
Abstract
Study design
Retrospective cohort study of prospectively registered and collected data.
Objectives
To compare the outcomes of people with a traumatic spinal cord injury (SCI) or cauda equina injury (CEI).
Setting
Victorian State Trauma System, Australia.
Methods
People from the Victorian State Trauma Registry (VSTR) with a diagnosis of traumatic SCI below T4 or CEI, with a date of injury from 2010 to December 2022, were included. Participants were divided into two groups; upper motor neuron (UMN) and lower motor neuron (LMN) injury groups. Demographic, injury event, and hospital details were extracted. Follow-up was conducted by the registry up to 24-months post injury, including the World Health Organization Disability Assessment Schedule (WHODAS), EuroQol EQ-5D scale, and return to work.
Results
Of the 1156 participants, 1113 were categorised as UMN, and 43 as LMN. Within both groups, the demographics were similar. Mixed effect regression modelling of the EQ-5D outcomes over time showed little improvement for both groups. The return to work rate was higher for the LMN injury group at all follow-up time points, with 57% of the UMN injury group returning to work at 24 months post-injury compared to 72% of the LMN injury group. At 24 months post-injury, 63% of people in the UMN injury group reported a WHODAS score equal or greater to ten, compared to 65% in the LMN injury group.
Conclusion
The patient demographics within the two groups were similar. Overall quality of life outcomes remained similarly poor over time for both groups, with little improvement.
Similar content being viewed by others


Introduction
The incidence of Spinal Cord Injury (SCI) in Australia is estimated to be between 21 and 32.3 per million per year and costs Australia $3.7 billion annually, reflecting the significance and severity of these injuries [1, 2]. A SCI or cauda equina injury (CEI) can occur following trauma, such as a road traffic crash or a fall [3]. Injuries to the spinal cord or conus medullaris are upper motor neuron (UMN) injuries and form part of the central nervous system. The cauda equina is the continuation of the end of the spinal cord, and forms part of the lower motor neuron (LMN) or peripheral nervous system. The presentation of both UMN and LMN injuries differs, as does the potential degree of recovery [4, 5].
The overall neurological impacts of these injuries can be devastating, and can result in impairment of the motor, sensory, and autonomic systems, depending on the level and extent of injury [6, 7]. Motor dysfunction can result in weakness or paralysis, sensory dysfunction can result in paraesthesia and anaesthesia, and autonomic dysfunction encompasses issues with bowel and bladder sphincter control, sexual function, autonomic dysreflexia, cardiovascular and respiratory function [6, 7]. These physical impairments can then impact on overall quality of life, mental health and participation in society [8].
Whilst SCI outcomes due to trauma have been documented, few studies have compared outcomes between higher and lower levels of traumatic SCI [3, 9,10,11,12]. Several studies reported a greater degree of neurological recovery in people with CEI and/or conus medullaris injury (CMI), than people with a higher-level SCI [3, 10, 12]. However, these findings differ to a cohort study by Kaneda et al., which reported greater improvement in motor outcomes in people with a SCI than people with a CMI or CEI [11]. Some studies have also shown no difference in overall functional or health quality of life outcomes between the different levels of SCI and CEI [3, 12]. The aim of this population-based study was to elucidate the epidemiology and longer-term outcomes of people with a traumatic UMN and LMN spinal injury. The hypothesis is that people with a traumatic LMN spinal injury should have a greater level of recovery than people with an UMN injury.
Methods
Setting
This was a retrospective cohort study of prospectively registered and collected data. Data from the population-based, Victorian State Trauma Registry (VSTR) was used. The VSTR was established in 2001 and collects data on all major trauma patients from the state of Victoria in Australia, which has a population of 6.9 million people [13, 14]. The VSTR collects data from all 138 trauma receiving hospitals in the Victorian State Trauma System (VSTS), including the three designated major trauma services (Level 1 trauma centre equivalent) [15]. Provision of data to the VSTR is mandatory for trauma-receiving hospitals. The major trauma inclusion criteria include death following injury, an Injury Severity Score (ISS) score greater than 12, 24 h or greater length of intensive care unit (ICU) stay and requiring mechanical ventilation, urgent surgery, and burns equal or greater to 20% of the total body surface area [16]. In the VSTS, Ambulance Victoria provides ambulance transport and retrieval of trauma patients, with patients triaged according to trauma guidelines [17]. The VSTR has ethics approval from the Department of Health and Department of Families, Fairness and Housing Human Research Ethics Committee to operate this registry. Ethics approval for this study was given by the Monash University Human Research Ethics Committee (project number 42181, approval date: 09/04/2024). This study only used non-identifiable data from a registry, thus informed consent was not sought from participants.
Participants and procedures
All major trauma patients in Victoria are assigned both an Abbreviated Injury Scale (AIS) 2008 revision, and an International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification (ICD-10-AM) code. The AIS is collected by train health coders at individual hospital sites or by Monash University. The ICD-10-AM is routine coding undertaken for all hospital admissions and is done by trained coders employed by individual health services.
Participants were included in this study if they met the following criteria
-
I.
Adults aged 16 years and over.
-
II.
Injury date from January 2010 to December 2022.
-
III.
An AIS or ICD-10-AM code for any spinal cord injury at or below T4 and patients with a cauda equina injury diagnosis, were included in this study (see supplementary materials Appendix 1 for specific injury codes).
Participants were excluded if the following were present
-
I.
A concomitant injury to the cervical spinal cord based on AIS and ICD-10-AM codes and text descriptors.
-
II.
A code for lumbar spinal cord injury without a level of injury specified.
Patients with a SCI from L1 to T4 inclusive, or conus medullaris injury, were assigned to the upper motor neuron (UMN) injury group. Patients with a code for cauda equina or participants coded as having a spinal cord injury L2 and below were assigned to the lower motor neuron (LMN) injury group. A cut-off of L2 has been used by similar studies, and the L1 region has been described as the median location for the conus medullaris in adults [9, 18]. People who had concomitant UMN injury and an LMN injury were assigned to the UMN injury group, as clinically these patients would exhibit UMN signs [19].
The data extracted from the VSTR included demographic, injury event, hospital stay and patient-reported outcome variables. Participants were classified to metropolitan or regional area of residence based on their residential postcode and the Accessibility/Remoteness Index of Australia (ARIA). [20] Participants’ residential postcodes were also assigned an Index of Relative Socio-Economic Advantage and Disadvantage (IRSAD) quintile, reflecting the level of disadvantage or advantage of certain areas [21]. The Charlson Comorbidity Index (CCI) reflects a person’s mortality risk due to a set of specific comorbidities based on ICD-10-AM diagnosis codes [22]. A CCI of zero reflects a person with no CCI conditions, whilst a higher CCI weight reflects an increasing risk of death. The CCI weight was categorized to zero, one, or higher than one. The ISS reflects a person’s overall injury severity, with scores ranging from one to 75 [23]. The registry also collects information about procedures and surgeries that are performed for each person. The registry receives the Australian Classification of Health Interventions (ACHI) procedure code and registry coders also allocate Victorian State Trauma Outcomes Registry and Monitoring Group (VSTORM) procedure codes, which reflect the treatment they received in hospital for their injuries. The Australian Classification of Health Interventions and VSTORM procedure codes were used to identify a relevant spinal operation, including spinal decompression, open and closed reductions, spinal fusions and internal fixation of the spine. This spinal surgery variable was collapsed into a binary variable, with patients classified as either receiving or not receiving spinal surgery during their hospital stay. The length of stay variable categories were based on quartiles.
Routine follow-up occurs at six, 12- and 24-months post injury by registry staff, using either telephone or online questionnaires [24]. A proxy may be used if the patient is unable to complete the interview themselves. Several phone calls are attempted before a person is deemed to be lost to follow-up. Deaths following hospital discharge are identified by linkage with the Victorian Registry of Deaths, Births and Marriages.
A commonly used and validated tool to explore health status is the EuroQol EQ-5D, which collects information about mobility, self-care, usual activities, pain and/or discomfort, and anxiety and/or depression [25]. The VSTR collects EQ-5D outcomes at each follow-up time point. A three-level and a five-level version of the EQ-5D tool exist, with the VSTR previously using the three-level prior to July 2018. Thus, the five-level version was subsequently mapped to the three-level version to allow for direct collation of data. The three-level version was further collapsed into two groups, due to low cell counts. The VSTR also administers the 12-item WHODAS 2.0 survey, which reflects a patient’s overall level of disability, reflecting the level of disability in the following categories: cognition, mobility, self-care, social interaction, general life activities and social participation [26]. Participants are asked to answer question pertaining to these categories following their experience in the previous 30 days. An overall WHODAS score is assigned to each participant, between zero and 48, with higher scores representing greater disability. In this study the total WHODAS score variable was collapsed into “<10” and “10 + ”, with the “10 + ” score signifying a greater level of disability, and “<10” representing a less severe level of disability [27]. Return to work outcomes are also captured in the follow-up, with patients asked to respond either “yes” or “no” to whether they had returned to work/study, whether they returned to the same workplace, and whether they returned to the same role at the same organization.
Data analysis
Descriptive statistics were used to summarise data. Categorical variables were summarised using frequencies and percentages, whilst normally distributed continuous variables were presented with the mean and standard deviation (SD), and the median and interquartile range (IQR) for non-normal distribution, with missing data highlighted in the tables for each variable. For each point of follow-up of the EQ-5D outcomes, predicted probabilities and 95% confidence intervals were calculated using mixed effects logistic regression modelling with random intercepts. The variables included in the mixed effects logistic regression modelling included the five EQ-5D domain categories and follow-up time, as well as spinal surgery, a binary variable demonstrating whether a participant had spinal surgery during their hospital stay, as a fixed effect. This variable was chosen as it reflects injury severity, such as instability and degree of neurological involvement, and is a known confounder for spine-related outcomes. The output of these models is presented in Appendix 2. Chi square tests were used to compare demographic variables, injury characteristics and outcome variables between the two injury groups, with their corresponding bootstrapped p-values and BCa 95% confidence intervals reported. As there was a substantial difference in the number of UMN and LMN cases, the disproportion between groups limited the power of the study, and bootstrapping was applied to the Chi square test of independence, with 2000 replications and a random seed set [28]. A p-value of <0.05 was considered statistically significant. For statistical analysis, Stata Version 17 (StataCorp, College Station, TX) was used, with all analysis performed in the Monash Secure eResearch Platform (SeRP).
Results
Cohort overview
There were 1156 participants on the VSTR who met the inclusion criteria for this study. Of these people, 47 died during their hospital stay (Fig. 1). The median age of people in the UMN group was 47 years of age, and was 50 years of age for the LMN group. Table 1 shows the key demographic characteristics of the cohort. The cause of injury, whether participants had spinal surgery during their initial hospitalisation, and their discharge destination were found to be statistically significant.

This figure shows the number of participants eligible for the study, as well as follow-up completion rates at each follow-up time point.
Health status outcomes
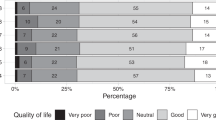
Of the survivors in the overall cohorts, N = 829 (77%) completed six-month follow-up, N = 794 (74%) completed 12-month follow-up and N = 697 (66%) completed 24-month follow-up (Fig. 1). Within the overall cohort at 24- months following injury, most reported some degree of problems on all the EQ-5D items except self-care (Table 2). The proportions of people reporting some degree of problems was similar across all EQ-5D items and time points with both the UMN and LMN injury groups. The proportion of participants reporting problems on the EQ-5D items did not change over time, overall or between groups (Fig. 2). The percentage of people scoring 10 or more on the WHODAS, signifying a greater level of disability, was marginally higher in the LMN injury group than the UMN injury group at all follow-up time pointsbut this difference was not statistically significant (Table 3). Six-hundred forty-two people were working or studying prior to their injury; return to work rates were higher in the LMN injury group than the UMN injury group across all follow-up times points (65 and 45% at six- months, 67 and 54% at 12- months, and 72 and 57% at 24- months for the LMN and UMN injury groups respectively) (Table 4). Of the participants that did return to work, most people in the LMN injury group returned to the same organisation. Within both injury groups, most people returned to the same role if they did return to work.

Each graph displays the proportions and 95% confidence intervals at each time point. A graph is shown for each injury group for each EQ-5D item.
Discussion
Key findings
In this population-based study, there were important differences in the causality of UMN and LMN injuries. Road trauma was the leading cause of injury for the UMN injury group, while a low fall or fall from standing height was the leading cause for the LMN injury group. In our study, the overall quality of life outcomes is represented by the EQ-5D and WHODAS outcome measures, and show similarly poor outcomes between the two groups. When considering the EQ-5D items, there seems to be little improvement over time in the UMN injury group, and improvement in the LMN injury groups is unclear. Overall, there were higher rates of return to work in the LMN injury group than the UMN injury group at every time point, with a majority of people in both injury groups returned to work at 24- months.
Whilst our study found most UMN injuries were caused by road trauma, a low fall or fall from standing height was the leading cause for LMN injuries. This contrasts with a retrospective cohort study of traumatic thoracolumbar spinal injuries by Kingwell et al, that found thoracic SCI below T11 inclusive and CMI were mostly due to falls (47 and 50% respectively), whilst CEI were caused equally by road traffic incidents (42%) and falls (42%) [3]. However, our results are consistent with the broader Victorian major trauma cohort, where the leading cause of major trauma is low falls in people aged over 64 years of age, followed by road trauma and falls from a height of more than one metre [16].
The EQ-5D tool has not been used in other comparative studies, however, differences in mobility have been reported on previously [3, 11, 12]. The current article showed little improvement in the EQ-5D item of mobility over time for both injury groups, with most reporting some degree of problems at all time points. This contrasts with the existing literature, where overall, people with CEI and/or CMI had better motor recovery than people with SCI. Kingwell et al. described worse motor improvement for people with a SCI and CEI than for people with a CMI, using a classification system assigning injury groupings based on MRI localisation of the Conus Medullaris. However, when these authors classified the level of injury based on vertebral levels, Kingwell et al. found no difference in motor improvement between these three groups [3]. Similarly, a prospective cohort study by Brouwers et al. described worse motor recovery for people with SCI than those with conus medullaris syndrome (CMS), and reported a difference in outcome of mobility, using the Spinal Cord Independence Measure (SCIM) sub-score for mobility indoors for SCI and cauda equina syndrome (CES), and between CMS and CES [12]. However, a retrospective cohort study by Kaneda et al. found better motor recovery in people with SCI than with CEI, however the motor score was worse at the final follow-up in people with SCI than people with CEI [11].
There is no clear consensus from the literature in regard to overall neurological outcomes between different levels of injury, and comparison is difficult due to the use of disparate tools. In our study, the WHODAS provides an overall disability measure, and shows little improvement over time for both injury groups. Similarly, the EQ-5D outcomes show little improvement for the UMN injury group, with outcomes unclear for the LMN injury group, however in both groups, a majority reported some degree of problems on all the EQ-5D items except self-care. A retrospective cohort study by Hashimoto et al. described worse overall neurological outcomes for people with epiconus lesions than people with cous medullaris or cauda equina lesions within two months of follow-up post-injury [10]. These findings contrast to those of Brouwers et al., who reported no difference in overall neurological outcomes using the SCIM between people with CES, CMS and SCI [12]. Similarly, a retrospective cohort study of different SCI syndromes by McKinely et al. found no difference in outcomes using the Functional Independence Measure score, rehabilitation length of stay or discharge disposition between patients with cauda equina syndrome and CMS, however these outcomes cannot be attributed specifically to a traumatic aetiology, as this study included patients with non-traumatic causes of injury [29]. A narrative literature review by Kingwell et al. also concluded that traumatic CEI and CMI have similar neurological outcomes [9]. Overall, previous articles in the literature report either no difference in overall neurological outcomes between different groups or in those that do report a difference in outcomes, it seems that SCI neurological outcomes are worse than outcomes reported for CMI and/or CEI.
The current article demonstrated most people returned to work at 24- months after injury in both groups, with higher rates of return in the LMN injury group. Comparison to existing literature is challenging, as to the authors’ knowledge, no comparison between traumatic SCI groups and return to work outcomes has been described.
Strengths
Our study is a novel contribution to the literatures. Firstly, the unique grouping of comparing spinal cord lesions to lower motor neuron lesions of the cauda equina, presents a distinct method of comparing different levels of spinal injury. By separating people with CEI from true spinal cord lesions, we were better able to compare the recoverability of the peripheral nervous system compared to the central nervous system. It is hypothesised peripheral nervous system injuries have a better ability to recover than central nervous system injuries [30]. Other key strength are the use of a population-based cohort, the longitudinal design, and comparison across multiple patient-centred outcomes.
Limitations
Our study had several limitations. Whilst attempts were made to include patients with a functional spinal injury below the level of T4, there may be a small number of patients who have had a concomitant higher-level thoracic injury. Comparison between the UMN and LMN injury groups was difficult due to an imbalance between the two groups, with a low prevalence of LMN injury in the overall cohort. A limitation of this study is the L1 vertebral level cut-off for assigning participants to either the upper or lower motor neuron injury groups. The L1 cut-off was based upon the reported average location of the conus medullaris [18, 31,32,33,34]. Furthermore, the L1 vertebral level was the most common level for the conus medullaris in five studies [31, 35,36,37,38]. However, its termination is variable, with a range of vertebral levels T11/12 to L3 reported in the literature [31,32,33, 35,36,37]. As a result, it is possible some cases of isolated cauda equina injuries were thus misclassified as upper motor neuron injuries in our study. The effect of the misclassification may dilute the differences between the two group, affecting result validity and potentially bias the results towards the null. The sample size for this study limited the number of potential confounding variables to be included in the mixed effects regression models. However, the inclusion of spinal surgery variable as a fixed effect, accounted for injury severity and the baseline difference between the two injury groups with regards to spinal surgery.
Further research is needed to more conclusively draw conclusions around recovery between different levels of spinal cord injury. In particular, consistent definitions and allocations of participants to SCI, CMI and CEI groupings are needed to enable better comparison. Most of the current research has focussed on motor recovery, with more research needed on other known complications including bowel, sex and sensory dysfunction.
Conclusion
In conclusion, the demographics of patients within the UMN and LMN injury groups were similar except for the cause of injury. Overall health quality of life outcomes remained similarly poor over time for both injury groups, with little improvement in outcomes over time.
Data availability
Data is available from the corresponding author upon reasonable request.
Code availability
Stata Version 17 code is available upon reasonable request.
References
New PW, Baxter D, Farry A, Noonan VK. Estimating the incidence and prevalence of traumatic spinal cord injury in Australia. Arch Phys Med Rehabil. 2015 Jan;96:76–83.
AlphaBeta Australia. Spinal Cord Injury in Australia; 2020. Available at: https://treasury.gov.au/sites/default/files/2021-05/171663_the_australian_spinal_cord_injury_research_collaborative_supporting_document_3.pdf. Accessed April 15, 2025.
Kingwell SP, Noonan VK, Fisher CG, Graeb DA, Keynan O, Zhang H, et al. Relationship of neural axis level of injury to motor recovery and health-related quality of life in patients with a thoracolumbar spinal injury. J Bone Jt Surg Am. 2010;92:1591–9.
Tator CH, Duncan EG, Edmonds VE, Lapczak LI, Andrews DF. Comparison of surgical and conservative management in 208 patients with acute spinal cord injury. Can J Neurol Sci. 1987;14:60–69.
Zayia LC, Tadi P Neuroanatomy, Motor Neuron. 2023. StatPearls Publisihing. Available at: https://www.ncbi.nlm.nih.gov/books/NBK554616/. Accessed April 15, 2025.
Henke AM, Billington ZJ, Gater DR. Autonomic dysfunction and management after spinal cord injury: a narrative review. J Pers Med. 2022;12:1110.
Rupp R Chapter 6 - Spinal cord lesions. In: Ramsey NF, Millán JdR, ed. Handbook of Clinical Neurology: Elsevier; 2020:51-65.
Halvorsen A, Pape K, Post MWM, Biering-Sørensen F, Mikalsen S, Hansen AN, et al. Participation and quality of life in persons living with spinal cord injury in Norway. J Rehabil Med. 2021;53:jrm00217.
Kingwell SP, Curt A, Dvorak MF. Factors affecting neurological outcome in traumatic conus medullaris and cauda equina injuries. Neurosurg Focus. 2008;25:E7.
Hashimoto T, Kaneda K, Abumi K. Relationship between traumatic spinal canal stenosis and neurologic deficits in thoracolumbar burst fractures. Spine. 1988;13:1268–72.
Kaneda K, Taneichi H, Abumi K, Hashimoto T, Satoh S, Fujiya M. Anterior decompression and stabilization with the Kaneda device for thoracolumbar burst fractures associated with neurological deficits. J Bone Jt Surg Am. 1997;79:69–83.
Brouwers E, Meent HV, Curt A, Maier DD, Abel RF, Weidner N, et al. Recovery after traumatic thoracic- and lumbar spinal cord injury: the neurological level of injury matters. Spinal Cord. 2020;58:980–7.
Australian Bureau of Statistics. National, state and territory population. 2024. Available at: https://www.abs.gov.au/statistics/people/population/national-state-and-territory-population/latest-release. Accessed April 15, 2025.
About the Victorian State Trauma Registry. Department of Health. Available at: https://www.health.vic.gov.au/patient-care/victorian-state-trauma-registry. Accessed April 15, 2025.
Victorian State Trauma System. Trauma Victoria. Available at: https://trauma.reach.vic.gov.au/guidelines/victorian-trauma-system/key-messages. Accessed April 15, 2025.
Victorian State Trauma Registry Annual Report 2021-2022. Melbourne, Victoria, 2021-2022.
Adult Retrieval Victoria. Ambulance Victoria. Available at: https://www.ambulance.vic.gov.au/about-us/our-services/adult-retrieval-victoria/. Accessed April 15, 2025.
Brouwers E, van de Meent H, Curt A, Starremans B, Hosman A, Bartels R. Definitions of traumatic conus medullaris and cauda equina syndrome: a systematic literature review. Spinal Cord. 2017;55:886–90.
Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves DE, Jha A, et al. International standards for neurological classification of spinal cord injury (Revised 2011). J Spinal Cord Med. 2011;34:535–46.
Remoteness Areas. Australian Bureau of Statistics. Available at: https://www.abs.gov.au/statistics/standards/australian-statistical-geography-standard-asgs-edition-3/jul2021-jun2026/remoteness-structure/remoteness-areas#:~:text=Relative%20geographic%20remoteness%20is%20measured,proxy%20measure%20for%20service%20availability. Accessed April 15, 2025.
IRSAD. Australian Bureau of Statistics. Available at: https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/2033.0.55.001~2016~Main%20Features~IRSAD~20. Accessed April 15, 2025.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–83.
Garcia MF, Gomes RT, Pugliesi EC, Dos Santos JPV, De Martino F, Gomes KHV, et al. Comparison between Injury Severity Score (ISS) and New Injury Severity Score (NISS) in predicting mortality of thoracic trauma in a tertiary hospital. Rev Col Bras Cir. 2024;51:e20243652.
Gabbe BJ, Hart MJ, Brown A, McLellan S, Morgan MJ, Beck B, et al. Does patient preference for online or telephone follow-up impact on response rates and data completeness following injury? J Trauma Acute Care Surg. 2022;93:679–85.
EuroQol Research Foundation. EQ-5D-5L User Guide, 2019. Available from: https://euroqol.org/publications/user-guides. Accessed April 15, 2025.
Andrews G, Kemp A, Sunderland M, Von Korff M, Ustun TB. Normative data for the 12 item WHO Disability Assessment Schedule 2.0. PLoS One. 2009;4:e8343.
Zubenko X, Liew S, Reeder S, Yang Y, Humadi A, Gabbe B. The incidence and outcomes of traumatic cauda equina syndrome in Victoria, Australia. N Am Spine Soc J. 2024;20:100558.
Lin JJ, Chang CH, Pal N. A revisit to contingency table and tests of independence: bootstrap is preferred to Chi-square approximations as well as Fisher’s exact test. J Biopharm Stat. 2015;25:438–58.
McKinley W, Santos K, Meade M, Brooke K. Incidence and outcomes of spinal cord injury clinical syndromes. J Spinal Cord Med. 2007;30:215–24.
Tator CH. Biology of neurological recovery and functional restoration after spinal cord injury. Neurosurgery. 1998;42:696–707.
Liu A, Yang K, Wang D, Li C, Ren Z, Yan S, et al. Level of conus medullaris termination in adult population analyzed by kinetic magnetic resonance imaging. Surg Radiol Anat. 2017;39:759–65. https://doi.org/10.1007/s00276-017-1813-3
Saifuddin A, Burnett SJ, White J. The variation of position of the conus medullaris in an adult population. a magnetic resonance imaging study. Spine. 1998;23:1452–6. https://doi.org/10.1097/00007632-199807010-00005
Soleiman J, Demaerel P, Rocher S, Maes F, Marchal G. Magnetic resonance imaging study of the level of termination of the conus medullaris and the thecal sac: influence of age and gender. Spine. 2005;30:1875–80. https://doi.org/10.1097/01.brs.0000174116.74775.2e
Rider LSME Cauda Equina and Conus Medullaris Syndromes. StatPearls. StatPearls Publishing; 2023.
Nakashima H, Ito K, Katayama Y, Tsushima M, Ando K, Kobayashi K, et al. The level of conus medullaris in 629 healthy Japanese individuals. J Clin Med. 2021;10:3182 https://doi.org/10.3390/jcm10143182
Nasr AY. Vertebral level and measurements of conus medullaris and dural sac termination with special reference to the apex of the sacral hiatus: anatomical and magnetic resonance imaging radiologic study. Folia Morphol. 2016;75:287–99. https://doi.org/10.5603/FM.a2016.0004
Elfiky T, El Mansy Y, Stienen MN, Yunusa S, Elkaref E, Nafady M. Magnetic resonance imaging-based anatomy of the conus medullaris: variations of location and morphology. World Neurosurg. Mar 2025;195:123646 https://doi.org/10.1016/j.wneu.2024.123646
Harrop JS, Hunt GE Jr., Vaccaro AR. Conus medullaris and cauda equina syndrome as a result of traumatic injuries: management principles. Neurosurg Focus. 2004;16:e4.
Acknowledgements
There are no additions sources of technical assistance, critical advice or other assistance to acknowledge.
Funding
The Victorian State Trauma Registry (VSTR) is funded by the Department of Health, State Government of Victoria and the Transport Accident Commission. Belinda Gabbe was supported by a National Health and Medical Research Council of Australia Investigator Grant (ID 2009998). Open Access funding enabled and organized by CAUL and its Member Institutions.
Author information
Authors and Affiliations
Contributions
XB was responsible for designing the study, analysing the data and wrote the manuscript. SL helped with the initial design of the study and provided feedback on the manuscript. SR helped with the initial design of the study and provided feedback on the manuscript. JD helped with the data analysis and interpretation of the data for the work, and provided feedback on the manuscript. BG helped with the initial design of the study and provided feedback on the manuscript. All authors gave approval of the version to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
Ethics approval for this study was given by the Monash University Human Research Ethics Committee (project number 42181). All methods were performed in accordance with the relevant guidelines and regulations
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Beaumont, X., Liew, S., Reeder, S. et al. Comparison of health outcomes between traumatic spinal cord and cauda equina injuries. Spinal Cord (2026). https://doi.org/10.1038/s41393-026-01191-4
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41393-026-01191-4
