
Abstract
Myopic traction maculopathy (MTM) affects around 30% of patients with pathologic myopia and is responsible for a high proportion of legal blindness cases in myopic population. The main surgical solutions to MTM are macular buckling (MB) ab-externo surgery and pars plana vitrectomy (PPV) ab-interno surgery. The recently proposed MTM staging system (MSS) provides a new classification of the condition based on evolutive changes occurring in the natural course of the disease. Based on MSS staging, a customised surgical approach has been proposed according to different stages of MTM. The aim of this systematic review is to describe literature from 2017 to the present date to assess concordance of recent literature to the results proposed from the authors of the MSS.
Similar content being viewed by others
Introduction
Myopic maculopathy (MM) is a functional and anatomical deterioration of the macular region that affects patients with pathologic myopia. It is one of the leading causes of visual impairment and legal blindness worldwide, and its prevalence is expected to rise alongside that of pathologic myopia in the coming decades [1, 2]. Progressive scleral ectasia at the posterior pole leads to choriocapillaris degeneration on one hand and the development of tractional forces on the other. These processes contribute to the onset and progression of atrophic, neovascular, and tractional complications of MM. The action of tangential and anteroposterior tractional forces at the vitreoretinal interface gives rise to a subgroup of complications known as myopic traction maculopathy (MTM), which affects approximately 30% of patients with pathologic myopia [3]. The presence of tractions is due to the effect of two factors: the presence of a vitreoretinal adhesion and the exceeding of the elastic limit of the ILM during bulbar elongation, a mechanism that progressively prevents the retina from adhering to the scleral profile. Different combinations of anteroposterior and tangential tractional forces result in different forms of MTM, namely foveoschisis, macular detachment(MD), full-thickness macular hole (FTMH), outer and inner lamellar macular hole (LMH). Advanced stages of MTM, including MD and MH, may develop in 34.5–72% of cases of MTM [4,5,6], conferring less favourable prognosis and requiring prompt treatment. Treatment of MTM is strictly surgical, with two main surgical techniques considered as the mainstay of treatment: macular buckle (MB) implantation and pars plana vitrectomy (PPV). The principle of PPV is to remove anteroposterior traction exerted by the vitreous and reduce retinal rigidity thus improving adherence to the ectatic scleral profile. Despite numerous advancements in PPV technique, surgical outcomes remained relatively poor for decades, with macular reattachment rates of 76.5% and 81.8% for light and for heavy silicon oil, respectively. Moreover, both groups experienced frequent MD relapses, often associated with the reopening of an FTMH [7]. Innovative surgical techniques have been proposed, among which internal limiting membrane peeling with foveal sparing has become the most popular [8, 9]. The rationale behind MB is to reduce scleral elongation by placing material over the posterior pole, thereby counteracting scleral ectasia and limiting the effects of anteroposterior tractional forces. Historical approaches to this surgical strategy include the use of donor scleral grafts, autologous fascia lata, and cadaveric dura mater [3]. The revival of this concept was driven by the unsatisfactory outcomes of PPV in the treatment of MTM. In 2001, Ripandelli et al. [10], and later in 2005, Theodossiadis and Theodossiadis [11] reported the success of MB using a sponge and a solid silicone exoplant, respectively. Since then, various modifications to the material, shape, and surgical technique of MB have been introduced, leading to progressive improvement in surgical outcomes and safety profile [12, 13]. A meta-analysis by Alkabes [14] explored surgical outcomes of MB and PPV in the treatment of MTM-associated MD and FTMH, based on international literature from 2010 to 2016. The study concluded that MB was associated with better functional and anatomical outcomes and a lower risk of re-detachment compared to PPV, while the risk of adverse events was similar between the two procedures. However, as mentioned earlier, recent advancements in PPV and MB techniques, along with an evolving scientific approach to MTM classification, have significantly altered the landscape since the publication of the meta-analysis.
The recently described MTM staging system (MSS) [15] was developed to account for the natural history of each manifestation of MTM, considering the impact of both types of forces at the vitreoretinal interface. The core idea to this system is that different morphologies of MTM do not represent distinct forms of the disease but rather different stages in its progression. The same authors suggested a customised surgical approach based on MSS stage [16]. According to their recommendations, MB implantation should be preferred over PPV in cases of MD with or without associated schisis (stages 3a and 4a) and with and without associated LMH (stages 3b and 4b). A combination of MB and PPV was recommended for FTMH accompanied by signs of anteroposterior traction, such as prevalently outer foveoschisis (stage 2c), foveoschisis with MD (stage 3c), and MD alone (stage 4c). Foveoschisis alone in stages 1a and 2a, or in combination with LMH (stages 1b or 2b) should be managed with observation alone. A similar surgical approach had already been proposed in a non-systematic manner by other authors even before 2021, the year MSS was introduced.
Nonetheless, this proposed MTM surgical management approach awaits validation through large clinical trials and would benefit from a comprehensive review of existing literature on the two surgical strategies applied at different MSS stages of the disease.
Aim of the systematic review
The aim of this systematic review is therefore to provide a critical analysis of recent literature on outcomes of MB and PPV in the treatment of different stages of MTM, discussing the results in the light of the surgical approach proposed by MSS. Table 1 provides a schematisation of MSS to use a reference for a better understanding of the results.
Research method
Since our study involves a review of previously published literature, no institutional approval was required. Our literature review was conducted using electronic databases, including: CENTRAL, Ovid MEDLINE, Embase, Clinical Trials.gov (www.clinicaltrials.gov), and the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP). No restrictions were applied regarding the date or language of the included studies. The last search of electronic databases was performed on 19 March 2023. The following keywords were used: macular buckle, myopic traction maculopathy, pars plana vitrectomy, macular detachment, full thickness macular hole, ILM peeling, foveal sparing, MTM staging system, MSS.
Selection process
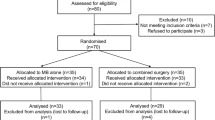
Types of study considered for review included clinical trials, case control studies, cohort studies, and case series including at least five [5] patients published between 1st January 2017 and 19th March 2023. We evaluated all studies in which participants underwent either PPV, MB, or both for MTM treatment. Different MB and PPV techniques were included and analysed separately in the results section. Two authors independently screened the search results and extracted data using standard methodological procedures. A third author resolved any disagreement regarding full-text assessments. Our initial search yielded 178 reports, and the final selection resulted in 12 articles included in the review. The study selection process and exclusion criteria are detailed in a PRISMA diagram in Fig. 1.

PRISMA diagram illustrating the selection process of the considered articles.
Results
Parolini et al. [16] reported outcomes of 157 eyes affected by MTM, treated either with MB alone, PPV alone, or combined MB + PPV based on MSS staging indications [15]. In stage 1, MB and PPV resolved schisis and the holes in 100% and 93% of cases, respectively, at the final follow-up. Additional PPV was required in 14% of MB treated eyes 6 months after primary surgery. PPV-treated eyes received additional PPV in 14% and additional MB in 21% of cases. Combined MB + PPV resolved schisis and holes in 100% of eyes without further surgery. Given the slow progression from stage 1 to more severe stages and the potential complications, the authors concluded that MB should not be indicated in this stage, and PPV with ILM flap should be performed only in the presence of FTMH. In stage 2, MB resolved, improved, and left holes unchanged in 79%, 7%, and 14% of eyes, respectively. Unresponsive cases were treated with secondary PPV (9 cases), leading to complete resolution. Some patients refusing secondary treatment experienced spontaneous resolution within the first year. PPV resolved the schisis and the holes in 75% of cases, but required a second PPV in 100% of cases and a MB in 66%. Combined MB + PPV achieved 100% schisis resolution and resolved or improved holes in 92% and 8% of cases, respectively, without further surgery. The authors recommended observation for stages 2a and 2b and combined MB + PPV with ILM flap for stage 2c. In Stage 3, MB resolved retinal pattern in 100% of cases. The foveal pattern was resolved or left unchanged in 89% and in 11% of eyes, respectively. PPV was later added in 17% of MB-treated eyes. The eyes in stage 3b and 3bO, operated with MB alone, showed a progressive relief of the perpendicular component of traction. All 18 cases (100%) operated with PPV alone obtained a resolved retinal and foveal pattern at the final follow-up, but only with further MB in 94% and further PPV in 72% of eyes; 13 eyes in stage 3a (87% of the eyes operated with PPV in this stage) ended in an iatrogenic FTMH. Combined MB + PPV achieved 100% retinal pattern resolution and 92% foveal pattern resolution, but required additional PPV in 42% of cases. In fact, some cases operated with MB + PPV developed an iatrogenic FTMH. Two eyes in stage 3b + , with a limited foveal detachment, had a temporary worsening of the detachment after combined MB + PPV. The authors recommended MB for stages 3a and 3b, and combined MB + PPV for stage 3c. In Stage 4, MB resolved the retinal pattern in 95% of eyes and left it unchanged in 5%, with no further MB or PPV required. The only PPV-treated eye experienced worsening and required combined MB + PPV. All the eyes operated with MB + PPV, presented a resolved retinal pattern. The foveal pattern (holes) needed a further PPV in two eyes (22%). The eyes in stage 4c, treated only with MB reached 100% retinal reattachment but only 60% reached hole closure. The Authors concluded that stages 4a and 4b should be treated only with a MB. Stage 4c should be treated with a combination of MB and PPV with ILM flap.
All the other studies included in the review reported results of MB, PPV, and MB + PPV not explicitly mentioning the MSS. We will thus split the results from each paper according to key concepts in MSS staging.
MTM with prevalently anteroposterior tractional forces
A total of 10 studies (4 prospective and 6 retrospective) evaluated the outcomes of MB in cases of macular schisis (MS) with or without MD, specifically in the absence of tangential traction leading to MH formation (see Table 2).
Prospective studies
A randomised controlled trial (RCT)published by Liu et al. [17] compared the anatomical and functional outcomes of MB combined with gas injection versus PPV in a cohort of 78 eyes. Only eyes with a refractive error < -8 D diagnosed with MS associated with MD and characterised by posterior staphyloma, were included. Key exclusion criteria included the presence of a FTMH (but not of an LMH), MD extending beyond the vascular arcades, and a history of previous vitrectomy or scleral buckling surgery. They reported an anatomical success rate of 97.5% for MB + gas injection compared to 81.6% for PPV. Functional outcomes were also significantly better with MB + gas injection, showing a postoperative improvement of 21.7 ± 18.7 ETDRS letters versus 4.5 ± 22.6 ETDRS letters with PPV.
A second small prospective series by Xiong et al. [18] analysed 7 eyes with MS and MD, reporting excellent results with a novel L-shaped buckle implantation combined with PPV. The technique involved standard 3-port 23 G PPV followed by the placement of a L-shaped titanium plate sheathed in a silicon sponge in the superior temporal quadrant, designed to indent the macular region. Postoperatively, patients were instructed to maintain a prone position for at least 2 weeks. Anatomical success was achieved in 100% of cases, with visual acuity improving from a preoperative mean of 1.55 ± 0.50 logMAR to a postoperative mean of 0.93 ± 0.40 logMAR.
Chen et al. [19] also reported highly favourable results in a prospective study involving 38 eyes with a short axial length (AL) (AL > 24 mm and <26.5 mm). Among them, 29 eyes showed minimal tangential traction (MS associated to MD alone), and none had prior history of vitrectomy or scleral buckling. The study used a T shaped MB, consisting of a silicone sponge rod embedded with a perforated titanium plate, a silicone band, and a silicone sponge cushion fixed at the junction site. The silicone sponge cushion was positioned at the macula to provide adequate indentation. Anatomical success was achieved in 100.0% of cases and 93.1% of patients experienced postoperative visual improvement. All patients reported metamorphopsias, which gradually resolved within 6 months post-surgery.
Lastly, Zou et al. [20] prospectively examined the outcomes of PPV with ILM peeling combined with the implantation of a customised MB designed using 3D reconstruction based on orbit magnetic resonance imaging (MRI). The study population consisted of patients with extremely long axial length (30.62 ± 1.20 mm), and no patient with MH were included. All participants demonstrated excellent functional outcomes, with complete anatomical success and no recurrence over a two-year follow-up.
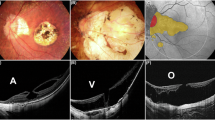
An example of anatomical and functional success of MB in a MS-MD case from EyeCare clinic is illustrated in Fig. 2.

A Case of MTM 3aO. SLO image with horizontal and vertical slab. BCVA 0,05; B same case horizontal widefield OCT Bscan; C same case vertical widefield OCT Bscan; D same case microperimetry with central scotoma; E same case after surgery with macular buckle only: horizontal (F) and vertical (G) widefield OCT Bscan; H same case, postoperative microperimetry with improved sensitivity and disappearance of the central scotoma. BCVA best corrected visual acuity, MB macular buckling, MTM myopic traction maculopathy, MS-MD macular schisis - macular detachment, OCT optical coherence tomography.
Retrospective studies
Wu et al. conducted a large retrospective study on 216 eyes diagnosed with MS and MD, reporting an anatomical success rate of 94.4% for MS and 99.5% for MD. Regarding functional outcomes, postoperative improvement in visual acuity (VA) was observed in all patients to varying degrees. Immediate postoperative VA was recorded at 1.459 ± 0.841 logMAR, with continuous improvement from the first postoperative month, stabilisation at one year and a final VA of 0.908 ± 0.606 at three years (t = 6.896, P < 0.01). Additionally, axial length values at the end of follow up were consistently shorter than preoperative measurements. Another retrospective study by Susvar et al. [21] analysed 16 cases of MS associated to MD, including 3 cases with a history of previous vitreoretinal surgery. Indications for surgery included recent progression of visual symptoms, changes on foveal OCT scans, worsening near-vision symptoms, recent onset of MD, or recent MH formation. One eye underwent combined MB and PPV, while the remaining 15 eyes were treated with MB alone using a T-shaped MB. The surgical technique involved the insertion of a solid silicone macular plate (Morin wedge) onto a 2-mm solid silicone band (Devin band), which was then passed under the lateral rectus (temporal), inferior oblique, inferior rectus, superior rectus, and superior oblique muscle. Both ends of the Devin band were positioned nasally, on the upper and lower sides of the medial rectus. The macular wedge was placed horizontally under the lateral rectus and carefully manoeuvrer along the globe’s contour toward the posterior pole. Once optimally positioned at the macula, the anterior end of the macular plate was trimmed and sutured beneath the lateral rectus muscle. The ends of the 2-mm band were trimmed and sutured to the sclera in their respective nasal locations using 5-0 polyester sutures, without connecting them to each other. With this technique, 87.5% anatomical success rate was reported, with only one case of MD recurrence over a mean follow up of 12.9 ± 16.1 years.
Sood et al. [22] compared the surgical outcome of MB in eyes with MTM characterised by type I and type II/IX staphyloma (two study groups). All patients underwent MB surgery under general anaesthesia, performed by a single surgeon (PS), using a solid silicone T-shaped macular implant (Morin–Devin wedge from France Chirurgie Instrumentation, FCI, France). Among the 11 eyes included, 7 showed no FTMH or LMH and 4 had MD. In these patients, MB resulted in a reduction of >90% of the schisis in 4/7 cases (57.1%) and of>90% of the MD in 75.0% of cases with preoperative MD (3/4 cases). Visual acuity improved from 1.11 logMar (range 1.3–0.6) to 0.84 logMar (range 1.3–0.48).
Li et al. analysed the association between EZ integrity and the anatomical and functional success of MB surgery in eyes with MS + MD. Among 44 patients, anatomical success was achieved in 13 out of 28 (46.4%) eyes with a preoperative disrupted EZ and in 14 out of 16 (87.5%) eyes with an intact EZ. Patients with an intact EZ also experienced greater postoperative visual improvement compared to those with a disrupted EZ (+ 26.88 ± 19.48 ETDRS letters and + 15.00 ± 14.14 ETDRS letters, respectively).
Zhao et al. retrospectively analysed a 3-year follow up of 28 eyes with MS + MD but without MH, treated with either MB alone (15 eyes) or MB + PPV (13 eyes). No significant difference in anatomical or functional success were observed between the two treatment groups. Anatomical success was achieved in 26 out of 28 eyes (92.8%) and visual acuity significantly improved during the first postoperative year, stabilising thereafter.
Factors associated with favourable functional outcome
In the study from Susvar et al. [21], shorter axial length and a mild grade of staphyloma were identified as positive prognostic factors for functional outcomes. Additionally, Sood et al [22]. reported an association between postoperative visual improvement and staphyloma characteristics, with type I staphyloma being linked to reduced postoperative visual improvement compared to type II/IX (p = 0.004). The study by Zhao et al. emphasised the importance of preoperative symptoms, demonstrating significant associations between both duration of preoperative symptoms (r = 0.430, p = 0.006) and preoperative best corrected visual acuity (BCVA) (r = 0.359, p = 0.016) with BCVA at three-year follow-up in a multiple linear regression analysis. In another study by Zhao et al. younger age was also identified as a positive functional prognostic factor for MD eyes undergoing MB [23]. Lastly, Li et al. reported that patients with an intact foveal EZ experienced better visual improvement compared to those with a disrupted EZ [24].
MTM with prevalently tangential tractional forces or with combined excess of traction
A total of 11 studies (4 prospective and 7 retrospective) evaluated the outcomes of MB in MS associated with MH, with or without MD (see Table 3).
Prospective studies
Zhao et al. compared the prospective outcomes of 62 eyes diagnosed with MH-MD, randomly assigned to either MB alone or MB + PPV + inverted flap technique. The MB technique involved the implantation of a silicone sponge-titanium exoplant as previously described by the same author [25]. Patients with MD extending beyond the vascular arcades were excluded. Despite similar MD resolution rates (97.0% success in MB alone versus 100.0% in the combined treatment group), a significantly higher rate of MH closure was observed in the combined group (82.8% versus 66.7% in MB alone). Successful flap inversion was achieved in 20 out of 29 eyes (69.0%), with a 100.0% closure rate in these cases. Notably, MD reattachment was significantly more frequent in the combined treatment group at 1 month postoperatively (p = 0.018), though this difference disappeared at subsequent follow-ups at 3,6,12, and 24 months. Both groups showed significant postoperative improvements in BCVA (P < 0.05), with the combination group demonstrating superior BCVA at 12 months (P = 0.021) and 24 months (P = 0.041), but not at 6 months (P = 0.132).
Another prospective study by Chen et al. [19] confirmed the excellent results of combined MB + PPV treatment in short axial length eyes, reporting a 100.0% success rate for both MD resolution and MH closure in a cohort of 5 MH-MD patients and 4 MH patients. However, only 6 out of 9 patients (66.7%) experienced postoperative visual improvement.
The outcomes of MB in patients with extremely high axial length were investigated in two prospective studies by Bedda et al. [26] and Ma et al. [27]. Bedda et al. evaluated a novel sutureless illuminated MB without adjuvant PPV in 20 MH patients, achieving 100.0% MD resolution but only 40.0% MH closure. No higher rate of exoplant displacement was reported. Ma et al. [27] compared PPV + ILM peeling versus PPV + ILM peeling + MB in 98 patients with extremely high axial length, demonstrating superior anatomical and functional outcomes with the latter. A successful case of PPV + ILM peeling + MB from our experience is illustrated in Fig. 3.

A Preoperative OCT showing a case of MD with tangential traction with a BCVA of 0.1 decimals. B OCT of the same case 2 years after MB + PPV; BCVA at follow up was 1.0 decimals. BCVA best corrected visual acuity, ILM inner limiting membrane, MB macular buckling, MD macular detachment, OCT optical coherence tomography, PPV pars plana vitrectomy.
Retrospective studies
Luo et al. [28] retrospectively compared MB alone with MB + PPV+ inverted flap technique in 26 patients with MH without MD. MH closure was achieved in 50.0% of patients treated with MB alone and in 92.8% of those who underwent the combined treatment. Additionally, the MB + PPV+inverted flap group exhibited greater postoperative visual acuity improvement (+16.36 ± 10.39 ETDRS letters versus + 10.42 ± 17.25 ETDRS letters in MB alone).
Sood et al. [22] included 1 patient with MH and 3 patients with MH-MD, all treated with MB alone. MH closure was achieved in 3 out of 4 cases (75.0%) and MD was reduced by>90% within 2 months in all cases, with significant visual acuity improvement (see Table 3).
A large retrospective cohort study by Wu et al. [29] described 162 eyes with MH-MD, of which 80 were treated with MB alone and 82 with MB + PPV. MH closure was achieved in 54.9% of cases, while MD resolution was observed in 97.5%. Postoperative visual acuity improved in all patients.
Zhao et al followed 21 MH-MD patients for 3 years, treated with either MB alone (52.4%) or MB + PPV (47.6%). Anatomical success rates were 100.0% for MD resolution and 76.2% for MH closure. Visual acuity improved significantly over the first two postoperative years before stabilising. However, no clear conclusions could be drawn regarding the superiority of one treatment over the other. Similarly, Susvar et al retrospectively analysed 9 MH-MD patients (5 treated with MB alone and 4 with MB + PPV), reporting MH and MD resolution in 7 out of 9 cases 77.8% with insufficient data to compare treatment effectiveness. Visual acuity improved from 1.68 logMAR (range 1.3–2.3) preoperatively to 1.4 logMAR (range 0.7–2.3) postoperatively.
Sun et al. introduced a novel exoplant combined with PPV and triamcinolone assisted ILM peeling in 8 MH-MD eyes. Silicone oil was injected in 3 eyes, and C3F8 gas was injected in 5 eyes as tamponade. The exoplant for MB was easily prepared in the operating room with a 5 × 3 mm silicone sponge (506 silicone sponge, MIRA, USA) and a malleable titanium plate (0.5 mm thick, 20 holes, titanium adoption plate, MatrixMIDFACE™ Plate, Depuy Synthes, West Chester, PA, USA). A tunnel was made into the silicone sponge with a 20-gauge microvitreoretinal (MVR) blade and the titanium plate was inserted into the tunnel. When the titanium plate reached the end of the silicone sponge, the tip was rolled to a snail shell shape. By this procedure, the short arm of the exoplant was thickened in height to threefold thickness of the long arm and the long arm was bent to fit the curvature of the eyeball. Rotating the eyeball inferonasally, the exoplant was inserted superotemporally to the posterior of the globe to reach the macula. The buckle height was adjusted under direct visualisation of the location of the buckle through the vitrectomy lens with the illuminator inserted through the trocar. The long arm of the exoplant was fixed to the sclera with a mattress suture posterior to the muscle insertion sites using 5–0 Dacron suture (Alcon, USA). The location was checked once again and a second mattress suture was fixed posterior to the first mattress suture. The remnant length of the exoplant was trimmed using a plate cutter and the titanium plate was cut more deeply into the silicone sponge to hide its end into the sponge. With this technique, they reported 100.0% success rate in treatment of MD and 75.0% MH closure rate.
LMH prognostic role and iatrogenic FTMH development
Parolini et al. [30] investigated the surgical outcomes of MTM complicated by the formation of an outer lamellar macular hole (O-LMH), analysing the results of either MB or PPV in a cohort of 48 eyes affected by MTM (24 with O-LMH and 24 control eyes). Their findings indicated that O-LMH predisposed to the formation of a FTMH after surgical treatment, but only in eyes treated with PPV. Therefore, MB may be preferable for MTM cases complicated by O-LMH to prevent the iatrogenic development of an FTMH. A successful case of MB surgery in an MD patient with a preoperative O-LMH (at risk for FTMH formation with PPV) treated at the EyeCare clinic is illustrated in Fig. 4.

A Preoperative OCT of a case of myopic schisis with macular detachment and outer lamellar macular hole (O-LMH) formation seen from different perspectives. B Brilliant anatomical resolution of the case after macular buckling at 3 months from surgery. OCT optical coherence tomography.
Similar findings were reported by Liu et al. [17], who documented the development of an FTMH in 10 eyes treated with PPV (26.3%), three of which did not show preoperative MD, and in one eye treated with MB (2.4%) (p < 0.001). All reported cases of FTMH developed within three months from PPV surgery, with risk factors including the presence of LMH and severe traction on the surface of a thin fovea. Figure 5 illustrates a case of FTMH development after PPV + ILM peeling in a patient with MS and a very thin residual fovea. Closure of the FTMH was subsequently achieved with a second surgery using the inverted flap technique.

A Preoperative OCT of an MS with very thin residual foveal material. B Formation of a FTMH after PPV + ILM peeling. C Closure of the FTMH after second surgery with inverted flap technique. FTMH full thickness macular hole, ILM internal limiting membrane, MS myopic Schisis, OCT optical coherence tomography, PPV pars plana vitrectomy.
Other complications
The most common complications of MB are diplopia, metamorphopsia and eye movement limitation, reported in 97.0% of cases in the RCT by Zhao et al. [31]. These symptoms gradually resolve during the follow up period, with metamorphopsias typically resolving within three months post-surgery [17]. However, in the large cohort study by Wu et al. [29], six patients (1.58%) underwent strabismus surgery for persistent esotropia, and in one patient (0.26%), the exoplant was removed due to intolerance to diplopia. Liu et al. [17] reported a similar prevalence of persistent esotropia (1/40,2.5%) and binocular diplopia (2/40,5.0%). A transient increase in intraocular pressure (IOP) was reported in 25.92% of cases by Wu et al. [29] and in 32.65% of cases by Zhao et al. [25]. The increase is usually mild, responds well to pressure-lowering agents, and generally resolves spontaneously within the first postoperative month [17]. Haemorrhagic complications are also not uncommon, including discrete subretinal haemorrhages at the staphyloma border [21], epiretinal haemorrhage (17.72%) [25, 29], and vitreous haemorrhage (2.38%) [17, 25, 29]. Susvar et al. [21] reported choroidal detachment in two cases, both of which required drainage and vitrectomy. Zhao et al. [31] reported the development of choroidal neovascularisation in one eye post-surgery. Buckle rejection was reported in four eyes by Wu et al [29] (1.05%) and in one eye by Liu et al [17]. (2.5%). A similar rate was observed for the need for buckle repositioning due to displacement or improper positioning [25, 29]. Lastly, cataract formation is less common in MB compared to PPV, with Zhao et al. reporting it in 5/32 (15.2%) eyes in the MB group [31].
Discussion
Findings from the reviewed studies confirm the importance of carefully selecting the surgical approach for MTM eyes. In agreement with Parolini et al. eyes in which anteroposterior forces are the primary factor benefit significantly from MB alone. ILM peeling in such eyes may induce FTMH formation and should be carefully considered. The presence of O-LMH is a risk factor for FTMH after PPV. Moreover, PPV alone has lower anatomical success rates compared to MB. While BCVA improvement is reported with all treatments, some evidence suggests that MB offers superior long-term outcomes. With MB, final visual acuity is often reached one post-surgery, with the first 3-6 months characterised by visual discomfort due to the high prevalence of metamorphopsia and binocular diplopia. Detailed preoperative counselling is therefore essential before treatment. An increase in IOP should be anticipated in the first postoperative month; however, it is typically mild, transient, and well-managed with topical pressure-lowering agents. It should also be noted that variants in buckle material across different studies impact surgical outcomes, influencing both intraoperative and postoperative complications and the technical complexity of the procedure. This variability should be considered a limitation when comparing study results.
In cases where tangential forces contribute and FTMH is present, combined treatment with MB and PPV provides the best anatomical and functional outcomes. ILM peeling is crucial for resolving of the tangential component of MTM, and the inverted flap technique appears to enhance anatomical success in FTMH cases. However, it should be considered that MB does not solely reduce anterior-posterior traction. In fact, the inverted force exerted by the MB can contribute to release tangential traction when combined with ILM peeling. Additionally, several factors influence postoperative BCVA improvement in all MTM eyes treated with MB, including the duration of preoperative symptoms, preoperative BCVA, patient age, EZ integrity, and the type and severity of the staphyloma. Specifically, younger patients with moderately preserved visual function, short preoperative symptoms duration, type II/IX staphyloma, and an intact EZ benefit the most from MB surgery, both anatomically and functionally. The MSS provides a structured representation of the disease, highlighting its dynamic nature and serving as a valuable tool for surgical decision-making.
Conclusion
The results of our systematic review support the rationale behind the MSS-guided surgical planning. Despite significant advances in MB surgical techniques over time [32], anatomical and functional outcomes have remained largely consistent across different approaches. This consistency reinforces MB surgery as a standard procedure for a broad subset of MTM cases, particularly those in which anteroposterior traction is the primary pathological factor. In contrast, PPV with ILM peeling plays a crucial role in cases involving LMH or FTMH, where it appears to be decisive in resolving tangential traction. A thorough risk-benefit assessment should be conducted, taking into account the specific risk of complications associated with each technique.
References
Ruiz-Medrano J, Montero JA, Flores-Moreno I, Arias L, García-Layana A, Ruiz-Moreno JM. Myopic maculopathy: current status and proposal for a new classification and grading system (ATN). Prog Retinal Eye Res. 2019;69:80–115.
Cheong KX, Xu L, Ohno-Matsui K, Sabanayagam C, Saw SM, Hoang QV. An evidence-based review of the epidemiology of myopic traction maculopathy. Surv Ophthalmol. 2022;67:1603–30.
Parolini B, Palmieri M, Finzi A, Besozzi G, Frisina R. Myopic traction maculopathy: a new perspective on classification and management. Asia-Pac J Ophthalmol. 2021;10:49.
Feng J, Yu J, Chen Q, Zhou H, Chen F, Wang W, et al. Long-term surgical outcomes and prognostic factors of foveal detachment in pathologic myopia: based on the ATN classification. BMC Ophthalmol. 2022;22:175.
Gaucher D, Haouchine B, Tadayoni R, Massin P, Erginay A, Benhamou N, et al. Long-term follow-up of high myopic foveoschisis: natural course and surgical outcome. Am J Ophthalmol. 2007;143:455–462.e1.
Fang X, Weng Y, Xu S, Chen Z, Liu J, Chen B, et al. Optical coherence tomographic characteristics and surgical outcome of eyes with myopic foveoschisis. Eye (Lond). 2009;23:1336–42.
Mete M, Parolini B, Maggio E, Pertile G. 1000 cSt silicone oil vs heavy silicone oil as intraocular tamponade in retinal detachment associated to myopic macular hole. Graefes Arch Clin Exp Ophthalmol. 2011;249:821–6.
Kadonosono K, Yazama F, Itoh N, Uchio E, Nakamura S, Akura J, et al. Treatment of retinal detachment resulting from myopic macular hole with internal limiting membrane removal. Am J Ophthalmol. 2001;131:203–7.
Kinoshita T, Onoda Y, Maeno T. Long-term surgical outcomes of the inverted internal limiting membrane flap technique in highly myopic macular hole retinal detachment. Graefes Arch Clin Exp Ophthalmol. 2017;255:1101–6.
Ripandelli G, Coppé AM, Fedeli R, Parisi V, D’Amico DJ, Stirpe M. Evaluation of primary surgical procedures for retinal detachment with macular hole in highly myopic eyes: a comparison [corrected] of vitrectomy versus posterior episcleral buckling surgery. Ophthalmology. 2001;108:2258–64. Decdiscussion 2265.
Theodossiadis GP, Theodossiadis PG. The macular buckling procedure in the treatment of retinal detachment in highly myopic eyes with macular hole and posterior staphyloma: mean follow-up of 15 years. Retina. 2005;25:285–9.
Tanaka T, Ando F, Usui M. Episcleral macular buckling by semirigid shaped-rod exoplant for recurrent retinal detachment with macular hole in highly myopic eyes. Retina. 2005;25:147–51.
Tian J, Tang LS, Guo XJ, Luo YH. Episcleral macular buckling for posterior retinal detachment in silicone oil filled eyes associated with myopic macular hole. Int J Ophthalmol. 2013;6:165–8.
Alkabes M, Mateo C. Macular buckle technique in myopic traction maculopathy: a 16-year review of the literature and a comparison with vitreous surgery. Graefes Arch Clin Exp Ophthalmol. 2018;256:863–77.
Parolini B, Palmieri M, Finzi A, Besozzi G, Lucente A, Nava U, et al. The new myopic traction maculopathy staging system. Eur J Ophthalmol. 2021;31:1299–312.
Parolini B, Palmieri M, Finzi A, Frisina R. Proposal for the management of myopic traction maculopathy based on the new MTM staging system. Eur J Ophthalmol. 2021;31:3265–76.
Liu B, Chen S, Li Y, Lian P, Zhao X, Yu X, et al. Comparison of macular buckling and vitrectomy for the treatment of macular schisis and associated macular detachment in high myopia: a randomized clinical trial. Acta Ophthalmol. 2020;98:e266–72.
Xiong SQ, Jiang HB, Li FL, Li YX, Yang J, Xia XB, et al. Treatment of myopic foveoschisis via macular buckling and vitrectomy. Int J Ophthalmol. 2017;10:815–8.
Chen J, Chen S, Zhao X, Lian P, Yu X, Huang X, et al. Characteristics and management of myopic traction maculopathy in myopic eyes with axial length less than 26.5 mm. Retina. 2022;42:540–7.
Zou J, Tan W, Li F, Zhou G, Li L, Xiong S, et al. Outcomes of a new 3-D printing-assisted personalized macular buckle combined with para plana vitrectomy for myopic foveoschisis. Acta Ophthalmol. 2021;99:688–94.
Susvar P, Singh N, Bhende P, Rao C. Outcomes of macular buckling with a T-shaped buckle for myopic tractional maculopathies associated with posterior staphyloma: an Indian experience. Indian J Ophthalmol. 2022;70:171–9.
Sood G, Susvar P. Correlation of morphological characteristics of staphyloma with the structural and functional outcomes of myopic traction maculopathy after macular buckle surgery. Indian J Ophthalmol. 2021;69:1464–8.
Zhao X, Wang Y, Chen Y, Tanumiharjo S, Wu Y, Lian P, et al. Factors affecting visual prognosis of myopic foveoschisis after macular buckling. J Ophthalmol. 2022;2022:9293347.
Li J, Li Y, Chen S, Ma W, Zhao X, Huang X, et al. Outcomes of macular buckling surgery in myopic foveal detachment eyes with and without disrupted ellipsoid zone band: a case-control study. Graefes Arch Clin Exp Ophthalmol. 2021;259:2513–9.
Zhao X, Ma W, Lian P, Tanumiharjo S, Lin Y, Ding X, et al. Three-year outcomes of macular buckling for macular holes and foveoschisis in highly myopic eyes. Acta Ophthalmol. 2020;98:e470–8.
Bedda AM, Abdel Hadi AM, Lolah M, Abd Al Shafy MS. A new sutureless illuminated macular buckle designed for myopic macular hole retinal detachment. J Ophthalmol. 2017;2017:6742164.
Ma J, Li H, Ding X, Tanumiharjo S, Lu L. Effectiveness of combined macular buckle under direct vision and vitrectomy with ILM peeling in refractory macular hole retinal detachment with extreme high axial myopia: a 24-month comparative study. Br J Ophthalmol. 2017;101:1386–94.
Luo N, Chen S, Zhao X, Huang Y, Wang Y, Li J, et al. Macular buckling combined with vitrectomy and inverted internal limiting membrane flap technique for macular holes with macular retinoschisis without retinal detachment in high myopia. Retina. 2022;42:2051–8.
Wu ZQ, Zhao XJ, Chen SD, Lian P, Li J, Ma W, et al. Macular buckling for highly myopic traction maculopathy]. Zhonghua Yan Ke Za Zhi. 2021;57:433–9.
Palmieri M, Frisina R, Finzi A, Besozzi G, Parolini B. The role of the outer lamellar macular hole in the surgical management of myopic traction maculopathy. Ophthalmologica. 2021;244:229–36.
Zhao X, Song H, Tanumiharjo S, Wang Y, Chen Y, Chen S, et al. Macular buckling alone versus combined inverted ILM flap on macular hole-associated macular detachment in patients with high myopia. Eye (Lond). 2023;37:2730–5.
Susvar P, Sood G. Current concepts of macular buckle in myopic traction maculopathy. Indian J Ophthalmol. 2018;66:1772–84.
Author information
Authors and Affiliations
Contributions
Design of the review: BP, EC; Literature Search: EC, FC, VM, RF; Draft: EC, FC, VM; Revision: BP, EC, FC, RF.
Corresponding author
Ethics declarations
Competing interests
RF is a member of the Eye editorial board. No conflict of interest exists for any other author
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Crincoli, E., Frisina, R., Catania, F. et al. Indications for macular buckle in myopic traction maculopathy based on MTM staging system: a systematic review. Eye 40, 765–775 (2026). https://doi.org/10.1038/s41433-026-04289-4
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41433-026-04289-4
