
Abstract
Study design
Guidelines update.
Objectives
To provide management recommendations and strategies for cognitive impairment (CI) in people with spinal cord injury (SCI) for healthcare professionals (HCPs).
Setting
SCI Units, NSW, Australia.
Methods
The development encompassed multiple stages, commencing with establishment of the multidisciplinary advisory committee, followed by expert consultations. A rapid review and e-Delphi surveys were undertaken for the seven identified themes to achieve consensus for a new section on CI in an existing psychosocial guide. The intended primary end-user for this guide consists of the HCPs providing treatment to people with SCI in the acute, rehabilitation, and community settings. The secondary end-user includes consumer organisations, health planners, and policy makers.
Results
The expert consultation resulted in developing seven key themes to provide a foundational structure to the guidance about CI. For the first round of the Delphi survey, 40 (out of 49) statements received agreement levels exceeding 95% and were accepted without revisions. In the second round, two statements were deleted, and seven statements were amended based on the feedback received. After the final round, a total of 47 statements were accepted and formed 20 recommendations under seven themes as the final version of the cognitive guide.
Conclusion
This updated guidance for managing CI in people with SCI emphasises the importance of person-centred care and the identification of barriers and facilitators for improved communication between the multidisciplinary HCPs and patients with SCI and their family members. This will ultimately enhance overall rehabilitation outcomes including self-efficacy, adjustment, and quality of life.

Similar content being viewed by others


Introduction
People with spinal cord injury (SCI) undoubtedly have to deal with a significant life-changing physical injury. Consequently, people with SCI face significant personal challenges in the process of recovering and adjusting to the long-term impairment and necessary life changes following their injury. In addition, SCI is commonly associated with a range of secondary health conditions, including cognitive impairment and other comorbid psychosocial conditions like chronic pain and chronic fatigue [1, 2]. Psychological health and wellbeing can also be significantly impacted by the many challenges associated with living with SCI [3, 4]. Furthermore, people with SCI are met with significant social challenges, including a high risk of partner separation, isolation, loneliness, social discrimination, and unstable employment [5, 6]. Despite this, most people with SCI show favourable long-term adjustment outcomes [2, 7].
Rehabilitation following a SCI typically involves an interdisciplinary team approach that focuses on improving functioning and independence through physical retraining, acquisition of new functional skills, utilisation of compensatory strategies, and the provision of assistive devices and equipment to support independent living [8]. Advances have also been made in reconstructive and restorative interventions, such as nerve transfers to restore upper limb function in people with tetraplegia [9]. Clinical interventions have predominantly focused on physical rehabilitation, with comparatively less emphasis on psychosocial aspects of rehabilitation [2]. This imbalance reflects a historical focus on survival after SCI, which later expanded to encompass quality of life considerations as life expectancy improved. The provision of comprehensive psychosocial care, which addresses psychological (e.g., emotions and thoughts) and social aspects (e.g., relationships and environment) of a person’s life is crucial for people with SCI to maximise their self-efficacy, autonomy, wellbeing, and overall quality of life [3,4,5, 10]. Thus, over the past decade or so, there has been a notable increase in research exploring these aspects of rehabilitation and long-term outcomes in people with SCI, thereby building an expanding evidence base for their rehabilitation [1, 2, 11,12,13].
Cognitive impairment (CI) refers to a decline in mental abilities, such as memory, attention, problem-solving, and decision-making. It can range from mild difficulties to severe limitations affecting daily functioning. Cognitive function after SCI is emerging as an important area of research [14, 15] given the relative risk of CI in people with SCI is around 13 times higher than an able-bodied adult, with rates of CI after SCI estimated to range between 17–36% [16,17,18]. Cognitive function, including memory, attention, and problem-solving, plays an important role in the success of rehabilitation for the person with SCI, so it is likely that adjustment and rehabilitation outcomes will be compromised if CI is not addressed [2, 18, 19]. Even with the growing appreciation of psychosocial interventions as essential for SCI rehabilitation [20], CI remains a challenge that needs to be addressed as a priority. There is also a need to educate and support clinicians and healthcare professionals (HCPs) on effectively communicating and engaging with people with SCI, especially those with CI, during rehabilitation [18, 19]. In response to this need, it was crucial to revise and update the existing “Guide for health professionals on the psychosocial care of adults with SCI” developed and published in 2014 [21] to include recommendations and strategies for managing CI in people with SCI. Inclusion of a care practice guide for CI in the context of SCI is novel and have not been previously published. Therefore, the purpose of this paper is to: [1] outline the process for developing a section on CI; [2] summarise the recommendations for HCPs in managing people with CI; and [3] provide strategies for implementing these recommendations within SCI units and extending their reach to the broader community.
Methods
This collaborative work to update the 2014 Psychosocial Care Practice Guide was undertaken in 2020–22, involving HCPs from three specialised SCI Units, a person with lived experience with SCI and a range of stakeholders working in the field of SCI, in NSW Australia.
Previous editions of the guide
The first edition of the guide was released in 2008, followed by the second edition in 2014 [21]. The development process of the 2008 edition involved extensive discussions with various stakeholders, including HCPs from SCI Units, specialised clinics, and hospitals. Furthermore, an international expert in spinal injury, Professor Paul Kennedy from Oxford, UK, visited Australia in 2005 to provide valuable insights into developing this initial guide. Following an extensive consultative process over a period of 2-years, a Statewide Committee in NSW was formed to advance the improvement of psychosocial care in SCI through the establishment of the psychosocial principles and guidelines which formed the basis of the 2008 guide.
In 2014, the guide [21] underwent significant updates to ensure alignment with the latest research and advancements in psychosocial care for people with SCI [20]. A comprehensive systematic literature search was conducted to identify relevant studies across various psychosocial domains. This edition also focused on the development of new and enhanced service delivery models in inpatient, outreach, and community-based settings, which empowered people with SCI to play an active role in their rehabilitation journey. Furthermore, the integration of peer support within the rehabilitation process was emphasised, leveraging their unique lived experiences and perspectives.
The 2023 edition of the guide
The latest update to the guide involved significant enhancements with 18 principles and 37 recommendations. The summary of changes and new additions in the 2023 Guide Edition are provided in Table 1. The updated version now includes a framework based on the SCI Adjustment Model or SCIAM [2, 7] and the Emotional Wellbeing Toolkit [22], which provides additional resources for addressing emotional and psychological challenges faced by people with SCI. The methodology and results for the 2023 psychosocial guide can be found in detail elsewhere [23].
Importantly, a new section was added addressing the issue of those with SCI and CI, offering evidence-based recommendations. Another notable addition is the inclusion of sections dedicated to the importance of screening, monitoring, follow-up assessment, and the role of peer support in the psychosocial care of people with SCI. The process of updating the guide involved a multidisciplinary team, ensuring a comprehensive and well-rounded approach to addressing the psychosocial needs of people with SCI.
Target end-users for the guide
The intended primary end-user for this guide consists of the HCPs providing treatment to people with SCI in the acute, rehabilitation, and community settings, as well as other specialised psychosocial care providers perhaps unfamiliar with the management of people with SCI. The secondary end-user includes interested community organisations, including not-for-profit consumer organisations (e.g., Spinal Cord Injuries Australia and Forward Ability Support NSW), as well as those involved in health planning and policy both within NSW and more broadly.
Development process – new section on cognitive impairment in people with SCI
The purpose of the new section on CI is to enhance knowledge, skills, and competency of HCPs for delivering person-centred care and support to people with SCI and CI in the rehabilitation setting. By adding a section on CI, it was believed that this would lead to positive outcomes for people with SCI. Notably, the content of this section can also be valuable in other contexts, such as cognitive dysfunction related to dementia, learning disabilities, limited educational background, and other socioeconomic barriers.
The development cycle encompassed multiple stages, commencing with the establishment of an advisory committee. This was followed by expert consultations, deriving seven key themes to provide a foundational structure to the guidance about CI. Rapid reviews of available data were conducted for the seven identified themes. Additionally, an e-Delphi survey was conducted to achieve consensus and further refine the guide. The process resulted in the finalisation of the section dedicated to CI in the guide, as illustrated in Fig. 1.

Provides an overview of the multi-stage development process of the section on CI in the psychosocial care guide.
Stage 1: advisory committee establishment
The Advisory Committee was established to provide strategic advice and support the development of the guide as well as ensure alignment with overall project priorities and inform the Project Steering Committee about the progress in a timely manner. The advisory committee consisted of 17 experts, including physiotherapists, occupational therapists, nurses, medical specialists, clinical psychologists, social workers, a neuropsychologist, a person with SCI lived experience, academics, and policy makers. The roles of Advisory Committee members included:
-
(a)
participating in concept development
-
(b)
providing oversight and expertise for the development of the guide with a pragmatic and implementable perspective
-
(c)
applying an evidence-based approach
-
(d)
monitoring the quality of the guide as they developed and identified any potential risks
-
(e)
advising on strategies for effective implementation and evaluation of the guide
-
(f)
participating in expert consultation and Delphi study.
Stage 2: expert consultations
Two rounds of expert consultations were conducted with the members of the Advisory Committee, to develop the foundational structure of the cognitive guide, ensuring a comprehensive and inclusive approach. Both rounds were moderated by one of the authors (AC and/or MA). During the first round, the focus was on idea generation and insight development regarding the themes that should be incorporated into the guide. This stage allowed for the exploration of a wide range of perspectives and considerations related to CI in people with SCI. In the second round, the expert consultation group further refined and finalised the seven key themes that were agreed upon during the initial round. This phase involved thorough discussions and deliberations to ensure the inclusion of the most relevant and impactful themes in the guide. The outcome of this stage and the seven key themes are outlined in Table 2, which form the basis for undertaking the rapid review.
Stage 3: rapid review
A rapid review [24] was undertaken to synthesise the current literature on CI in people with SCI, considering seven themes.
Search strategy and databases used
Evidence for the specific and generic practice guide was gathered by conducting a series of literature searches using primary search terms such as “spinal cord injury”, “rehabilitation”, “adjustment”, “treatment”. These primary terms were used in combination with secondary search terms related to cognition and cognitive impairment. Search engines used included Medline, EMBASE, PsycINFO, and Google Scholar (detailed search terms were presented as Appendix A). Google Scholar was used to search for clinical practice guides in use by other relevant professionals in Australia and overseas. While the searches were carried out during a six-months timeframe in 2021 (May to October), they covered studies from the inception of the relevant research field up to the most current available literature.
Inclusion and exclusion criteria
Criteria that were applied to outcome measures to update the Guide included:
-
objective measures that reflect how a person with SCI adapts, adjusts, and copes with their injury
-
measures that have demonstrated validity and an evidence base
-
reliable measures that have face validity, that is, they have relevance to rehabilitation intervention goals
-
measures that cover multiple domains that reflect useful products for consumers
-
measures used with a range of disorders and injuries that would provide scope for comparisons.
For example, we considered the Neuropsychiatry Unit Cognitive Assessment Tool (NUCOG), a brief objective screening tool that assesses five cognitive domains relevant to how people with SCI may be adapting post-injury, particularly in the context of ageing, brain injury, or comorbidities [25]. It has demonstrated validity and reliability in rehabilitation settings, supporting goal setting and intervention planning. While not specific to SCI, NUCOG’s broad domain coverage, clinical utility, and use across multiple conditions support its inclusion under the applied criteria.
Evidence synthesis
When evidence for a recommendation was available, the process of evaluating the evidence was adhered to the National Health and Medical Research Council (NHMRC) guidelines 2009 for rating the strength of evidence. An example of synthesis of evidence and its evaluation is presented as Appendix B. Where there was no evidence base, or the level of evidence was low or insufficient, a best practice guidance was developed using a rigorous Delphi process, followed by a consensus by a multidisciplinary panel of health professionals and experts in SCI rehabilitation. For more details on Delphi survey, refer to Stage 4. Only the key references were cited in the Guide, and these were selected on their scientific merit.
Stage 4: e-delphi survey
The development of consensus-based key recommendations supported by evidence and expert input on the seven identified key themes involved three rounds of e-Delphi surveys. The surveys were facilitated by MA and moderated by AC, with the panel of experts comprising members from the Advisory Committee responsible for achieving consensus on the guide’s recommendations. The personal characteristics of the expert group are presented in Table 3.
In the first round of the e-Delphi survey, 17 participants were presented with a set of 49 statements related to the seven key themes (see Appendix C). They were asked to assess each statement by indicating their agreement or disagreement. Participants also had the opportunity to provide suggestions for improving the syntax or content of the statements. Statements that did not reach an agreement level above 80% in the first round were carried forward to subsequent rounds to seek further possible consensus. This iterative process aimed to achieve a broader consensus on the initially disagreed statements. Subsequently, a second and third e-Delphi round were conducted to gather additional input and reach consensus on the remaining items.
Out of the initial 49 statements, 40 statements received agreement levels exceeding 95% and were accepted without revisions. Only nine statements were disagreed upon and required further revisions. An example of a statement with disagreement encountered during the e-Delphi survey is illustrated in Table 4. In the second round, two statements were suggested for deletion, and seven statements were amended based on the feedback received. All the accepted and amended statements were then presented to the Delphi panel in the third round, resulting in 100% agreement being achieved. After the third round, a total of 47 statements were accepted and formed 20 recommendations under seven themes as the final version of the cognitive guide including one or more suggested implementation strategies (presented as Appendix D).
Stage 5: finalisation of the guide
The finalisation of the guide involved a comprehensive and iterative process, drawing on the collaborative input and expertise of the Guide Advisory Committee, expert consultations, rapid review, and e-Delphi surveys. The Guide Advisory Committee played a vital role in providing overarching guidance and direction throughout the development process of the guide. The collective expertise and insights of the Advisory Committee ensured a well-rounded approach to addressing the psychosocial aspects including CI after SCI. The guide was also reviewed by an independent evaluator from the NSW Agency for Clinical Innovation, which is a pillar organisation working in partnership with the NSW Ministry of Health. The final guide was then endorsed by the three Statewide Services SCI Units Directors in NSW, Australia.
Results
Themes, recommendations, and implementation strategies for cognitive impairment
Theme 1: Raise awareness of causes of mild to moderate CI and sub-types of CI in people with SCI when participating in rehabilitation
Recommendation 1: It is recommended that all staff and treating team members receive training to increase awareness of the likely occurrence of cognitive impairment following SCI
Given that a phase of intensive rehabilitation occurs after a SCI, treating staff being aware of a possible CI is essential, as it can significantly impact long-term rehabilitation outcomes. By raising awareness, the risk of poor rehabilitation outcomes can be mitigated, leading to more effective and tailored care for those with SCI [16, 26, 27]. Current evidence suggests that patients with SCI have substantially increased risk of cognitive impairment [16, 27,28,29].
Suggested implementation strategies:
-
(1)
Raise awareness by developing and distributing relevant materials for staff, treating team, people with SCI, their families, and the broader community to promote understanding and reduce stigma surrounding cognitive impairment.
Recommendation 2: It is recommended that healthcare providers understand and thoroughly assess all possible contributors to cognitive impairment in people with SCI
It is important to avoid assuming that cognitive changes in people with SCI are purely situational or reactive. Each person should be assessed thoroughly to understand the full scope of possible CI. CI may stem from a variety of underlying causes, including neurological changes associated with the injury itself. A thorough, individualised assessment allows HCPs to identify accurately and understand the nature of any impairment, ensuring that any cognitive challenges are addressed appropriately and effectively, rather than overlooked or misattributed. While comorbid traumatic brain injury (TBI) is a common cause of CI following a traumatic SCI [16, 18, 30,31,32], there are numerous other contributors or causes [31, 33, 34]:
-
severe mental illness or a psychological disorder (e.g., depression, anxiety, chronic stress, or alcohol and substance use disorder)
-
decentralised cardiovascular function
-
sleep apnoea
-
polypharmacy (e.g., use of opioids, anticholinergics)
Other possible contributors or causes that may impair cognitive function in SCI include [16, 34]:
-
injury or inflammation to CNS (other than TBI)
-
personal factors (e.g., age, sex, and education)
-
environmental factors (e.g., critical care, intensive hospitalisation, community transition)
-
secondary health conditions (e.g., chronic pain, fatigue).
People with SCI may experience significant cognitive challenges due to environment contextual factors. Sudden changes in the environment, social dynamics, and responsibilities can overwhelm people, impacting their cognitive function. For example, transitioning from hospital to the community (at first discharge) is often associated with increased anxiety and feeling emotionally overwhelmed [7, 35], which can contribute to temporary cognitive fluctuations or cognitive burden rather than true CI. However, prolonged exposure to stress and limited cognitive stimulation could contribute to cognitive difficulties if not addressed.
Suggested implementation strategies:
-
(2)
Develop educational materials and training programs for healthcare professionals to enhance their understanding of the causes and implications of mild to moderate CI in people with SCI.
Theme 2: Improve awareness of terminology of what constitutes mild, moderate, and severe CI in people with SCI and associated symptoms
Recommendation 3: It is recommended that healthcare providers use standardised terminology when defining mild, moderate, and severe cognitive impairment in people with SCI.
Research has shown there is a lack of understanding of what constitutes levels of CI in rehabilitation teams, so it is important to standardise terminology [36]. Clear and consistent language will enhance reliable communication across care teams and improve the accuracy of assessment and treatment plans. However, clinical judgment should be applied in conjunction with the definitions outlined below to ensure that the unique cognitive and functional needs of each patient are appropriately addressed.
-
a.
Mild CI can be defined as impairment in cognitive function (e.g., mild memory loss) in adults that is greater than expected for a person’s age and education level but does not significantly interfere with activities of daily life [37, 38].
-
b.
Moderate to severe CI in adults can be defined as a significant cognitive decline from a previous level of performance, greater than expected for the person’s age and education level, in one or more cognitive domains, such as memory, attention, perceptual-motor skills, language, social cognition, and executive function.
The severity rating should be based on the extent to which cognitive deficit/s interfere with independence and everyday functioning, potentially resulting in a loss of independence and a substantial need for assistance with daily tasks, such as managing finances and taking medications. It is important to identify sub-types of CI such as amnestic CI (primary memory impairment) versus non-amnestic CI (where non-memory domains dominate) [38]. The cognitive decline should not be attributed to delirium.
Suggested implementation strategies:
-
(3)
Establish a standardised set of terms and definitions related to CI after SCI to ensure consistent language for interpretation and communication across healthcare settings.
-
(4)
Disseminate the standardised terminology through educational resources, guidelines, and training programs to ensure widespread adoption among healthcare professionals.
Recommendation 4: It is recommended that healthcare providers develop a thorough understanding of the common signs and symptoms of cognitive impairment following SCI
Early recognition of signs and symptoms of CI is essential for understanding its impact on patients with SCI. CI can manifest in various ways [18, 19, 39], including the following:
-
a.
forgetfulness or memory loss
-
b.
low motivation and inaction
-
c.
difficulty with solving life problems
-
d.
difficulties communicating with slower processing of information and verbal response time
-
e.
trouble recognising familiar people and places
-
f.
problems with attention
-
g.
difficulty understanding or implementing multiple step instructions or tasks
-
h.
trouble exercising judgment, such as knowing what to do in an emergency
-
i.
difficulty planning and carrying out tasks
-
j.
problems with managing emotions and with adjustment, including elevated anxiety and depressive mood, frustration
-
k.
disorganisation.
Suggested implementation strategies:
-
(5)
Promote staff awareness through training modules or reference guides designed to help healthcare providers recognise the signs of CI (see Fig. 2).
Fig. 2 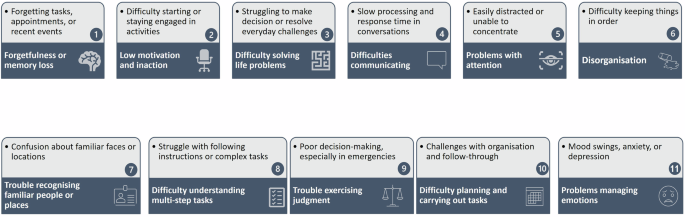
Infographic: Signs of cognitive impairment.

Recommendation 5: It is recommended to provide appropriate orientation and ongoing professional development opportunities for staff to acquire and maintain the necessary skills for effectively supporting people with SCI who have cognitive impairment
Structured, employer-assisted education and support programs should be developed for staff to be adequately resourced and skilled to effectively implement care for people with SCI at high risk or suspected of CI. In addition, support will be required to promote the continued use of these skills, such as access to supervision.
Suggested implementation strategies:
-
(6)
Professional development for detecting, assessing, and managing CI should also be offered, with regular evaluations and feedback to ensure the continuous improvement and application of these skills.
Theme 3: Describe best approaches to assessing CI in people with SCI, including screening processes, time points, assessment tools, and health professionals involved
Recommendation 6: It is recommended that an initial brief validated cognitive screening be conducted as soon as practicable following SCI, regardless of mechanism and level of SCI
Current evidence suggests that a person with SCI has substantially increased risk of CI [16,17,18,19]. Therefore, it is imperative to assess cognitive function in people with SCI during rehabilitation [16, 28, 39]. The purpose of the cognitive assessment using a validated screening tool is to ensure that the treating team is aware of any possible underlying level of CI that can impact on the process of rehabilitation through the continuum of care.
Recommendation 7: Conduct cognitive screening for patients upon admission to SCI rehabilitation and periodically throughout their lifetime to monitor any changes over time
Other considerations:
-
Valid and objective cognitive assessment should be conducted after the patient has settled into the rehabilitation phase, based on clinical discretion.
-
It should not be done on a patient if they are unwell. In this scenario, the assessment may be based upon their history as obtained from significant others (such as family members and general practitioner), regarding risk factors such as a previous history of psychiatric disorder. As soon as the patient can communicate, a direct assessment should occur involving them.
Recommendation 8: It is recommended that cognitive screening and psychosocial assessment be conducted for patients who are at a high risk of cognitive impairment or who have suspected co-morbid conditions (such as TBI) or other risk factors (such as, older age)
A psychosocial assessment of risk factors associated with CI should be conducted. Identifying CI in people with SCI is essential for developing tailored management strategies and be integrated into rehabilitation planning.
Suggested implementation strategies:
-
(7)
Develop guidelines and protocols for the comprehensive assessment of CI in people with SCI, incorporating validated assessment screening tools and procedures.
-
(8)
Provide training and resources for healthcare professionals on the administration and interpretation of cognitive assessment measures specific to SCI.
Recommendation 9: It is recommended that validated neurocognitive capacity screens be utilised
Valid neurocognitive screens can be important tools that can be used to detect the presence of mild to moderate CI after SCI. However, there are no validated neurocognitive measures created specifically for people with SCI [16, 19] including those with limited hand functions. Hence SCI Units should develop a regimen of validated cognitive capacity screens that could be used to determine the possible presence of CI after SCI [19, 25, 40]. Rehabilitation staff should receive training (such as from a neuropsychologist or clinical psychologist) in conducting cognitive screening and interpreting the results.
Accurate screening for CI in people with SCI is crucial for optimising rehabilitation outcomes. Despite its clinical importance, there is a notable lack of screening tools developed specifically for SCI, leading clinicians to rely on instruments validated in other populations. This creates a unique challenge, as many existing cognitive screening tests were not designed to capture the specific deficits seen in SCI. Cognitive performance in people with SCI may be influenced by a combination of injury-related factors, secondary health conditions, and neurological changes that differ from those typically observed in neurodegenerative disorders. The limitations in validity and applicability of currently available tools for CI screening in people with SCI are summarised as Appendix E.
Recommendation 10: It is strongly recommended that if the results of a neurocognitive screen indicate cognitive impairment, healthcare providers should consider referral for comprehensive neuropsychological testing depending on the individual case
Depending on the mechanism of injury and irrespective of level of injury, evidence suggests people with SCI should be screened for evidence of TBI (e.g., post-traumatic amnesia, Glasgow Coma Scale) when admitted to the emergency department and/or acute care to inpatient rehabilitation [41]. In cases where people with SCI are suspected to have sustained a TBI, the Abbreviated Westmead Post-Traumatic Amnesia Scale (or equivalent) should be administered on admission to ED or in acute care, where possible.
Theme 4: Define person-centred care (PCC) in the context of mild to moderate CI in people with SCI when engaged in rehabilitation
Recommendation 11: It is recommended that person-centred care (PCC) be prioritised when treating people with SCI who also has cognitive impairment
Focusing on the injured person’s unique needs, preferences, values, and circumstances is essential for delivering effective and compassionate care. This is achieved through a dynamic relationship among those who are important to them, and all relevant providers [42, 43].
PCC involves the SCI rehabilitation team engaging a person with SCI in a collaborative, flexible, encouraging, and sensitive manner, which will most likely result in improved SCI perceptions/ participation in rehabilitation for those with CI [44, 45]. Factors essential to PCC like trust in relationships, emotional intimacy, and participation encourage post-traumatic growth in people with a SCI [46].
Suggested implementation strategies:
-
(9)
Foster a PCC approach in the delivery of care, recognising the unique needs, preferences, and goals of people with SCI and CI.
-
(10)
Promote shared decision-making and involve people with SCI with CI in their care planning and goal-setting processes.
Theme 5: Develop a list of recommended ways to improve how SCI rehabilitation health professionals (and caregiver/family) verbally communicate to those with mild to moderate CI
Recommendation 12: It is recommended that verbal, language, and speech strategies be utilised to enhance communication with people with SCI and cognitive impairment
The use of cognitive support strategies may improve communication between rehabilitation staff when interacting with people with SCI and CI [47, 48]. Supportive and helpful language employing strengths-based approaches should be used when communicating with people who have mild to moderate CI after SCI. Some of the recommended general suggestions are presented as an infographic (Fig. 3).

General verbal communication strategies for healthcare providers when treating people with SCI and cognitive impairment.
Suggested implementation strategies:
-
(11)
Provide training to healthcare professionals on effective communication strategies tailored to people with SCI and CI.
-
(12)
Develop educational modules and communication aids and resources, such as visual supports, simplified language, and alternative communication methods, to facilitate effective (verbal) communication.
Recommendation 13: When engaging in verbal interactions with people who have cognitive impairment, it is recommended to avoid open-ended questions
When communicating with people who have CI, using open-ended questions can sometimes lead to confusion and hinder understanding. Instead, it is recommended to use clear, direct questions that guide responses, such as yes/no or multiple-choice formats, tailored to the person’s needs and abilities. Selecting the appropriate question type, the healthcare provider should consider factors like the patient’s severity of impairment, education level, literacy, and comprehension. For example, when reliable yes/no responses are possible, these can enhance clarity and reduce frustration, helping to create a more effective and supportive communication experience.
Theme 6: Develop a list of recommended ways to improve how SCI rehabilitation health professionals (also caregiver/family) non-verbally communicate to those with mild to moderate CI
Recommendation 14: It is recommended that non-verbal strategies, such as gestures, facial expressions, and body language, be utilised to enhance communication when needed
Effective communication is essential in healthcare settings, particularly when managing people with complex needs, such as those with cognitive or physical impairments. By incorporating non-verbal strategies, healthcare professionals can improve understanding, and ensure that critical information is conveyed accurately, especially in situations where verbal communication may be limited or ineffective [47, 48]. This approach supports PCC, ensuring that communication barriers are minimised. Some of the recommended suggestions are presented as an infographic (Fig. 4).

General non-verbal communication strategies for healthcare providers when treating people with SCI and CI.
Suggested implementation strategies:
-
(13)
Educate healthcare professionals on the importance of non-verbal communication cues and develop resources and training programs that focus on enhancing non-verbal communication skills.
Theme 7: Determine challenges and barriers to improve communication and care for those with SCI and who also have CI
Recommendation 15: It is recommended that clients receive timely and tailored information that aligns with their cognitive function status, ensuring accessibility and comprehension for effective self-management and care
A person admitted with an acute SCI requires timely and targeted information about medical diagnosis and prognosis of their SCI when it is deemed that they are ready. However, this needs to be done without overwhelming them. This is also crucial to their understanding of the processes involved in their rehabilitation. The person depends on accurate information to facilitate their active engagement in the discussion of treatment options.
Fluctuating clinical presentations, and the development of secondary health conditions, result in an on-going need for good quality information. Certainly, there is a need for information about diagnosis and prognosis to be repeated as necessary. Overcoming barriers to shared decision-making is important. There are a range of barriers and facilitators to effective shared decision-making. These may include the:
-
age, sex, culture, attitudes, opinions, level of education, and past experience of being a patients
-
health literacy
-
emotional readiness for partnering
-
degree of trust and confidence in the healthcare system and clinicians
-
communication style and skills of both parties.
Most common barriers are organisational structure/administrative supports (e.g., lack of decision trees for the condition or scenario) and lack of time to build relationships and trust and explore all the options, or a lack of available evidence, to allow informed decision-making. The following approaches have been found to augment shared decision-making:
-
actively supporting people to be involved in decision-making
-
emphasising options and problem solving
-
developing care plans as a partnership between patients and professionals
-
setting PCC goals and following up on the extent to which these are achieved over time
-
using decision aids rather than merely providing information
-
providing opportunities to share and learn from peers with the same condition.
Recommendation 16: Recognise that people with SCI and cognitive impairment may have difficulty sustaining a conversation due to problems with attention, processing information, and short-term memory
Short-term memory issues often intersect with other factors such as forgetting, distractions, and attentional difficulties, further complicating communication. This can further result in confusion, difficulty following conversations, and a need to frequently re-establish context or clarify information. To address these barriers, healthcare providers should adopt strategies that accommodate these limitations. These strategies include providing additional time for processing information, repeating key points as needed, and using supportive communication techniques to enhance understanding.
In addition, creating an environment conducive to focus is crucial. Minimising distractions can help the person better engage in the interaction. Structured aids, such as steps, checklists, written handouts, or visuals, can also support comprehension and retention. It is equally important to consider the impact of fatigue. Interactions should ideally take place when the person feels rested, alert, and not overwhelmed by tiredness.
Recommendation 17: Be aware that people with SCI and cognitive impairment may quickly forget information they have understood during conversations, which can hinder long-term retention and follow-up communication
People with SCI and CI may often struggle with retaining information shared during conversations, even if they initially understand it. This can lead to confusion and miscommunication, as they may not retain key details needed for decision-making or ongoing discussion. This can disrupt the flow of communication, as they might frequently lose track of what was discussed, making it challenging for them to follow or respond accurately. Identifying this challenge enables healthcare providers to support people by using methods like repetition, simplifying messages, and providing written or visual aids to reinforce understanding and facilitate clearer, more effective communication.
Recommendation 18: Ensure that people with SCI and cognitive impairment are provided with necessary adjustments, such as additional time or written reminders, to support their full participation in treatment and decision-making processes
Providing adjustments like additional time to process information, written reminders (visuals or handouts) for key details, and simplified instructions can significantly enhance people’s ability to understand and participate in their care. These supportive measures not only promote independence but also promote a more inclusive environment where people feel empowered and engaged in their treatment journey, leading to better overall outcomes.
Recommendation 19: Understand that people with SCI and cognitive impairment may face communication challenges that lead to frustration, negative moods, and behaviours, which can further hinder effective communication and engagement
Difficulties in expressing thoughts and needs may cause the person to feel isolated or unheard, intensifying their frustration. Recognising these emotional responses enables healthcare providers to respond with empathy and patience, using strategies that promote calm and understanding, thereby reducing barriers and supporting a more positive communication experience.
Suggested implementation strategies:
-
(14)
Conduct research and gather feedback from people with SCI, healthcare professionals, and stakeholders to identify common challenges and barriers to effective communication.
-
(15)
Use the findings to inform the development of targeted interventions, policies, and support systems to address these challenges and promote improved communication outcomes.
Recommendation 20: Recognise and consider system-level barriers and facilitators that may impact the implementation of the recommended strategies
A list of potential barriers and facilitators are presented in Fig. 5 that may arise when implementing the above recommendations in clinical practice [49].

Potential barriers and facilitators when implementing the recommendations.
Limitations
This project followed a rigorous multi-stage process to develop cognitive guidelines for people with SCI, however, several limitations are noted. The Advisory Committee, while diverse, may not have fully represented all perspectives particularly those from under-represented healthcare settings and people with lived experience of cognitive impairment. Engagement from frontline healthcare providers, caregivers, and people with SCI may also have been limited, potentially narrowing the scope of recommendations.
The rapid review methodology, though efficient, did not include grey literature or non-English publications and lacked the depth of a formal systematic review, possibly leading to evidence gaps. The Delphi process, reliant on expert consensus, may have been influenced by individual biases, varying engagement, and self-reported expertise.
We also acknowledge that the database search is now almost four years old. However, this work is part of a broader update to the psychosocial guidelines, and due to scope and resource limitations, re-running the search strategy is not feasible at this stage. In addition, the implementation phase of the guidelines is currently ongoing across three SCI services in NSW, Australia [50]. New learnings and updated literature identified during this phase will inform the next iteration of the guidelines. A full update, including a revised and expanded search, is anticipated to take place in 2028.
Finally, some recommendations have yet to be validated in practice, and implementation challenges were not explored. As research on CI in SCI evolves, future updates will be necessary to reflect emerging evidence.
Future research implications
Future research and updates to the guide will further optimise psychosocial care for people with SCI and CI, enhancing rehabilitation outcomes and quality of life. Longitudinal studies using validated neurocognitive tools specific to SCI are needed to explore the trajectory and contributing factors of CI. Investigating cognitive rehabilitation programs and effective interventions can enhance cognitive functioning and outcomes. Future research could also benefit from incorporating advanced brain imaging techniques, such as Magnetic Resonance Imaging, functional Near-Infrared Spectroscopy, or neural activity monitoring tools like Electroencephalography, to explore the relationship between changes in the brain and SCI, offering deeper insights into CI.
Emerging perspectives suggest that cognitive changes after SCI may be adaptive rather than purely a deficit, possibly involving structural, functional, and/or neurophysiological changes as the result of cognitive rehabilitation [51]. While neuroplasticity supports recovery, there is little evidence that cognitive slowing is intentional or functional. Further research is needed to explore the mechanisms behind these changes and any potential compensatory roles.
Addressing CI in people with SCI requires expanding beyond communication-focused strategies to include broader rehabilitation approaches. While current recommendations emphasise what HCPs can say or do during interactions, emerging evidence highlights the need to enhance HCP skills in recommending and supporting interventions that may improve cognitive function. For example, recent studies suggest that physical activity combined with cognitive training shows promise, while diet modification and supplements have limited impact [52,53,54]. Future updates to guidelines should incorporate these evolving insights to support more comprehensive, evidence-based care. Additionally, an implementation study of the psychosocial guide, incorporating these CI recommendations, is currently ongoing across three specialist SCI Services in NSW, Australia. Evaluating these CI recommendations in real-world clinical settings is essential to enhancing psychosocial practices and patient outcomes, ultimately strengthening person-centred care in SCI rehabilitation [50].
Conclusion
This paper outlines the development of a guide for people with SCI and CI, marking a significant step in addressing their complex rehabilitation needs. Through expert consultations, rapid review, and e-Delphi surveys, evidence-based recommendations were created to advance psychosocial care. The guide offers healthcare professionals a comprehensive framework to address cognitive challenges, as well as psychosocial aspects of SCI, emphasising PCC, standardised communication, and the identification of barriers and facilitators to improve interactions among multidisciplinary teams, patients, and families.
References
Craig A, Tran Y, Siddall P, Wijesuriya N, Lovas J, Bartrop R, et al. Developing a model of associations between chronic pain, depressive mood, chronic fatigue, and self-efficacy in people with spinal cord injury. J. Pain. 2013;14:911–20.
Craig A, Tran Y, Arora M, Pozzato I, Middleton JW. Investigating dynamics of the spinal cord injury adjustment model: mediation model analysis. J. Clin. Med. 2022;11:4557.
Craig A, Nicholson Perry K, Guest R, Tran Y, Dezarnaulds A, Hales A, et al. Prospective study of the occurrence of psychological disorders and comorbidities after spinal cord injury. Arch. Phys. Med. Rehabil. 2015;96:1426–34.
Williams R, Murray A. Prevalence of depression after spinal cord injury: a meta-analysis. Arch. Phys. Med. Rehabil. 2015;96:133–40.
Bonanno GA, Kennedy P, Galatzer-Levy IR, Lude P, Elfström ML. Trajectories of resilience, depression, and anxiety following spinal cord injury. Rehabil. Psychol. 2012;57:236–47.
Craig A, Nicholson Perry K, Guest R, Tran Y, Middleton J. Adjustment following chronic spinal cord injury: determining factors that contribute to social participation. Br. J. Health Psychol. 2015;20:807–23.
Craig A., Tran Y., Middleton J. Theory of adjustment following severe neurological injury: evidence supporting the spinal cord injury adjustment model. In: A Costa and E Villalba,(Eds.). Horizons in Neuroscience Research. New York: Nova Science Publishers; 2017;29:117–139.
Burns AS, Marino RJ, Kalsi-Ryan S, Middleton JW, Tetreault LA, Dettori JR, et al. Type and timing of rehabilitation following acute and subacute spinal cord injury: a systematic review. Glob. Spine J. 2017;7:175s–94s.
van Zyl N, Hill B, Cooper C, Hahn J, Galea MP. Expanding traditional tendon-based techniques with nerve transfers for the restoration of upper limb function in tetraplegia: a prospective case series. Lancet. 2019;394:565–75.
Craig A. The sir ludwig guttmann lecture 2023: psychosocial factors and adjustment dynamics after spinal cord injury. Spinal Cord. 2025;63:194–200.
Geyh S, Nick E, Stirnimann D, Ehrat S, Müller R, Michel F. Biopsychosocial outcomes in individuals with and without spinal cord injury: a Swiss comparative study. Spinal Cord. 2012;50:614–22.
Savic G, DeVivo MJ, Frankel HL, Jamous MA, Soni BM, Charlifue S. Long-term survival after traumatic spinal cord injury: a 70-year British study. Spinal Cord. 2017;55:651–8.
Shavelle RM, DeVivo MJ, Brooks JC, Strauss DJ, Paculdo DR. Improvements in long-term survival after spinal cord injury? Arch. Phys. Med. Rehabil. 2015;96:645–51.
Arora M, Pozzato I, McBain C, Tran Y, Sandalic D, Myles D, et al. Cognitive reserve and its association with cognitive and mental health status following an acute spinal cord injury. J. Clin. Med. 2023;12:4258.
Pozzato I, Arora M, McBain C, Wijesuriya N, Tran Y, Middleton JW, et al. Cognitive failure in adults with spinal cord injury: a valuable adjunct measure for enhancing cognitive assessment and rehabilitation outcomes. Neurol. Int. 2023;15:1371–82.
Craig A, Guest R, Tran Y, Middleton J. Cognitive impairment and mood states after spinal cord injury. J. Neurotrauma. 2017;34:1156–63.
Distel DF, Amodeo M, Joshi S, Abramoff BA. Cognitive dysfunction in persons with chronic spinal cord injuries. Phys. Med. Rehabil. Clin. N. Am. 2020;31:345–68.
Sandalic D, Craig A, Tran Y, Arora M, Pozzato I, McBain C, et al. Cognitive impairment in individuals with spinal cord injury: findings of a systematic review with robust variance and network meta-analyses. Neurology. 2022;99:e1779–e90.
Sandalic D, Tran Y, Craig A, Arora M, Pozzato I, Simpson G, et al. The Need for a specialized neurocognitive screen and consistent cognitive impairment criteria in spinal cord injury: analysis of the suitability of the neuropsychiatry unit cognitive assessment tool. J. Clin. Med. 2022;11:3344.
Middleton J, Nicholson Perry K, Craig A. A clinical perspective on the need for psychosocial care guidelines in spinal cord injury rehabilitation. Int. J. Phys. Med. Rehabilitation. 2014;2:1–6.
Craig A. and Nicholson Perry K. Guide for health professionals on the psychosocial care for people with spinal cord injury. Ed. 2, Publisher NSW Agency for Clinical Innovation: NSW State Spinal Cord Injury Service, NSW Australia.2014. https://www.aci.health.nsw.gov.au/__data/assets/pdf_file/0019/155233/Guide-Psychosocial-Care.pdf Accessed 29 August 2024.
NSW State Spinal Cord Injury Service Psychosocial Strategy. Emotional Wellbeing Toolkit: A Clinicians Guide to working with Spinal Cord injury. Agency for Clinical Innovation NSW. 2016. https://aci.health.nsw.gov.au/networks/spinal-cord-injury/resources/emotional-wellbeing Accessed on 29 August 2024.
Craig A., Arora M., Middleton J. W. Guide for health professionals: psychosocial care of adults with spinal cord injuries. Ed. 3, NSW Australia. Publisher NSW Agency for Clinical Innovation: NSW State Spinal Cord Injury Service. 2023. https://aci.health.nsw.gov.au/networks/spinal-cord-injury/resources/psychosocial-care Accessed on 29 August 2024.
King VJ, Stevens A, Nussbaumer-Streit B, Kamel C, Garritty C. Paper 2: performing rapid reviews. Syst. Rev. 2022;11:151.
Walterfang M, Siu R, Velakoulis D. The NUCOG: validity and reliability of a brief cognitive screening tool in neuropsychiatric patients. Aust. N. Z. J. Psychiatry. 2006;40:995–1002.
Dowler RN, Harrington DL, Haaland KY, Swanda RM, Fee F, Fiedler K. Profiles of cognitive functioning in chronic spinal cord injury and the role of moderating variables. J. Int. Neuropsychol. Soc. 1997;3:464–72.
Roth E, Davidoff G, Thomas P, Doljanac R, Dijkers M, Berent S, et al. A controlled study of neuropsychological deficits in acute spinal cord injury patients. Paraplegia. 1989;27:480–9.
Chiaravalloti ND, Weber E, Wylie G, Dyson-Hudson T, Wecht JM. Patterns of cognitive deficits in persons with spinal cord injury as compared with both age-matched and older individuals without spinal cord injury. J. Spinal Cord. Med. 2020;43:88–97.
Molina B, Segura A, Serrano JP, Alonso FJ, Molina L, Pérez-Borrego YA, et al. Cognitive performance of people with traumatic spinal cord injury: a cross-sectional study comparing people with subacute and chronic injuries. Spinal Cord. 2018;56:796–805.
Davidoff G, Morris J, Roth E, Bleiberg J. Cognitive dysfunction and mild closed head injury in traumatic spinal cord injury. Arch. Phys. Med. Rehabil. 1985;66:489–91.
Sachdeva R, Gao F, Chan CCH, Krassioukov AV. Cognitive function after spinal cord injury: a systematic review. Neurology. 2018;91:611–21.
Wilmot CB, Cope DN, Hall KM, Acker M. Occult head injury: its incidence in spinal cord injury. Arch. Phys. Med. Rehabil. 1985;66:227–31.
Coupland CAC, Hill T, Dening T, Morriss R, Moore M, Hippisley-Cox J. Anticholinergic drug exposure and the risk of dementia: a nested case-control study. JAMA Intern. Med. 2019;179:1084–93.
Wecht JM, Bauman WA. Decentralized cardiovascular autonomic control and cognitive deficits in persons with spinal cord injury. J. Spinal Cord. Med. 2013;36:74–81.
Kennedy P, Kilvert A, Hasson L. A 21-year longitudinal analysis of impact, coping, and appraisals following spinal cord injury. Rehabil. Psychol. 2016;61:92–101.
Wanlass RL, Reutter SL, Kline AE. Communication among rehabilitation staff: “mild,” “moderate,” or “severe” deficits? Arch. Phys. Med. Rehabil. 1992;73:477–81.
Centers for Disease Control and Prevention 2011. Cognitive Impairment: A Call for Action. Now! Department of Health and Human Services,USA 2020. https://www.cdc.gov/aging/pdf/cognitive_impairment/cogimp_poilicy_final.pdf.
Gauthier S, Reisberg B, Zaudig M, Petersen RC, Ritchie K, Broich K, et al. Mild cognitive impairment. Lancet. 2006;367:1262–70.
Davidoff GN, Roth EJ, Richards JS. Cognitive deficits in spinal cord injury: epidemiology and outcome. Arch. Phys. Med. Rehabil. 1992;73:275–84.
Cullen B, O’Neill B, Evans JJ, Coen RF, Lawlor BA. A review of screening tests for cognitive impairment. J. Neurol. Neurosurg. Psychiatry. 2007;78:790–9.
Sikka S, Vrooman A, Callender L, Salisbury D, Bennett M, Hamilton R, et al. Inconsistencies with screening for traumatic brain injury in spinal cord injury across the continuum of care. J. Spinal Cord. Med. 2019;42:51–6.
American Geriatrics Society Expert Panel on Person-Centered Care.Person-centered care: a definition and essential elements. Journal of the American Geriatrics Society. 2016;64:15-8.
Kogan AC, Wilber K, Mosqueda L. Person-centered care for older adults with chronic conditions and functional impairment: a systematic literature review. J. Am. Geriatrics Soc. 2016;64:e1–7.
Heinemann AW, LaVela SL, Etingen B, Miskovic A, Locatelli SM, Neumann HD, et al. Perceptions of person-centered care following spinal cord injury. Arch. Phys. Med. Rehabil. 2016;97:1338–44.
Melin J, Persson LO, Taft C, Kreuter M. Patient participation from the perspective of staff members working in spinal cord injury rehabilitation. Spinal Cord. 2018;56:614–20.
Chun S, Lee Y. The experience of posttraumatic growth for people with spinal cord injury. Qual. Health Res. 2008;18:877–90.
Orange JB, Molloy DW, Lever JA, Darzins P, Ganesan CR. Alzheimer’s disease. physician-patient communication. Can. Fam. Physician. 1994;40:1160–8.
Amsters D, Schuurs S, Pershouse K, Power B, Harestad Y, Kendall M, et al. Factors which facilitate or impede interpersonal interactions and relationships after spinal cord injury: a scoping review with suggestions for rehabilitation. Rehabil. Res. Pract. 2016;2016:9373786.
Correa VC, Lugo-Agudelo LH, Aguirre-Acevedo DC, Contreras JAP, Borrero AMP, Patiño-Lugo DF, et al. Individual, health system, and contextual barriers and facilitators for the implementation of clinical practice guidelines: a systematic metareview. Health Res. Policy Syst. 2020;18:74.
McBain C, Sarandrea AM, Pozzato I, Arora M, Myles D, Bourke J, et al. Implementing psychosocial guidelines into specialized spinal cord injury rehabilitation services to strengthen person-centred health care: protocol for a mixed methods study. Front. Rehabil. Sci. 2025;6:1537890.
Galetto V, Sacco K. Neuroplastic changes induced by cognitive rehabilitation in traumatic brain injury: a review. Neurorehabil Neural Repair. 2017;31:800–13.
Li Y, Hu Y, Pozzato I, Arora M, Schoffl J, McBain C, et al. Efficacy of interventions to improve cognitive function in adults with spinal cord injury: a systematic review. J. Neurotrauma. 2024;41:2075–88.
Pacheco N, Mollayeva S, Jacob B, Colantonio A, Mollayeva T. Interventions and cognitive functioning in adults with traumatic spinal cord injuries: a systematic review and meta-analysis. Disabil. Rehabil. 2021;43:903–19.
Vints WAJ, Gökçe E, Langeard A, Pavlova I, Çevik ÖS, Ziaaldini MM, et al. Myokines as mediators of exercise-induced cognitive changes in older adults: protocol for a comprehensive living systematic review and meta-analysis. Front. Aging Neurosci. 2023;15:1213057.
Acknowledgements
The authors gratefully acknowledge the support provided by the NSW State Spinal Cord Injury Service, Agency for Clinical Innovation and icare NSW. Special thanks are extended to the SCI Cognitive Study Steering and Guide Advisory Committees for their invaluable input and guidance throughout this project. Members of the Advisory Committee: Ashley Craig, Annalisa Dezarnaulds, Alison Hales, Catherine Ephraums, Danielle Sandalic, Grahame Simpson, Ilaria Pozzato, Jackson Singleton, James Middleton, Jasbeer Kaur, Joe Hanna, Lisa Benad, Lisa Harvey, Lynn Blecher, Mohit Arora, Nick Taylor, Ruyi Yao, Wilhelmina Long and Yvonne Tran.
Funding
This work was supported and funded by a research grant from icare NSW (2019–2022). The funder does not take direct responsibility for any of the following: study design, data collection, data analysis, drafting of the manuscript, or decision to publish.
Author information
Authors and Affiliations
Contributions
Conceptualisation, MA, JM and AC; methodology, MA, IP and AC; validation, MA, IP and AC; formal analysis, MA; resources, MA and JK; writing—original draft preparation, MA; writing—review and editing, MA, JM, AMS, IP, CM, DM, YT, JK and AC; project administration, MA, IP, CM, and DM; funding acquisition, MA, JM, IP and AC. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics statement
This work is a component of a bigger longitudinal cohort study approved by Northern Sydney Local Health District Human Research Ethics Committee (2019/ETH00592). Informed consent was not applicable for this group, as the participants involved (specifically those contributing to the Delphi survey) were members of the Guide Advisory Committee who were engaged in the project in an expert advisory capacity.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Arora, M., Middleton, J., Sarandrea, A. et al. Evidence based recommendations for health professionals to improve care of people with spinal cord injury and cognitive impairment: an update to the psychosocial care practice guide. Spinal Cord (2025). https://doi.org/10.1038/s41393-025-01124-7
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41393-025-01124-7
