
Abstract
The COVID-19 pandemic has intensified the global burden of mental disorders, yet the gap between observed and counterfactual burdens without the pandemic, especially for major depressive and anxiety disorders, remains unexplored. To assess this gap, including its impact on specific regions and populations, thereby guiding future mental health services and policy development. Data of age-standardized prevalence rate (ASPR), age-standardized incidence rate (ASIR) and age-standardized disability-adjusted life years rate (ASDR) for mental disorders from 1990 to 2021 were extracted from the Global Burden of Disease dataset. This study employed a counterfactual model that combines Autoregressive Integrated Moving Average and Long Short-Term Memory to assess the impact of the COVID-19 pandemic on the global burden of mental disorders by quantifying the difference between actual and predicted rates. In 2021, mental disorders were more prevalent in higher Social Development Index (SDI) regions such as the North Americas, and European region. During the COVID-19 pandemic (2020-2021), these regions, including countries like Denmark and the United States, saw significant increases in the ASPR, ASIR and ASDR of mental disorders, far exceeding predictions. Globally, the ASIR for men increased from a predicted 3917 to an observed 4435 per 100,000, while for women, it rose from a predicted 5497 to an observed 6382 per 100,000. Specific disorders like major depressive disorder and anxiety disorders showed even larger discrepancies, with ASPR of anxiety disorders exceeding predictions by 1135 and 1043 per 100,000 in Bolivia and Peru, respectively, and ASIR of major depressive disorder in Greenland surpassing predictions by 1156 per 100,000. The pandemic also had a significant impact on mental health across different age groups, with individuals aged 15–40 years experiencing the greatest increase in anxiety and major depressive disorders, particularly among women. In conclusion, during the COVID-19 pandemic, the global burden of mental disorders far exceeded the counterfactual predictions, with major depressive and anxiety disorders showing the largest increases. This underscores the pandemic’s severe impact on mental health and the urgent need for enhanced global mental health services, including ongoing evaluation and support.
Similar content being viewed by others

Introduction
Mental disorders, ranking among the top 10 globally prevalent diseases over the past three decades, have consistently been a leading contributor to the global burden [1], accounting for approximately 14% of the total disease burden [2]. In 2019, the global burden of mental disorders reached 125.3 million disability-adjusted life years (DALYs) (93.0–163.2), representing 4.9% (3.9–6.1) of the total global DALYs [1]. According to the latest World Health Organization (WHO) report, approximately 970 million people worldwide suffer from mental disorders, with anxiety and depression being the most prevalent and severe [3]. Compared to the general population, patients with mental disorders often exhibit negative behaviors such as higher smoking rates, substance use, physical inactivity, and poor diet [4], resulting in a mortality rate more than twice that of the general population and a relatively shorter life expectancy [5, 6]. With the rapid changes in global socio-economic conditions and lifestyles, the burden of mental disorders has significantly increased over the past few decades [7,8,9].
From 2020 to 2023, the COVID-19 pandemic precipitated profound health [10] and economic consequences worldwide, further exacerbating this trend, as lockdowns, isolation measures, economic uncertainty, and widespread health crises around the world have led to a marked rise in mental health issues [11]. A study reports a notable surge in anxiety and depression cases in 2020, linked to the COVID-19 pandemic, potentially stemming from containment strategies [12]. The impact of the pandemic on mental health has been particularly severe in regions with higher Social Development Index (SDI). In Eastern Europe, a notable 29.4% surge in major depressive disorder cases and a 30.8% increase in anxiety disorders were observed [13].
However, the gap between the observed burden of mental disorders during the pandemic and predicted levels, especially for depression and anxiety disorders, has not been fully assessed. Currently, numerous models have been developed to forecast disease burden, including the Autoregressive Integrated Moving Average (ARIMA) model, which is widely utilized for predicting the incidence of infectious diseases with complex long-term trends, and the Long Short-Term Memory (LSTM) model, which identifies patterns in historical data to forecast future disease trajectories. Some investigations have successfully applied the LSTM model to predict mental disorders at the individual level [14], and the integration of these two models has been shown to enhance predictive accuracy [15]. However, no existing research has yet developed a model to predict the global burden of mental disorders.
To address this gap and better understand the global impact, this study is the first to compare the actual prevalence, incidence, and DALYs of mental disorders during the pandemic with predicted values. Furthermore, it explores the implications of this gap across different regions and age groups, offering valuable insights for the development of future mental health services and policy interventions.
Methods
Data collection
The 2021 Global Burden of Disease (GBD) dataset furnished data on the annual age-standardized prevalence rate (ASPR), age-standardized incidence rate (ASIR) and age-standardized disability-adjusted life years rate (ASDR) with 95% uncertainty interval (UI) associated with 12 mental disorders: major depressive disorder, anxiety disorders, schizophrenia, autism spectrum disorders, dysthymia, bipolar disorder, conduct disorder, idiopathic developmental intellectual disability (IDID), anorexia nervosa, bulimia nervosa, attention−deficit/hyperactivity disorder (ADHD), other mental disorders in 204 countries and territories, ranging from 1990 to 2021. The definition of mental disorder and its 12 subcategories has been documented elsewhere [1]. Additionally, we analyzed health loss due to mental disorders across WHO regions (Region of Americas, European Region, Eastern Mediterranean Region, South-East Asia Region, African Region and Western Pacific Region), SDI levels (High, High-middle, Middle, Low-middle and Low Region), age groups (in five-year increments), and sex. Data were collected from the Global Health Data Exchange (GHDx) query tool, an online data repository (http://ghdx.healthdata.org/gbd-results-tool, accessed on 17 May 2024). Earlier research has outlined the basic procedures for the GBD 2021 [16].
The COVID-19 Government Response Tracker (GRT) was utilized to compile regulations enacted during the COVID-19 pandemic [17]. The Containment Health Index (CHI) measures the number and intensity of closure and containment policies, as well as policies towards disease surveillance. This index includes non-pharmacological interventions (NPIs) such as school closures, workplace closures, public event cancellations, restrictions on gatherings, closing public transport, stay-at-home requirements, movement restrictions and facial coverings. The first seven NPIs were classified as physical distancing if any one measure was implemented, while facial coverings were recognized when specifically enforced. Based on the types of NPIs, countries were classified into four groups: Group A (no facial coverings or physical distancing), Group B (only physical distancing), Group C (only facial coverings), and Group D (both facial coverings and physical distancing). The World Bank’s website provided demographic and economic data for 204 countries and territories in 2020 and 2021 (https://data.worldbank.org/?ask).
Models descriptions
ARIMA Model encompasses the autoregressive (AR) and moving average (MA) components. Rooted in the theory that time-dependent random variable data series exhibit autocorrelation patterns captured by the ARIMA model, allowing for future predictions based on historical data. The model ranks among the most universal methods in time series prediction, boasting a high level of accuracy [18,19,20].
In contrast, LSTM, an advanced machine learning algorithm leveraging a recurrent neural network architecture, is designed to retain short-term learning and facilitate long-term training [21]. It incorporates three crucial gating mechanisms: input gate (it), forgetting gate (ft) and output gate (ot), which orchestrate the deletion of irrelevant information, the updating of salient data, and the controlled release of information within the cell state, respectively. Several studies have employed the ARIMA model and the LSTM model to predict chronic disease trends [18, 22, 23]. Previous studies have demonstrated that the ARIMA-LSTM combined model offers superior predictive capabilities, particularly for morbidity data, which inherently exhibits non-linear and non-smooth time series characteristics [18].
For forecasting the global burden of mental disorders during 2020–2021, we trained our models using historical data on ASPR, ASIR, and ASDR for mental disorders from 1990 to 2016, while the period from 2017 to 2019 was reserved for validation. The ARIMA model refers to the direct application of ARIMA, which captures only linear dependencies, to generate forecasts for 2017–2019; its predictions for this period are denoted as Y₁. The ARIMA–LSTM combined model was constructed in several steps. First, we calculated the residuals between the ARIMA forecasts (Y₁) and the observed values for 2017–2019, thereby extracting the nonlinear components that ARIMA alone could not capture. Next, these residuals were used to train an LSTM model, which produced predictions of the residual sequence for 2017–2019, denoted as Y₂. The final combined forecasts were obtained by summing Y₁ and Y₂, thus integrating both the linear and nonlinear components of the data. Model performance was evaluated using Root Mean Square Error (RMSE) and Mean Absolute Error (MAE) on the validation set (2017–2019). We then compared the ARIMA model with the ARIMA–LSTM combined model, and the model yielding lower error metrics was selected to forecast the global burden of mental disorders during 2020–2021.
Statistical analysis
The 2021 global mental disorders landscape was characterized by ASPR, ASIR, and ASDR. Comparative analyses of two-year average (2018–2019 pre-pandemic vs. 2019–2020 post-pandemic) was calculated across 204 countries and territories, 6 WHO regions and 5 SDI levels. We then estimated the Annual Percentage Change (EAPC) for ASPR, ASIR, and ASDR of mental disorders from 1990 to 2018, which was achieved by fitting a log-linear regression model to delineate annual trends. ARIMA model and the ARIMA-LSTM combined model were utilized to predict the ASPR, ASIR, and ASDR of mental disorders in 2020 and 2021 across different countries and territories, 6 WHO regions and 5 SDI levels. Additionally, to quantify the impact of COVID-19 and the NPIs implemented against COVID-19 on mental disorders, the difference was used as the primary metric, defined by the formula: difference = observed rate - predicted rate. Furthermore, to mitigate potential confounding factors arising from regulatory interventions, multiple multivariable generalized linear models (GLM) were constructed to investigate the association between CHI and the disparity between actual and predicted mental disorder outcomes in 2020 and 2021. CHI was stratified into low and medium-to-high groups using tertile categorization. Following this, we assessed the difference of ASPR, ASIR and ASDR for mental disorders among different CHI levels and NPIs.
ARIMA modeling was performed by R 4.3.2 leveraging the forecast::auto.arima() function, while LSTM and the hybrid model fitting and predictions were executed in Python 3.1. All results achieved statistical significance at P < 0.05 with two sides.
Results
In 2021, the global mental health burden remained substantial, with reported ASPR, ASIR, and ASDR of 13,554 (95% UI: 12,525–14,677), 5460 (95% UI: 4874–6241), and 1909 (95% UI: 1440–2438) per 100,000, respectively. These figures were notably higher in high SDI regions, including Greenland (ASPR: 18,972 [95% UI: 16,755–21,421]; ASIR: 11,345 [95% UI: 9041–14,171]; ASDR: 3062 [95% UI: 2211–4094]) and Portugal (ASPR: 19,936 [95% UI: 17,055–22,999]; ASIR: 8913 [95% UI: 7111–11,290]; ASDR: 3038 [95% UI: 2167–3968]) (Fig. 1A). Between 1990 and 2019, the global ASPR, ASIR, and ASDR of mental disorders decreased annually by 0.14% (95% [confidence interval]CI: 0.11%–0.17%), 0.18% (95% CI: 0.11%–0.24%), and 0.07% (95% CI: 0.04%–0.10%), respectively (Supplementary Figure 1). However, the COVID-19 pandemic (2020–2021) led to a significant increase in these rates, particularly in regions severely affected by the pandemic. Notable increases were observed in Greenland (ASPR: 2216; ASIR: 2436; ASDR: 440 per 100,000) and the United States (ASPR: 1935; ASIR: 1785; ASDR: 354 per 100,000) (Fig. 1B).

A ASPR, ASIR and ASDR of mental disorders in 2021; B Difference between pandemic and pre-pandemic indicated the rates odds of the mean rates of 2020–2021 minus the mean rate of 2018–2019; C Difference between actual and predicted rates during the pandemic indicated the rates odds of the actual rates of 2020–2021 minus the predicted rate of 2020–2021; D Actual and predicted rates of mental disorders from 1990 to 2021. ASPR: age-standardized prevalence rate; ASIR: age-standardized incidence rate; ASDR: age-standardized disability-adjusted life years rate.
During the pandemic, the actual disease burden exceeded predictions, with an additional ASPR of 12,528; ASIR of 4699; and ASDR of 167 per 100,000 individuals. This was especially pronounced in regions with high socioeconomic conditions, such as Greenland (ASPR: 2403; ASIR: 2656; ASDR: 483 per 100,000), the United States (ASPR: 2003; ASIR: 1758; ASDR: 363 per 100,000), and Peru (ASPR: 2221; ASIR: 1107; ASDR: 338 per 100,000) (Fig. 1C). The pandemic period also saw notable increases in both men and women across ASPR, ASIR and ASDR. Specifically, the global ASIR for men increased from a predicted 3917 to 4435 per 100,000, while for women, it rose from 5497 to 6382 per 100,000. Similarly, the ASPR for men increased from 12,010 to 12,623 per 100,000, and for women, it rose from 13,005 to 14,085 per 100,000. The ASDR for men rose from 1607 to 1715 per 100,000, and for women, it increased from 1870 to 2054 per 100,000 (Fig. 1D).
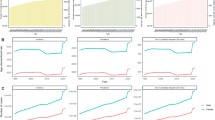
During the COVID-19 pandemic, the global ASPR, ASIR, and ASDR for mental disorders markedly exceeded pre-pandemic predictions, with the most pronounced deviations observed in high SDI regions, notably region of the Americas and European region (Fig. 2). This divergence was particularly accentuated among females. Among specific mental disorders, major depressive disorder and anxiety disorders exhibited the greatest increases, with observed ASPR, ASIR, and ASDR substantially surpassing predicted values during the pandemic period.

A: Impact of the COVID-19 Pandemic on the ASPR. B: Impact of the COVID-19 Pandemic on the ASIR. C: Impact of the COVID-19 Pandemic on the ASDR. ASPR: age-standardized prevalence rate; ASIR: age-standardized incidence rate; ASDR: age-standardized disability-adjusted life years rate.
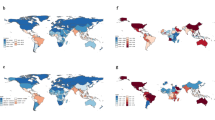
Globally, for major depressive disorder, the ASPR in Greenland and Tunisia was 780 and 532 per 100,000, respectively, exceeding the predicted values; the ASIR in Greenland was 1156 per 100,000 higher than predicted; and the ASDR in Greenland and the United States of America were 160 and 106 per 100,000, respectively higher than predicted. For anxiety disorders, Bolivia and Peru showed the largest increases above predicted levels for anxiety disorders, with ASPR at 1135 and 1043 per 100,000, ASIR at 183 and 169 per 100,000, and ASDR at 135 and 125 per 100,000, respectively (Fig. 3).

A: Impact of the COVID-19 Pandemic on the ASPR. B: Impact of the COVID-19 Pandemic on the ASIR. C: Impact of the COVID-19 Pandemic on the ASDR. ASPR: age-standardized prevalence rate; ASIR: age-standardized incidence rate; ASDR: age-standardized disability-adjusted life years rate.
The impacts of the COVID-19 pandemic on the ASPR, ASIR and ASDR of mental disorders are depicted in Fig. 4. Among 12 mental disorders, major depressive disorder and anxiety disorders exhibited the most pronounced increases in ASPR, ASIR, and ASDR, particularly among individuals aged 15–40 years, with the rise being especially marked in females. In contrast, dysthymia exhibited greater increases in the 40–70-year age group. Childhood emerged as a high-risk period for elevated ASPR and ASDR of IDID and ADHD. Furthermore, schizophrenia exhibited a notable increase in ASPR among individuals aged 35–60 years during the pandemic period.

Impact of the COVID-19 Pandemic on the ASPR, ASIR and ASDR of Mental Disorders Across Different Age Groups and Sexes.
The predicted and actual rates for mental disorders, major depressive disorder, and anxiety disorder from 1990 to 2021 were presented in Fig. 5. Predictions for mental disorders and major depressive disorder were made using an ARIMA model, while a combined ARIMA-LSTM model was employed for anxiety disorders. Both models demonstrated strong predictive performance, with RMSE and MAE values below 20 (Supplementary Table 1). During the two-year COVID-19 pandemic period (2020-2021), the global mean differences between actual and predicted rates for mental disorders were substantial: ASPR: 928; ASIR: 720; ASDR: 157 per 100,000. Major depressive disorder and anxiety disorder were the primary contributors to these differences. Specifically, for major depressive disorder, the differences were ASPR: 410; ASIR: 617; ASDR: 82 per 100,000, while for anxiety disorder, they were ASPR: 628; ASIR: 102; ASDR: 74 per 100,000.

ASPR: age-standardized prevalence rate; ASIR: age-standardized incidence rate; ASDR: age-standardized disability-adjusted life years rate.
It is noteworthy that the CHI, alongside other factors such as the female-to-male gender ratio and urban proportion, exhibits a positive correlation with the average rate differences of disease burden for mental disorders, major depressive disorder and anxiety disorders (Supplementary Figure 2A). Among these variables, the CHI stands out as a pivotal factor in influencing these disparities. Regions with a middle-high CHI score exhibited notably higher average rate differences than those with low CHI scores (Supplementary Figure 2B). In low-CHI regions, no consistent pattern was observed between average rate differences and the presence of NPIs. However, in middle-high CHI regions, average rate differences were higher in settings where NPIs included both restrictions on physical gatherings and mandatory mask use.
Discussion
In this study, the results indicated that region of Americas, European region, and other regions with high socioeconomic conditions, had higher disease burden of mental disorders, highlighting the urgent need to improve mental health services and social support systems. Compared to the pre-pandemic period, the COVID-19 pandemic showed a significant increase in the ASPR, ASIR, and ASDR of mental disorders in Greenland, Bolivia, Peru and the United States, which reflected the challenges faced by different regions in mental health during the pandemic, particularly in countries severely impacted by COVID-19 and with stringent NPIs. These findings underscore the need for global public health strategies to include mental health considerations, particularly in response to future pandemics. The disproportionate impact on major depressive and anxiety disorders among females and high-SDI regions calls for proactive mental health interventions, enhanced accessibility to services, and targeted support for vulnerable populations. Additionally, mental health should be prioritized in global policy development, ensuring sustained infrastructure and services to address both immediate and long-term mental health needs during global health crises.
This study employs both ARIMA and an ARIMA–LSTM combined model for time series forecasting [24]. ARIMA is well suited for modelling linear temporal patterns, whereas LSTM networks are capable of capturing complex nonlinear dynamics. The ARIMA–LSTM combined model has demonstrated high predictive accuracy in domains such as economics and environmental science [25]. However, its application in forecasting the burden of mental health disorders remains limited within the field of epidemiology. Our study is among the first to implement this hybrid modelling approach for predicting the burden of mental disorders. Model selection was based on RMSE and MAE, ensuring optimal model performance across scenarios. Consistent with previous findings that highlight the superior predictive performance of ARIMA–LSTM over standalone ARIMA models, our results further demonstrate reduced error metrics [18]. Notably, the combined model in our analysis achieved lower RMSE and MAE values than those reported in prior studies [26], underscoring its enhanced accuracy in this context.
The impact of COVID-19 on mental disorders is multifaceted. From a pathological standpoint, the psychopathological mechanisms underlying post-COVID-19 depression symptoms are primarily associated with the viral infection triggering a cytokine storm, leading to systemic inflammation. This excessive inflammation can damage the blood-brain barrier, resulting in central nervous system inflammation [27]. Additionally, SARS-CoV-2 can directly reach and trigger an inflammatory process within the nervous system, contributing to the development or exacerbation of mental health symptoms such as depression [28]. A national symptom monitoring survey conducted in the UK in 2020 indicated that individuals with symptomatic SARS-CoV-2 infection had a significantly higher risk of experiencing moderate to severe anxiety (OR: 2.41, 95% CI 2.01-2.90) and depression (OR: 3.64, 95% CI 3.06-4.32) compared to those who had never experienced symptoms [29]. The COVID-19 pandemic has exerted a profound and multifaceted impact on the global population, extending far beyond the direct effects of the virus itself. Rather, it is the intricate interplay of a constellation of pandemic-associated factors that has contributed to the substantial burden on mental health. These factors encompass a wide range of domains, including social, environmental, and psychological aspects, as well as the limited availability of mental health services. From a sociological perspective, the losses of financial stability, future prospects, and family resources precipitated by the COVID-19 pandemic may be associated with probable depression [30]. In addition to social factors, governmental response measures also play a significant role. Our study reveals that, globally, countries or regions with stricter implementation of NPIs have a higher disease burden of mental disorders. This observation is consistent with findings from a study of older adults in Europe, which reported that individuals living in countries with more stringent government measures were more likely to report increased levels of depression [31]. Research from various regions suggests a marked rise in the prevalence of depression and anxiety symptoms during periods of social restrictions [32, 33]. Furthermore, the highly contagious and potentially fatal nature of the virus, coupled with the pervasive fear of infection, has significantly contributed to the psychological burden and driven the increased prevalence of anxiety and depression. A global systematic review suggests that daily SARS-CoV-2 infection rates were associated with an increased prevalence of major depressive disorder (regression coefficient 18.1, 95% CI 7.9 to 28.3, p = 0.0005) and anxiety disorders (0.9, CI 0.1 to 1.7, p = 0.022) [34]. Amidst this widespread psychological strain, mental health services in many countries have been severely disrupted. The inability of some individuals to access timely professional support and treatment has further exacerbated the persistence and severity of mental health issues [35].
The study’s findings revealed that during the COVID-19 pandemic, the actual occurrence of mental disorders significantly surpassed predictions, underscoring the profound impact of the pandemic on mental health and the significant challenges countries faced in managing this crisis. This was particularly evident in the United States, Brazil, India, the United Kingdom, and Russia, where the mental health burden greatly exceeded expected levels. Additionally, the actual ASPR of mental disorders during the pandemic was significantly higher than predicted, especially in high SDI regions, such as region of the Americas and Eastern Mediterranean region, consistent with findings from previous studies [34]. Several interrelated factors may underlie this disproportionate increase. First, High SDI countries had stricter and longer lockdowns that, though necessary for infection control, limited social interactions and increased isolation, worsening mental health [36]. Secondly, heightened media exposure and the digitalisation of daily life may have amplified psychological stress, especially in populations already vulnerable to anxiety and mood disorders [37]. Finally, higher baseline expectations for economic and social stability in high SDI settings may have intensified the psychological impact of pandemic-induced uncertainties [38, 39]. In this study, the results highlight the significant and growing burden of mental disorders over the past three decades, with a particularly sharp increase observed during the COVID-19 pandemic. The marked rise in ASIR rates and ASDR for both men and women demonstrate how the pandemic has exacerbated existing mental health challenges. The discrepancy between predicted and actual outcomes indicates that current mental health systems may be inadequate to cope with the surge in cases, especially during global crises like a pandemic.
The data also reveal significant variations in the ASPR, ASIR, and health burden of mental disorders across age groups, with anxiety and depressive disorders having the most profound impact on health during middle age. In 2021, our observations revealed that while the global distribution of mental disorders remained comparable to the period from 1990 to 2019 [1], there was a notable increase in the disease burden. Depression and anxiety disorders continue to be significant contributors to the global disease burden, with ASPR and ASIR estimates that are relatively higher than other diseases. Importantly, the COVID-19 pandemic had a disproportionately greater impact on women. For both major depressive disorder and anxiety disorders, the rise in prevalence among women outpaced that observed in men. This gender gap is largely explained by the intersection of pre-existing gender inequalities with stressors introduced by the pandemic. Women experienced heightened economic pressures, including higher unemployment rates and pronounced instability in female-dominated sectors such as healthcare and education. They also shouldered increased caregiving responsibilities, frequently serving as primary caregivers for children and elderly relatives during lockdowns [40]. At the same time, a disturbing rise in gender-based violence further exacerbated psychological distress among women [41]. Together, these factors intensified the mental health burden among women, underscoring the need for gender-responsive interventions to mitigate disparities exacerbated by the pandemic. Additionally, the rise in mental health issues among middle-aged adults may be linked to increased work-related stress during the pandemic, due to sudden changes in work practices, social distancing, heightened stress, and unemployment, all of which have exacerbated the burden of mental illness in this demographic [42, 43].
Some limitations of our study should be mentioned. Firstly, due to data constraints, we were unable to incorporate countries or regions where socioeconomic indicators and NPI measures were not available, potentially introducing a bias in our assessment of the association between CHI and the average rate differences. Secondly, variations in socioeconomic conditions and NPI measures across different regions within countries were not accounted for at a finer level, which may have contributed to spatial heterogeneity in our results.
In conclusion, during the COVID-19 pandemic, the global ASPR, ASIR, and ASDR of mental disorders markedly exceeded predicted levels, with the greatest increases observed in high-SDI regions such as North America and Europe. Specific mental disorders, particularly major depressive disorder and anxiety disorders, showed substantial surges in burden. Moreover, women experienced a disproportionately higher impact from anxiety and depressive disorders. These findings demonstrate the profound adverse effect of the pandemic on global mental health, especially in high-SDI settings and among women, and highlight the urgent need to reinforce mental health services and support systems worldwide.
Data availability
The data that support the findings of this study are available from Global Burden of Disease study 2021 (http://ghdx.healthdata.org/gbd-results-tool).
References
GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry. 2022;9:137–50.
Prince M, Patel V, Saxena S, Maj M, Maselko J, Phillips MR, et al. No health without mental health. Lancet (Lond, Engl). 2007;370:859–77.
GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet (Lond, Engl). 2020;396:1204–22.
Colton CW, Manderscheid RW. Congruencies in increased mortality rates, years of potential life lost, and causes of death among public mental health clients in eight states. Prev Chronic Dis. 2006;3:A42.
Husky MM, Alvarez Fernandez V, Tapia G, Oprescu F, Navarro-Mateu F, Kovess-Masfety V. Mental disorders and medical conditions associated with causing injury or death: a population-based study. Psychiatry Res. 2020;287:112899.
Walker ER, McGee RE, Druss BG. Mortality in mental disorders and global disease burden implications: a systematic review and meta-analysis. JAMA Psychiatry. 2015;72:334–41.
Patel V, Chisholm D, Parikh R, Charlson FJ, Degenhardt L, Dua T, et al. Addressing the burden of mental, neurological, and substance use disorders: key messages from Disease Control Priorities, 3rd edition. Lancet (Lond, Engl). 2016;387:1672–85.
Jorm AF, Patten SB, Brugha TS, Mojtabai R. Has increased provision of treatment reduced the prevalence of common mental disorders? Review of the evidence from four countries. World Psychiatry. 2017;16:90–99.
Thornicroft G. Most people with mental illness are not treated. Lancet (Lond, Engl). 2007;370:807–8.
GBD 2019 Demographics Collaborators. Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950-2019: a comprehensive demographic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396:1160–203.
Daly M, Sutin AR, Robinson E. Longitudinal changes in mental health and the COVID-19 pandemic: evidence from the UK Household Longitudinal Study. Psychol Med. 2022;52:2549–58.
Romanyukha AA, Novikov KA, Avilov KK, Nestik TA, Sannikova TE. The trade-off between COVID-19 and mental diseases burden during a lockdown: Mathematical modeling of control measures. Infect Dis Model. 2023;8:403–14.
Sandmann FG, Davies NG, Vassall A, Edmunds WJ, Jit M. The potential health and economic value of SARS-CoV-2 vaccination alongside physical distancing in the UK: a transmission model-based future scenario analysis and economic evaluation. Lancet Infect Dis. 2021;21:962–74.
Durstewitz D, Koppe G, Meyer-Lindenberg A. Deep neural networks in psychiatry. Mol Psychiatry. 2019;24:1583–98.
Xu D, Zhang Q, Ding Y, Zhang D. Application of a hybrid ARIMA-LSTM model based on the SPEI for drought forecasting. Environ Sci Pollut Res Int. 2022;29:4128–44.
GBD 2021 Diabetes Collaborators. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet (Lond, Engl). 2023;402:203–34.
Hale T, Angrist N, Goldszmidt R, Kira B, Petherick A, Phillips T, et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat Hum Behav. 2021;5:529–38.
Zheng W, Li H, Yang X, Wang L, Shi Y, Shan H, et al. Trends and prediction in the incidence rate of hepatitis C in Shandong Province in China from 2004 to 2030. Prev Med. 2023;177:107749.
Yan C, Zhang Y, Zhong W, Zhang C, Xin B. A truncated SVD-Based ARIMA model for multiple QoS prediction in mobile edge computing. Tsinghua Sci Technol. 2022;27:315–24.
Khan S. Alghulaiakh H ARIMA model for accurate time series stocks forecasting. Int J Adv Comput Sci Appl. 2020;11:524–28.
Kırbaş İ, Sözen A, Tuncer AD, Kazancıoğlu FŞ. Comparative analysis and forecasting of COVID-19 cases in various European countries with ARIMA, NARNN and LSTM approaches. Chaos Solitons Fractals. 2020;138:110015.
Li Y, Ning Y, Shen B, Shi Y, Song N, Fang Y, et al. Temporal trends in prevalence and mortality for chronic kidney disease in China from 1990 to 2019: an analysis of the Global Burden of Disease Study 2019. Clin Kidney J. 2023;16:312–21.
Saif D, Sarhan AM, Elshennawy NM. Deep-kidney: an effective deep learning framework for chronic kidney disease prediction. Health Inf Sci Syst. 2024;12:3.
Wang M, Pan J, Li X, Li M, Liu Z, Zhao Q, et al. ARIMA and ARIMA-ERNN models for prediction of pertussis incidence in mainland China from 2004 to 2021. BMC Public Health. 2022;22:1447.
Xue S, Chen H, Zheng X. Detection and quantification of anomalies in communication networks based on LSTM-ARIMA combined model. Int J Mach Learn Cyber. 2022;13:3159–72.
Tsan Y-T, Chen D-Y, Liu P-Y, Kristiani E, Nguyen KLP, Yang C-T. The prediction of influenza-like illness and respiratory disease using LSTM and ARIMA. Int J Environ Res Public Health. 2022;19:1858.
Mazza MG, De Lorenzo R, Conte C, Poletti S, Vai B, Bollettini I, et al. Anxiety and depression in COVID-19 survivors: Role of inflammatory and clinical predictors. Brain Behav Immun. 2020;89:594–600.
Grolli RE, Mingoti MED, Bertollo AG, Luzardo AR, Quevedo J, Réus GZ, et al. Impact of COVID-19 in the mental health in elderly: psychological and biological updates. Mol Neurobiol. 2021;58:1905–16.
Alacevich C, Thalmann I, Nicodemo C, de Lusignan S, Petrou S. Depression and anxiety during and after episodes of COVID-19 in the community. Sci Rep. 2023;13:8257.
Mazza MG, Palladini M, Poletti S, Benedetti F. Post-COVID-19 depressive symptoms: epidemiology, pathophysiology, and pharmacological treatment. CNS Drugs. 2022;36:681–702.
Lüdecke D, von dem Knesebeck O. Decline in mental health in the beginning of the COVID-19 outbreak among european older adults-associations with social factors, infection rates, and government response. Front Public Health. 2022;10:844560.
Lok V, Sjöqvist H, Sidorchuk A, Flodin P, Osika W, Daly M, et al. Changes in anxiety and depression during the COVID-19 pandemic in the European population: a meta-analysis of changes and associations with restriction policies. Eur Psychiatry. 2023;66:e87.
Harling G, Gómez-Olivé FX, Tlouyamma J, Mutevedzi T, Kabudula CW, Mahlako R, et al. Protective behaviors and secondary harms resulting from nonpharmaceutical interventions during the COVID-19 epidemic in South Africa: multisite, prospective longitudinal study. JMIR Public Health Surveill. 2021;7:e26073.
COVID-19 Mental Disorders Collaborators. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet (Lond, Engl). 2021;398:1700–12.
Ahmed N, Barnett P, Greenburgh A, Pemovska T, Stefanidou T, Lyons N, et al. Mental health in Europe during the COVID-19 pandemic: a systematic review. Lancet Psychiatry. 2023;10:537–56.
Ahmed F, Shafer L, Malla P, Hopkins R, Moreland S, Zviedrite N, et al. Systematic review of empiric studies on lockdowns, workplace closures, and other non-pharmaceutical interventions in non-healthcare workplaces during the initial year of the COVID-19 pandemic: benefits and selected unintended consequences. BMC Public Health. 2024;24:884.
Amundsen OM, Hoffart A, Johnson SU, Ebrahimi OV. Pandemic information dissemination and its associations with the symptoms of mental distress during the COVID-19 pandemic: cross-sectional study. JMIR Form Res. 2021;5:e28239.
Agid O, Kohn Y, Lerer B. Environmental stress and psychiatric illness. Biomed Pharmacother. 2000;54:135–41.
Patel V, Saxena S, Lund C, Thornicroft G, Baingana F, Bolton P, et al. The Lancet Commission on global mental health and sustainable development. Lancet. 2018;392:1553–98.
Dai F, Cai Y, Chen M, Dai Y. Global trends of depressive disorders among women of reproductive age from 1990 to 2021: a systematic analysis of burden, sociodemographic disparities, and health workforce correlations. BMC Psychiatry. 2025;25:263.
Burki T. The indirect impact of COVID-19 on women. Lancet Infect Dis. 2020;20:904–5.
Kawohl W, Nordt C. COVID-19, unemployment, and suicide. Lancet Psychiatry. 2020;7:389–90.
Kniffin KM, Narayanan J, Anseel F, Antonakis J, Ashford SP, Bakker AB, et al. COVID-19 and the workplace: implications, issues, and insights for future research and action. Am Psychol. 2021;76:63–77.
Acknowledgements
We appreciate the valuable data shared by the Global Burden of Disease study 2021.
Funding
This study was supported by grants from the National Natural Science Foundation of China (Grant Numbers: 82173577, U23A20496, 81672005); the Mega-Project of National Science and Technology for the 13th Five-Year Plan of China (Grant Numbers: 2018ZX10715-014-002); The Zhejiang Province Vanguard Goose-Leading Initiative (2024C03216).
Author information
Authors and Affiliations
Contributions
SY, CZ, and ND conceptualized the study. MC, JM, CC, RQ, WZ, JQ, KC, XW, YW, YY, JZ, and RY collected the data. MC, JM, and CC analyzed, interpreted, and visualized the data. MC and JM wrote the preliminary draft. SY supervised the manuscript and revised it from the preliminary draft to submission. All authors reviewed and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The data used in this study does not include confidential or personally identifiable information, and the institutional review board has granted an exemption for this study. Informed consent was not needed as the study did not involve patient-specific data.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chen, M., Miao, J., Chen, C. et al. The impact of the COVID-19 pandemic on the global burden of mental disorders: a counterfactual modeling study from 1990 to 2021. Transl Psychiatry 15, 493 (2025). https://doi.org/10.1038/s41398-025-03697-6
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41398-025-03697-6
