
Abstract
Mild cognitive impairment (MCI) is an early stage in the progression toward dementia. Lipids are central to neurodegeneration, yet the biomarker potential of lipidomics from saliva, plasma, and feces remains underexplored. As part of the Microbiome in Aging Gut and Brain (MiaGB) consortium, saliva, plasma, and fecal samples were collected from older adults with MCI and healthy controls. Samples were analyzed by high-performance liquid chromatography coupled with high-resolution mass spectrometry (LC/MS), to profile lipidomic alterations and identify candidate biomarkers. Lipidomic profiling annotated over 200 molecular species spanning five major lipid classes. Compared with controls, MCI patients exhibited increased oxidized triacylglycerols (oxTGs) in saliva, reduced cholesteryl linoleate (CE 18:2) in plasma, and decreased fatty acid esters of hydroxy fatty acids (FAHFAs) in feces. Receiver operating characteristic (ROC) analysis identified α-linolenic acid (FA 18:3), docosapentaenoic acid (FA 22:5), and CE 18:2 as discriminatory metabolites with notable diagnostic performance. Moreover, elevated fecal triacylglycerols containing medium-chain fatty acids (TG-MCFAs) were observed in MCI, suggesting impaired lipid absorption or altered metabolism. This multi-sample lipidomics strategy highlights TG-MCFAs as fecal biomarkers for MCI detection, supporting further mechanistic and longitudinal validation.
Similar content being viewed by others


Introduction
Alzheimer’s disease (AD) is the most common progressive neurodegenerative disorder and the leading cause of dementia in older populations, characterized by gradual memory loss and cognitive decline, posing a growing global health concern and economic burden [1]. The World Health Organization estimates that over 55 million people suffer from dementia globally. In the absence of effective therapeutic interventions, this number is expected to increase to 152 million by 2050. AD pathology is defined by the cerebral deposition of amyloid-β (Aβ) plaques and phosphorylated tau (p-tau) neurofibrillary tangles [2]. The disease follows a progressive course, beginning with a preclinical asymptomatic phase, advancing to mild cognitive impairment (MCI), and eventually culminating in dementia [3]. MCI affects over 15% of the older adult population and represents a critical window for interventions aimed at mitigating risk factors for cognitive decline and dementia [4, 5]. Early diagnosis of MCI is limited [6], highlighting the need for effective biomarkers, since current AD diagnostics rely on invasive procedures, neuropsychological tests, and neuroimaging that lack disease specificity [7, 8].
Lipidomics offers significant potential for identifying novel lipid biomarkers for early dementia diagnosis [9]. Lipids constitute ~50% of brain dry weight and support neuronal membrane functions, including proliferation, apoptosis, structure, and signaling [10, 11]. Disrupted brain lipid metabolism impairs membrane integrity and synaptic function, promoting Aβ aggregation and tau hyperphosphorylation [12]. Alteration in plasma lipid homeostasis is linked to AD development, positioning lipids as potential biomarkers for its early detection [13, 14]. Recent case-control analysis revealed that lower plasma membrane lipids and triacylglycerol (TG) levels correlate with an increased risk of cognitive decline over 12 years, especially in older adults carrying the APOE-ɛ4 allele [15]. However, current research has failed to clarify the relationship between AD progression and alterations in host lipid homeostasis, particularly during the MCI phase [16]. Liquid chromatography/mass spectrometry (LC/MS) is a widely applied approach in lipidomics, enabling simultaneous characterization of diverse lipid species that may reveal metabolic alterations relevant to AD detection [17]. Prior studies have reported significant alterations in sphingomyelin (SM), cholesterol esters (CE), phosphatidylcholine (PC), lysophosphatidylcholine (LPC), phosphatidylethanolamine (PE), lysophosphatidylethanolamine (LPE), phosphatidylinositol (PI), monoacylglycerol (MG), diacylglycerol (DG), and TG in AD plasma using LC/MS [18, 19]. Furthermore, longitudinal plasma lipidome profiling has demonstrated a notable reduction in ether-phospholipids in individuals converting to dementia compared to control and MCI groups [20]. Additionally, a panel of ten blood phospholipids predicted phenoconversion from normal cognition to amnestic MCI or AD with over 90% accuracy within 2–3 years [21]. Moreover, lipidomic profiling of cerebrospinal fluid (CSF) samples from individuals with MCI and dementia revealed significant reductions in phosphatidylglycerol (PG), monohexosyl ceramide, SM, PI, PC, PE, and CE levels [11].
To date, lipidomic investigations aimed at identifying diagnostic lipid biomarkers in both invasive (plasma) and non-invasive (saliva and fecal) samples from patients with MCI remain limited. In this study, high-performance liquid chromatography coupled with linear trap quadrupole–Orbitrap mass spectrometry (HPLC/LTQ-Orbitrap-MS) was employed to comprehensively characterize lipidomic alterations in saliva, plasma, and feces from healthy controls, individuals with MCI, and dementia patients. Furthermore, sex- and weight-dependent lipid changes were evaluated within the MCI cohort, as illustrated in Fig. 1A.

A Study design for lipidomic analysis of invasive (plasma) and non-invasive (saliva, feces) samples from healthy controls, MCI, and dementia patients. B Donut charts showing lipid class distribution in saliva, plasma, and feces of control and MCI groups. C Violin plots of saturated fatty acids (SFAs), monounsaturated fatty acids (MUFAs), and polyunsaturated fatty acids (PUFAs) in control vs. MCI groups. D Bar graphs of ω-6:ω-3 PUFAs ratios in saliva, plasma, and feces. Statistical significance was determined using Ordinary two-way ANOVA with Sidak’s multiple comparison tests (***p < 0.001, p > 0.05 (ns), ns: not significant). Data are shown as mean ± standard error of the mean (SEM).
Methods
Chemicals
This study employed LC/MS grade solvents- specifically isopropanol, methanol, 1 M aqueous solution of ammonium acetate, and chloroform- sourced from Wako Pure Chemical Industries, Ltd. (Osaka, Japan) and Sigma-Aldrich (St. Louis, MO, USA). Oleic acid-d9 and EquiSPLASH LIPIDOMIX (Lot: 330731-1EA-013) quantitative standard mixtures were obtained from Avanti Polar Lipids (Alabaster, AL, USA).
Sample information
The study utilized saliva, plasma, and fecal samples collected from same participants of healthy controls (saliva: n = 81; plasma: n = 60; feces: n = 87), patients with MCI (saliva: n = 37; plasma: n = 26; feces: n = 37), and patients with dementia (saliva: n = 6; plasma: n = 4; feces: n = 4) from the Microbiome in Aging Gut and Brain (MiaGB) consortium cohort, comprising community-dwelling older adults aged 65 to 85 years old in the United states of America. The samples were collected from the participants visiting the Department of Psychiatry and Behavioral Neurosciences at Byrd Center and the USF Memory Disorders clinic, as well as from the communities in different areas of the Tampa Bay area between August 2022 to December 2023. Exclusion criteria of the participants comprised brain and gut surgery within five years, recent antibiotic use (past 30 days), neurological disorders (Epilepsy, Parkinson’s disease, and Amyotrophic Lateral Sclerosis), inflammatory bowel disease, recent cancer treatment, diarrhea, extreme Body Mass Index (BMI) (>45 or <18 kg/m²), recent significant weight loss, and inability to communicate in English. Participants were grouped by sex, age, and cognitive function was assessed using the Montreal Cognitive Assessment (MoCA) score, as described previously [22,23,24,25]. BMI was used to classify the participants into underweight (UW) (BMI < 18.5 kg/m²), normal weight (NW) (BMI 18.5–24.9 kg/m²), and overweight (OW) (BMI ≥ 25 kg/m²) groups. Ethical approval was obtained from the Institutional Review Board of the University of South Florida (approval no. 002365) and the Ethics Committee of the Department of Health Sciences, Hokkaido University (approval no. 22–87).
Extraction of lipids
Saliva, plasma, and fecal samples from healthy controls, MCI patients, and dementia patients among older adults were subjected to total lipid extraction. The samples were received and stored at −80 °C for subsequent analysis. Saliva, plasma, and fecal samples were extracted using the Folch technique [26], with minor modifications, as pioneered previously in our laboratory [27, 28]. Briefly, saliva samples (150–200 µL) were added to a 2 mL Eppendorf tube, to which ice-cold methanol (100 µL, with 0.01% Butylated hydroxytoluene (BHT)) was added. Then, 100 µL of an internal standard (IS) solution was mixed and vortexed for 1 min at 3500 rpm. The IS solution consists of 10 µg/mL of oleic acid-d9 and EquiSPLASH LIPIDOMIX (1 µg/mL of PI (15:0/18:1(d7)), PC (15:0/18:1(d7)), PE (15:0/18:1(d7)), PG (15:0/18:1(d7)), PS (15:0/18:1(d7)), LPE 18:1(d7), LPC 18:1(d7), SM d18:1/18:0(d9), Cer (d18:1/15:0(d7)), TG (15:0/18:1(d7)/15:0), DG (15:0/18:1(d7)), CE 18:1(d7), and MG 18:1(d7)) mixtures in methanol. Subsequently, chloroform (400 µL) and Milli-Q (100 µL) were added sequentially, followed by vigorous vortexing for 5 min. The mixture was subsequently centrifuged at 15000 rpm for 10 min, to form distinct biphasic layers. The upper layer was re-extracted with chloroform, after which the pooled extracts were combined and dried using a centrifuge evaporator at 4 °C for 3 h. The dried extracts were then redissolved in methanol (100 µL). Prior to transfer to LC vials, the lipid extracts in methanol were vortexed and centrifuged at 15000 rpm for 10 min. Following the above-described protocol, a plasma sample (50 μL) was used for lipid extraction. For fecal samples, each sample (approximately 100 mg) was collected in a 2 mL Eppendorf tube, and then ice-cold methanol (0.5 mL, with 0.01% BHT) was added. The mixture was then homogenized using ceramic beads (1.4 mm, catalog no. 15–340-159, Fisherbrand, Fisher Scientific, Pittsburgh, PA, USA) for 1 min (two repeated 30 s cycles) using a Bead Mill 4 homogenizer (Fisherbrand, Tokyo, Japan); for extraction, a 100 µL aliquot of the homogenate was used according to the protocol described above. The extracted samples were injected into the LC/MS with an injection volume of 10 µL per run.
Untargeted LC/MS analysis
High performance liquid chromatography system (Shimadzu Corp., Kyoto, Japan) attached to a linear trap quadrupole Orbitrap XL mass spectrometer (Thermo Fisher Scientific Inc., San Jose, CA, USA) was used for lipid analysis. An Atlantis T3 C18 column (2.1 mm × 150 mm, 3 μm, Waters, Milford, MA) was used for the separation of lipids with a flow rate of 200 µL/min and an oven temperature kept at 40 °C. The mobile phase consisted of A: aqueous 10 mM CH3COONH4, B: isopropanol, and C: methanol. The elution gradient conditions were set as outlined in our previous study. All the MS parameters were identical to those described in our previous study [29]. The investigation was carried out in negative and positive ionization modes using electrospray ionization with the following parameters: nitrogen sheath gas flow, 50 units; capillary temperature, 330 °C; and nitrogen auxiliary gas flow, 20 units. The capillary and source voltages were set to 10 V and 3 kV in negative ionization mode, with the range set to m/z 160–1900, and to 25 V and 4 kV in positive ionization mode, with the range set to m/z 150–1950. The analysis was conducted in Fourier transform mode with a resolving power of 60,000 to acquire the MS spectra, whereas MS/MS spectra were obtained in ion-trap mode using a collision energy of 40 V.
Lipid annotation and quantification
Lipid molecular species were identified using MS-DIAL software (version 4.9) for data alignment, peak extraction, and annotation. Accurate mass spectral analysis and data integration were performed using Xcalibur software (version 2.2; Thermo Fisher Scientific, Waltham, USA) to ensure reliable lipid identification. Lipids concentration was determined semi-quantitatively based on the amount of internal standard added during extraction. The relative concentrations were normalized by the amount of the sample used for analysis.
Statistical analysis
Data visualization was performed using Microsoft Excel 2021, and results were plotted with GraphPad Prism (version 8.0.1). To evaluate data variation, orthogonal partial least squares discriminant analysis (OPLS-DA) was conducted in MetaboAnalyst 6.0 (https://www.metaboanalyst.ca, accessed December 4, 2024). As a supervised method, OPLS-DA enhances classification accuracy while reducing the risk of overfitting [30]. Score plots were generated to assess intergroup similarities, and variable importance in projection (VIP) plots were used to identify discriminatory lipid features. Statistical analyses included two-way ANOVA with Sidak’s multiple comparison test, as well as unpaired t-tests and with Welch’s correction for pairwise comparisons. A significance threshold of p < 0.05 was applied. Data are reported as mean ± standard error of the mean (SEM).
Results
Lipid class distribution and fatty acyl composition in saliva, plasma, and fecal samples from older adults
The study included saliva, plasma, and fecal specimens collected from the same individuals of healthy controls and patients diagnosed with MCI and dementia. Due to the limited number of dementia samples, these were excluded from comparative analyses. Both control and MCI participants are often characterized by an age of approximately 65 to 85 years old. Across sample types, both control and MCI groups were predominated by females (control: 60/43/64, MCI: 22/15/23) compared to males (control: 21/17/23, MCI: 15/11/14). OW participants comprised the majority in both groups (control: 50/33/53, MCI: 20/11/20) compared to NW participants (control: 29/26/32, MCI: 17/15/17), while UW participants were excluded from the study. MCI participants had significantly lower MOCA scores compared to controls in all three clinical samples, reflecting impaired cognitive performance. Full demographic and clinical characteristics are provided in Supporting Information Table S1.
Untargeted lipidomic profiling of saliva, plasma, and fecal samples identified 266, 217, and 260 lipid molecular species, respectively, spanning five major lipid classes: fatty acyls (FAs), glycerophospholipids (GPs), glycerolipids (GLs), sphingolipids (SPs), and sterols (STs). Comprehensive lists of lipid species and their relative abundances are provided in Supplementary Information Tables S2–S4. Donut charts (Fig. 1B) illustrate the percentage distribution of lipid classes in saliva, plasma, and fecal samples from control and MCI groups. In saliva, FAs were the predominant lipid class in both groups, followed by GLs, GPs, SPs, and STs (Fig. 1Bi). In plasma, GPs were the most abundant lipid class, followed by GLs, FAs, SPs, and STs (Fig. 1Bii). In fecal samples, FAs were the dominant class in both groups (Fig. 1Biii). Lipid class distributions in dementia samples are presented in Supplementary Figure S1.
Figure 1C depicts violin plots of saturated fatty acids (SFAs), monounsaturated fatty acids (MUFAs), and polyunsaturated fatty acids (PUFAs) in saliva, plasma, and feces. No statistically significant differences were observed between MCI and controls. Nonetheless, slightly higher SFAs, MUFAs, and PUFAs levels were noted in saliva and plasma of the MCI group (Fig. 1Ci and Cii), whereas levels were modestly lower in fecal samples (Fig. 1Ciii). PUFAs were further subclassified into ω-3 and ω-6 fatty acids, and the corresponding ω-6:ω-3 ratios are shown in Fig. 1D. A significant decrease in the ω-6:ω-3 ratio (approximately 12:1) was detected in saliva from MCI patients compared to controls. By contrast, no significant differences in ω-6:ω-3 ratios were observed in plasma or fecal samples.
Multivariate and volcanic plot analysis of the saliva, plasma, and fecal lipidomes
Multivariate analysis was performed to identify group-specific lipidomic differences between control and MCI cohorts in saliva, plasma, and fecal samples. The OPLS-DA models and their corresponding score and VIP plots are shown in Figure 2Ai–iii. In saliva, the score plot demonstrated modest group separation between control and MCI groups, explaining 45.6% of total model variance (Fig. 2Ai). The associated VIP plot identified the lipid species contributing to this variation. Similarly, plasma analysis revealed minor group separation, with the model accounting for 32.4% of the variance (Fig. 2Aii), while fecal analysis demonstrated weaker separation between groups, explaining 13.1% of the variance (Fig. 2Aiii). In each case, the VIP plots highlight lipid species driving the observed group differences.

A Orthogonal partial least squares discriminant analysis (OPLS-DA) and variable importance in projection (VIP) plots of lipid profiles in control and MCI groups for (i) saliva, (ii) plasma, and (iii) feces. B Volcano plots showing altered lipids (Parametric t-test, p < 0.1) in the same groups of (i) saliva, (ii) plasma, and (iii) feces. Sample sizes: saliva (81 controls, 37 MCI), plasma (60 controls, 26 MCI), feces (87 controls, 37 MCI).
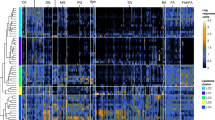
Volcano plot analysis (Fig. 2Bi–iii) was employed to evaluate lipid alterations between control and MCI groups, where red indicates increased and blue indicates decreased lipid species in MCI, based on −log10(p-value) plotted against log2(fold change). In saliva, multiple TG molecular species, particularly those containing oleic acid (FA 18:1), linoleic acid (FA 18:2), oxidized TGs (oxTGs), and PUFAs, including FA 20:5, FA 22:5, and FA 20:4, were increased in MCI compared with controls (Fig. 2Bi). In plasma, several fatty acids (FA 12:0, FA 20:4, FA 20:5, FA 22:5) and lysophospholipids (LPC 14:0, LPC 22:5, LPE 22:5) were increased in MCI, whereas cholesteryl linoleate (CE 18:2) was decreased (Fig. 2Bii). In feces, the majority of TG and DG molecular species, particularly those containing medium-chain fatty acids (MCFAs), were increased in MCI, while several fatty acid esters of hydroxy fatty acids (FAHFAs) were reduced relative to controls (Fig. 2Biii). Additional multivariate and volcano plot comparisons of control vs. dementia and MCI vs. dementia samples are presented in Supplementary Figures S2 and S3. Supplementary Figures S4 and S5 provide bar plots of selected altered lipids between control and MCI groups, as well as heatmaps showing the top 50 altered lipid species across control, MCI, and dementia cohorts in saliva, plasma, and fecal samples.
Identification of lipid biomarkers for early-stage MCI diagnosis in older adults
Given the pronounced elevation of TG-MCFAs and DG-MCFAs in fecal samples from MCI patients, we compared their levels across saliva, plasma, and feces from control and MCI groups to evaluate their potential as early diagnostic biomarkers (Fig. 3A). In saliva, TG-MCFAs showed a non-significant reduction in the MCI group relative to controls (Fig. 3Ai). In plasma, TG-MCFAs exhibited a non-significant increase in MCI (Fig. 3Aii), while DG-MCFAs were exclusively detected in fecal samples. Notably, fecal samples demonstrated elevated levels of both TG-MCFAs and DG-MCFAs, in MCI compared to controls (Fig. 3Aiii), suggesting that fecal TG-MCFAs and DG-MCFAs may serve as promising non-invasive biomarkers for the detection of MCI.

A Bar graphs of TG-MCFA and DG-MCFA levels in (i) saliva, (ii) plasma, and (iii) feces from controls and MCI patients. B Classical univariate receiver operating characteristic (ROC) curves analysis of top discriminatory lipids in (i) saliva, (ii) plasma, and (iii) feces. Statistical significance was determined using unpaired Student’s t-test (**p < 0.01, *p < 0.05, p > 0.05 (ns)). Data are shown as mean ± SEM.
To further evaluate diagnostic performance, receiver operating characteristic (ROC) curve analysis was performed for key altered lipids in saliva, plasma, and feces (Fig. 3B). A ranked list of the top 30 discriminatory lipids, along with their specificity and corresponding area under the curve (AUC) values, is provided in Supplementary Information Tables S5–S7. In saliva, FA 18:3 (AUC = 0.6947) showed the highest discriminatory power, while FA 22:5 (AUC = 0.5526) and CE 18:2 (AUC = 0.5475) demonstrated moderate accuracy (Fig. 3Bi). In plasma, CE 18:2 (AUC = 0.6865) exhibited the strongest diagnostic potential, followed by FA 22:5 (AUC = 0.6090), whereas FA 18:3 (AUC = 0.5840) had moderate predictive value (Fig. 3Bii). In feces, CE 18:2 (AUC = 0.6095) showed notable discriminatory capacity, while FA 18:3 (AUC = 0.5166) and FA 22:5 (AUC = 0.5026) displayed moderate diagnostic efficacy (Fig. 3Biii). Together, these findings indicate that specific lipid metabolites, including FA 18:3, FA 22:5, CE 18:2, and fecal TG-MCFAs, may represent candidate biomarkers for the early diagnosis of MCI in older adults.
Sex-specific alterations in lipid metabolites of saliva, plasma, and feces in MCI patients
Sex-dependent differences in lipidomic alterations between the control and MCI groups are presented in Fig. 4. The OPLS-DA score plots for saliva (Fig. 4Ai and Aii) revealed subtle separation between control and MCI groups in both male and female participants, with corresponding VIP plots identifying discriminative lipid species (Supplementary Figure S6A). In plasma, male participants exhibited marked group separation (28.6% of variance explained; Fig. 4Aiii), with discriminatory lipids highlighted in Supplementary Figure S6B, whereas female participants showed only minimal separation (Fig. 4Aiv), suggesting fewer lipid perturbations. For fecal samples, minor group separation was observed in both sexes (Fig. 4Av and vi), with contributing lipids shown in Supplementary Figure S6C.

A OPLS-DA score plots of sex-specific lipidomic profiles in control and MCI groups for (i–ii) saliva, (iii–iv) plasma, and (v–vi) feces from male and female participants. B Volcano plots of sex-specific altered lipids (Parametric t-test, p < 0.1) in the same groups of (i–ii) saliva, (iii–iv) plasma, and (v–vi) feces. Sample sizes: saliva (males: 21 controls, 15 MCI; females: 60 controls, 22 MCI), plasma (males: 17 controls, 11 MCI; females: 43 controls, 15 MCI), feces (males: 23 controls, 14 MCI; females: 64 controls, 23 MCI).
Volcano plot analyses further delineated sex-specific lipid alterations (Fig. 4B). In saliva, no significant lipid changes were observed in males (Fig. 4Bi), whereas female MCI samples exhibited increased levels of FA 18:3 and TG molecular species containing FA 18:1 and FA 18:2 (Fig. 4Bii). Plasma samples of male participants with MCI displayed increased levels of PI (20:4/17:1;O1), LPC 14:0, and several additional lipid species, alongside reduced HexCer (d18:1/23:1;O) (Fig. 4Biii). In contrast, female MCI plasma samples exhibited increases in LPC 22:5, LPE 22:5, FA 12:0, HexCer (d18:0/21:0;O), LPC 22:6, and PS (18:0/18:1), with concurrent decreases in CE 18:1 and CE 18:2 levels relative to controls (Fig. 4Biv). In fecal samples, male MCI participants showed an increase in FA 22:5;(2OH), FA 24:0;(2OH), and FA 25:0;(2OH), accompanied by reductions in TG (16:0/16:0/18:1), FAHFA (18:1/24:5;O), and PG (O-18:2/16:0) levels (Fig. 4Bv). Conversely, female MCI participants demonstrated increased levels of FA 10:0, PE (15:0/17:0), TG-MCFAs, and DG-MCFAs, alongside decreased FAHFAs (Fig. 4Bvi). Bar plots of selected sex-specific lipid alterations and a heatmap of the top 50 differentially abundant lipids across sex-stratified control and MCI groups are provided in Supplementary Figures S7 and S8.
BMI-specific alterations in lipid metabolites of saliva, plasma, and feces in MCI patients
BMI-stratified lipidomic alterations between control and MCI participants are shown in Fig. 5. Due to a limited sample size, UW participants were excluded from the analysis. In saliva, OPLS-DA score plots revealed minor group separation between control and MCI groups for both NW and OW participants (Fig. 5Ai and Aii), with discriminatory lipids highlighted in Supplementary Figure S9A. Plasma analysis also showed modest separation across NW and OW groups (Fig. 5Aiii and Aiv; Supplementary Figure S9B), while fecal analyses demonstrated similar minor group separations in both NW and OW participants (Fig. 5Av and Avi; Supplementary Figure S9C).

A OPLS-DA score plots of weight-specific lipidomic profiles in control and MCI groups for (i–ii) saliva, (iii–iv) plasma, and (v–vi) feces, stratified by normal weight (NW) and overweight (OW). B Volcano plots of weight-specific altered lipids (Parametric t-test, p < 0.1) in the same groups of (i–ii) saliva, (iii–iv) plasma, and (v–vi) feces. Sample sizes: saliva (NW: 29 controls, 17 MCI; OW: 50 controls, 20 MCI), plasma (NW: 26 controls, 13 MCI; OW: 50 controls, 11 MCI), feces (NW: 32 controls, 17 MCI; OW: 53 controls, 20 MCI).
Volcano plot analysis further revealed BMI-specific lipid alterations (Fig. 5B). In saliva, NW participants with MCI exhibited increased FA 18:3, FA 20:4, FA 22:5, and reduced TG (O-17:1/18:1/20:1) levels (Fig. 5Bi), whereas OW participants showed an increase in TGs containing FA 18:1 and FA 18:2 levels (Fig. 5Bii). In plasma, NW MCI participants displayed increased LPC 14:0, LPE 22:5, and other species, but decreased CE 18:2 and CE 22:6 levels compared to controls. OW participants exhibited elevated LPC 22:6, LPC 18:3, and LPC 16:1, alongside reduced HexCer (d18:1/23:1;O) levels (Fig. 5Biii and Biv). In fecal samples, NW participants with MCI showed increased DGs, particularly DG-MCFAs, accompanied by reduced FAHFA levels (Fig. 5Bv). In contrast, OW participants exhibited increased levels of LPE 18:0, PE (15:0/17:0), HexCer (t18:0/24:0(2OH)), and DG (10:0/12:0), while FAHFA (18:1/24:4;O) and FAHFA (18:1/24:5;O) were decreased (Fig. 5Bvi). Bar plots of selected altered lipids and heatmaps of the top 50 discriminant lipids across BMI groups are presented in Supplementary Figures S10 and S11.
Discussion
This study presents the first comprehensive untargeted lipidomic profiling of plasma, saliva, and fecal samples to investigate lipid alterations associated with AD progression and to identify potential lipid biomarkers capable of distinguishing MCI from normal aging. Previous lipidomic investigations have primarily relied on invasive sample types such as plasma or CSF [31,32,33] and dementia individuals [15, 34], limiting their ability to capture dynamic lipid alteration and discover promising lipid biomarkers for MCI. By employing a multi-biofluid approach, this study overcomes the constraints posed by previous studies and provides novel insights into lipid dysregulation in MCI, enhancing non-invasive lipid biomarker discovery for diagnosing MCI.
Consistent with earlier studies reporting GPs as the predominant plasma lipids with decreased levels in MCI, our findings confirmed similar reductions in GPs within plasma samples (Fig. 1B) [18]. Fatty acids play essential roles in neurogenesis and neurotransmitter synthesis, processes critical for brain development and maintenance [35]. We observed a non-significant elevation of SFAs in saliva and plasma of MCI patients compared to controls (Fig. 1C), in agreement with earlier meta-analyses documenting similar trends in serum/plasma SFAs [36]. Elevated SFAs, often reflecting high dietary intake, have been recognized as a major risk factor for MCI [37]. Moreover, prior studies link an increased ω-6:ω-3 ratio with cognitive decline [38]. Intriguingly, our saliva data demonstrated a reduced ω-6:ω-3 ratio in MCI (Fig. 1D), suggesting potential PUFAs imbalances that may reflect early inflammatory processes during disease progression [39]. Several studies suggest that targeting ω-6 and ω-3 lipid pathways may mitigate cognitive decline by modulating lipid metabolism and inflammatory responses. Long-term ω-3 fatty acid supplementation improves cognitive performance in various AD animal models [40, 41], were α-linolenic acid in the diet promotes the nonamyloidogenic pathway in Aβ25–35 injected mice [42]. Clinical evidence further supports the protective role of ω-3 supplements, showing a 64% reduced AD risk in longitudinal cohorts and a 20% reduction in meta-analyses of over 100,000 individuals [43]. Prior trials report cognitive benefits in individuals receiving ω-3 fatty acids [44, 45], via modulating Aβ deposition and suppression of pro-inflammatory mediators through inhibition of lipoxygenases, cyclooxygenases, nuclear factor‑κB, and cytochrome P450 to improve neuronal survival [46, 47]. However, dysregulation of ω-3 and ω-6 in the AD brain correlates with PUFA metabolism imbalance driven by disease pathological factors [48]. These underscore that balanced ω-6:ω-3 ratios associate with slower cognitive decline and lower dementia risk [49]. Collectively, mechanistic and clinical studies support targeting PUFAs lipid pathways to attenuate AD-related neurodegeneration. Multivariate analyses (Fig. 2A) revealed only modest compositional differences between control and MCI groups, likely reflecting confounding influences of diet, lifestyle, and aging [50, 51].
GPs regulate neuronal membrane integrity, ion transport, and cell proliferation [52]. Dysregulation of LPC and LPE metabolism has been closely linked to neuroinflammation in AD [53]. Increased LPC levels have been previously reported in AD plasma and mouse brain tissue [54, 55], consistent with our observation of elevated specific LPC species in MCI plasma (Fig. 2B). Early activation of phospholipase A2 by Aβ accumulation and oxidative stress may underlie these increases [56]. GLs also play key roles in neuronal energy homeostasis and structural stability of axons and myelin [57]. Previous cohort studies reported elevated TG levels in the plasma and serum of cognitively impaired and AD patients [58, 59], and increased TGs and oxTGs in CSF and plasma of AD cases [60, 61], findings aligned with our saliva and fecal lipidomic data in MCI (Fig. 2B). Such TG elevations may represent early microglial responses to Aβ deposition through diacylglycerol O-acyltransferase-2 (DGAT2) upregulation [62]. Notably, TG-MCFAs can be metabolized into ketone bodies, an alternative energy source for neurons and astrocytes [63, 64], while dietary TG-MCFAs supplementation has demonstrated cognitive benefits in AD patients [65]. Our study observed increased fecal TG-MCFAs in MCI (Fig. 3A), suggesting malabsorption or excessive excretion, thus indicating their potential as non-invasive diagnostic biomarkers. Interestingly, elevated TG-MCFAs were particularly pronounced in female participants (Fig. 4B), consistent with reports of greater vulnerability to AD-related pathology in women [66].
Pathway-based lipid subclass distribution analysis, performed using the Kyoto Encyclopedia of Genes and Genomes (KEGG) lipid biosynthesis pathway, further illustrated altered lipid metabolism (Fig. 6) [67]. Most lipid classes showed no significant changes; however, FAHFAs a recently discovered novel class of endogenous anti-inflammatory and antidiabetic lipids [68] were significantly reduced in MCI feces. This is consistent with prior observations of FAHFAs depletion in AD brain tissue [69]. Additionally, decreased plasma CEs in MCI align with previous findings. The possible reflecting impaired activity of cholesterol-esterifying enzymes, lecithin–cholesterol acyltransferase (LCAT) and acyl-CoA:cholesterol acyltransferase 1 (ACAT1) may underlie these decreases [70]. In support of this observation, a previous study identified a combination of 24 molecules, including CE/TG, that helps to classify the AD patients with >70% accuracy, indicating a promising AD biomarker in predicting the disease progression and brain atrophy [34]. Overall, this study provides novel insights into saliva, plasma, and fecal lipidome profiles in MCI older adults, identifying 266, 217, and 260 lipid molecular species, respectively. While multivariate analyses revealed only modest separations between groups, ROC analysis identified FA 18:3, FA 22:5, and CE 18:2 as promising candidate biomarkers for MCI. Moreover, elevated fecal TG-MCFAs may represent a non-invasive biomarker for MCI detection. Nevertheless, this study has several limitations. First, this cross-sectional study design limits the ability to determine cause-and-effect relationships and observe changes over time of temporal associations with the progression of MCI. Second, the relatively small sample size of MCI participants reduces the statistical power, particularly in stratified analyses, thereby constraining the robustness and generalizability of the specific findings. Third, the study lacks replication and validation test analysis, highlighting the need for future investigations to confirm the study findings and establish their clinical utility. Given the exploratory nature of this work, which aims to generate preliminary hypotheses and identify potent biomarkers for MCI, the results should be considered as a basis for future research. Additionally, the present study did not include longitudinal data on conversion from MCI to dementia, which precludes assessment of the association between observed lipidomic alterations with disease progression and brain atrophy of AD. Furthermore, the study relied on semi-quantitative lipidomic data. The lack of control for potentially major confounding factors such as diet, physical activity, medication use, and genetic background may also influence the observed associations. Finally, the mechanistic links between lipid dysregulation and MCI pathology remain incompletely understood.

Data are shown as mean ± SEM (y-axis: lipid subclass concentration in ng/µL for fluids and ng/mg for feces; x-axis: control vs. MCI). Significance was assessed using unpaired t-tests with Welch’s correction (***p < 0.001, *p < 0.05, p > 0.05 (ns)).
In summary, our study provides the first comprehensive comparative lipidomic analysis of saliva, plasma, and fecal samples from control, MCI, and dementia participants. The findings highlight distinct lipid alterations associated with MCI, identifying FA 18:3, FA 22:5, CE 18:2, and fecal TG-MCFAs as promising biomarker candidates. Further mechanistic and longitudinal studies are required to validate these biomarkers and elucidate their roles in AD pathogenesis.
Data availability
All data relevant to the study are contained within the article and supplementary information.
References
DeTure MA, Dickson DW. The neuropathological diagnosis of Alzheimer’s disease. Mol Neurodegener. 2019;14:32.
Bloom GS. Amyloid-β and tau: the trigger and bullet in Alzheimer disease pathogenesis. JAMA Neurol. 2014;71:505–8.
Porsteinsson AP, Isaacson RS, Knox S, Sabbagh MN, Rubino I. Diagnosis of early alzheimer’s disease: clinical practice in 2021. J Prev Alzheimers Dis. 2021;8:371–86.
Petersen RC, Roberts RO, Knopman DS, Boeve BF, Geda YE, Ivnik RJ, et al. Mild cognitive impairment: ten years later. Arch Neurol. 2009;66:1447–55.
Bai W, Chen P, Cai H, Zhang Q, Su Z, Cheung T, et al. Worldwide prevalence of mild cognitive impairment among community dwellers aged 50 years and older: a meta-analysis and systematic review of epidemiology studies. Age Ageing. 2022;51:afac173. https://doi.org/10.1093/ageing/afac173.
Thambisetty M, Lovestone S. Blood-based biomarkers of Alzheimer’s disease: challenging but feasible. Biomark Med. 2010;4:65–79.
Brookmeyer R, Abdalla N. Estimation of lifetime risks of Alzheimer’s disease dementia using biomarkers for preclinical disease. Alzheimers Dement. 2018;14:981–8.
Hane FT, Robinson M, Lee BY, Bai O, Leonenko Z, Albert MS. Recent progress in alzheimer’s disease research, part 3: diagnosis and treatment. J Alzheimers Dis. 2017;57:645–65.
Zhang X, Liu W, Zan J, Wu C, Tan W. Untargeted lipidomics reveals progression of early Alzheimer’s disease in APP/PS1 transgenic mice. Sci Rep. 2020;10:14509.
O’Brien JS, Sampson EL. Lipid composition of the normal human brain: gray matter, white matter, and myelin. J Lipid Res. 1965;6:537–44.
Byeon SK, Madugundu AK, Jain AP, Bhat FA, Jung JH, Renuse S, et al. Cerebrospinal fluid lipidomics for biomarkers of Alzheimer’s disease. Mol Omics. 2021;17:454–63.
Kao Y-C, Ho P-C, Tu Y-K, Jou I-M, Tsai K-J Lipids and Alzheimer’s disease. Int J Mol Sci 2020; 21. https://doi.org/10.3390/ijms21041505.
Huynh K, Lim WLF, Giles C, Jayawardana KS, Salim A, Mellett NA, et al. Concordant peripheral lipidome signatures in two large clinical studies of Alzheimer’s disease. Nat Commun. 2020;11:5698.
Walter A, Korth U, Hilgert M, Hartmann J, Weichel O, Hilgert M, et al. Glycerophosphocholine is elevated in cerebrospinal fluid of Alzheimer patients. Neurobiol Aging. 2004;25:1299–303.
Lefèvre-Arbogast S, Hejblum BP, Helmer C, Klose C, Manach C, Low DY, et al. Early signature in the blood lipidome associated with subsequent cognitive decline in the elderly: A case-control analysis nested within the Three-City cohort study. EBioMedicine. 2021;64:103216.
Wood PL. Lipidomics of Alzheimer’s disease: current status. Alzheimers Res Ther. 2012;4:5.
Ferré-González L, Lloret A, Cháfer-Pericás C. Systematic review of brain and blood lipidomics in Alzheimer’s disease mouse models. Prog Lipid Res. 2023;90:101223.
Peña-Bautista C, Álvarez-Sánchez L, Roca M, García-Vallés L, Baquero M, Cháfer-Pericás C Plasma lipidomics approach in early and specific alzheimer’s disease diagnosis. J Clin Med 2022; 11. https://doi.org/10.3390/jcm11175030.
Liu Y, Thalamuthu A, Mather KA, Crawford J, Ulanova M, Wong MWK, et al. Plasma lipidome is dysregulated in Alzheimer’s disease and is associated with disease risk genes. Transl Psychiatry. 2021;11:344.
Wang T, Arnold M, Huynh K, Weinisch P, Giles C, Mellett NA, et al. Trajectory of plasma lipidome associated with the risk of late-onset Alzheimer’s disease: a longitudinal cohort study. EBioMedicine. 2025;118:105826.
Mapstone M, Cheema AK, Fiandaca MS, Zhong X, Mhyre TR, MacArthur LH, et al. Plasma phospholipids identify antecedent memory impairment in older adults. Nat Med. 2014;20:415–8.
James AS, Adil NA, Goltz D, Tangudu D, Chaudhari DS, Shukla R, et al. Abnormalities in gut virome signatures linked with cognitive impairment in older adults. Gut Microbes. 2024;16:2431648.
Walters KF, Shukla R, Kumar V, Schueren S, Yadav H, Schilaty ND et al. Resting-State EEG power spectral density analysis between healthy and cognitively impaired subjects. Brain Sci 2025; 15. https://doi.org/10.3390/brainsci15020173.
Jayaprakash J, Gowda D, M Gangadhara R, Jain S, Yadav H, et al. Discovering novel short- and medium-chain esters of hydroxy fatty acids in human fecal samples using untargeted liquid chromatography/mass spectrometry. Rapid Commun Mass Spectrom. 2025;39:e10032.
Chaudhari DS, Jain S, Yata VK, Mishra SP, Kumar A, Fraser A, et al. Unique trans-kingdom microbiome structural and functional signatures predict cognitive decline in older adults. Geroscience. 2023;45:2819–34.
Folch J, Lees M, Sloane Stanley GH. A simple method for the isolation and purification of total lipides from animal tissues. J Biol Chem. 1957;226:497–509.
Minami Y, B Gowda SG, Gowda D, Chiba H, Hui S-P. Regio-specific lipid fingerprinting of edible sea cucumbers using LC/MS. Food Res Int. 2024;184:114253.
Jayaprakash J, B Gowda SG, K Shukla P, Gowda D, et al. Sex-Specific effect of ethanol on colon content lipidome in a mice model using nontargeted LC/MS. ACS Omega. 2024;9:16044–54.
Nath LR, B Gowda SG, Roberts TH, Gowda D, Khoddami A, Hui SP. Nontargeted lipidomics of sorghum grain reveals novel fatty acid esters of hydroxy fatty acids and cultivar differences in lipid profiles. J Agric Food Chem. 2024;72:20690–703.
Zhao L, Duan X, Liu H. Novel grade classification tool with lipidomics for indica rice eating quality evaluation. Foods. 2023;12:944 https://doi.org/10.3390/foods12050944.
Sakr F, Dyrba M, Bräuer A, Teipel S. Alzheimer’s disease neuroimaging initiative. association of lipidomics signatures in blood with clinical progression in preclinical and prodromal alzheimer’s disease. J Alzheimers Dis. 2022;85:1115–27.
Barupal DK, Baillie R, Fan S, Saykin AJ, Meikle PJ, Arnold M, et al. Sets of coregulated serum lipids are associated with Alzheimer’s disease pathophysiology. Alzheimers Dement. 2019;11:619–27.
Wang X, Bui H, Vemuri P, Graff-Radford J, Jack CR, Petersen RC, et al. Lipidomic network of mild cognitive impairment from the mayo clinic study of aging. J Alzheimers Dis. 2021;81:533–43.
Proitsi P, Kim M, Whiley L, Simmons A, Sattlecker M, Velayudhan L, et al. Association of blood lipids with alzheimer’s disease: a comprehensive lipidomics analysis. Alzheimers Dement. 2017;13:140–51.
Youdim KA, Martin A, Joseph JA. Essential fatty acids and the brain: possible health implications. Int J Dev Neurosci. 2000;18:383–99.
Hosseini M, Poljak A, Braidy N, Crawford J, Sachdev P. Blood fatty acids in Alzheimer’s disease and mild cognitive impairment: A meta-analysis and systematic review. Ageing Res Rev. 2020;60:101043.
Nien S-W, Lin I-H, Wu H-C, Chen Y-H, Yang S-C Evaluation of dietary intake in individuals with mild cognitive impairment. Nutrients 2023; 15. https://doi.org/10.3390/nu15173694.
Baierle M, Vencato P, Oldenburg L, Bordignon S, Zibetti M, Trentini C, et al. Fatty acid status and its relationship to cognitive decline and homocysteine levels in the elderly. Nutrients. 2014;6:3624–40.
Dakterzada F, Jové M, Cantero JL, Mota-Martorell N, Pamplona R, Piñoll-Ripoll G. The shift in the fatty acid composition of the circulating lipidome in Alzheimer’s disease. Alzheimers Dement. 2024;20:3322–33.
Cole GM, Frautschy SA. Docosahexaenoic acid protects from amyloid and dendritic pathology in an Alzheimer’s disease mouse model. Nutr Health. 2006;18:249–59.
Park YH, Shin SJ, Kim HS, Hong SB, Kim S, Nam Y et al. Omega-3 fatty acid-type docosahexaenoic acid protects against aβ-mediated mitochondrial deficits and pathomechanisms in alzheimer’s disease-related animal model. Int J Mol Sci 2020; 21. https://doi.org/10.3390/ijms21113879.
Lee AY, Lee MH, Lee S, Cho EJ. Alpha-Linolenic Acid from Perilla frutescens var. japonica Oil Protects Aβ-Induced Cognitive Impairment through Regulation of APP Processing and Aβ Degradation. J Agric Food Chem. 2017;65:10719–29.
Wei B-Z, Li L, Dong C-W, Tan C-C. Alzheimer’s disease neuroimaging initiative, xu w. the relationship of omega-3 fatty acids with dementia and cognitive decline: evidence from prospective cohort studies of supplementation, dietary intake, and blood markers. Am J Clin Nutr. 2023;117:1096–109.
Lázaro I, Brugulat-Serrat A, Suárez-Calvet M, Fauria K, Minguillon C, Gispert J-D, et al. Red blood cell ω-3 status and longitudinal cognition in individuals at risk of Alzheimer disease. J Nutr. 2025;155:4514–22. https://doi.org/10.1016/j.tjnut.2025.09.032.
Naaman RK, Alashmali S, Bakhsh MA, Muqaibil AA, Ghunaim FM, Alattas AH. Association of omega-3 polyunsaturated fatty acids intake and cognitive function in middle-aged and older adults. Nutr Neurosci. 2025;28:649–58.
Grimm MOW, Kuchenbecker J, Grösgen S, Burg VK, Hundsdörfer B, Rothhaar TL, et al. Docosahexaenoic acid reduces amyloid beta production via multiple pleiotropic mechanisms. J Biol Chem. 2011;286:14028–39.
Barros MI, Brandão T, Irving SC, Alves P, Gomes F, Correia M. Omega-3 polyunsaturated fatty acids and cognitive decline in adults with non-dementia or mild cognitive impairment: an overview of systematic reviews. Nutrients. 2025;17:3002 https://doi.org/10.3390/nu17183002.
Snowden SG, Ebshiana AA, Hye A, An Y, Pletnikova O, O’Brien R, et al. Association between fatty acid metabolism in the brain and Alzheimer disease neuropathology and cognitive performance: a nontargeted metabolomic study. PLoS Med. 2017;14:e1002266.
de Oliveira Otto MC, Wu JHY, Thacker EL, Lai HTM, Lemaitre RN, Padhye N, et al. Circulating omega-3 and omega-6 fatty acids, cognitive decline, and dementia in older adults. J Alzheimers Dis. 2023;95:965–79.
Hwangbo N, Zhang X, Raftery D, Gu H, Hu S-C, Montine TJ, et al. Predictive modeling of alzheimer’s and parkinson’s disease using metabolomic and lipidomic profiles from cerebrospinal fluid. Metabolites. 2022;12:277.
Macias S, Yilmaz A, Kirma J, Moore SE, Woodside JV, Graham SF, et al. Non-targeted LC–MS/MS metabolomic profiling of human plasma uncovers a novel Mediterranean diet biomarker panel. Metabolomics. 2023;20:3.
Nitsch R, Pittas A, Blusztajn JK, Slack BE, Growdon JH, Wurtman RJ. Alterations of phospholipid metabolites in postmortem brain from patients with Alzheimer’s disease. Ann N Y Acad Sci. 1991;640:110–3.
Xu S, Zhu Z, Delafield DG, Rigby MJ, Lu G, Braun M, et al. Spatially and temporally probing distinctive glycerophospholipid alterations in Alzheimer’s disease mouse brain via high-resolution ion mobility-enabled sn-position resolved lipidomics. Nat Commun. 2024;15:6252.
Peña-Bautista C, Roca M, López-Cuevas R, Baquero M, Vento M, Cháfer-Pericás C. Metabolomics study to identify plasma biomarkers in alzheimer disease: ApoE genotype effect. J Pharm Biomed Anal. 2020;180:113088.
Ahsanul Haque M, Omori N, Md Sheikh A, Yano S, Osago H, Mitaki S, et al. Analysis of the time-dependent changes of phospholipids in the brain regions of a mouse model of Alzheimer’s disease. Brain Res. 2023;1800:148197.
Chalbot S, Zetterberg H, Blennow K, Fladby T, Grundke-Iqbal I, Iqbal K. Cerebrospinal fluid secretory Ca2+-dependent phospholipase A2 activity is increased in Alzheimer disease. Clin Chem. 2009;55:2171–9.
Yin F. Lipid metabolism and Alzheimer’s disease: clinical evidence, mechanistic link and therapeutic promise. FEBS J. 2023;290:1420–53.
Iqbal G, Braidy N, Ahmed T. Blood-Based biomarkers for predictive diagnosis of cognitive impairment in a pakistani population. Front Aging Neurosci. 2020;12:223.
Castillo-Mendieta T, Arana-Lechuga Y, Campos-Peña V, Sosa AL, Orozco-Suarez S, Pinto-Almazán R, et al. Plasma levels of amyloid-β peptides and tau protein in mexican patients with alzheimer’s disease. J Alzheimers Dis. 2021;82:S271–S281.
Dakterzada F, Benítez ID, Targa A, Carnes A, Pujol M, Jové M, et al. Cerebrospinal fluid lipidomic fingerprint of obstructive sleep apnoea in Alzheimer’s disease. Alzheimers Res Ther. 2023;15:134.
Dakterzada F, Benítez ID, Targa A, Carnes A, Pujol M, Jové M, et al. Blood-based lipidomic signature of severe obstructive sleep apnoea in Alzheimer’s disease. Alzheimers Res Ther. 2022;14:163.
Prakash P, Manchanda P, Paouri E, Bisht K, Sharma K, Rajpoot J, et al. Amyloid-β induces lipid droplet-mediated microglial dysfunction via the enzyme DGAT2 in Alzheimer’s disease. Immunity. 2025;58:1536–1552.e8.
Dunn E, Zhang B, Sahota VK, Augustin H. Potential benefits of medium chain fatty acids in aging and neurodegenerative disease. Front Aging Neurosci. 2023;15:1230467 https://doi.org/10.3389/fnagi.2023.1230467.
Espina A, Mendoza E, Lao A Modelling the effects of medium-chain triglycerides on cerebral ketone body metabolism. Front Syst Biol 2022; 2. https://doi.org/10.3389/fsysb.2022.907957.
Juby AG, Blackburn TE, Mager DR Use of medium chain triglyceride (MCT) oil in subjects with Alzheimer’s disease: a randomized, double-blind, placebo-controlled, crossover study, with an open-label extension. Alzheimers Dement: TRCI. 2022;8. https://doi.org/10.1002/trc2.12259.
Podcasy JL, Epperson CN. Considering sex and gender in Alzheimer disease and other dementias. Dialogues Clin Neurosci. 2016;18:437–46.
Jayaprakash J, Gowda SGB, Gowda D, Ikeda A, Bamai YA, Ketema RM, et al. Plasma lipidomics of preadolescent children: a hokkaido study. J Lipids. 2025;2025:3106145.
Wood PL Fatty acyl esters of hydroxy fatty acid (FAHFA) lipid families. Metabolites 2020; 10. https://doi.org/10.3390/metabo10120512.
Obis E, Sol J, Andres-Benito P, Martín-Gari M, Mota-Martorell N, Galo-Licona JD, et al. Lipidomic alterations in the cerebral cortex and white matter in sporadic alzheimer’s disease. Aging Dis. 2023;14:1887–916.
Proitsi P, Kim M, Whiley L, Pritchard M, Leung R, Soininen H, et al. Plasma lipidomics analysis finds long chain cholesteryl esters to be associated with alzheimer’s disease. Transl Psychiatry. 2015;5:e494.
Acknowledgements
We would like to acknowledge the resources provided by the University of South Florida (USF) Center for Microbiome Research, the Microbiomes Institute, the Center for Excellence in Aging and Brain Repair, the Department of Neurosurgery and Brain Repair, and the USF Morsani College of Medicine.
Funding
This work was supported by the JST SPRING (Grant Number JPMJSP2119) and the Japan Society for the Promotion of Science KAKENHI Grants (25K00258 and 23K06861). Additional support was provided by the Ed and Ethel Moore Alzheimer’s Disease Research Program of the Florida Department of Health (Grant Number 22A17), as well as the U.S. National Institutes of Health, the National Institute on Aging (Grant Numbers RF1AG071762, R21AG072379, U01AG076928, and R21AG085881).
Author information
Authors and Affiliations
Consortia
Contributions
Jayashankar Jayaprakash: methodology, data curation, visualization, writing – original draft. Siddabasave Gowda B. Gowda: conceptualization, methodology, funding acquisition, resources, visualization, supervision, writing –review and editing. Divyavani Gowda: data curation, visualization, writing – original draft. Shalini Jain: resources, writing – review and editing. Hariom Yadav: samples, resources, funding acquisition, writing – review and editing. Shu-Ping Hui: resources, writing –review and editing.
Corresponding authors
Ethics declarations
Competing interests
Dr. Hariom Yadav is the cofounder and chief scientific officer of Postbiotics Inc., and BiomAge Inc. He is also cofounder of MusB LLC., MusB Research LLC., and MeraBiome Inc., with Dr. Shalini Jain. However, they have no conflict of interest with respect to the work/literature reviewed and presented in this manuscript. Other authors have no conflicts of interest to declare.
Ethics approval
Ethical approval was obtained from the Institutional Review Board of the University of South Florida (approval no. 002365), USA and the Ethics Committee of the Department of Health Sciences, Hokkaido University (approval no. 22–87), Japan. All methods were performed in accordance with the relevant guidelines and regulations.
Informed consent
All participants involved in this study provided written informed consent.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Jayaprakash, J., B. Gowda, S.G., Gowda, D. et al. Lipidomic signatures reveal biomarkers of mild cognitive impairment. Transl Psychiatry 16, 115 (2026). https://doi.org/10.1038/s41398-026-03893-y
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41398-026-03893-y
