
Abstract
Introduction Hospitals have a burden of responsibility for their contribution to climate change and pollution. The Hospital Environmental Audit and Improvement Tool (HEAIT) provides a comprehensive hospital-wide stakeholder engagement to mitigate hospital environmental impacts. HEAIT is a metric-based institutional advocacy tool for auditing, evaluating and improving environmental practice in hospitals.
Method HEAIT was implemented in the Department of Restorative Dentistry, Charles Clifford Dental Hospital, Sheffield Teaching Hospital NHS Trust, Sheffield, UK. A thematic scoping review identified all the environmental impacts arising from the practice of oral healthcare: 124 action statements across 16 specific theme categories that were coded and categorised according to: i) level of importance and environmental benefit; and ii) degree of implementation difficulty. Progress in each activity area is audited and graded (point allocation), identifying areas for improvement and measurable goals for improved performance.
Results The toolkit was mapped against industry standard audit and improvement parameters. All parameters have been addressed, with identification of required further actions. The calculator was compliant against the audit criteria providing a baseline of environmental sustainability activity.
Conclusion HEAIT provides an effective and validated way of achieving real engagement of the whole workforce in a meaningful manner to achieve measurable goals as part of a collaborative environmental mitigation strategy.
Key points
-
There is an imperative need to identify and mitigate the environmental impacts that arise from the secondary care health sector.
-
The Hospital Environmental Audit and Improvement Tool (HEAIT) is an evidence-based instrument for auditing, evaluating and improving environmental practice in hospitals.
-
The HEAIT will systematically assess and measure all the environmental impacts that arise in a hospital to achieve meaningful mitigation. It does so in an iterative way with staff engagement from across all sectors and career grades.
Similar content being viewed by others
Introduction
Planetary health is human health and are both dependent on healthy flourishing natural systems and the wise stewardship of those natural systems.1 Climate change is not only detrimental to the physiology of patients but also impacts the operations and effectiveness of health services. Although the World Health Organization has called climate change ‘the greatest threat to global health in the twenty-first century', many hospital priorities do not reflect the urgency of this danger to human health, including oral health.
The environmental impacts of healthcare provision in hospitals are associated with high energy consumption, waste production, and resource usage. A 2019 estimate places healthcare's global carbon footprint at 4.4% of the world's total greenhouse gas emissions and the US healthcare activities accounting for 8.5% of the nation's greenhouse gas emissions.2,3 A recent systematic review identifies that 50–75% of the total emissions were scope three (greenhouse gas protocol), primarily attributed to disposables, equipment and pharmaceuticals.4
From a waste perspective, hospitals and laboratories contribute to over five million tonnes of waste annually.5 The essential requirement for hospitals to operate in a continuous manner creates huge energy consumption that contributes to the environmental impacts.6 In this context, it is incumbent on all hospital stakeholders to mitigate the health impacts of climate change and other anthropogenic environmental changes. This ethical consideration is underlined by local and national objectives that enforce a top-down approach to its management. Within the NHS in the UK, this has been legislated as a net zero target of directly controlled emissions by 2040 and those we can influence by 2045.7 We can achieve this through a systematic and pragmatic combination of activities that promote knowledge awareness, audit and service evaluation exercises and focused high-impact research.
A bottom-up approach from individual departments that drives collaborative active staff engagement, is arguably more effective with individual stakeholder engagement. The challenge is that the environmental sustainability (ES) metrics of our current hospital practice are not quantified, nor are the steps required to improve this. There is no unified and comprehensive tool that will measure and report on ES practice in secondary care. There is a need for a quality improvement audit tool that will systematically assess and measure all the ES impacts that arise in a hospital. This should be based on best evidence-based practical knowledge, to mitigate these impacts in the different areas that the hospital can influence, such as waste management, recycling or patient transport. Such a tool should be to continuously and systematically audit environmental sustainability activities in a hospital to improve planetary health awareness and impact mitigation. A strategic objective for this tool is to ensure staff engagement across all sectors and career grades with proactive multi-stakeholder corrective measures. Activities associated with the audit can then be tracked over time to demonstrate meaningful improvement. Specific objectives for the tool are:
-
Systematically audit activity across all categories of ES
-
Promote improvement through an iterative audit-activity programme
-
Encourage and engage staff and services from all sectors and career grades in the conduct of ES projects
-
Establish achievable evidence-based targets that can be accomplished in a practical and pragmatic manner
-
Achieve meaningful environmental sustainability impacts
-
Award discrete metrics for each ES activity that cumulatively lead to an institutional grade
-
Encourage corporate and national accountability for ES in hospitals
-
Drive service improvement and cost reduction
-
Provide a model that can be translated to all secondary care hospitals.
The case study presented in this manuscript focuses on oral health as a representative example of a well-defined entity. The application of the audit tool to this secondary care hospital enables translation and escalation to any other secondary care hospital setting. A series of diverse and closely interlinked themes have been identified from the current literature.8,9 These themes determine the environmental sustainability of oral health provision on a world-wide basis that have been further validated and endorsed in the consensus on environmentally sustainable oral healthcare.10 They cover, in a comprehensive manner, all the environmental impacts arising from the practice of oral healthcare, in its widest context:8,9,10
-
Environmental impacts (carbon dioxide equivalent, air and water)
-
Reduce, reuse, recycle and rethink
-
Policy and guidelines
-
Biomedical waste management and plastics
-
Procurement
-
Research and education
-
Materials.
The expert knowledge arising from the ‘consensus on environmentally sustainable oral healthcare' forms the backbone of an earlier quality improvement tool developed for the primary care oral healthcare sector – the Sustainability in Dentistry Toolkit, created and hosted by the Sustainability in Dentistry Task Team of the World Dental Federation.11 This project seeks to translate this work into a secondary care environment. The sustainability in dentistry toolkit provides dentists and their teams in dental practices with a set of challenges that are categorised according to the ease of implementation and their importance in mitigating environmental impacts. In this way, the dental team can earn bronze (easy and essential), silver (moderately difficult and moderately important) or gold (difficult and aspirational) recognition awards for their practice. It is an evidence-based tool that captures all ES impacts arising from the provision of primary dental care. Engagement with the toolkit enables the dental team to mitigate their environmental impacts in an engaging, progressive and collaborative approach. The success of this toolkit in primary care presents an opportunity to translate the concept to secondary care hospital settings. The aim of this study was to create a toolkit that can be used in secondary care, considering the nuances of a hospital environment.
Method
A Hospital Environmental Audit and Improvement Tool (HEAIT) was developed to meet most of the criteria identified for the provision of an effective corporate audit and improvement tool. The tool was created and trialled as a proof of concept for the restorative department of a dental hospital (Charles Clifford Dental Hospital, Sheffield, UK). The methodology, and the sections within it, that are used to report this healthcare improvement initiative follows the structure of a corporate internal audit and improvement tool (Table 1).12,13,14
Development of the tool
Scope
The literature identified in the scoping reviews by Martin et al. (2021) was analysed using a thematic analysis following the approach laid out by Braun and Clarke (2006).8,9,15 The range of the themes identified in the literature enabled the authorship to create a comprehensive list of evidence-based ES action statements that are arranged into the different categories of a dental hospital context (Table 2). Each of these categories is described in detail in the aforementioned supporting literature review that was used to derive them. The outcome consisted of 124 action statements across 16 specific categories. The standards for quality improvement reporting excellence guidelines have been used to provide a framework for reporting this quality improvement innovation that is designed to mitigate hospital-derived environmental impacts and improve healthcare.16
Relevance and alignment
This is derived from the previously identified comprehensive review of the literature and further evaluation in expert focus group discussions held within the department. The outcome was a consensus classification of the action statements mapped to the identified literature themes, that avoids repetition and is aligned to the operation of the hospital setting (Table 2). The classification and statements are derived from the themes in the literature and informed by knowledgeable and experienced experts in restorative dentistry in secondary care settings and environmental sustainability in oral healthcare.
Critical risk inclusion
In this context, critical risk management considers the effective allocation of key indicators and metrics used in the categorisation of tasks. To ensure that all critical risk actions are covered, the action statements are coded and categorised according to two specific attributes and three variables arranged in an implementation relational table (Fig. 1): i) Y axis – the level of importance for environmental benefit (essential, important and aspirational); and ii) X axis – the degree of implementation difficulty (easy, moderate and difficult). This concept is adapted from the widely accepted and established Ebel standard setting concept for pedagogic assessments.17 For example, switching off the lights in empty clinics is ‘essential and easy', whereas installing roof-top solar panels is ‘aspirational and difficult'. The use of these two attributes and the three variables within it enables the engagement and delivery of tasks in a practical and pragmatic manner. In the manner of the primary care toolkit described previously, the cells use the red-amber-green (RAG) coding to represent the level of importance and implementation feasibility. A focus group, including the authorship, attributed each ES action statement (or sub-statement) to the most appropriate cell in the implementation relational table (Fig. 1). This provides a two-letter code for each statement that identifies the two parameters, e.g., an action statement that is ‘essential and easy' is labelled ‘E-E' and one that is ‘important and moderately difficult' is labelled ‘I-M'.

Implementation relational table. Easy-essential (green), moderate-important (amber) and difficult-aspirational (red)
Implementation of the tool
The current user interface uses a combination of MS Excel and Word documents with all categories arranged consecutively in the manner of a questionnaire allowing user input for each of the action statements (Fig. 2). Team leads are appointed to manage specific projects, monitor and report progress periodically as required. Team collaboration is assured by inviting all staff (all sectors and career grades) in the hospital to actively participate and engage, in small working groups, to identify and deliver proactive multi-stakeholder corrective measures. This brings together previously isolated action statement projects under one overall umbrella allowing shared learning. The HEAIT project and the actions within can be developed at a department or hospital level; the latter being preferable. Teams within a specific department will be able to engage with the required hospital infrastructure services to make proposals and lobby hospital management to implement the required changes. The ES actions attributed to each domain category are reviewed periodically as part of an institutional iterative audit programme. The authors propose an annual periodic review for the institutional grading exercise. In addition, we also recommend regular meetings with project leads/champions to report on activity, to maintain the momentum and identify emerging challenges for the different levels of activity. At the end of the assessment period (e.g., calendar year), responders (team leads) complete the questionnaire as accurately as possible with justification for each score. It is anticipated that responders will need to seek input from other stakeholders (e.g., service providers, building and estates managers, hospital leads and managers).

User interface for each statement in the different categories
Each question is answered by selecting one option from the list of four presented:
-
Fully addressed – a thorough understanding of the subject is achieved
-
Partially addressed – a limited understanding of the subject is achieved. Some of the suggested points and/or related topics are covered. The subject topics are not covered in detail, and a superficial subject understanding is achieved
-
Initial subject exploration commenced – a baseline analysis and assessment of the current situation has been commenced. minimum progress to date
-
Not addressed – the action point has not yet been addressed.
At each iteration of the audit cycle, each of the action projects are reevaluated with further activity to progress until the point that it is ‘fully addressed'. These action statements always remain on the list to ensure that the activity status is current and also to ensure their ongoing validity, the need for revision or the need for the inclusion of new statements.
Performance metrics
The ES actions attributed to each category are reviewed periodically as part of an institutional iterative audit programme. The authors propose an annual periodic review for the institutional grading exercise. In addition, we also recommend regular meetings with project leads/champions to report on activity, to maintain the momentum and identify emerging challenges for the different levels of activity.
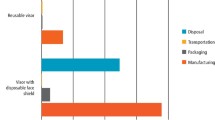
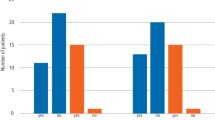
Following the updating of the report as indicated above, activity for each action statement is graded (point allocation) depending on the level of progress (i.e., fully addressed would gain four points and not addressed would gain zero points as shown in Figure 2). The scores are then weighted according to the RAG rating attributed to the action. This then determines the level of action delivered in recognition of the degree of difficulty to deliver the impacts that are represented using RAG categories: red category (weighting of ×3); amber category (weighing of ×2); and green category (weighting of ×1), e.g., an action deemed aspirational and difficult would have a red RAG rating (Fig. 1). If this action's level of progress was deemed partially addressed, it would be assigned a score of 3. The overall score given to that action would be nine (3 x [weighted score of 3]).
The scores are automatically tabulated in several ways to provide detailed information including:
-
Points achieved for each ES action statement, showing the RAG rating for that statement
-
Points achieved for each ES thematic category (e.g., waste management, plastics etc.)
-
Actual ES actions achieved (n value and %) for each RAG category
-
Overall institutional attainment for the whole of that audit cycle, obtained by calculating the total number of points available and the total achieved to give a percentage. This percentage is then converted to a letter score (Table 3). This key information is shown on the front cover of the annual report (see data availability for online data repository).
Table 3 Audit and improvement requirements mapped against HEAIT (italics denotes actions not addressed)
Once the tool has been completed for the first time, this baseline data are subsequently used in an iterative audit to demonstrate changes and drive improvements over time. The ongoing performance across all projects is assessed in the periodic review (e.g., annually) to provide a project-specific and an overall hospital performance score which are then used to produce an updated annual activity report. Thus, the metrics in the report identify the status of activity, areas for improvement and provide measurable goals for year-on-year hospital wide improved performance.
Reporting and insights
Action statements or sub-statements are allocated to a group of staff/trainees/students as appropriate to the action. They self-manage their workflow to identify, pursue and ultimately implement the ES action. Annual progress is reported to the audit lead who will collate all progress and complete this report. Teams are encouraged to engage further with evidence of real and substantial progress that can be measured and evidenced. There is strong evidence in the literature that indicators of progress (even small wins) is the most powerful motivator for teams18 and that specific and difficult goals, coupled with feedback in the form of measurable evidence of progress is a strong driver for higher performance and motivation.19 The aim is that each iterative assessment should demonstrate a gradual and consistent improvement in outcomes achieved towards a more environmentally sustainable hospital.
Customisation and scalability
Prior use of the toolkit concept in the oral healthcare primary care setting provides a basis to explore the customisation and translation to a hospital setting.11 A comprehensive inclusion of all themes and action statements was sought from a review of the literature. Expert focus group analysis enabled thematic classification of the impact mitigation statements and construction of the toolkit.
The toolkit is designed to be translated to other hospital departments and settings as required with an element of customisation. While a significant proportion of the impact statements are generic to any hospital setting, there is a clear expectation that a proportion of the impact statements will have to be customised to the intended implementation setting. A setting-specific assessment of activity and requirements of a different environment would enable complete translation of the existing toolkit.
The toolkit can be translated and scaled up to diverse and larger institutions by following the steps:
-
1.
Validate the pilot success
-
2.
Build a scalable infrastructure
-
3.
Secure resources and budget
-
4.
Adopt a phased rollout strategy
-
5.
Foster change and culture management.
Compliance and regulatory adherence
The toolkit is compliant with best clinical governance practice in hospitals and addresses local, national and international recommendations and legislation. For example, this toolkit has the potential to provide the workforce mindset change and level of engagement required to help reach the NHS England commitment of delivering net zero emissions by 2040–2045.7
Results
The tool was implemented in 2024 as a pilot in the department of restorative dentistry, Charles Clifford Dental Hospital (Sheffield Teaching Hospital NHS Trust), Sheffield, UK. All actions were tested and scored against current levels of activity and scored accordingly.
The criteria of a corporate audit and improvement tool were reviewed against this toolkit. All the required parameters to be considered have been addressed to some extent, with identification of required further actions as per the examples identified in online Supplementary Table 1 and the full report (see data availability for online data repository). The built-in calculator was considered compliant against the audit required criteria by providing a baseline level of environmental sustainability activity and in this way validating the toolkit.
An overall departmental percentage score of 29.9% was reached and measurable metrics were obtained for each impact statement, with a significant proportion scoring a value of zero, demonstrating a lack of activity in that category. The results provided evidence of activity for the green, amber and red categories in accordance with the level of importance and relevance. The distribution of points was representative of the ease/difficulty of implementation for each action, validating the attribution of actions to the RAG rating. The highest score was achieved for the green actions (66.7%), followed by those in the amber section (32%) and least for the actions in the red category (26%).
The overall experience of this case study pilot implementation process has been positive. The pilot was completed as a baseline study by the authors and other volunteer staff across the various domains (clinical, nursing, clerical, auxiliary). The focus of the case study was the department of restorative dentistry, which is the largest in the dental hospital. There was agreement in the understanding and relevance of each of the tasks and the required action. There was consensus within the teams for the score awarded for each action. The process identified areas that required greater levels of ES activity, because they were partially or completely neglected.
An important finding was that staff were generally very enthusiastic to engage in this project as they felt that their individual involvement fed directly into a greater ES movement within the department. The pilot also identified that despite willingness to engage, the absence of allocated time for this task was a barrier for more generalised staff participation, beyond those prepared to participate. Volunteer staff were recruited and participated from a sense of altruism and did so in addition to their planned work activities. This finding would need to be addressed with ‘buy in' from hospital management, required to promote, encourage and enable this activity.
Discussion
The HEAIT addressed the aim and all the objectives for this pilot project. The process was tested in a real secondary care clinical hospital setting and mapped to a compiled set of audit and improvement requirements. Compliance across all audit criteria was achieved and thus validating the effectiveness of the tool.
Staff engagement can be driven with the appointment of project champions to increase awareness and to manage, promote and engage staff with activities across all hospital areas and disciplines. Continuous motivation and positive drive can be achieved through incentives and acknowledgement of contributions. It is essential to disseminate these positive activities and report at departmental or hospital level to further motivate the workforce and encourage collaborative shared decision-making. A key enabler is the provision of effective training and interactive educational sessions.20 A barrier to engagement is that staff often cite being overworked, projects being outside their job description or lack of institutional incentive or reward.21 Despite a desire to engage broadly, there was a work prioritisation conflict, with the requirement to allocate staff time and resources to this activity as part of the overall workload allocation. In essence, ES is not prioritised sufficiently by the hospital executive to warrant defined time allocation within staff work schedules. Currently, all ES activities are conducted as an ‘additional' vocational activity by enthusiasts, as an addition to the main workload. There is scope to include this activity into the work schedule of all hospital staff as a key performance indicator. This would require a significant organisational systems adaptation led by the hospital executive. This approach may be considered to be disruptive of ‘established' work practice, but the reality is that hospitals must engage with environmental sustainability at a workforce level to ensure co-ownership of the responsibility and effective participation in the solution. Currently, there is a huge disengagement between hospital staff and environmental sustainability actions and goals, with a generalised attitude that ES is the problem and responsibility of the hospital executive. Hospitals employ a huge workforce of hundreds if not thousands of staff across all sectors, that are capable and that can be mobilised to engage with a minimum time commitment with any of the 120+ ES tasks identified in this tool. This type of organisational shift is required and urgent to mitigate the environmental crisis caused by the healthcare sector. A significant feature of this toolkit is that there is no minimum level of engagement required. Any activity, in any domain will be recorded, create an evidence-based metric that translates into impactful outcomes – the greater the level of engagement, the greater the impact that is generated.
The mapping process of the HEAIT against the pre-established audit and improvement criteria, has identified specific areas for further development to the scope of the tool:
-
User interface: scope for the creation of customisable dashboards and reporting features
-
Compliance and regulatory adherence: scope for mapping to industry, government regulations/legislation with automated compliance tracking and reporting
-
Real-time monitoring and alerts: scope to provide automated alerts for anomalies, risks, or policy violations
-
Workflow automation: scope to create a streamlined audit processes with automated checklists. Scope to create a task assignments and progress tracking mechanism
-
Collaboration and communication: scope to engage with organisational stakeholders outside the audit process by means of project-focused, social activities. Scope to engage all stakeholders in a pro-active manner with real time allocation to the project
-
Security and data protection: scope for strong encryption and access control mechanisms
-
Customisation and scalability; scope to adapt to different settings (hospitals) and organisation sizes. Scalable for growing needs
-
Reporting and insights: scope for benchmarking and trend analysis for continuous improvement.
Conclusion
The HEAIT provides an effective and validated way of achieving real engagement of the whole workforce in a meaningful manner to achieve measurable goals as part of a collaborative environmental mitigation strategy.
Data availability
The templates used to audit and map outcomes and subsequent reporting that support this research publication have been shared – this data can be freely downloaded from the University of Sheffield Research Data Repository at https://doi.org/10.15131/shef.data.28695842 under the terms of the Creative Commons Attribution (CC BY NC 4.0) licence.
Change history
17 April 2026
When this was originally published, the link in the PDF version was incorrect and missing in the online version. The article has been updated.
References
Whitmee S, Haines A, Beyrer C et al. Safeguarding human health in the Anthropocene epoch: report of the Rockefeller Foundation-Lancet Commission on planetary health. Lancet 2015; 386: 1973–2028.
Hensher M, McGain F. Health care sustainability metrics: building a safer, low-carbon health system. Health Aff 2020; 39: 2080–2087.
Seervai S, Gustafsson L, Abrams M K. How the US health care system contributes to climate change. Commonwealth Fund 2022. Available at https://www.commonwealthfund.org/publications/explainer/2022/apr/how-us-health-care-system-contributes-climate-change (accessed 1 February 2026).
Rodríguez-Jiménez L, Romero-Martín M, Spruell T, Steley Z, Gómez-Salgado J. The carbon footprint of healthcare settings: a systematic review. J Adv Nurs 2023; 79: 2830–2844.
Budd K. Hospitals race to save patients – and the planet. 2019. Available at https://www.aamc.org/news/hospitals-race-save-patients-and-planet (accessed 1 February 2026).
Jen Choi A. The environmental impact of healthcare. 2022. Available at https://pursuit.unimelb.edu.au/articles/the-environmental-impact-of-healthcare (accessed 1 February 2026).
National Health Service. Delivering a net zero NHS. Available at https://www.england.nhs.uk/greenernhs/a-net-zero-nhs/ (accessed 1 November 2025).
Martin N, Sheppard M, Gorasia G, Arora P, Cooper M, Mulligan S. Awareness and barriers to sustainability in dentistry: a scoping review. J Dent 2021; DOI: 10.1016/j.jdent.2021.103735.
Martin N, Sheppard M, Gorasia G, Arora P, Cooper M, Mulligan S. Drivers, opportunities and best practice for sustainability in dentistry: a scoping review. J Dent 2021; DOI: 10.1016/j.jdent.2021.103737.
Martin N, Mulligan S, Shellard I J, Hatton P V. Consensus on Environmentally Sustainable Oral Healthcare: A Joint Stakeholder Statement. York: White Rose University Press, 2022.
Martin N, Mulligan S. The sustainability in dentistry toolkit. 2022. Available at https://sustainability-platform.fdiworlddental.org/# (accessed 5 February 2025).
AuditBoard. Audit management: definition, tools, and building blocks. 2025. Available at https://www.auditboard.com/blog/audit-management-definition-tools-and-building-blocks (accessed 1 November 2025).
AuditBoard. Step-by-step internal audit checklist. 2025. Available at https://www.auditboard.com/blog/audit-checklist-how-to-conduct-an-audit-step-by-step (accessed 1 November 2025).
Mehta A M. Internal auditing: a practical approach. Selecting using audit tools. Available at https://ecampusontario.pressbooks.pub/internalauditing/chapter/08-02-selecting-and-using-audit-tools/ (accessed 1 November 2025).
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol 2006; 3: 77–101.
Equator Network. Revised standards for quality improvement reporting excellence. 2015. Available at https://www.equator-network.org/reporting-guidelines/squire/ (accessed 1 November 2025).
Thompson N. Ebel method of standard setting. 2022. Available at https://assess.com/ebel-method-standard-setting/ (accessed 05 February 2025).
Amabile T, Kramer S. The Progress Principle: Using Small Wins to Ignite Joy, Engagement, and Creativity at Work. Massachusetts: Harvard Business Press, 2011.
Locke E A, Latham G P. Building a practically useful theory of goal setting and task motivation. A 35 year odyssey. Am Psychol 2002; 57: 705–717.
O'Brien S, Wilson C, Duck M, Nieva G, Rao M P, Haskell L. Review article: a primer for clinical researchers in the emergency department: part XIII. Strategies to engage staff and enhance participant recruitment in emergency department research. Emerg Med Australas 2024; 36: 834–840.
Flanagan M R, Foster C C, Schleyer A et al. Aligning institutional priorities: engaging house staff in a quality improvement and safety initiative to fulfill clinical learning environment review objectives and electronic medical record meaningful use requirements. Am J Surg 2016; 211: 390–397.
Acknowledgements
To staff and colleagues in the Charles Clifford Dental Hospital, UK for their support in the development and implementation of this tool.
Author information
Authors and Affiliations
Contributions
NM; conception or design of the work; the acquisition, analysis, interpretation of data and significant contribution to the writing and editing of the manuscript. JH; conception or design of the work; the acquisition, analysis, interpretation of data and significant contribution to the writing and editing of the manuscript. PH; conception or design of the work; the acquisition, analysis, interpretation of data and significant contribution to the writing and editing of the manuscript.
Corresponding author
Ethics declarations
The authors declare no conflicts of interest. Ethical approval was not required as this manuscript reports on a hospital quality improvement audit exercise of systems and processes. We did not use any data that related to any persons or involved any named people other than the authors undertaking the audit exercise. No individual persons were involved in the study and as such consent was not required as part of this audit report.
Supplementary Information
41415_2026_9529_MOESM1_ESM.pdf (download PDF )
Representative examples of action statements that were completed in the case study – department of restorative dentistry (PDF 84KB)
Rights and permissions
Open Access. This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0.© The Author(s) 2026.
About this article

Cite this article
Martin, N., Hudson, J. & Hoyle, P. Hospital Environmental Audit and Improvement Tool: dental hospital case study. Br Dent J (2026). https://doi.org/10.1038/s41415-026-9529-6
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41415-026-9529-6
