
Abstract
Pulmonary arterial hypertension (PAH) has a poor prognosis despite available treatments. TPN171H, structurally modified from traditional Chinese medicine (Epimedium), was reported to have a high affinity for phosphodiesterase type 5 and exhibited anti-inflammatory and vasodilatory effects in preclinical studies. This phase 2a randomized trial (NCT04483115) evaluated the hemodynamic effects and safety of TPN171H in PAH. Sixty patients with PAH were randomly assigned to receive placebo, TPN171H (2.5, 5, or 10 mg) or tadalafil (20 or 40 mg) and evaluated for hemodynamic changes for 24 h. The primary endpoint was the maximum change (%) in pulmonary vascular resistance (PVR) from baseline. The key secondary endpoint was the change (%) in PVR to systemic vascular resistance (SVR) ratio at each observation point from baseline. Compared to the placebo group, the least square mean differences in the maximum change in PVR were −16.8% (95% CI, −29.1 to −4.5, p = 0.008) in TPN171H 5 mg, −15.4% (95% CI, −28.2 to −2.7, p = 0.019) in tadalafil 20 mg, and −13.3% (95% CI, −25.6 to −0.9, p = 0.036) in the tadalafil 40 mg group. Moreover, TPN171H 5 mg, but none of the tadalafil doses, showed a significant reduction in PVR/SVR ratio at 2 h (p = 0.026), 3 h (p = 0.030), and 5 h (p = 0.046) compared to the placebo group. No serious adverse events occurred. TPN171H 5 mg demonstrated favorable acute hemodynamic effects and an acceptable short-term safety profile in this exploratory trial, supporting further evaluation in adequately powered trials.
Similar content being viewed by others
Introduction
Pulmonary arterial hypertension (PAH) is a life-threatening disorder characterized by progressive pulmonary vascular remodeling, leading to increased pulmonary vascular resistance (PVR) and right ventricular afterload, which ultimately culminates in right heart failure and premature death.1,2 Over the past two decades, the approval of therapies targeting the prostacyclin, endothelin-1, and nitric oxide pathways has improved patient outcomes by alleviating symptoms and slowing disease progression.3,4 More recently, sotatercept, a first-in-class fusion protein acting as a ligand trap for transforming growth factor-β superfamily members, has introduced a paradigm shift by addressing underlying vascular remodeling.5 Despite these advances, PAH remains incurable. Mortality rates are still unacceptably high, and many patients experience diminished treatment response or significant side effects over time.6 Consequently, a considerable unmet medical need persists for novel therapeutic agents with improved efficacy and safety profiles.
Traditional Chinese medicine has gained substantial recognition globally as a potential source of novel therapeutics. As a major subdiscipline of complementary medicine, traditional Chinese medicine offers a rich pharmacopeia honed over millennia. A growing body of evidence suggests that traditional Chinese medicine formulations and their isolated active compounds may supplement current therapies for various cardiovascular diseases, including chronic heart failure, acute myocardial infarction, and hypertension, often through pleiotropic mechanisms involving anti-inflammatory, antioxidant, and anti-apoptotic effects.7,8,9 This expanding interest underscores the potential of traditional Chinese medicine to provide innovative solutions for complex cardiovascular disorders where conventional treatments fall short.
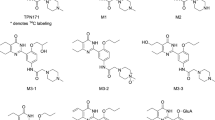
TPN171H is a promising new chemical entity developed from this lineage. It is a structurally modified derivative of an active ingredient originally isolated from Epimedium, an herb with a long history of medicinal use in China, first documented in the Divine Farmer’s Classic of Materia Medica (circa A.D. 200–210).10 Traditionally classified as a kidney Yang tonic and prescribed for male sexual dysfunction, Epimedium has now been repositioned into cardiovascular medicine through modern pharmacological research. Preclinical studies have demonstrated that TPN171H is a highly potent and selective phosphodiesterase type 5 (PDE5) inhibitor, exhibiting a selectivity profile superior to that of established agents like tadalafil and sildenafil. Functionally, it has shown robust capacity to decrease right ventricular systolic pressure and alleviate pulmonary arterial remodeling in animal models of pulmonary hypertension.11 Building on these findings, a phase 1 study confirmed that TPN171H is safe, well-tolerated, and exhibits a favorable pharmacokinetic profile in healthy subjects, providing a clear rationale for its advancement into patient populations.12
Based on this foundation of preclinical efficacy and phase 1 safety data, we initiated the present phase 2a clinical trial, designed to bridge the gap between preclinical promise and clinical application by evaluating the acute hemodynamic effects and safety of a single oral dose of TPN171H in patients with PAH. This investigation is particularly important as it represents the first clinical evaluation of a novel PDE5 inhibitor derived from a traditional Chinese medicinal herb in PAH patients. A successful outcome could not only validate TPN171H as an effective and safe treatment option but also pave the way for further drug development from traditional Chinese medicine sources, ultimately addressing the persistent unmet medical need in the management of this devastating disease.
Results
Patients
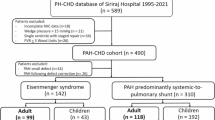
From November 19, 2020, to July 3, 2022, we screened 91 patients, of whom 60 were equally randomized into six groups receiving placebo, TPN171H 2.5 mg, TPN171H 5 mg, TPN171H 10 mg, tadalafil 20 mg, and tadalafil 40 mg (10 patients in each group) (Fig. 1). Demographic and baseline clinical characteristics did not differ significantly among the six groups (Table 1). The mean age was 34.0 years, and 83.3% were female. Idiopathic PAH was the most common etiology (53.3%). The mean pulmonary arterial pressure and PVR were 56.1 mmHg and 13.5 Wood units, respectively.

Patient selection, randomization, and flow through the trial. A total of 91 patients were screened, of whom 60 were enrolled and equally randomized into six groups receiving placebo, TPN171H 2.5 mg, TPN171H 5 mg, TPN171H 10 mg, tadalafil 20 mg and tadalafil 40 mg (ten patients in each group). APVT acute pulmonary vasoreactivity testing, CHD congenital heart disease, FEV1 forced expiratory volume in 1 s; FVC forced vital capacity, mPAP mean pulmonary arterial pressure; PAH pulmonary arterial hypertension, PAWP pulmonary artery wedge pressure, PH pulmonary hypertension
Primary endpoint
From baseline to 24 h, the maximum percentage changes in PVR were a decrease of 38.4 ± 11.3%, 40.1 ± 13.7%, 33.6 ± 13.9%, 42.8 ± 20.0%, 33.4 ± 18.9%, and 23.0 ± 15.9% in the groups with TPN171H 2.5 mg, TPN171H 5 mg, TPN171H 10 mg, tadalafil 20 mg, tadalafil 40 mg, and placebo, respectively. The median time to achieve the maximum change in PVR was 1.93 h (interquartile range [IQR], 1.48–5.94), 4.92 h (IQR, 2.98–7.96), 3.98 h (IQR, 1.97–8.00), 8.93 h (IQR, 4.03–9.95), 1.79 h (IQR, 1.47–5.96), and 2.93 h (IQR, 2.01–9.99) in the groups treated with TPN171H 2.5 mg, 5 mg, 10 mg, tadalafil 20 mg, 40 mg, and placebo, respectively.
In comparison to the placebo group, the groups with TPN171H 5 mg, tadalafil 20 mg and tadalafil 40 mg showed a least-squares mean difference (LSMD) in PVR of −16.8% (95% confidence interval [CI], −29.1 to −4.5; p = 0.008), −15.4% (95% CI, −28.2 to −2.7; p = 0.019), and −13.3% (95% CI, −25.6 to −0.9; p = 0.036), respectively. The maximum percentage changes in PVR of the TPN171H 2.5 and 10 mg groups did not differ significantly compared to the placebo group (Fig. 2 and Supplementary Table 1). Individual PVR maximum percentage changes are shown in Supplementary Fig. 1.

Maximum change in PVR from baseline to 24 h. Mean maximum changes (in %) from baseline to 24 h in PVR in each group. Compared to the placebo group, the least-squares mean differences were −16.8% (95% CI, −29.1 to −4.5, p = 0.008), −15.4% (95% CI, −28.2 to −2.7, p = 0.019) and −13.3% (95% CI, −25.6 to −0.9, p = 0.036) in the TPN171H 5 mg, Tadalafil 20 mg, and Tadalafil 40 mg groups, respectively. The maximum changes in PVR of the TPN171H 2.5 and 10 mg groups did not differ significantly from the placebo group. An analysis of covariance model was used, with the maximum change in pulmonary vascular resistance as a percentage from baseline as the dependent variable, treatment as a fixed effect, and baseline pulmonary vascular resistance as a covariate. PVR pulmonary vascular resistance
Secondary endpoints
The TPN171H 5 mg, tadalafil 20 mg, and tadalafil 40 mg groups, with a significant difference in the primary endpoint from the placebo group, were further analyzed for secondary endpoints. The LSMDs in the percentage change of PVR to systemic vascular resistance ratio (PVR/SVR) between the TPN171H 5 mg and placebo groups were −20.5% (95% CI, −38.4 to −2.5; p = 0.026) at 2 h, −19.1% (95% CI, −36.3 to −1.9; p = 0.030) at 3 h, and −14.9% (95% CI, −29.6 to −0.3; p = 0.046) at 5 h. The percentage changes in PVR/SVR did not differ significantly at other time points between the TPN171H 5 mg group and the placebo group. The changes in PVR/SVR did not differ significantly at any time point between the tadalafil groups and the placebo group (Fig. 3). Over the entire 24-h period, the TPN171H 5 mg group showed a numerically pronounced negative trend with a placebo-adjusted area under the curve (AUC)PVR/SVR of −1.07 (95% CI, −2.83 to 0.70) h·ratio, compared to 0.40 (95% CI, −1.38 to 2.17) h·ratio for the tadalafil 20 mg group and −0.42 (95% CI, −2.21 to 1.37) h·ratio for the tadalafil 40 mg group (Supplementary Table 2).

Percentage change in PVR/SVR from baseline to 24 h. The least-squares mean differences in the percentage change in the PVR/SVR ratio between the TPN171H 5 mg and placebo groups were −20.5% (95% CI, −38.4 to −2.5; p = 0.026) at 2 h, −19.1% (95% CI, −36.3 to −1.9; p = 0.030) at 3 h, and −14.9% (95% CI, −29.6 to −0.3; p = 0.046) at 5 h. *p < 0.05 refers to comparisons between the TPN171H 5 mg and the placebo groups. Analysis of the mixed model repeated-measures method was used, with the change in PVR/SVR ratio (%) from baseline as the dependent variable, with treatment, hours of observation, and treatment-by-hour interaction as fixed effects, and the baseline PVR/SVR ratio as a covariate. PVR pulmonary vascular resistance, SVR systemic vascular resistance
The LSMDs of the maximum percentage changes in SVR were −14.2% (95% CI, −25.3 to −3.1, p = 0.013) in the tadalafil 20 mg group and −12.1% (95% CI, −22.8 to −1.4, p = 0.027) in the tadalafil 40 mg group compared to the placebo group. The maximum changes in SVR of the TPN171H 5 mg group did not differ significantly from the placebo group (LSMD −8.7%, 95% CI [−19.4 to 2.0], p = 0.107).
The LSMD of the maximum percentage changes in mean pulmonary arterial pressure was −10.2% (95% CI, −17.8 to −2.5, p = 0.011) between the TPN171H 5 mg and placebo groups. The maximum changes in the mean pulmonary arterial pressure of the two tadalafil groups did not differ significantly from those of the placebo group.
The LSMDs of the maximum changes in mixed venous oxygen saturation were 10.5% (95% CI, 0.9 to 20.2, p = 0.032) in the TPN171H 5 mg group and 12.9% (95% CI, 3.4 to 22.4, p = 0.009) in the tadalafil 20 mg group compared to the placebo group. The maximum changes in mixed venous oxygen saturation of the tadalafil 40 mg group did not differ significantly from those of the placebo group.
The LSMD of the maximum percentage change in the cardiac index was 37.8% (95% CI, 10.4 to 65.2, p = 0.008) in the tadalafil 20 mg group compared to the placebo group. The maximum changes in the cardiac index of the TPN171H 5 mg and tadalafil 40 mg groups did not differ significantly from those of the placebo group (Table 2).
Exploratory endpoints
Pharmacokinetic parameters for the different TPN171H doses are summarized in Supplementary Table 3. The time to maximum plasma concentration (Tmax) was 1.51 h for the 2.5 mg dose, 2.48 h for the 5 mg dose, and 1.26 h for the 10 mg dose. The mean maximum plasma concentration (Cmax) was 11.8 ± 4.3 ng/mL, 27.8 ± 5.6 ng/mL, and 68.2 ± 41.8 ng/mL in the 2.5, 5, and 10 mg groups, respectively. Correspondingly, the area under the plasma concentration-time curve from time 0 to time point t (AUC0-t) was 112.1 ± 33.5, 264.7 ± 85.2, and 499.0 ± 194.3 h·ng/mL for the 2.5, 5, and 10 mg groups, respectively.
Safety endpoints
A total of 65 adverse events occurred in 28 patients (46.7%) in all study groups. Common adverse events in the TPN171H group included vomiting, headache, dysuria, flushing, hypokalemia, and elevated blood bilirubin (Table 3). All these adverse events were mild-to-moderate, and no serious adverse events occurred during the observation period.
Discussion
In this exploratory, phase 2a trial, a single oral intake of TPN171H 5 mg led to a reduction in PVR in patients with PAH, and TPN171H tended to have good selectivity for pulmonary circulation, reflected by a significant reduction in the PVR/SVR ratio. No serious adverse events occurred. These findings inform the design of subsequent phase 2b/3 efficacy trials.
Epimedium plays a significant role in traditional Chinese medicine, known for its roles in boosting Yang energy, fortifying tendons, and alleviating rheumatic conditions. Clinically, it is often prescribed for male sexual dysfunctions such as impotence and premature ejaculation, as well as urinary incontinence and female infertility.13 TPN171H, structurally modified from the natural ingredient of Epimedium, was proven to have a higher PDE5 selectivity than tadalafil and sildenafil in preclinical studies.11 Its half-life ranges from 8-11 hours, allowing for once daily administration. Among the three TPN171H dosage groups evaluated in this study, a significant reduction in PVR was observed only in the 5 mg group compared with the placebo group (LSMD −16.82%), while the effect was attenuated in the 10 mg group (LSMD −7.36%). This nonlinear dose-response profile might be explained by distinct effect kinetics and pharmacokinetic variability, as well as the small sample size. First, the 5 mg dose produced the latest peak hemodynamic effect (~4.92 h), suggesting more favorable distribution or target engagement kinetics that contributed to a sharper and greater peak response. In contrast, despite achieving higher systemic exposure, the 10 mg dose elicited an earlier peak effect, which may reflect a shift in its mechanism of action (e.g., rapid saturation triggering counter-regulatory responses14). Second, the 10 mg dose was associated with >3-fold higher inter-individual variability in peak concentration (coefficient of variation of Cmax ~61% vs. ~20% for 5 mg), accounting for its inconsistent pharmacodynamic response. Accordingly, individual PVR maximum changes (Supplementary Fig. 1) demonstrated a consistent response profile in the 5 mg group, whereas the 10 mg group showed scattered and heterogeneous responses. Lastly, the larger effect in the 5 mg dose group than in the other dose groups might be due to random error. Together, these integrated pharmacokinetic-pharmacodynamic findings provide a critical foundation for dose selection in subsequent clinical trials.
Tadalafil, one of the widely used PDE5 inhibitors for the treatment of patients with PAH,15,16,17 was included as an active-controlled group in this study, and both the 20 and 40 mg tadalafil groups showed significantly decreased PVR in patients with PAH compared with the placebo group, which was in line with a previous acute hemodynamic study.18 However, given the purpose of exploring the effect of TPN171H on acute hemodynamics in patients with PAH, rather than a superior or noninferior design to conventional PDE5 inhibitors, we made no direct comparison between the TPN171H and tadalafil groups. Further studies are needed to compare the efficacy and safety of TPN171H to tadalafil or other PDE5 inhibitors.
Pulmonary circulation selectivity is an important index for evaluating ideal vasodilators for the treatment of PAH, which can be reflected by the change in the PVR/SVR ratio.18,19 A previous study investigating the acute hemodynamic impact of conventional PDE5 inhibitors in patients with PAH indicated that sildenafil and tadalafil, but not vardenafil, showed good pulmonary circulation selectivity, reflected by a significant reduction in the PVR/SVR ratio.18 In this study, compared with the placebo group, the TPN171H 5 mg group showed a significant reduction in PVR/SVR at 2, 3, and 5 h after medication. Additionally, the maximum changes in SVR in the TPN171H 5-mg group did not differ significantly from those in the placebo group. All these data indicated good pulmonary circulation selectivity of TPN171H. In contrast, different from a previous study,18 both tadalafil dosages significantly reduced SVR but did not show significant differences in the change in PVR/SVR compared with the placebo group. This may be ascribed to the small sample size of the previous study and ours.18 Another important reason was the placebo-controlled design in this study, and the LSMDs adjusted by the placebo group were calculated, which contributed to more reliable results.
For other hemodynamic parameters, TPN171H 5 mg was associated with a decrease in mean pulmonary arterial pressure and an increase in mixed venous oxygen saturation, but no difference in cardiac index compared to placebo. This pattern might indicate that the reduction in PVR in this acute setting is afterload reduction, specifically by lowering the pressure against which the right ventricle must eject. The fact that the cardiac index did not rise concomitantly might suggest that, after a single dose, the reduction in right ventricular afterload was not immediately translated into a measurable increase in forward flow under the conditions of this short-term study. Whether sustained afterload reduction through multiple dosing can lead to improved right ventricular function and a consequent increase in cardiac output over the long term remains to be established in further multiple-dose trials.
As an exploratory phase 2a study, the present trial was designed to characterize the acute hemodynamic impact of a single oral dose of TPN171H in patients with PAH. The observed reductions in PVR and the PVR/SVR ratio provided direct evidence of its pulmonary vasodilatory activity and selectivity. While these acute improvements do not in themselves establish long-term clinical benefit, they represent the essential pharmacodynamic foundation upon which sustained therapeutic efficacy and improved clinical outcomes are built. Importantly, the integrated pharmacokinetic and pharmacodynamic data from this acute study, particularly the identification of 5 mg as the dose with optimal efficacy and consistency, offer a critical rationale for dose selection in subsequent clinical development. Future studies investigating the effects of multiple-dose administration of TPN171H on exercise capacity, functional class, and long-term outcomes are therefore warranted and will be informed by the acute hemodynamic profile established here.
Notably, this study enrolled a relatively young cohort (mean age 34 years) composed predominantly of females with idiopathic PAH, which might limit the extrapolation of our findings to older patients, those with comorbidities, or populations with a different etiologic distribution. Furthermore, since the trial was conducted in patients without background therapy to evaluate the intrinsic hemodynamic effect of TPN171H, our results do not address its efficacy or safety in patients already receiving background therapy for PAH. Therefore, further studies in broader populations, including patients on background therapy for PAH, are warranted to confirm the generalizability of the hemodynamic response observed here.
There are eleven subfamilies of human PDEs (PDE1-11), possessing a conserved C-terminal catalytic domain for hydrolysis of the ubiquitous second messenger.20 High selectivity is thus crucial, and inhibition of PDE isozymes other than PDE5 may lead to other adverse effects. Studies found similar adverse events among available PDE5 inhibitors, including sildenafil, tadalafil, and vardenafil, including headache, flushing, dyspepsia, visual disturbance, nasal congestion, back pain, myalgia, nausea, and dizziness, considered due to their selectivity of various PDE subgroups. A preclinical study showed that TPN171H showed better potency and selectivity than sildenafil and tadalafil.11 The present study also found a favorable safety profile of TPN171H, and even a single dose of 10 mg could be well tolerated. All adverse events were mild-to-moderate, and no serious adverse events occurred during the trial. However, due to the single-dose administration design, more information on the adverse events of TPN171H with multiple administrations needs to be observed in further studies.
This study has several limitations. First, as an exploratory, single-dose, acute hemodynamic study, it was designed to establish a proof-of-mechanism and guide dose selection. These short-term findings do not establish the long-term clinical efficacy or safety of TPN171H, which must be evaluated in future multiple-dose trials assessing functional capacity and clinical outcomes. Second, the study exclusively enrolled patients who were not receiving any background PAH-targeted therapy. Consequently, the findings do not support conclusions regarding the efficacy or safety of TPN171H when used in combination with existing PAH drugs. Further trials are warranted to evaluate its role as an add-on therapy in patients already receiving approved PAH treatment. Third, the sample size was small in each group, which was partly because no previous example for sample size calculation could be referred to for this exploratory acute hemodynamic study with multiple-dose groups. Nevertheless, the efficacy of the TPN171H 5 mg group with respect to the primary and secondary endpoints provided sufficient data for further trial development. Fourth, differences in efficacy and safety between TPN171H and tadalafil were not established in this study.
In conclusion, TPN171H 5 mg demonstrated favorable acute hemodynamic effects and an acceptable short-term safety profile in this exploratory phase 2a study, supporting further evaluation in longer-term, adequately powered trials.
Materials and methods
Study design and oversight
The trial was registered at ClinicalTrials.gov (NCT04483115) before initiation and conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. Written informed consent was obtained from all subjects prior to participation, and the protocol was approved by the ethics committees of the lead institutions (Peking University First Hospital [Ethics number: 2020009] and Peking Union Medical College Hospital [Ethics number: KS2020263]), as well as each participating center.
We conducted this randomized, double-blind, placebo- and active-controlled phase 2a trial at 7 pulmonary hypertension referral centers in China. This was an exploratory, acute hemodynamic study designed to establish a proof-of-mechanism and to inform dose selection for the design of subsequent phase 2b/3 trials. The study was designed by the steering committee in collaboration with the sponsor (Vigonvita Life Sciences Co., Ltd., China), as detailed in the supplementary materials. The steering committee had access to the complete database.
Selection of patients
Eligibility criteria included the following: (1) age 18 to 75 years; (2) the etiology was idiopathic or hereditary or associated with connective tissue disease or corrected congenital heart disease, drug use or toxin exposure; and (3) World Health Organization (WHO) functional class II or III. The diagnosis of PAH was confirmed with right heart catheterization. Patients were excluded if they were responders at acute pulmonary vasoreactivity testing or had received any treatment for PAH within 1 month before study entry, based on the patient’s existing treatment status; no washout of ongoing PAH-targeted therapy for the purpose of eligibility was allowed. Concomitant basic treatments for PAH, such as anticoagulants, diuretics, digoxin, and oxygen therapy, were permitted in this study. These regimens were required to be stable for at least 2 weeks before randomization and were maintained unchanged throughout the study period. A full list of inclusion and exclusion criteria is provided in the supplementary materials.
Procedures
Right heart catheterization and acute pulmonary vasoreactivity testing were performed in patients potentially eligible for trial participation after initial screening. Patients who met the hemodynamic criteria of precapillary pulmonary hypertension (mean pulmonary arterial pressure ≥25 mmHg, pulmonary artery wedge pressure ≤15 mmHg and PVR >3 Wood U at rest) and nonresponders at vasoreactivity testing were finally included in the trial. After insertion of a Swan-Ganz catheter followed by a 120-min washout period, eligible patients were randomly assigned in a 1:1:1:1:1:1 ratio to one of the six treatment groups: placebo, TPN171H (2.5, 5, or 10 mg) or tadalafil (20 or 40 mg). Randomization was performed using a centralized interactive web-response system (Clinflash IRT, Tigermed), which implemented a block randomization scheme (with an undisclosed block size) to ensure balanced allocation throughout the trial. No stratification was used when generating the randomization list. The investigators, patients, site staff, and sponsor personnel involved in the study conduct and data analysis remained blinded to the treatment assignments until the final unblinding after the database was locked. Following oral medication, hemodynamic changes were subsequently observed for 24 h (Supplementary Fig. 2). Adverse events and laboratory results were recorded throughout the observation period. Upon completion of the study, all patients were initiated on guideline-recommended drugs approved for PAH. The methods for catheterization, vasoreactivity testing, and hemodynamic monitoring are provided in the supplementary materials.
Endpoints
The primary endpoint was the maximum change (%) in PVR from baseline to 24 h. The key secondary endpoint was the change (%) in PVR/SVR from baseline at each time point shown in Supplementary Fig. 2. Other secondary endpoints included the maximum changes (%) from baseline to 24 hours in mean pulmonary arterial pressure, mixed venous oxygen saturation, SVR, and cardiac index. Exploratory endpoints were pharmacokinetic parameters, including Cmax, Tmax, AUC0-t, elimination half-life (t1/2), apparent clearance (CL/F), apparent volume of distribution (Vz/F), and elimination rate constant (λz). The safety endpoints included all adverse events and abnormal laboratory test results that started or worsened from the time of administration of the study drug until the end of the observation period.
Statistical analysis
This trial was designed to provide meaningful acute hemodynamic effect data to support design decisions for future trials. Therefore, no sample size calculations were performed. Continuous variables are expressed as the mean ± standard deviation or median (IQR), and categorical variables are expressed as numbers (%). All efficacy and safety analyses were performed in the intention-to-treat population, which included all the patients who underwent randomization and were based on the observed data set without imputation for missing values.
For analysis of the primary endpoint, the analysis of covariance (ANCOVA) model was used to evaluate the difference between each treatment group (TPN171H 2.5, 5, or 10 mg, or tadalafil 20 or 40 mg) and the placebo group in maximum change (%) in PVR from baseline. The model took the maximum change (%) in PVR from baseline as the dependent variable, treatment as a fixed effect, and baseline PVR as a covariate, from which the adjusted LSMDs between the two groups, together with their 95% CIs, were calculated. If the result for the primary endpoint was significant, secondary endpoints were evaluated.
For analysis of the key secondary endpoint, the mixed model repeated-measures method was used to evaluate the LSMDs in the PVR/SVR ratio between each treatment group (TPN171H 5 mg, or tadalafil 20 or 40 mg) and the placebo group at each time point. The model included the change in PVR/SVR ratio (%) from baseline as the dependent variable, with treatment, hours of observation, and treatment-by-hour interaction as fixed effects, and baseline PVR/SVR ratio as a covariate and subject as a random effect, from which the adjusted LSMDs between the two groups together with their 95% CIs were calculated. Other secondary endpoints included the maximum percentage changes in mean pulmonary arterial pressure, mixed venous oxygen saturation, SVR, and cardiac index, which were analyzed with ANCOVA. Safety endpoints were evaluated descriptively.
All statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, NC). A two-sided p value of <0.05 was considered statistically significant.
Data availability
The protocol, statistical analysis plan, and other relevant study materials are publicly available online. Deidentified participant data generated and analyzed during the current study are available in figshare with the identifier (10.6084/m9.figshare.31289446).
References
Humbert, M. et al. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Respir. J. 61, 2200879 (2023).
Hassoun, P. M. Pulmonary arterial hypertension. N. Engl. J. Med. 385, 2361–2376 (2021).
Mocumbi, A. et al. Pulmonary hypertension. Nat. Rev. Dis. Prim. 10, 1 (2024).
Zhang, R. et al. Survival of Chinese patients with pulmonary arterial hypertension in the modern treatment era. Chest 140, 301–309 (2011).
Hoeper, M. M. et al. Phase 3 trial of sotatercept for treatment of pulmonary arterial hypertension. N. Engl. J. Med. 388, 1478–1490 (2023).
Global, regional, and national burden of pulmonary arterial hypertension, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Respir. Med. 13, 69–79 (2025).
Cheang, I. et al. The traditional Chinese medicine Qiliqiangxin in heart failure with reduced ejection fraction: a randomized, double-blind, placebo-controlled trial. Nat. Med. 30, 2295–2302 (2024).
Yang, Y. et al. Traditional Chinese medicine compound (Tongxinluo) and clinical outcomes of patients with acute myocardial infarction: the CTS-AMI Randomized clinical trial. JAMA 330, 1534–1545 (2023).
Hao, P. et al. Traditional Chinese medicine for cardiovascular disease: evidence and potential mechanisms. J. Am. Coll. Cardiol. 69, 2952–2966 (2017).
Wang, G. et al. Design, synthesis, and pharmacological evaluation of monocyclic pyrimidinones as novel inhibitors of PDE5. J. Med. Chem. 55, 10540–10550 (2012).
Zhao, C. et al. TPN171H alleviates pulmonary hypertension via inhibiting inflammation in hypoxia and monocrotaline-induced rats. Vasc. Pharm. 145, 107017 (2022).
Qian, H. et al. A phase I study to evaluate the safety, tolerability, and pharmacokinetics of TPN171H, a novel phosphodiesterase type 5 inhibitor, in healthy subjects. Drug Des. Devel. Ther. 15, 2947–2959 (2021).
Wang, S. et al. Epimedium and its chemical constituents in cancer treatment: a comprehensive review of traditional applications, antitumor effects, pharmacokinetics, delivery systems, and toxicology. J. Ethnopharmacol. 347, 119738 (2025).
Kenakin, T. P. Pharmacology in Drug Discovery and Development (Academic Press, 2017).
Galiè, N. et al. Initial use of ambrisentan plus tadalafil in pulmonary arterial hypertension. N. Engl. J. Med. 373, 834–844 (2015).
Grünig, E. et al. Randomized trial of macitentan/tadalafil single-tablet combination therapy for pulmonary arterial hypertension. J. Am. Coll. Cardiol. 83, 473–484 (2024).
Galiè, N. et al. Tadalafil therapy for pulmonary arterial hypertension. Circulation 119, 2894–2903 (2009).
Ghofrani, H. A. et al. Differences in hemodynamic and oxygenation responses to three different phosphodiesterase-5 inhibitors in patients with pulmonary arterial hypertension: a randomized prospective study. J. Am. Coll. Cardiol. 44, 1488–1496 (2004).
Grimminger, F. et al. First acute haemodynamic study of soluble guanylate cyclase stimulator riociguat in pulmonary hypertension. Eur. Respir. J. 33, 785–792 (2009).
Nemr, M. T. M., Abdelaziz, M. A., Teleb, M., Elmasry, A. E. & Elshaier, Y. An overview on pharmaceutical applications of phosphodiesterase enzyme 5 (PDE5) inhibitors. Mol. Divers 29, 4765–4785 (2024).
Acknowledgements
The authors express their gratitude to all patients, their families, and the investigators who participated in the study. This trial is sponsored by Vigonvita Life Sciences Co., Ltd., China, and funded by the Noncommunicable Chronic Diseases-National Science and Technology Major Project (2024ZD0526700).
Author information
Authors and Affiliations
Contributions
Zhi-Cheng Jing, Yong Huo, Yu-Ping Zhou, Lu-Hong Qiu, and Wei Ma contributed to the conception and design of the study. Yu-Ping Zhou, Wei Ma, Yun-Shan Cao, Jiang Li, Wei Huang, Lan Wang, and Dao-Wen Wang provided study materials or recruited patients and collected the data. Yu-Ping Zhou, Lu-Hong Qiu, Wei Ma, Hua-Qing Duan, and Zhen Wang were involved in data collection and assembly. Yu-Ping Zhou, Lu-Hong Qiu, Yong Huo, Xi-Qi Xu, Xin Jiang, Wei-Guo Ma, and Zhi-Cheng Jing contributed to data analysis and interpretation. All authors have read and approved the article.
Corresponding authors
Ethics declarations
Competing interests
Hua-Qing Duan is employed by Vigonvita Life Sciences Co., Ltd., and the other authors have no conflicts of interest to disclose.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhou, YP., Qiu, LH., Ma, W. et al. Acute hemodynamic effects of TPN171H in pulmonary arterial hypertension: a randomized, controlled, phase 2a trial. Sig Transduct Target Ther 11, 171 (2026). https://doi.org/10.1038/s41392-026-02686-5
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41392-026-02686-5
