
Abstract
Several studies have demonstrated that the severity of social communication problems, a core symptom of Autism Spectrum Disorder (ASD), is correlated with specific speech characteristics of ASD individuals. This suggests that it may be possible to develop speech analysis algorithms that can quantify ASD symptom severity from speech recordings in a direct and objective manner. Here we demonstrate the utility of a new open-source AI algorithm, ASDSpeech, which can analyze speech recordings of ASD children and reliably quantify their social communication difficulties across multiple developmental timepoints. The algorithm was trained and tested on the largest ASD speech dataset available to date, which contained 99,193 vocalizations from 197 ASD children recorded in 258 Autism Diagnostic Observation Schedule, Second edition (ADOS-2) assessments. ASDSpeech was trained with acoustic and conversational features extracted from the speech recordings of 136 children, who participated in a single ADOS-2 assessment, and tested with independent recordings of 61 additional children who completed two ADOS-2 assessments, separated by 1–2 years. Estimated total ADOS-2 scores in the test set were significantly correlated with actual scores when examining either the first (r(59) = 0.544, P < 0.0001) or second (r(59) = 0.605, P < 0.0001) assessment. Separate estimation of social communication and restricted and repetitive behavior symptoms revealed that ASDSpeech was particularly accurate at estimating social communication symptoms (i.e., ADOS-2 social affect scores). These results demonstrate the potential utility of ASDSpeech for enhancing basic and clinical ASD research as well as clinical management. We openly share both algorithm and speech feature dataset for use and further development by the community.
Similar content being viewed by others


Introduction
Autism Spectrum Disorder (ASD) is diagnosed by the presence of social communication difficulties and the existence of Restricted and Repetitive Behaviors (RRBs) [1]. Most ASD children exhibit language delays during early childhood [2], with 25–30% remaining minimally verbal (i.e., use < 50 words) throughout childhood [3]. However, core ASD symptoms are not necessarily evident in the amount of speech produced by an individual and may instead be evident in the way they speak. Some ASD children exhibit poorer fluency [4], echolalia (i.e., speech repetition) [5], mix pronouns [6], and use atypical articulation and prosody [7, 8] that are apparent in the acoustic features of their vocalizations [9, 10]. Studies have reported, for example, that verbal ASD children tend to speak with higher pitch and larger pitch variability than typically developing (TD) children [8, 9]. ASD children also exhibit significantly fewer phoneme vocalizations [11], fewer conversational turns (i.e., reciprocating in a conversation) [11,12,13], more non-speech vocalizations [12, 14], more distressed vocalizations (crying, screaming) [15], and a lower ratio of syllables to vocalizations [16] than TD children.
Several studies have used automated speech analysis techniques to classify ASD and TD children based on extracted speech features [17,18,19,20,21,22,23,24]. In some studies, diagnostic classification was based on linguistic features such as vocabulary and fluency [24] while in others it was based on acoustic features such as pitch [18,19,20, 22, 23], jitter [20, 23], shimmer [20, 23], energy [18, 19], Zero-Crossing Rate (ZCR) [18, 19], and Mel-Frequency Cepstral Coefficients (MFCCs) [19].
Three recent studies have extended this research by training machine and deep learning algorithms to estimate ASD severity according to extracted speech features. In all these studies ground truth was established by clinicians using the Autism Diagnostic Observation Schedule Second edition (ADOS-2), a semi-structured assessment where clinicians score the behavior of children during specific tasks/games [25]. The ADOS-2 yields a total severity score as well as separate Social Affect (SA) and Restricted and Repetitive Behaviors (RRB) scores that quantify social difficulties and RRB symptoms, respectively. In one recent study, the authors extracted vocalization rates and durations from speech recordings of 33 ASD children during an ADOS-2 assessment and reported that a trained synthetic random forest model was able to accurately estimate their ADOS-2 Social Affect (SA) scores [26]. Another study extracted hundreds of conversational, acoustic, and lexical speech features from speech recordings of 88 adolescents and adults with ASD during an ADOS assessment (First edition) and reported that a trained Deep Neural Network (DNN) was able to accurately estimate scores of four specific ADOS items that quantify the ability to maintain a mature social conversation [27]. Finally, in a third study, from our group, we extracted acoustic features such as pitch and energy, and conversational features such as turn-taking and speech rate from speech recordings of 72 children (56 with ASD) during an ADOS-2 assessment [28]. We demonstrated that a trained Convolutional Neural Network (CNN) model was able to accurately estimate total ADOS-2 scores across multiple train-test subsamples.
While these results are encouraging, algorithms developed so far were trained and tested with relatively small ASD samples that are not likely to represent the large heterogeneity of speech styles and characteristics in the broad ASD population [9]. Moreover, previous studies examined only a single timepoint of data from each participant, thereby limiting the ability to assess the reliability of algorithms to assess ASD symptom severity at different developmental timepoints. Previous studies also did not compare the ability of deep learning models to successfully estimate the severity of social ASD symptoms versus RRB symptoms. Most importantly, previous studies did not share their algorithms and data in a transparent manner that would enable re-production of results and further development of algorithms by the research community.
To address these limitations, we created the largest speech recording dataset available to date, which contained 99,193 vocalizations from 197 ASD children recorded in 258 ADOS-2 assessments, with 61 of the children participating in two ADOS-2 assessments that were separated by 1–2 years. This comprehensive dataset enabled us to train and test the ASDSpeech algorithm on different subsets of children and compare its accuracy across two developmental timepoints as well as sex and age sub-groups. In addition, we also examined the ability to estimate ADOS-2 SA versus RRB scores (i.e., social difficulties versus RRB symptoms). We intentionally used raw ADOS-2 scores, which have a considerably wider range than ADOS-2 calibrated severity scores [29, 30], thereby increasing the potential sensitivity of the algorithm. Finally, we openly share the algorithm and speech feature dataset to promote transparency and enable further use and development by the research community.
Methods
Participants and setting
We analyzed data collected at the Azrieli National Centre for Autism and Neurodevelopment Research (ANCAN), a collaboration between Ben-Gurion University of the Negev (BGU) and eight partner clinical centers where ASD is diagnosed throughout Israel. ANCAN manages the national autism database of Israel with data from >3000 children in 2023 and growing [31, 32]. All recordings used in the current study were performed in a single ANCAN assessment room located at Soroka University Medical Center (SUMC), the largest partner clinical site. A total of 197 children (1–7-years-old) who completed at least one ADOS-2 assessment between 2015 and 2021 and received an ASD diagnosis were included in this study (Table 1). Of the participating children, 136 completed a single ADOS-2 assessment and 61 completed two ADOS-2 assessments at two timepoints separated by 10–29 months, yielding 258 ADOS-2 assessments in total. All ADOS-2 assessments were performed by a clinician with research reliability. In addition, all participating children received an ASD diagnosis from both a developmental psychologist and a child psychiatrist or pediatric neurologist, according to Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria [33] and received ADOS-2 Calibrated Severity Score (CSS) ≥3 at their assessments.
ADOS-2 assessments
ADOS-2 is a semi-structured behavioral assessment where a clinician administers specific tasks, observes the behavior of the child, and scores their behavior [25]. The total ADOS-2 score (range: 0–30) is the sum of the Social Affect (SA, range: 0–22) and Restricted and Repetitive Behavior (RRB, range: 0–8) scores, with higher scores indicating more severe symptoms. In addition, it is possible to compute CSS scores (range: 1–10) from total, SA, and RRB scores to standardize autism severity across ages and language levels that differ across ADOS-2 modules [34].
Recording setup
All ADOS-2 recordings were performed using a single microphone (CHM99, AKG, Vienna) located on a wall, ~1–2 m from the child, and connected to a sound card (US-16x08, TASCAM, California). Each ADOS-2 session lasted ~ 40-min (40.75 ± 11.95 min) and was recorded at a sampling rate of 44.1 kHz, 16 bits/sample (down-sampled to 16 kHz).
Detection of child vocalizations
Recordings were manually annotated to identify segments with each child’s vocalizations. We chose to use manual annotation rather than automated diarization, because current diarization algorithms for children’s speech in noisy environments exhibit low accuracy with error rates of ~30% even when analyzing recordings of older children [35, 36]. We would expect error rates in recordings of young ASD children to be even higher.
We instructed the manual annotators to label segments that contained the child’s speech, laughing, moaning, crying, or screaming (i.e., any vocalization). To assess the accuracy of manual labeling we examined inter-rater reliability across two raters who labeled child vocalizations within the same 10-min recordings of 25 children. This analysis yielded an inter-rater accuracy of 88.48% ± 5.97, kappa of 0.60 ± 0.13, and F1 score of 79.56% ± 15.82.
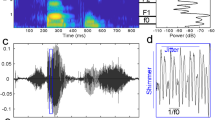
Manually annotated child segments often contained multiple vocalizations (e.g., multiple utterances) separated by silence (Supplementary Fig. S1). Each segment was separated into multiple vocalizations using energy thresholds relative to the background noise. Specifically, the start of a vocalization was defined as the point where the energy level exceeded 2.79 dB + Eb for at least 50 ms, and the end was marked when the energy exceeded 0.4 dB + Eb for 50 ms (Eb = background noise energy throughout the recording) [28]. The background noise equaled the most frequent energy level within each recording, based on the assumption that vocalizations are sparse. Vocalizations that were shorter than 110 ms were excluded from further analysis (too short to contain an utterance).
Features
We extracted 49 speech features from the child vocalizations that were categorized into nine groups: pitch, formants, jitter, voicing, energy, Zero-Crossing Rate (ZCR), spectral slope, duration, and quantity/number of vocalizations. All features, except duration and quantity, were first extracted in 40 ms windows (window overlap of 75%), resulting in a vector of feature values per vocalization. The minimum, the maximum, and the mean pitch of the voiced vocalizations (across windows) were computed, deriving one value for each vocalization. We then selected a group of 10 consecutive vocalizations and computed the mean and variance across vocalizations for relevant features (Supplementary Table S1). We also computed the mean duration of vocalizations and the overall number of vocalizations in the recording. Taken together, these steps yielded a vector with 49 values corresponding to the 49 features per 10 vocalizations. We performed this procedure 100 times, selecting random groups of ten consecutive vocalizations from the recording. Combining these 100 samples yielded a features matrix of 100×49 per child (Supplementary Fig. S2), with the last column (quantity of vocalizations) containing the same value across all rows. Features included:
Frequency related features:
-
Pitch (F0): Vocal cords vibration frequency (the fundamental frequency) that exists only in voiced speech (e.g., vowels). Voiced Vocalization (VV) was defined as a vocalization where most of its frames (≥ 60%) [10] were voiced (voicing threshold 0.45).
-
Formants: The resonant frequencies of the vocal tract that shape vowel sounds [37]. The first two formants (F1 and F2) relate to tongue position (vertical and horizontal) and influence vowel quality. Their bandwidths affect the clarity of speech.
-
Jitter: Variation across adjacent pitch values representing frequency instability [38].
-
Voicing: Pitch peak amplitude as determined by the autocorrelation function.
Pitch and formants were calculated using the PRAAT software [39], with a pitch range set to 60–1600 Hz (a wide range to increase sensitivity to atypical vocal characteristics).
Energy/amplitude related features:
-
Energy: We computed the energy ratio between each child’s vocalization and the background noise level to normalize this feature across recordings performed on different days where background noise may have varied. The background noise equaled the most frequent energy level within each recording, based on the assumption that vocalizations are sparse.
Spectral features:
-
Zero-Crossing Rate (ZCR): The number of zero-crossings apparent in audio segments with child vocalizations [40].
-
Spectral slope: The slope of the linear regression on the logarithmic power spectrum within the frequency bands of 20–500 Hz (lower band) and 500–1500 Hz (higher band) [41, 42].
Conversational features:
-
Duration: Child’s mean vocalization length.
-
Quantity: The total number of vocalizations.
All features, except for Pitch and Formants, were extracted with custom-written code in Matlab (Mathworks, Inc.).
Training and testing ASDSpeech
Training was performed with data from the 136 children who completed a single ADOS-2 session only. Feature matrices were used to train two deep learning models with an identical CNN architecture (Supplementary Fig. S3). The first model estimated ADOS-2 SA scores and the second estimated ADOS-2 RRB scores. Training was based on minimizing the Mean Squares Error (MSE) of a regression analysis between estimated and actual scores, using the RMSprop (Root Mean Square Propagation) as the optimization algorithm [43]. The training process was preformed 25 times, creating 25 different SA and 25 RRB models that were trained with different combinations of training data sub-samples and learning parameters. We considered this analogous to having 25 clinicians, each with a different learning style and different clinical experience. First, we performed the feature extraction procedure described above five times for each child. Since feature extraction included a random selection of consecutive vocalizations, this resulted in five different sub-samples of the data. When training each model (separately for SA and RRB) we split the training data into a training-set (80%) and validation set (20%) and applied a random search algorithm to optimize the following learning parameters: batch size, number of epochs, and learning rate, while applying early stopping of patience after 20 epochs to reduce overfitting [44]. Optimal learning hyper-parameters were selected based on the highest concordance correlation coefficient [45], between estimated and actual ADOS-2 scores in the training and validation sets respectively. This procedure was performed five times using different selections of validation data (i.e., 5-fold cross validation), yielding 5 models with different learning parameters per data sub-sample and 25 models in total for SA and RRB scores separately.
Testing was performed with an entirely independent dataset of 61 ASD children who completed two ADOS-2 assessments. For each of these children we estimated a separate SA and RRB score from each of the 25 models described above and then computed their mean, yielding a single SA and RRB score per child. This is analogous to a clinical consensus across the 25 models. Accuracy of ASDSpeech estimation was measured using Pearson correlation and NRMSE (RMSE / (ymax - ymin), where y is the actual ADOS-2 score), which were calculated between the estimated and actual ADOS-2 scores in the testing dataset, separately for the first and second ADOS-2 assessments (i.e., T1 and T2).
In addition, we trained and tested additional models to estimate ADOS-2 total, SA, and RRB CSS instead of raw scores while using the same procedures described above.
Estimating feature importance
We assessed the importance of specific features for accurately estimating ADOS-2 scores by excluding each feature from the testing dataset and checking the impact on the model’s accuracy. We replaced the values of individual features in the test data with zeros, one feature at a time, and then checked the model's performance by computing the correlation between estimated and real total ADOS-2 scores (Supplementary Fig. S5). The performance degradation resulting from excluding each feature provided an estimate of that feature’s importance, with larger reductions in correlation indicating higher importance of the feature.
Hardware
All model training, optimization, and training were performed using custom-written code in Python 3.9.13 using a Keras API 2.6.0 with TensorFlow (version 2.6.0) backend. The training was conducted on an IntelI XI(R) Gold 6140 CPU@2.30GHz and NVIDIA GPU Tesla T4.
Statistical analysis
All statistical analyses were conducted using custom-written code in Python. Associations between each of the features and ADOS-2 scores were quantified using Pearson correlations. To evaluate their statistical significance, we performed a random permutation test where we randomly shuffled the actual ADOS-2 scores across children before calculating the correlation with each feature. This non-parametric randomization procedure was performed 1,000 times, generating a null distribution of correlation values expected by chance when using the sample distribution of ADOS-2 scores that was not necessarily normal (a necessary pre-requisite for parametric statistical tests). For a correlation between a speech feature and ADOS-2 score to be considered significant, the actual correlation value had to exceed the 97.5 percentile of the null distribution. We used an equivalent analysis to assess the statistical significance of correlations between actual and estimated ADOS-2 scores. We also performed a similar analysis with NRMSE values, where we assessed whether the actual NRMSE value was smaller than the 2.5 percentile of the null distribution. These statistical tests assessed whether correlation values were higher than expected by chance and NRMSE values were lower than expected by chance.
To determine the significance of a feature for accurate estimation of ADOS-2 scores, we performed the following bootstrap procedure. We drew 61 samples (with replacement) from the test set and calculated the Pearson correlation between actual and estimated ADOS-2 scores once while including all features and again when excluding one feature (i.e., setting its values to zero). We repeated this procedure 1000 times and computed the difference in correlation values per iteration, yielding a distribution of 1000 values representing the difference in accuracy when removing a feature. For the feature to be considered significantly important, 97.5% of the difference distribution had to exceed zero.
We also used the same analysis to determine the significance of accuracy differences across estimations of SA and RRB scores, estimations of male and female children, and estimations of younger and older children. In all cases we used the same bootstrapping procedure to select subgroups of 61 children (with replacement) and computed the Pearson correlation between actual and estimated ADOS-2 scores per iteration. We then computed the correlation difference across groups (e.g., SA and RRB or males and females) and determined what percentile of the difference distribution was larger than zero to assess significance (e.g., 97.5 percentile would correspond to a p-value of 0.05 in a two-tailed test).
Power analysis
Given our previous findings [28] showing a strong correlation between estimated and actual ADOS scores (r = 0.718), the sample size of 61 subjects in the test set provides 100% power for detecting a significant correlation in the current study.
Results
Using the data from the 136 ASD children in the training dataset, we examined the relationships between each of the 49 features and ASD symptom severity as defined clinically by the children’s ADOS-2 scores. Thirty-one features exhibited significant Pearson correlation coefficients with total ADOS-2 scores (i.e., sum of SA and RRB scores), 31 with ADOS-2 SA scores, and 28 with ADOS-2 RRB scores (Fig. 1). While some features, such as the number of vocalizations, exhibited a stronger correlation with SA than RRB score, others, such as mean jitter, exhibited the opposite (Supplementary Fig. S4). Hence, different features seem to carry distinct information regarding each of the two core ASD symptoms, demonstrating the potential opportunity for a deep learning algorithm to learn relevant associations.

Correlation coefficients are presented for total ADOS-2 scores (a), ADOS-2 SA scores (b), and ADOS-2 RRB scores (c). Each color represents a different group of features. Asterisks: significant Pearson correlation (*< 0.05, **≤ 0.01, *3 ≤ 0.001, *4 ≤ 0.0001).
Longitudinal stability of ADOS-2 scores
The 61 ASD children in the test dataset exhibited similar ADOS-2 scores across their two assessments, which were separated by 1–2 years, indicating overall stability in severity over time. Significant correlations were apparent across first and second assessments for ADOS-2 total (r(59) = 0.743, P < 0.001), ADOS-2 SA (r(59) = 0.666, P < 0.001), and ADOS-2 RRB (r(59) = 0.5, P < 0.001) scores (Fig. 2).

a ADOS-2 SA scores. b ADOS-2 RRB scores. c Total ADOS-2 scores (sum of SA and RRB scores). Asterisk: statistical significance of the Pearson correlation coefficient (P < 0.0001). Shaded areas: 95% confidence intervals. Children located below the diagonal (dashed line) exhibited lower ASD severity at T2 (improvement), while children above the diagonal exhibited the opposite.
Training and testing the ASDSpeech algorithm
We trained the ASDSpeech algorithm with data from 136 ASD children in the training dataset. The algorithm included two separate CNN models that were trained to estimate ADOS-2 SA and RRB scores independently, given that different speech features were associated with each symptom domain. The accuracy of the algorithm was tested with data from two independent ADOS-2 recordings of the 61 children in the testing dataset where ASDSpeech estimated the SA, RRB, and total ADOS-2 (sum of SA and RRB) scores of each child per recording (Fig. 3).

Scatter plots demonstrating the fit between estimated and actual scores for the children at T1 (left column) and T2 (right column). a, b Total ADOS-2 scores (sum of SA and RRB scores). c, d ADOS-2 SA scores. e, f ADOS-2 RRB scores. Pearson correlation coefficients and NRMSE values are noted in each panel. Solid line: Linear fit. Dashed line: diagonal (unity line). Asterisks: statistical significance as determined by randomization test (P < 0.05).
Estimated total ADOS-2 scores were significantly correlated with actual scores at T1 (r(59) = 0.544, P < 0.0001) and T2 (r(59) = 0.605, P < 0.0001). Similarly, estimated ADOS-2 SA scores were significantly correlated with actual scores at T1 (r(59) = 0.502, P < 0.0001) and T2 (r(59) = 0.592, P < 0.0001). In contrast, estimated ADOS-2 RRB scores were not significantly correlated with actual RRB scores at T1 (r(59) = 0.093, P = 0.474), exhibiting significant correlations only at T2 (r(59) = 0.332 P = 0.009) with a relatively weaker effect size. Correlations of estimated and actual ADOS-SA score were significantly higher than correlations of estimated and actual ADOS-RRB score as assessed by a permutation analysis (T1: P = 0.016, T2: P = 0.038).
Normalized Root Mean Squared Error (NRMSE) between estimated and actual total ADOS-2 scores was significantly smaller than expected by chance when computed at T1 (NRMSE = 0.164, P < 0.0001) and T2 (NRMSE = 0.149, P = 0.0001). Similarly, NRMSE between estimated and actual ADOS-2 SA scores was significantly smaller than expected by chance when computed at T1 (NRMSE = 0.200, P < 0.0001) and T2 (NRMSE = 0.170, P < 0.0001). In contrast, NRMSE between estimated and actual ADOS-2 RRB scores was not significantly smaller than expected by chance at T1 (NRMSE = 0.219, P = 0.460), exhibiting significant results only at T2 (NRMSE = 0.225, P = 0.006). The statistical significance of the NRMSE results was determined with a randomization analysis (see Methods). NRMSE values of ADOS-SA score were significantly lower than the NRMSE values of ADOS-RRB score at T2 (P = 0.012) but not at T1 (P = 0.432) as assessed using a permutation analysis.
Similar results were also found when training and testing the model with ADOS-2 CSS scores. Most importantly, consistent significant correlations were found between estimated and actual ADOS-2 SA CSS scores at both timepoints (Supplementary Table S2).
Differences across age and sex subgroups
Next, we examined whether ASDSpeech accuracy differed across age and sex subgroups (Fig. 4). Estimated total ADOS-2 scores were significantly correlated with actual scores when examining children above the median age at T1 (r(28) = 0.604, P < 0.0001, median age = 45 months) or T2 (r(25) = 0.612, P < 0.0001, median age = 61 months) and children below the median age at T1 (r(29) = 0.485, P = 0.008) or T2 (r(32) = 0.657, P < 0.0001). There were no significant differences in the algorithm’s accuracy between younger and older children at T1 (P = 0.540) or T2 (P = 0.780) as tested with a bootstrap permutation analysis. Similarly, estimated total ADOS-2 scores were significantly correlated with actual scores when examining males at T1: (r(40) = 0.631, P < 0.0001) or T2 (r(40) = 0.601, P < 0.0001). Estimated ADOS-2 scores were also significantly correlated with actual scores when examining females at T2 (r (17) = 0.627, P = 0.008), but not at T1 (r (17) = 0.363, P = 0.140). Nevertheless, there were no significant differences in the algorithm’s accuracy between males and females at T1 (P = 0.198) or T2 (P = 0.930) as tested with a bootstrap permutation analysis.

a, b Pearson correlation values. c, d Normalized Root Mean Squared Error (NRMSE) values. a, c Comparison between younger and older children (median split according to age at each timepoint). b, d Comparison between males and females. Asterisks: statistical significance as determined by randomization test (P < 0.05).
Comparison of NRMSE across subgroups showed similar results. NRMSE between the estimated and actual ADOS-2 scores was significantly smaller than expected by chance when examining younger children at T1 (NRMSE = 0.173, P = 0.008) or T2 (NRMSE = 0.150, P < 0.0001) as well as older children at T1 (NRMSE = 0.154, P < 0.0001) or T2 (NRMSE = 0.149, P < 0.0001). There were no significant differences in the algorithm’s accuracy between younger and older children at T1 (P = 0.434) or T2 (P = 0.992). NRMSE were also significantly smaller than expected by chance when examining males at T1 (NRMSE = 0.149, P < 0.0001) or T2 (NRMSE = 0.144, P < 0.0001). For females this was the case only at T2 (NRMSE = 0.161, P = 0.008) and not at T1 (NRMSE = 0.193, P = 0.140). Nevertheless, there were no significant differences in the algorithm’s accuracy between males and females at T1 (P = 0.094) or T2 (P = 0.588) as tested with a bootstrap permutation test.
Longitudinal stability of ASDSpeech
Next, we examined the stability of ASDSpeech estimated ADOS-2 scores across the two time-points. There were significant correlations between the estimated ADOS-2 SA scores (r(59) = 0.649, P < 0.0001) and total ADOS-2 scores (r(59) = 0.687, P < 0.0001) at T1 and T2. There was no significant correlation between estimated ADOS-2 RRB scores (r(59) = 0.203, P = 0.117) across timepoints (Fig. 5).

a Estimated ADOS-2 SA scores. b Estimated ADOS-2 RRB scores. c Estimated total ADOS-2 scores (sum of estimated SA and RRB scores). Asterisk: statistical significance (P < 0.0001). Shaded areas: 95% confidence intervals.
Feature importance
To determine the relative importance of each feature in accurately estimating ADOS-2 total scores we eliminated individual features from the test dataset by replacing their values with zeros, one at a time. We then examined whether accuracy was reduced (i.e., correlations were smaller) when each feature was excluded (Supplementary Fig. S5). The results revealed that excluding individual features had limited impact on the accuracy of the algorithm. When examining T1 data, excluding variance of Second formant, mean of pitch in voiced vocalizations, mean spectral slope in range [500, 1500]Hz in voiced vocalizations, mean Second derivate of energy, and variance of ZCR in voiced vocalizations yielded significant reductions in accuracy (i.e., weaker correlations between estimated and actual ADOS-2 total scores). However, in T2 data accuracy was not significantly negatively affected by exclusion of any feature and only positively affected by the exclusion of mean First derivative of the energy. This suggested that there was large redundancy across features such that removing individual features did not have a strong or consistent impact on accuracy.
Discussion
Our results demonstrate the ability of ASDSpeech to quantify the severity of social symptoms in ASD children from recordings of their speech during ADOS-2 assessments. The algorithm, trained with recordings from 136 ASD children, was able to accurately estimate total ADOS-2 and ADOS-2 SA scores in an entirely independent sample of 61 ASD children, who were recorded at two different developmental timepoints separated by 1–2 years (Fig. 3). It is remarkable that ASDSpeech was able to achieve this despite the large heterogeneity in language fluency and speech articulation abilities apparent across ASD children [46] as well as the large developmental changes that take place in speech abilities during the examined period of early childhood [47]. Moreover, the accuracy of ASDSpeech is remarkable given that many social difficulties assessed during the ADOS-2 assessment manifest themselves in behaviors that have little to do with speech including difficulties with eye contact, imitation, joint attention, and other social behaviors [3, 48]. This suggests that combining ASDSpeech with analysis of eye tracking [49,50,51], facial expressions [52], and body movement [53] data from the same children will enable even higher accuracy and reliability in estimating ASD symptoms.
Correlation analyses revealed that ASDSpeech was considerably more accurate and reliable at estimating social ASD symptoms captured by the ADOS-2 SA scores in contrast to the RRB symptoms captured by the ADOS-2 RRB scores (Figs. 3 and 5). Note that accurate estimation of total ADOS-2 scores (Fig. 3) was likely based on the accurate estimation of SA scores that account for two-thirds of the total scores. We believe there may be several reasons for the more accurate estimation of SA scores. First, the limited range of the ADOS-2 RRB scale (0–8) relative to the SA scale (0–22) may make it difficult for the algorithm to identify differences across children. Indeed, a recent study reported that the limited number of items on the RRB scale resulted in poor scale reliability across participants [54]. Second, the selected speech features in the current study exhibited weaker correlations with RRB than SA scores (Fig. 1). Extraction of additional speech features, such as phrase or intonation repetitions (indicative of echolalia) may improve the accuracy of ADOS-2 RRB score estimates. Regardless, our results motivate separate modeling of social and RRB symptom domains as each of them is likely associated with distinct features of speech.
Models trained and tested on raw ADOS-2 scores (Fig. 3) clearly out -performed models trained on ADOS-2 CSS scores (Supplementary Table S2). While ADOS-2 CSS are important for longitudinal assessments of coarse changes in severity [2, 55], their restricted scoring range likely limits the sensitivity of deep learning algorithms in identifying differences across children. By demonstrating that ASDSpeech achieves robust accuracy in estimating raw ADOS-2 SA scores across different age groups and developmental timepoints we show that severity estimations are independent of these factors, thereby justifying the use of raw scores.
Diagnostic classification with speech analysis algorithms
A variety of previous studies have reported that individuals with ASD, on average, speak differently than TD individuals [4, 8,9,10,11,12,13,14,15,16]. According to these studies, ASD individuals exhibit atypical speech characteristics, including significantly fewer phonemes per utterance [11], fewer conversational turns [13], higher pitch [9, 19], and larger pitch range and variability [8, 9] than TD children. Differences in these and other speech characteristics have enabled the development of machine and deep learning classification algorithms that can identify ASD and TD individuals with reported accuracy rates of 75–98% [17,18,19,20,21,22,23].
However, these relatively high classification accuracies are likely to be inflated due to the small sample size of most studies (<40 ASD participants) that are not likely to capture the true heterogeneity of ASD symptoms or speech styles/characteristics of the broad ASD population. Indeed, even “gold standard” clinical tests such as the ADOS-2, exhibit ~80% accuracy in identifying children who will eventually receive an ASD diagnosis [56]. This is because establishing an ASD diagnosis requires clinicians to incorporate additional information from parent interviews and other clinical assessments [57]. Clinicians also report high diagnosis certainty in only ~70% of ASD children because the presentation of ASD symptoms is equivocal in ~30% of cases [58]. These studies suggest an expected upper limit of 70–80% accuracy when attempting to identify ASD using digital phenotyping techniques such as speech analysis. Nevertheless, it is highly encouraging that speech features contain information enabling the separation of ASD and TD children.
Quantifying ASD severity with speech analysis algorithms
A more complex task is to develop machine and deep learning algorithms that can quantify the severity of core ASD symptoms. Results presented in the current and previous study from our lab [28] demonstrated that multiple speech features were significantly correlated with SA and/or RRB ADOS-2 scores (Fig. 1), suggesting that distinct combinations of speech features are associated with each of the two core ASD domains.
Three recent studies have attempted to use these relationships to estimate ADOS-2 scores by analyzing speech recordings of ASD individuals [26,27,28]. The first trained a synthetic random forest model to estimate ADOS-2 SA scores according to vocalization rate and turn-taking features extracted from ADOS-2 recordings of 33 ASD children. The algorithm was able to estimate ADOS-2 SA scores that were significantly correlated with actual scores (r = 0.634). The second study utilized a DNN model to estimate four ADOS (first edition) item scores using hundreds of conversational and acoustic features extracted from speech recordings of 88 high-functioning ASD adolescents/adults during an ADOS assessment [27]. This algorithm was able to estimate scores that exhibited significant Spearman correlations with the actual scores (ρ = 0.519–0.645). Finally, in a previous study from our lab [28], we demonstrated that a CNN model was able to estimate ADOS-2 total scores that were significantly correlated with actual scores (r = 0.718) when using 60 conversational and acoustic features extracted from speech recordings of 72 children (56 of them with ASD) during ADOS-2 assessment.
The current study extends previous work in several critical ways. First, we utilized a considerably larger dataset (258 ADOS-2 recordings) that was at least three times larger than the ones used to date. This was important for training ASDSpeech with speech recordings form a large cohort with heterogeneous language abilities. Second, the 61 ASD children in our testing dataset were recorded twice during two ADOS-2 assessments separated by 1–2 years. This enabled us to test the robustness of ASDSpeech across two developmental timepoints. Third, we trained ASDSpeech to estimate ADOS-2 SA and ADOS-2 RRB scores using separate CNN models. The results demonstrated that this separation was critical with accurate performance apparent primarily for the ADOS-2 SA scores. Fourth, the large sample size enabled us to demonstrate that ASDSpeech accuracy was similar across age and sex subgroups. Fifth, the recordings utilized in the current study were performed over a 6-year period in a busy public healthcare medical center that services a population of ~1 million people. Recordings were performed with a wall mounted microphone (see Methods) in “real world” noisy conditions (e.g., announcement system in the hallway). This demonstrates the robustness of ASDSpeech to variable recording conditions.
ASDSpeech achieved similar accuracy to that reported in previous studies. The important advance in the current study is in demonstrating that this accuracy is specific to social symptoms captured by ADOS-SA scores and robust to age and developmental stage of the examined children when examining a large heterogeneous population within an active clinical setting. Most importantly, we openly share ASDSpeech and its associated dataset with the research community.
Limitations
The current study has several limitations. First, we did not examine the language content of the recordings, which is likely to improve the estimation of ASD symptom severity [4, 24]. Second, we did not identify echolalia, crying, or shouting events that are likely to be informative of RRB symptoms. Indeed, our weaker results estimating RRB scores suggest that different speech features are necessary for estimating severity in this domain. Third, we did not apply any noise reduction or multi-speaker analysis techniques to improve the quality of the analyzed vocal segments. Fourth, our sample had a (4:1) male to female ratio, which is equivalent to the sex ratio in the national ASD population of Israel [59]. Hence, higher ASDSpeech accuracy for males at T1 may be due to the larger number of males in the training and testing datasets, a sampling bias that could be rectified by future studies. Fifth, we used manual annotation to identify child vocalizations, which is highly accurate, but also labor-intensive and not scalable. Future work could investigate integration of automated diarization methods. Finally, our analyses were limited to 1–7-years-old children and the accuracy of ASDSpeech in estimating ASD severity in older children remains to be determined.
Conclusions
This study adds to accumulating evidence demonstrating that speech recordings contain reliable information about the social symptom severity of ASD children. We demonstrate the ability of the ASDSpeech algorithm to quantify these symptoms in a robust manner across two developmental timepoints with recordings that were performed within a busy community healthcare center. We openly share the algorithm and its associated dataset for further use, testing, and development by the research community and are confident that future versions of the algorithm will achieve even higher and more robust accuracy rates, yielding a transformative new tool for clinical and basic ASD research.
Data availability
The entire feature dataset used for training and testing are available at https://github.com/Dinstein-Lab/ASDSpeech.
Code availability
The ASDSpeech algorithm source-code is available at https://github.com/Dinstein-Lab/ASDSpeech.
References
Lord C, Elsabbagh M, Baird G, Veenstra-Vanderweele J. Autism spectrum disorder. Lancet. 2018;392:508–20.
Gabbay-Dizdar N, Ilan M, Meiri G, Faroy M, Michaelovski A, Flusser H, et al. Early diagnosis of autism in the community is associated with marked improvement in social symptoms within 1–2 years. Autism. 2022;26:1353–63.
Tager-Flusberg H, Kasari C. Minimally verbal school-aged children with autism spectrum disorder: the neglected end of the spectrum. Autism Res. 2013;6:468–78.
Salem AC, MacFarlane H, Adams JR, Lawley GO, Dolata JK, Bedrick S, et al. Evaluating atypical language in autism using automated language measures. Sci Rep. 2021;11:10968 https://doi.org/10.1038/S41598-021-90304-5.
Chi NA, Washington P, Kline A, Husic A, Hou C, He C, et al. Classifying autism from crowdsourced semistructured speech recordings: machine learning model comparison study. JMIR Pediatr Parent. 2022;5:e35406.
Mostek J. Cognitive development and language acquisition in autistic children. Sci Insig. 2022;41:719–24.
Loukusa S. Autism spectrum disorder. In: Cummings L, editors. Handbook of pragmatic language disorders. Cham: Springer International Publishing; 2021, pp. 45–78.
Bonneh YS, Levanon Y, Dean-Pardo O, Lossos L, Adini Y. Abnormal speech spectrum and increased pitch variability in young autistic children. Front Hum Neurosci. 2011;4:237.
Asghari SZ, Farashi S, Bashirian S, Jenabi E. Distinctive prosodic features of people with autism spectrum disorder: a systematic review and meta-analysis study. Sci Rep. 2021;11:23093.
Oller DK, Niyogi P, Gray S, Richards JA, Gilkerson J, Xu D, et al. Automated vocal analysis of naturalistic recordings from children with autism, language delay, and typical development. Proc Natl Acad Sci USA. 2010;107:13354–9.
Moffitt JM, Ahn YA, Custode S, Tao Y, Mathew E, Parlade M, et al. Objective measurement of vocalizations in the assessment of autism spectrum disorder symptoms in preschool age children. Autism Res. 2022;15:1665–74.
Ferguson EF, Nahmias AS, Crabbe S, Liu T, Mandell DS, Parish-Morris J. Social language opportunities for preschoolers with autism: Insights from audio recordings in urban classrooms. Autism. 2020;24:1232–45.
Warren SF, Gilkerson J, Richards JA, Oller DK, Xu D, Yapanel U, et al. What automated vocal analysis reveals about the vocal production and language learning environment of young children with autism. J Autism Dev Disord. 2010;40:555–69.
Warlaumont AS, Richards JA, Gilkerson J, Oller DK. A social feedback loop for speech development and its reduction in autism. Psychol Sci. 2014;25:1314–24.
Plumb AM, Wetherby AM. Vocalization development in toddlers with autism spectrum disorder. J Speech Lang Hear Res. 2013;56:721–34.
Tenenbaum EJ, Carpenter KL, Sabatos‐DeVito M, Hashemi J, Vermeer S, Sapiro G, et al. A six‐minute measure of vocalizations in toddlers with autism spectrum disorder. Autism Res. 2020;13:1373–82.
Pokorny FB, Schuller BW, Marschik PB, Brueckner R, Nyström P, Cummins N, et al. Earlier identification of children with autism spectrum disorder: an automatic vocalisation-based approach. Proceedings of the annual conference of the international speech communication association. Proc. Interspeech. 2017;309–13. https://doi.org/10.21437/Interspeech.2017-1007.
Mohanta A, Mittal VK. Classifying speech of ASD affected and normal children using acoustic features. In: 2020 National conference on communications (NCC) Kharagpur, India. IEEE, 2020, pp. 1–6.
Mohanta A, Mittal VK. Analysis and classification of speech sounds of children with autism spectrum disorder using acoustic features. Comput Speech Lang. 2022;72:101287.
Asgari M, Shafran I. Robust and accurate features for detecting and diagnosing autism spectrum disorders. Proceedings of the annual conference of the international speech communication association. Interspeech. 2013;2013:191–4.
Yankowitz LD, Schultz RT, Parish-Morris J. Pre- and paralinguistic vocal production in ASD: birth through school age. Curr Psychiatry Rep. 2019;21:126.
Lee S, Yeo EJ, Kim S, Chung M. Knowledge-driven speech features for detection of Korean-speaking children with autism spectrum disorder*. Phonetics and Speech Sci. 2023;15:53–9.
Briend F, David C, Silleresi S, Malvy J, Ferré S, Latinus M. Voice acoustics allow classifying autism spectrum disorder with high accuracy. Transl Psychiatry. 2023;13:250.
MacFarlane H, Salem AC, Chen L, Asgari M, Fombonne E. Combining voice and language features improves automated autism detection. Autism Res. 2022;15:1288–300.
Lord C, Rutter M, Di Lavore P, Risi S, Gotham K, Bishop S. Autism and diagnostic observation schedule, Second Edition (ADOS-2) Manual (Part I): Modules. 2012, pp. 1–4.
Sadiq S, Castellanos M, Moffitt J, Shyu M, Perry L, Messinger D. Deep learning based multimedia data mining for autism spectrum disorder (ASD) diagnosis. In: 2019 International conference on data mining workshops (ICDMW). IEEE. 2019, pp. 847–54.
Chen C-P, Gau SS-F, Lee C-C. Learning converse-level multimodal embedding to assess social deficit severity for autism spectrum disorder. In: 2020 IEEE international conference on multimedia and expo (ICME). IEEE, 2020, pp. 1–6.
Eni M, Dinstein I, Ilan M, Menashe I, Meiri G, Zigel Y. Estimating autism severity in young children from speech signals using a deep neural network. IEEE Access. 2020;8:139489–500.
Esler AN, Bal VH, Guthrie W, Wetherby A, Weismer SE, Lord C. The autism diagnostic observation schedule, toddler module: standardized severity scores. J Autism Dev Disord. 2015;45:2704–20.
Gotham K, Pickles A, Lord C. Standardizing ADOS scores for a measure of severity in autism spectrum disorders. J Autism Dev Disord. 2009;39:693–705.
Dinstein I, Arazi A, Golan HM, Koller J, Elliott E, Gozes I, et al. The national autism database of Israel: a resource for studying autism risk factors, biomarkers, outcome measures, and treatment efficacy. J Mol Neurosci. 2020;70:1303–12.
Meiri G, Dinstein I, Michaelowski A, Flusser H, Ilan M, Faroy M, et al. The negev hospital-university-based (HUB) autism database. J Autism Dev Disord. 2017;47:2918–26.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. American Psychiatric Publishing: Arlington, VA; 2013. https://doi.org/10.1176/appi.books.9780890425596.744053.
Hus V, Gotham K, Lord C. Standardizing ADOS domain scores: separating severity of social affect and restricted and repetitive behaviors. J Autism Dev Disord. 2014;44:2400–12.
Hansen JHL, Najafian M, Lileikyte R, Irvin D, Rous B. Speech and language processing for assessing child–adult interaction based on diarization and location. Int J Speech Technol. 2019;22:697–709.
Kumar M, Kim SH, Lord C, Lyon TD, Narayanan S. Leveraging linguistic context in dyadic interactions to improve automatic speech recognition for children. Comput Speech Lang. 2020;63:101101.
Padmini P, Gupta D, Zakariah M, Alotaibi YA, Bhowmick K. A simple speech production system based on formant estimation of a tongue articulatory system using human tongue orientation. IEEE Access. 2021;9:4688–710.
Rusz J, Benova B, Ruzickova H, Novotny M, Tykalova T, Hlavnicka J, et al. Characteristics of motor speech phenotypes in multiple sclerosis. Mult Scler Relat Disord. 2018;19:62–9.
Boersma P, van Heuven V. Speak and unSpeak with Praat. Glot Int. 2001;5:341–7.
Pillai L, Sherly E. A deep learning based evaluation of articulation disorder and learning assistive system for autistic children. Int J Nat Lang Comput. 2017;6:19–36.
Tamarit L, Goudbeek M, Scherer K. Spectral slope measurements in emotionally expressive speech. In: Proceedings of ISCA tutorial and research workshop (ITRW) on speech analysis and processing for knowledge discovery. ISCA, 2008, pp. 1–4.
Eyben F, Scherer KR, Schuller BW, Sundberg J, Andre E, Busso C, et al. The Geneva Minimalistic Acoustic Parameter Set (GeMAPS) for voice research and affective computing. IEEE Trans Affect Comput. 2016;7:190–202.
Taqi AM, Awad A, Al-Azzo F, Milanova M. The impact of multi-optimizers and data augmentation on tensorflow convolutional neural network performance. In: Proceedings - IEEE 1st conference on multimedia information processing and retrieval, MIPR 2018. IEEE, 2018, 140–5.
Prechelt L. Early stopping — but when? In: Neural networks: tricks of the trade. Springer: Berlin, Heidelberg, 2012, pp. 53–67.
MacFarlane H, Salem AC, Bedrick S, Dolata JK, Wiedrick J, Lawley GO, et al. Consistency and reliability of automated language measures across expressive language samples in autism. Autism Res. 2023;16:802–16.
Tager-Flusberg H. Defining language phenotypes in autism. Clin Neurosci Res. 2006;6:219–24.
Tager-Flusberg H, Rogers S, Cooper J, Landa R, Lord C, Paul R, et al. Defining spoken language benchmarks and selecting measures of expressive language development for young children with autism spectrum disorders. J Speech Lang Hear Res. 2009;52:643–52.
Vivanti G, Bottema-Beutel K, Turner-Brown L. Understanding and addressing restricted and repetitive behaviors in children with autism. In: Clinical guide to early interventions for children with autism. Springer, 2020, pp. 61–77.
Avni I, Meiri G, Bar‐Sinai A, Reboh D, Manelis L, Flusser H, et al. Children with autism observe social interactions in an idiosyncratic manner. Autism Re. 2020;13:935–46.
Chong E, Clark-Whitney E, Southerland A, Stubbs E, Miller C, Ajodan EL, et al. Detection of eye contact with deep neural networks is as accurate as human experts. Nat Commun. 2020;11:6386.
Jones W, Klaiman C, Richardson S, Aoki C, Smith C, Minjarez M, et al. Eye-tracking-based measurement of social visual engagement compared with expert clinical diagnosis of autism. JAMA. 2023;330:854–65.
Perochon S, Di Martino JM, Carpenter KLH, Compton S, Davis N, Eichner B, et al. Early detection of autism using digital behavioral phenotyping. Nat Med. 2023;29:2489–97.
Budman I, Meiri G, Ilan M, Faroy M, Langer A, Reboh D, et al. Quantifying the social symptoms of autism using motion capture. Sci Rep. 2019;9:7712.
Frazier TW, Whitehouse AJO, Leekam SR, Carrington SJ, Alvares GA, Evans DW, et al. Reliability of the commonly used and newly-developed autism measures. J Autism Dev Disord. 2023. https://doi.org/10.1007/s10803-023-05967-y.
Waizbard-Bartov E, Ferrer E, Young GS, Heath B, Rogers S, Wu Nordahl C, et al. Trajectories of autism symptom severity change during early childhood. J Autism Dev Disord. 2021;51:227–42.
Maddox BB, Brodkin ES, Calkins ME, Shea K, Mullan K, Hostager J, et al. The accuracy of the ADOS-2 in identifying autism among adults with complex psychiatric conditions. J Autism Dev Disord. 2017;47:2703.
Bishop SL, Lord C. Commentary: best practices and processes for assessment of autism spectrum disorder - the intended role of standardized diagnostic instruments. J Child Psychol Psychiatry. 2023;64:834–8. https://doi.org/10.1111/JCPP.13802.
Klaiman C, White S, Richardson S, McQueen E, Walum H, Aoki C, et al. Expert clinician certainty in diagnosing autism spectrum disorder in 16-30-month-olds: a multi-site trial secondary analysis. J Autism Dev Disord. 2022. https://doi.org/10.1007/S10803-022-05812-8.
Raz R, Weisskopf MG, Davidovitch M, Pinto O, Levine H. Differences in autism spectrum disorders incidence by sub-populations in Israel 1992–2009: a total population study. J Autism Dev Disord. 2015;45:1062–9.
Acknowledgements
This study was supported by the Israeli Science Foundation (Grant no. 1150/20) and the Israel Ministry of Science & Technology (Grant no. 3-17422).
Author information
Authors and Affiliations
Contributions
ME collected the data, performed the experiments, built the models, analyzed the data, and wrote the paper. ID, and YZ designed the study, guided data collection and analysis, and wrote the paper. MI, AM, HMG, GM, and IM contributed to participant recruitment, behavioral assessments, data collection, and interpretation of the findings. All authors approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
All of the methods were performed in accordance with the relevant guidelines and regulations. Approval has been obtained from the SUMC Helsinki committee (SOR-0222-14), and informed consent was obtained from all parents.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Eni, M., Zigel, Y., Ilan, M. et al. Reliably quantifying the severity of social symptoms in children with autism using ASDSpeech. Transl Psychiatry 15, 14 (2025). https://doi.org/10.1038/s41398-025-03233-6
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41398-025-03233-6
