
Abstract
Chronic Insomnia Disorder (ID) is characterized by hyperarousal, a key pathophysiological feature. While Cognitive-Behavioral Therapy for Insomnia (CBT-I) is the first-line treatment, its physiological effects on sleep-related hyperarousal remain underexplored. This study assessed the impact of CBT-I on cortical hyperarousal using quantitative EEG (qEEG) during non-REM (NREM) sleep, with the delta/beta ratio as the primary outcome. Secondary aims included evaluating changes in sleep stability and exploring phenotypic differences in treatment response. Ninety-eight ID patients across five centers completed a 6-8-week CBT-I program. Pre-and post-treatment assessments included polysomnography (PSG), sleep diaries, and Insomnia Severity Index (ISI). Cortical hyperarousal was indexed by the NREM delta/beta ratio; sleep stability (Sstab) was derived from a transition probability matrix. Patients were categorized as insomnia with short (ISSD) or normal sleep duration (INSD) based on PSG-derived total sleep time (median TST = 347.3 min). CBT-I significantly improved ISI and sleep parameters (sleep onset latency, wake after sleep onset, time in bed, sleep efficiency) in both self-reported and PSG, with smaller effects in the latter. qEEG analyses revealed a significant increase in the delta/beta ratio post-CBT-I (baseline:13.4 ± 4.9, end-of-treatment:14.6 ± 5.9; p = 0.002), indicating reduced cortical hyperarousal, with no center effects. Sstab improved significantly (p = 0.005), though it was not correlated with delta/beta changes. ISSD showed greater delta/beta improvements than INSD (p = 0.014), suggesting phenotypic differences. CBT-I reduces cortical hyperarousal in ID, as reflected by increased delta/beta ratio. The dissociation from sleep stability suggests distinct mechanisms. These findings support qEEG biomarkers as valuable tools for understanding the neurophysiological mechanisms of insomnia treatment and guiding precision medicine approaches.
Similar content being viewed by others


Introduction
Chronic insomnia disorder (ID) is the most common sleep disorder worldwide [1], imposing a substantial societal burden through heightened risks of depression and suicidality [2,3,4], cardiovascular complications and mortality [5,6,7], decreased job performance, increased absenteeism, and higher risks of disability [8, 9]. Furthermore, ID is associated with increased healthcare utilization and costs [8], as well as compromised public safety due to elevated accident risks [10]. The first-line treatment for ID is Cognitive Behavioral Therapy for Insomnia (CBT-I), a structured, multi-component intervention that includes sleep restriction, stimulus control, cognitive therapy, sleep hygiene education, and relaxation techniques [11]. Numerous reviews and meta-analyses have supported CBT-I’s efficacy and effectiveness [12] for both insomnia without comorbidities [13] and comorbid insomnia [14] (for an extensive list see [15]). Importantly, the efficacy of CBT-I is frequently evaluated using self-reported measures, such as the Insomnia Severity Index, and sleep diary indices [12]. These outcomes are valuable for assessing improvements from the patient’s perspective, reflecting perceived changes in sleep quality and daily functioning. Accordingly, current European and United States guidelines recommend subjective assessments for diagnosing ID [1, 16]. However, reliance on self-reported measures may overlook critical physiological aspects of sleep improvements, as they do not capture underlying neurophysiological changes induced by treatment. This limitation is particularly relevant for research purposes, as a deeper understanding of the psychophysiological mechanisms of CBT-I is essential [17, 18]. Furthermore, physiological evaluations of nocturnal sleep could be instrumental in identifying distinct insomnia subtypes and providing deeper insights into the disorder’s pathophysiology [19,20,21,22].
The most extensively studied pathophysiologic construct in insomnia and its treatment is the hyperarousal model [23]. According to this model, ID is characterized by heightened arousal levels persisting throughout the day-night cycle [24, 25]. This hyperarousal manifests itself at different levels [26, 27] affecting physiological functions such as heart rate and skin conductance [28, 29] and involving increased brain activity as observed in evoked potentials and electroencephalographic (EEG) frequencies [25, 30,31,32]. These conditions hinder the transition from wakefulness to sleep and contribute to sleep fragmentation [33, 34]. Likewise, fMRI (functional Magnetic Resonance Imaging) studies support insomnia-related hyperarousal, indicating altered brain activity and connectivity patterns [35, 36]. In line with this, despite the presence of all macrostructural stages, including REM and NREM, insomnia hyperarousal leads to fragmented sleep with frequent awakenings and transitions to lighter stages [37].
CBT-I aims to mitigate hyperarousal, but evidence supporting this effect on physiological processes is limited [38,39,40]. CBT-I has been linked to reductions in body temperature [41], while effects on heart rate variability and cortisol levels have been negative [41, 42]. Neuroimaging studies regarding CBT-I’s impact on hyperarousal are scarce, often constrained by methodological variations and small sample sizes [43,44,45,46]. For example, Smith et al. [47] and Lee et al. [48] observed changes in cerebral blood flow and functional connectivity following CBT-I, though these findings were limited by the absence of control groups [49].
Regarding sleep-related outcomes, findings on standard macrostructural sleep indices recorded by polysomnography (PSG) following CBT-I are controversial, with some studies reporting significant changes [50, 51] while others find no substantial effects [52, 53]. On the other hand, quantitative and microstructural EEG indices, such as high and slow frequencies [54,55,56], delta power dynamics [57], and sleep spindle indices [58], offer insights into treatment responses. As early as 2004, Cervena et al. [54] suggested that CBT-I may reduce cortical hyperarousal in psychophysiological insomnia patients, by decreasing high EEG frequencies and enhancing sleep pressure, thereby improving homeostatic sleep regulation through increased slow-wave activity. Consistently, Vallières et al. [56] reported decreases in beta-1 and −2 power during sleep restriction, indicating decreased hyperarousal. More recently, Hogan et al. [55] observed that high-frequency EEG power, in the range of sigma and beta, decreased following CBT-I. Likewise, Maurer et al. conducted a randomized controlled trial investigating the specific effects of sleep restriction therapy (SRT), a core behavioral component of CBT-I that limits time in bed to match actual sleep time in order to increase sleep pressure and consolidate sleep, on delta power and arousal levels [59]. They found that SRT significantly increased sleep pressure, leading to greater sleepiness, reduced vigilance, and decreased arousal, thereby supporting the hypothesis that SRT can effectively reduce hyperarousal and restore sleep homeostasis, particularly in the early stages of treatment. Additionally, they observed improvements in relative delta power during NREM sleep and overall sleep consolidation. Other studies have specifically focused on identifying physiological markers of sleep homeostasis, providing insights into both the pathophysiological characteristics of insomnia [60], and the mechanisms underlying treatment effects [57, 61]. Nevertheless, research on the detection of specific hyperarousal indices and their resolution, crucial for achieving sleep stability, remains scarce. A reliable indicator of hyperarousal to effectively capture the physiological improvements of CBT-I might be the delta/beta ratio, serving as a robust index of arousal levels [62,63,64] and representing an integrated electrophysiological EEG measure of neural activation [65,66,67]. This index, expressed by the ratio of the relative power of delta and beta EEG frequencies, provides a quantitative assessment of the brain’s hyperarousal state. High delta/beta ratios are typically associated with lower arousal and increased drowsiness, while lower ratios indicate heightened arousal and alertness [62]. Thus, it is a valuable tool for monitoring and interpreting changes in brain activation during sleep.
This study aimed to evaluate the efficacy of CBT-I in patients with ID by employing a comprehensive index of arousal levels derived from quantitative EEG indices of NREM sleep, specifically the delta/beta ratio as a primary outcome. Secondary analyses further explored the impact of CBT-I on physiological hyperarousal and its underlying mechanisms. Building on research emphasizing the role of sleep instability in insomnia [37], we evaluated whether CBT-I led to improvements in sleep stability, an index of physiological arousal derived from the probability of transitioning between sleep stages. Subsequently, we examined whether changes in sleep stability were associated with reductions in cortical hyperarousal, as measured by the delta/beta ratio, to determine whether these two indices capture related aspects of the physiological effects of CBT-I. Additionally, given the relevance of total sleep time (TST) in subtyping insomnia [18, 22, 68, 69] and predicting treatment outcomes [18], we examined whether TST influenced the primary outcome, the delta/beta ratio. Finally, as an exploratory aim, we investigated the relationship between the primary outcome (delta/beta ratio) and traditional efficacy markers, including PSG-derived macrostructural sleep indices, and sleep diaries. These analyses aim to provide a deeper understanding of the effects of CBT-I on the physiological dimensions of sleep hyperarousal in patients with chronic insomnia.
Materials and methods
Patients
A total of 98 participants with chronic ID were included using a retrospective multicenter data-sharing design. Specifically, we pooled pre-existing clinical and polysomnographic datasets from five research centers, each of which had previously collected data from patients who had completed a standardized CBT-I protocol. The distribution of participants was as follows: 39 individuals (38%) from the School of Psychology at Laval University in Canada, 21 individuals (21%) from Concordia University in Canada, 11 individuals (11%) from the Department of Psychiatry and Behavioral Health at Penn State University in the USA, 16 individuals (19%) from the National Institute of Mental Health’s Ward of Sleep Disorders in the Czech Republic, and 11 individuals (11%) from the Sleep Disorder Center at San Raffaele Hospital in Milan, Italy. Details regarding the clinical and research settings are reported in the supplementary materials (see Suppl. 1, sTable 1 for more details).
Study design
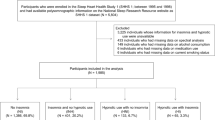
This retrospective multicenter study includes patients who were clinically evaluated and diagnosed with ID by certified sleep medicine experts at each site. Depending on the time period of data collection, clinicians applied the most recent diagnostic manual available at the time [1, 16, 70, 71]. Regardless of edition, diagnostic criteria for insomnia have remained consistent, describing a persistent report of sleep initiation or maintenance problems, adequate opportunity and circumstances to sleep, and daytime consequences. Standardized clinical interviews were performed in accordance with international guidelines to ensure consistency across centers [72]. Each participant completed a 6–8 CBT-I protocol and underwent pre- and post-treatment assessments, including PSG, Insomnia Severity Index (ISI), and one-week sleep diary (shown in Fig. 1).

Abbreviations: CBT-I: Cognitive-Behavioral Therapy for Insomnia; BL: baseline; FU: follow-up.
Exclusion criteria included untreated major medical conditions, current primary psychiatric disorders, other sleep disorders, recent shift work, changes in time zones within the prior 2 months, and the use of recreational or prescription drugs that could affect sleep or cortical electrophysiology. Participants with stable medical or selected psychiatric conditions (e.g., anxiety or depressive symptoms in remission) were eligible if these conditions were not judged to be the primary cause of insomnia and if they were not taking psychoactive medications. All patients were required to discontinue such medications prior to the baseline PSG: specifically, patients had to be benzodiazepine-free for at least one week before PSG assessment and off antidepressants for two weeks to a month prior. Thus, no EEG- or sleep-modulating medications were permitted during the recording periods.
All participants provided written informed consent to share their data for the study, which received approval from the local research ethics committee and complied with the ethical standards set forth in the 1964 Declaration of Helsinki.
Treatment
CBT-I [11, 73,74,75], administered by psychologists certified in sleep medicine, is a multi-component approach comprising psycho-education on sleep hygiene [74] and sleep health, behavioral interventions, such as stimulus control [76] and sleep restriction [77], cognitive therapy [75], as well as relaxation strategies [78] consisting of 6–8 sessions of 30–120 min each. (see Suppl. 1, sTable 1 for more details).
Measures
Self-reported outcomes
-
Insomnia Severity Index (ISI): ISI is a 7-item self-report questionnaire to evaluate subjective symptoms and daytime consequences of insomnia as well as the degree of distress caused by these difficulties. A high score indicates greater insomnia severity [79,80,81].
-
Sleep diaries: The indices of one week of pre-treatment and one-week post-treatment diaries were sleep onset latency (SOL), total sleep time (TST), time in bed (TIB), wake after sleep onset (WASO), and sleep efficiency (SE) calculated as TST / TIB × 100 [82].
Physiological outcomes
-
PSG sleep macrostructural outcomes: SOL, TST, TIB, WASO, and SE in minutes, NREM1 (stage 1 of non-REM sleep), NREM2 (stage 2 of non-REM sleep), NREM3 (stage 3 of non-REM sleep), REM (Rapid Eye Movements phase of sleep), NREM (non-REM phase of sleep) in percentages.
-
NREM EEG relative power bands: Delta (1–4 Hz) and Beta (16–30 Hz).
-
Delta/Beta Ratio: the ratio between delta and beta relative power band.
-
Stability of Sleep (Sstab): Calculated as the average of the diagonal values of NREM2, NREM3, and REM sleep within the Probability Transition Matrix, which represents the likelihood of transitioning from one sleep stage to another. Specifically, Sstab reflects the average probability of remaining in stages NREM 2, NREM 3, and REM.
-
ISSD/INSD Phenotypes: Participants were categorized into Insomnia with short sleep duration (ISSD) and Insomnia with normal sleep duration (INSD) phenotypes. This categorization was based on the baseline median PSG-derived Total Sleep Time (median TST = 347.3 min).
PSG and EEG analyses
Each polysomnographic assessment was performed following the American Academy of Sleep Medicine guidelines [83]: the montages of all sites included at least two EOG (LOC/A2 and ROC/A1) and six EEG electrodes referenced to contralateral mastoids (F3-C3-O1/A2 and F4-C4-O2/A1) and a bipolar mentalis EMG.
We used Python 3.8 as well as various libraries such as “Yasa” [84], “MNE-python” [85] “PyWavelets” [86], “Pytorch” [87] and “GPytorch” [88] for pre-processing and EEG analyses.
Pre-processing
The first step for EEG analyses was a visual inspection of PSG traces in order to assess the quality of acquisition. This step was implemented through the software EDFbrowser (https://www.teuniz.net/edfbrowser/), a free, open-source, multiplatform, universal viewer, annotator, and toolbox. The signals were downsampled at 128 Hz and filtered with a high-pass filter at 0.3 Hz and a low-pass filter at 35 Hz [83]. We performed a first 30 s epochs-visual inspection of all traces, in order to exclude from the analysis epochs contaminated by artifacts, e.g. eye movements, eye blinks, and muscular artifacts [83]. Finally, through the Python library “Yasa” [84], we executed a standard-deviation-based artifact rejection of 5-second epochs, first calculating the standard deviations in micro-volts of each epoch and each channel. The resulting array of standard deviations is log-transformed and z-scored. Epochs exceeding a z-score threshold of > 3 were marked as artifacts and excluded.
Automatic sleep stage scoring
In order to execute the sleep scoring consistently across centers, as well as to eliminate inter-rater variability, we used an automatic algorithm [84]. A central EEG derivation (C3/A2 or C4/A1), electrooculographic (EOG), and electromyographic (EMG) signals were analyzed in 30-second epochs. This algorithm comes with a default set of pre-trained classifiers, which were trained and validated on ~3000 nights from the National Sleep Research Resource, and the median accuracy across all testing nights was 87.5% [89, 90]. In addition, the Sstab index was calculated using the Probability Transition Matrix generated by the algorithm. This matrix quantifies the likelihood of transitioning from one sleep stage to another, providing a detailed representation of sleep dynamics. The Sstab index was derived as the average of the diagonal values of the Probability Transition Matrix for NREM2, NREM3, and REM sleep, which reflect the probability of a given sleep stage persisting over time. By leveraging these transitions, the algorithm offers a measure of sleep stability.
Power spectral analyses
The power spectral analyses calculated the EEG power in specific frequency bands during NREM sleep (NREM1, NREM2, and NREM3), with a sampling rate of 128 Hz. Specifically, Welch’s periodogram was used, which consists of averaging consecutive Fourier transform, with a frequency resolution of 0.25 Hz, by using 4-second sliding windows with no overlapping [91]. The analysis was conducted on a central EEG derivation (C3/A2 or C4/A1). Spectral analysis quantified the relative power in the delta (1–4 Hz) and beta (16–30 Hz) frequency bands, i.e., the power for a chosen frequency band divided by the total power derived from all of the frequency bands.
Statistical analyses
We utilized JASP software to perform statistical analyses [92]. The Shapiro-Wilk test was conducted to assess the normality of the variable distributions. For evaluating post-treatment changes in self-reported and physiological outcomes, different statistical approaches were applied based on the results of the Shapiro-Wilk test. If the Shapiro-Wilk test indicated non-significant deviation from normality, the paired sample t-test was employed, and the corresponding statistical indices, p-values, and effect sizes (Cohen’s d) were reported. Conversely, if the Shapiro-Wilk test indicated significant deviation from normality, the Wilcoxon test was utilized, with statistical indices, p-values, and effect sizes (matched rank biserial correlation) being reported. For the primary outcome of changes in the physiological index of hyperarousal Delta/Beta ratio, we employed repeated measures ANOVA, with Time (baseline vs. post-treatment) included as a within-subject factor, reporting partial eta squared (η2) as the effect size. Cohen [93] has provided benchmarks to define small (η2 = 0.01), medium (η2 = 0.06), and large (η2 = 0.14) effects. Moreover, to assess the influence of center membership on our results, Center was included as the between-subject factor. A one-way ANOVA with Brown-Forsythe homogeneity correction was performed to evaluate differences between centers in terms of Delta/Beta improvement (Delta/Beta at end of treatment – Delta/Beta at baseline). Post-hoc comparisons with Bonferroni corrections were conducted following the one-way ANOVA with Brown-Forsythe homogeneity correction to explore pairwise differences between centers in Delta/Beta ratio improvements. The Sstab index was analyzed using the Wilcoxon signed-rank test to evaluate changes in sleep stability before and after CBT-I treatment. In addition, to assess site effects on the improvement in sleep stability, Center was included as the between-subject factor, and a one-way Brown–Forsythe ANOVA was performed on the Sstab improvement index (Sstab at end of treatment − Sstab at baseline). To assess the influence of insomnia phenotypes (ISSD vs. INSD) on Delta/Beta ratio improvements, participants were categorized based on the median TST of 347.3 min. A Mann-Whitney U test was conducted, and descriptive statistics were reported. We also compared all other sleep diary, PSG-derived, and spectral improvement indices between phenotypes, selecting the appropriate test for each variable based on normality and variance assumptions (Student’s t, Welch, or Mann–Whitney as required). Lastly, to explore associations between Delta/Beta ratio improvements and other key sleep metrics, Spearman’s rank correlation coefficient (ρ) was used based on normality assumption checks. Significance levels were set at p < 0.05, and all results were interpreted accordingly.
Results
Efficacy of CBT-I
All subjectively reported indices (ISI, SOL, WASO, TIB, SE) at post-treatment displayed an amelioration (p < 0.001), except for TST (p = 0.068) (shown in Table 1).
Additionally, the PSG-derived macrostructural sleep indices—specifically SOL, WASO, TIB, and SE—showed significant improvements between pre- and post-treatment, as shown in the table (p < 0.001). However, TST did not exhibit any notable changes (p = 0.457) (shown in Table 2).
Effect of CBT-I on quantitative non-REM EEG indices
The relative power of the EEG frequency bands of NREM sleep showed an increase in the Delta band (p < 0.05) and a decrease in the Beta band (p < 0.05) following CBT-I treatment, (for more details see Suppl. 2).
In testing the main hypothesis of this research, we assessed the pre-to-post-treatment change in the Delta/Beta ratio index, an EEG measure of sleep-related cortical hyperarousal, where the higher the value, the lower the arousal level. Consistent with our research hypothesis, the results showed a statistically significant increase in the Delta/Beta ratio index following CBT-I treatment (Delta/Beta baseline: 13.4 ± 4.9, Delta/Beta end of treatment: 14.6 ± 5.9; F = 10.05; p = 0.002; η2 = 0.09) (shown in Fig. 2).

Mean ± standard error are displayed. The higher the value, the lower arousal level. *p = 0.002.
Moreover, we tested the influence of center membership on our results, and we found no differences between centers in terms of Delta/Beta amelioration (for more details see Suppl. 3).
Secondary outcomes
Effect of CBT-I on sleep stability
To further evaluate the effectiveness of CBT-I on sleep EEG hyperarousal, we assessed changes in sleep stability using the Stability of Sleep index (Sstab), calculated as the average of the diagonal values of NREM2, NREM3, and REM sleep within the Probability Transition Matrix. This index represents the likelihood of a sleep stage persisting over time, providing insight into the dynamics of sleep maintenance. The results of the paired Wilcoxon signed-rank test demonstrated a statistically significant improvement in Sstab following CBT-I treatment (Stab baseline: 0.83 ± 0.07; Sstab end of treatment: 0.85 ± 0.06; z = −2.81, p = 0.005, Rank-Biserial Correlation = −0.33) (shown in Fig. 3).

Mean ± 95% Confidence Interval are displayed. The Sstab index was calculated as the average of the diagonal values of NREM2, NREM3, and REM sleep within the Probability Transition Matrix, representing the likelihood of a given sleep stage persisting over time. *p = 0.005.
Consistent with the analysis conducted for Delta/Beta, we additionally examined whether Sstab improvement varied by center. No significant differences across centers were observed for the Sstab improvement index (Sstab at end of treatment − Sstab at baseline), indicating that improvements in sleep stability were consistent across sites (for more details see Suppl. 3).
Influence of ISSD/INSD phenotypes on Delta/Beta ratio amelioration
To examine whether the effectiveness of CBT-I on sleep EEG hyperarousal, as measured by changes in the Delta/Beta ratio, was influenced by ISSD/INSD phenotypes, participants were categorized into short sleepers (ISSD n = 49, ISIbaseline=16.6 ± 3.7, TSTbaseline=282.9 ± 52.5) and normal sleepers (INSD n = 49, ISIbaseline=17.1 ± 3.3, TSTbaseline=392.5 ± 29.8) based on the median PSG-derived Total Sleep Time (TST = 347.3) (ISSDvsINSD= ISIbaseline t = 0.76 p = 0.452; TSTbaseline U = 2401.00 p < 0.001); notably, the two groups did not differ in terms of insomnia severity. A Mann-Whitney U test revealed a statistically significant difference in Delta/Beta ratio amelioration between the two groups (U = 856.00, p = 0.014, Rank-Biserial Correlation = −0.29, SE = 0.12). The mean Delta/Beta ratio improvement was higher in the ISSD group (Delta/Beta amelioration mean = 2.0 ± 3.7) compared to the INSD group (Delta/Beta amelioration mean=0.4 ± 3.7). These results suggest that changes in the Delta/Beta ratio may vary according to insomnia subtypes defined by TST (shown in Fig. 4).

Mean ± 95% Confidence Interval are displayed. Participants were categorized based on median PSG-derived Total Sleep Time (TST = 347.3), and a significant difference was observed between the two groups (*p = 0.014).
Further analyses showed that the ISSD/INSD difference was mainly driven by a larger increase in NREM delta power in the ISSD group (p = 0.037), with no group difference in NREM beta (p = 0.117). Phenotype-related differences also emerged for PSG-defined WASO (p = 0.002), TST (p < 0.001), and SE (p < 0.001). Detailed results are available in the Supplementary Materials (see Suppl. 4).
Associations between Delta/Beta ratio improvements and sleep metrics
As part of the exploratory analyses, we examined the relationships between Delta/Beta ratio amelioration and the improvements in PSG and subjective sleep indices. Significant positive correlations were observed between Delta/Beta ratio amelioration and sleep diary-based TIB amelioration (Spearman’s ρ = 0.22, p = 0.034). Additionally, significant positive associations were found with PSG-derived WASO amelioration (Spearman’s ρ = 0.50, p < 0.001) and PSG-derived SE amelioration (Spearman’s ρ = 0.33, p = 0.001). These findings indicate a relationship between improvements in cortical hyperarousal, as indexed by Delta/Beta ratio amelioration, and enhancements in both sleep diary and PSG-derived sleep metrics (shown in Table 3).
Discussion
This multicenter study represents the first study to evaluate the effectiveness of CBT-I in reducing cortical hyperarousal using a comprehensive electrophysiological index derived from qEEG during NREM sleep, namely the delta/beta ratio. By employing this measure, we aimed to deepen the understanding of the neurophysiological mechanisms underlying insomnia treatment, providing a potential biomarker within the context of CBT-I, and novel insights into its impact on cortical hyperarousal, a well-established pathophysiological construct in insomnia.
First, we confirmed that CBT-I showed the expected effectiveness for self-reported sleep parameters (ISI, SOL, WASO, TIB, SE). Additionally, PSG indices showed the expected improvements in SOL, WASO, TIB, and SE, albeit with lower effect sizes than sleep diary self-reports. Second, we showed a statistically significant increase in the Delta/Beta ratio index following CBT-I treatment, indicating a reduction in cortical hyperarousal with no influence of center membership, confirming the hypothesis of this study (for a schematic overview of the computation and clinical interpretation of the Delta/Beta ratio, see Suppl. 5, sFigure 1). Further analyses revealed that CBT-I enhanced sleep stability with no influence of center membership, as reflected by an improvement in the Stability of Sleep index (for a schematic overview of the computation and clinical interpretation of the Sstab index, see Suppl. 5, sFigure 2), although this improvement does not seem to be related to the improvement of our primary outcome. Moreover, short sleepers showed greater improvements in the Delta/Beta ratio compared to normal sleepers, suggesting phenotypic differences in treatment response. Finally, exploratory analyses revealed associations between Delta/Beta ratio improvements and both self-reported (TIB) and physiological measures (WASO and SE) of sleep quality.
Effectiveness of CBT-I in improving macrostructural self-reported and PSG sleep measures
Consistent with previous findings [12], CBT-I led to significant improvements in self-reported sleep parameters, including ISI, SOL, WASO, TIB, and SE. Additionally, PSG-based indices showed improvements in SOL, WASO, TIB, and SE, although with smaller effect sizes than those observed for self-reported sleep measures. These findings align with meta-analyses and clinical practice guidelines [15, 94] that have consistently demonstrated CBT-I as an effective intervention for insomnia, with strong evidence supporting its impact on both self-reported and physiological sleep parameters, although the latter report less consistent results [50,51,52,53].
CBT-I effects on cortical hyperarousal
A key finding of this study was the significant increase in the delta/beta ratio following CBT-I, supporting the hypothesis that CBT-I reduces cortical hyperarousal. This result aligns with previous research demonstrating changes in slow and fast EEG frequencies after behavioral interventions targeting insomnia.
Prior studies have reported an increase in slow-frequency activity (i.e., absolute or relative power in slow-wave activity or the delta band) and a decrease in fast-frequency activity (i.e., absolute or relative power in sigma, beta, beta-1, or beta-2 bands) following CBT-I or its core component, sleep restriction therapy (SRT) [54, 55, 59]. These spectral power analyses suggest that non-pharmacological behavioral therapies may promote either a reduction in cortical hyperarousal, an increase in sleep pressure indicative of more efficient homeostatic sleep regulation, or both. More specifically, decreased beta-1 and beta-2 power after a single night of SRT has been interpreted as a sign of reduced hyperarousal [56]. Similarly, Cervena et al. [54] observed a reduction in high-frequency EEG activity alongside an increase in slow-wave activity, suggesting a strengthening of sleep homeostasis in psychophysiological insomnia patients. Consistent with these findings, our study demonstrated a significant increase in relative delta power and a decrease in relative beta power following CBT-I, further supporting the role of behavioral interventions in modulating arousal levels during sleep. Additionally, Hogan et al. [55] reported a reduction in high-frequency EEG power, specifically in the sigma and beta bands, following CBT-I, reinforcing the idea that treatment influences cortical excitability. Maurer et al. [59] further highlighted the impact of SRT on various arousal and sleep pressure indices, showing that power spectral analysis of NREM sleep demonstrated an increase in relative, but not absolute, EEG delta power, along with a decrease in relative EEG beta power. Together, these findings suggest that CBT-I induces neurophysiological changes consistent with both a reduction in hyperarousal and an enhancement of sleep homeostasis. The delta/beta ratio, as assessed in this study, integrates these effects into a single index, capturing the interplay between fast- and slow-frequency EEG activity. As such, it emerges as a promising biomarker, particularly in research, for monitoring the neurophysiological response to CBT-I in insomnia patients and assessing its underlying mechanism of action.
Sleep stability and its relationship with cortical hyperarousal
Our findings indicate that CBT-I improves sleep stability, as evidenced by an increase in the Sstab index. However, this improvement was not directly correlated with changes in the delta/beta ratio, suggesting that these measures capture distinct aspects of sleep regulation.
Given that sleep instability has been associated with cortical hyperarousal, this dissociation warrants further investigation. Insomnia is characterized by increased EEG activity across multiple frequency bands, which has been linked to persistent cortical processing during sleep, leading to disrupted sleep continuity and frequent state transitions [95, 96]. Notably, individuals with insomnia exhibit a greater probability of transitioning to lighter sleep stages, which may prevent the consolidation of deeper sleep [37]. Neuroimaging studies suggest that CBT-I may influence both cortical and subcortical brain regions involved in sleep-wake regulation. Increased regional cerebral blood flow in the basal ganglia has been reported following CBT-I [47], while other studies have identified changes in functional connectivity in key regulatory structures, such as the thalamus, amygdala, caudate nucleus, and orbitofrontal cortex [48]. Additionally, enhanced connectivity between the default-mode network and the premotor/dorsolateral prefrontal cortex has been correlated with improved sleep [49]. These findings suggest that CBT-I may restore the balance between wakefulness and sleep, possibly through its effects on both cortical excitability and state transition stability, rather than directly reducing hyperarousal [35, 97].
While CBT-I improved both cortical arousal and sleep stability, their lack of correlation suggests partially independent neurophysiological mechanisms. One possibility is that CBT-I acts on multiple regulatory pathways, modulating both EEG spectral power (hyperarousal) and state transition dynamics (stability). Alternatively, the delta/beta ratio may not fully capture all aspects of hyperarousal that contribute to sleep instability, highlighting the need for further investigation with alternative EEG-derived indices. This interpretation is also consistent with the fact that delta/beta and Sstab reflect distinct facets of sleep regulation: the former indexes microstructural cortical arousal within stable NREM epochs, whereas the latter captures the probability of maintaining or switching vigilance states—processes influenced by homeostatic pressure, circadian stability, and autonomic balance, in addition to cortical activation. As a consequence, CBT-I may exert its effects along partially separate pathways, with cognitive components primarily targeting cortical hyperarousal and behavioral components (e.g., sleep restriction) more strongly shaping sleep-state dynamics [98]. Interindividual variability in how patients respond to these components may further decouple changes in the two indices. Moreover, Sstab typically shows greater night-to-night variability than spectral measures, which may reduce sensitivity to detect correlations in single-night data. Taken together, these considerations suggest that delta/beta and Sstab represent complementary, rather than tightly coupled, dimensions of CBT-I–related improvement.
Phenotypic differences in treatment response
This study provides further evidence that individuals with insomnia and short sleep duration (ISSD) exhibit a distinct treatment response to CBT-I compared to those with normal sleep duration (INSD). Specifically, we found that ISSD individuals demonstrated greater improvements in the delta/beta ratio following CBT-I, suggesting a stronger reduction in cortical hyperarousal. These findings challenge the traditional two-phenotype model of insomnia, which posits that ISSD is primarily characterized by physiological hyperarousal—including HPA axis overactivation and increased autonomic activity—whereas INSD is associated more with cortical and cognitive-emotional hyperarousal [99, 100]. Importantly, while ISSD individuals exhibited significant improvements in cortical hyperarousal following CBT-I, TST did not increase at the overall sample level. This pattern aligns with prior evidence indicating that, unlike pharmacological treatments capable of extending TST in ISSD, CBT-I does not reliably produce such an effect [101, 102]. These findings raise questions about whether CBT-I’s effect on ISSD reflects genuine sleep physiology improvements or primarily targets cognitive-emotional hyperarousal. It is possible that ISSD individuals exhibit both forms of hyperarousal, with cortical hyperarousal being more responsive to CBT-I. Although this pattern was not detectable at the overall sample level, phenotype-stratified analyses indicated that ISSD patients showed relatively greater improvements in PSG-defined WASO, TST, and SE, as well as a more pronounced increase in NREM delta power, compared with INSD. This pattern suggests a stronger homeostatic sleep-drive response to CBT-I within the ISSD subgroup. At the same time, despite the fact that ISSD individuals showed physiological improvements, prior evidence indicates that they may still exhibit lower remission and response rates compared with INSD patients. Indeed, studies have reported mixed findings regarding ISSD and INSD responses to CBT-I, with recent meta-analytic evidence suggesting that ISSD individuals exhibit a 26% lower remission rate and a 29% lower response rate compared to INSD patients [18]. Nevertheless, these findings are constrained by methodological limitations, including small sample sizes, heterogeneity in age, gender, and assessment methods (actigraphy vs. PSG), as well as variability in CBT-I treatment components across studies. While our results indicate that CBT-I effectively reduces cortical hyperarousal in ISSD, further research is needed to determine whether these improvements translate into sustained clinical benefits. Future studies should explore whether individualized treatment approaches—such as combining CBT-I with pharmacological interventions for ISSD patients—can enhance treatment outcomes and whether reductions in hyperarousal predict long-term improvements in insomnia severity.
Links between Delta/Beta changes and sleep metrics
Exploratory correlations revealed that greater delta/beta improvement was associated with reductions in PSG-defined WASO, increases in PSG sleep efficiency, and changes in diary-based TIB. This pattern is consistent with the notion that improvements in sleep continuity and consolidation occur alongside parallel reductions in cortical hyperarousal [59], without implying a specific causal direction. The association with diary-based TIB may reflect patients’ progressive recalibration of sleep opportunity as their sleep becomes more consolidated during CBT-I, in line with the behavioral principles of sleep restriction [11]. Nonetheless, these interpretations remain speculative, and the directionality of these relationships cannot be inferred from the present data. Future studies should investigate whether specific components of CBT-I differentially mediate the link between reduced hyperarousal and improved sleep continuity.
Strengths and limitations
A key strength of this study is its multicenter design, which enhances the generalizability of our findings. This structure naturally introduced heterogeneity in CBT-I delivery across sites, including differences in format (group vs. individual), number of sessions, treatment duration, and group size. That consistent improvements emerged across these diverse protocols underscores both the flexibility of CBT-I and the robustness of the observed clinical and neurophysiological effects. Consistently, we detected no effect of center membership on improvements in either the delta/beta ratio or the sleep stability indices. Finally, the use of a physiological, EEG-based index of cortical hyperarousal (delta/beta ratio) provides novel insights into the neurophysiological effects of CBT-I.
However, several limitations should be noted. First, the lack of a control group limits the ability to draw causal inferences regarding the specific effects of CBT-I; however, this limitation is partly mitigated by the within-subject, multicenter design and the consistency of results across sites. At the same time, while our findings support the role of CBT-I in reducing cortical hyperarousal, we were unable to disentangle the contributions of specific CBT-I components (e.g., sleep restriction, stimulus control, cognitive therapy) to these effects. Furthermore, the use of a single central EEG derivation precludes detailed analyses of topographical changes in brain activity before and after treatment. Also, PSG and qEEG outcomes were derived from a limited number of nights (baseline and post-treatment only). Although this approach aligns with standard clinical and research practice in CBT-I trials, it may not fully capture night-to-night variability in sleep architecture and cortical arousal. Finally, while all PSG signals were visually inspected and cleaned before automated staging, no internal validation against manual scoring was performed in this cohort. This limitation should be viewed in the context of the fact that the algorithm’s training datasets included only a small proportion of individuals with insomnia (4.50–6.95%), which may further affect staging reliability in this population.
Conclusions and future directions
Despite these limitations, our findings highlight the potential utility of PSG-derived qEEG metrics, such as the delta/beta ratio, in evaluating the neurophysiological effects of CBT-I, to refine mechanistic models of treatment response.
While our results demonstrate that CBT-I effectively reduces cortical hyperarousal, an important question remains regarding the durability of this effect. Specifically, it is unclear whether reductions in hyperarousal persist beyond the treatment period or if they are primarily driven by the more intensive sleep restriction phase of CBT-I. Future research should investigate whether qEEG measures can help identify individuals at higher risk for relapse and whether hyperarousal reductions serve as a predictor of long-term treatment success. Longitudinal studies with extended follow-ups will be critical in addressing these questions and clarifying the trajectory of neurophysiological changes post-CBT-I. Additionally, further characterization of EEG markers related to sleep homeostasis and cortical arousal—both across full treatment protocols and within individual CBT-I components—may provide deeper insights into the mechanisms underlying treatment response. Given the scarcity of neuroimaging studies examining the neurobiological effects of CBT-I, future work would benefit from integrating EEG with neuroimaging modalities such as fMRI. A multimodal approach could provide complementary perspectives on cortical, subcortical, and network-level mechanisms of hyperarousal, thereby accelerating mechanistic discovery and enhancing the development of precision interventions. Moreover, integrating self-reported, macrostructural, and microstructural sleep measures will enhance the understanding of individual differences in both clinical outcomes and underlying neurophysiological mechanisms.
Finally, by advancing EEG-based biomarkers, future research can enhance precision-based interventions for insomnia while providing deeper insights into the neurobiological mechanisms underlying sleep disturbances and CBT-I’s mode of action. Specifically, refining these biomarkers may help elucidate how CBT-I modulates cortical arousal, sleep homeostasis, and stability, ultimately guiding more targeted therapeutic approaches. This advancement should also support the implementation of innovative strategies, to better address the heterogeneity of insomnia disorder [17, 18, 21, 103].
Data availability
The data supporting the findings of this study are available upon request to the corresponding author. The data are not publicly available because they contain information that could compromise the privacy of research participants.
References
American Academy of Sleep Medicine. The international classification of sleep disorders (ICSD-3). 2014.
Baglioni C, Battagliese G, Feige B, Spiegelhalder K, Nissen C, Voderholzer U, et al. Insomnia as a predictor of depression: A meta-analytic evaluation of longitudinal epidemiological studies. J Affect Disord. 2011;135:10–19.
Rössler W, Angst J, Ajdacic-Gross V, Haker H, Berrouiguet S, Ujeyl M, et al. Sleep disturbances and suicidality–a longitudinal analysis from a representative community study over 30 years. Front Psychiatry. 2018;9:320.
Hertenstein E, Benz F, Schneider CL, Baglioni C. Insomnia—A risk factor for mental disorders. J Sleep Res. 2023;32:e13930.
Vgontzas AN, Liao D, Pejovic S, Calhoun S, Karataraki M, Basta M, et al. Insomnia with short sleep duration and mortality: The Penn state cohort. Sleep. 2010;33:1159–64.
Vgontzas AN, Liao D, Bixler EO, Chrousos GP, Vela-Bueno A. Insomnia with objective short sleep duration is associated with a high risk for hypertension. Sleep. 2009;32:491–7.
Li Y, Vgontzas AN, Fernandez-Mendoza J, Bixler EO, Sun Y, Zhou J, et al. Insomnia with physiological hyperarousal is associated with hypertension. Hypertension. 2015;65:644–50.
Daley M, Morin CM, LeBlanc M, Grégoire J-P, Savard J. The economic burden of insomnia: direct and indirect costs for individuals with insomnia syndrome, insomnia symptoms, and good sleepers. Sleep. 2009;32:55–64.
Sivertsen B, Overland S, Neckelmann D, Glozier N, Krokstad S, Pallesen S, et al. The long-term effect of insomnia on work disability. Am J Epidemiol. 2006;163:1018–24.
Garbarino S, Magnavita N, Guglielmi O, Maestri M, Dini G, Bersi FM, et al. Insomnia is associated with road accidents. Further evidence from a study on truck drivers. PLoS ONE. 2017;12:e0187256.
Baglioni C, ECA, & RD. Cognitive-Behavioural Therapy For Insomnia (CBT-I) Across The Life Span. Wiley; 2022.
van Straten A, van der Zweerde T, Kleiboer A, Cuijpers P, Morin CM, Lancee J. Cognitive and behavioral therapies in the treatment of insomnia: A meta-analysis. Sleep Med Rev. 2018;38:3–16.
Trauer JM, Qian MY, Doyle JS, Rajaratnam SMW, Cunnington D. Cognitive behavioral therapy for chronic insomnia: A systematic review and meta-analysis. Ann Intern Med. 2015;163:191–204.
Geiger-Brown JM, Rogers VE, Liu W, Ludeman EM, Downton KD, Diaz-Abad M. Cognitive behavioral therapy in persons with comorbid insomnia: A meta-analysis. Sleep Med Rev. 2015;23:54–67.
Riemann D, Espie CA, Altena E, Arnardottir ES, Baglioni C, Bassetti CLA, et al. The European Insomnia Guideline: An update on the diagnosis and treatment of insomnia 2023. J Sleep Res. 2023;32:e14035.
American Psychiatric Association. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders Fifth Edition. 2013.
Galbiati A, Sforza M, Fasiello E, Castronovo V, Ferini-Strambi L. Impact of phenotypic heterogeneity of insomnia on the patients’ response to cognitive-behavioral therapy for insomnia: current perspectives. Nat Sci Sleep. 2019;ume 11:367–76.
He D, Guo Z, Mcclure MA, Mu Q, Jiang B. Cognitive-behavioral therapy for insomnia with objective short sleep duration phenotype: A systematic review with meta-analysis. Sleep Med Rev. 2023;67:101736.
Ancoli-Israel S, Cole R, Alessi C, Chambers M, Moorcroft W, Pollak CP. The role of actigraphy in the study of sleep and circadian rhythms. Sleep. 2003;26:342–92.
Crönlein T, Geisler P, Langguth B, Eichhammer P, Jara C, Pieh C, et al. Polysomnography reveals unexpectedly high rates of organic sleep disorders in patients with prediagnosed primary insomnia. Sleep Breath. 2012;16:1097–103.
Ferini-Strambi L, Fossati A, Sforza M, Galbiati A. Subtyping insomnia disorder. Lancet Psychiatry. 2019;6:284.
Nyhuis CC, Fernandez-Mendoza J. Insomnia nosology: a systematic review and critical appraisal of historical diagnostic categories and current phenotypes. J Sleep Res. 2023;32:e13910.
Morin CM, Drake CL, Harvey AG, Krystal AD, Manber R, Riemann D, et al. Insomnia disorder. Nat Rev Dis Primers. 2015. 2015. https://doi.org/10.1038/nrdp.2015.26.
Pérusse AD, Turcotte I, St-Jean G, Ellis J, Hudon C, Bastien CH. Types of primary insomnia: Is hyperarousal also present during napping?. J Clin Sleep Med. 2013;09:1273–80.
Dai Y, Ma J, Vgontzas AN, Chen B, Chen L, Wu J, et al. Insomnia disorder is associated with 24-hour cortical hyperarousal. Sleep Med. 2024;124:681–7.
Perlis ML, Merica H, Smith MT, Giles DE. Beta EEG activity and insomnia. Sleep Med Rev. 2001;5:365–76.
Vgontzas AN, Bixler EO, Lin H-M, Prolo P, Mastorakos G, Vela-Bueno A, et al. Chronic insomnia is associated with nyctohemeral activation of the hypothalamic-pituitary-adrenal axis: Clinical implications. J Clin Endocrinol Metab. 2001;86:3787–94.
Perlis ML, Smith MT, Pigeon WR. Etiology and pathophysiology of insomnia. Principles and Practice of Sleep Medicine. 2005.
Vgontzas AN, Tsigos C, Bixler EO, Stratakis CA, Zachman K, Kales A, et al. Chronic insomnia and activity of the stress system: A preliminary study. J Psychosom Res. 1998;45:21–31.
Bastien CH, Turcotte I, St-Jean G, Morin CM, Carrier J. Information processing varies between insomnia types: Measures of N1 and P2 during the night. Behav Sleep Med. 2013;11:56–72.
Turcotte I, St-Jean G, Bastien CH. Are individuals with paradoxical insomnia more hyperaroused than individuals with psychophysiological insomnia? Event-related potentials measures at the peri-onset of sleep. Int J Psychophysiol. 2011;81:177–90.
Zhao W, Van Someren EJW, Li C, Chen X, Gui W, Tian Y, et al. EEG spectral analysis in insomnia disorder: A systematic review and meta-analysis. Sleep Med Rev. 2021;59:101457.
Riemann D, Spiegelhalder K, Nissen C, Hirscher V, Baglioni C, Feige B REM Sleep Instability – A New Pathway for Insomnia? Pharmacopsychiatry. 2012. 30 January 2012. https://doi.org/10.1055/s-0031-1299721.
Feige B, Nanovska S, Baglioni C, Bier B, Cabrera L, Diemers S, et al. Insomnia - Perchance a dream? Results from a NREM/REM sleep awakening study in good sleepers and patients with insomnia. Sleep. 2018;41:https://doi.org/10.1093/sleep/zsy032.
Kay DB, Buysse DJ. Hyperarousal and beyond: New insights to the pathophysiology of insomnia disorder through functional neuroimaging studies. Brain Sci. 2017;7:23.
Zou G, Li Y, Liu J, Zhou S, Xu J, Qin L, et al. Altered thalamic connectivity in insomnia disorder during wakefulness and sleep. Hum Brain Mapp. 2021;42:259–70.
Van Someren EJW. Brain mechanisms of insomnia: new perspectives on causes and consequences. Physiol Rev. 2021;101:995–1046.
Rosen RC, Lewin DS, Goldberg L, Woolfolk RL. Psychophysiological insomnia: combined effects of pharmacotherapy and relaxation-based treatments. Sleep Med. 2000;1:279–88.
Vincent N, Lewycky S. Logging on for better sleep: RCT of the effectiveness of online treatment for insomnia. Sleep. 2009;32:807–15.
Wu R, Bao J, Zhang C, Deng J, Long C. Comparison of sleep condition and sleep-related psychological activity after cognitive-behavior and pharmacological therapy for chronic insomnia. Psychother Psychosom. 2006;75:220–8.
Miller CB, Kyle SD, Gordon CJ, Espie CA, Grunstein RR, Mullins AE, et al. Physiological markers of arousal change with psychological treatment for insomnia: A preliminary investigation. PLoS ONE. 2015;10:e0145317.
Jarrin DC, Chen IY, Ivers H, Lamy M, Vallières A, Morin CM. Nocturnal heart rate variability in patients treated with cognitive–behavioral therapy for insomnia. Health Psychol. 2016;35:638–41.
O’Byrne JN, Berman Rosa M, Gouin JP, Dang-Vu TT. Neuroimaging findings in primary insomnia. Pathologie Biologie. 2014;62:262–9.
Spiegelhalder K, Regen W, Baglioni C, Nissen C, Riemann D, Kyle SD. Neuroimaging insights into insomnia. Curr Neurol Neurosci Rep. 2015;15:9.
Spiegelhalder K, Regen W, Baglioni C, Riemann D, Winkelman JW. Neuroimaging Studies in Insomnia. Curr Psychiatry Rep. 2013;15:405.
Tahmasian M, Noori K, Samea F, Zarei M, Spiegelhalder K, Eickhoff SB, et al. A lack of consistent brain alterations in insomnia disorder: An activation likelihood estimation meta-analysis. Sleep Med Rev. 2018;42:111–8.
Smith MT, Perlis ML, Chengazi VU, Soeffing J, McCann U. NREM sleep cerebral blood flow before and after behavior therapy for chronic primary insomnia: preliminary single photon emission computed tomography (SPECT) data. Sleep Med. 2005;6:93–94.
Lee YJG, Kim S, Kim N, Choi JW, Park J, Kim SJ, et al. Changes in subcortical resting-state functional connectivity in patients with psychophysiological insomnia after cognitive–behavioral therapy: Changes in resting-state FC after CBT for insomnia patients. Neuroimage Clin. 2018;17:115–23.
Park HY, Lee H, Jhee JH, Park KM, Choi EC, An SK, et al. Changes in resting-state brain connectivity following computerized cognitive behavioral therapy for insomnia in dialysis patients: A pilot study. Gen Hosp Psychiatry. 2020;66:24–29.
Morin CM, Colecchi C, Stone J, Sood R, Brink D. Behavioral and pharmacological therapies for late-life insomnia. JAMA. 1999;281:991.
Morin CM, Vallières A, Guay B, Ivers H, Savard J, Mérette C, et al. Cognitive Behavioral Therapy, Singly and Combined With Medication, for Persistent Insomnia. JAMA. 2009;301:2005.
Mitchell LJ, Bisdounis L, Ballesio A, Omlin X, Kyle SD. The impact of cognitive behavioural therapy for insomnia on objective sleep parameters: A meta-analysis and systematic review. Sleep Med Rev. 2019.
Perrault AA, Pomares FB, Smith D, Cross NE, Gong K, Maltezos A, et al. Effects of cognitive behavioral therapy for insomnia on subjective and objective measures of sleep and cognition. Sleep Med. 2022;97:13–26.
Cervena K, Dauvilliers Y, Espa F, Touchon J, Matousek M, Billiard M, et al. Effect of cognitive behavioural therapy for insomnia on sleep architecture and sleep EEG power spectra in psychophysiological insomnia. J Sleep Res. 2004. 2004. https://doi.org/10.1111/j.1365-2869.2004.00431.x.
Hogan SE, Delgado GM, Hall MH, Nimgaonkar VL, Germain A, Buysse DJ, et al. Slow-oscillation activity is reduced and high frequency activity is elevated in older adults with insomnia. J Clin Sleep Med. 2020. 2020. https://doi.org/10.5664/jcsm.8568.
Vallières A, Ceklic T, Bastien CH, Espie CA. A preliminary evaluation of the physiological mechanisms of action for sleep restriction therapy. Sleep Disord. 2013;2013:1–15.
Krystal AD, Edinger JD Sleep EEG predictors and correlates of the response to cognitive behavioral therapy for insomnia. Sleep. 2010. 2010. https://doi.org/10.1093/sleep/33.5.669.
Dang-Vu TT, Hatch B, Salimi A, Mograss M, Boucetta S, O’Byrne J, et al. Sleep spindles may predict response to cognitive-behavioral therapy for chronic insomnia. Sleep Med. 2017. 2017. https://doi.org/10.1016/j.sleep.2017.08.012.
Maurer LF, Espie CA, Omlin X, Emsley R, Kyle SD. The effect of sleep restriction therapy for insomnia on sleep pressure and arousal: a randomized controlled mechanistic trial. Sleep. 2022;45:zsab223.
Lunsford-Avery JR, Edinger JD, Krystal AD. Optimizing computation of overnight decline in delta power: Evidence for slower rate of decline in delta power in insomnia patients. Clin Neurophysiol. 2021;132:545–53.
Sforza M, Morin CM, Dang-Vu TT, Pomares FB, Perrault AA, Gouin J, et al. Cognitive-behavioural therapy for insomnia mechanism of action: Exploring the homeostatic K-complex involvement. J Sleep Res. 2024. 30 December 2024. https://doi.org/10.1111/jsr.14452.
Krystal AD. Non-REM sleep EEG spectral analysis in insomnia. Psychiatr Ann. 2008;38:615–20.
Maes J, Verbraecken J, Willemen M, De Volder I, van Gastel A, Michiels N, et al. Sleep misperception, EEG characteristics and Autonomic Nervous System activity in primary insomnia: A retrospective study on polysomnographic data. Int J Psychophysiol. 2014;91:163–71.
Gorgoni M, Scarpelli S, Annarumma L, D’atri A, Alfonsi V, Ferrara M, et al. The regional eeg pattern of the sleep onset process in older adults. Brain Sci. 2021;11:1261.
D’Atri A, Scarpelli S, Schiappa C, Pizza F, Vandi S, Ferrara M, et al. Cortical activation during sleep predicts dream experience in narcolepsy. Ann Clin Transl Neurol. 2019;6:445–55.
Scarpelli S, D’atri A, Bartolacci C, Gorgoni M, Mangiaruga A, Ferrara M, et al. Dream recall upon awakening from non-rapid eye movement sleep in older adults: Electrophysiological pattern and qualitative features. Brain Sci. 2020;10:343.
Fasiello E, Gorgoni M, Galbiati A, Sforza M, Berra F, Scarpelli S, et al. Decreased Delta/Beta ratio index as the sleep state-independent electrophysiological signature of sleep state misperception in Insomnia disorder: A focus on the sleep onset and the whole night. Neuroimage. 2024;298:120782.
Dai Y, Vgontzas AN, Chen L, Zheng D, Chen B, Fernandez-Mendoza J, et al. A meta-analysis of the association between insomnia with objective short sleep duration and risk of hypertension. Sleep Med Rev. 2024;75:101914.
Saulnier KG, Singh R, Lenker KP, Calhoun SL, He F, Liao D, et al. Association of insomnia phenotypes based on polysomnography-measured sleep duration with suicidal ideation and attempts. Sleep Health. 2022;8:391–7.
American Academy of Sleep Medicine. International Classification of Sleep Disorders: Diagnostic and Coding Manual. (ICSD-2). 2005.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-IV. Washington, DC; 1994.
Sateia MJ. International classification of sleep disorders-third edition highlights and modifications. Chest. 2014;146:1387–94. https://doi.org/10.1378/chest.14-0970. International classification of sleep disorders-third edition Sateia, M. J. (2014)highlights and m. Chest. 2014.
Espie CA The psychological treatment of insomnia. Chichester: Wiley; 1991.
Hauri PJ Sleep Hygiene, Relaxation Therapy, and Cognitive Interventions. In: Case Studies in Insomnia. Boston, MA: Springer US; 1991. pp. 65–84.
Morin CM Insomnia: Psychological assessment and management. Guilford Press; 1993.
Bootzin RR, Epstein D, Wood JM Stimulus Control Instructions. In: Case Studies in Insomnia. Boston, MA: Springer US; 1991. pp. 19–28.
Spielman AJ, Saskin P, Thorpy MJ. Treatment of chronic insomnia by restriction of time in bed. Sleep. 1987;10:45–56.
Lichstein KLL Clinical relaxation strategies. New York: Wiley; 1988.
Bastien C. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2:297–307.
Castronovo V, Galbiati A, Marelli S, Brombin C, Cugnata F, Giarolli L, et al. Validation study of the Italian version of the Insomnia Severity Index (ISI). Neurol Sci. 2016;37:1517–24.
Morin CM, Belleville G, Bélanger L, Ivers H. The insomnia severity index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep. 2011;34:601–8.
Natale V, Léger D, Bayon V, Erbacci A, Tonetti L, Fabbri M, et al. The consensus sleep diary: Quantitative criteria for primary insomnia diagnosis. Psychosom Med. 2015;77:413–8.
Berry RB, Budhiraja R, Gottlieb DJ, Gozal D, Iber C, Kapur VK, et al. Rules for scoring respiratory events in sleep: Update of the 2007 AASM manual for the scoring of sleep and associated events. J Clin Sleep Med. 2012. 2012. https://doi.org/10.5664/jcsm.2172.
Vallat R, Walker MP. An open-source, high-performance tool for automated sleep staging. eLife. 2021;10:e70092.
Gramfort A. MEG and EEG data analysis with MNE-Python. Front Neurosci. 2013;7:267.
Lee G, Gommers R, Waselewski F, Wohlfahrt K, O’Leary A. PyWavelets: A Python package for wavelet analysis. J Open Source Softw. 2019;4:1237.
Adam Paszke SGFMSC. PyTorch: an imperative style, highperformance deep learning library. Vancouver; 2019.
Gardner JGPKQWDBAGW. GPyTorch: Blackbox Matrix-Matrix Gaussian Process Inference with GPU Acceleration. Montreal; 2018.
Dean DA, Goldberger AL, Mueller R, Kim M, Rueschman M, Mobley D, et al. Scaling up scientific discovery in sleep medicine: The national sleep research resource. Sleep. 2016;39:1151–64.
Zhang G-Q, Cui L, Mueller R, Tao S, Kim M, Rueschman M, et al. The National Sleep Research Resource: towards a sleep data commons. J Am Med Inform Assoc. 2018;25:1351–8.
Welch P. The use of fast Fourier transform for the estimation of power spectra: A method based on time averaging over short, modified periodograms. IEEE Trans Audio Electroacoust. 1967;15:70–3.
Love J, Selker R, Marsman M, Jamil T, Dropmann D, Verhagen J, et al. JASP: Graphical statistical software for common statistical designs. J Stat Softw. 2019;88:1–17.
Cohen J Statistical power analysis for the behavioural sciences. Hillside. NJ: Lawrence Earlbaum Associates; 1988.
Edinger JD, Arnedt JT, Bertisch SM, Carney CE, Harrington JJ, Lichstein KL, et al. Behavioral and psychological treatments for chronic insomnia disorder in adults: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2021;17:255–62.
Bonnet MH, Arand DL. Hyperarousal and insomnia: State of the science. Sleep Med Rev. 2010;14:9–15.
Perlis ML, Ellis JG, Kloss JD, Riemann DW Etiology and Pathophysiology of Insomnia. In: Principles and Practice of Sleep Medicine. Elsevier; 2017. pp. 769–84.e4.
Altena E, Ellis J, Camart N, Guichard K, Bastien C. Mechanisms of cognitive behavioural therapy for insomnia. J Sleep Res. 2023;32:e13860.
Lancee J, Harvey AG, Morin CM, Ivers H, van der Zweerde T, Blanken TF. Network Intervention Analyses of cognitive therapy and behavior therapy for insomnia: Symptom specific effects and process measures. Behav Res Ther. 2022;153:104100.
Fernandez-Mendoza J Insomnia with objective short sleep duration. In: Encyclopedia of Sleep and Circadian Rhythms. Elsevier; 2023. pp. 64–72.
Vgontzas AN, Fernandez-Mendoza J, Liao D, Bixler EO. Insomnia with objective short sleep duration: The most biologically severe phenotype of the disorder. Sleep Med Rev. 2013.
Li Y, Vgontzas AN, Fernandez-Mendoza J, Fang J, Puzino K, Bixler EO. Effect of trazodone versus cognitive-behavioural treatment on high- and slow-frequency activity during non-rapid eye movement sleep in chronic insomnia: A pilot, randomized clinical trial. J Sleep Res. 2021;30:e13324.
Vgontzas AN, Puzino K, Fernandez-Mendoza J, Krishnamurthy VB, Basta M, Bixler EO. Effects of trazodone versus cognitive behavioral therapy in the insomnia with short sleep duration phenotype: a preliminary study. J Clin Sleep Med. 2020;16:2009–19.
Blanken TF, Benjamins JS, Borsboom D, Vermunt JK, Paquola C, Ramautar J, et al. Insomnia disorder subtypes derived from life history and traits of affect and personality. Lancet Psychiatry. 2019;6:151–63.
Funding
This study was not supported by any sponsor or funder.
Author information
Authors and Affiliations
Contributions
MS: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Supervision; Validation; Visualization; Writing - original draft; and Writing – review & editing. CMM: Conceptualization; Data curation; Investigation; Methodology; Supervision; Validation; Writing - review & editing. TTD: Conceptualization; Data curation; Investigation; Methodology; Supervision; Validation; Writing - review & editing. FBP: Data curation; Investigation; Methodology; Supervision; Validation; Writing - review & editing. AAP: Data curation; Investigation; Methodology; Supervision; Validation; Writing - review & editing. JPG: Data curation; Investigation; Methodology; Supervision; Validation; Writing - review & editing. JB: Data curation; Investigation; Methodology; Supervision; Validation; Writing - review & editing. KJ: Conceptualization; Data curation; Investigation; Methodology; Supervision; Validation; Writing - review & editing. AV: Conceptualization; Data curation; Investigation; Methodology; Supervision; Validation; Writing - review & editing. JFM: Conceptualization; Data curation; Investigation; Methodology; Supervision; Validation; Writing - review & editing. CHB: Conceptualization; Data curation; Investigation; Methodology; Supervision; Validation; Writing - review & editing. DR: Conceptualization; Data curation; Investigation; Methodology; Supervision; Validation; Writing - review & editing. CB: Conceptualization; Data curation; Investigation; Methodology; Supervision; Validation; Writing - review & editing. GC: Data curation; Formal analysis; Methodology; Writing - review & editing. FC: Investigation; Supervision; Validation; Writing - review & editing. MZ: Investigation; Supervision; Validation; Writing - review & editing. VC: Investigation; Methodology; Supervision; Validation; Writing - review & editing. AG: Conceptualization; Data curation; Investigation; Methodology; Project administration; Supervision; Validation; Visualization; Writing - review & editing. LFS: Conceptualization; Data curation; Investigation; Methodology; Project administration; Supervision; Validation; Visualization; Writing - review & editing.
Corresponding author
Ethics declarations
Competing interests
MS: none. CMM: Eisai, Idorsia, Lallemand Health, Mapi Research Trust, Haleon. TTD: Canadian Institutes of Health Research, Natural Sciences and Engineering Research Council of Canada, Weston Family Foundation, Hypersomnia Foundation, Jazz Pharmaceuticals, Paladin Labs, Eisai, Idorsia. FBP: none. AAP: Concordia Horizon Fellowship, Centre de Recherche de l’Institut Universitaire Geriatrique de Montreal (CRIUGM) Postdoctoral Fellowship. JPG: none. JB: none. KJ: none. AV: none. JFM: none. CHB: none. DR: none. CB: Italian Ministry for University and Research, European Sleep Research Society, Idorsia. GC: none. FC: Bruno Farmaceutici, Italfarmaco, Polifarma, Viatris, Vivisol. MZ: none. VC: none. AG: Idorsia. LFS: none.
Ethics
All participants provided written informed consent prior to their inclusion in the study. Ethical approval was obtained from the institutional review boards of all participating centers, in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. The study was conducted within a multicenter research protocol approved by the coordinating center’s Ethics Committee at San Raffaele Hospital, Milan, Italy (approval number 188/INT/2020), which explicitly included all participating satellite centers.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Sforza, M., Morin, C.M., Dang-Vu, T.T. et al. The effectiveness of Cognitive behavioral therapy for insomnia on sleep EEG hyperarousal: a multicentric polysomnographic study. Transl Psychiatry 16, 88 (2026). https://doi.org/10.1038/s41398-026-03882-1
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41398-026-03882-1
