (2009).
El-Khuffash, A., Barry, D., Walsh, K., Davis, P. G. & Molloy, E. J. Biochemical markers may identify preterm infants with a patent ductus arteriosus at high risk of death or severe intraventricular haemorrhage. Arch. Dis. Child. Fetal Neonatal Ed. 93, F407–F412 (2008).
EL-Khuffash, A. & Molloy, E. The use of N-terminal-Pro-BNP in preterm infants. Int. J. Pediatr. 2009, 1–7 (2009).
Noori, S. & Seri, I. Pathophysiology of newborn hypotension outside the transitional period. Early Hum. Dev. 81, 399–404 (2005).
Reynolds, E. W., Ellington, J. G., Vranicar, M. & Bada, H. S. Brain-type natriuretic peptide in the diagnosis and management of persistent pulmonary hypertension of the newborn. Pediatrics 114, 1297–1304 (2004).
Llitjos, J.-F. et al. Enhancing sepsis biomarker development: key considerations from public and private perspectives. Crit. Care 28, 238 (2024).
Funding
Open Access funding provided by the IReL Consortium.
Author information
Authors and Affiliations
Consortia
Contributions
All authors contributed significantly to drafting different sections of the manuscript. All authors were involved in reviewing the manuscript, revising it critically for important intellectual content and editing accordingly. SL and MP were responsible for the included figures and echocardiographic images, respectively. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The author declares no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Duignan, S.M., Lakshminrusimha, S., Armstrong, K. et al. Neonatal sepsis and cardiovascular dysfunction II: assessment. Pediatr Res (2026). https://doi.org/10.1038/s41390-026-04903-x
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41390-026-04903-x
