
Abstract
Identifying reliable biomarkers of treatment response is central to advancing personalized psychiatry. While whole-brain functional connectivity models have shown promise in predicting clinical outcomes, especially for broad-spectrum interventions like cognitive-behavioral therapy, targeted treatments may benefit from more specific neuromarkers. In social anxiety disorder (SAD), Gaze-Contingent Music Reward Therapy (GC-MRT) is a novel attention bias modification (ABM) intervention designed to reduce preferential attentional allocation to socially threatening stimuli. Given the dorsal attention network’s (DAN) key role in top-down attentional control, we tested whether resting-state intra-network DAN connectivity could serve as a neural predictor of response to GC-MRT. Participants with SAD were randomized to either receive GC-MRT (n = 22) or to a waitlist control condition (n = 24). Resting-state fMRI data were collected before and after the intervention. Intra-DAN connectivity at baseline and post-treatment were associated with post-treatment symptom severity in the GC-MRT group. Post-treatment intra-DAN connectivity significantly differed in the GC-MRT group relative to controls. These findings suggest that intra-network connectivity within the DAN may have the potential to function both as a predictive biomarker and as a neural marker of successful intervention. Our findings highlight the role of the DAN in attention-based clinical interventions and show that network-specific connectivity metrics may offer a more precise understanding of how targeted neuromodulation affects symptom change in SAD.
Similar content being viewed by others

Introduction
Identifying reliable biomarkers of treatment response advances personalized psychiatry [1, 2]. Connectome-based predictors show promise in forecasting clinical outcome across psychiatric disorders [3,4,5]. In social anxiety disorder (SAD) [6] prior work has largely relied on whole-brain connectivity models [7, 8], an approach well-suited to predicting outcomes of cognitive-behavioral therapy (CBT), which utilizes many therapeutic tactics. By contrast, response to treatments that target a specific neurocognitive process, such as attention bias modification (ABM), may be better captured by network-specific biomarkers indexing function within targeted systems. Here, we extend prior work on neuromarkers of treatment response to an emerging ABM intervention for SAD - Gaze-Contingent Music Reward Therapy (GC-MRT) [9, 10]. Previous findings indicate that resting-state connectivity between the executive control network, and the salience and default mode networks, predicted symptom improvement following GC-MRT [11]. Prior analyses in the current sample further demonstrated GC-MRT-related effects on task-evoked brain activation in the inferior frontal gyrus and anterior cingulate cortex [12]. Building on these works and given that GC-MRT behaviorally targets threat-related top-down attentional control, we tested whether resting-state intra-network connectivity within the dorsal attention network (DAN), the core system supporting top-down attentional control, predicts clinical response in SAD.
ABM treatments are designed to remediate threat-related attentional biases in anxiety disorders [13, 14]. Their rationale derives from evidence linking anxiety to preferential attention allocation to threatening over neutral information [15,16,17], and with poor attention control [18,19,20,21]. GC-MRT is an emerging ABM treatment for SAD, tested in randomized controlled trials suggesting efficacy [9, 10]. GC-MRT employs real-time eye-tracking feedback and operant conditioning to rebalance maladaptive attentional patterns during the viewing of threat-related and neutral faces embedded in simulated social crowds [9, 16, 17, 22,23,24,25]. By reinforcing gaze allocation away from threat cues and toward neutral stimuli [16, 17], GC-MRT aims to remediate threat-related attentional biases. This process is hypothesized to specifically engage the DAN, which supports top-down goal-directed control of visual attention through regions such as the superior parietal lobule (SPL) and frontal eye fields (FEF) [26, 27]. Altered DAN function, together with heightened stimulus-driven attentional capture, has been consistently implicated in anxiety [18, 28]. Importantly, extant first-line treatments for SAD, such as CBT and Selective Serotonin Reuptake Inhibitors (SSRIs), do not directly target threat-related attentional processes. In contrast, GC-MRT is specifically designed to modify the characteristic tendency of individuals with SAD toward increased attentional allocation to socially threatening faces relative to neutral faces [23, 29, 30]. Given the DAN’s central role in attentional control, its intra-network connectivity is a plausible neural substrate supporting GC-MRT’s therapeutic effects.
Connectome-based predictive modeling (CPM) has been effectively applied to link neural measures and clinical outcomes in anxiety disorders. Previous research has shown that pre-treatment resting-state connectivity predicts CBT response in SAD [7], as well as longitudinal depression and anxiety severity [31]. The functional connectome at rest has also been shown to predict degrees of trait anxiety [32]. Here, we adapted CPM to specifically explore DAN involvement in GC-MRT outcome, given its functional specialization and particular relevance to the attentional mechanism underpinning its therapeutics.
The following analyses were conducted: 1) network-based predictive modeling to test the association between intra-DAN connectivity at baseline and post-treatment symptom severity; 2) network-based predictive modeling to test the association between intra-DAN connectivity and symptom severity at post-treatment; 3) comparison of post-treatment intra-DAN connectivity between GC-MRT patients and untreated waitlist participants, controlling for baseline connectivity; and 4) specificity of the findings was tested in relation to other neural networks and relative to SSRI treatment.
Materials and methods
This study reports secondary analyses of previously unanalyzed data from a subsample of patients who participated in a randomized controlled trial [10, 12, 33]. The parent trial included a third arm treated with SSRIs alone. These patients were excluded from the main analyses, which focus specifically on identifying neuromarkers of GC-MRT efficacy (relevant specificity results pertaining to SSRI treatment are presented in Supplementary Materials).
Participants
Forty-six treatment-seeking participants with SAD (mean age=28.48, SD = 6.28, range=21–48, 15 females), who provided clinical and resting-state functional neuroimaging data before and after treatment/waitlist were included in analyses (for full details of the RCT and associated findings for symptoms see Arad et al. [10] and Azriel et al. [12, 33]). Participants received either GC-MRT (n = 22, mean age=29.14, SD = 7.54, range=22–48, 9 females) or were allocated to a waitlist (WL) control group (n = 24, mean age=27.88, SD = 4.95, range=21–40, 6 females). Waitlist control participants did not receive treatment between the two MRI scans and were offered GC-MRT after their participation in the study ended. For participants’ demographic and clinical characteristics by group, see Table 1. All participants provided written informed consent prior to study participation. The study was approved by the Tel Aviv University, Tel Aviv Sourasky Medical Center, and Sheba Medical Center Institutional Review Boards. Clinicaltrials.gov Identifier: NCT03346239.
SAD assessment
Diagnosis and inclusion/exclusion criteria
A diagnosis of SAD was established using the Liebowitz Social Anxiety Scale (LSAS) [34] interview and further validated using the Mini-International Neuropsychiatric Interview (MINI [35]). Comorbid diagnoses were determined using MINI. Inclusion criteria were social anxiety disorder as the main source of distress and impairment, age 18–65 years, LSAS score≥50, and a Clinical Global Impressions severity score≥4.438 [22] Exclusion criteria were posttraumatic stress disorder, psychotic or bipolar disorders, epilepsy or brain injury, suicidal ideation or risk, drug abuse, and concurrent pharmacological or psychological treatment. Clinical interviews were conducted at the Tel Aviv University Anxiety Clinic by two clinical psychologists trained to 85% reliability with a senior clinician.
SAD severity assessment
SAD symptom severity was measured using the Social Phobia Inventory (SPIN) [36]. The SPIN is a 17-item self-reported questionnaire designed to assess social anxiety symptoms, aligning with the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5 [6]) criteria for SAD. Participants rated the extent to which each SPIN item had bothered them in the past week on a 5-point Likert scale ranging from 0 (“Not at all”) to 4 (“Extremely”). The sum of responses to all SPIN items served as the clinical indicator of SAD severity. Although the LSAS is a well-validated and widely used measure of SAD severity, summed scores of the SPIN questionnaire were used here as the primary clinical outcome as SPIN items map more directly onto diagnostic criteria for SAD according to the DSM-5. Cronbach’s alphas in the current subsample were 0.93 and 0.91 at baseline and post-treatment, respectively.
Conditions
For detailed descriptions of the GC-MRT and waitlist control conditions, see Arad et al. [10].
GC-MRT: This 12-week GC-MRT protocol included 11 sessions. The first session (week 1; ~45 min) focused on building rapport, providing psychoeducation about SAD and ABM, and explaining the study procedures. The remaining 10 sessions (~ 20 min each) consisted of GC-MRT training designed to reduce dwell time on threatening (disgusted) faces [9]. Training was administered twice weekly during weeks 2–5, and once weekly in weeks 8 and 11. In each session, patients selected a 12 min preferred music track and viewed 30 face matrices (24 s each) while gaze was continuously tracked. Music played when patients fixated on neutral faces and paused when they fixated on threat faces (Fig. 1). This operant conditioning paradigm is designed to promote attentional preference for neutral over threatening faces, addressing the characteristic tendency of individuals with SAD to dwell longer on threat faces relative to non-anxious individuals.

Participants viewed 30 distinct face matrices consisting of neutral and threatening faces (right). When participants fixated on a neutral face, a self-selected music track was played. The music stopped when fixating a threat face.
Waitlist Control: Patients underwent two MRI scans 12 weeks apart and did not receive treatment in between. Clinical evaluations and self-reported symptom measures were collected. Participants were told that they would receive GC-MRT following the waiting period.
Measurement of threat-related attention patterns
GC-MRT effects on percent dwell time on threat faces were assessed using a validated free viewing measurement task [23] at baseline, mid-treatment and post GC-MRT. The free viewing task consisted of 30 face matrices, comprising faces of different actors than the ones used for GC-MRT, presented without music feedback. Attentional dwell time (DT%) on threat was computed per matrix as dwell time on threat faces divided by total dwell time on faces (neutral + threat) and averaged across the 30 matrices. [10, 33].
MRI acquisition and preprocessing
The full protocol consisted of structural, task functional MRI (fMRI), and resting-state fMRI scans (for the complete scanning protocol and preprocessing pipeline, see Azriel et al. [12]). The current analyses relate to the resting-state functional data. Briefly, participants underwent two identical MRI scans spaced 12 weeks apart: One at baseline and one following GC-MRT or an equivalent waiting period for the control group. Neuroimaging data was acquired on a Siemens Magnetom Prisma 3 T scanner (Siemens, Erlangen, Germany), using a 64 channel phased array head coil. High resolution anatomical localizer image (MPRAGE) was scanned with the following parameters: TR = 1750 ms, TE = 2.61 ms, TI = 900 ms, flip angle=8°, isotropic resolution of 1mm3. Functional MRI data was obtained by multiband echo-planar imaging (EPI) images with the following parameters: TR=2000ms; TE = 30 ms; flip angle=82°; IPAT = 2, multiband factor=2, isotropic resolution of 2mm3 and 66 axial slices 2 mm thick (no gap) to ensure full brain coverage. Field-maps were acquired using two opposite coded (AP, PA) echo-planar scans: TR = 8152 ms; TE = 66 ms; flip angle=90°; multiband factor=1; isotropic resolution of 2mm3 and 66 axial slices 2 mm thick (no gap). All images were acquired in the anterior commissure - posterior commissure (AC–PC) line extending down from the top of the brain.
Functional images preprocessing pipeline incorporated a set of tools provided by FMRIB Software Library (FSL), version 6.0.0 [37]. Several preprocessing steps were implemented to minimize noise and motion bias in the fMRI data, including rigid-body motion correction using MCFLIRT [38] and temporal high-pass filtering with a 100 s cutoff to remove low-frequency drifts. Data underwent alignment to middle volume as an initial template image, spatial smoothing (5 mm isotropic Gaussian kernel) and non-linear registration to the 152T1 Montreal Neurological Institute (MNI) common space. Image normalization to the MNI template was carried out as follows: low-resolution EPI images were registered to higher-resolution EPI reference images (expanded functional images), then to a high resolution T1 images (using a linear, normal search registration) [38, 39] and then to the 152T1 MNI template (using a non-linear registration) [40]. To further minimize motion and artifact-related noises, we employed Independent Component Analysis (ICA)-based denoising using FSL’s MELODIC and FIX [41]. Specifically, ICA components from ten representative participants were manually classified as “signal” or “noise” to generate a study-specific training set. This classifier was then applied to all participants’ data via FIX (version 1.066), which automatically removed components associated with motion, physiological artifacts (e.g., cardiac and respiratory noise), and scanner-related fluctuations. The resting-state fMRI scan was 10 min long, resulting in 300 data volumes.
Statistical analysis
All the analyses reported in this work were conducted using MATLAB (version R2024a).
Impact of treatment on symptom severity
The impact of GC-MRT on symptom severity in the parent sample is reported in Arad et al [10]. To test whether the original findings maintained in the current sub-sample, analysis of variance (ANOVA) was performed with group (GC-MRT, waitlist) as a between-subjects factor and time (baseline, post-treatment) as a within-subject factor (see Supplemental Methods for details).
Impact of GC-MRT on attentional dwell time on threat faces
Changes in DT% over time were evaluated using FDR-corrected one-tailed Wilcoxon signed-rank tests. In addition, to gauge change in DT% over time during GC-MRT, changes in DT% between the first and last treatment sessions were evaluated using a one-tailed Wilcoxon signed-rank test. For additional details, see Supplemental Methods.
Intra-network functional connectivity matrices
For each participant, seven intra-network connectivity matrices were calculated corresponding to the seven networks defined by Yeo et al. [42]. Within each network, Pearson correlations were calculated among nodes for the resting-state activation time series of all constituent parcels, based on the 100-region parcellation by Schaefer et al. [43] The current work focused on the 105 within-DAN functional connections derived from the 15 Schaefer parcels that compose the DAN.
For a list of the parcels comprising the DAN, including parcel numbers, hemisphere and location, see Supplemental Methods Table S1. For the full MNI centroid coordinates, see Schaefer et al. [43]. Separate matrices were derived for baseline and for post-treatment. All correlation scores were converted to \(Z\)-values using a Fisher transformation.
Association between post-treatment SAD symptom severity and intra-DAN functional connectivity
The relation between post-treatment SAD symptom severity (SPIN) following GC-MRT and intra-DAN connectivity was examined using connectome-based predictive modeling (CPM) [44, 45], employing the code provided in the original CPM paper [44]. Post-treatment symptom severity was predicted from: (1) baseline intra-DAN connectivity, and (2) post-treatment intra-DAN connectivity.
Prior to CPM, normality of the symptom severity data distribution was assessed with a one-sample Kolmogorov–Smirnov test.
To verify that post-treatment SPIN scores were not correlated with head motion [44], an average frame displacement measure was extracted for each participant using the FSL Motion Outliers tool [38, 39] accessible at https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/FSLMotionOutliers. A Pearson correlation score was calculated between each participant’s post-treatment SPIN score and average frame displacement measure.
In line with previous work employing CPM with small dataset, we adopted a leave-one-out cross-validation (LOO-CV) approach [5, 32, 44, 46]. In each iteration, a model was developed using data from N–1 participants. The left-out participant, unseen during training, served as an independent test case. Within each iteration’s training set, functional connectivity features were normalized within participants and correlated with their post-treatment SPIN score as part of the feature selection procedure. Edges with significant Pearson correlation coefficients (α < 0.05) were retained as model features. Feature selection was performed within each CV-LOO iteration, thereby preventing any data leakage and ensuring that the model was evaluated on data from a participant it had not encountered during training. Within each iteration, significant positive and negative edges were summed separately for each training-set of participants and then used to train the predictive model before applying it on the test participant in the LOO paradigm. Prediction accuracy was evaluated as the Pearson correlation between actual and predicted symptom severity scores. Significance was confirmed using a permutation test with 10000 iterations. To further characterize the intra-DAN neural connections that contributed most to the prediction, we identified consensus edges that served as predictors in all LOO-CV iterations. We then calculated the Pearson correlation coefficient between each of the consensus edges at baseline and SPIN score post-treatment.
To test the robustness of the reported neural-clinical association to analytical variability, predictions of post-treatment symptom severity from intra-DAN connectivity at baseline and post-treatment were also performed using a linear ridge regression. A CV-LOO approach was employed here as well, and feature selection and model evaluation were conducted as in the CPM procedure. Hyperparameters were tuned via nested cross-validation: within each outer LOO fold, the edge-selection threshold and ridge penalty (\({\rm{\lambda }}\)) were chosen by inner CV (grid search minimizing mean squared error) using only training data, with no information leakage.
To rule out potential effects of baseline SPIN scores, sex and age on the observed results, CPM analysis was also conducted with baseline SPIN scores, sex and age as covariates (see Supplemental Methods).
Post-Treatment differences in intra-DAN connectivity between GC-MRT and Waitlist control
To examine treatment-induced group differences in intra-DAN connectivity, an analysis of covariance (ANCOVA) was conducted with post-treatment intra-DAN connectivity as the dependent variable and group (GC-MRT, waitlist control), as a between-groups factor. Baseline intra-DAN connectivity was entered as a covariate. Edges with greater than medium effect size (Cohen’s \(f\) ≥ 0.25) are reported. To localize regions contributing most to group differences, weighted node degree was computed for each DAN parcel, as the sum of its edges exhibiting medium or larger effect sizes. This analysis was also repeated with baseline SPIN scores, sex and age as additional covariates (see Supplemental Methods). In addition, a two-sample \(t\)-test was performed to compare the two groups on post-treatment intra-DAN connections, averaged across participants.
Results
SAD symptom severity (SPIN)
The results of the current analysis concur with the results reported in Arad et al. [10], indicating greater reduction in SAD symptoms in the GC-MRT group relative to the waitlist control group (see Supplemental Figure S1).
Attentional dwell time on threat faces
Consistent with prior reports from this dataset, the present subsample showed a significant decline in DT% in the GC-MRT group from baseline to mid-treatment (\(W\)=43, \(z\)=−2.69, \(p\)=0.0035, \(n\)=22), and from baseline to post-treatment (\(W\)=18, \(z\)=0.0035, \(p\)=0.0001, \(n\)=23). The decrease in DT% between mid- and post-treatment was non-significant (\(W\)=78, \(z\)=−1.56, \(p\)=0.0596, \(n\)=22). The decline in DT% was not significant within the SSRI and waitlist control groups (see Supplementary Table S2 and Figure S2A). In addition, DT% significantly declined between the first and last GC-MRT sessions (\(W\)=14, \(z\)=−3.51, \(p\)=0.0002, \(n\)=21) in the GC-MRT group (see Supplemental fig. S2B).
Association between post-treatment SAD symptom severity and intra-DAN functional connectivity
A Kolmogorov–Smirnov test confirmed that the clinical data did not significantly deviate from normality (\(p\)>0.05). Participants’ average framewise displacement did not correlate with post-treatment SPIN scores (\({r}_{{Pearson}{\prime} s}\) = −0.23, \(p\)=0.29).
Baseline intra-DAN connectivity and post-treatment SAD symptom severity
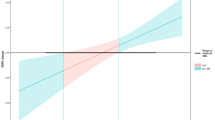
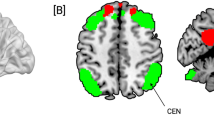
Baseline intra-DAN connectivity predicted post GC-MRT SAD symptom severity (\(r\)Pearson’s = 0.50, \(p\)=0.0074, MAE = 25.68, RMSE = 30.51, \(n\)=23, Fig. 2A). Prediction accuracy was confirmed by a permutation test with 10000 iterations (\(p\) = 0.036, Fig. 2B). The same analysis, with baseline SPIN scores, sex and age serving as additional predictors, resulted in a similar predictive accuracy score (\({r}_{{Pearson}\mbox{'}s}\) = 0.481, \(p\)=0.01, \(n\)=23, Figure S4A). The linear ridge regression prediction yielded similar but marginally significant results (\({r}_{{\rm{Pearson}}{\prime} {\rm{s}}}\) = 0.29, \(p\)=0.089, MAE = 10.27, RMSE = 13.34, \(n\)=23, Fig. 2C). Out of a total of 105 edges within the DAN, one positive consensus edge and one negative consensus edge emerged as predictors in all LOO-CV iterations (Fig. 2D). The positive consensus edge was between parcels 22 and 72 in the left and right premotor cortex, respectively, including the homotopic FEF. The negative consensus edge was between parcel 20 in the superior part of the left precuneus, and parcel 70 in the right SPL. The Pearson correlation coefficient was \(r\)Pearson’s = 0.54 (\(p\)=0.004, Fig. 2E) between the positive consensus edge at baseline and participants’ SPIN scores post-treatment, and \(r\)Pearson’s = −0.59 (\(p\)=0.0014, Fig. 2E) between the negative consensus edge at baseline and participants’ SPIN scores post-treatment. Analyses of the other functional networks by Yeo et al. [42] within the GC-MRT group, as well as of the DAN within the SSRI group, did not yield significant predictions (see Supplemental Results, Figure S3, Table S3), underscoring the specificity of intra-DAN-clinical outcome association to GC-MRT.

A A scatter plot showing prediction accuracy. Each point represents a single participant’s real and predicted test scores. Pearson’s \(r\) between actual and predicted scores is reported at the top-left corner. B A histogram of Pearson correlation coefficients (\(r\)) between actual and predicted SPIN scores across all iterations of the permutation test. The red vertical line indicates the observed \(r\) value obtained from the true CPM model. C A scatter plot showing prediction accuracy using linear ridge regression. D A brain map showing nodes of positive (blue) and negative (red) consensus edges identified across all CPM LOO-CV iterations. E Correlation between the positive (left) and negative (right) consensus edges at baseline with post-treatment SPIN scores. Each point represents a single participant’s edge connectivity and SPIN score. † \(p\) < 0.1, * \(p\) < 0.05, ** \(p\) < 0.01.
Post-treatment within-DAN connectivity and post-treatment SAD symptom severity
Post-treatment intra-DAN connectivity predicted post-treatment SPIN scores (\(r\)Pearson’s = 0.51, \(p\)=0.0075, MAE = 23.28, RMSE = 25.58, \(n\)=22, Fig. 3A). A permutation test with 10000 iterations confirmed the significance of the prediction (\({\rm{p}}\)=0.041, Fig. 3B). The same analysis, with baseline SPIN scores, sex, and age serving as additional predictors, resulted in a similar predictive accuracy score (\({r}_{{Pearson}\mbox{'}s}\) = 0.483, \(p\)=0.01, \(n\)=22, Figure S4B). Linear ridge regression prediction also yielded similar results (\({r}_{{\rm{Pearson}}{\prime} {\rm{s}}}\) = 0.54, \(p\)=0.005, MAE = 8.37, RMSE = 10.32, \(n\)=22, Fig. 3C). A positive consensus edge was detected between homotopic parcels 17 and 68 in the left and right anterior intraparietal sulcus, respectively (Fig. 3D). Negative edges were found between parcel 23 in the left FEF [43] and two other parcels: parcel 18 in the left SPL and parcel 20 in the left precuneus (Fig. 3D). The Pearson correlation coefficient with participants’ post-treatment SPIN scores was \(r\)Pearson’s = 0.58 (\(p\)=0.0024) for the positive consensus edge, \(r\)Pearson’s = −0.55 (\(p\) = 0.004) for the negative consensus edge between parcels 23 and 18, and \(r\)Pearson’s = −0.53** (\(p\)= 0.0057) for the negative consensus edge between parcels 23 and 20. Analyses of the other functional networks by Yeo et al. [42] within the GC-MRT group, as well as of the DAN within the SSRI group, yielded non-significant results (see Supplemental Results, Figure S3, Table S3), further qualifying the specificity of the intra-DAN–clinical outcome association to GC-MRT.

A A scatter plot showing prediction of the SPIN scores following GC-MRT, based on intra-DAN connectivity at post-treatment. Each point represents a single participant’s real and predicted test scores. Pearson’s \(r\) between actual and predicted scores is reported at the top-left corner. B A histogram of Pearson correlation coefficients (\(r\)) between actual and predicted SPIN scores across all iterations of the permutation test. The red vertical line indicates the observed \(r\) value obtained from the true CPM model. C A scatter plot showing prediction accuracy using linear ridge regression. D A brain map showing nodes of positive (blue) and negative (red) consensus edges identified across all CPM LOO-CV iterations of each prediction. ** \(p\) < 0.01.
Post-Treatment differences in intra-DAN connectivity between the GC-MRT and waitlist control groups
Thirty-seven out of 105 intra-DAN connections showed medium or larger effect sizes (Cohen’s \(f\)≥0.25), reflecting group differences in intra-DAN connectivity post-treatment/waitlist while controlling for baseline connectivity (Fig. 4A). For the full list of DAN edges with effect sizes of Cohen’s \(f\)≥0.25 see Table S4 in Supplemental Results. Parcel 20 in the left precuneus exhibited the highest weighted node degree, suggesting its central role in post-treatment DAN reorganization (Fig. 4B). The same analysis, with baseline SPIN scores, sex, and age serving as additional covariates, yielded similar results (see Supplemental Results, Figure S5). A paired t-test between within-DAN connections post-treatment, averaged across participants, revealed weaker connectivity in the GC-MRT group compared to the waitlist control group (\(t\)=−6.42, \(p\)=9.14e-10, \(n\)GC-MRT = 22, \(n\)WL = 24, Fig. 4C).

A Circular graph depicting intra-network connections showing a medium-or-greater effect size in group differences post-treatment, as identified by ANCOVA controlling for baseline intra-DAN connectivity. B Weighted node degree of DAN parcels based on the number of connections meeting the medium effect size threshold. Parcels are ordered by weighted node degree from highest (left) to lowest (right). C Boxplot illustrating post-treatment intra-DAN connectivity in the GC-MRT group (left) and the WL control group (right) for the subset of connections showing group differences. *** \(p\) < 0.001.
Discussion
The current study generated four key findings: 1) Baseline intra-DAN connectivity is predictively associated with post-treatment symptom severity in patients receiving GC-MRT; 2) Intra-DAN connectivity following GC-MRT is associated with post-treatment symptom severity; 3) Significant group differences in intra-DAN connectivity were noted between GC-MRT and waitlist control participants at post-treatment, with the most pronounced difference observed in the left precuneus; and 4) The observed associations were specific to GC-MRT, appearing in neither the waitlist control nor the SSRI treatment groups, and were confined to intra-DAN connectivity, with no comparable effects in any other Yeo network.
This study provides converging behavioral and neurobiological evidence that clinically meaningful improvements in SAD symptoms generated by GC-MRT relate to altered intra-DAN functional connectivity. The finding that baseline intra-DAN connectivity is associated with treatment outcome suggests that the intrinsic organization of the attentional control circuitry may carry potential as a prognostic biomarker for GC-MRT responsiveness. This is consistent with prior work demonstrating that higher baseline functional integration within attentional networks may predict greater benefit from targeted interventions in anxiety and mood disorders [18, 28].
The DAN is critically involved in sustaining goal-directed attention, orienting toward task-relevant stimuli, and suppressing distractors [26]. The current results extend this functional role to the domain of social anxiety treatment, suggesting that effective symptom reduction may depend on the capacity of the DAN to support reallocation of attentional resources away from threat cues and toward a more adaptive attentional allocation to socially relevant stimuli. The identified consensus edges, linking FEF nodes and parietal hubs such as the precuneus and superior parietal lobule, align with known frontoparietal pathways supporting spatial attention [26, 27, 47, 48]. Their association with symptom change underscores the possibility that GC-MRT may operate by recalibrating these circuits.
Post-treatment intra-DAN connectivity was also associated with post-treatment symptom severity, with effects driven by edges involving the SPL, intraparietal sulcus, FEF, and precuneus. These regions are implicated in visuomotor integration, spatial updating, and internally guided shifts of attention [49,50,51,52,53], functions that may be particularly relevant for reorienting gaze and cognitive focus during socially demanding situations. The fact that multiple consensus edges involved homotopic bilateral regions further suggests that GC-MRT may enhance interhemispheric coordination within attentional control systems.
The observed post-treatment reductions in intra-DAN connectivity, relative to the waitlist control participants, may reflect a shift toward a more efficient, less over-coupled attentional network configuration. Hyperconnectivity within control-related networks has been reported in anxiety disorders [28], potentially reflecting compensatory over-engagement. GC-MRT-associated decoupling may index a release from maladaptive hyper-synchronization, permitting more flexible, context-appropriate allocation of attentional resources. The centrality of the left precuneus in post-treatment reorganization is noteworthy, given its role in internally directed cognition and integration of visuospatial information [49,50,51]. Reduced overconnectivity involving this hub could facilitate a shift in social threat processing that facilitates symptom reduction. The left precuneus also presents a potential target for inhibitory neuromodulation that could be applied before or in parallel to GC-MRT and potentially enhance its clinical effect.
The current findings indicate specificity of the association between intra-DAN connectivity and clinical response to GC-MRT in SAD. Complementary analyses did not yield similar indication for other large-scale networks, and intra-DAN connectivity did not relate to clinical outcome following SSRI treatment. These results underscore the potential of targeting mechanism-specific neural-cognitive systems implicated in particular psychiatric conditions. Here, the clinical efficacy of a behavioral eye-tracking-based intervention is predicted by intra-network connectivity within the very attention-control system hypothesized to be directly engaged by the treatment. Such associations have important implications for personalized intervention approaches that draw on connectome-based indices [3,4,5, 7, 8], and for treatment development strategies informed by neuromarkers alongside traditional behavioral markers.
Previous work by Zhu et al. [11] has provided valuable insights into the neural mechanisms underlying GC-MRT-related neural mechanisms. Zhu et al focused on early connectivity shifts (within the first 2–3 weeks of treatment) and on specific ROIs and identified broader inter- and intra-network associations with treatment outcome, including the executive control, default, and salience networks, predicting symptom change following eight GC-MRT sessions. The current approach focused on within-network functional specialization, examining functional connectivity at baseline and after 12 intervention sessions, predicting post-treatment symptom severity. Differences in findings between the two studies likely reflect differences in measurement timing and analytic scope.
Unlike the common pattern in predictive modeling, where predicted values typically cluster around the mean of the actual scores, the CPM predictions in this study exhibited a wider range of values than the observed scores. LOO-CV may extrapolate when the held-out participant lies in a sparsely represented region of feature space. In relatively small, high-dimensional data, noise can amplify this effect and broaden the range of the predicted values. Importantly, this unconventionality was not observed when applying a linear ridge regression, in which predicted scores were within the range of the actual scores.
Several limitations should be acknowledged. First, the study possessed a modest overall sample size, which can reduce the stability of predictive estimates (including CPM). This also limited the possibility of employing an independent sample for tests of generalizability. Both these factors limit the generalizability of the findings. Independent replications in larger samples are warranted. Second, although the focus on the DAN was hypothesis-driven and statistically validated, the functional specificity of the identified consensus edges remains to be replicated in new independent samples. Third, leave-one-out cross-validation may yield higher variance performance estimates, an inherent constraint in clinical neuroimaging where small samples are common. Despite this limitation, the current analyses demonstrate a consistent neural–clinical association and corroborate model performance with permutation testing and an alternate approach (linear ridge regression), mitigating to an extent overfitting concerns and landing support to the robustness of the reported effects. Fourth, testing the specificity of the current intra-DAN predictive model to SAD versus other psychiatric disorders was beyond the scope of this study. Future work applying this model to GC-MRT outcomes in additional disorders may help clarify whether it captures SAD-specific mechanisms or more general effects of the intervention. Finally, the current study only collected baseline and post-treatment neuroimaging data. The longer-term impact of GC-MRT on SAD symptoms and its relation to intra-DAN connectivity could be determined in future studies that include follow-up data collection.
In conclusion, this study identifies the dorsal attention network as a specific neural substrate potentially underlying prognosis in GC-MRT for SAD. The results suggest that baseline within network connectivity and plasticity of attention control circuits, particularly frontoparietal pathways integrating premotor, parietal, and motion-sensitive regions, may be key determinants of therapeutic success. Beyond their theoretical implications for models of attentional dysregulation in SAD, these findings highlight intra-DAN connectivity as a promising biomarker for stratifying patients and personalizing interventions aimed at optimizing attentional allocation in socially salient contexts.
Code availability
Custom MATLAB code used in this work will be provided upon request.
Data availability
Local law and consent limitations prohibit publicly sharing of patients’ data. Deidentified data will be provided for review purposes upon request.
References
Kapur S, Phillips AG, Insel TR. Why has it taken so long for biological psychiatry to develop clinical tests and what to do about it?. Mol Psychiatry. 2012;17:1174–9.
García-Gutiérrez MS, Navarrete F, Sala F, Gasparyan A, Austrich-Olivares A, Manzanares J. Biomarkers in psychiatry: concept, definition, types and relevance to the clinical reality. Front Psychiatry. 2020;11:527209.
Reggente N, Moody TD, Morfini F, Sheen C, Rissman J, O’Neill J, et al. Multivariate resting-state functional connectivity predicts response to cognitive behavioral therapy in obsessive–compulsive disorder. Proc Natl Acad Sci USA. 2018;115:2222–7.
Korgaonkar MS, Chakouch C, Breukelaar IA, Erlinger M, Felmingham KL, Forbes D, et al. Intrinsic connectomes underlying response to trauma-focused psychotherapy in post-traumatic stress disorder. Transl Psychiatry. 2020;10:270.
Zugman A, Ringlein GV, Finn ES, Lewis KM, Berman E, Silverman WK, et al. Brain functional connectivity and anatomical features as predictors of cognitive behavioral therapy outcome for anxiety in youths. Psychol Med. 2025;55:e91.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. Diagnostic and Statistical Manual of Mental Disorders 2022. https://doi.org/10.1176/APPI.BOOKS.9780890425787.
Whitfield-Gabrieli S, Ghosh SS, Nieto-Castanon A, Saygin Z, Doehrmann O, Chai XJ, et al. Brain connectomics predict response to treatment in social anxiety disorder. Molecular Psychiatry. 2016;21:680–5.
Doehrmann O, Ghosh SS, Polli FE, Reynolds GO, Horn F, Keshavan A, et al. Predicting treatment response in social anxiety disorder from functional magnetic resonance imaging. JAMA Psychiatry. 2013;70:87–97.
Lazarov A, Pine DS, Bar-Haim Y. Gaze-Contingent music reward therapy for social anxiety disorder: a randomized controlled trial. American Journal of Psychiatry. 2017;174:649–56.
Arad G, Azriel O, Pine DS, Lazarov A, Sol O, Weiser M, et al. Attention bias modification treatment versus a selective serotonin reuptake inhibitor or waiting list control for social anxiety disorder: a randomized clinical trial. American Journal of Psychiatry. 2023;180:357–66.
Zhu X, Lazarov A, Dolan S, Bar-Haim Y, Dillon DG, Pizzagalli DA, et al. Resting state connectivity predictors of symptom change during gaze-contingent music reward therapy of social anxiety disorder. Psychol Med. 2022;53:3115.
Azriel O, Arad G, Tik N, Weiser M, Bloch M, Garber E, et al. Neural activation changes following attention bias modification treatment or a selective serotonin reuptake inhibitor for social anxiety disorder. Psychol Med. 2024;54:3366–78.
Bar-Haim Y. Research Review: attention bias modification (ABM): a novel treatment for anxiety disorders. Journal of Child Psychology and Psychiatry. 2010;51:859–70.
MacLeod C, Clarke PJF. The attentional bias modification approach to anxiety intervention. Clinical Psychological Science. 2015;3:58–78.
Clauss K, Gorday JY, Bardeen JR. Eye tracking evidence of threat-related attentional bias in anxiety- and fear-related disorders: a systematic review and meta-analysis. Clin Psychol Rev. 2022;93:102142.
Bar-Haim Y, Lamy D, Pergamin L, Bakermans-Kranenburg MJ, Van Ijzendoorn MH. Threat-related attentional bias in anxious and nonanxious individuals: a meta-analytic study. Psychol Bull. 2007;133:1–24.
Armstrong T, Olatunji BO. Eye tracking of attention in the affective disorders: a meta-analytic review and synthesis. Clin Psychol Rev. 2012;32:704–23.
Bishop SJ. Trait anxiety and impoverished prefrontal control of attention. Nat Neurosci. 2009;12:92–98.
Eysenck MW, Derakshan N, Santos R, Calvo MG. Anxiety and cognitive performance: attentional control theory. Emotion. 2007;7:336–53.
Moran TP. Anxiety and working memory capacity: a meta-analysis and narrative review. Psychol Bull. 2016;142:831–64.
Derryberry D, Reed MA. Anxiety-related attentional biases and their regulation by attentional control. J Abnorm Psychol. 2002;111:225–36.
Pergamin-Hight L, Naim R, Bakermans-Kranenburg MJ, van IJzendoorn MH, Bar-Haim Y. Content specificity of attention bias to threat in anxiety disorders: a meta-analysis. Clin Psychol Rev. 2015;35:10–18.
Lazarov A, Abend R, Bar-Haim Y. Social anxiety is related to increased dwell time on socially threatening faces. J Affect Disord. 2016;193:282–8.
Ginat-Frolich R, Gilboa-Schechtman E, Huppert JD, Aderka IM, Alden LE, Bar-Haim Y, et al. Vulnerabilities in social anxiety: integrating intra- and interpersonal perspectives. Clin Psychol Rev. 2024;109:102415.
Vrijsen JN, Grafton B, Koster EHW, Lau J, Wittekind CE, Bar-Haim Y, et al. Towards implementation of cognitive bias modification in mental health care: State of the science, best practices, and ways forward. Behaviour Research and Therapy. 2024;179:104557.
Corbetta M, Shulman GL. Control of goal-directed and stimulus-driven attention in the brain. Nature Reviews Neuroscience. 2002;3:201–15.
Vossel S, Geng JJ, Fink GR. Dorsal and ventral attention systems: distinct neural circuits but collaborative roles. The Neuroscientist. 2014;20:150.
Sylvester CM, Corbetta M, Raichle ME, Rodebaugh TL, Schlaggar BL, Sheline YI, et al. Functional network dysfunction in anxiety and anxiety disorders. Trends Neurosci. 2012;35:527–35.
Schofield CA, Johnson AL, Inhoff AW, Coles ME. Social anxiety and difficulty disengaging threat: evidence from eye-tracking. Cogn Emot. 2012;26:300–11.
Buckner JD, Maner JK, Schmidt NB. Difficulty disengaging attention from social threat in social anxiety. Cognit Ther Res. 2010;34:99–105.
Morfini F, Kucyi A, Zhang J, Bauer CCC, Bloom PA, Pagliaccio D, et al. Brain functional connectivity predicts depression and anxiety during childhood and adolescence: a connectome-based predictive modeling approach. Imaging Neuroscience. 2025;3:2025.
Wang Z, Goerlich KS, Ai H, Aleman A, Luo YJ, Xu P. Connectome-Based predictive modeling of individual anxiety. Cerebral Cortex. 2021;31:3006–20.
Azriel O, Arad G, Pine DS, Lazarov A, Bar-Haim Y. Attention bias vs. attention control modification for social anxiety disorder: a randomized controlled trial. J Anxiety Disord. 2024;101:102800.
Liebowitz MR Social Phobia. 1987, pp 141-73.
Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. Clin Psychiatry. 1998;59:22–33.
Connor KM, Davidson JRT, Erik Churchill L, Sherwood A, Foa E, Weisler RH. Psychometric properties of the social phobia inventory (SPIN): new self-rating scale. The British Journal of Psychiatry. 2000;176:379–86.
Jenkinson M, Beckmann CF, Behrens TEJ, Woolrich MW, Smith SMFSL Neuroimage 2012; 62: 782-90.
Jenkinson M, Bannister P, Brady M, Smith S. Improved optimization for the robust and accurate linear registration and motion correction of brain images. Neuroimage. 2002;17:825–41.
Jenkinson M, Smith S. A global optimisation method for robust affine registration of brain images. Med Image Anal. 2001;5:143–56.
Andersson JLR, Jenkinson M, Smith S Non-linear optimisation FMRIB Technical Report TR07JA1. 2007.
Griffanti L, Salimi-Khorshidi G, Beckmann CF, Auerbach EJ, Douaud G, Sexton CE, et al. ICA-based artefact removal and accelerated fMRI acquisition for improved resting state network imaging. Neuroimage. 2014;95:232–47.
Thomas Yeo BT, Krienen FM, Sepulcre J, Sabuncu MR, Lashkari D, Hollinshead M, et al. The organization of the human cerebral cortex estimated by intrinsic functional connectivity. J Neurophysiol. 2011;106:1125–65.
Schaefer A, Kong R, Gordon EM, Laumann TO, Zuo X-N, Holmes AJ, et al. Local-Global parcellation of the human cerebral cortex from intrinsic functional connectivity MRI. Cerebral Cortex. 2018;28:3095–114.
Shen X, Finn ES, Scheinost D, Rosenberg MD, Chun MM, Papademetris X, et al. Using connectome-based predictive modeling to predict individual behavior from brain connectivity. Nat Protoc. 2017;12:506–18.
Finn ES, Shen X, Scheinost D, Rosenberg MD, Huang J, Chun MM, et al. Functional connectome fingerprinting: identifying individuals using patterns of brain connectivity. Nat Neurosci. 2015;18:1664–71.
Yip SW, Scheinost D, Potenza MN, Carroll KM. Connectome-Based prediction of cocaine abstinence. American Journal of Psychiatry. 2019;176:156–64.
Giesbrecht B, Woldorff MG, Song AW, Mangun GR. Neural mechanisms of top-down control during spatial and feature attention. Neuroimage. 2003;19:496–512.
Shulman GL, Astafiev SV, Franke D, Pope DLW, Snyder AZ, McAvoy MP, et al. Interaction of stimulus-driven reorienting and expectation in ventral and dorsal frontoparietal and basal ganglia-cortical networks. The Journal of Neuroscience. 2009;29:4392–407.
Putra HA, Park K, Oba H, Yamashita F. Adult attention-deficit/hyperactivity disorder traits in healthy adults associated with brain volumetric data identify precuneus involvement in traffic crashes. Sci Rep. 2023;13:22466.
Cavanna AE, Trimble MR. The precuneus: a review of its functional anatomy and behavioural correlates. Brain. 2006;129:564–83.
Halbertsma HN, Elshout JA, Bergsma DP, Norris DG, Cornelissen FW, de, et al. Functional connectivity of the Precuneus reflects effectiveness of visual restitution training in chronic hemianopia. Neuroimage Clin. 2020;27:102292.
Amano K, Wandell BA, Dumoulin SO. Visual field maps, population receptive field sizes, and visual field coverage in the human MT + complex. J Neurophysiol. 2009;102:2704–18.
Wu Y, Wang J, Zhang Y, Zheng D, Zhang J, Rong M, et al. The neuroanatomical basis for posterior superior parietal lobule control lateralization of visuospatial attention. Front Neuroanat. 2016;10:178329.
Acknowledgements
This research was supported by the European Research Council (ERC-2023-ADG 101141436) and JOY Ventures, Grant #R01- 30-2017-8156.
Author information
Authors and Affiliations
Contributions
YC conceptualized the current work, wrote the initial draft of the manuscript, generated the figures, and conducted the statistical analyses; NY contributed to data analysis; OA and GA recruited the participants, collected the data and designed the original study; OS, MW, EG, MB contributed to the clinical work; DP conceptualized the original study and revised the current manuscript; IT contributed to conceptualization of the current work and revised the manuscript; YBH conceptualized the current work and original study, revised the manuscript, and secured funding of original study. All authors revised the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study was approved by the Tel Aviv University, Tel Aviv Sourasky Medical Center, and Sheba Medical Center Institutional Review Boards. Clinicaltrials.gov Identifier: NCT03346239. All methods were performed in accordance with the relevant guidelines and regulations. Informed consent was obtained from all study participants.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Coldham, Y., Yair, N., Azriel, O. et al. The role of the dorsal attention network in attention bias modification for social anxiety disorder. Transl Psychiatry 16, 178 (2026). https://doi.org/10.1038/s41398-026-03957-z
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41398-026-03957-z
