
Abstract
Background
Biomarkers are important for early diagnosis, guiding prognosis, and identifying potential therapeutic agents. Many biomarkers have been investigated as potential prognostic markers in Neonatal Encephalopathy (NE), none are measured routinely. We examined current evidence of serum biomarkers to predict outcome.
Methods
We prospectively registered with PROSPERO. We searched EMBASE, PubMed, World of Science, and the Cochrane Library databases for studies of biomarkers in NE. We dichotomised participants by normal or adverse outcome and calculated the mean difference (MD) in biomarkers between groups.
Results
Literature search provided 3046 results. 98 studies of >20 different biomarkers were eligible. We completed meta-analyses, including 47 studies, for serum interleukin (IL)-1β, IL-6, IL-8, IL-10, Neuron Specific Enolase (NSE), S100, and Tumour Necrosis Factor (TNF)-α. Higher IL-6 70.22 pg/ml (95% confidence interval (CI) 0.55, 139.89), IL-8 15.72 pg/ml (95% CI 3.59, 27.85), NSE 38.95 pg/ml (95% CI 18.33, 59.57), and TNF-α 20.84 pg/ml (95% CI 6.24, 35.45) were associated with adverse long-term outcome. Higher IL-6 22.57 pg/ml (95% CI 0.66, 44.49) and lactate 4.5 mg/dL (95% CI 0.66, 44.49) were associated with adverse short-term outcomes.
Conclusion
Several biomarkers especially provide promising prognostic value in NE. Greater uniformity in biomarker outcome reporting would allow improved evidence synthesis.
Impact Statement
-
Elevated biomarkers such as Serum IL-6, IL-8, NSE, and TNF-α were associated with adverse long-term outcomes in NE and are promising as surrogate biomarkers of early outcomes
-
Small sample size, lack of uniformity of timing and sampling, as well as analysis, make definitive conclusions challenging.
-
Future collaboration to standardise timing and analysis of biomarkers in larger international cohorts would facilitate translation to the bedside.
Similar content being viewed by others


Introduction
Neonatal Encephalopathy (NE) describes central nervous system dysfunction in the first few days of life in term and near-term infants.1 It has a multifactorial aetiology.2 The incidence of NE is between 0.5–3 per 1000 live births in high-income countries, but is much more frequent in low-income settings.3 NE is associated with a high incidence of early mortality and disability in survivors.4 NE is difficult to diagnose, to treat, and to predict outcomes. Currently, diagnosis and prognosis are based on clinical, neuroimaging and electrophysiological markers when available.5 However, accurate prediction of prognosis and identification of patients at risk of adverse neurodevelopmental outcomes remains a significant challenge.6 In recent years, there has been extensive research in blood, urine and cerebrospinal fluid (CSF) biomarkers in NE.7 Biomarkers function to provide an understanding of the pathophysiology of the condition and therefore pathways that can be targeted with future therapies, and to provide individualised prognosis for patients. Biomarkers may help identify infants at high risk of NE, objectively classify the severity of NE, predict response to treatment and prognosticate outcome. Despite this research, there is no gold standard biomarker known at present. Although prediction of adverse outcomes is difficult, there is increasing evidence for the benefit of early recognition and intervention for high-risk patients.8 With limited resources, it is essential to identify those patients at high risk so that they can be prioritised for early intervention services. Identifying prognostic biomarkers has implications for counselling parents on expected neurodevelopmental outcomes, future adjunctive therapies, and guiding research.
Methods
The study was prospectively registered with Prospero (CRD42017056763). The systematic review followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and the Cochrane Handbook.
Search strategy
Four major databases, EMBASE, MEDLINE, World of Science and the Cochrane Library were systematically searched in January 2017 for studies published between January 1966 and December 2016. A repeat search, using an identical search strategy, was conducted in March 2021, as the original search was out of date. The search strategy included the following relevant terms: ‘neonatal’ or ‘newborn’, ‘neonatal encephalopathy’ or ‘hypoxic ischaemic encephalopathy’ or ‘perinatal asphyxia’, ‘biomarker’ or ‘biological indicator’ or ‘serum marker’. The complete search strategy and MESH terms used are reported in Supplement S1. Authors were contacted for additional details not included in the publication if they were required for inclusion in a meta-analysis.
Eligibility criteria
Studies were eligible for inclusion if they reported prognostic blood or CSF biomarkers for NE and outcomes including severity of NE (by a standardised scoring system), death or neurodevelopmental outcomes at ages ≥12 months. Studies that used any definition of NE, HIE, or birth asphyxia that included features of encephalopathy in the first 24 h of life in patients ≥35 weeks of gestational age were included in the qualitative analysis. To be included in a meta-analysis, studies had to report outcomes that could be categorised as ‘normal’ or ‘adverse’. Studies also had to report continuous data for prognostic biomarkers in means and standard deviations, or data that could be converted reliably into means and standard deviations, to be included in a meta-analysis. Studies that included patients who received TH and those that did not were included in the study. Case reports were excluded, but studies of all other design types were included. No language or publication restrictions were applied.
Outcome definition
The primary outcome was defined as a composite of mortality in the first 28 days of life, abnormal MRI brain, or abnormal clinical assessment within the first week of life for the short-term outcome, and a composite of death or adverse neurodevelopmental outcome at ≥12 months of age for the long-term outcome. Neurodevelopmental outcomes used to define adverse outcomes included cerebral palsy, developmental delay, abnormal neurological exam, or adverse result on several standardised tests of child development, including Bayley Scales of Infant Development or Griffith Scales. The timing, reported outcome, and definition of adverse outcome for each included study are outlined in the Supplement S2.
Study search and selection
Results from the study search were uploaded to Covidence software and duplicates were removed. The title, abstract and full text screening were conducted independently by two investigators (MOD and TH for the original search, TH, AB, PS, and ST for the updated search). Disagreements were resolved by consensus. Studies deemed eligible for inclusion were categorised by prognostic biomarker and included in the meta-analysis if outcomes were reported in a comparable manner.
Risk of bias and quality assessment
Risk of bias for included studies was assessed using the Quality in Prognostic Studies (QUIPS) tool.9 Each study was assessed and assigned a rating of low, moderate, or high risk of bias according to 6 criteria: study participation, study attrition, prognostic factor measurement, outcome measurement, study confounding and statistical analysis and reporting. Assessment was completed independently by two researchers (MOD & TH) and disagreements resolved by consensus. Studies with ≥1 criteria at high risk of bias were excluded from the meta-analysis.
Data extraction
A standard data extraction table was created following the CHARMS (CHecklist for critical Appraisal and data extraction for systematic Reviews of prediction Modelling Studies) checklist.10 The following data were collected: characteristics of included studies, patient characteristics, prognostic factors and outcome definitions and measurements. The data extraction form was completed independently by two researchers (MOD and TH) and disagreements were resolved by consensus. We included all data in a meta-analysis if the study met our inclusion and exclusion criteria, if the biomarker measurement was reported in sufficient detail, and if there was sufficient data provided to dichotomise participant outcome as normal or abnormal. Studies variably reported biomarker measurement as means and standard deviations or medians and ranges. To assimilate studies using different statistics for reported measures, conversion was completed when required using the methods described by Hozo et al, Wan et al, and Luo et al.11,12,13. When missing data were encountered, authors were contacted by email to request data.
Statistical analysis
A meta-analysis was completed if there were at least two studies that provided data that could be synthesised appropriately. For all completed meta-analyses, we compared continuous data for the biomarker from two groups: a normal or good outcome group compared to the adverse outcome group. For categorical data, the odds ratio (OR) of adverse outcome was calculated with 95% confidence intervals. Between-group mean differences and 95% confidence intervals were calculated for each biomarker for which a meta-analysis was completed, to compare normal and abnormal outcome groups. A random effects model was used due to differences in patient demographic profiles between studies, differences in severity profiles between studies, and differences in the use of TH between studies. The leave-one-out method was used to assess the effect of individual studies on the pooled effect estimate. Small study effects were assessed by visual inspection of the funnel plot. We intended to quantify the effect using the Peters linear regression test, however no meta-analysis included more than 10 studies. Meta-analysis and statistical analysis were completed using RevMan software (v5.4). Tests were 2-tailed, and results were considered significant at the level p < 0.05.
Results
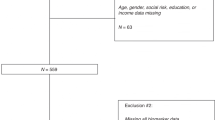
We identified 2464 studies from the literature search following removal of duplicates, and grey literature sources provided a further 22 studies (Fig. 1). Following title and abstract screening, there were 468 studies suitable for full text screening, of which 132 studies were included for qualitative synthesis. From these 132 studies, we identified over 30 individual prognostic biomarkers, and 47 studies could be included in meta-analyses for biomarkers to predict long- or short-term outcomes in NE. Articles were published between 1994 and 2021 and originated from more than 20 different countries. The 47 studies included in the meta-analyses included over 1000 participants, ranging from 19 to 95 participants per study. There were over 50 different primary outcomes reported from studies included in the meta-analyses in keeping with previous reviews. Studies of all design types, including cohort, retrospective and prospective, case-control studies, and randomised controlled trials if the non-intervention group could be examined independently, were included in this systematic review. All studies were conducted in a hospital setting. We intended to exclude any study that was judged to be high risk of bias, however this was not required for the current review.

PRISMA flow diagram.
Blood and serum biomarkers to predict long-term outcome in neonatal encephalopathy
We could complete meta-analyses for 8 serum biomarkers including interleukin (IL)-1β,14,15,16,17 IL-6,14,15,17,18,19,20 IL-8,14,18,20 IL-1019,20, neuron specific enolase (NSE),21,22,23 S100,15,24 S100B,22,25 and tumour necrosis factor (TNF)-α14,15,16,17,26 to predict long-term outcome in NE (Table 1). The number of eligible studies for analysis of any individual serum biomarker ranged from two to eight. In total, 1077 individual participant results are included in the study, from 13 different studies. Included studies were published between 1998 and 2021, and included participants treated and not treated with TH. All included studies were at moderate risk of bias. Significant clinical or statistical between-study heterogeneity was identified in each meta-analysis. Higher serum IL-6, IL-8, NSE, and TNF-α were associated with adverse outcomes in NE (Fig. 2). However, we found no evidence of a significant difference in serum IL-1β, IL-10, S100, or S100B between groups (Table 1).

Forest plot comparison of serum biomarkers between newborns with normal and adverse long-term outcomes in neonatal encephalopathy.
Higher serum IL-6, mean difference 70.22 pg/ml (95% CI 0.55–139.89), was associated with increased risk of adverse outcome (Fig. 2a).14,15,17,18,19,20 The meta-analysis included 260 participants from six studies. Individual study results consistently associated higher IL-6 with abnormal outcome; however, the size of the effect varied significantly between studies, and the point estimates are highly disparate. One included study had extremely wide confidence intervals, but further analysis of this study did not indicate any risk of bias, and exclusion of the study did not affect the conclusions of the meta-analysis.18
Higher serum IL-8, mean difference 15.72 pg/ml (95% CI 3.59–27.85), was associated with increased risk of adverse outcome (Fig. 2b).14,18,20 The meta-analysis included 103 participants from three studies. Individual study results consistently associated higher IL-8 with abnormal outcomes. These tests do not accurately reflect the heterogeneity in the meta-analysis nor the between-study variability, which is evident from visual inspection of the forest plot. One included study has extremely wide confidence intervals.18 Further analysis of this study did not indicate any risk of bias and exclusion of the study did not affect the conclusions of the meta-analysis.
Higher serum NSE, mean difference 38.95 pg/ml (95% CI 18.33–59.57), was associated with increased risk of adverse outcome (Fig. 2c).21,22,23 The meta-analysis included 124 participants from three studies. Individual study results consistently associated higher NSE with abnormal outcome, however, the size of the effect varied significantly between studies.
Higher serum TNF-α, mean difference 20.84 pg/ml (95% CI 6.24–35.45), was associated with increased risk of adverse outcome (2D).14,15,16,17,26 The meta-analysis included 184 participants from five studies. Individual study results consistently associated higher TNF-α with abnormal outcomes. Although only two of the five studies reached statistical significance, there is substantial overlap of confidence intervals for four of the five included studies. However, the size of the effect varied significantly between studies and the point estimates are moderately disparate. One outlier study reported substantially higher mean TNF-α for both groups and the study (26). Further analysis of this study did not indicate any risk of bias and exclusion of the study did not affect the conclusions of the meta-analysis, although it did substantially affect the effect size.
Some consistent sources of heterogeneity between included studies in all the meta-analyses are variation in the timing of sampling, method of biomarker measurement, and the inclusion of participants undergoing therapeutic hypothermia and those without.
Serum and blood biomarkers to predict short-term outcomes
We could complete meta-analyses for 11 serum and blood biomarkers in NE including ionised calcium,27,28,29 glucose,27,30,31,32 IL-1β,15,16,33 IL-6,15,18,34,35,36 lactate,37,38,39,40 lactate dehydrogenase,28,37,41,42,43 nucleated red blood cells (nRBC),44,45 S100,15,24,25 TNF-α,15,16,18,34,35 troponin,39,46,47 and white cell count (WCC)28,37 to predict short-term outcome in NE (Table 2). The number of eligible studies for analysis of individual serum biomarkers ranged from two to twelve, however the number of studies included in any meta-analysis was reduced due to variability in predictor measurement and reporting methods. We included 26 different studies with a total of 1742 individual participants. Included studies were published between 1998 and 2021, and included participants treated and not treated with TH. All included studies were at moderate risk of bias. Significant clinical or statistical between-study heterogeneity was identified in each meta-analysis. Higher serum IL-6 and lactate were associated with adverse short-term outcome in NE (Fig. 3). However, we found no evidence of a significant difference in ionised calcium, glucose, IL-1β, lactate dehydrogenase, nucleated red blood cells (nRBC), S100, TNF-α, troponin, or white cell count (WCC) between groups.

Forest plot comparison of serum biomarkers between newborns with normal and adverse long-term outcomes in neonatal encephalopathy.
Higher serum IL-6, mean difference 22.57 pg/ml (95% CI 0.66–44.49), was associated with increased risk of adverse outcome compared to patients who survived with a normal outcome (Fig. 3a).15,18,34,35,36 The meta-analysis included 172 participants from five studies. Only two of five studies reached statistical significance independently. There is substantial overlap of confidence intervals, although the confidence intervals for some studies are quite wide and point estimates for each individual study are all close to the summary point estimate. Due to very high standard deviations (SDs), some of the included studies were given very small weighting in the meta-analysis. There is significant heterogeneity in the meta-analysis (Chi2 6.2, df 4). The proportion of total variability in the meta-analysis attributable to between-study heterogeneity was moderate (I2 35%, Tau 198.7). One included study has extremely wide confidence intervals.18 Further analysis of this study did not indicate any risk of bias and exclusion of the study did not affect the conclusions of the meta-analysis.
Higher serum lactate, mean difference 4.5 mg/dL (95% CI 0.66–44.49), was associated with increased risk of adverse outcome compared to patients who survived with normal outcome (Fig. 3b).37,38,39,40 The meta-analysis included 267 participants from four studies. Individual study results consistently associated higher lactate with abnormal outcome, and three of four studies reached statistical significance. There is substantial overlap of confidence intervals, although the confidence intervals for some studies are quite wide. Point estimates for each individual study are all close to the summary point estimate. Due to very high SDs, some of the included studies were given very small weighting in the meta-analysis. There is evidence of heterogeneity in the meta-analysis, although the statistical tests do not confirm this (Chi2 2.88, df 3). The proportion of total variability in the meta-analysis attributable to between-study heterogeneity was very small (I2 0%, Tau 0.00), but this is likely to be an underestimate due to very small weighting given to two of the studies with large standard deviations. Further analysis of these studies did not indicate any risk of bias and exclusion of these studies did not affect the conclusions of the meta-analysis.
Sources of this heterogeneity include variation in the timing of sampling, method of biomarker measurement, and the inclusion of participants undergoing therapeutic hypothermia and those without.
Discussion
This systematic review and meta-analysis found that lower serum IL-6, IL-8, NSE, and TNF-α were associated with good long-term outcomes in NE. However, the confidence intervals around the point estimate in the meta-analysis for all these biomarkers were very wide. Although the direction of the effect was consistent within each meta-analysis, confidence intervals of individual included studies were also very wide and crossed the line of no effect, and there was very limited overlap of confidence intervals between studies. IL-6, IL-8, and TNF-α are all cytokines that promote inflammation in NE, and inflammation is an established causal mechanism of injury in NE.48 NSE is an enzyme released in response to neuronal damage, and is a sensitive marker of neuronal injury.49 There are no minimal clinically important differences established for any of the included biomarkers. Given the wide confidence intervals, we suggest interpreting the threshold values for each biomarker with caution. Therefore, we are interpreting the association of higher serum IL-6, IL-8, NSE, and TNF-α and an increased risk of adverse outcome with extreme caution and as providing only very low-level evidence. The inconsistency of results means it would not be appropriate to interpret these results as providing cut-off values for prognostic purposes for infants with NE and further investigation is required.
We found that lower serum IL-6 and blood lactate levels were associated with good short-term outcomes in infants with NE. The meta-analysis for IL-6 included 5 studies, of which two individual studies demonstrated a significant difference between groups. The confidence intervals for all other studies crossed the line of no effect and there was very limited overlap of confidence intervals. Therefore, we are interpreting the association of higher in serum IL-6 and an increased risk of abnormal short-term outcome with extreme caution and providing very low-level evidence only. We suggest that the question requires further investigation. There was excellent consistency of effect direction for blood lactate, with 3 of 4 included studies demonstrating a significant difference between group and a high degree of overlap between studies. However, the confidence interval around the point estimate for the meta-analysis was wide. Therefore, the inconsistency of results means it would not be appropriate to interpret these results as providing cut-off values for prognostic purposes for infants with NE. As there are many individual factors that influence biomarker levels, including severity of NE, cause of NE, sex, presence of sepsis or infection, timing of biomarker measurement, treatment with therapeutic hypothermia, the more detail on these factors reported from individual studies would facilitate greater understanding of the influence of each. In the absence of this detail, we included all relevant studies and recognise the limitations on the interpretation that we can conclude from the results.
This is the first systematic review to our knowledge to examine a wide range of blood, and serum biomarkers to predict outcome in NE in the era of therapeutic hypothermia. Ramaswamy et al. published a systematic review in 2009 that demonstrated similar results to our study in the pre-TH era.50 They found that serum IL-1β, serum IL-6, CSF IL-1β, and CSF NSE were putative predictors of long-term outcome in infants with NE. However, this was prior to the introduction of routine treatment with TH in high-resource settings. TH influences circulating inflammatory cytokines, as demonstrated by the study by Jenkins.20 However, the influence has not been explored in greater depth through a systematic review to date. We intended to assess the specific influence of TH on each cytokine through subgroup analyses, however this was not possible as there were insufficient included studies in any meta-analysis.
Despite large volume of work and resources being applied to the understanding of blood, serum, and CSF biomarkers in NE, the current evidence for any individual biomarker remains very limited. A very large number of studies could not be included in a meta-analysis despite providing useful prognostic information due to variations in reporting mechanisms and a standardised approach to measurement and reporting of biomarkers in NE would improve this issue. The EQUATOR Network provides a framework for reporting and following its recommendations would result in greater certainty of evidence from meta-analyses.51
The prognostic information from blood and serum biomarkers compares poorly with other prognostic markers.5 There is much greater consistency of prognostic information from MRI and MRS compared to any biomarker in this study. However, systemic biomarkers provide additional information regarding the pathogenesis of the condition compared to other prognostic measurements.
Biomarkers not only provide prognostic outcomes but can also provide improved understanding of the underlying pathophysiology of the condition, which remains incompletely understood. Much of our understanding of the pathophysiology of NE comes from pre-clinical models52. However, many pre-clinical models involve ligation of the carotid artery in rodents or post-natal systemic hypoxia insults in piglets. While these models have vastly improved our understanding of the pathophysiology of the condition, they may not completely reflect the multiple aetiologies associated with NE in human neonates. It would aid our understanding of the pathophysiology of NE if we could accurately correlate the mechanisms in pre-clinical models and human neonates diagnosed with NE and it could also lead to faster development of adjunctive therapies in NE. Measurement of inflammatory biomarkers in patients with NE will help with this to assess if the pre-clinical model accurately reflects the pathophysiology in NE but will likely require examination of samples from a very large cohort of patients. Despite the limitations of combining studies in a meta-analysis, this may be the most pragmatic method to improve our understanding.
Unfortunately, the studies included in this systematic review are too small and there is too much variability between studies in the timing of measurement and the characteristics of included patients to draw any significant conclusions. Another limitation of this systematic review is that it is difficult to capture the complexity of the different phases of injury in NE, as the timing of blood sampling varied between each study. There were an insufficient number of included studies and insufficient consistency of sampling timing between studies to complete a subgroup analysis by timing. Biomarkers are also influenced by the presence of infection, duration of hypoxia, sex at birth, time of day when sampling is completed, whether the infant is undergoing TH, other medications used in their treatment, and this is not represented in this systematic review.
There are several international groups that are disease-specific aiming to standardise and harmonise the measurement of blood biomarkers. The following controllable factors can be standardised in an SOP: time of collection, needle size and location of draw, handling of tubes, time of last feed, tube type and additives, centrifugation parameters, time from collection to freeze, temperature of freeze, freeze-thaw cycles, aliquot size. However, other factors are uncontrollable, particularly individual factors like demographic characteristics, genomic results, gestation, placental abnormalities, medications, sedation and ventilation, which can all result in variation in biological biomarkers.53 In other diseases, following a systematic review of the evidence, expert groups have developed recommendations using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) methodology.54 These recommendations promote the application of blood-based biomarkers to clinical settings by using them to predict disease progression, guide prognosis, and evaluate response to new therapies. In Alzheimer’s disease, there are standardised guidelines for sample collection and management of blood-based biomarkers, and they are in the implementation phase for clinical use beyond clinical trials.52 Following these models and examples will advance neonatal encephalopathy biomarker research. Longitudinal measurements of biomarkers will also improve the evaluation of the disease-modifying effects of new therapies. However, larger cohorts with standardised blood biomarker assessment would be required with cross-site validation and robustness. Professional bodies such as the Newborn Brain Society, Society for Paediatric Research and the European Society for Paediatric Research have worked on consensus definitions and core datasets of NE.55 These collaborative models could be extended to implementation for biomarker research, in collaboration with families and clinical teams linking neonatology to neurodevelopmental teams.
Conclusion
We found evidence of an association between higher serum IL-6, IL-8, NSE, and TNF-α and adverse long-term outcome, and between higher IL-6 and blood lactate and adverse short-term outcome in NE. However, these results only provided very low certainty evidence and require further evaluation. These biomarkers should be the focus of future studies of prognostic biomarkers in NE.
References
Report of the American College of Obstetricians and Gynecologists’ Task Force on Neonatal Encephalopathy. Executive summary Neonatal encephalopathy and neurologic outcome, second edition. Report of the American College of Obstetricians and Gynecologists’ Task Force on Neonatal Encephalopathy. Obstet. Gynecol. 123, 896–901 (2014).
Aslam, S., Strickland, T. & Molloy, E. J. Neonatal Encephalopathy: need for recognition of multiple etiologies for optimal management. Front Pediatr. 7, 2019 (2019).
McIntyre, S. et al. Neonatal encephalopathy: Focus on epidemiology and underexplored aspects of etiology. Semin Fetal Neonatal Med. [cited 2025 Oct 28] 26, Available from: https://doi.org/10.1016/j.siny.2021.101265.
Azzopardi, DV, et al. Moderate hypothermia to treat perinatal Asphyxial Encephalopathy. N. Engl. J. Med. 361, 1349–1358.
Ouwehand, S. et al. Predictors of outcomes in hypoxic-ischemic encephalopathy following hypothermia: a meta-Analysis. Neonatology 117, 411–427 (2020).
Novak, I. et al. Early, accurate diagnosis and early intervention in cerebral palsy: advances in diagnosis and treatment. JAMA Pediatr. 171, 897–907 (2017).
Douglas-Escobar, M.V. & Weiss, M.D. Biomarkers of Hypoxic-Ischemic Encephalopathy in Newborns. Front. Neurol. 3, Available from: https://www.frontiersin.org/journals/neurology/articles/10.3389/fneur.2012.00144. (2012).
Morgan, C. et al. Early intervention for children aged 0 to 2 years with or at high risk of cerebral palsy: International Clinical Practice Guideline Based on Systematic Reviews. JAMA Pediatr. 175, 846–858 (2021).
Hayden, J. A., van der Windt, D. A., Cartwright, J. L., Côté, P. & Bombardier, C. Assessing bias in studies of prognostic factors. Ann. Intern Med. 158, 280–286 (2013).
Moons, K. G. M. et al. Critical appraisal and data extraction for systematic reviews of prediction modelling studies: The CHARMS Checklist. PLOS Med. 11, e1001744 (2014).
Hozo, S. P., Djulbegovic, B. & Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 5, 13 (2005).
Wan, X., Wang, W., Liu, J. & Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 14, 135 (2014).
Luo, D., Wan, X., Liu, J. & Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 27, 1785–1805 (2018).
Bartha, A. I. et al. Neonatal Encephalopathy: Association of Cytokines with MR Spectroscopy and Outcome. Pediatr. Res. 56, 960–966 (2004).
Çelik, Y. et al. The effects of selective head cooling versus whole-body cooling on some neural and inflammatory biomarkers: a randomized controlled pilot study. Ital. J. Pediatr. 41, 79 (2015).
Oygür, N., Sönmez, Ö, Saka, O. & Yeǧin, O. Predictive value of plasma and cerebrospinal fluid tumour necrosis factor-α and interleukin-1β concentrations on outcome of full term infants with hypoxic–ischaemic encephalopathy. Arch. Dis. Child - Fetal Neonatal Ed. 79, F190 (1998).
Šumanović-Glamuzina, D., Čulo, F., Čulo, M. I., Konjevoda, P. & Jerković-Raguž, M. A comparison of blood and cerebrospinal fluid cytokines (IL-1β, IL-6, IL-18, TNF-α) in neonates with perinatal hypoxia. Biomol. Biomed. 17, 203–210 (2017).
Chalak, L. F. et al. Biomarkers for Severity of Neonatal Hypoxic-Ischemic Encephalopathy and Outcomes in Newborns Receiving Hypothermia Therapy. J. Pediatr. 164, 468–474.e1 (2014).
Dietrick, B. et al. Plasma and cerebrospinal fluid candidate biomarkers of neonatal encephalopathy severity and neurodevelopmental outcomes. J. Pediatr. 226, 71–79.e5 (2020).
Jenkins, D. D. et al. Serum Cytokines in a Clinical Trial of Hypothermia for Neonatal Hypoxic-Ischemic Encephalopathy. J. Cereb. Blood Flow. Metab. 32, 1888–1896 (2012).
Kelen, D. et al. Serum copeptin and neuron specific enolase are markers of neonatal distress and long-term neurodevelopmental outcome. PLOS One. 12, e0184593 (2017).
Roka, A. et al. Serum S100B and neuron-specific enolase levels in normothermic and hypothermic infants after perinatal asphyxia. Acta Paediatr. 101, 319–323 (2012).
Verdú-Pérez, A. et al. Blood neuronal specific enolase in newborns with perinatal asphyxia. Rev. Neurol. 32, 714–717 (2001).
Thorngren-Jerneck, K., Alling, C., Herbst, A., Amer-WÅhlin, I. & Marsal, K. S100 Protein in serum as a prognostic marker for cerebral injury in term newborn infants with hypoxic ischemic encephalopathy. Pediatr. Res. 55, 406–412 (2004).
Nagdyman, N., Grimmer, I., Scholz, T., Müller, C. & Obladen, M. Predictive value of brain-specific proteins in serum for neurodevelopmental outcome after birth asphyxia. Pediatr. Res. 54, 270–275 (2003).
Wang, Q. L. et al. Effect of Hypothermia on Serum Myelin Basic Protein and Tumor Necrosis Factor–α in Neonatal Hypoxic-Ischemic Encephalopathy. Am. J. Perinatol. 39, 1367–1374 (2021).
Florio, P. et al. Activin A in asphyxiated full-term newborns with hypoxic ischemic encephalopathy. Front. Biosci. (Elite Ed) 2, 36–42 (2010).
Liu, F., Yang, S., Du, Z. & Guo, Z. Dynamic changes of cerebral-specific proteins in full-term newborns with hypoxic–ischemic Encephalopathy. Cell Biochem. Biophys. 66, 389–396 (2013).
Yoneda, S. et al. Low adjusted serum ionized calcium concentration shortly after birth predicts poor outcome in neonatal hypoxic–ischemic encephalopathy. J. Obstet. Gynaecol. Res. 31, 57–64 (2005).
Basu, P., Som, S., Choudhuri, N. & Das, H. Contribution of the blood glucose level in perinatal asphyxia. Eur. J. Pediatr. 168, 833–838 (2009).
Basu, S. K., Salemi, J. L., Gunn, A. J. & Kaiser, J. R. Hyperglycaemia in infants with hypoxic–ischaemic encephalopathy is associated with improved outcomes after therapeutic hypothermia: a post hoc analysis of the CoolCap Study. Arch. Dis. Child - Fetal Neonatal Ed. 102, F299 (2017).
Nadeem, M., Murray, D. M., Boylan, G. B., Dempsey, E. M. & Ryan, C. A. Early blood glucose profile and neurodevelopmental outcome at two years in neonatal hypoxic-ischaemic encephalopathy. BMC Pediatr. 11, 10 (2011).
Aly, H., Khashaba, M. T., El-Ayouty, M., El-Sayed, O. & Hasanein, B. M. IL-1β, IL-6 and TNF-α and outcomes of neonatal hypoxic ischemic encephalopathy. Brain Dev. 28, 178–182 (2006).
Shang, Y. et al. Clinical significance of interleukin‑6, tumor necrosis factor‑α and high‑sensitivity C‑reactive protein in neonates with hypoxic‑ischemic encephalopathy. Exp. Ther. Med. 8, 1259–1262 (2014).
Silveira, R. C. & Procianoy, R. S. Interleukin-6 and tumor necrosis factor-α levels in plasma and cerebrospinal fluid of term newborn infants with hypoxic–ischemic encephalopathy. J. Pediatr. 143, 625–629 (2003).
Tekgul, H. et al. Value of biochemical markers for outcome in term infants with asphyxia. Pediatr. Neurol. 31, 326–332 (2004).
Beken, S. et al. Can biochemical markers predict the severity of hypoxic-ischemic encephalopathy? Turk. J. Pediatr. 56, 62–68 (2014).
Shah, P., Riphagen, S., Beyene, J. & Perlman, M. Multiorgan dysfunction in infants with post-asphyxial hypoxic-ischaemic encephalopathy. Arch. Dis. Child - Fetal Neonatal Ed. 89, F152 (2004).
Simovic, A. M. et al. Predictive value of biochemical, echocardiographic and electrocardiographic markers in non-surviving and surviving asphyxiated full-term newborns. Turk. J. Pediatr. 56, 243–249 (2014).
Radford, S. Blood hyperlactaemia as a predictor of morbidity and mortality in infants with hypoxic ischaemic encephalopathy; Abstract 057. J. Matern. Fetal Neonatal. Med. 29, (2016).
Karlsson, M. et al. Lactate dehydrogenase predicts hypoxic ischaemic encephalopathy in newborn infants: a preliminary study. Acta Paediatr. 99, 1139–1144 (2010).
Thoresen, M. et al. Lactate dehydrogenase in hypothermia-treated newborn infants with hypoxic-ischaemic encephalopathy. Acta Paediatr. 101, 1038–1044 (2012).
Yum, S. K., Moon, C. J., Youn, Y. A. & Sung, I. K. Changes in lactate dehydrogenase are associated with central gray matter lesions in newborns with hypoxic-ischemic encephalopathy. J. Matern Fetal Neonatal Med. 30, 1177–1181 (2017).
Boskabadi, H. et al. Nucleated red blood cells count as a prognostic biomarker in predicting the complications of asphyxia in neonates. J. Matern Fetal Neonatal Med. 30, 2551–2556 (2017).
Walsh, B.H. et al. Cord blood proteins and multichannel-electroencephalography in hypoxic-ischemic encephalopathy*. Pediatr. Crit. Care Med. 14, Available from: https://journals.lww.com/pccmjournal/fulltext/2013/07000/cord_blood_proteins_and.8.aspx (2013).
Montaldo, P., Rosso, R., Chello, G. & Giliberti, P. Cardiac troponin I concentrations as a marker of neurodevelopmental outcome at 18 months in newborns with perinatal asphyxia. J. Perinatol. 34, 292–295 (2014).
Shastri, A. T., Samarasekara, S., Muniraman, H. & Clarke, P. Cardiac troponin I concentrations in neonates with hypoxic-ischaemic encephalopathy. Acta Paediatr. 101, 26–29 (2012).
Davidson, J. O., Gonzalez, F., Gressens, P. & Gunn, A. J. Update on mechanisms of the pathophysiology of neonatal encephalopathy. Unanswer. Quest. Neonates NE Treat. Hypotherm. 26, 101267 (2021).
Mochetti, M. M. et al. Neuron-specific enolase at admission as a predictor for stroke volume, severity and outcome in ischemic stroke patients: a prognostic biomarker review. Sci. Rep. 14, 2688 (2024).
Ramaswamy, V. et al. Systematic Review of Biomarkers of Brain Injury in Term Neonatal Encephalopathy. Pediatr. Neurol. 40, 215–226 (2009).
Altman, D. G. & Simera, I. A history of the evolution of guidelines for reporting medical research: the long road to the EQUATOR Network. J. R. Soc. Med. 109, 67–77 (2016).
O’Bryant, S. E. et al. Guidelines for the standardization of preanalytic variables for blood-based biomarker studies in Alzheimer’s disease research. Alzheimer's Dement. 11, 549–560 (2015).
Aziz, N. et al. Biological variation of immunological blood biomarkers in healthy individuals and quality goals for biomarker tests. BMC Immunol. 20, 33 (2019).
Foroutan, F. et al. GRADE Guidelines 28: Use of GRADE for the assessment of evidence about prognostic factors: rating certainty in identification of groups of patients with different absolute risks. J. Clin. Epidemiol. 121, 62–70 (2020).
Quirke, F. A. et al. COHESION: a core outcome set for the treatment of neonatal encephalopathy. Pediatr. Res. 95, 922–930 (2024).
Funding
This research was funded by a grant from the Health Research Board of Ireland. Neonatal Brain Injury Consortium Ireland; CDA-2018-008. Open Access funding provided by the IReL Consortium.
Author information
Authors and Affiliations
Contributions
Mary O’Dea: co-first author for manuscript. Tim Hurley: co-first author for manuscript. Aoife Branagan: assisted with research for paper. Robert McCarthy: editing and preparation for submission. Philip Stewart: assisted with research for the paper. Sean Tamgumus: assisted with research for paper, provided feedback for edits. Kasper Jacobsen Kyng: assisted with research for paper, provided feedback for edits. David Mockler: assisted with library search for papers and methodology. Lina Chalak: assisted with research for paper, provided feedback for edits. Eleanor J Molloy: primary supervisor.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
O’Dea, M., Hurley, T., Branagan, A. et al. Neonatal Encephalopathy biomarkers: outcome prediction from blood samples: systematic review and meta-analysis. Pediatr Res (2026). https://doi.org/10.1038/s41390-026-04924-6
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41390-026-04924-6
