
Abstract
Objectives
The present study assesses the clinical performance and occlusal wear of low-shrinkage giomer and nanohybrid composite in proximal restorations.
Methods
Fifty participants with proximal caries in posterior teeth (n = 25) were recruited. Teeth were restored with either conventional nano-hybrid composite (Filtek Z250XT, 3M ESPE, USA) or low-shrinkage giomer (Beautifil II LS, Shofu Inc, Japan). Clinical performance was assessed using revised FDI criteria at baseline, 6 and 12 months. Wear was assessed after 12 months by using 3D inspection and metrology software (Geomagic Control X; 3D Systems, USA). FDI scores were analyzed using Chi‑square test for intergroup comparisons and Cochran’s Q‑test for intragroup comparisons. Wear data were analyzed using independent t test for intergroup comparison and paired t test for intragroup comparisons.
Results
At the 12-month follow-up, both Beautifil II LS and Filtek Z250XT exhibited high clinical success rates, with 100% and 96% success rates, respectively. Beautifil II LS restorations had a 4% lower risk of failure compared to Filtek Z250XT (ARR = 4.0 (95% CI −12.6 to 19.5, P > 0.05)). The mean wear after 12 months was 0.036 ± 0.01 mm for Beautifil II LS and 0.038 ± 0.01 mm for Filtek Z250XT. The difference between groups was minimal (0.0026 mm; 95% CI: –0.0271 to 0.0324) and not statistically significant (P = 0.8178).
Conclusion
Low-shrinkage giomer showed satisfactory clinical performance and wear resistance compared to nanohybrid resin composite after one year. Both materials are considered clinically acceptable as per the American Dental Association (ADA) standards.
Similar content being viewed by others


Introduction
Over the past decade, the state of art of composite materials has undergone substantial advancements driven by superior esthetic outcomes and ease of handling. Major developments in composite restorations have predominantly focused on modifications to the monomer composition, filler technology, and initiator systems [1]. Filler type, for instance, plays a critical role in determining radiopacity and mechanical performance, while also contributing to improved translucency and handling characteristics, including consistency, polishability, and long-term gloss stability [2]. Additionally, continuous reduction in filler particle size has been pursued to enhance initial surface polish while maintaining gloss over time. These innovations have led to the progressive evolution of composites from hybrid, microhybrid, and microfilled formulations till reaching nano-sized composites [3].
Despite the merits of nanohybrid composites, resin composite material still faces certain challenges, such as technique sensitivity, lack of antibacterial property and polymerization shrinkage [4]. Polymerization shrinkage is perhaps one of the most critical problems of direct restorative materials. Polymerization shrinkage of resin-based composites ranges from 2.6 to 7.1% [5]. Polymerization stresses can lead to microleakage, marginal discoloration, postoperative sensitivity, stress at the tooth-restoration interface, and secondary caries [6]. Moreover, the absence of antibacterial property and remineralization potential are another critical factors that may increase the possible incidence of secondary caries around restorations [4].
In the early 2000s, Shofu (Kyoto, Japan) developed a line of fluoride-releasing materials called “giomer”. Giomers are considered true hybridization of glass ionomer and composite resin, containing surface pre-reacted glass ionomer (S-PRG) filler particles within a resin matrix [7]. These S-PRG fillers allows the material to release fluoride and be recharged with fluoride, which in theory makes it able to release fluoride over long term [8]. Moreover, this technology enables the controlled release of multiple therapeutic ions other than fluoride, including strontium, sodium, borate, aluminum, and silicate contributing to remineralization, acid buffering, antimicrobial activity, and inhibition of demineralization [9].
Furthermore, the continuous modifications and changes in composite formulations have resulted in expanded range of giomer materials including Beautifil II, a bioactive restorative composite, with improved filler loading, allowing for enhanced polishability and shade stability [7]. Recently, low-shrinkage giomer resin composite (LS-GRC) was introduced to the market enhanced by their low-shrinkage property through implementing filler technology in the matrix system. According to the manufacturer, low-shrinkage giomer resin composite (LS-GRC) demonstrates volumetric shrinkage of 0.8% and polymerization shrinkage stress of 2.72 MPa, which contributes to superior clinical performance over time [10].
Several studies have been conducted to evaluate the overall clinical performance of LS-GRC with comparable success rates when compared to other restorative materials [11, 12]. However, further research is still needed to evaluate the performance and quantitative amount of wear after placement of LS-GRC in stress-bearing areas. Assessing wear behavior of composite materials is crucial as excessive occlusal wear may result in loss of occlusal morphology, marginal breakdown, loss of vertical dimension, food impaction, and deterioration of functional and esthetic performance of the restoration [13]. Traditional wear assessment methods, such as study casts, clinical examination, and intraoral photographs, have limited accuracy in detecting early or minor wear changes. In contrast, digital intraoral scanning enables precise three-dimensional quantitative analysis of wear allowing for reliable longitudinal comparisons [14].
Therefore, the aim of the present study was to assess the clinical performance and wear behavior of LS-GRC versus nanohybrid composite in proximal restorations. The null hypothesis tested was that there would be no difference between the two tested materials after one year in proximal restorations of posterior teeth.
Materials and methods
Study settings, trial registration, ethical approval and trial design
The current randomized clinical trial was held in the Faculty of Dentistry, Cairo University, Egypt. All procedures performed in this study, involving human participants, were in accordance with the principles of the Declaration of Helsinki in 2013 and the ethical standards of Research Ethics Committee of Faculty of Dentistry, Cairo University (REC), (Approval no. 8-7-23). The present clinical trial was registered in (www.clinicaltrials.gov) under registration I.D (NCT05949502) at 24-06-2023. The trial design was double-blind, randomized clinical trial (RCT) in parallel arm design. The trial framework was superiority frame with an allocation ratio of 1:1. The present trial was reported according to CONSORT (Consolidated Standards of Reporting Trials) 2025 guidelines [15].
Sample size collection
The sample size was calculated based on a previous study [16] in which success rate of nanohybrid composites in proximal posterior restorations was 100%. A two-tailed Z test for the difference between two independent proportions was applied, with an alpha level of 5% and a power of 80%. In order to detect a difference of 30%, the required sample size was calculated as 22 per group. To compensate for possible dropouts, sample size was raised by 15% to reach 25, with a total of 50 participants. The sample size calculation was performed using G*Power software (version 3.1.9.2 for Windows).
Eligibility criteria
Participants ranging from 19 to 30 years, with good oral hygiene, stable occlusion, healthy periodontium, compliance and could be present for further periodic follow-ups were included. Vital first and second molars or premolars with moderately sized compound class II lesions involving 2/3 of the dentin thickness (Si/Sta 2.2) were included. The selected teeth were in occlusal contact with natural dentition and exhibiting proximal contact with the adjacent teeth.
On the other hand, patients with poor oral hygiene, heavy occlusal stresses, heavy smokers, patients with xerostomia, or participating in another clinical trial were excluded from the study. The exclusion criteria of teeth were fracture, evidence of crack, periapical pathosis and teeth adjacent or opposing to defective restorations.
Recruitment
Participants were recruited from the diagnostic center, Faculty of Dentistry, Cairo University between 15/07/2023 and 30/09/2023 according to the eligibility criteria using convenient consecutive sampling till the required sample size was fulfilled. All participants in the trial approved and signed the written informed consent after acceptance to participate.
Randomization, allocation concealment, and blinding
Allocation sequence was determined using simple randomization through generating random allocation sequence using (https://www.random.org). Sequence was created by generating random numbers from 1 to 50 into two columns. Participants were randomly allocated according to the assigned group. Each participant selected a random number from a sealed, opaque envelope [17]. Participants and outcome assessors were blinded to the materials’ assignment, while difference in the application protocol prohibited blinding of the operator.
Participants’ preparation
Before any restorative procedures, the selected teeth were polished, followed by preoperative occlusal assessment, periapical and bitewing radiographs, and vitality testing using a pulp vitality tester (Parkell Pulp Vitality Tester, Parkell Electronics DN, Farmingdale, NY, USA).
Field isolation and cavity preparation procedures
Local anesthesia was administrated prior to cavity preparation using Artpharmadent 1:100,000 (Artpharma, Egypt). All restorative procedures were done in a multiple isolation technique using rubber dam (Sanctuary Dental Dam, Sanctuary Health Sdn Bhd, Perak, Malaysia) with suitable clamps (KSK Clamps, Dentech Corporation, Tokyo, Japan) [18]. Cavities were prepared using sterile #330 and #245 carbide burs (Mani Inc., Tochigi, Japan) running at high speed (380,000–450,000 rpm) under profuse coolant, burs were discarded after five cavities [19]. Caries was removed according to the International Caries Consensus Collaboration (ICCC) [20]. Soft caries was excavated by a small, sharp excavator (Dentsply® Maillefer, Ballaigues, Switzerland) till reaching a firm dentin. Enamel walls were finished after cavity preparation using high-speed, yellow-coded diamond stone (Dia-burs, Mani Inc., Tochigi, Japan).
A sectional matrix system (Composi-Tight 3D Fusion Sectional Matrix System, Garrison Dental Solutions, Spring Lake, Michigan, USA) was used to restore the proximal wall. The sectional matrix size was chosen according to the size of the prepared cavity, then a wedge was chosen and placed according to the size of the cervical embrasure. Further, a suitable-sized ring was placed over them using the ring placement forceps [21].
Interventions
All materials used in the study were placed in accordance with the manufacturers’ instructions (Table 1). Selective etching technique (Scotchbond Universal Etchant, 3M ESPE, Germany) was applied using a 35% phosphoric acid gel on the enamel margins surrounding the whole cavity for 15 s followed by rinsing for 15 s and air drying using a water/oil-free air for 5 s. The excess moisture was blot dried using a moist cotton pellet [22].
Low-shrinkage giomer
Universal adhesive (BeautiBond Xtreme, Shofu, Japan) was applied to the cavity walls for 10 s, gently air-blown with water/oil-free air for 3 s until the surface appeared glossy, then photopolymerized for 10 s using LED light curing unit (LED F, Woodpecker Medical Instrument Co., Ltd, Guangdong, China) with an output of 1600–1800 mW/cm2 [23]. The output was checked regularly using radiometer between participants. Flowable composite (Beautifil Flow Plus X F03, Shofu Inc, Kyoto, Japan) was applied on the gingival seat as a first increment followed by low-shrinkage bioactive giomer material (Beautifil II LS, Shofu Inc, Kyoto, Japan) by snow-plow technique [24]. Centripetal technique was performed to restore the proximal wall followed by oblique incrementation of ~2 mm thick composite resin on each cusp using a gold-plated applicator (Nordent Manufacturing Inc. Illinois, USA). This was followed by light curing for 20 s of each increment till the whole cavity is filled [25].
Nanohybrid composite
A single layer from the adhesive (Single Bond Universal, 3M ESPE, Germany) was actively agitated for 20 s on the entire cavity, then gently air-blown with water/oil-free air for 5 s till reaching a glossy surface that cannot be visibly moved under further air pressure [26]. The adhesive was light-cured for 10 s using LED light-curing unit. Nano-hybrid flowable composite (Filtek™ Supreme XTE Flow, 3M ESPE, St. Paul, MN, USA) was applied on the gingival seat as a first increment followed by application of nano-hybrid universal composite (Filtek Z250XT, 3M ESPE, St. Paul, MN, USA) by snow-plow technique [24]. The proximal wall was restored first by centripetal technique followed by oblique incrementation of ~2 mm thick composite resin according to the manufacturer instructions [25]. Light curing was performed for 20 s on each cusp till the whole cavity was filled.
Finishing and polishing
Restorations were finished by a yellow-coded flame stone (Dia-burs, Mani Inc., Tochigi, Japan) rotating at high-speed under water coolant. Occlusion was checked and adjusted using a double sided, 35 microns, articulating paper (Accufilm II, Parkell Inc., New York, USA). Fine and super-fine diamond points were used for removal of excess composite flashes. Polishing was performed using pre-impregnated rubber cups under intermittent water spray (OneGloss PS, Shofu Dental Corportation, California, USA) [27, 28].
Outcome assessment
Clinical assessment
The primary outcome of this study was clinical performance of the restorations using revised FDI criteria, while the secondary outcome was measuring the restoration wear quantitatively using digital intra-oral scanner and 3D inspection software (Geomagic Control X, 3D Systems, Rock Hill, SC, USA) [14, 29].
The revised FDI criteria was used to evaluate the quality of the restorations over time through a set of standardized criteria covering functional parameters (fracture and retention (F1), marginal adaptation (F2), proximal contact (F3), form and contour (F4), occlusion and wear (F5)); biological parameters (caries at the restoration margin (B1), dental hard tissue defects at restoration margin (B2), and postoperative hypersensitivity (B3)), and esthetic parameters (surface luster and texture (A1), marginal staining (A2), and color matching (A3)). Restorations were rated on a five-point scale ranging from excellent (1) to poor (5). Scores between 1 and 3 were considered clinically acceptable, a score of 4 indicated an unacceptable restoration that could be repaired, and a score of 5 denoted an unacceptable restoration where repair was not feasible [29].
Each restoration was assessed by two experienced blinded assessors with more than 15 years of expertise in restorative dentistry. The evaluators were trained and calibrated prior to evaluation on using the revised FDI criteria for assessment of clinical performance. Assessments were performed at baseline, 6- and 12-month follow-up. Any discrepancies between examiners were resolved through discussion to reach a consensus. Figure 1 shows a representative case using LS-GRC for all procedural steps and follow-up assessments.

A Pre-operative view of tooth 46, B after cavity preparation, C After matrix placement and building the proximal wall, D Immediately after placement of low-shrinkage Giomer resin composite, E Follow-up periods after 6 months, F After 12 months.
Wear assessment (quantitative analysis)
For each case, baseline records and records after 1 year were obtained using CEREC Omnicam® digital intraoral scanner (Dentsply Sirona, York, Pennsylvania, USA). Data were exported into standard tessellation language (STL) format, then introduced to Geomagic Control X software (3D Systems, Rock Hill, SC, USA). The two scans were superimposed using “initial alignment” then “best-fit alignment” process. Root mean square (RMS) values were then calculated using “3D-compare” method, this was followed by comparison at different surface points (buccal, palatal, central, marginal ridge) between the reference baseline record and after one year providing a colored map with a deviation of ±0.01 mm. The green areas denoted superior matching, while the red to yellow areas indicated positive positioning of the follow-up to the baseline, light to dark blue areas donated negative positioning of the follow-up to the baseline [30]. The root mean square (RMS) values were calculated as \({RMS}=\frac{1}{\sqrt{n}}\sqrt{{\sum }_{i=1}^{n}\left({x}_{1},i-{x}_{2},i\right)\,2.}\) [14, 31] (Fig. 2).

A Baseline intra-oral scan; B Intra-oral scan after one year; C Combined STL files using best-fit alignment method; D 3D compare method between the two scans; E Comparison at different points between the baseline and after one year.
Statistical analysis
Data analysis was conducted using MedCalc software version 22 (MedCalc Software Ltd, Ostend, Belgium). Categorical data were presented as frequencies and percentages. Intergroup comparisons were carried out using Chi-squared test (P ≤ 0.05), while intragroup comparisons within each intervention were performed using Cochran’s Q test with Bonferroni correction (P ≤ 0.016). Clinical effect size was assessed by calculating absolute risk reduction. Survival analysis was performed using Kaplan–Meier analysis followed by log-rank test. Wear data were analyzed using an independent t-test for intergroup comparison and paired t-test for intragroup comparisons (P ≤ 0.05).
Ethics approval and consent to participate
The study protocol was registered at clinicaltrials.gov under the identifier NCT05949502 (24-06-2023). Ethical approval was obtained from the Research Ethics Committee of the Faculty of Dentistry, Cairo University (approval ID: 8-7-23), in accordance with the principles outlined in the Declaration of Helsinki (2013).
Results
Demographic data
In the current study, 50 participants with proximal carious lesions were randomly assigned to the intervention and control arms (n = 25). After 12 months, all participants were assessed with 100% retention rate. The mean age of participants was 30.6 ± 5.56 years; 30.0 ± 5.02 years in the Beautifil II LS group and 31.2 ± 6.10 years in the Filtek Z250XT group. Gender distribution was comparable, with Beautifil II LS having 8 males (32%) and 17 females (68%), and Filtek Z250XT having 11 males (44%) and 14 females (56%).
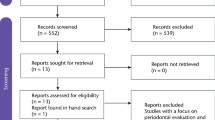
Regarding tooth type, Beautifil II LS restorations were placed in maxillary premolars (16%), maxillary molars (16%), mandibular premolars (36%), and mandibular molars (32%), while Filtek Z250XT restorations were placed in maxillary premolars (36%), maxillary molars (20%), mandibular premolars (8%), and mandibular molars (36%). There were no statistically significant differences between both groups for age, gender, or tooth distribution (P > 0.05) (Table 2). Figure 3 shows the Consort 2025 flow diagram of participants and teeth in the current trial [15].

CONSORT 2025 flow diagram.
Assessment of clinical performance
After 12 months, both Beautifil II LS and Filtek Z250XT exhibited high clinical success rates. Beautifil II LS group showed 100% success rate, whereas one restoration in the Filtek Z250XT group failed, scoring 5 in fracture of material and retention (F2), resulting in a 96% success rate, Log-rank test showed no statistically significant difference between both materials (P = 0.3173) (Fig. 4). Beautifil II LS restorations had a 4% lower risk of failure compared to Filtek Z250XT (ARR = 4.0 (95% CI −12.6 to 19.5, P > 0.05)). Minor deviations from ideal scores were observed in the Beautifil II LS group, where four restorations scored 2; two for postoperative hypersensitivity (B3) and two for fracture and retention (F1). In the Filtek Z250XT group, six restorations scored 2 across multiple criteria, including surface luster (A1), marginal staining (A2), color match (A3), marginal adaptation (F2), proximal contact (F3), form and contour (F4), and occlusion/wear (F5) (Fig. 5). Overall, both materials demonstrated excellent clinical performance over the 12-month period, with no significant difference for all assessed criteria (P > 0.05) (Table 3).

Survival analysis of both materials in proximal restorations at 12 months.

A Material chipping (F1) score 2 (Beautifil II LS group), B Slight loss of surface luster (A1) score 2 (Filtek Z250XT group), C Minor marginal staining detectable after air drying (A2) score 2 (Filtek Z250XT group).
Assessment of wear
The mean wear after 12 months was 0.036 ± 0.01 mm for Beautifil II LS and 0.038 ± 0.01 mm for Filtek Z250XT. The difference between groups was minimal (0.0026 mm; 95% CI: –0.0271 to 0.0324) and not statistically significant (P = 0.8178).
Discussion
The continuous modifications and changes in composite formulations by dental manufacturers have resulted in an expanded range of restorative materials with favorable long-term clinical performance [32]. The clinical use of fluoride-releasing adhesive restorative materials has risen significantly. These materials include giomer, which is valued for successfully integrating the protective advantages of conventional glass ionomers with the desirable characteristics of resin composites [8]. Giomer materials utilize S-PRG (Surface Pre-Reacted Glass ionomer) fillers that are notable for releasing multiple types of ions, such as F-, Al3+, BO3 3-, Na+, SiO3 2, and Sr2+ ions which are beneficial for remineralization and by acting as a pH modulator; they help to neutralize the acidity in the surrounding oral environment following an acid attack [7]. Previous studies have evaluated the clinical performance of giomer compared to other restorative materials [11, 33, 34], yet no studies evaluated the clinical performance alongside assessment of quantitative amount of wear.
Wear resistance is an essential property of dental restorative materials, as restorations should ideally exhibit wear behavior comparable to natural teeth to maintain long-term occlusal stability [13]. Although natural teeth show relatively low annual occlusal wear, resin composites demonstrate higher wear rates, particularly during the first five years after placement, which may be related to the composite material itself, or patient-related factors and evaluation methods [35]. Quantitative assessment of occlusal wear is considered a sensitive method for evaluation of wear resistance of composite restorations [14]. Digital scanning followed by analysis software has been widely employed in previous studies effectively for recording the amount of occlusal wear objectively, therefore eliminating issues with physical storage of measurement indices [36].
According to the manufacturer instructions, adhesives and restorative materials from the same manufacturer were used as these systems are chemically designed and validated to function synergistically as a restorative system, thereby producing more stable bond strength by minimizing the risk of cross-incompatibility [37]. In the present study, both systems were applied in selective enamel etching technique to ensure optimal adhesion between tooth structure and the resin composite [22]. The presence of functional monomer (10-MDP phosphate monomer) in the single bond universal offers stable calcium salts with hydroxyapatite contributing to a more durable chemical bond with the tooth structure [26]. While carboxylic and phosphonic acid monomers in BeautiBond Xtreme promote strong chemical bond with tooth structure, enhancing resistance to hydrolytic degradation and contributing to long-term stability of the adhesive interface [23].
According to the results of the current study, the two materials exhibited similar acceptable clinical outcomes when evaluated for their biological compatibility, functional performance, and aesthetic appearance. These results were in accordance with recent literature, which has shown that fluoride-releasing composites and traditional resin composites exhibit comparable mechanical, biological and esthetic properties, consequently, the null hypothesis could not be rejected [12, 38]. Regarding functional properties, four restorations in the Beautifil II LS group, scored 2 for fracture and retention (F1), while in Filtek Z250XT group, one restoration scored 5 for fracture and retention exhibiting complete loss of the restoration due to adhesive failure. This failure may be attributed to the thickness of the adhesive layer during bonding procedure. Previous literature [39] denoted that excessive thinning of the adhesive layer exceeding the thickness of the oxygen-inhibited layer may result in compromising the hybrid layer formation, thereby reducing the mechanical integrity of the bonding interface and potentially impairing its long-term stability. In addition, six restorations scored 2 for marginal adaptation (F2), proximal contact (F3), form and contour (F4), and occlusion/wear (F5). According to Toz Alkin et al. [40], the minor deviation from ideal scores over time could be related to several factors such as technique sensitivity during application of the adhesive systems, the clinical expertise of the clinicians, and adhesive system-related factors.
Regarding esthetic properties, six restorations of Filtek Z250XT group scored 2 for surface luster (A1), marginal staining (A2), and color match (A3). These results were consistent with a recent systematic review [41], who reported minor changes in surface texture and staining of some nanohybrid restorations after finishing and polishing. These changes might be attributed to the exfoliation of larger filler particles from the resin matrix during polishing. Additionally, the hydrophilic nature of the resinous material might lead to noticeable color change [42]. Another study reported that voids may be entrapped during the incremental layering technique, thereby affecting surface texture. This problem is considered crucial since rougher surfaces would cause surface staining; therefore, increasing plaque retention and bacterial adhesion [43]. However, according to FDI criteria score 2 is considered clinically good, so these six restorations were considered successful [29, 44].
Regarding biological properties, four restorations in the Beautifil II LS group scored 2 for postoperative sensitivity (B3) indicating minor postoperative pain upon chewing one week after placement of the restorations. Although LS-GRC exhibits low tendency for volumetric shrinkage, attributed to its unique Steric Repulsion Structured (SRS) molecule, which limits shrinkage to a considerable level [10], some unrelieved stresses upon polymerization might have led to this outcome, subsequently leading to gap formation at the margins and postoperative sensitivity [12]. Another assumption by previous research linked the post-operative sensitivity of resin composite restorations to the technique sensitivity associated with the adhesion procedures [39]. According to literature, significant concerns have been raised regarding the interfacial aging associated with degradation of the adhesive interface over time [45]. On the other hand, secondary caries at the restoration margins was not reported in any of the restorations of Beautifil II LS group, aligning with a previous study [46] correlating the ability of S-PRG fillers to create an acid-resistant surface layer with the reduction in plaque accumulation and bacterial adhesion on the surface of the composite restorations. Additionally, the S-PRG fillers act as rechargeable fluoride reservoirs when exposed to fluoride toothpaste or mouth rinses, leading to continuation of the fluoride re-release process [7, 47].
Regarding quantitative wear, the mean occlusal wear after 12 months was 0.036 ± 0.01 mm for Beautifil II LS and 0.038 ± 0.01 mm for Filtek Z250XT. The difference between groups was minimal and not statistically significant (P = 0.8178) indicating comparable wear resistance for both materials. A previous study [48] reported that the annual enamel wear rate is ranging from 0.015 mm for premolars and 0.029 mm for molars. Another study [13] reported an annual vertical enamel loss ~0.02–0.04 mm under physiological conditions, these wear rates suggested normal physiological wear of both restorative materials over one year when compared to enamel. Filtek Z250XT showed a non-significant higher wear rate compared to Beautiful II LS, this may be correlated with the deterioration detected during clinical assessment using FDI criteria [49].
According to literature, the abrasive wear of composite resin material is influenced by multiple factors, including the size, shape, concentration, orientation, and distribution of filler particles. These factors are further modulated by masticatory forces acting on the composite, rendering the wear process highly complex [50]. Further studies have found that the abrasive wear of resin composites is minimized when filler particle size and interparticle spacing are reduced; therefore, enhancing the degree of resin polymerization and increasing the filler–matrix bond strength [51]. Both restorative materials in the current study demonstrated mean particle size of 0.02 µm and 0.4 µm for Filtek Z250XT and Beautifil II LS, respectively, which may have contributed to minimal occlusal wear over time [10, 52].
Overall, both materials demonstrated excellent clinical performance over 12-month period, with no significant difference for all assessed criteria (P > 0.05). According to American Dental Association (ADA) standards, adhesive restorations are considered fully acceptable only when clinical failures, including loss of restorations and microleakage, remain below 10 percent after an 18-month period, therefore both restorative materials were considered clinically acceptable after 12 months [53, 54]. These findings were in agreement with earlier research [38], they evaluated giomer resin composites in various cavity types over a follow-up period of 1–13 years and reported acceptable clinical outcomes and overall comparable morphological, functional, and mechanical performance of giomers to conventional resin composites. Further studies evaluating the performance of giomer composite material in different cavities also reported satisfactory outcomes over significant follow-up periods [33, 55].
To the best of our knowledge, this is the first clinical trial to quantitatively assess the occlusal wear of low-shrinkage giomer resin composites over a 12-month period. However, it should be highlighted that the current trial did not involve large sample size, which may have constrained the external validity of the conclusions. Moreover, a one-year follow-up duration may not fully represent the long-term behavior of the restorative materials. Therefore, larger-scale trials with longer observation periods are necessary to confirm these results and evaluate the long-term performance. Nevertheless, it is advised to consider the cost effectiveness of each restorative material and its correlation with the long-term clinical success. Finally, further research comparing giomer resin composite with other restorative materials, especially in poor oral hygiene patients is also recommended.
Conclusion
Low-shrinkage giomer showed satisfactory clinical performance and wear resistance compared to nanohybrid resin composite after one year in proximal restorations of posterior teeth. Both materials are considered clinically acceptable as per the ADA standards.
Data availability
The data that supports the findings of this study are available from the corresponding author upon reasonable request.
References
Maran BM, de Geus JL, Gutierrez MF, Heintze S, Tardem C, Barceleiro MO, et al. Nanofilled/nanohybrid and hybrid resin-based composite in patients with direct restorations in posterior teeth: a systematic review and meta-analysis. J Dent. 2020;99:103407.
Angerame D, De Biasi M. Do nanofilled/nanohybrid composites allow for better clinical performance of direct restorations than traditional microhybrid composites? a systematic review. Oper Dent. 2018;43:E191–E209.
Ferracane JL. Resin composite - state of the art. Dent Mater. 2011;27:29–38.
Albelasy EH, Hamama HH, Chew HP, Montaser M, Mahmoud SH. Secondary caries and marginal adaptation of ion-releasing versus resin composite restorations: a systematic review and meta-analysis of randomized clinical trials. Sci Rep. 2022;12:19244.
Maghaireh GA, Taha NA, Alzraikat H. The silorane-based resin composites: a review. Oper Dent. 2017;42:E24–E34.
Dejak B, Młotkowski A. A comparison of stresses in molar teeth restored with inlays and direct restorations, including polymerization shrinkage of composite resin and tooth loading during mastication. Dent Mater. 2015;31:e77–e87.
Burtea LC, Prejmerean C, Prodan D, Baldea I, Vlassa M, Filip M, et al. New pre-reacted glass containing dental composites (giomers) with improved fluoride release and biocompatibility. Materials. 2019;12:1–20.
Rusnac ME, Gasparik C, Irimie AI, Grecu AG, Mesaroş AŞ, Dudea D. Giomers in dentistry - at the boundary between dental composites and glass-ionomers. Universitatea de Medicina si Farmacie Iuliu Hatieganu.2019;92:123-8
Thein S, Sunami A, Okkar K, Hatano K, Kanazawa M, Inokoshi M. Bioactivity and potential applications of surface pre-reacted glass-ionomer (S-PRG) filler-containing dental materials for geriatric oral health: a scoping review. Jpn Dent Sci Rev. 2025;61:280–91.
Shofu INC. Therapeutic Restoratives With Esthetic Results. https://www.shofu.com/wp-content/uploads/Article-US-Inside-Dentistry-Therapeutic-Restoratives-with-Esthetic-Results-E-Book.pdf 2022.
Toz-Akalin T, Öztürk-Bozkurt F, Kusdemir M, Özsoy A, Yüzbaşıoğlu E, Özcan M. Three-year clinical performance of direct restorations using low-shrinkage Giomer vs. nano-hybrid resin composite. Front Dent Med. 2024;5:1–11.
Ozer F, Patel R, Yip J, Yakymiv O, Saleh N, Blatz MB. Five-year clinical performance of two fluoride-releasing giomer resin materials in occlusal restorations. J Esthet Restor Dent. 2022;34:1213–20.
Dionysopoulos D, Gerasimidou O. Wear of contemporary dental composite resin restorations: a literature review. Restor Dent Endod. 2021;46:1–13.
Travassos da Rosa Moreira Bastos R, Teixeira da Silva P, Normando D. Reliability of qualitative occlusal tooth wear evaluation using an intraoral scanner: a pilot study. PLoS ONE. 2021;16:1–12.
Hopewell S, Chan AW, Collins GS, Hróbjartsson A, Moher D, Schulz KF, et al. CONSORT 2025 explanation and elaboration: updated guideline for reporting randomised trials. BMJ. 2025;389:1–61.
Gernhardt CR, Nguyen AD, Michaelis M, Pütz N. Clinical outcome of class I and II restorations with and without an intermediary layer of a flowable composite after 24 months: a prospective, randomized, split-mouth-designed, controlled and single-blinded clinical trial. Appl Sci. 2023;13:1–16.
Baghbaninaghadehi F, Armijo-Olivo S, Woodhouse L. Fundamentals of randomization in clinical trial. IJANHS. 2016;4:174–87.
Miao C, Yang X, Wong MCM, Zou J, Zhou X, Li C, et al. Rubber dam isolation for restorative treatment in dental patients. Cochrane Database Syst Rev. 2021:5:CD009858.
Albelasy EH, Chen R, Fok A, Montasser M, Hamama HH, Mahmoud SH, et al. Inhibition of caries around restoration by ion-releasing restorative materials: an in vitro optical coherence tomography and micro-computed tomography evaluation. Materials. 2023;16:1–20.
Schwendicke F, Frencken JE, Bjørndal L, Maltz M, Manton DJ, Ricketts D, et al. Managing carious lesions: consensus recommendations on carious tissue removal. Adv Dent Res. 2016;28:58–67.
Anantula K, Vankayala B, Yadav SS. Proximal contact tightness of direct Class II composite resin restorations with various matrix systems: a systematic review. J Conserv Dent Endod. 2024;27:11–6.
Pena CE, Rodrigues JA, Ely C, Giannini M, Reis AF. Two-year randomized clinical trial of self-etching adhesives and selective enamel etching. Oper Dent. 2016;41:249–57.
Raucci Neto W, Barbosa AFS, Baltazar AF, Pereira LF, Silva Sousa YTC, Messias DCF, et al. A randomized prospective clinical study evaluating the effectiveness of the Beautibond Xtreme adhesive system using different bonding techniques in class I and II restorations: one-year results. J Appl Oral Sci. 2025;33:1–15.
Gomaa MM, Mosallam RS, Abou-Auf EA, Hassanien OE. Clinical evaluation of “snowplow” technique versus bulk-fill technique in restoration of class II cavities: a randomized clinical trial. J Int Oral Health. 2024;16:158–65.
Bud M. The Interdental Contacts: Direct Restoration Techniques of the Proximal Walls by the Centripetal Method. In: Direct Restorations. Springer, Cham; 2024;179–228.
Carrilho E, Cardoso M, Ferreira MM, Marto CM, Paula A, Coelho AS. 10-MDP based dental adhesives: adhesive interface characterization and adhesive stability-a systematic review. Materials. 2019;12:1–18.
Celik C, Ozgünaltay G. Effect of finishing and polishing procedures on surface roughness of tooth-colored materials. Quintessence Int. 2009;40:783-9.
Molaei M, Mohammadzadeh A, Ghasemi A, Badiee M. Effect of dry and wet finishing and polishing on color change and opacity of nanofill and nanohybrid composites. BMC Oral Health. 2024;24:1–5.
Hickel R, Mesinger S, Opdam N, Loomans B, Frankenberger R, Cadenaro M, et al. Revised FDI criteria for evaluating direct and indirect dental restorations—recommendations for its clinical use, interpretation, and reporting. Clin Oral Invest. 2023;27:2573–592.
Taha D, Allam S, Morsi T. Accuracy of computer-aided design trial restorations fabricated with different digital workflows. J Prosthet Dent. 2024;132:578–85.
Wang F, Zhang T, Zhou Q, Lu Y. Comparison of the morphological accuracy of automatic crowns designed by multiple computer-aided design software programs with different levels of dentition information acquisition. J Prosthet Dent. 2024;132:441–52.
Abozaid D, Azab A, Bahnsawy MA, Eldebawy M, Ayad A, soomro R, et al. Bioactive restorative materials in dentistry: a comprehensive review of mechanisms, clinical applications, and future directions. Odontology. 2025;1–29.
Hendam R, Mosallam R, Kamal D. Clinical evaluation of giomer-based injectable resin composite versus resin-modified glass ionomer in class v carious lesions over 18 months: a randomized clinical trial. J Conserv Dent Endod. 2025;28:50–6.
Abdelwahed A, Abdelaziz M, Fahim S. Clinical evaluation of flowable versus packable bulk-fill giomer restorative materials: a two-year randomized clinical trial. Egypt Dent J. 2024;70:2094–105.
Liqun C, Xinyi Z, Xu G, Shouliang Z. An in vitro investigation of wear resistance and hardness of composite resins. Int J Clin Exp Med. 2013;6:423–30.
Hai-li MU, Fu-cong T, Xiao-yan W, Xue-jun GAO. Evaluation of wear property of Giomer and universal composite in vivo. J Peking Univ. 2020;53:120–5.
Sabatini C, Campillo M, Hoelz S, Davis EL, Munoz CA. Cross-compatibility of methacrylate-based resin composites and etch-and-rinse one-bottle adhesives. Oper Dent. 2012;37:37–44.
Gordan VV, Blaser PK, Watson RE, Mjör IA, McEdward DL, Sensi LG, et al. A clinical evaluation of a giomer restorative system containing surface prereacted glass ionomer filler: results from a 13-year recall examination. J Am Dent Assoc. 2014;145:1036–43.
Schulz-Kornas E, Tittel M, Schneider H, Bemmann M, Pellino M, Meissner T, et al. Tooth-composite bond failure with a universal and an etch-and-rinse adhesive depending on mode and frequency of application. Dent Mater. 2024;40:359–69.
Toz-Akalin T, Öztürk-Bozkurt F, Kusdemir M, Özsoy A, Yüzbaşıoğlu E, Özcan M. Clinical evaluation of low-shrinkage bioactive material giomer versus nanohybrid resin composite restorations: a two-year prospective controlled clinical trial. Oper Dent. 2023;48:10–20.
Sengupta A, Naka O, Mehta SB, Banerji S. The clinical performance of bulk-fill versus the incremental layered application of direct resin composite restorations: a systematic review. Evid-Based Dent. 2023;24:143.
SarialİOĞLu, GÜNgÖR, DÖNmez A, Kahya N, HergÜNer DS, SİSo Ş. Impact of a surface sealant application on the color stability of a nano-hybrid composite resin. Bezmialem Sci. 2022;10:219–25.
Yazici AR, Antonson SA, Kutuk ZB, Ergin E. Thirty-six-month clinical comparison of bulk fill and nanofill composite restorations. Oper Dent. 2017;42:478–85.
Marquillier T, Doméjean S, Le Clerc J, Chemla F, Gritsch K, Maurin JC, et al. The use of FDI criteria in clinical trials on direct dental restorations: a scoping review. J Dent. 2018;68:1–9.
Vinagre A, Ramos J, Marques F, Chambino A, Messias A, Mata A. Randomized clinical trial of five adhesive systems in occlusal restorations: one-year results. Dent Mater J. 2020;39:397–406.
Yamamoto S, Sayed M, Takahashi M, Matin K, Hiraishi N, Nikaido T, et al. Effects of a surface prereacted glass–ionomer filler coating material on biofilm formation and inhibition of dentin demineralization. Clin Oral Investig. 2021;25:683–90.
Shimazu K, Ogata K, Karibe H. Evaluation of the ion-releasing and recharging abilities of a resin-based fissure sealant containing S-PRG filler. Dent Mater J. 2011;30:923–7.
Lambrechts P, Braem M, Vuylsteke-Wauters M, Vanherle G. Quantitative in vivo wear of human enamel. J Dent Res. 1989;68:1752–4.
Guo J, Bing Z, Yang J, Tsoi JKH, Wang Y. Effect of roughness and acidic medium on wear behavior of dental resin composite. BMC Oral Health. 2022;22:1–11.
Han JM, Zhang H, Choe HS, Lin H, Zheng G, Hong G. Abrasive wear and surface roughness of contemporary dental composite resin. Dent Mater J. 2014;33:725–32.
Turssi CP, Ferracane JL, Vogel K. Filler features and their effects on wear and degree of conversion of particulate dental resin composites. Biomaterials. 2005;26:4932–7.
3M ESPE. Filtek™ Z250 XT Nano Hybrid Universal Restorative Technical Data Sheet. https://multimedia.3m.com/mws/media/2130487O/3m-filtek-z250xt-universal-restorative.pdf 2021;1–6.
Dhar V, Pilcher L, Fontana M, González-Cabezas C, Keels MA, Mascarenhas AK, et al. Evidence-based clinical practice guideline on restorative treatments for caries lesions: a report from the American Dental Association. J Am Dent Assoc. 2023;154:551–66.e51.
Dawoud B, Abou-Auf E, Shaalan O. 24-Month clinical evaluation of cervical restorations bonded using radio-opaque universal adhesive compared to conventional universal adhesive in carious cervical lesions: a randomized clinical trial. Sci Rep. 2025;15:5505.
El Ghamrawy M, Kamal D, Hamza H. Clinical performance and cost-effectiveness of low-shrinkage giomer resin composite versus resin-modified glass ionomer in cervical carious lesions: a 12-month randomized controlled trial. BMC Oral Health. 2025;25:1–17.
Funding
The authors received no financial support for the current research. Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB).
Author information
Authors and Affiliations
Contributions
MA: Conceptualization, study design, definition of intellectual content, operative procedures, literature review, data collection, and manuscript drafting, editing, and revision. OS: Conceptualization, study design, definition of intellectual content, sample size determination, literature review, data collection, data analysis, statistical analysis, auditing, and manuscript drafting, editing, and revision. HH: Conceptualization, study design, definition of intellectual content, literature review, data collection, principal investigator duties, auditing, and manuscript drafting, editing, and revision.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
AbdelHafez, M.I., Shaalan, O. & Hamza, H. Clinical performance of low-shrinkage giomer compared to nanohybrid resin composite in proximal restorations after one year: a randomized clinical trial. BDJ Open 12, 36 (2026). https://doi.org/10.1038/s41405-026-00423-2
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41405-026-00423-2
