
Abstract
Introduction This pilot study investigates barriers and facilitators to Black dental students' engagement with academic careers in dentistry, focusing on underrepresentation in academia despite efforts to diversify the workforce.
Methods and results Through qualitative analysis of focus group discussions with Black dental students from two UK dental schools, several key themes emerged. Participants highlighted the importance of active patronage in addressing underrepresentation, advocating for proactive support systems beyond mere mentoring. They also emphasised the significance of various forms of capital – economic, cultural, and social – in shaping career trajectories and success in academia. Intersectionality, encompassing experiences of sexism, racism, and classism, emerged as a significant barrier, particularly affecting Black female students. Cultural specificity and individualism versus collectivism were also explored, revealing how cultural influences shape career choices and perceptions of academia.
Conclusion The study underscores the need for greater cultural competence and understanding among stakeholders to reduce barriers and promote inclusivity. While the study offers valuable insights, its limitations, such as sampling bias and cultural homogeneity among participants, should be acknowledged. Nevertheless, the findings call for concerted efforts from universities, policymakers, and research institutions to provide explicit support, foster inclusive environments, and promote diversity in dental academia. By addressing these challenges, academia can better reflect the populations it serves and ensure equitable opportunities for all aspiring dental professionals.
Key points
-
The study highlights the persistent underrepresentation of Black dental students in academia, prompting institutions to confront systemic gaps in diversity and inclusion.
-
Participants emphasised the need for active patronage – intentional, sustained support that goes beyond traditional mentoring – to help Black students navigate academic career paths.
-
The study sheds light on how intersecting identities (e.g., race, gender, class) uniquely affect Black dental students, particularly Black women, in their academic journeys.
-
It explores how access to economic, cultural, and social capital influences the likelihood of pursuing academic careers, thereby offering a broader understanding of structural inequities.
Similar content being viewed by others


Introduction
A workforce should ideally represent the population it serves so that everyone's needs can be met, and collectively individuals can feel valued. Diversity in the workplace means employing people of different ages, genders, ethnicities, sexual orientations, disabilities, cultural backgrounds, religion or belief. The current worldwide resurgence of the Black Lives Matter movement has fashioned attention on Black people's representation in workforces and while there are many different careers in dentistry, one area of dentistry identified in the literature as having low representation of Black people is the field of academia and research.1,2,3 The Black ethnic group, at 3.4%, is the third largest percentage of the population in England and Wales but within academic dentistry, just 1.1% of full-time equivalent clinical academics employed at dental schools in the United Kingdom (UK) identified as Black in 2017.4,5 This picture is reflected internationally with little change despite longitudinal efforts.6
Recent opinion pieces by Black dental students from Queen Mary University of London and University of Plymouth, Peninsula Dental School highlight a lack of understanding of pathways into an academic career in dentistry.7,8 Debate was sparked between these two institutions, which differ significantly in underpinning pedagogy, training and care pathways and models of delivery, staff and student demographics, and location (urban versus rural and coastal), about why this might be the case and whether the perceived barriers were generalisable across or unique to each locality.
This paper aims to explore the previous issues raised to improve understanding of the barriers faced by Black dental students in England engaging with academic careers in dentistry, and the facilitators that can improve engagement with these careers. By drawing on experiences from students at two dental schools in different regions of England, this paper aims to explore a range of perspectives on clinical academic careers among Black dental students, with the goal of identifying patterns that could inform efforts to bring about meaningful change.
Methods
A purposive sampling approach targeted known Black dental students from two dental schools in England through non-academic widening participation networks. Additional participants were recruited using a snowballing technique. Ethical approval (QMERC22242) and internal funding supported the study. Focus group logistics were collaboratively determined with students, ensuring co-creation. Training on how to run a focus group was provided to two volunteer students, who conducted the two-hour focus group based on a prepared topic guide (Appendix 1). Staff members assisted the opening and closing, introduced the study, obtained final consent, and ensured access to debriefing and support. Academic staff maintained distance during the focus group to encourage authentic dialogue, with consent granted for non-academic staff proximity for support. The session recording underwent verbatim transcription and thematic analysis using Braun and Clarke's techniques. Staff and students, guided by senior qualitative research experts, independently analysed the data. Regular team meetings on the Microsoft Teams platform facilitated consensus on final codes and themes, overseen by senior staff from each school.9
Findings
A focus group comprising nine participants from the University of Plymouth, Peninsula Dental School and Queen Mary University of London was conducted to explore perceived barriers and facilitators to pursuing academic careers in dentistry. Participants included students from years 2–4, as well as recent graduates.
A total of nine individuals participated in the study, comprising eight women and one man. At one participating dental school, 20 students (6% of the Bachelor of Dental Surgery population) identified as being from Black backgrounds in the year the study was conducted. Four of these students took part in the study, representing approximately 20% of the Black student population at that institution. Equivalent demographic data were not available for the second school. Most participants identified with a West African cultural background, which provides important context for interpreting the findings.
Initially, multiple codes were generated from the data through individual inductive categorisation of the entire data body corpus by all researchers. A deductive approach was then used to find patterns and create themes according to the research questions of barriers and facilitators to an academic career in dentistry. Themes were revised and honed via an iterative process of reviewing codes and returning to the data, revising and redefining themes in response to developing patterns and evolving interpretations. Consensus was reached by discussion with the whole group and the process was overseen and quality assured by the lead researchers with expertise in qualitative thematic analysis (SH and AR).
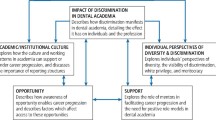
Table 1 summarises the key themes identified through qualitative analysis, illustrating both the barriers and facilitators influencing Black dental students' perceptions of academic career pathways in England. The key themes presented in the table are explored in detail in the subsequent text, with supporting participant quotes used to illustrate and substantiate each theme.
Active patronage
Active patronage addresses the underrepresentation of Black individuals in academic dentistry by offering proactive support beyond mentoring. The Royal College of Surgeons England, describe patronage as taking a more junior surgeon (or trainee/student) under your care and giving advice.10
Active patronage was seen to have been useful in guiding Black dental students towards undiscovered opportunities, filling the void left by the absence of Black academic role models. Active patronage, encompassing mentorship, role models, and support systems, was thought to instil confidence for aspiring openly. Participants suggested that while achieving racial parity in academia may be distant, aid from individuals of various backgrounds is crucial for progress. It was suggested that those individuals need not be Black:
-
‘That's what we're asking for…someone that's gone the way, that knows the way, to show the way. We're not asking you to walk it for us, because you can't. Let us do that but support us while we're doing it' (P5)
-
‘You need someone to champion you. It makes a huge difference' (P3)
-
‘I think open door policy is terrible. You say your door is open, I'm scared to go into your door…' (P7)
-
‘I don't even need the mentor itself to be Black. I just need someone who'll appreciate me as a person and just want to help me' (P4).
Capital
Bourdieu's theory highlights the importance of capital and social position in determining an individual's success in dentistry. He argued that social, cultural, and economic capital are distinct forms of ‘currency' for success in society.11
Bourdieu's classification of capital was recognised from the participant comments as having influenced the reported experiences of Black dental students, highlighting the significance of these factors in their career progression.
Economic capital
This relates to anything that can be converted into money or financial consideration that can help or hinder Black students secure or succeed in academia or research:11
-
‘The idea of not working, not earning, for a period of time does not sit well with me in my spirit. It doesn't make any sense. How am I supposed do that?' (P7)
-
‘Money is a big thing. Not everyone can afford to do things unpaid' (P1)
-
‘I didn't even know there were paid options. It just felt like academic stuff was for people with time and money' (P8).
Cultural capital
Bourdieu defined cultural capital as one's knowledge and familiarity with the dominant culture of a society.11
It was reported that the knowledge, skills and education associated with the dominant cultures in dentistry could help or hinder Black students secure or succeed in academia or research:
-
‘If you don't have connections, it's harder to know where to even start' (P6).
Social capital
Exploring social capital, participants highlighted challenges in building positive relationships in academia, noting easier interactions between staff and students from other ethnic backgrounds hindering success for those feeling like outsiders:
-
‘I do not know a Black dentist, somebody who will speak to you in your language …of course you get along with them [white students] better because you guys have more in common. So what am I supposed to do? I feel already crossed out of so many spaces. I think that might also be the case sometimes in, in academic settings' (P6).
Cultural specificity
Individual culture influences career progression, shaping motivations and preferences. In this study, mainly comprising West African women, cultural specificity within this subset significantly impacted career choices, shaping identity and professional paths from the outset:12,13
-
‘Our culture values humility and teamwork, which sometimes isn't seen as “leadership” in academic spaces' (P8)
-
‘The way we communicate and express ourselves isn't always understood' (P2)
-
‘There's a difference between how African and Caribbean parents approach education and gender expectations' (P6)
-
‘I was taught to respect authority. That doesn't mean I know how to challenge a professor if I disagree' (P3)
-
‘Our dynamic in the Black culture is close…everyone is your auntie and uncle. They take you under their wing and just look after you. Like, if I needed help in dental school when I knew there was a Black tutor or someone that I could go to, I would have a reassurance that they would just help me' (P1).
Intersectionality
Intersectionality recognises that individuals' lives are shaped by the interplay of power, privilege, and inequality across multiple identities, beyond singular categories like gender, race, sexuality, or class.1
Intersectionality was revealed in sub-themes relating primarily to sexism, classism, racism, identity, and ethnicity. Academic interactions were reported to have exposed gender bias and racial discrimination, impacting Black students who felt they also had to adapt their behaviour due to class. Identity challenges, stereotypes, and biases complicated entry into dentistry and academia for Black women:
-
‘My suffering is the suffering of dental school and then being Black and then being a woman. That's intersectionality…the suffering is just compounded. My suffering comes from a lot of different areas of life' (P3)
-
‘As Black students, we must question everything that we do. Every interaction we have, we're already thinking about, “has my race modified how this person thinks of me? how do I change my behaviour? If my hair looks like this, will I look less professional?”' (P3)
-
‘As a Black woman, you're navigating race and gender. Sometimes I wonder which one's affecting me more today' (P4)
-
‘It's not just about being Black; it's being a Black woman from a working-class background' (P7).
Individualism versus collectivism
Drawing from Hofstede's Cultural Dimensions Theory,14 this theme explored individual characteristics within a collective context. Participants discussed being pioneers and viewed individual success as a potential catalyst for broader Black student involvement in dentistry. Challenges included feeling like outsiders and academic disparities due to limited Black student representation. Identified codes encompassed mentorship, community support, in-group/out-group dynamics, role models, and self-motivation. Participants believed that prior individual successes in other areas indicated potential success for Black students in dentistry, positioning personal aspirations as facilitators for broader collective entry into the dental field and academia:
-
‘It's all about individual success here, but we're brought up thinking about the whole community' (P9)
-
‘There's not many spaces where we can be us, together' (P3)
-
‘I'm like the Martin Luther King of my generation where I'm the first Black everything in this. You know, so even in dentistry, I've been the first Black. I've never seen any other Black person go down this path. My turn, I will do it' (P7).
The discussion revealed a strong feeling of camaraderie between Black dentists and Black dental students due to their shared background and experiences:
-
‘I shadowed an orthodontist in the summer. That sort of influenced me, maybe because he was Black it allowed me to have some sort of mentor to look up to' (P8).
It was noted that the lack of shared characteristics and unconscious camaraderie was also relevant and that the world of dental academia is worse off than other areas of the profession:
-
‘I feel like going into academia is going into a place where I know I'm going to be alone. Whereas if I look at any other specialities, I'm sure I could find a Black ortho or Black endo or Black oral surgeon, people that would listen to me and be okay' (P4)
The findings shed light on multifaceted challenges faced by Black dental students, emphasising the need for facilitators such as active patronage, addressing capital disparities, understanding intersectionality, recognising cultural specificity, and balancing individualism with collective support. These insights contribute to discussions on enhancing diversity and inclusivity in dental academia.
Discussion
Active patronage and mentorship
This pilot study focuses on the barriers and facilitators Black students face in considering clinical academic careers in dentistry.7,8 The focus group discussions revealed students' desire for earlier exposure and opportunities to participate in academia but lack of awareness of opportunities. They recommended transparency, overt tutoring, and active expert input as specific areas to support this. Sanchez and co-workers identified the need for deliberate support.15 A UK-based publication observed that academic dentistry is failing to attract a new generation of academics, further exacerbated by shortcomings in ethnic diversity.3
A recent systematic review highlights systems-level initiatives, such as the National Institute for Health and Care Research, which are expanding requirements to include all nine protected characteristics in the Equality Act 2010 in UK academia and research to promote ethnic diversity.13 Faculty diversity is also influential, with participants acknowledging the negative impact a lack of diversity could have on students. The wider literature suggests that faculty may avoid discussing cultural diversity issues due to uncertainty about how to approach the topic.16
Understanding the impact of social, personal, and professional factors on Black students' pursuit of clinical academic careers is crucial. An intersectional lens is needed to improve understanding, communication, and treatment of diverse groups. Mentorship plays a pivotal role in shaping minority students' trajectories in academia.17 This study echoes explicitly perspectives in existing literature, notably the importance of active mentorship,18 where the mentee is not left to set the agenda of the relationships and its outcomes. It is important to note that the use of the term mentor and mentoring is recognised in this study in the context of expert advisor and is therefore labelled ‘patronage' as per the definition used in the Royal College of Surgeons of England 2019 and 2022 mentoring guidelines.19
The findings highlight clear implications for academic institutions: support strategies must prioritise authenticity and proactive engagement from faculty members, including the provision of clear and structured guidance to help students navigate academic pathways.
One finding that challenges conventional assumptions is the diminished emphasis on racial concordance in mentorship. While the underrepresentation of Black role models in dentistry is well-documented,7 participants in this study highlighted that the most valued aspects of mentorship were authenticity, empathy, and support, rather than shared racial identity. This aligns with existing literature suggesting that meaningful mentorship can transcend racial matching.20 Given that only around 3% of the dental workforce identifies as Black, it is important that academic institutions foster inclusive and supportive mentoring relationships irrespective of racial background.
A critique also emerged regarding the perceived limitations of passive ‘open door' mentorship policies. Participants expressed that such approaches may place undue responsibility on students, particularly those from underrepresented backgrounds, to initiate contact, often in unfamiliar or intimidating academic environments. This supports literature highlighting the importance of proactive engagement by mentors, rather than relying on students to seek support themselves.21 The findings suggest a need to reconsider and strengthen institutional mentoring policies to ensure they are truly accessible and effective.
The desire would be to have professionals from all races and backgrounds become attentive to the struggles faced by the current generation of Black dentists and dental students and willingly choosing to walk alongside them, pointing them in the right direction to succeed in the profession to allow a cycle of mentorship and aspiration for the following generations to come.
Capital (economic, social, cultural)
The ability to detect the extent capital of all kinds plays in progressing the field of dentistry which can be highlighted even before one undergoes working in the field. From the point of looking for work experience to seeking advice on specialist training in the profession, it is evident that ‘who you know' and ‘what you know' matters. If finding work experience is difficult, having a family member that is a dentist will alleviate that struggle, which by many is still seen as a prerequisite for studying dentistry. However, many Black dental students cannot boast in the knowledge of relations in their family to a dentist.
Understanding the different forms of capital and how they interact is seen to be key to succeeding in dental school and pursuing a career in academia. Participants in the study expressed concerns over the high cost of pursuing academia, including the opportunity cost of not working while training or studying, and the perception that academia is not a well-paying field, consistent with other research.22 Interestingly, there are established paid pathways into academia, but none of the participants were aware of them. This highlights a need for better dissemination of information, which could increase the number of Black individuals pursuing academia.
The data suggests that Black dental students may feel isolated and unsupported during their undergraduate experience, due to their small numbers in the field and lack of social and cultural capital compared to other ethnic groups. This has led to a negative perception of their future in academia. Recent research supports the extrapolation of negative undergraduate experiences to postgraduate courses.23 Improving the undergraduate experience by increasing faculty support and creating a more culturally competent learning environment may be key to improving Black dental students' perception of future postgraduate education and reducing barriers to academia.
Cultural specificity and career motivation
This study reveals that an individual's culture significantly influences career progression, as different values can lead to different motivations, preferences, and outlooks that can impact professional paths. African cultures have unique customs and beliefs that can have a significant impact on career choices, such as the belief that children have the primary responsibility of growing up and providing financial support for their families. This can lead to an emphasis on career paths that are seen as having the potential to bring in higher income, while academia is typically not seen as the primary option.
Other African cultures and Caribbean cultures may have different attitudes towards career progression. African cultures often emphasise the importance of supporting one's family and is often seen as a responsibility of both genders, while in the Caribbean, traditional gender roles are sometimes more pronounced. African cultures often have strong respect for authority figures and expect individuals to work hard and stay within their social class, while Caribbean cultures may be more open to challenging the status quo and taking risks in pursuit of career advancement.12,24
The environment plays a major role in motivating people to choose certain occupations, with most youths choosing occupations to please their parents or guardians.12 Career choice is influenced by student characteristics, beliefs about self, culture, information technology, mentors, income of parents, and social network.24 African cultures have their own unique set of customs and beliefs which can have a significant impact on career choices. For example, in some parts of Western Africa, parents want their children to experience success, financial and otherwise, and these careers (doctor, lawyer, engineer) have traditionally been seen as stable, socially prestigious, and financially sound.25
In Nigeria, dental students' top reasons for interest in the study of dentistry are motivation from parents, motivation from family and relatives, and the increased prospect of being self-employed.26,27,28 This relates directly to the individualism versus collectivism element of Hofstede's cultural dimensions and the way Black students may relate to their communities, which may contrast with white and/or Asian students.
Greater cultural competence and understanding by all may help reduce barriers and increase the efficacy of facilitators for these students to enter and pursue an academic career. An implication of these findings is the possibility of providing better transparency and advertisement regarding career pathways, pay, flexible working opportunities, and more. With a greater understanding, students would be able to explain their career progression, job security, and salary expectations to their families and make plans accordingly, especially if they have the responsibility of looking after their family financially.
Intersectionality
Intersectionality, rooted in Black feminism and critical race theory, emerged as a significant barrier to pursuing specific career pathways.29,30,31 This theory recognises that individuals' lives are shaped by the interplay of power, privilege, and inequality across multiple identities, beyond singular categories like gender, race, sexuality, or class.32,33,34 Black female students, as underrepresented minorities, reported experiencing a complex interplay of sexism, racism, and classism in dental school and academia, a recognised issue in STEM (science, technology, engineering, and mathematics); fields historically dominated by white neurotypical men. The consequences include discrimination, insufficient support, and limited career progression for women of colour, emphasising the urgency of addressing intersectionality in research and academia to achieve true equity.35
To combat these injustices, a coordinated effort involving policymakers, grant holders, universities, and research institutions, with the active involvement of scientists with intersecting minority identities, is crucial.36,37,38 Creating an inclusive career development framework, acknowledging intersectional identities, and ensuring equitable progression in STEM subjects are essential steps. Additionally, public endorsement and promotion of intersectionality by policymakers, academic journals, grant holders, and institutions are necessary for increasing diversity in academia. Efforts to ‘decolonialise' universities – challenging and remaking imperial and colonial pedagogies – also play a role in promoting diversity. However, the complexity of decolonising dental and medical curricula goes beyond superficial changes, requiring a nuanced approach that considers various influencing discourses and avoids becoming a tokenistic exercise led by those already holding power and privilege.39
Individualism versus collectivism
This theme highlights how cultural orientations, specifically collectivism, may shape Black dental students' perspectives on academic careers. Participants, particularly those from West African backgrounds, often framed their ambitions not only in personal terms but also in relation to their wider community. For some, the decision to pursue academia was seen as a pioneering step, a way to create a pathway for others and fulfil a broader responsibility to increase Black representation within the profession.
Collectivist values, such as shared achievement, community uplift, and role modelling contrasted with the dominant culture of individualism in academia, which emphasises self-promotion, competition, and solitary success.40 This cultural mismatch may explain participants' feelings of discomfort or isolation when considering academic careers, as reflected in narratives around being ‘the only one' or fearing loneliness in academic spaces. Such insights suggest that academic institutions may need to recognise and accommodate more collectivist values within their culture and mentoring models.
Furthermore, the perception that other specialities in dentistry offer greater opportunity for shared identity and camaraderie than academia may deter talented individuals from considering teaching and research roles. Participants' desire to ‘give back' and act as role models could be a powerful facilitator, if institutions create culturally affirming spaces where this motivation is recognised and supported.
This finding aligns with research that stresses the importance of cultural competence in dental education.41 Understanding how collectivist values influence career motivation and progression can inform both curriculum design and faculty development, helping to create more inclusive and supportive environments for racially minoritised students. Future research should explore how these dynamics vary across Black communities, including African and Caribbean backgrounds, to develop a more comprehensive understanding of how cultural orientation impacts academic aspirations.
Strengths and limitations
This study's strengths lie in its qualitative approach, offering a detailed insight into Black dental students' perceptions of entering clinical academic careers. However, limitations arise from the purposive sampling of nine participants across only two dental schools in England, the potential for self-selection bias, and the predominantly West African cultural background of participants, which may not capture the full diversity of experiences among Black dental students.
The limited gender diversity within the sample restricts deeper exploration of how gender may influence access to academic careers among Black dental students. Although existing literature suggests minimal gender-based differences in motivations for studying dentistry, this study identified subtle patterns that may reflect the impact of gendered cultural expectations and socialisation.26,42,43,44,45
Further research with more balanced gender representation is needed to better understand how gender, in interaction with race and other contextual factors, may shape academic career trajectories.
Despite limitations, the study's methodological rigour supports the trustworthiness of its findings. The insights may be transferable to similar educational contexts46,47,48 and offer theoretical relevance for understanding the experiences of students from minority ethnic groups in dental education.
Conclusion
This study amplifies the voices of Black dental students from two English dental schools, shedding light on the barriers they face in pursuing academic careers. Participants revealed that unequal access to support, limited networks, and a lack of culturally resonant role models make the academic path more difficult to navigate.
Facilitators to make this process more effective include active patronage and proactive support; enhancing cultural competence and using an intersectional lens; highlighting and promoting successful pioneering individuals; and coordinating efforts across higher education institutions, the regulator and policymakers to develop, publicise and appropriately remunerate inclusive career frameworks.
To truly diversify the clinical academic workforce, we must move beyond passive inclusion and commit to active, visible, and sustained support. This means targeted mentoring, skill-building, and emotional backing delivered without students having to ask. Equity must be built into every stage of the academic journey.
Universities, deaneries, and professional bodies have a clear mandate: to dismantle structural obstacles and create pathways that empower Black students to thrive in academic dentistry. Co-created with those most affected, this study offers actionable insights to guide institutional change and resource investment.
Data availability
The data that support the findings of this study are not publicly available due to the potential for identifying participants and the sensitive nature of the qualitative data. Requests for access to anonymised excerpts may be considered on a case-by-case basis by the corresponding author, subject to ethical approval.
References
Nichols S, Stahl G. Intersectionality in higher education research: a systematic literature review. High Educ Res Dev 2019; 38: 1255–1268.
Lala R, Baker S R, Muirhead V E. A critical analysis of underrepresentation of racialised minorities in the uk dental workforce. Community Dent Health 2021; 38: 142–149.
Burns L, Coelho C, Addy A. Ethnic diversity in academic dentistry in the United Kingdom. Eur J Dent Educ 2022; 27: 610–613.
Office for National Statistics. Ethnicity and national identity in England and Wales 2011. 2012. Available at https://www.ons.gov.uk/peoplepopulationandcommunity/culturalidentity/ethnicity/articles/ethnicityandnationalidentityinenglandandwales/2012-12-11 (accessed 13 March 2023).
Watson N, Tang P, Knight E. Report on Survey Results of Clinical Academic Staffing levels in UK Dental Schools at 31 July 2017. Dental Schools Council, 2018.
Cain L, Brady M, Inglehart M R, Istrate E C. Faculty diversity, equity, and inclusion in academic dentistry: revisiting the past and analyzing the present to create the future. J Dent Educ 2022; 86: 1198–1209.
Kadiyo T, Mellish V. Black Lives Matter: the impact and lessons for the UK dental profession. Br Dent J 2021; 230: 134–142.
Coelho C, Ukoha O, Onamusi V et al. ‘It is difficult to think about becoming what you have never seen': Black students' reflections around a career in academic dentistry. Br Dent J 2022; 232: 142–146.
Braun V, Clarke V. What can ‘thematic analysis' offer health and wellbeing researchers? Int J Qual Stud Health Well Being 2014; 9: 26152.
Royal College of Surgeons of England. Mentoring: a guide to good practice. 2018. Available at https://www.rcseng.ac.uk/-/media/files/rcs/standards-and-research/standards-and-policy/good-practice-guides/new-docs-may-2019/rcs-_mentoring.pdf (accessed 1 November 2023).
Weininger E B. Pierre Bourdieu on Social Class and Symbolic Violence. 2003.
Okojide A, Adekeye O A, Bakare E. Factors influencing career choice among undergraduates in covenant university, Nigeria. ICERI2018 Proceedings, 2018.
Akosah-Twumasi P, Emeto T I, Lindsay D, Tsey K, Malau-Aduli B S. A systematic review of factors that influence youths career choices – the role of culture. Front Educ 2018; DOI: 10.3389/feduc.2018.00058.
Hofstede G. Dimensionalizing cultures: the Hofstede Model in context. Online Readings Psychol Cult 2011; DOI: 10.9707/2307-0919.1014.
Sánchez J P, Peters L, Lee-Rey E et al. Racial and ethnic minority medical students' perceptions of and interest in careers in academic medicine. Acad Med 2013; 88: 1299–1307.
Powell Sears K. Improving cultural competence education: the utility of an intersectional framework. Med Educ 2012; 46: 545–551.
Brown W C, Magaña L, Crespo C J, White W B. Mentoring underrepresented minoritized students for success. Pedagogy Health Promot 2021; DOI: 10.1177/23733799211054086.
Ghitulescu B E, Khazanchi S, Tang Z, Yu Y. One size does not fit all: the role of mentoring context in proactive individuals' scholarly impact. Career Dev Int 2021; 26: 888–905.
Royal College of Surgeons of England. Toolkit introduction. Available at https://diversity.rcseng.ac.uk/develop-and-learn/mentorship/ (accessed 1 November 2023).
Fries-Britt S, Snider J. Mentoring outside the line: the importance of authenticity, transparency, and vulnerability in effective mentoring relationships. New Dir Higher Educ 2015; DOI: 10.1002/he.20137.
Eller L S, Lev E L, Feurer A. Key components of an effective mentoring relationship: a qualitative study. Nurse Educ Today 2014; 34: 815–820.
Pásztor A, Wakeling P. All PhDs are equal but…institutional and social stratification in access to the doctorate. Br J Sociol Educ 2018; 39: 982–997.
Badrie R, MacDonnell J, Patel B A. Barriers to pursing postgraduate research study among final year undergraduate minority ethnic students at a post-1992 UK university. Equity Educ Soc 2023; 2: 206–222.
Kerka S. Career Development and Gender, Race, and Class. Citeseer, 1998.
Akosah-Twumasi P, Emeto T I, Lindsay D, Tsey K, Malau-Aduli B S. Restrictive reciprocal obligations: perceptions of parental role in career choices of Sub-Saharan African migrant youths. Front Psychol 2021; 12: 576193.
Khami M R, Murtomaa H, Jafarian M, Vehkalahti M M, Virtanen J I. Study motives and career choices of Iranian dental students. Med Princ Pract 2008; 17: 221–226.
Crossley M L, Mubarik A. A comparative investigation of dental and medical student's motivation towards career choice. Br Dent J 2002; 193: 471–473.
Folayan M O, Sofola O O, Khami M R et al. Study motives, career choices and interest in paediatric dentistry among final year dental students in Nigeria. BMC Med Educ 2014; 14: 130.
Carbado D W, Crenshaw K W, Mays V M, Tomlinson B. Intersectionality: mapping the movements of a theory. Du Bois Rev 2013; 10: 303–312.
Wyatt T R, Johnson M, Zaidi Z. Intersectionality: a means for centering power and oppression in research. Adv Health Sci Educ Theory Pract 2022; 27: 863–875.
Chellappa S L. Intersectional inequities in academia. Lancet 2023; 401: 1076.
Cech E A. The intersectional privilege of white able-bodied heterosexual men in STEM. Sci Adv 2022; DOI: 10.1126/sciadv.abo1558.
Täuber S. Women academics' intersectional experiences of policy ineffectiveness in the European context. Front Psychol 2022; 13: 810569.
Schucan Bird K, Pitman L. How diverse is your reading list? Exploring issues of representation and decolonisation in the UK. Higher Educ 2020; 79: 903–920.
Ali K, Winter J, Webb O, Zahra D. Decolonisation of curricula in undergraduate dental education: an exploratory study. Br Dent J 2022; 233: 415–422.
Bhambra G K, Gebrial D, Nişancıoğlu K. Decolonising the University. London: Pluto Press, 2018.
Ali K, McColl E, Tredwin C, Hanks S, Coelho C, Witton R. Addressing racial inequalities in dental education: decolonising the dental curricula. Br Dent J 2021; 230: 165–169.
Hartland J, Larkai E. Decolonising medical education and exploring white fragility. BJGP Open 2020; DOI: 10.3399/BJGPO.2020.0147.
Harold L. What Is white fragility? Available at https://www.verywellmind.com/white-fragility-4847115 (accessed 1 November 2023).
Chuenjitwongsa S, Bullock A, Oliver R G. Culture and its influences on dental education. Eur J Dent Educ 2018; 22: 57–66.
Fatehi K, Priestley J L, Taasoobshirazi G. The expanded view of individualism and collectivism: one, two, or four dimensions? Int J Cross Cult Manag 2020; 20: 7–24.
Hallissey J, Hannigan A, Ray N. Reasons for choosing dentistry as a career–a survey of dental students attending a dental school in Ireland during 1998–99. Eur J Dent Educ 2000; 4: 77–81.
Sofola O O, Uti O G, Akpene O I. Does exposure to dental education change the perceptions of Nigerian students to dentistry as a profession? Eur J Dent Educ 2008; 12: 159–162.
Orenuga O O. A survey of challenges and career aspirations of clinical dental students in Nigerian universities. Niger Dent J 2009; 17: 19–23.
Butters J M, Winter P A. The effects of gender and race on practice pattern preferences of dental students. J Am Coll Dent 1999; 66: 39–46.
Lincoln Y S, Guba E G. Naturalistic Inquiry. California: Sage Publications, 1985.
Maxwell J A, Chmiel, M. Generalization in and from qualitative analysis. In Flick U (ed) The SAGE Handbook of Qualitative Data Analysis. pp 540–533. London: SAGE Publications Ltd, 2014.
Carminati L. Generalizability in qualitative research: a tale of two traditions. Qual Health Res 2018; 28: 2094–2101.
Author information
Authors and Affiliations
Contributions
AR, FO, TAJK, OMU, CC and SH contributed to the conception and design of the study, data acquisition and interpretation, conducted all analyses, and were involved in drafting and critically revising the manuscript. VBO contributed to the study design, data acquisition and interpretation, and supported manuscript drafting and revision. RAAO, NME, OHA, AOOA, MTO, KS-B and AMAA contributed to data transcription and interpretation. NE also contributed to manuscript drafting. AR and JM contributed to the conception and design of the study, data acquisition and interpretation, and critically revised the manuscript. ND contributed to the study conception and design. All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
The authors declare no conflicts of interest. Ethical approval (QMERC22242) supported the study and consent to participate was obtained.
Rights and permissions
Open Access. This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0.© The Author(s) 2025.
About this article

Cite this article
Ranauta, A., Onwudiwe, F., Kadiyo, T. et al. Barriers and facilitators to engaging with academia: a Black dental student perspective – pilot study. Br Dent J (2025). https://doi.org/10.1038/s41415-025-8910-1
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41415-025-8910-1
