
Abstract
In the primary analysis (32.3-month median follow-up) of the randomized, phase 3 AURIGA study (NCT03901963), daratumumab-lenalidomide (D-R) maintenance significantly improved MRD-negative conversion rates and reduced the risk of disease progression or death by 47% versus R maintenance in anti-CD38 monoclonal antibody–naïve and post-transplant MRD-positive patients with newly diagnosed MM. Here, we present a post hoc analysis across relevant subgroups, including high-risk cytogenetic abnormalities (HRCAs) per original, revised, and modified International Myeloma Society (IMS) 2024 criteria. MRD-negative (10−5) conversion rates by 12 months of maintenance were higher for D-R versus R across cytogenetically high-risk subgroups per original (31.8% vs 6.7%), revised (43.8% vs 13.3%), and modified IMS 2024 (41.2% vs 0%) criteria and cytogenetically ultra-high–risk disease (≥2 revised HRCAs; 54.5% vs 0%). Similar trends in overall MRD-negative conversion rates were observed across subgroups. D-R demonstrated a trend towards improved PFS versus R (HR [95% CI]) in cytogenetically high-risk subgroups per original (0.60 [0.21–1.70]), revised (0.53 [0.21–1.31]), and modified IMS 2024 (0.45 [0.13–1.53]) criteria and cytogenetically ultra-high–risk disease (0.61 [0.17–2.25]). Similar outcomes were observed regardless of age or race, with no additional safety concerns among older (≥65 years) or Black patients. These data support the benefit of D-R maintenance regardless of age, race, and risk status.

Similar content being viewed by others

Introduction
Daratumumab is a human IgGκ monoclonal antibody (mAb) targeting CD38 with direct on-tumor [1,2,3,4] and immunomodulatory [5,6,7] mechanisms of action. Due to its favorable clinical benefit [8,9,10,11,12,13], daratumumab is approved as monotherapy for patients with relapsed/refractory multiple myeloma (MM) and in combination with standard-of-care regimens for patients with relapsed/refractory or newly diagnosed MM (NDMM) [14, 15]. Moreover, daratumumab is the first anti-CD38 mAb to exhibit clinical benefit among transplant-eligible [9, 16], non-transplant [17], and transplant-ineligible patients with NDMM [8, 10] across multiple phases of therapy, including induction/consolidation and maintenance.
The randomized phase 3 AURIGA study (ClinicalTrials.gov Identifier, NCT03901963) was the first study designed to evaluate the addition of subcutaneous (SC) daratumumab to lenalidomide (D-R) maintenance in transplant-eligible patients with NDMM who were anti-CD38 mAb naïve, minimal residual disease (MRD) positive, and had achieved very good partial response or better (≥VGPR) after autologous stem cell transplant (ASCT) [18]. In the primary analysis of AURIGA (median follow-up, 32.3 months), D-R maintenance resulted in a significant increase in the MRD-negative (10–5) conversion rate by 12 months of maintenance versus lenalidomide (R) alone (50.5% vs 18.8%, respectively; odds ratio, 4.51 [95% confidence interval (CI), 2.37–8.57]; P < 0.0001) and a 47% reduction in the risk of disease progression or death (hazard ratio [HR], 0.53 [95% CI, 0.29–0.97]; P = 0.0361) [18].
Despite rapid advancements in the treatment of NDMM, certain patient and disease characteristics predict poor prognosis [19], including ethnicity, age, and the presence of high-risk cytogenetic abnormalities (HRCAs) [20]. For several decades, high-risk cytogenetics have been defined based upon the presence of t(4;14), t(14;16), and/or del(17p) [21]. Several years ago, this definition was revised to also include the presence of t(14;20) and/or gain/amp(1q21) as HRCAs [22]. With continued advancement in cytogenetic assessment methodologies and increased availability of clinical trial data in patients with specific HRCAs, an updated consensus definition of high-risk MM was recently presented at the 2024 International Myeloma Society (IMS) Annual Meeting, stating the single occurrence of either del(17p) with 20% of cells positive, TP53 mutation, or biallelic del(1p32) is sufficient to meet the criteria for high-risk disease [23, 24]. Co-occurrence of monoallelic del(1p32) with gain/amp(1q21) and co-occurrence of t(4;14), t(14;16), and/or t(14;20) with gain/amp(1q21) and/or monoallelic del(1p32) are also considered high-risk disease, as well as the combination of high beta-2-microglobulin (ß2M; >5.5 mg/dL) with normal creatinine (<1.2 mg/dL) [23, 24].
Clinical studies are crucial to determine the efficacy of varying treatment strategies in patients with commonly defined and newly emerging high-risk characteristics. Given that the IMS 2024 high-risk MM definition was presented very recently, few studies have reported on the clinical outcomes of patients with these specific risk factors. Therefore, we present a post hoc analysis of several clinically relevant subgroups from AURIGA, including older adults, Black patients, patients with high-risk disease per International Staging System (ISS), and patients with cytogenetically high-risk disease per the original, revised, and the recent IMS 2024 criteria (slightly modified based on data availability).
Methods
Patients and study design
The detailed design of the multicenter, randomized, open-label, active-controlled, phase 3 AURIGA study has been previously reported [18]. The study protocol and all amendments were approved by the institutional review board or independent ethics committee at each site, a listing of which can be found in the Supplementary Appendix. The study adhered to the International Council for Harmonisation’s good clinical practice guidelines and the principles of the Declaration of Helsinki, complying with all relevant regulatory and country-specific requirements. Written informed consent was obtained from all patients. The full protocol and analysis plan can be accessed at ClinicalTrials.gov.
Briefly, the study enrolled patients from 52 sites across the United States and Canada who were aged 18–79 years, had NDMM with ≥4 prior cycles of induction therapy, had received high-dose therapy and ASCT within 12 months of the start of induction, were randomized within 6 months of ASCT, were anti-CD38 mAb naïve, were MRD positive (10–5 by next-generation sequencing; Adaptive Biotechnologies), had achieved ≥VGPR (per International Myeloma Working Group [IMWG] 2016 criteria) post-ASCT [25], and had an Eastern Cooperative Oncology Group performance status of 0–2. Eligible patients were randomized 1:1 via an interactive web response system to receive D-R or R maintenance after stratification by cytogenetic risk per investigator’s assessment (standard risk/unknown vs high risk), as assessed by fluorescence in situ hybridization/karyotype testing, with high risk defined as the presence of ≥1 of the following HRCAs: del(17p), t(4;14), and/or t(14;16).
All patients received 10 mg of R daily on Days 1–28 of each 28-day cycle, potentially increasing to a dose of 15 mg after 3 cycles if tolerated and per investigator discretion. Patients randomized to the D-R group also received daratumumab SC (1800 mg daratumumab co-formulated with recombinant human hyaluronidase PH20 [2000 U/mL; ENHANZE® drug delivery technology; Halozyme, Inc.]) weekly during Cycles 1 and 2, every 2 weeks during Cycles 3–6, and every 4 weeks from Cycle 7 thereafter. Treatment continued for a planned maximum duration of 36 cycles or until disease progression, unacceptably toxicity, or consent withdrawal.
Subgroups
This post hoc analysis included the intent-to-treat (ITT) population, defined as all patients who were randomized to the study treatment. Patients were categorized into the following patient subgroups: race (Black or White), age (<65 years or ≥65 years), ISS disease stage at diagnosis (I, II, or III), baseline response status at study entry (VGPR or complete response or better [≥CR]), cytogenetic risk per original definition (del[17p], t[4;14], and/or t[14;16]), cytogenetic risk per revised definition (t[4;14], t[14;16], t[14;20], del[17p], and/or gain/amp[1q21]), number of HRCAs (0, 1, or, ≥2 per the revised definition), gain/amp(1q21), isolated gain/amp(1q21), and risk per modified IMS 2024 criteria. In AURIGA, data were not collected on TP53 mutation, differentiation between monoallelic versus biallelic del(1p32), or ß2M and creatinine levels at the time of MM diagnosis; hence, the IMS 2024 high-risk definition was modified to the following: ≥20% del(17p); del(1p32) co-occurring with gain/amp(1q21); and t(4;14), (14;16), and/or (14;20) co-occurring with gain/amp(1q21) and/or del(1p32). Risk assessment used mutation data collected at diagnosis and was based on local laboratory results. Subgroup definitions can be found in Supplementary Table 1.
Endpoints and assessments
The primary endpoint of AURIGA was MRD-negative conversion rate from baseline to 12 months of maintenance, defined as the proportion of patients who converted to MRD-negative status (10–5) by 12 months after the initiation of maintenance treatment and prior to progressive disease or initiation of subsequent antimyeloma therapy, and has been previously published [18]. Endpoints explored in this post hoc analysis of clinically relevant subgroups include MRD-negative conversion rate (10–5) by 12 months of maintenance, overall MRD-negative conversion rate, ≥CR rate, and progression-free survival (PFS).
Per protocol, MRD was assessed by next-generation sequencing of bone marrow aspirate samples by central laboratory (clonoSEQ®; Adaptive Biotechnologies) at a minimum sensitivity threshold of 10–5. Bone marrow samples were collected at screening and after 12, 18, 24, and 36 months of maintenance within an accepted ± 30-day window of the scheduled visit. Response and disease progression were assessed with a validated computerized algorithm in accordance with IMWG 2016 response criteria [25].
Statistical analysis
This post hoc analysis was conducted at the time of the primary analysis, which was conducted after all randomized patients had completed 12 months of maintenance, had disease progression, died, or discontinued study treatment. Sample size justification and additional statistical methods have been previously described [18] and are available at ClinicalTrials.gov.
The MRD-negative conversion rate by 12 months of study treatment and the overall MRD-negative conversion rate were evaluated between treatment groups using the Mantel-Haenszel estimate of the common odds ratio for stratified (ITT population) and unstratified tables (subgroups), with 2-sided 95% CIs. PFS was assessed using the Kaplan-Meier method, with HRs and 95% CIs calculated from a Cox proportional hazards model and treatment as the sole explanatory variable.
Results
Patients and treatment
A total of 200 patients were enrolled and randomized to receive either D-R (n = 99) or R (n = 101) maintenance. Summary of treatment disposition has been previously published [18]. Baseline demographic and disease characteristics were generally well balanced across treatment groups and have been previously published [18]; 22% of patients were Black (Supplementary Table 2). An imbalance between treatment groups in the original high-risk cytogenetic criteria (D-R, n = 22; R, n = 15) was observed, primarily due to a higher number of D-R patients having del(17p). This was driven by investigators mixing cytogenetic risk assessments at the time of randomization with assessments made based on cytogenetic data either at screening or MM diagnosis. Per the revised high-risk cytogenetic criteria, the 2 treatment groups had a similar number of patients with 1 HRCA (D-R, n = 21; R, n = 20) and ≥2 HRCAs (n = 11; n = 10), with a slight imbalance noted for isolated gain/amp(1q21) (n = 10; n = 15). For modified IMS 2024 high-risk criteria, an imbalance was observed between treatment groups, with a higher number of patients having high-risk disease in the D-R group (D-R, n = 17; R, n = 8), primarily due to the higher frequency of del(17p) (≥20% of cells positive; n = 10; n = 2), as well as an imbalance in the co-occurrence of del(1p32) with gain/amp(1q21) (n = 4; n = 0).
Subgroup analysis of MRD-negative (10–5) conversion rate
At the time of this analysis, D-R improved MRD-negative (10–5) conversion rate by 12 months of maintenance (primary endpoint) versus R across all subgroups explored, suggesting a benefit with D-R regardless of race and age (Fig. 1). D-R was also associated with higher rates of MRD-negative (10–5) conversion by 12 months of maintenance across all definitions of cytogenetically high-risk disease, including per original (D-R, 31.8% [7/22]; R, 6.7% [1/15]), revised (43.8% [14/32]; 13.3% [4/30]), and modified IMS 2024 (41.2% [7/17]; 0% [0/8]) criteria. Of emphasis, among the modified IMS 2024 high-risk subgroups, no MRD-negative conversions were observed in the R group, whereas MRD-negative conversion rates for these subgroups ranged from 20%–75% with D-R. No patient with cytogenetically ultra-high–risk disease (≥2 revised HRCAs) in the R group achieved MRD-negative (10–5) conversion, whereas 54.5% (6/11) of patients in the D-R group achieved MRD-negative (10–5) conversion in this difficult-to-treat population.

MRD minimal residual disease, D-R daratumumab/lenalidomide, R lenalidomide, CI confidence interval, ITT intent-to-treat, ISS International Staging System, VGPR very good partial response, CR complete response, HRCA high-risk cytogenetic abnormality, NE not estimable, IMS International Myeloma Society. aDefined as the proportion of patients who were MRD positive at baseline and achieved MRD-negative status (at 10–5) by next-generation sequencing by 12 months after maintenance treatment and prior to progressive disease or subsequent antimyeloma therapy. bMantel-Haenszel estimate of the common odds ratio for stratified tables was used for the ITT population; Mantel-Haenszel estimate of the common odds ratio for unstratified tables was used for subgroups. An odds ratio >1 indicates an advantage for D-R maintenance. cITT population is defined as all patients who were randomized to treatment. dResponse status upon entering the study as assessed by International Myeloma Working Group 2016 criteria. eHigh-risk cytogenetics per the original definition are defined as ≥1 abnormality including del(17p), t(4;14), and/or t(14;16). fRevised high-risk cytogenetics per the revised definition are defined as ≥1 abnormality including del(17p), t(4;14), t(14;16), t(14;20), and/or gain/amp(1q21). gNot evaluable because no patient in the R group had MRD-negative conversion. hHigh risk per the modified IMS 2024 criteria is defined as the presence of ≥20% del(17p); del(1p32) co-occurring with gain/amp(1q21); or t(4;14), t(14;16), and/or t(14;20) co-occurring with gain/amp(1q21) and/or del(1p32). In the AURIGA study, data were not available on TP53 mutations, beta-2-microglobulin and creatinine levels at the time of multiple myeloma diagnosis, and differentiation between monoallelic versus biallelic del(1p32).
D-R maintenance was also associated with higher rates of overall (any time point in study after randomization) MRD-negative (10–5) conversion versus R maintenance across all subgroups, including those with ≥2 HRCAs (D-R, 63.6% [7/11]; R, 0% [0/10]) and in the modified IMS 2024 high-risk subgroups (D-R, 40%–75%; R, 0%; Supplementary Fig. 1).
Subgroup analysis of CR rate
In an analysis of best response on study, or the achievement of ≥CR rate while on study treatment, treatment with D-R maintenance demonstrated a trend towards improvement of study entry response versus R maintenance across the majority of subgroups (Supplementary Fig. 2). This trend was also maintained among patients with various definitions of cytogenetically high-risk disease, including per original (D-R, 81.8% [18/22]; R, 53.3% [8/15]), revised (87.5% [28/32]; 50.0% [15/30]), and modified IMS 2024 (76.5% [13/17]; 37.5% [3/8]) criteria. Among patients who were in VGPR at study entry, the addition of daratumumab led to a greater proportion of patients achieving ≥CR versus R maintenance alone (D-R, 66.2% [47/71]; R, 45.1% [32/71]).
Subgroup analysis of PFS
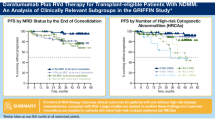
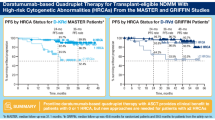
At a median follow-up of 32.3 months, PFS favored D-R versus R maintenance across all subgroups, suggesting a trend in PFS benefit with D-R regardless of age, race, disease stage, or various definitions of cytogenetic risk status (Supplementary Fig. 3). PFS HR point estimates were consistently <1 among patients with cytogenetically high-risk disease per the original (HR, 0.60 [95% CI, 0.21–1.70]; Fig. 2A) and revised (HR, 0.53 [95% CI, 0.21–1.31]) criteria (Fig. 2B), indicating a trend towards improvement with D-R versus R. In patients with cytogenetically high-risk disease per the original criteria, median PFS was not reached versus 16.7 months in the D-R and R groups, respectively; per the revised criteria, PFS was not reached in either group. When looking closely at patients with cytogenetically high-risk disease per modified IMS 2024 criteria, the PFS HR point estimate was even lower (HR, 0.45 [95% CI, 0.13–1.53]; Fig. 2C), with a median PFS of 32.8 and 16.7 months in the D-R and R groups, respectively, indicating that the favorable PFS trend with the addition of daratumumab SC further improved with more recent high-risk criteria. In addition, a PFS trend favoring D-R maintenance was observed versus R alone among patients with 0 HRCAs (HR, 0.69 [95% CI, 0.24–1.95]), 1 HRCA (HR, 0.36 [95% CI, 0.09–1.45]), and cytogenetically ultra-high–risk disease (≥2 HRCAs; HR, 0.61 [95% CI, 0.17–2.25]; Fig. 2D). In patients with gain/amp(1q21) irrespective of other HRCAs, the PFS HR point estimate indicated a trend towards improvement with D-R versus R alone (HR, 0.46 [95% CI, 0.13–1.59]); however, the treatment effect could not be quantified in those with isolated gain/amp(1q21) as no PFS events were observed in the D-R group versus 4 PFS events in the R group (Supplementary Fig. 4a, b). Consistent with observations across other subgroups, a PFS trend favoring D-R versus R maintenance was seen regardless of response status at study entry; however, this trend was less pronounced for patients in VGPR at study entry (Supplementary Fig. 4c).

A PFS by cytogenetic risk per original criteria. High-risk cytogenetics per the original definition are defined as ≥1 abnormality including del(17p), t(4;14), and/or t(14;16). B PFS by cytogenetic risk per revised criteria. Revised high-risk cytogenetics per the revised definition are defined as ≥1 abnormality including del(17p), t(4;14), t(14;16), t(14;20), and/or gain/amp(1q21). C PFS by cytogenetic risk per modified IMS 2024 criteria. High risk per the modified IMS 2024 criteria is defined as the presence of ≥20% del(17p); del(1p32) co-occurring with gain/amp(1q21); or t(4;14), t(14;16), and/or t(14;20) co-occurring with gain/amp(1q21) and/or del(1p32). In the AURIGA study, data were not available on TP53 mutations, beta-2-microglobulin and creatinine levels at the time of multiple myeloma diagnosis, and differentiation between monoallelic versus biallelic del(1p32). D PFS by the number of HRCAs, defined as the number of abnormalities from del(17p), t(4;14), t(14;16), t(14;20), and/or gain/amp(1q21). Cytogenetic results at diagnosis (based on clinical report form collected data from local labs) were used in the analysis. PFS, progression-free survival; IMS, International Myeloma Society; HRCA, high-risk cytogenetic abnormality; D-R, daratumumab/lenalidomide; R, lenalidomide; HR, hazard ratio; CI, confidence interval. aHR and 95% CI from a Cox proportional hazards model with treatment as the sole explanatory variable. An HR <1 indicates an advantage for D-R maintenance.
Safety
The safety and tolerability profiles of D-R and R maintenance in the overall AURIGA study population have been previously published [18]. The aim of this analysis was to verify any specific safety concerns in the older patient population, as well as in Black patients. When looking at safety data by race, no additional safety concerns were observed with D-R maintenance among Black patients. Median duration of therapy among White patients was 23.7 months (D-R, 29.3 months; R, 18.9 months) and among Black patients was 25.4 months (D-R, 28.3 months; R, 25.4 months). Table 1 provides a summary of the most common treatment-emergent adverse events (TEAEs) in all patients who received ≥1 dose of study treatment, separated by White (D-R, n = 64; R, n = 65) or Black (D-R, n = 20; R, n = 24) race. The incidence of grade 3/4 TEAEs was higher with D-R versus R maintenance for both White patients (D-R, 76.6%; R, 70.8%) and Black patients (75.0%; 66.7%). The most common grade 3/4 TEAE was neutropenia, with similar incidences in White patients (D-R, 45.3%; R, 43.1%) and Black patients (50.0%; 45.8%). The incidence of grade 3/4 cytopenia was similar across treatment groups for White patients (D-R, 54.7%; R, 47.7%) and Black patients (50.0%; 50.0%). The incidence of grade 3/4 infections was higher with D-R versus R maintenance among White patients (D-R, 20.3%; R, 12.3%) but was comparable among Black patients (20.0%; 20.8%). Similarly, serious TEAEs were higher with D-R versus R maintenance among White patients (D-R, 31.3%; R, 21.5%) but comparable among Black patients (30.0%; 29.2%). TEAEs leading to treatment discontinuation were highest among White patients, with greater rates observed with D-R versus R maintenance (D-R, 21.9%; R, 10.8%), while no trend was observed among Black patients (0%; 4.2%). Deaths due to TEAEs were low (n = 3), which all occurred among White patients (D-R, n = 2 [3.1%]; R, n = 1 [1.5%]).
In an analysis of safety by age, no specific safety concerns were observed with the addition of daratumumab SC to R maintenance, including among older patients. The median duration of therapy among patients aged <65 years was 25.0 months (D-R, 30.5 months; R, 23.5 months) and 24.4 months (32.7 months; 19.2 months) among patients aged ≥65 years. Table 2 provides a summary of the most common TEAEs, separated by age subgroup (<65 years: D-R, n = 59; R, n = 58; ≥65 years: D-R, n = 37; R, n = 40). The incidence of grade 3/4 TEAEs was higher for D-R versus R maintenance among patients aged <65 years (D-R, 76.3%; R, 63.8%) but comparable between treatments among patients aged ≥65 years (70.3%; 72.5%). Neutropenia was the most common grade 3/4 TEAE both in patients aged <65 years (D-R, 44.1%; R, 43.1%) and in those aged ≥65 years (51.4%; 40.0%). A similar proportion of patients aged <65 years and ≥65 years experienced grade 3/4 cytopenia within each treatment group, with a higher overall incidence reported with D-R compared with R among both the younger (D-R, 52.5%; R, 46.6%) and older patients (56.8%; 47.5%). The incidence of grade 3/4 infections was lower among patients aged <65 who received R maintenance (D-R, 18.6%; R, 10.3%) but was similar across treatment groups among patients aged ≥65 years (18.9%; 17.5%). Among patients aged <65 years, the incidence of serious TEAEs was higher with D-R versus R maintenance (D-R, 23.7%; R, 12.1%), whereas for patients aged ≥65 years, the incidence was similar (40.5%; 37.5%). The frequency of TEAEs leading to treatment discontinuation was higher with D-R versus R maintenance in both age groups (<65 years: D-R, 11.9%; R, 6.9%; ≥65 years: D-R, 18.9%; R, 10.0%). Deaths due to TEAEs were low (n = 3), with all deaths occurring among the older patients (D-R, n = 2 [5.4%]; R, n = 1 [2.5%]).
Discussion
Despite treatment advancements in NDMM, certain patient subgroups continue to have inferior outcomes [19]. Here, we report data from a post hoc analysis of the phase 3 AURIGA study in patient subgroups with high unmet medical need, including older and Black patients and those with cytogenetically high-risk disease according to established and recent criteria. In all subgroups explored, the addition of daratumumab SC to R maintenance led to an improved MRD-negative (10–5) conversion rate from baseline to 12 months of maintenance and overall MRD-negative conversion rate, regardless of race, age, and risk status. In addition, favorable trends in response from baseline and PFS were also observed with D-R maintenance, with no unexpected safety concerns among Black patients or patients aged ≥65 years.
Among patients with NDMM, HRCAs have been shown to confer suboptimal outcomes and are highly prognostic; therefore, these high-risk patients constitute a group with high unmet medical need. The original definition of cytogenetically high-risk disease included the presence of abnormalities such as t(4;14), t(14;16), and/or del(17p) [21]. A subsequent “revised” definition encompassed additional factors, including t(14;20) and gain/amp(1q) abnormalities [22]. Most recently, an updated IMWG consensus definition of cytogenetically high-risk MM was presented at the 2024 annual IMS meeting [23, 24]. This new definition includes additional genomic factors, including the presence of TP53 mutation and biallelic del(1p32), both associated with worse overall survival [26, 27]. A clinical threshold of ≥20% for del(17p); the co-occurrence of monoallelic del(1p32) with gain/amp(1q21); and the co-occurrence of t(4;14), t(14;16), and/or t(14;20) with gain/amp(1q21) and/or monoallelic del(1p32) were also included as high-risk criteria [24]. While this updated definition aims to enhance the use of risk-stratified therapeutic approaches in clinical practice and to inform the design of clinical studies focused on high-risk MM, its recent introduction means that only a few studies have examined the efficacy of treatments for patients with these specific characteristics.
As reported here, the use of D-R maintenance led to an improvement versus R maintenance in MRD-negative (10–5) conversion rate by 12 months of maintenance across all subgroups, including those with cytogenetically high-risk disease per original (31.8% vs 6.7%), revised (43.8% vs 13.3%), and modified IMS 2024 high-risk (41.2% vs 0%) definitions. Similar benefits in favor of D-R maintenance were observed among the varying IMS 2024 high-risk subgroups, including those with ≥20% del(17p) (20.0% vs 0%); t(4;14), (14;16), and/or (14;20) co-occurring with gain/amp(1q21) and/or del(1p32) (40.0% vs 0%); and del(1p32) co-occurring with gain/amp(1q21) (75.0% vs 0%). Furthermore, among patients with ultra-high–risk cytogenetics (≥2 revised HRCAs), a patient population with high unmet medical need and treatment challenges, 54.5% of patients achieved MRD-negative (10–5) conversion by 12 months of maintenance with D-R versus 0% of patients with R maintenance alone, with similar trends observed for overall MRD-negative (10–5) conversion. Given that achieving MRD negativity is associated with prolonged PFS and overall survival [28], the demonstrated benefit of adding daratumumab SC to standard maintenance therapy in patients with high-risk, and especially ultra-high–risk, MM is promising. Another interesting observation includes the trend towards PFS improvement in patients with ≥CR at study entry, particularly among patients treated with D-R maintenance. This may indicate the importance of using optimal induction therapy (eg, quadruplet therapy) to obtain deep, early responses. Both optimal induction therapy and optimal maintenance therapy are needed to maximize patient outcomes in NDMM.
While cross-study comparisons should be done with caution, data from this post hoc analysis corroborate those observed in other clinical studies of transplant-eligible patients with NDMM. In a post hoc analysis of the phase 2 GRIFFIN study completed at the time of final analysis (median follow-up, 49.6 months), the addition of daratumumab SC to both bortezomib/lenalidomide/dexamethasone (D-VRd) induction/consolidation and R maintenance showed a trend towards the improvement of clinical outcomes versus VRd induction/consolidation and R maintenance among transplant-eligible patients with NDMM, including those with varying high-risk characteristics [29]. For instance, among patients with revised cytogenetically high-risk disease, a higher proportion of patients achieved MRD negativity (10–5) with D-VRd versus VRd (54.8% [23/42] vs 32.4% [12/37], respectively), and median PFS was not reached versus 47.9 months, respectively, thus favoring D-VRd (HR, 0.38 [95% CI, 0.14–1.01]) [29]. Similarly, in the phase 3 PERSEUS study, D-VRd induction/consolidation followed by D-R maintenance led to improved MRD-negative (10–5) rate and PFS across clinically relevant subgroups versus VRd followed by R maintenance [9]. Among patients with cytogenetically high-risk disease per the revised definition, the overall MRD-negative (10–5) rate was greater with D-VRd versus VRd (73.1% [95/130] vs 49.3% [73/148], respectively), and PFS similarly favored D-VRd (HR, 0.53 [95% CI, 0.35–0.81]) [30]. Furthermore, in an analysis of the ITT maintenance population from the phase 3 CASSIOPEIA study, PFS consistently favored daratumumab maintenance versus observation alone across all clinically relevant subgroups, including patients with cytogenetically high-risk disease (t[4;14] and/or del[17p]) for whom median PFS was not estimable versus 27.2 months in the daratumumab and observation groups, respectively (HR, 0.39 [95% CI, 0.25–0.63]) [13]. Collectively, these data support the benefit of adding daratumumab SC to standard-of-care maintenance treatment in clinically relevant subgroups of patients with transplant-eligible NDMM, including those with cytogenetically high-risk disease. The phase 3 CEPHEUS and IMROZ studies, which evaluated anti-CD38 mAb–based quadruplet regimens versus non–anti-CD38 mAb–based triplet regimens, demonstrated PFS HRs in transplant-ineligible and transplant-deferred patients with cytogenetically high-risk disease of 0.88 (95% CI, 0.42–1.84) [17] and 0.97 (95% CI, 0.48–1.96) [31], respectively. These results should be interpreted with caution given the limited sample size of the cytogenetically high-risk subgroups, although the PFS HRs for CD38 mAb–based quadruplet regimens in these subgroups are less favorable than the PFS HRs in all patients. Nevertheless, per data reported from the phase 3 MAIA study, favorable trends for PFS (median follow-up, 64.5 months; HR, 0.57 [95% CI, 0.34–0.96]) [32] and overall survival (median follow-up, 89.3 months; HR, 0.65 [95% CI, 0.40–1.06]) [33] were observed in transplant-ineligible patients with cytogenetically high-risk NDMM following daratumumab plus lenalidomide/dexamethasone versus lenalidomide/dexamethasone alone.
Evidence indicates that the addition of daratumumab confers benefit not only in high-risk but also standard-risk patients. The addition of daratumumab improved MRD-negative rates among patients with revised cytogenetically standard-risk disease in the AURIGA (D-R, 53.8%; R, 22.6%), GRIFFIN (D-VRd, 75.0%; VRd, 31.7%), and PERSEUS (D-VRd, 75.3%; VRd, 47.3%) studies, leading to a trend in PFS improvement (AURIGA, HR 0.69, [95% CI, 0.24–1.95]; GRIFFIN, HR 0.39 [95% CI, 0.10–1.51]; PERSEUS, HR 0.29 [95% CI, 0.15–0.56]) [18, 29, 30]. When considering the new IMS 2024 criteria, patients in AURIGA with standard-risk disease per modified IMS 2024 criteria also exhibited favorable MRD and PFS trends with the addition of daratumumab SC to R maintenance. Overall, the clinical benefit of daratumumab SC was evident in both high-risk and standard-risk disease, supporting its role as a versatile treatment option for all transplant-eligible patients with NDMM, rather than being reserved solely for patients with high-risk disease.
No specific safety concerns were identified in Black or older patients, corroborating observations from the GRIFFIN study [29, 34]. Per the AURIGA study, no increase in the incidences of grade 3/4 infection or cytopenia was observed in younger compared with older patients, nor when comparing treatment groups. In an analysis of Black patients from GRIFFIN, a greater proportion of patients experienced a higher frequency of TEAEs leading to discontinuation of ≥1 component of the study regimen (D-VRd, 64.3%; VRd, 38.9%) compared with White patients (28.9%; 25.7%); this higher frequency of TEAEs leading to discontinuation in Black patients was primarily driven by neuropathy-related events (D-VRd, 28.6%; VRd, 22.2), leading to the discontinuation of bortezomib [34]. As reported in the current analysis of AURIGA, only 4.2% of Black patients experienced TEAEs that led to discontinuation of ≥1 component of the study regimen, all of which were in the R group. Given that AURIGA enrolled a notable proportion of Black patients (22%), findings from this post hoc analysis support the safety of daratumumab SC in this patient population, which is often underrepresented in clinical studies.
This post hoc analysis has some limitations. Firstly, while subgroups were generally well balanced, a few subgroups had relatively low sample sizes, thus limiting the robustness of the observed data and the strength of inferences made. Secondly, in the AURIGA study, data were not collected for TP53 mutation, differentiation between monoallelic versus biallelic del(1p32), and ß2M or creatinine levels at the time of MM diagnosis prior to induction therapy; therefore, the impact of D-R maintenance across all IMS 2024 high-risk subgroups could not be analyzed. Given these limitations, larger phase 3 clinical studies with greater sample sizes aiming to specifically enroll patients with high-risk NDMM are needed to help draw more definitive conclusions regarding these new high-risk stratification categories. Finally, it should be noted that all patients enrolled in the AURIGA study were anti-CD38 mAb naïve, so our findings may not be applicable to patients who have received anti-CD38 mAb–based induction/consolidation treatment, which is currently considered standard of care. The phase 3 PERSEUS study, which evaluated the addition of daratumumab to VRd induction/consolidation and R maintenance, demonstrated a deepening of MRD negativity over time during D-R maintenance, suggesting a benefit in patients with prior daratumumab exposure; however, PERSEUS did not include a second randomization prior to maintenance to more specifically evaluate the role of daratumumab-based maintenance [35]. Therefore, the added value of anti-CD38 mAb treatment during maintenance after receiving anti-CD38 mAb–based induction/consolidation remains unclear; however, additional trials such as DRAMMATIC (SWOG S1803) [36] and GMMG-HD7 [37] will provide insight into this important question in the near future.
In summary, results of this post hoc analysis of AURIGA showed the consistent ability of D-R maintenance compared with standard-of-care R maintenance alone to improve MRD-negative (10–5) conversion rate, depth of response, and a trend towards PFS improvement among anti-CD38 mAb–naïve patients with NDMM who were MRD positive post-ASCT with either high-risk or standard-risk disease. Additionally, no unexpected safety concerns were observed among patients aged ≥65 years or Black patients. This study supports the addition of daratumumab SC to R maintenance in all transplant-eligible patients with NDMM regardless of age, race, and cytogenetic risk status; however, additional studies with larger sample sizes are needed to confirm these findings.
Data availability
The data sharing policy of Johnson & Johnson is available at https://innovativemedicine.jnj.com/our-innovation/clinical-trials/transparency. As noted on this site, requests for access to the study data can be submitted through Yale Open Data Access (YODA) Project site at http://yoda.yale.edu.
References
de Weers M, Tai YT, van der Veer MS, Bakker JM, Vink T, Jacobs DC, et al. Daratumumab, a novel therapeutic human CD38 monoclonal antibody, induces killing of multiple myeloma and other hematological tumors. J Immunol. 2011;186:1840–8.
Lammerts van Bueren J, Jakobs D, Kaldenhoven N, Roza M, Hiddingh S, Meesters J, et al. Direct in vitro comparison of daratumumab with surrogate analogs of CD38 antibodies MOR03087, SAR650984 and Ab79. Blood. 2014;124:3474.
Overdijk MB, Verploegen S, Bögels M, van Egmond M, Lammerts van Bueren JJ, Mutis T, et al. Antibody-mediated phagocytosis contributes to the anti-tumor activity of the therapeutic antibody daratumumab in lymphoma and multiple myeloma. MAbs. 2015;7:311–21.
Overdijk MB, Jansen JH, Nederend M, Lammerts van Bueren JJ, Groen RW, Parren PW, et al. The therapeutic CD38 monoclonal antibody daratumumab induces programmed cell death via Fcgamma receptor-mediated cross-linking. J Immunol. 2016;197:807–13.
Krejcik J, Casneuf T, Nijhof IS, Verbist B, Bald J, Plesner T, et al. Daratumumab depletes CD38+ immune regulatory cells, promotes T-cell expansion, and skews T-cell repertoire in multiple myeloma. Blood. 2016;128:384–94.
Adams HC III, Stevenaert F, Krejcik J, Van der Borght K, Smets T, Bald J, et al. High-parameter mass cytometry evaluation of relapsed/refractory multiple myeloma patients treated with daratumumab demonstrates immune modulation as a novel mechanism of action. Cytometry A. 2019;95:279–89.
Casneuf T, Adams HC III, van de Donk NWCJ, Abraham Y, Bald J, et al. Deep immune profiling of patients treated with lenalidomide and dexamethasone with or without daratumumab. Leukemia. 2021;35:573–84.
Facon T, Kumar S, Plesner T, Orlowski RZ, Moreau P, Bahlis N, et al. Daratumumab plus lenalidomide and dexamethasone for untreated myeloma. N Engl J Med. 2019;380:2104–15.
Sonneveld P, Dimopoulos MA, Boccadoro M, Quach H, Ho PJ, Beksac M, et al. Daratumumab, bortezomib, lenalidomide, and dexamethasone for multiple myeloma. N Engl J Med. 2024;390:301–13.
Mateos MV, Cavo M, Blade J, Dimopoulos MA, Suzuki K, Jakubowiak A, et al. Overall survival with daratumumab, bortezomib, melphalan, and prednisone in newly diagnosed multiple myeloma (ALCYONE): a randomised, open-label, phase 3 trial. Lancet. 2020;395:132–41.
Sonneveld P, Chanan-Khan A, Weisel K, Nooka AK, Masszi T, Beksac M, et al. Overall survival with daratumumab, bortezomib, and dexamethasone in previously treated multiple myeloma (CASTOR): a randomized, open-label, phase III trial. J Clin Oncol. 2023;41:1600–9.
Dimopoulos MA, Oriol A, Nahi H, San-Miguel J, Bahlis NJ, Usmani SZ, et al. Overall survival with daratumumab, lenalidomide, and dexamethasone in previously treated multiple myeloma (POLLUX): a randomized, open-label, phase III trial. J Clin Oncol. 2023;41:1590–9.
Moreau P, Hulin C, Perrot A, Arnulf B, Belhadj K, Benboubker L, et al. Bortezomib, thalidomide, and dexamethasone with or without daratumumab and followed by daratumumab maintenance or observation in transplant-eligible newly diagnosed multiple myeloma: long-term follow-up of the CASSIOPEIA randomised controlled phase 3 trial. Lancet Oncol. 2024;25:1003–14.
DARZALEX® (daratumumab) [package insert]. Horsham, PA: Janssen Biotech, Inc.; April 2025.
DARZALEX FASPRO® (daratumumab and hyaluronidase-fihj) [package insert]. Horsham, PA: Janssen Biotech; July 2024.
Voorhees PM, Sborov DW, Laubach J, Kaufman JL, Reeves B, Rodriguez C, et al. Addition of daratumumab to lenalidomide, bortezomib, and dexamethasone for transplantation-eligible patients with newly diagnosed multiple myeloma (GRIFFIN): final analysis of an open-label, randomised, phase 2 trial. Lancet Haematol. 2023;10:e825–37.
Usmani SZ, Facon T, Hungria V, Bahlis NJ, Venner CP, Braunstein M, et al. Daratumumab plus bortezomib, lenalidomide and dexamethasone for transplant-ineligible or transplant-deferred newly diagnosed multiple myeloma: the randomized phase 3 CEPHEUS study. Nat Med. 2025;31:1195–202.
Badros AZ, Foster L, Anderson LD Jr, Chaulagain CP, Pettijohn EM, et al. Daratumumab with lenalidomide as maintenance after transplant in newly diagnosed multiple myeloma: the AURIGA study. Blood. 2025;145:300–10.
Mateos MV, Martinez BP, Gonzalez-Calle V. High-risk multiple myeloma: how to treat at diagnosis and relapse? Hematology Am Soc Hematol Educ Program. 2021;2021:30–6.
Hanamura I. Multiple myeloma with high-risk cytogenetics and its treatment approach. Int J Hematol. 2022;115:762–77.
Fonseca R, Bergsagel PL, Drach J, Shaughnessy J, Gutierrez N, Stewart AK, et al. International Myeloma Working Group molecular classification of multiple myeloma: spotlight review. Leukemia. 2009;23:2210–21.
Rajkumar SV. Multiple myeloma: 2022 update on diagnosis, risk stratification, and management. Am J Hematol. 2022;97:1086–107.
Moreau P. Opening Ceremony President’s Address. Presented at the International Myeloma Society (IMS) Annual Meeting; September 25-28, 2024; Rio de Janeiro, Brazil.
Avet-Loiseau H, Davies FE, Samur MK, Corre J, D'Agostino M, Kaiser MF, et al. International Myeloma Society/International Myeloma Working Group consensus recommendations on the definition of high-risk multiple myeloma. J Clin Oncol. 2025;43:2739–51.
Kumar S, Paiva B, Anderson KC, Durie B, Landgren O, Moreau P, et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol.2016;17:e328–46.
Schavgoulidze A, Talbot A, Perrot A, Cazaubiel T, Leleu X, Manier S, et al. Biallelic deletion of 1p32 defines ultra-high-risk myeloma, but monoallelic del(1p32) remains a strong prognostic factor. Blood. 2023;141:1308–15.
Corre J, Perrot A, Caillot D, Belhadj K, Hulin C, Leleu X, et al. del(17p) without TP53 mutation confers a poor prognosis in intensively treated newly diagnosed patients with multiple myeloma. Blood. 2021;137:1192–5.
Munshi NC, Avet-Loiseau H, Anderson KC, Neri P, Paiva B, Samur M, et al. A large meta-analysis establishes the role of MRD negativity in long-term survival outcomes in patients with multiple myeloma. Blood Adv. 2020;4:5988–99.
Chari A, Kaufman JL, Laubach J, Sborov DW, Reeves B, Rodriguez C, et al. Daratumumab in transplant-eligible patients with newly diagnosed multiple myeloma: final analysis of clinically relevant subgroups in GRIFFIN. Blood Cancer J. 2024;14:107.
Dimopoulos MA, Sonneveld P, Rodríguez-Otero P, Quach H, Ho PJ, Beksac M, et al. Daratumumab (DARA)/bortezomib/lenalidomide/dexamethasone (D-VRd) with D-R maintenance (maint) in transplant-eligible (TE) newly diagnosed myeloma (NDMM): PERSEUS cytogenetic risk analysis. Presented at the International Myeloma Society (IMS) Annual Meeting; September 25-28, 2024; Rio De Janeiro, Brazil.
Facon T, Dimopoulos MA, Leleu XP, Beksac M, Pour L, Hajek R, et al. Isatuximab, bortezomib, lenalidomide, and dexamethasone for multiple myeloma. N Engl J Med. 2024;391:1597–609.
Moreau P, Facon T, Usmani SZ, Bahlis N, Raje N, Plesner T, et al. Daratumumab plus lenalidomide and dexamethasone (D-Rd) versus lenalidomide and dexamethasone (Rd) in transplant-ineligible patients with newly diagnosed multiple myeloma (NDMM): clinical assessment of key subgroups of the phase 3 MAIA study. Presented at the American Society of Hematology (ASH) Annual Meeting & Exposition; December 10-13, 2022; New Orleans, LA, USA.
Facon T, Kumar SK, Orlowski RZ, Bahlis N, Moreau P, Goldschimdt H, et al. Final survival analysis of daratumumab plus lenalidomide and dexamethasone versus lenalidomide and dexamethasone in transplant-ineligible patients with newly diagnosed multiple myeloma: MAIA study. Presented at the European Hematology Association (EHA) Hybrid Congress; June 13-16, 2024; Madrid, Spain.
Nooka AK, Kaufman JL, Rodriguez C, Jakubowiak A, Efebera Y, Reeves B, et al. Post hoc analysis of daratumumab plus lenalidomide, bortezomib and dexamethasone in Black patients from final data of the GRIFFIN study. Br J Haematol. 2024;204:2227–32.
Rodríguez-Otero P, Moreau P, Dimopoulos MA, Beksac M, Perrot A, Broijl A, et al. Daratumumab (DARA) + bortezomib/lenalidomide/dexamethasone (VRd) in transplant-eligible (TE) patients (pts) with newly diagnosed multiple myeloma (NDMM): analysis of minimal residual disease (MRD) in the PERSEUS trial. Presented at the American Society of Clinical Oncology (ASCO) Annual Meeting; May 31–June 4, 2024; Chicago, IL, USA.
SWOG Cancer Research Network. S1803, lenalidomide +/- daratumumab/rHuPh20 as post-ASCT maintenance for MM w/MRD to direct therapy duration (DRAMMATIC). ClinicalTrials.gov ID NCT04071457. https://clinicaltrials.gov/study/NCT04071457. Accessed June 23, 2025.
University of Heidelberg Medical Center. Trial on the effect of isatuximab to lenalidomide/bortezomib/dexamethasone (RVd) induction and lenalidomide maintenance in patients with newly diagnosed myeloma (GMMG HD7). ClinicalTrials.gov ID NCT03617731. https://www.clinicaltrials.gov/study/NCT03617731. Accessed June 23, 2025.
Acknowledgements
This study was sponsored by Johnson & Johnson. The authors would like to thank the patients who volunteered to participate in this study, their families, and the staff members at the study sites who cared for them. In addition, we would like to thank all the study personnel at the participating sites. Medical writing and editorial support were provided by Holly Clarke, PhD, and Charlotte D. Majerczyk, PhD, of Lumanity Communications Inc., and were funded by Johnson & Johnson.
Author information
Authors and Affiliations
Contributions
DWS, PV, and TSL contributed to conceptualization and study design. LF, LDA, A Chung, CPC, EP, AJC, CC, SL, KHS, RS, PV, MK, and AB contributed to the investigation. LF, LDA, A Chung, CPC, EP, AJC, CC, SL, DWS, KHS, RS, PV, MK, and AB contributed to patient enrollment. DWS, KHS, SP, VK, A Cortoos, RC, and TSL contributed to study supervision (DWS and KHS trial steering committee). SP, VK, and A Cortoos contributed to project administration. LF, LDA, A Chung, CPC, EP, AJC, CC, SL, DWS, KHS, RS, PV, MK, and AB contributed to data collection. SP, VK, and A Cortoos contributed to data curation. HP contributed to the statistical analysis. All authors contributed to data interpretation. All authors additionally participated in writing, critically reviewing, and revising the manuscript; approved the final version of the manuscript for publication; and agreed to be accountable for the work.
Corresponding author
Ethics declarations
Competing interests
LF served on advisory boards and as a site principal investigator for Bristol Myers Squibb, Johnson & Johnson, and Pfizer. LDA served as a consultant and on advisory boards for Johnson & Johnson, Celgene, Bristol Myers Squibb, Amgen, GSK, AbbVie, BeiGene, Cellectar Biosciences, Sanofi, and Prothena; served on the data safety monitoring board for Prothena; and received institutional research funding from Bristol Myers Squibb, AbbVie, Regeneron, Caelum, CARsgen, Cellectar Biosciences, AstraZeneca, Arcellx, and Johnson & Johnson. A Chung served as a consultant and on an advisory board for Bristol Myers Squibb and Johnson & Johnson; and received institutional research funding from AbbVie, Bristol Myers Squibb, Caelum, CARsgen, Cellectis, Johnson & Johnson, K36 Therapeutics, and Merck. CPC received honoraria from Johnson & Johnson and Sanofi/Genzyme. EP has nothing to declare. AJC served as a consultant or in an advisory role for Sebia, Johnson & Johnson, Bristol Myers Squibb, Sanofi, HopeAI, Adaptive Biotechnologies, and AbbVie; and received institutional research funding from Johnson & Johnson, Bristol Myers Squibb, Juno/Celgene, Sanofi, Regeneron, IGM Biosciences, Nektar, Harpoon, and Caelum. CC served as a consultant for Bristol Myers Squibb, Johnson & Johnson, Pfizer, Karyopharm, and Genentech; and received institutional research funding from Bristol Myers Squibb, Johnson & Johnson, Takeda, Ionis, Poseida, and Harpoon. SL received institutional research funding from Johnson & Johnson, Allogene, Bioline, Pfizer, Bristol Myers Squibb, Regeneron, Sanofi, Ionis, and ImmPACT Bio; and owns stock or stock options for TORL BioTherapeutics. DWS served as a consultant or in an advisory role for GSK, Johnson & Johnson, Sanofi, AbbVie, Bristol Myers Squibb, Pfizer, Opna Bio, Arcellx, AstraZeneca, and Genentech; and received institutional research funding from Pfizer. KHS served on an advisory board for Bristol Myers Squibb, Johnson & Johnson, Sanofi, and GSK; received institutional research funding from AbbVie and Karyopharm; and received honoraria from Karyopharm, Johnson & Johnson, Adaptive Biotechnologies, GSK, Bristol Myers Squibb, Sanofi/Genzyme, and Regeneron. RS served as a consultant or in an advisory role for Sanofi, Johnson & Johnson, and Oncopeptides; and received institutional research funding from Sanofi. PV served as a consultant for, received honoraria from, and holds a membership on an entity’s board of directors or advisory committees for AbbVie, Bristol Myers Squibb, Karyopharm, Regeneron, and Sanofi. MK, HP, SP, VK, RC, and TSL are employees of and may hold stock in Johnson & Johnson. A Cortoos is a former employee of and may hold stock in Johnson & Johnson. AB received research funding from Bristol Myers Squibb, GSK, BeiGene, Roche, and Johnson & Johnson.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Foster, L., Anderson, L.D., Chung, A. et al. Daratumumab plus lenalidomide maintenance in newly diagnosed multiple myeloma after transplant: AURIGA subgroup analyses. Blood Cancer J. 15, 154 (2025). https://doi.org/10.1038/s41408-025-01355-0
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41408-025-01355-0
