
Abstract
Background
White spot lesions (WSLs) is a caries lesion distinguished by white opacity due to subsurface enamel demineralization. These lesions resulting from a disparity between detrimental and protective factors and can continue to demineralize if untreated. Early diagnosis and remineralization can reverse WSLs, supporting minimally invasive dental care.
Aim
To compare and assess the color of WSLs through spectrophotometer after application of Self-assembling peptide P11-4, 2% Arginine Enriched Sodium Fluoride varnish and Functionalized Tri Calcium Phosphate Fluoride varnish.
Methods
This randomized controlled triple-blind clinical trial enrolled pediatric participants (ages 8–12 years) presenting with moderate caries risk as defined by CAMBRA (Caries Management By Risk Assessment) criteria, with visible white spot lesions (WSLs) on the labial surfaces of maxillary permanent anterior teeth, classified as ICDAS scores 1 or 2. A total of 39 WSLs were incorporated into the study and randomly allocated into one of the three groups 13/each. Group I: Self-assembling peptide P11-4 varnish (study group), Group II: Arginine-enriched Sodium Fluoride varnish (study group) and Group III: Tri Calcium Phosphate Fluoride varnish (positive control group). The color change ΔE of each WSL was quantified using a spectrophotometer at the baseline. Dimensions of WSLs were assessed by digital photography, remineralizing agents were applied then patients were recalled for further applications after 3 and 6 months and for WSLs assessment after 3, 6 and 9 months.
Results
All groups demonstrated progressive color improvement over time. At 3 months, Group I showed the least improvement (ΔE = 16.39 ± 3.04), followed by Group III (14.80 ± 3.11) and Group II (14.06 ± 4.46). By 9 months, Group II achieved (ΔE = 9.37 ± 3.79), and Group III (9.15 ± 2.74) surpassing Group I (12.21 ± 3.03). so both Group II and III ultimately outperformed Group I in color correction by the study’s end. Group II achieved significantly greater WSL reduction (14.98 ± 7.55%) compared to both Group I (27.93 ± 8.98%) and Group III (22.32 ± 8.61%), with no significant difference observed between Groups I and III.
Conclusions
Although all the three tested materials demonstrated an enhancement in the color and dimension of WSLs, 2% of Arginine Enriched Sodium Fluoride showed the best results followed by Functionalized Tri Calcium Phosphate Fluoride varnish, while self-assembling peptide P11-4 showed the lowest results.
Similar content being viewed by others

Background
White spot lesion is characterized as a white opacity resulting from subsurface enamel demineralization on smooth surfaces. The white look is attributed to alterations in the optical light scattering characteristics of the decalcified enamel. Consequently, early treatment including remineralization instead of restoring such WSLs is considered a crucial element of minimally invasive dentistry [1].
White spot lesions are triggered by pH changes resulting from the metabolic activities of bacteria present in the biofilm. These variations induce demineralization and remineralization. Consequently, the demineralization of tooth hard tissues occurs, resulting in the initiation of dental caries [2, 3].
In recent decades, various treatments, in addition to the necessity for superior oral hygiene, have been implemented to prevent the formation of white spot lesions (WSL), particularly the topical use of fluoride, which serves as the benchmark for other remineralization systems [4, 5]. The optimal remineralizing substance must facilitate the transfer of calcium and phosphate into the lesion. Fluoride agents can remediate initial lesions, although their impact is merely superficial [6]. This may lead to the remineralization of the porous surface layer, resulting in the obstruction of enamel pores, hindering ionic exchange at the surface enamel, and obstructing the remineralization of the lesion’s body, so challenging the achievement of complete remineralization [6].
One of the recent advances in remineralization is self-assembling peptides, produced by Credentis AG, Windisch, Switzerland, and devoid of human or animal-derived components. Biocompatibility testing performed according to ISO 10993 standards has confirmed that peptide P11-4 demonstrates no evidence of cytotoxicity in biological systems [7]. In a randomized controlled trial by Bröseler et al. [8], researchers evaluated the effectiveness of combining P11-4 peptide with fluoride varnish for white spot lesion treatment. Their findings revealed significantly greater reduction in early caries lesion size with P11-4 compared to fluoride varnish monotherapy.
L-arginine, an endogenous component of human saliva, is present in the oral cavity at physiological concentrations averaging 50 μM. Oral microbiota including Streptococcus, Lactobacillus, and Treponema species catabolize this amino acid through the arginine deiminase pathway, producing ornithine, ammonia, and CO₂. The resulting ammonia release elevates local pH, potentially contributing to oral ecological homeostasis [9]. Prior studies indicated that including arginine into dentifrices improved white spot lesions in comparison to non-arginine toothpastes. Furthermore, the integration of arginine with 5% sodium fluoride varnish produced a synergistic effect with increased F/Arg release [10, 11].
Modern fluoride varnishes incorporating bioactive tricalcium phosphate compounds (e.g., Clinpro™ 5% varnish) exhibit enhanced efficacy in managing incipient carious lesions. These formulations function through a unique mechanism where a protective calcium ion matrix forms during product formulation. Subsequent exposure to the oral environment triggers controlled release of fluoride, calcium, and phosphate ions from this matrix, enabling targeted remineralization of demineralized enamel [12]. Previous research documented that TCP fluoride varnish has greater protection against a cariogenic challenge and showed more reduction in lesion depth when compared with varnish containing 5% sodium fluoride alone [13, 14].
Demineralization modifies the physiological reflectivity of enamel, the disparity in refractive index between normal enamel and the demineralized region produces a milky white opaque look, distinctly identifiable from the adjacent intact enamel, facilitating the assessment of enamel color alterations caused by WSL treatment via spectrophotometric analysis [15,16,17].
The color of teeth can be assessed via a spectrophotometer on a CIELAB scale. The International Commission on Illumination, developed the CIELAB scale, which situates an object’s color inside a three-dimensional color space. The three axes are L*, a*, and b*. The coordinate L* quantifies an object’s lightness, ranging from 0 (absolute darkness) to 100 (pure white). Consequently, an elevated L* value indicates increased light reflectance of the object (CIE, 1978). The a* and b* coordinates measure color, representing an object’s location between red and green (a*) and yellow and blue (b*) [18].
Clinical dental photography is a helpful tool in assessment of percentage of WSLs. Recent computer programs are now used to analyze the digital images such as Adobe Photoshop and Auto CAD [19].
Aim of the study
This randomized controlled clinical investigation evaluated chromatic changes and dimension of white spot lesions following treatment with three distinct modalities: self-assembling peptide therapy, 2% arginine-enriched sodium fluoride varnish, and tri-calcium phosphate fluoride varnish.
The study postulated the null hypothesis that no statistically significant differences would exist among the remineralization efficacies of: P11-4 self-assembling peptide, 2% arginine-enriched sodium fluoride varnish and functionalized tri-calcium phosphate fluoride varnish, when treating incipient carious lesions.
Subjects, materials, and methods
Ethical considerations
The study protocol was reviewed by the Research Ethics Committee and Institutional Review Board, Faculty of Dentistry, Ain Shams University, with reference number (FDASU-Rec ID 032107). Both verbal and written consent were obtained from the participant’s caregiver following an explanation of the study’s aims and a guarantee of complete data confidentiality. All caregivers and subjects were apprised of their ability to quit from the study at any time. Additionally, subjects were requested to fill out an assent form after receiving an appropriate age-specific description of the study methodology and objectives. All consent and assent documents were rendered into Arabic.
Study design and settings
The investigation employed a randomized controlled trial design with three parallel treatment arms, utilizing equal allocation (1:1:1 ratio) across study groups. The trial protocol has been submitted at ClinicalTrials.gov PRS with ID NCT05127889. The study was conducted at the outpatient clinic of the Pediatric Dentistry and Dental Public Health department, Faculty of Dentistry, Ain Shams University.
Sample size estimation
A power analysis was designed to have adequate power to apply a three-sided statistical test of the null hypothesis that there is no significant difference between tested groups. By adopting an alpha level of (0.05) a beta of (0.2) i.e., power = 80% and an effect size (d) of (1.30) calculated based on the results of previous studies [8, 20]; the predicted sample size (n) was a total of (33) WSLs. Sample size calculation was performed using G*Power version 3.1.9.7 [21].
The group’s sample was raised by 15% to consider attrition, resulting in a total inclusion of 39 WSLs / 13 per group.
Eligibility criteria
Participants were screened using CAMBRA-based criteria: presence of active WSLs (disease indicator), adequate salivary function (protective factor), and no xerostomia (risk factor exclusion) [22].
Inclusion criteria
-
Patients aged from 8 to 12 years old have WSLs on the labial surface of upper permanent anterior teeth with a score of 1 & 2 according to the ICDAS that don’t require operative intervention indicating moderate caries risk per CAMBRA criteria [22, 23].
-
Patients who exhibited normal salivary flow (>0.7 mL/min stimulated) and no xerostomia, confirming adequate remineralization potential (protective factor).
-
Patients free from any systemic, genetic or developmental abnormalities [23].
Exclusion criteria
-
patients with high-risk CAMBRA indicators (e.g., xerostomia, frequent sugar exposure >3x/day), developmental enamel defects, or malocclusion impairing plaque control.
-
Patients who received tetracyclines or any other medication known to stain teeth or causing xerostomia [1].
-
Uncooperative patients [5].
-
Patients with class II or III malocclusion [5].
-
Mouth breathers [5].
-
Participants having non- carious lesions (enamel hypoplasia, dental fluorosis, etc.) [23].
Randomization and allocation
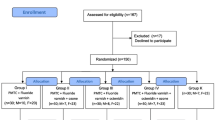
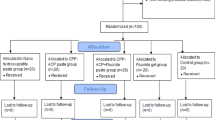
The research design adhered strictly to the Consolidated Standards of Reporting Trials (CONSORT) guidelines, with the study flowchart presented as Fig. 1. Each tooth exhibiting WSL was assigned a numerical designation from (1) to (39) and randomly distributed among the three experimental groups (13 teeth per group) by using IBM SPSS V26 (IBM, USA) statistical analysis software. Each tooth in each participant represented its own control. In the current study, randomization was dependent on two interrelated aspects, efficient sequence generation and unpredictable allocation concealment until the trial was completed. The allocation system was set up to enroll participants. All participant records were available only to the main investigator [24].

Flowchart depicting trial recruitment, randomization, allocation, and analysis during the follow-up period in accordance to CONSORT principles.
Groupings
Group I: Self-assembling peptide P11-4 varnish (study group n = 13)
Group II: Arginine-enriched, Sodium Fluoride varnish (study group n = 13)
Group III: Tri Calcium Phosphate Fluoride varnish (positive control group n = 13).
Blinding
The investigation utilized a triple-blind design, maintaining blinding of participants, outcome assessors and statistician throughout all follow-up evaluations. Reliability assessments included calculation of Intraclass Correlation Coefficients (ICC) to determine both inter- and intra-examiner consistency. ICC for intra examiner reliability was 0.82 which indicated consistency of the examiner over time, while it was 0.8 for inter examiner reliability which indicated strong agreement between examiners [21].
Methods
Clinical procedures
All intervention procedures were performed by the primary investigator as follows:
-
1)
Dental prophylaxis was performed for all patients with a polishing brush and non-fluoridated prophylactic paste (PROPHY PASTE by PSP, universal grit, ENGLAND) during the first clinical examination and before any application to remove dental plaque [17].
-
2)
For each tooth, baseline color change(ΔE) readings between normal tooth color and each WSL were performed by Vita Easyshade Spectrophotometer Compact (Vita Zahnfabrik, Bad Sa¨ckingen,Germany) [16].
-
The device was calibrated prior to every visit with a white table provided by the manufacturer. Excess saliva was evacuated using an air syringe without causing undue desiccation. Each WSL was assessed by positioning the probe tip perpendicularly to the surface, and the measurements were documented. To reduce measurement mistakes, three consecutive measurements were obtained for each evaluated region, with the mean value calculated and used for subsequent analysis [25].
-
The Model of the Commission International de l'Éclairage Lab (CIE L*a*b) color model was utilized to determine color variation. ΔE was computed using the subsequent equation: ΔE = √[(ΔL*)² + (Δa*)² + (Δb*)²], where: L* represents the lightness dimension (0 = black, 100 = white), a* indicates position on the red-green axis (positive = red, negative = green), b* denotes position on the yellow-blue axis (positive = yellow, negative = blue). Based on established perceptual thresholds, ΔE values ≤ 3.3 were considered clinically imperceptible color differences [26].
-
3)
Photographic assessment was done at baseline, where all the photographs were taken with the digital camera, macro lens configuration and external flash source.
-
The camera was configured in manual mode with an aperture setting of f/22 and a shutter speed of 1/125 s. The image quality was set to Fine, and the ISO sensitivity was fixed at 200. All photos were saved in JPEG (Joint Photographic Experts Group) format, ensuring compatibility with image analysis software for further processing.
-
The clinical photographs were processed using photographic editing software (Adobe Photoshop 7.0, Adobe Systems Inc., San Jose, California, USA), then the WSL area was calculated as % of the total teeth area using Image J software (version 1.53a National Institutes of Health, USA). The image analysis steps, and measurement technique were performed as follows [27] (Fig. 2):
-
i.
Step 1: The Photoshop software was used for the segmentation of each tooth by its outline, using the semiautomatic outline selection tool. In that way, each tooth was isolated from the rest of the image. After that, the areas with WSLs were automatically detected with the blue color range command and highlighted with blue and then separated from the rest of the image [28].
-
ii.
Step 2: Using image j software, the entire visible tooth area was automatically measured in pixels. From the images of isolated WSL which separated in step 1 and applying a threshold, the WSL in each tooth was automatically measured in pixels, and thcalculated as % of the total teeth area using the following equation: [28]
-
4)
Application of remineralizing agents
-
A.
Group I (Self assembling peptide P11-4): The lesions were treated with NaOCl to eliminate pellicle, etched for 20 s with 35% H3PO4 etching gel (BISCO SELECT, HV ETCH high viscosity) to partially demineralize tooth surface, and washed with water for 20 s. The lesions were dried using air tip syringe for 5 s and isolated using cotton rolls. The stick of self-assembling peptide (Curodont Repair TM, Credentis AG, Windisch, Switzerland) solution was inserted and subsequently withdrawn with its dampened sponge tip. Application of Curodont Repair ensued, allowing the solution to diffuse for five minutes until the tooth surface appeared dry (Fig. 3) [8].
-
B.
Group II (Arginine Enriched Sodium fluoride group): The Arginine powder (L-arginine A5006, Sigma-Aldrich, St. Louis, MO, USA) was applied at 2% w/v with 5% sodium fluoride varnish (Citrine sodium fluoride varnish Dharma Research, Inc). This was achieved by mixing 200 mg of arginine with 10 ml of sodium fluoride varnish for 60 s using a sterile micro brush. WSLs were gently dried using air tip syringe. The prepared varnish was then applied evenly with a micro brush and allowed to remain undisturbed for five minutes (Fig. 4) [29, 30].
-
C.
Group III (Tri Calcium Phosphate fluoride): TCP varnish (Clinpro white varnish, 3 M ESPE) was first mixed with the supplied brush to avoid the separation of the material during storage [31] A thin uniform layer of the varnish was applied on the lesion surface using the supplied micro brush (Fig. 5).
Post treatment instructions
-
Patients were instructed to refrain from rinsing, consuming food, or drinking for the longest restriction period required among the applied materials (30 minutes for P11-4 [28], 2 h for arginine-enriched fluoride varnish [29], or immediate eating with food restrictions for TCP fluoride varnish [31]). All participants were advised to avoid hard, sticky, or hot foods for 4 h post-treatment. Cool water consumption was permitted immediately after application.
-
All patients were advised to keep up proper dental hygiene by engaging in regular brushing.
Follw up
Patients were recalled for further applications after 3 and 6 months [8] and for WSLs assessment both photographic and colorimetric after 3, 6, 9 months followed CAMBRA guidelines for monitoring early caries intervention [8, 22].

Steps of WSLs % calculation.

Application of (Self assembling peptide P11-4).

Application of Arginine Enriched Sodium fluoride group.

Application of Clinpro White Varnish.
Statistical methods
Quantitative variables were reported as means ± standard deviations. Normality of distribution was verified using the Shapiro–Wilk test, while homogeneity of variance was assessed with Levene’s test. Parametric analysis of normally distributed color change data was achieved using a mixed-model analysis of variance (ANOVA). Post hoc pairwise comparisons were accomplished with Bonferroni-adjusted p-values to control for multiple comparisons. The alpha level for statistical significance was set a priori at p < 0.05. All analyses were done using R statistical software (version 4.4.0) [32, 33].
In photographic assessment, the percentage of change was calculated by the following equation:
-
P-value ≤ 0.05 was considered statistically significant (95% significance level), while p-value ≤ 0.001 was deemed highly statistically significant (99% significance level).
Results
Color change
Inter group comparison of color change
ΔE values for all test materials are summarized in (Table 1).
Baseline ΔE measurements revealed no significant intergroup differences (p > 0.05). At 3-month evaluation, Group I demonstrated significantly higher ΔE values (indicating less color improvement) compared to Groups II and III (p < 0.05). Longitudinal analysis showed progressive color improvement in all groups at 6- and 9-month intervals, with Group I maintain significantly elevated ΔE values versus both groups (p < 0.001). No statistically significant differences were seen between Groups II and III at any timepoint (3/6/9 months).
Intragroup comparison of color change
Quantitative comparisons of color change (ΔE) at each timepoint are summarized in (Table 2).
In group I, there was a significant decrease in Mean ± SD of ΔE values at 6- and 9-months intervals compared to baseline and 3 months (p < 0.001). While in group II and group III a significant difference was found in ΔE (p < 0.001) among successive time intervals.
Photographic assessment results
Assessment of the mean lesion percentage
Intra-group comparison of the percentage of white spot lesions:
Effect of the time interval on the percentage of white spot lesions under the same group type presented in Table 3.
All three treatment groups demonstrated progressive and statistically significant reductions in white spot lesion (WSL) percentages over the 9-month study period (p < 0.001).
In Group I (P11-4), the mean WSL percentage decreased from 47.43 ± 8.91% at baseline to 41.08 ± 9.51% at 3 months, 34.67 ± 6.87% at 6 months, and 27.93 ± 8.98% at 9 months. Significant reductions were observed between baseline vs. 6 and 9 months (p < 0.05), while changes between 3 vs. 6 months and 6 vs. 9 months were not statistically significant.
Group II (Arginine-Fluoride) showed the most substantial improvement, declining from 34.19 ± 5.95% at baseline to 25.43 ± 6.87% at 3 months, 19.36 ± 7.67% at 6 months, and 14.98 ± 7.55% at 9 months. All time intervals demonstrated significant differences (p < 0.05) except between 6 and 9 months.
For Group III (TCP Fluoride), the mean WSL percentage reduced from 41.04 ± 13.73% at baseline to 33.49 ± 11.35% at 3 months, 27.38 ± 9.86% at 6 months, and 22.32 ± 8.61% at 9 months. Significant improvements were seen between baseline and all follow-up intervals (p < 0.05) and between 3 and 9 months (p < 0.05), while differences between 3 vs. 6 months and 6 vs. 9 months were not statistically significant.
Assessment of the change in lesion percentage after different follow-ups
Intra-group comparison of the change % of Lesion area:
Effect of the time interval on the change % of Lesion area under the same group presented in Table 4.
All three treatment groups demonstrated progressive and statistically significant increases in lesion area reduction percentages over time (p < 0.001). Group I showed mean changes of 13.57 ± 10.19% at 3 months, 26.63 ± 7.22% at 6 months, and 40.13 ± 16.76% at 9 months. Group II exhibited the most substantial improvements with 25.94 ± 12.85%, 43.28 ± 18.6%, and 56.21 ± 19.12% reduction at respective intervals. Group III displayed intermediate results with 17.63 ± 10.69%, 32.88 ± 13.01%, and 45 ± 12.27% reduction.
Inter-group comparison of the change % of Lesion area
Effect of the group type on the change % of lesion area under the same time interval presented in Table 5.
From Table 5, we can conclude the following:
-
For all time intervals, Group II achieved the highest means of change% while Group I achieved the lowest mean.
-
There was no significant difference between Group I and Group III means at all time intervals.
-
Also, there was a significant difference between Group I and Group II as well as between Group II and Group III at all time intervals.
Discussion
A white spot lesion is a visual phenomenon caused by the loss of subsurface tissue. The surface features of active WSLs display enlarged intercrystalline spaces and diminished interprismatic mineral content in the surface layer. The restorative treatment of first enamel lesions results in adverse effects on the dental structure. The objective of contemporary dentistry emphasizes noninvasive treatment of WSLs [23, 31].
Given the lack of reliable evidence supporting remineralizing or camouflaging strategies for treating white spot lesions, further well performed clinical studies are necessary to determine the most effective clinical methods [34].
This randomized controlled trial aimed to evaluate color improvement in white spot lesions (WSLs) following treatment with three remineralizing agents: a self-assembling peptide (P11-4), a 2% arginine-enriched sodium fluoride varnish, and a tri-calcium phosphate (TCP) fluoride varnish. Lesion shade was measured at baseline, 3, 6, and 9 months using a VITA Easyshade spectrophotometer. These materials have been shown to provide effective, minimally invasive treatment for early caries, offering superior results compared to traditional fluoride therapies [29, 35, 36].
The participants included were selected from an age range of 8–12 years as the prevalence of white spot lesions significantly escalates during the pre-adolescent stage. Moreover, younger patients exhibit greater susceptibility to remineralization compared to older individuals. No conclusive evidence exists regarding a sexual predisposition to WSLs, whereas the labial surfaces of maxillary anterior teeth accounted for 73% of WSLs. The participants were free from systemic illnesses or concurrent drugs that could reduce salivary flow rate [37]. Patients exhibiting developmental enamel defects such as hypomineralization disorders (e.g., fluorosis, hypoplasia) were not included in this research. These conditions involve genetic mutations that disrupt enamel matrix formation, making the affected tooth structure less responsive to remineralization therapies compared to typical caries lesions [24, 38].
White spot lesions were visually evaluated using the air dryness test, as it is considered the gold standard for assessing color changes and the depth of these lesions [24]. Prior to the assessment in the current study, dental prophylaxis was performed to prevent masking the tooth color and to ensure accurate readings [16].
Color evaluation was conducted utilizing a VITA Easyshade® guide spectrophotometer. Instrumental color analysis presents a distinct advantage over ocular color assessment due to its objective, quick, and quantifiable nature. VITA Easyshade® when compared to other spectrophotometers, is considered feasible, applicable and convenient with acceptable repeatability [39].
Dimensions of WSLs were assessed by digital photography as it was proven that standardized photographic technique is reliable, accurate, and reproducible compared to direct ICDAS II examination, confirming its effectiveness for assessing WSLs in digital images. The percentage area of WSL per total facial tooth surface was calculated to control magnification differences [19].
Digital cameras offer notable benefits, as highlighted by Benson et al. [27] by minimizing inconsistencies in image capture and improving efficiency. Quantitative assessment of enamel demineralization can be achieved by measuring either the dimensions of white spot lesions or the degree of mineral loss.
Digital camera canon D800 was used as it allows full flexibility regarding exposure controls and accessories, such as the use of a macro lens (sigma 108 mm) for close-up work and external flash ring units (Godox flash ring) to capture important differences in enamel color. This camera also produces high-resolution images [27].
Self-assembling peptide was implemented in accordance with the equipment manufacturer’s standardized operational guidelines. The rationale for treating enamel with 2% sodium hypochlorite is to remove surface organic pellicle, thus increasing the diffusion of Ca²⁺ and PO₄³⁻ ions into the enamel subsurface lesion. Teeth were conditioned with 35% Phosphoric acid for 20 s to remove the pseudo-calcified outermost 25 μm of the enamel surface which would increase surface porosity enhancing the remineralization process and allowing easier access for the minerals to the body of the lesion [40].
In present study, 2% by w/v arginine was used, because it was reported that combining 2% L-arginine into 5% NaF varnish enhances the physical characteristics of fluoride and creates a stable matrix that consistently releases greater levels of F/Arg compared to other concentrations [41].
Tri-calcium phosphate fluoride varnish used as positive control, was selected for its effectiveness as a fluoride-based remineralizing agent. The varnish facilitates remineralization by supplying calcium, phosphate, and fluoride ions, with a high fluoride concentration (22,600 ppm) allowing for a single application [31, 42, 43].
Follow up was performed at 3, 6, 9 months as the mineral deposition is expected to occur within 3–6 months [36]. Multiple applications were performed at different intervals 0, 3, 6 months as repeated applications performed ensures the consistent availability of ions to promote mineral growth. Over time, this leads to substantial repair and filling of the lesion. Another reason for multiple applications is that remineralization is not immediate and requires a consistent therapeutic effect over weeks or even months [36, 44, 45].
The findings of the current investigation indicated that all three evaluated materials demonstrated an enhancement in the hue of WSL. For color change (ΔE) measured at baseline, there was no statistically significant difference between different materials. At 3 months, the highest ΔE value was found (lowest color change) in group I (16.39 ± 3.04), which was significantly higher than group II (14.06 ± 4.46) and group III (14.80 ± 3.11). At 6 and 9 months, all the tested materials showed color improvement with the highest values in group I at 6 months (12.85 ± 3.23) and 9 months (12.21 ± 3.03) followed by group III at 6 months (11.50 ± 3.28) and 9 months (9.15 ± 2.74), while the lowest values were recorded in group II at 6 months (11.58 ± 2.77) and 9 months (9.37 ± 3.79).
In the clinical assessment of white spot lesions (WSLs), all tested materials reduced lesion percentage, but to varying degrees. Group II (2% arginine-enriched sodium fluoride varnish) showed the greatest reduction (14.98 ± 7.55), performing significantly better than the other groups. Group I (self-assembling peptide) had the highest lesion percentage (27.93 ± 8.98), followed by Group III (functionalized tricalcium phosphate fluoride varnish) (22.32 ± 8.61), with no significant difference between them. However, Group I differed significantly from Group II at all time points, highlighting the superior efficacy of the arginine-enriched fluoride varnish in reducing WSLs.
In group I, there was a significant decrease in Mean ± SD of ΔE values at 6- and 9-months intervals compared to baseline and 3 months (p < 0.001). While in group II and group III a significant difference was found in ΔE (p < 0.001) among successive time intervals.
The findings of this investigation suggested that group I (self-assembling peptide) improved the color of WSLs, but to a lesser extent than the other groups and this came in agreement with Wierichs et al. [46] who reported that P 11-4 could reduce lesion progression but did not significantly improve the visual appearance or mask the white spots as effectively as low-viscosity resin infiltrates.
These results also concurred with, Golland et al. [47] who showed that the application of P11-4 on demineralized bovine enamel did not result in increased fluorescence, as evaluated by quantitative laser fluorescence, suggesting either a lack of remineralization or the existence of irregular crystals. Additionally, Memarpour et al. [48] revealed that P11-4 peptide treatment resulted in primary teeth exhibiting the lowest percentage of surface enamel microhardness compared to CPP-ACP, fluoridated bioactive glass toothpaste, and fluoridated toothpaste. Recently, a study by Wahba et al. [49] reported the inability of P11-4 peptide to remineralize caries in deciduous teeth.
These results diverged with those of Alkilzy et al. [45] who reported superior clinical outcomes for P11-4 in managing early occlusal caries in pediatric patients. Their study demonstrated significantly reduced laser fluorescence measurements and improved visual assessment scores in the peptide-treated group versus fluoride controls. Furthermore, they observed caries regression (ICDAS index improvement) and lesion inactivation (Nyvad criteria), suggesting P11-4’s biomimetic properties combined with fluoride may enhance early caries reversal through noninvasive remineralization.
Jablonski-Momeni et al. [20] and Sedlakova Kondelova et al. [50] also reported the benefits of P11-4 in conjunction with fluoride compared to the application of fluoride varnish alone. Kamal et al. [40] also showed that the P11-4 peptide had enhanced efficacy when coupled with either fluoride or CCP-ACPF, compared to its solitary use.
The findings of this study indicated no significant improvement at 3-months- interval in group I. However, with multiple applications over a longer period (6 and 9 months), noticeable improvement was observed. This came compatible with Rathore et al. [44] and Vas et al. [51] who showed that significant mineral gains between 8 and 12 weeks after self-assembling peptide treatment occur, with increased effectiveness over longer intervals.
The results of group II (2% Arginine Enriched Sodium Fluoride varnish) showed higher improvement in color than other groups at all intervals. This could be attributed to its efficacy in halting caries progression, as arginine-fluoride complexes can be retained within enamel, serving as a reservoir that releases fluoride during acid exposure, thereby facilitating the remineralization process. Additionally, it elevates pH, establishing favorable conditions for remineralization and augmenting the synergistic effect of fluoride [41].
These results came in agreement with Bijle et al. [52] reported that 2% arginine-enhanced sodium fluoride toothpaste significantly improved enamel lesion remineralization rates. Similar outcomes were observed with Cheng et al. [10] and Oliveira et al. [53] whose studies on bovine enamel showed that the fluoride-arginine combination enhanced surface microhardness in both sound and demineralized specimens.
Furthermore, this came in line with Alblooshi et al. [30] who assessed the fluoride release potential of L-arginine incorporated into fluoride varnishes. Results showed that arginine significantly increased fluoride release compared to controls (Four readily available F varnishes), with the primary fluoride concentration being lower in the arginine groups, indicating a chemical interaction between fluoride and arginine. This suggests that adding arginine enhances the fluoride release potential, boosting the varnish’s effectiveness in remineralization and caries prevention.
Group III (Functionalized Tri Calcium Phosphate Fluoride varnish) showed improvement in the color of WSLs. This may result from fTCP’s capacity to function as a bioactive source of mineralizing constituents. TCP collaborates with fluoride to produce more robust, acid-resistant minerals compared to those formed by fluoride alone [14]. This result also came in agreement with Alamoudi et al. [14] reported significantly higher surface microhardness values for fluoride varnish containing functionalized tri-calcium phosphate (fTCP) compared to conventional fluoride formulations. Their study demonstrated mean Knoop hardness numbers (KHN) of 56.2 for 5% NaF+fTCP versus 45.7 for NaF alone, with untreated controls showing the lowest hardness (35.1 KHN).
Likewise, Rirattanapong et al. [54] also showed that fluoride varnish containing tricalcium phosphate had a high remineralization effect and can inhibit progression of WSLs. Elkassas and Arafa [55] found that remineralizing agents containing different calcium-phosphate formulas and fluoride have increased remineralization potential compared to artificial saliva. TCP varnish presented the highest remineralization tendency with the greatest resistance for acid challenge when compared to Tooth Mousse Plus and Vanish™XT.
None of the evaluated materials produced a color alteration in the white spot lesions (WSLs) that matched that of normal teeth as clinically tolerable color changes, deemed not visually noticeable, arise when ΔE* ≤3.3 which was not evident in any of the three groups [26].
The result of this study rejected the null hypothesis, demonstrating a substantial difference in color change (ΔE) across the investigated materials. The study designed as a randomized controlled double-blinded approach, reduces bias and improves the dependability of the findings. Moreover, the use of three distinct remineralizing agents facilitates a thorough comparison of efficacy in treating white spot lesions (WSLs). The evaluations at 3, 6, and 9 months yield significant insights into the long-term effect of the treatments.
On the other hand, the Vita Easy Shade Spectrophotometer primarily measures surface color and does not provide information on the depth of theWSL, which could be an important factor for treatment evaluation. The study focuses on color change as the primary outcome, potentially overlooking other important aspects of WSL improvement, such as surface integrity or depth of remineralization.
Conclusions
All three examined materials demonstrated an enhancement in the coloration of WSLs. However, 2% Arginine Enriched Sodium Fluoride exhibited the most favorable outcomes, succeeded by Functionalized Tri Calcium Phosphate Fluoride varnish, whilst self-assembling peptide P11-4 demonstrated the least enhancement in color.
Data availability
The datasets generated and/or analyzed during the current study are available from the first author “Bardis Salah” upon request.
References
Bakry AS, Abbassy MA. Increasing the efficiency of CPP-ACP to remineralize enamel white spot lesions. J Dent. 2018;76:52–7.
Guo L, Shi W. Salivary biomarkers for caries risk assessment. J Calif Dental Assoc. 2013;41:107–18.
Yap J, Walsh LJ, Naser-Ud Din S, Ngo H, Manton DJ. Evaluation of a novel approach in the prevention of white spot lesions around orthodontic brackets. Aust Dent J. 2014;59:70–80.
Du M, Cheng N, Tai B, Jiang H, Li J, Bian Z. Randomized controlled trial on fluoride varnish application for treatment of white spot lesion after fixed orthodontic treatment. Clin Oral Investig. 2012;16:463–8.
Zero DT. Dentifrices, mouthwashes, and remineralization/caries arrestment strategies. In: BMC Oral Health. BioMed Central Ltd.; 2006.
Deyhle H, Dziadowiec I, Kind L, Thalmann P, Schulz G, Müller B. Mineralization of early stage carious lesions in vitro-a quantitative approach. Dent J. 2015;3:111–22.
Davies RPW, Aggeli A, Beevers AJ, Boden N, Carrick LM, Fishwick CWG, et al. Self-assembling β-sheet tape forming peptides. Supramolecular Chem. 2006;18:435–43.
Bröseler F, Tietmann C, Bommer C, Drechsel T, Heinzel-Gutenbrunner M, Jepsen S. Randomised clinical trial investigating self-assembling peptide P11-4 in the treatment of early caries. Clin Oral Investig. 2020;24:123–32.
Morris SM. Arginine: beyond protein23. Am J Clin Nutr. 2006;83:508S–512S.
Cheng X, Xu P, Zhou X, Deng M, Cheng L, Li M, et al. Arginine promotes fluoride uptake into artificial carious lesions in vitro. Aust Dent J. 2015;60:104–11.
Agnello M, Cen L, Tran NC, Shi W, McLean JS, He X. Arginine Improves pH Homeostasis via Metabolism and Microbiome Modulation. J Dent Res. 2017;96:924–30. https://doi.org/10.1177/0022034517707512.
Kobeissi R, Badr SBY, Osman E. Effectiveness of self-assembling peptide P11-4 compared to tricalcium phosphate fluoride varnish in remineralization of white spot lesions: a clinical randomized trial. Int J Clin Pediatr Dent. 2020;13:451–6.
Tuloglu N, Bayrak S, Tunc E Sen, Ozer F. Effect of fluoride varnish with added casein phosphopeptide-amorphous calcium phosphate on the acid resistance of the primary enamel. BMC Oral Health. 2016;16:103.
AlAmoudi SA, Pani SC, AlOmari M. The effect of the addition of tricalcium phosphate to 5% sodium fluoride varnishes on the microhardness of enamel of primary teeth. Int J Dent. 2013;2013:486358.
Vitai V, Teutsch B, Németh A, Borbély J. Comparison between intraoral scanner and spectrophotometer shade matching: a systematic review and meta-analysis. J Dent. 2024;147:105168.
Kim HK. Evaluation of the repeatability and matching accuracy between two identical intraoral spectrophotometers: an in vivo and in vitro study. J Adv Prosthodontics. 2018;10:252–8.
Corciolani G, Vichi A. Repeatability of colour reading with a clinical and a laboratory spectrophotometer. Int Dent South Afr. 2006;8:62–70.
Ly B, Dyer E, Feig J, Chien A, Bino S. Research techniques made simple: cutaneous colorimetry: a reliable technique for objective skin color measurement. J Invest Dermatol. 2020;140:3–12.e1.
Hassan IT, Allam GG. A standardized in vivo photographic technique to assess the remineralization of white spot lesions after orthodontic treatment. Egypt Dent J. 2017;63:121–8.
Jablonski-Momeni A, Korbmacher-Steiner H, Heinzel-Gutenbrunner M, Jablonski B, Jaquet W, Bottenberg P. Randomised in situ clinical trial investigating self-assembling peptide matrix P11-4 in the prevention of artificial caries lesions. Sci Rep. 2019;9:269.
Faul F, Erdfelder E, Lang AG, Buchner A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39:175–91.
Featherstone, JDB, Crystal, YO, Gomez, FR. CAMBRA® caries management by risk assessment: A comprehensive caries management guide for dental professionals. ResearchGate. 2019. https://www.researchgate.net/publication/334401386.
Schwendicke F, Splieth C, Breschi L, Banerjee A, Fontana M, Paris S, et al. When to intervene in the caries process? An expert Delphi consensus statement. Clin Oral Investig. 2019;23:3691–703.
Hadler-Olsen S, Sandvik K, El-Agroudi MA, Ogaard B. The incidence of caries and white spot lesions in orthodontically treated adolescents with a comprehensive caries prophylactic regimen - a prospective study. Eur J Orthod. 2012;34:633–9.
Tekçe N, Tuncer S, Demirci M, Serim ME, Baydemir C. The effect of different drinks on the color stability of different restorative materials after one month. Restor Dent Endod. 2015;40:255.
Karaarslan ES, Mehmet B, Ertan E, Cebe MA, Usumez A. Assessment of changes in color and color parameters of light-cured composite resin after alternative polymerization methods. Eur J Dent. 2013;7:110–6.
Benson PE, Shah AA, Willmot DR. Measurement of white lesions surrounding orthodontic brackets: captured slides vs digital camera images. Angle Orthod. 2005;25:226–30.
Amin O, Shaalan O, Riad M. Remineralization potential of curodont repair flouride plus versus CPP-ACP in white spot lesions. Advanced Dent J. 2023;5:110–8.
Yip K, Abdalla MM, Bijle MN, Yiu C. Effect of arginine-fluoride varnish on preventing enamel erosion by paediatric liquid medicaments. BMC Oral Health. 2023;23:892.
Alblooshi NA, Krithikadatta J, Yiu C, Bijle MN. Fluoride release potential of arginine-incorporated fluoride varnishes. Dent Mater J. 2024;43:146–54.
Handa A, Chengappa D, Sharma P, Handa JK. Effectiveness of Clinpro Tooth Crème in comparison with MI Varnish with RECALDENTTM for treatment of white spot lesions: a randomized controlled trial. Clin Oral Investig. 2023;27:1473–81.
Team RC. RA language and environment for statistical computing, R Foundation for Statistical Computing. Vienna, Austria: Team RC; 2020.
Manarelli MM, Delbem ACB, Báez-Quintero LC, de Moraes FRN, Cunha RF, Pessan JP. Fluoride varnishes containing sodium trimetaphosphate reduce enamel demineralization in vitro. Acta Odontol Scand. 2017;75:376–8.
Raphael S, Blinkhorn A. Is there a place for Tooth Mousse® in the prevention and treatment of early dental caries? A systematic review. BMC Oral Health. 2015;15:113.
Karlinsey RL, Pfarrer AM. Fluoride plus functionalized β-TCP: a promising combination for robust remineralization. Adv Dent Res. 2012;24:48–52. https://doi.org/10.1177/0022034512449463.
Alkilzy M, Tarabaih A, Santamaria RM, Splieth CH. Self-assembling peptide P11-4 and fluoride for regenerating enamel. J Dent Res. 2018;97:148–54.
Julien KC, Buschang PH, Campbell PM. Prevalence of white spot lesion formation during orthodontic treatment. Angle Orthod. 2013;83:641–7.
Braga MM, Oliveira LB, Bonini GAVC, Bönecker M, Mendes FM. Feasibility of the international caries detection and assessment system (icdas-ii) in epidemiological surveys and comparability with standard world health organization criteria. Caries Res. 2009;43:245–9.
Horuztepe SA, Baseren M. Effect of resin infiltration on the color and microhardness of bleached white-spot lesions in bovine enamel (an in vitro study). J Esthet Restor Dent. 2017;29:378–85.
Kamal D, Hassanein H, Elkassas D, Hamza H. Complementary remineralizing effect of self-assembling peptide (P11-4) with CPP-ACPF or fluoride: an in vitro study. J Clin Exp Dent. 2020;12:e161–8.
Bijle MN, Ekambaram M, Lo E, Yiu C. Physicochemical characteristics of arginine enriched naf varnish: an in vitro study. Polymers. 2020;12:1–14.
Buckshey S, Anthonappa RP, King NM, Itthagarun A. Remineralizing potential of ClinPro ® and tooth mousse plus ® on artificial carious lesions. J Clin Pediatr Dent. 2019;43:103–8.
Manchanda S, Liu P, Sardana D, Peng S, Lo ECM, Yiu CKY. Randomized clinical trial to compare three fluoride varnishes in preventing early childhood caries. J Dent. 2024;147:105141.
Rathore K, Patnana AK, Chugh VK, Chugh A, Kumar P. Self-assembling peptides for managing white spot lesions: a systematic review and meta-analysis. Eur Arch Paediatr Dent. 2023;24:519–31. https://doi.org/10.1007/s40368-023-00821-2.
Alkilzy M, Qadri G, Splieth CH, Santamaría RM. Biomimetic Enamel Regeneration Using Self-Assembling Peptide P11-4. Biomimetics. 2023;8:290.
Wierichs RJ, Kogel J, Lausch J, Esteves-Oliveira M, Meyer-Lueckel H. Effects of self-assembling peptide P11-4, fluorides, and caries infiltration on artificial enamel caries lesions in vitro. Caries Res. 2017;51:451–9. https://doi.org/10.1159/000477215.
Golland L, Schmidlin PR, Schätzle M. The potential of self-assembling peptides for enhancement of in vitro remineralisation of white spot lesions as measured by quantitative laser fluorescence. Oral Health Prev Dent. 2017;15:147–52.
Memarpour M, Razmjouei F, Rafiee A, Vossoughi M. Remineralization effects of self-assembling peptide P11-4 associated with three materials on early enamel carious lesions: an in vitro study. Microsc Res Tech. 2022;85:630–40.
Wahba N, Schwendicke F, Kamel MA, Allam G, Kabil N, Elhennawy K. Preventing and arresting primary tooth enamel lesions using self- assembling peptide P11-4 in vitro. J Int Soc Prev Community Dent. 2022;12:58–70.
Sedlakova Kondelova P, Mannaa A, Bommer C, Abdelaziz M, Daeniker L, di Bella E, et al. Efficacy of P11-4 for the treatment of initial buccal caries: a randomized clinical trial. Sci Rep. 2020;10:20211. https://doi.org/10.1038/s41598-020-77057-3.
Vas NV, Jain RK. Self Assembling Peptide P11-4 for management of white spot lesions in subjects undergoing orthodontic treatment. Int J. Orthodontic Rehabilit. 2024;15:13–25.
Bijle MNA, Ekambaram M, Lo ECM, Yiu CKY. The combined enamel remineralization potential of arginine and fluoride toothpaste. J Dent. 2018;76:75–82.
Oliveira PHC, Oliveira MRC, Oliveira LHC, Sfalcin RA, Pinto MM, Rosa EP, et al. Evaluation of different dentifrice compositions for increasing the hardness of demineralized enamel: an in vitro study. Dent J. 2019;7:14.
Rirattanapong P, Vongsavan K, Saengsirinavin C, Pornmahala T. Effect of fluoride varnishes containing tri-calcium phosphate sources on remineralization of initial primary enamel lesions. 2014;45:499–504.
Elkassas D, Arafa A. Remineralizing efficacy of different calcium-phosphate and fluoride based delivery vehicles on artificial caries like enamel lesions. J Dent. 2014;42:466–74.
Funding
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB).
Author information
Authors and Affiliations
Contributions
All authors participated in the study of conception and design. All clinical procedures were performed by BS. Data analysis was done by BS, NK, DH and MG. BS wrote the first draft of the manuscript. NK and DH revised and edited the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests. The study protocol was reviewed by the Research Ethics Committee and Institutional Review Board, Faculty of Dentistry, Ain Shams University, with reference number (FDASU-Rec ID 032107). Both verbal and written consent were obtained from the participants’ caregiver following an explanation of the study’s aims and a guarantee of complete data confidentiality. All caregivers and subjects were apprised of their ability to quit from the study at any time. Additionally, subjects were requested to fill out an assent form after receiving an appropriate age-specific description of the study methodology and objectives.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Elaziz, B.S.A., Hamdy, D., Galal, M. et al. The remineralizing ability of self-assembling peptide P11-4, 2% arginine enriched sodium fluoride and functionalized tri calcium phosphate fluoride varnishes in treatment of white spot lesions – a randomized controlled trial. BDJ Open 11, 70 (2025). https://doi.org/10.1038/s41405-025-00353-5
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41405-025-00353-5
