
Abstract
Background There are documented health inequalities between ethnic groups in the United Kingdom (UK). However, the evidence regarding ethnic inequalities in oral health is limited and not synthesised.
Aim This scoping review aimed to provide an overview of UK ethnic oral health inequalities.
Methods A search was conducted using Medline, Embase, PsycInfo, PubMed, and Cochrane. After identification and screening, extracted studies were categorised according to clinical, subjective, and oral health behaviour/service-related outcomes.
Results In total, 44 articles were included. Compared to their white counterparts, caries levels were higher among Asian children and oral and pharyngeal cancers rates were higher among Asian women, while lower rates of tooth loss and edentulousness were found among most minority ethnic groups, except for Black adults, who had higher rates. Limited evidence suggests a higher likelihood of poor self-rated oral health among minority ethnic groups, compared to the white majority adult population. The patterns of ethnic oral health inequalities were heterogenous and inconsistent across most other outcomes.
Conclusions There is evidence of ethnic inequalities in oral health within the UK, largely based on limited data from England. This review highlights the need for more robust, large-scale research to broaden understanding and help shape policies to address these inequalities.
Key points
-
The limited available evidence indicates higher rates of caries among Asian children, higher rates of oral cancer among Asian women, and a higher likelihood of poor self-rated oral health among minority ethnic groups in comparison to their white counterparts.
-
For tooth loss, Black adults had higher rates, but other minority ethnic groups had lower rates than white adults. For other clinical, subjective and behavioural/service-related outcomes, the evidence was more limited, and the patterns of ethnic inequalities were inconsistent.
-
This overview of the peer-reviewed literature regarding ethnic oral health inequalities in the UK revealed methodological limitations in the limited evidence. Future research on ethnic inequalities in oral health should include larger sample sizes from across the UK and disaggregated ethnic groupings.
Similar content being viewed by others

Introduction
Health inequalities – the uneven and unfair distribution of health between different groups in a population – are universal, and linked to societal, economic, political and cultural contexts.1 Socioeconomically deprived groups generally experience poorer health outcomes and lower life expectancy than more advantaged socioeconomic groups.2 Health inequalities are also evident according to geography, social vulnerability, and protected characteristics, such as ethnicity.
Within the United Kingdom (UK), approximately 13% of the population belong to a minority ethnic group,3 and by 2061, this is projected to increase to 30%.4 There is evidence of ethnic inequalities in health, with minority ethnic groups having lower disability-free life expectancy and higher cardiovascular and diabetes rates than white ethnic groups.5,6 Yet, for some health outcomes (e.g., overall cancer and dementia mortality rates), higher rates have been noted in white ethnic groups in comparison to minority ethnic groups.5 Significant changes in the pattern of ethnic health inequalities can be observed over time. For example, at the outset of the COVID-19 pandemic in 2020, UK Black and Asian ethnic groups had higher rates of COVID-19 mortality compared to white groups;7 these higher rates remained even after adjusting for socioeconomic disadvantage,8 but by 2022, COVID-19 mortality rates were no longer significantly higher among minority ethnic groups.9
Although higher rates of socioeconomic disadvantage among minority ethnic groups contribute to ethnic health inequalities, the relationship between ethnicity and socioeconomic position is complex.5 In England, people from white British, white Irish and white other groups are less likely than all other minority ethnic groups to live in the 10% most deprived neighbourhoods.10 However, breakdown of ethnic categories into constituent groups reveals variations between groups often included within the same category; compared to white British people, people who identify as of Pakistani heritage are over three times more likely, whereas people who identify as Indian are less likely, to live in the 10% most deprived neighbourhoods.10 This highlights the importance of disaggregated data; however, research is often based on aggregated ethnic categories due to small sample sizes and limited representation of minority ethnic groups in datasets.6
There are other, less explored factors which may partly account for ethnic health inequalities, such as structural racism. Structural racism refers to prejudice enforced through political, legal, economic systems, social customs.11 Both structural and interpersonal racism may impact provision of healthcare, health behaviours and access to health services.6,11
For oral health inequalities, substantive evidence documents clear social gradients according to socioeconomic position in the UK,12,13 mirroring those for general health outcomes. However, there is much less evidence pertaining to oral health inequalities according to ethnicity. A briefing report from 2013 concluded that minority ethnic groups experienced higher caries rates and identified some differences in the use of dental services in comparison to the overall population.14 No study has looked at a wide range of oral health outcomes to synthesise the peer-reviewed evidence on ethnic oral health inequalities in the UK. Therefore, this paper aims to provide an overview and synthesis of the evidence on ethnic oral health inequalities in the UK between 2000 and 2021.
Methods
This scoping review was conducted according to a local review protocol developed by the research team, which has not been registered publicly. The review was conducted and reported in accordance with PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) extension for Scoping Reviews (PRISMA-ScR).15 The online Supplementary Information contains a completed PRISMA-ScR checklist. This review adapted a modified five-stage Arksey and O'Malley framework.16
Research question
The research question was: ‘what is the evidence of oral health inequalities according to ethnicity in the UK?'.
Inclusion and exclusion criteria
There were no restrictions on study design or quality. This review included peer-reviewed systematic reviews and original research studies, based on UK data, and published in English. Grey literature was excluded from this review.
Data sources, search strategy and study selection
A literature search on Ovid (Medline, Embase, PsycInfo), PubMed, and Cochrane databases was conducted between November 2021 and January 2022 to cover all relevant literature published between January 2000 and December 2021.17 The search strategy and syntax used appropriate medical subject heading terms (Appendix 1). Reference lists of reviewed articles were screened to identify possible additional papers for inclusion. Duplicate articles and those not relevant to this review were excluded, followed by screening of titles, then abstracts and finally, full texts of the identified articles by two independent reviewers. Any discrepancies between reviewers were settled following discussion.
Data extraction
Data were extracted regarding the publication author and date, study population and dataset, sample size, study design, ethnic group categories included, study outcomes, main study findings, and evidence for oral health inequalities. Data extraction was performed by one reviewer.
Summarising and reporting results
Studies were categorised according to their outcome(s) as clinical, subjective, behavioural (relating to oral hygiene and sugar consumption) or service-related, with some studies included in multiple categories.
Results
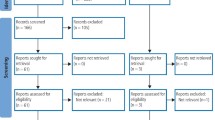
The literature searches retrieved 833 articles; 363 duplicates were removed, 325 papers were excluded after screening the title and abstract, and a further 101 papers were removed after reading the full text, resulting in 44 papers included in this review (Fig. 1).

PRISMA flowchart of literature search
Most studies included cross-sectional data, but some also contained longitudinal, ecological, and retrospective analyses. There were many variations in ethnicity classification and terminology, with some studies using aggregated categories and terms such as ‘white', ‘Asian', ‘non-Asian' and ‘Black,' while many studies presented disaggregated ethnic data within each group (e.g., ‘Black Caribbean', ‘Black African'). For the purposes of this review, we employ the terminology reported in each study. One study included only one minority ethnic group, with no comparison.18 Most studies were conducted solely within England (n = 36). Some studies used data originating from surveys covering more than one UK country or UK data19,20,21,22,23,24 and one study was conducted only in Scotland.25 One study did not specify the geographical source of the data presented.26
Clinical outcomes
Online Supplementary Table 1 presents the studies relating to clinical outcomes and ethnicity.
Dental caries
In total, 13 articles were identified (nine focused exclusively on children,20,25,27,28,29,30,31,32,33 four mainly on adults).19,34,35,36 With the exception of one relatively small study,28 all other studies (including studies using larger samples from national datasets) among children indicated higher caries prevalence among ‘Asian' groups in comparison to ‘white' or ‘non-Asian' groups.20,25,27,29,30,31,32,33
Higher caries rates were reported among children who identified as ‘Eastern European white' in comparison to ‘white British' children.30,32 In contrast, two studies found lower caries rates in ‘Black Caribbean' and ‘Black African' in comparison to ‘white' children.20,33
For adults, two studies indicated a lower likelihood of untreated decay and lower caries prevalence among ‘Asian' and ‘Black' ethnic groups in comparison to ‘white' groups.19,34
In the only adult study to include data on ‘Eastern European white' and ‘other white' groups, caries prevalence was higher in these groups compared to ‘white British' adults.34
Ethnic inequalities in caries remained when socioeconomic position and/or area deprivation were accounted for.19,20,25,28,32,34 Two studies assessed ethnic inequalities in dental caries by area deprivation, with one showing no variation between areas with different levels of deprivation,19 while the other showed more prominent ethnic inequalities in dental caries in deprived areas.28
Periodontal disease
Six articles related to periodontal disease.19,20,37,38,39,40 A nationally representative study found that, compared to ‘white' children, five-year-old and 12-year-old ‘Bangladeshi' children were more likely to experience gingivitis, plaque, and poor periodontal health (gingivitis, plaque, or calculus in more than one sextant), while ‘Black Caribbean' children had lower probability of poor periodontal health at age five. However, there were no significant ethnic differences in periodontal outcomes at age 15.20
For adults, analysis of nationally representative data revealed no significant differences in the risk of having ≥6 periodontal pockets between ‘Asian' and ‘white' adults in unadjusted models and after adjusting for demographics, socioeconomic position, behavioural factors, and service use.19 Four smaller studies based in London and South East England focused on different ethnic groups and showed a mixed pattern of results.37,38,39,40
Tooth loss
Seven articles examined tooth loss.18,19,34,36,41,42,43 A nationally representative study found higher rates of tooth loss and edentulousness among ‘white' and ‘Black' ethnic groups, with lower rates among people from ‘Pakistani', ‘Bangladeshi', and ‘Indian' ethnic groups.19
Most of the remaining studies also demonstrated lower tooth loss and edentulousness rates among minority ethnic groups (‘Black African', ‘Black other', ‘Pakistani', ‘Indian', ‘Bangladeshi', ‘Chinese') compared to ‘white British' adults,34,36,42 with these lower rates persisting after adjustment for socioeconomic position for people from ‘Indian', ‘Pakistani', ‘Bangladeshi', and ‘Chinese' ethnic groups.42 Another study showed that first-generation migrant ‘Black Caribbean' adults and second-generation migrants from ‘Pakistani' ethnic groups had higher odds of edentulousness than ‘white British' adults.43
Dental trauma
Only three studies in children were identified.44,45,46 Using the same dataset from adolescents in East London, two studies found no association between traumatic dental injuries and ethnicity in unadjusted analyses and also adjusted for demographics, overjet, bullying and parental socioeconomic position.44,45 Another study confirmed no significant association between traumatic dental injuries and ethnicity, but found lower likelihood of traumatic dental injuries among ‘Black Caribbean' children in comparison to ‘Black African', ‘Pakistani' or ‘white UK' children.46
Oral cancer
Eight studies examined oral and pharyngeal cancer.24,26,47,48,49,50,51,52 Five studies were based on analyses of cancer registry data,48,49,50,51,52 while others used an ecological design,24,47 or hospital retrospective and prospective data.26 Most studies showed higher rates of oral and pharyngeal cancer in ‘Asian' ethnic groups compared to ‘white' groups or ‘non-Asian/other' groups.47,48,49,51,52 In the studies which included comparisons with ‘white' groups,49,52 higher rates of oral cancer were observed in women from ‘Indian', ‘Pakistani', and ‘Bangladeshi' ethnic groups, and lower rates observed in ‘Black African', ‘Black Caribbean' and women from the ‘Chinese' ethnic group. For men, the evidence was inconsistent, with one study reporting higher risk of oral cancer but no increased risk for pharyngeal cancer in ‘Asian' compared to ‘non-Asian' groups.51 Two other studies found higher rates of nasopharyngeal cancer for ‘Chinese' compared to ‘white' men.49,52 Better survival rates were observed for ‘South Asian' in comparison to ‘non-Asian' men, but no ethnic differences in survival rates were observed among women after adjustment for age at diagnosis, relative area deprivation and cancer stage at diagnosis.50 However, ethnic groups in this study were determined via a name recognition algorithm, an important conceptual and methodological limitation.
Subjective oral health outcomes
Online Supplementary Table 2 presents the studies on subjective oral health outcomes and ethnicity.
Subjective/perceived oral health
Four studies were identified, one on orthodontic self-perception in adolescents,53 and three on self-rated oral health in adults.18,19,54 Two studies analysed the same nationally representative dataset and included comparisons of ethnic groups with ‘white' groups. One (using only four ethnic group categories) reported higher likelihood of poor self-rated oral health among all ethnic groups (except people from the ‘Indian' ethnic group),19 while the other (using nine ethnic group categories) did so only for adults from the ‘Bangladeshi' and ‘Pakistani' ethnic groups.54 Ethnicity was not associated with aesthetic self-perception or self-perceived orthodontic treatment need in a small sample of adolescents.53
Dental/facial pain
All six studies focused on adults, used different outcomes, and presented a mixed picture of results.18,21,39,42,43,55 A large study in England found higher likelihood of toothache among the ‘Irish' and ‘Black Caribbean' ethnic groups and lower likelihood among the ‘Bangladeshi' ethnic group, compared to the ‘white' group.42 In another smaller English study, first and second-generation ‘Black Caribbean', first-generation ‘Indian', and second-generation ‘Irish' and ‘Pakistani' migrants had higher odds of toothache in comparison to ‘white British' adults.43 A large UK-wide study that assessed facial pain and compared minority ethnic groups with ‘white' adults reported a higher likelihood among mutliracial adults, lower likelihood among adults from the ‘Chinese' ethnic group and no differences for ‘Asian' or ‘Black' adults.21 One small study showed lower frequency of pain when eating certain foods among the ‘Chinese' and ‘Bangladeshi' ethnic groups,39 while another reported higher likelihood of oral and facial pain among the ‘Chinese' and ‘Indian' ethnic groups.55
Oral health-related quality of life
Six studies (all on adults) were included, and the evidence is mixed.19,23,35,39,55,56 In a nationally representative study, all minority ethnic groups reported higher prevalence of difficulty eating due to dental problems than ‘white' people.19 Two smaller studies identified ‘Black' groups as having worse quality of life,23,56 but socioeconomic position accounted for the inequalities between ‘white' and ‘Black' groups.56 There were discrepancies regarding oral health-related quality of life among ‘Asian' groups, with one large study reporting worse19 and another much smaller study reporting better56 quality of life. Two studies did not include a ‘white' ethnic group and found no ethnic differences in oral impacts and symptoms between the included minority groups.35,39 One study reported higher likelihood of oral impacts in terms of difficulty chewing, speaking, and eating among ‘Chinese' and ‘Indian' ethnic groups compared to all other ethnic groups combined.55
Oral health behaviours and service use
Online Supplementary Table 3 presents the studies on ethnic inequalities in oral health behaviours and service use.
Oral hygiene
Four studies were included. One was based on nationally representative survey data,19 two used relatively smaller samples from Manchester33 and South Thames,36 and one small study included data on older adults from the ‘Chinese' ethnic group only.18 The national survey analysis indicated higher likelihood for less frequent toothbrushing among adults from the ‘Indian' ethnic group and less prevalent use of additional oral hygiene products across all minority ethnic groups compared to ‘white' adults.19 A smaller non-representative study on children indicated higher likelihood of ‘good' oral cleanliness among ‘African Caribbean' and lower likelihood among ‘Asian' groups, compared to ‘white' children.33 On the whole, the limited available evidence was inconclusive.
Sugar consumption
Seven studies were included, split between adults19,36,57,58 and children.22,59,60 Two were on small samples from local areas.57,59 The results were inconsistent, with some studies indicating higher sugar consumption in ‘Pakistani' and ‘Bangladeshi' ethnic groups compared to ‘white' groups,22,58,59 and another showing no significant differences in sugar consumption between ‘white' and ‘Asian' adolescents.60 Socioeconomic factors accounted for a large amount of ethnic inequality in one of these studies.22 Analysis of nationally representative survey data did not provide a clear pattern either, with minority ethnic groups generally reporting lower consumption of sweets and adding sugar to hot drinks, but also being less likely to rarely or never have fizzy drinks than the ‘white' group.19
Service use
Five studies were identified,18,19,36,54,61 two of which analysed the same nationally representative dataset.19,54 One study found all minority ethnic groups to be less likely to receive private dental care, visit the dentist more than two times per year, or ever receive a scale and polish.19 The other found that adults from the ‘Indian' ethnic group, ‘Asian other' and the ‘Black African' group were more likely to be symptomatic dental attenders than ‘white' adults.54 Two of the three smaller studies18,36 did not include comparisons with ‘white' ethnic groups; one simply reported dental attendance for ‘Chinese' adults only,18 and the other showed higher prevalence of dental attendance in ‘Black Caribbean', ‘Indian' and ‘Black African' groups compared to ‘Pakistani', ‘Chinese/Vietnamese' and ‘Bangladeshi' groups.36 In another small study, the ‘Asian' group was more likely to have attended dental services within the past two years than the ‘white' group, and this association was attenuated when accounting for socioeconomic factors.61
Discussion
This scoping review provided some evidence of ethnic inequalities in oral health in the UK, but for most outcomes, the patterns were inconsistent or inconclusive. Overall, caries prevalence was reported as higher among ‘Asian' and ‘Eastern European' children compared to ‘white British' children, but lower among ‘Black' and ‘Asian' adults compared to their ‘white' counterparts. The evidence suggests a higher risk of oral and pharyngeal cancers among ‘Asian' compared to ‘white' women, and lower rates of tooth loss and edentulousness among most minority ethnic groups, except for ‘Black' groups, compared to ‘white' groups. Nevertheless, all these findings are based on a limited number of studies. There was no evidence of ethnic inequalities for dental trauma in the studies reviewed, while no relevant literature was available for odontogenic pain and ethnicity. For subjective oral health and behavioural outcomes, the limited available evidence suggests higher likelihood of poor self-rated oral health among minority ethnic groups, compared to ‘white' adults, but the respective evidence for oral health-related quality of life, oral hygiene, sugar consumption and service use was largely inconclusive.
Methodological limitations and characteristics of various studies affect their validity and hinder comparability. Very few studies were based on nationally representative data, mainly consisting of non-generalisable, smaller local samples, some of which were not randomly selected. A nationally representative dataset used by several studies (Adult Dental Health Survey 2009) did not oversample minority ethnic groups and hence contained relatively small numbers of these groups. Small samples sizes in some studies likely led to grouping of disparate ethnic groups into aggregated categories such as ‘Black,' ‘Asian' and ‘white,' which may have masked important differences. Some studies focused on a single ethnic group or did not include a ‘white' ethnic group, which limited comparisons. Ethnicity was not always self-reported, with some studies gauging ethnicity based on names or visual assessment. Similar methodological issues were also identified regarding the evidence surrounding ethnic inequalities in general health.6
Notwithstanding these limitations, this scoping review summarises the relatively limited available evidence of ethnic inequalities in oral health in the UK and highlights important research implications. Some evidence suggests that ethnic inequalities in oral health may remain after considering socioeconomic or behavioural factors. However, socioeconomic position and ethnicity are not impacting on health in isolation; therefore, their intersecting roles on oral health inequalities should be explored further. This calls for research into how structural racism can shape ethnic inequalities in oral health in the UK. Future research should include nationally representative data with sufficient sample sizes for minority ethnic groups to avoid aggregation of ethnicity data and allow more in-depth analyses of ethnic inequalities. This is timely and feasible in the context of a growing UK minority ethnic population. Research should shift focus onto investigating potential mechanisms and intersecting social factors behind differential oral health outcomes between ethnic groups. This will provide better-quality evidence about the patterns of ethnic inequalities and can support policy initiatives aimed at reducing them.
Conclusion
There is evidence of ethnic inequalities in oral health in the UK, mainly based on data from England and particularly in respect to dental caries, oral and pharyngeal cancer, tooth loss and self-rated oral health. More robust research is needed to broaden our understanding, and future studies should consider exploration of the broader determinants using an intersectional approach. Such evidence can shape policy towards creating a fairer society with good oral health for all.
Data availability
The data used in this review originates from previously published studies available in the listed references.
References
Marmot M. Fair society, healthy lives: the Marmot Review: strategic review of health inequalities in England post-2010. 2010. Available at https://www.gov.uk/research-for-development-outputs/fair-society-healthy-lives-the-marmot-review-strategic-review-of-health-inequalities-in-england-post-2010 (accessed 1 October 2025).
The Kings Fund. What are health inequalities? 2022. Available at https://www.kingsfund.org.uk/insight-and-analysis/long-reads/what-are-health-inequalities (accessed 25 April 2024).
Office for National Statistics. Ethnic group by measures. 2011. Available at https://www.nomisweb.co.uk/census/2011/KS201UK/view/2092957697?cols=measures (accessed 9 October 2022).
Rees P, Wohland P, Clark S, Lomax N, Norman P. The future is diversity: new forecasts for the UK's ethnic groups. 2016. Available at https://epc2016.eaps.nl/papers/161123 (accessed 9 October 2022).
The Kings Fund. The health of people from minoritised ethnic groups in England. 2023. [cited 2023 Mar 6] Available at https://www.kingsfund.org.uk/insight-and-analysis/long-reads/health-people-ethnic-minority-groups-england (accessed 6 March 2023).
NHS Race and Health Observatory. Ethnic inequalities in healthcare: a rapid evidence review. 2022. Available at https://www.nhsrho.org/wp-content/uploads/2023/05/RHO-Rapid-Review-Final-Report_.pdf (accessed 9 May 2024).
UK Government. Disparities in the risk and outcomes of COVID-19. 2020. Available at https://assets.publishing.service.gov.uk/media/5f328354d3bf7f1b12a7023a/Disparities_in_the_risk_and_outcomes_of_COVID_August_2020_update.pdf (accessed 3 February 2021).
Office for National Statistics. Why have Black and South Asian people been hit hardest by COVID-19? 2020. Available at https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/articles/whyhaveblackandsouthasianpeoplebeenhithardestbycovid19/2020-12-14 (accessed 25 April 2024).
Office for National Statistics. Updating ethnic and religious contrasts in deaths involving the coronavirus (COVID-19) England: 24 January 2020 to 23 November 2022. 2023. Available at https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/articles/updatingethniccontrastsindeathsinvolvingthecoronaviruscovid19englandandwales/24january2020to23november2022 (accessed 25 April 2024).
UK Government. People living in deprived neighbourhoods. 2020. Available at https://www.ethnicity-facts-figures.service.gov.uk/uk-population-by-ethnicity/demographics/people-living-in-deprived-neighbourhoods/latest (accessed 6 March 2022).
Jamieson L, Peres M A, Guarnizo-Herreño C C, Bastos J L. Racism and oral health inequities: an overview. EClinicalMedicine 2021; 34: 100827.
Steele J, Shen J, Tsakos G et al. The interplay between socioeconomic inequalities and clinical oral health. J Dent Res 2015; 94: 19–26.
Guarnizo-Herreño C C, Watt R G, Fuller E et al. Socioeconomic position and subjective oral health: Findings for the adult population in England, Wales and Northern Ireland. BMC Public Health 2014; 14: 827.
Race Equality Foundation. Oral health and access to dental services for people from Black and minority ethnic groups. 2013. Available at www.better-housing.org.uk (accessed 1 October 2025).
Tricco A C, Lillie E, Zarin W et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann Intern Med 2018; 169: 467–473.
Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol 2005; 8: 19–32.
UK Government. Inequalities in oral health in England. 2021.. Available at https://www.gov.uk/government/publications/inequalities-in-oral-health-in-england (accessed 1 October 2025).
Pau A K H, Croucher R. Self-reported oral health status and oral-health related behaviours of a sample of Chinese elders in Inner London, UK. a pilot investigation. Int J Health Promot Educ 2001; 39: 80–85.
Arora G, Mackay D F, Conway D I, Pell J P. Ethnic differences in oral health and use of dental services: Cross-sectional study using the 2009 Adult Dental Health Survey. BMC Oral Health 2017; 17: 1.
Rouxel P, Chandola T. Socioeconomic and ethnic inequalities in oral health among children and adolescents living in England, Wales and Northern Ireland. Community Dent Oral Epidemiol 2018; 46: 426–434.
Macfarlane T V, Beasley M, Macfarlane G J. Self-reported facial pain in UK biobank study: prevalence and associated factors. J Oral Maxillofac Res 2014; DOI: 10.5037/jomr.2014.5302.
Dykes J, Watt R G, Nazroo J. Socio-economic and ethnic influences on infant feeding practices related to oral health. Community Dent Health 2002; 19: 137–143.
McGrath C, Bedi R. An evaluation of a new measure of oral health related quality of life – OHQoL-UK(W). Community Dent Health 2001; 18: 138–143.
Elledge R O C, Khazaee-Farid R, Walker R J, Sundaram K, Monaghan A. A library-based ecological study to investigate the contribution of ethnicity to the incidence of oral cancer within health authorities in England and Wales. Br J Oral Maxillofac Surg 2011; 49: 42–46.
Conway D I, Quarrell I, McCall D R, Gilmour H, Bedi R, Macpherson L M D. Dental caries in 5-year-old children attending multi-ethnic schools in Greater Glasgow – the impact of ethnic background and levels of deprivation. Community Dent Health 2007; 24: 161–165.
McGurk M, Chan C, Jones J, O'Regan E, Sherriff M. Delay in diagnosis and its effect on outcome in head and neck cancer. Br J Oral Maxillofac Surg 2005; 43: 281–284.
Davies G M, Blinkhorn F A, Duxbury J T. Caries among 3-year-olds in Greater Manchester. Br Dent J 2001; 190: 381–384.
Dugmore C R, Rock W P. The effect of socio-economic status and ethnicity on the comparative oral health of Asian and White CaucAsian 12-year-old children. Community Dent Health 2005; 22: 162–169.
Gray M, Morris A J, Davies J. The oral health of South Asian five-year-old children in deprived areas of Dudley compared with White children of equal deprivation and fluoridation status. Community Dent Health 2000; 17: 243–245.
Marcenes W, Muirhead V E, Murray S, Redshaw P, Bennett U, Wright D. Ethnic disparities in the oral health of three- to four-year-old children in East London. Br Dent J 2013; DOI: 10.1038/sj.bdj.2013.687.
Pine C, Burnside G, Craven R. Inequalities in dental health in the North-West of England. Community Dent Health 2003; 20: 55–56.
Weston-Price S, Copley V, Smith H, Davies G M. A multi-variable analysis of four factors affecting caries levels among five-year-old children; deprivation, ethnicity, exposure to fluoridated water and geographic region. Community Dent Health 2018; 35: 217–222.
Bedi R, Lewsey J D, Gilthorpe M S. Changes in oral health over ten years amongst UK children aged 4–5 years living in a deprived multiethnic area. Br Dent J 2000; 189: 88–92.
Delgado-Angulo E K, Bernabé E, Marcenes W. Ethnic inequalities in dental caries among adults in East London. J Public Health 2016; DOI: 10.1093/pubmed/fdv097.
Newton J T, Robinson P G, Khan F, Gelbier S, Gibbons D E. Testing a model of the relationship between gender, ethnicity, clinical status and impact in older adults from minoritised ethnic groups. Gerodontology 2002; 19: 102–108.
Robinson P G, Bhavnani V, Khan F A et al. Dental caries and treatment experience of adults from minoritised ethnic communities living in the South Thames Region, UK. Community Dent Health 2000; 17: 41–47.
Delgado-Angulo E K, Bernabé E, Marcenes W. Ethnic inequalities in periodontal disease among British adults. J Clin Periodontol 2016; 43: 926–933.
Moore S, Ide M, Wilson R F et al. Periodontal health of London women during early pregnancy. Br Dent J 2001; 191: 570–573.
Newton J T, Khan F A, Bhavnani V, Pitt J, Gelbier S, Gibbons D E. Self-assessed oral health status of ethnic minoritised residents of South London. Community Dent Oral Epidemiol 2000; 28: 424–434.
Shaharyar S A, Bernabé E, Delgado-Angulo E K. The intersections of ethnicity, nativity status and socioeconomic position in relation to periodontal status: a cross-sectional study in London, England. Int J Environ Res Public Health 2021; 18: 10519.
Harper R S, Khan I, Chen R, Nevill A. Oral health inequalities in 0–17-year-old children referred for dental extractions under general anaesthesia in Wolverhampton. Community Dent Health 2020; 37: 247–252.
Delgado-Angulo E K, Mangal M, Bernabé E. Socioeconomic inequalities in adult oral health across different ethnic groups in England. Health Qual Life Outcomes 2019; 17: 85.
Delgado-Angulo E K, Zúñiga Abad F, Scambler S, Bernabé E. Is there a healthy migrant effect in relation to oral health among adults in England? Public Health 2020; 181: 53–58.
Agel M, Marcenes W, Stansfeld S A, Bernabé E. School bullying and traumatic dental injuries in East London adolescents. Br Dent J 2014; DOI: 10.1038/sj.bdj.2014.1123.
Ramchandani D, Marcenes W, Stansfeld S A, Bernabé E. Problem behaviour and traumatic dental injuries in adolescents. Dent Traumatol 2016; 32: 65–70.
Shujaat N G, Idris S H. Relationship Between Ethnicity and Traumatic Dental inuries among 14 year old children in Newham, a deprived area of London. Pak Oral Dent J 2008; 28: 289–294.
Ravaghi V, Durkan C, Jones K et al. Area-level deprivation and oral cancer in England 2012–2016. Cancer Epidemiol 2020; 69: 101840.
Csikar J, Aravani A, Godson J, Day M, Wilkinson J. Incidence of oral cancer among South Asians and those of other ethnic groups by sex in West Yorkshire and England, 2001–2006. Br J Oral Maxillofac Surg 2013; 51: 25–29.
Donaldson C D, Jack R H, Møller H, Lüchtenborg M. Oral cavity, pharyngeal and salivary gland cancer: disparities in ethnicity-specific incidence among the London population. Oral Oncol 2012; 48: 799–802.
Moles D R, Fedele S, Speight P M, Porter S R. The unclear role of ethnicity in health inequalities: The scenario of oral cancer incidence and survival in the British south Asian population. Oral Oncol 2007; 43: 831–834.
Moles D R, Fedele S, Speight P M, Porter S R, Silva I D S. Oral and pharyngeal cancer in South Asians and non-South Asians in relation to socioeconomic deprivation in South East England. Br J Cancer 2008; 98: 633–635.
Tataru D, Mak V, Simo R, Davies E A, Gallagher J E. Trends in the epidemiology of head and neck cancer in London. Clin Otolaryngol 2017; 42: 104–114.
Mandall N A, McCord J F, Blinkhorn A S, Worthington H V, O'Brien K D. Perceived aesthetic impact of malocclusion and oral self-perceptions in 14–15-year-old Asian and CaucAsian children in Greater Manchester. Eur J Orthod 2000; 22: 175–183.
Csikar J, Kang J, Wyborn C, Dyer T A, Marshman Z, Godson J. The self-reported oral health status and dental attendance of smokers and non-smokers in England. PLos One 2016; DOI: 10.1371/journal.pone.0148700.
Newton J T, Corrigan M, Gibbons D E, Locker D. The self-assessed oral health status of individuals from White, Indian, Chinese and Black Caribbean communities in South-east England. Community Dent Oral Epidemiol 2003; 31: 192–199.
Abdelrahim R, Delgado-Angulo E K, Gallagher J E, Bernabé E. Ethnic disparities in Oral Health Related Quality of Life among adults in London, England. Community Dent Health 2017; 34: 122–127.
Goff L M, Timbers L, Style H, Knight A. Dietary intake in Black British adults; An observational assessment of nutritional composition and the role of traditional foods in UK Caribbean and West African diets. Public Health Nutr 2015; 18: 2191–2201.
Bryant M, Sahota P, Santorelli G, Hill A. An exploration and comparison of food and drink availability in homes in a sample of families of White and Pakistani origin within the UK. Public Health Nutr 2015; 18: 1197–1205.
Sahota P, Gatenby L A, Greenwood D C, Bryant M, Robinson S, Wright J. Ethnic differences in dietary intake at age 12 and 18 months: The Born in Bradford 1000 Study. Public Health Nutr 2016; 19: 114–122.
Stone M A, Bankart J, Sinfield P et al. Dietary habits of young people attending secondary schools serving a multiethnic, inner-city community in the UK. Postgrad Med J 2007; 83: 115–119.
Al-Haboubi M, Klass C, Jones K, Bernabé E, Gallagher J E. Inequalities in the use of dental services among adults in inner South East London. Eur J Oral Sci 2013; 121: 176–181.
Acknowledgements
The authors would like to thank Dr Masuma Mishu, Dr Egle Petrauskiene, Dr Marta Paisi, Dr Janine Doughty, Sana Daniyal, Afshan Mirza and Dr Alex Blokland for their valuable assistance with the literature search and data extraction.
Author information
Authors and Affiliations
Contributions
GT, AH, RGW and RV contributed to the conceptualisation of the study. Data collection, literature screening, and data synthesis and interpretation was conducted by RV, MS, GT, and AH. Manuscript drafting was led by MS, GT, AH. RGW, SM, and KJ contributed to the review and editing of the manuscript. All authors revised and approved the final version.
Corresponding author
Ethics declarations
The authors declare no conflicts of interest related to this research. Ethical approval and consent was not required for this scoping review which only included data derived from publicly available studies.
Supplementary Information
Rights and permissions
Open Access. This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0.© The Author(s) 2025.
About this article

Cite this article
Stennett, M., Venturelli, R., Makhani, S. et al. Ethnic inequalities in oral health within the United Kingdom: a scoping review. Br Dent J (2025). https://doi.org/10.1038/s41415-025-8876-z
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41415-025-8876-z
