
Abstract
The role of serum uric acid as a predictor of stroke among the general Japanese population remains controversial. We conducted a prospective cohort study of 5235 men and 8185 women aged 40–79 years at baseline between 1985 and 1994 in four Japanese communities, who were initially free from stroke, coronary heart disease, and medication for hyperuricemia or gout. Cox proportional hazards models were used to estimate sex-specific hazard ratios of stroke and its types in relation to serum uric acid level. During a median follow-up of 23.1 years, we recorded 1018 (488 men and 530 women) incident strokes, including 222 (99 and 123) intraparenchymal hemorrhages, 113 (33 and 80) subarachnoid hemorrhages and 667 (347 and 320) ischemic strokes. After adjustment for age, community and known cardiovascular risk factors, the multivariable hazard ratios (95% CIs) in the highest vs. lowest quintile of serum uric acid were 1.45 (1.07–1.96) for total stroke, 1.20 (0.65–2.20) for intraparenchymal hemorrhage, 1.46 (0.69–3.09) for subarachnoid hemorrhage and 1.61 (1.07–2.41) for ischemic stroke in women. The corresponding multivariable hazard ratios (95% CIs) in men were 1.02 (0.74–1.35), 0.83 (0.40–1.72), 1.19 (0.38–3.75) and 1.00 (0.70–1.41). Furthermore, those positive associations with risks of total and ischemic strokes in women were more evident in nonusers of antihypertensive medication than the users. In conclusion, elevated serum uric acid level is an independent predictor of total stroke in women but not in men. The positive association in women was mostly attributable to ischemic stroke and was more pronounced among nonusers of antihypertensive medication.
Similar content being viewed by others

Introduction
Uric acid is the end product of purine catabolism, and it is positively associated with known cardiovascular risk factors, e.g., obesity, dyslipidemia, impaired glucose tolerance, chronic kidney disease and hypertension [1,2,3]. Elevated serum uric acid levels could stimulate the renin–angiotensin system and restrain release of endothelial nitric oxide, contributing to preglomerular arteriolosclerosis and increasing blood pressure [4,5,6]. Furthermore, elevated serum uric acid has been an indicator of oxidative stress due to its compensatory mechanism against oxidative stress resulting from atherosclerosis and aging [7]. A recent meta-analysis of 13 cohort studies showed that serum uric acid level was positively associated with risk of stroke in both sexes, whereas this association trended to be nonlinear in men [8]. European prospective cohort studies reported consistent results to support the predictive role of serum uric acid in the risk of stroke [9,10,11,12,13], but findings from American [14, 15] and Asian cohort studies [16,17,18,19,20] remain controversial.
Elevated serum uric acid is regularly observed among hypertensive patients with antihypertensive medication use, especially diuretic use [21]. The Atherosclerosis Risk in Communities (ARIC) study found that serum uric acid level was positively associated with the risk of ischemic stroke in nonusers of diuretic stroke but not in users [15], suggesting that diuretic-induced elevated serum uric acid is not a predictor of the risk of ischemic stroke. Based on prior studies, we hypothesized that elevated serum uric acid would be an independent predictor of the risk of stroke among the general Japanese population and that this association would be mainly observed in subjects without antihypertensive medication use.
Methods
Study population
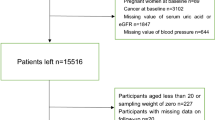
The present study is part of the Circulatory Risk in Communities Study (CIRCS), a prospective community-based study of cardiovascular disease among the general Japanese population that has run since 1963 [22, 23]. The surveyed population included 5442 men and 8279 women aged 40–79 years who participated in annual health checkups that included the examination of serum uric acid between 1985 and 1994. The subjects were enrolled from four communities: Ikawa (a rural town in Akita Prefecture in northwestern Japan), the Minami-Takayasu district in Yao (a southwestern suburb in Osaka Prefecture), Noichi (a rural community in Kochi Prefecture in southwestern Japan), and Kyowa (a rural town in Ibaraki Prefecture in central Japan). The baseline surveys were conducted in 1985–1990, 1985–1994, 1985–1990 and 1985–1991, respectively. After the exclusion of subjects who had a history of stroke or coronary heart disease (162 men and 92 women) and users of medication for hyperuricemia or gout (45 men and 2 women) at baseline, 5235 men and 8185 women were eligible for this analysis. Subjects were followed to track incident strokes and their types until the end of 2010 for Noichi, 2011 for Kyowa, and 2013 for Ikawa and Yao. Informed consent was obtained from the community representatives rather than each subject because the present study was a secondary use of existing data for public health practice on cardiovascular disease prevention in local communities. Ethical approval of the CIRCS study has been given by the Ethics Committee of the Osaka Center for Cancer and Cardiovascular Disease Prevention and of Osaka University.
Ascertainment of cases
The previous CIRCS publications have reported the details of endpoint determination [22, 23]. Candidate cases of stroke were obtained from various information sources of death certificates, national insurance claims, annual household questionnaires, annual cardiovascular risk surveys, and reports by either local physicians, public health nurses, or health volunteers. To confirm the diagnoses, all living suspected stroke patients were phoned, visited or invited to take part in risk factor surveys, or alternatively, a medical history was obtained from their families. Furthermore, medical records in the local clinics and hospitals were reviewed. In the case of death, histories from families and/or attending physicians were obtained, and medical records were reviewed. Stroke was defined as a focal neurological disorder that had a rapid onset and lasted at least 24 h or until death. Stroke subtypes were classified as intraparenchymal hemorrhage, subarachnoid hemorrhage, ischemic stroke (large-artery occlusive infarction, lacunar infarction or others), and unclassified stroke, primarily by using CT or MRI [24], which were available for 93.8% of stroke cases. The same diagnostic criteria for incident stroke and its types were used in all communities throughout the whole study period.
Baseline examination
For all subjects, blood samples were drawn while the patient was in a seated position, stored in plain, siliconized glass tubes, and centrifuged. The serum was separated within 30 min. The blood test method and measurement instrument changed twice: on September 1, 1986 and on July 22, 1993. Serum uric acid was first measured with the phosphotungstic acid method using an SMA-6/60 automatic analyzer (Technicon, Tarrytown, NY, USA), then the uricase method using an SMAC automatic analyzer (Technicon), and finally the same uricase method using an Autoanalyzer 7250 (Hitachi Medical Corp., Ibaraki, Japan). Serum glucose was measured with the cupric-neocuproine method using the SMA-6/60, the hexokinase method using the SMAC and the glucokinase method using the Autoanalyzer 7250. The values of serum glucose (mmol/L) measured using the cupric-neocuproine method were adjusted by using a linear regression formula: serum glucose concentration (mg/dL) × 0.0474 + 0.541. Serum creatinine was measured originally with the noncompensated kinetic Jaffe method using the SMA-6/60, SMAC, and Autoanalyzer 7250 in different periods and was converted to a value consistent with the enzymatic method by subtracting 0.2 mg/dL [25]. These measurements were performed at the Osaka Medical Central for Cancer and Cardiovascular Disease, an international member of the US National Cholesterol Reference Method Laboratory Network [26, 27].
An interview was conducted by trained observers to ascertain the smoking status, number of cigarettes smoked per day, usual weekly intake of alcohol evaluated in go units (a traditional Japanese unit of volume corresponding to 23 g of ethanol), and use of medication for hypertension or diabetes mellitus. In women, menopausal status was ascertained, and postmenopausal status was defined by the end of menstruation more than 6 months earlier. Height in stocking feet and weight in light clothing were measured during health checkups, and body mass index was calculated as weight (kg) divided by the square of height (m2). Systolic and diastolic blood pressure in the right arm were measured using standard mercury sphygmomanometers [28]. Diabetes mellitus was defined as a fasting glucose level of ≥7.0 mmol/L, a nonfasting glucose level of ≥11.1 mmol/L or use of medication for diabetes mellitus. The estimated glomerular filtration rate (eGFR) was calculated using a standardized formula from the Japan Society of Nephrology Chronic Kidney Disease Initiative Guidelines: eGFR (ml/min per 1.73 m2) = 194 × (serum creatinine [enzyme method])−1.094 × (age)−0.287 × (0.739 in women) [29]. Atrial fibrillation was diagnosed using the standard 12-lead electrocardiogram.
Statistical analyses
In view of the different levels of serum uric acid between men and women, sex-specific analyses were performed in the present study. Age- and community-adjusted mean values or the prevalence of baseline characteristics were compared according with quintiles of serum uric acid using analysis of covariance. Cox proportional hazards models were used to calculate sex-specific hazard ratios (with 95% confidence intervals (CIs)) of stroke and its types according to quintile of serum uric acid and per 1-standard-deviation (SD) increment of serum uric acid (1.3 mg/dL in men and 1.0 mg/dL in women).
The initial hazard ratio model was adjusted for age and community, while the multivariable model added body mass index (sex-specific quartiles), cigarette smoking status (never, former, or current 1-19 or 20 cigarettes per day), alcohol intake status (never, former, or current <23, 23–45, or ≥46 g ethanol per day), systolic blood pressure (mmHg), antihypertensive medication use (no or yes), atrial fibrillation (no or yes), serum total cholesterol (mmol/L), serum triglycerides (sex-specific quartiles), eGFR (sex-specific quartiles), and diabetes mellitus (no or yes), plus menopausal status (pre- or postmenopausal) in women. To assess whether antihypertensive medication-induced changes in serum uric acid modified these associations, we conducted a subgroup analysis and stratified subjects into users and nonusers of antihypertensive medication.
The SAS System (version 9.4; SAS Inc., Cary, NC) was used in all statistical analyses. P values < 0.05 were defined as statistically significant with two-tailed statistical tests.
Results
Table 1 shows sex-specific, age- and community-adjusted mean values or the prevalence of known cardiovascular risk factors at baseline according to serum uric acid quintile. Subjects with elevated serum uric acid levels were older than the other subjects among the women but similar in age to normouricemic subjects among the men. In both sexes, serum uric acid level was positively associated with body mass index, systolic and diastolic blood pressure, the prevalence of antihypertensive medication use, serum total cholesterol, triglycerides and ethanol intake, and negatively associated with eGFR. Serum uric acid level was positively associated with the prevalence of postmenopausal status in women. In addition, serum uric acid level was positively associated with the prevalence of current smokers in women but negatively associated with the prevalence in men. Subjects with higher serum uric acid levels had a higher prevalence of atrial fibrillation and a lower prevalence of diabetes mellitus in men but a similar prevalence in women.
During the median 23.1-year follow-up, a total of 275,535 person-years, 1018 (488 men and 530 women) cases of incident stroke, including 222 (99 men and 123 women) intraparenchymal hemorrhages, 113 (33 men and 80 women) subarachnoid hemorrhages, 667 (347 men and 320 women) ischemic strokes, and 16 (9 men and 7 women) unclassified stroke, were documented.
Table 2 lists sex-specific, age-adjusted, and community-adjusted multivariable hazard ratios of total stroke, intraparenchymal hemorrhage, subarachnoid hemorrhage, and ischemic stroke according to serum uric acid quintiles. After adjustment for age, community, and main cardiovascular risk factors, the multivariable hazard ratios (95% CIs) of total stroke in the highest vs. lowest quintile of serum uric acid were 1.02 (0.74–1.35) (P for trend = 0.89) in men and 1.45 (1.07–1.96) (P for trend = 0.007) in women. The multivariable hazard ratios (95% CIs) of total stroke for a 1 SD increment in serum uric acid were 1.02 (0.92–1.13) in men and 1.12 (1.03–1.22) in women. The positive association was confined to women, and the sex interaction was statistically significant (P for interaction < 0.05). When stratified by age, the association with the risk of total stroke in women did not vary; the multivariable hazard ratios (95% CIs) for each 1 SD increment of serum uric acid were 1.17 (0.99-1.38) for ages 40–54 and 1.12 (1.01-1.25) for ages 55–79 (data not shown). In women, serum uric acid level was positively associated with the risk of ischemic stroke, but not with intraparenchymal hemorrhage or subarachnoid hemorrhage. The multivariable hazard ratios (95% CIs) of ischemic stroke, intraparenchymal hemorrhage and subarachnoid hemorrhage stroke in the highest vs. lowest quintile of serum uric acid were 1.61 (1.07–2.41) (P for trend = 0.07), 1.20 (0.65–2.20) (P for trend = 0.18) and 1.46 (0.69–3.09) (P for trend = 0.15), respectively. In men, no positive associations were observed, and the corresponding multivariable hazard ratios (95% CIs) were 1.00 (0.70–1.41) (P for trend = 0.94), 0.83 (0.40–1.72) (P for trend = 0.83) and 1.19 (0.38–3.75) (P for trend = 0.27).
We next conducted a subgroup analysis, stratified by use of antihypertensive medication or not, and the results are summarized in Table 3. In women, serum uric acid level was positively associated with the risks of total stroke and ischemic stroke in nonusers of antihypertensive medication, but not in the users, although the interaction with antihypertensive medication was not statistically significant (P for interaction = 0.87); the multivariable hazard ratios (95% CIs) in the highest vs. lowest quintile of serum uric acid was 1.46 (1.02–2.09) (P for trend = 0.02) for total stroke and 1.62 (1.00–2.63) (P for trend = 0.12) for ischemic stroke in nonusers of antihypertensive medication. The multivariable hazard ratios (95% CIs) for each 1 SD increment in serum uric acid were 1.11 (1.00–1.24) for total stroke and 1.06 (0.91–1.22) for ischemic stroke in nonusers of antihypertensive medication. In men, no positive association with quintile of serum uric acid or per 1 SD increment of serum uric acid was observed for total or ischemic stroke in either nonusers or users of antihypertensive medication.
Discussion
In this prospective community-based study of 5235 men and 8185 women aged 40–79 years, we found that serum uric acid level was positively associated with the risk of total stroke in women, but not in men. The positive association in women was mostly attributable to ischemic stroke and was more pronounced among nonusers of antihypertensive medication.
A recent meta-analysis of 12 prospective cohort and one nested case-control study showed the positive association of serum uric acid with risk of stroke in both sexes; the relative risk (95% CI) of stroke for a 1 mg/dL increment in serum uric acid was 1.10 (1.05–1.14) in men and 1.11 (1.09–1.13) in women. In that meta-analysis, a dose-response association was found in women (P for nonlinear trend = 0.51). However, the association of serum uric acid with risk of stroke tended to be nonlinear in men (P for nonlinear trend < 0.001), and the risk of stroke increased significantly and steeply when the value of serum uric acid exceeded 6 mg/dL [8].
Although European perspective cohort studies consistently found a positive association of serum uric acid level with risk of stroke [9,10,11,12,13], findings from Asian studies have remained inconsistent [16,17,18,19,20]. The Chin‐Shan Community Cardiovascular Cohort Study of 1703 Taiwanese men and 1899 women aged 35 years or older with an 11-year follow-up reported that plasma uric acid was positively associated with risk of incident stroke; the multivariable hazard ratios (95% CIs) of each 1 mg/dL increment of plasma uric acid were 1.13 (0.88–1.46) in men and 1.32 (1.00–1.73) in women [16]. A 2-year follow-up study of 61,304 Japanese men and 94,018 women aged 40–73 years reported J-shaped associations of serum uric acid level with risk of self-reported nonfatal stroke; the multivariable odds ratio (95% CI) in the highest (≥7.1 mg/dL in men and ≥5.5 mg/dL in women) vs. the third quintile (5.7–6.2 mg/dL in men and 4.4–4.8 mg/dL in women) of serum uric acid was 1.26 (1.04–1.54) in men and 1.24 (1.00–1.48) in women [17]. However, the NIPPON DATA 80 study of 3596 Japanese men and 4576 women aged 30 years or older with 14-year follow-up and the Evidence for Cardiovascular Prevention from Observational Cohorts in Japan (EPOCH-JAPAN) Study of 15,628 Japanese men and 20,685 women aged 35–89 years with 441,771 person-years of follow-up reported that serum uric acid level was not associated with risk of stroke mortality in either sex [18, 19]. A 9-year-follow-up study of 22,698 Korean men aged 30–77 years reported no association with risk of stroke mortality [20].
The associations of serum uric acid level with risk of stroke tended to be nonlinear. The NIPPON DATA 80 study reported that the multivariable hazard ratios (95% CIs) of total stroke for each quartile of serum uric acid were 0.84 (0.45–1.59), 0.66 (0.33–1.33) and 1.71 (0.92–3.17) in men and 1.40 (0.54–3.63), 0.95 (0.37–2.45), and 1.12 (0.46–2.74) in women, respectively [18]. The EPOCH-JAPAN study reported that the corresponding multivariable hazard ratios (95% CIs) for each quintile of serum uric acid were 0.83 (0.58–1.18), 0.77 (0.52–1.13), 0.77 (0.52–1.13), and 1.19 (0.84–1.68) in men and 1.27 (0.90–2.01), 0.98 (0.62–1.54), 1.05 (0.67–1.64), and 1.46 (0.98–2.19) in women [19]. Men had higher serum uric acid levels than women, even than postmenopausal women. The absence of an association between serum uric acid level and the risk of stroke in the present study in men could be due to the antioxidant effect of serum uric acid. Furthermore, our study found J-shaped associations with risks of subarachnoid hemorrhage and ischemic stroke in men and intraparenchymal and subarachnoid hemorrhage in women, which could be influenced in part by the antioxidant effect.
Antihypertensive medications, such as diuretics, β-blockers, angiotensin-converting enzyme inhibitors, and non-losartan angiotensin II receptor blockers, have an effect of increasing blood uric acid concentrations, while other medications, such as calcium channel blockers and losartan, have an opposite effect in hypertensive patients [21]. The ARIC study of 13,413 American men and women aged 45–64 years with a 12.6-year follow-up reported a positive association of serum uric acid level with risk of ischemic stroke in nonusers of diuretics, but not in the users; the multivariable hazard ratios (95% CIs) of ischemic stroke in the highest (≥6.9 mg/dL) vs. lowest quartile (≤4.8 mg/dL) of serum uric acid were 1.49 (1.00–2.23) in nonusers of diuretics and 0.73 (0.40–1.34) in the users [15]. In Japan during the 1980s, calcium channel blockers and angiotensin-converting enzyme inhibitors were approved by the Ministry of Health, Labor and Welfare and were selected as first-choice drugs for hypertension treatment [30]. Those drugs were likely to induce decreased or elevated serum uric acid levels and could weaken the association of serum uric acid level with risk of stroke.
The potential mechanisms underlying the positive association of elevated uric acid with risk of stroke remain uncertain, although several possibilities have been proposed. First, elevated uric acid level has been associated with increased mean platelet volume [31], vascular endothelial function [32], vascular smooth muscle cell proliferation and inflammation [33], thereby increasing the risk of ischemic stroke. Second, uric acid-induced microvascular injury, e.g., vascular smooth muscle cell proliferation, could lead to preglomerular vascular disease and elevated blood pressure [4,5,6]. Animal studies found that once microvascular injury occurred, hypertension became salt-driven and was independent of uric acid [34], while uric acid continued to cause preglomerular vascular disease, even under diuretic treatment [35]. These findings suggest that uric acid-induced microvascular disease other than hypertension may account for the increased risk of stroke. Third, uric acid has a powerful free radical–scavenging capacity, helping fight oxidative stress [36]. A nested case-control study of 150 cases with elevated carotid intimal-medial thickness and 150 age-sex-matched controls within the ARIC study cohort showed that atherosclerosis patients had higher oxygen radical absorbance capacities than controls, and this difference was explained mostly by their higher serum uric acid levels [7]. Such a protective effect might explain the positive association of serum uric acid level with risk of stroke in men, partly due to their higher serum uric acid levels compared with those in women.
As for the strengths of our study, we used incident cases of stroke and its types as the target endpoints because serum uric acid may be more directly associated with these than with fatal outcomes. In addition, we analyzed these associations stratified by antihypertensive medication use, which allowed us to investigate these sex-specific associations among subjects with pharmacologically inducted hyperuricemia.
Our study has several potential limitations. The single measurement of serum uric acid at baseline could make the associations biased toward null due to the random measurement variations. In that case, the real association would be greater than that we reported. We have no data on the use of diuretics or other type-specific antihypertensive medications, so we could not investigate the impact of medication-induced elevated or decreased serum uric acid levels on risk of stroke.
In conclusion, elevated serum uric acid level is an independent predictor for total stroke in women but not in men of the general Japanese population. The positive association in women was mostly attributable to ischemic stroke and was more pronounced among nonusers of antihypertensive medication.
References
Wu AH, Gladden JD, Ahmed M, Ahmed A, Filippatos G. Relation of serum uric acid to cardiovascular disease. Int J Cardiol. 2016;213:4–7.
Borghi C, et al. Serum uric acid and the risk of cardiovascular and renal disease. J Hypertens. 2015;33:1729–41.
Feig DI, Kang DH, Johnson RJ. Uric acid and cardiovascular risk. N. Engl J Med. 2008;359:1811–21.
Perlstein TS, et al. Uric acid and the state of the intrarenal renin-angiotensin system in humans. Kidney Int. 2004;66:1465–70.
Mazzali M, et al. Elevated uric acid increases blood pressure in the rat by a novel crystal-independent mechanism. Hypertension. 2001;38:1101–6.
Lee SW, et al. Age-differential association between serum uric acid and incident hypertension. Hypertens Res. 2019;42:428–37.
Nieto FJ, Iribarren C, Gross MD, Comstock GW, Cutler RG. Uric acid and serum antioxidant capacity: a reaction to atherosclerosis? Atherosclerosis. 2000;148:131–9.
Zhong C, Zhong X, Xu T, Xu T, Zhang Y. Sex-specific relationship between serum uric acid and risk of stroke: a dose-response meta-analysis of prospective studies. J Am Heart Assoc. 2017;6:e005042.
Holme I, Aastveit AH, Hammar N, Jungner I, Walldius G. Uric acid and risk of myocardial infarction, stroke and congestive heart failure in 417,734 men and women in the Apolipoprotein MOrtality RISk study (AMORIS). J Intern Med. 2009;266:558–70.
Strasak A.VHM&PP Study Group. et al. Serum uric acid and risk of cardiovascular mortality: a prospective long-term study of 83,683 Austrian men. Clin Chem. 2008;54:273–84.
Strasak AM.VHM&PP Study Group. et al. Serum uric acid is an independent predictor for all major forms of cardiovascular death in 28,613 elderly women: a prospective 21-year follow-up study. Int J Cardiol. 2008;125:232–9.
Bos MJ, Koudstaal PJ, Hofman A, Witteman JC, Breteler MM. Uric acid is a risk factor for myocardial infarction and stroke: the Rotterdam Study. Stroke. 2006;37:1503–7.
Storhaug HM, et al. Uric acid is a risk factor for ischemic stroke and all-cause mortality in the general population: a gender specific analysis from The Tromsø Study. BMC Cardiovasc Disord. 2013;13:115.
Jimenez MC, Curhan GC, Choi HK, Forman JP, Rexrode KM. Plasma uric acid concentrations and risk of ischaemic stroke in women. Eur J Neurol. 2016;23:1158–64.
Hozawa A, et al. Serum uric acid and risk of ischemic stroke: the ARIC Study. Atherosclerosis. 2006;187:401–7.
Chien KL, et al. Hyperuricemia as a risk factor on cardiovascular events in Taiwan: the Chin‐Shan Community Cardiovascular Cohort Study. Atherosclerosis. 2005;183:147–55.
Kamei K, et al. Associations between serum uric acid levels and the incidence of nonfatal stroke: a nationwide community-based cohort study. Clin Exp Nephrol. 2017;21:497–503.
Sakata K, Hashimoto T, Ueshima H, Okayama A. NIPPON DATA 80 Research Group. Absence of an association between serum uric acid and mortality from cardiovascular disease: NIPPON DATA 80, 1980–1994. Eur J Epidemiol. 2001;17:461–8.
Zhang W, et al. EPOCH-JAPAN GROUP. Serum uric acid and mortality form cardiovascular disease: EPOCH-JAPAN Study. J Atheroscler Thromb. 2016;23:692–703.
Jee SH, Lee SY, Kim MT. Serum uric acid and risk of death from cancer, cardiovascular disease or all causes in men. Eur J Cardiovasc Prev Rehabil. 2004;11:185–91.
Choi HK, Soriano LC, Zhang Y, Rodríguez LA. Antihypertensive drugs and risk of incident gout among patients with hypertension: population based case-control study. BMJ. 2012;344:d8190.
Imano H, et al. Trends for blood pressure and its contribution to stroke incidence in the middle-aged Japanese population: the Circulatory Risk in Communities Study (CIRCS). Stroke. 2009;40:1571–7.
Yamagishi K, et al. The Circulatory Risk in Communities Study (CIRCS): a long-term epidemiological study for lifestyle-related disease among japanese men and women living in communities. J Epidemiol. 2019;29:83–91.
Iso H, Rexrode K, Hennekens CH, Manson JE. Application of computer tomography-oriented criteria for stroke subtype classification in a prospective study. Ann Epidemiol. 2000;10:81–87.
Coresh J, et al. Calibration and random variation of the serum creatinine assay as critical elements of using equations to estimate glomerular filtration rate. Am J Kidney Dis. 2002;39:920–9.
Nakamura M, et al. Total cholesterol performance of Abell-Levy-Brodie-Kendall reference measurement procedure: certification of Japanese in-vitro diagnostic assay manufacturers through CDC’s Cholesterol Reference Method Laboratory Network. Clin Chim Acta. 2015;445:127–32.
Nakamura M, et al. Comparison between the triglycerides standardization of routine methods used in Japan and the chromotropic acid reference measurement procedure used by the CDC Lipid Standardization Programme. Ann Clin Biochem. 2016;53:632–9.
Kirkendall WM, Feinlieb M, Freis ED, Mark AL. Recommendations for human blood pressure determination by sphygmomanometers. Subcommittee of the AHA Postgraduate Education Committee. Circulation. 1980;62:1146A–1155A.
Matsuo S, et al. Collaborators developing the Japanese equation for estimated GFR. Collaborators developing the Japanese equation for estimated GFR. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53:982–92.
Ozawa H. Fifty years history of new drugs in Japan: the developments and trends of antihypertensive drugs. Yakushigaku Zasshi. 2000;35:63–71. [Article in Japanese]
Shimodaira M, et al. Gender differences in the relationship between serum uric acid and mean platelet volume in a Japanese general population. Platelets. 2014;25:202–6.
Otani N, et al. Effects of uric acid on vascular endothelial function from bedside to bench. Hypertens Res. 2018;41:923–31.
Kanellis J, et al. Uric acid stimulates monocyte chemoattractant protein-1 production in vascular smooth muscle cells via mitogen-activated protein kinase and cyclooxygenase-2. Hypertension. 2003;41:1287–93.
Watanabe S, et al. Uric acid, hominoid evolution, and the pathogenesis of salt-sensitivity. Hypertension. 2002;40:355–60.
Feig DI, et al. Hypothesis: Uric acid, nephron number, and the pathogenesis of essential hypertension. Kidney Int. 2004;66:281–7.
Glantzounis GK, Tsimoyiannis EC, Kappas AM, Galaris DA. Uric acid and oxidative stress. Curr Pharm Des. 2005;11:4145–51.
Acknowledgements
We thank our colleagues from Osaka University Center of Medical Data Science, Advanced Clinical Epidemiology Investigator’s Research Project for providing their insight and expertise for our research.
Appendix
The CIRCS Investigators are: Takeo Okada, Yuji Shimizu, Yasuhiko Kubota, Shinichi Sato, Mina Hayama-Terada and Masahiko Kiyama, Osaka Center for Cancer and Cardiovascular Disease Prevention; Hironori Imano, Renzhe Cui, Isao Muraki, Akihiko Kitamura, Hiroshige Jinnouchi, Mizuki Sata and Hiroyasu Iso, Osaka University; Kazumasa Yamagishi, Mitsumasa Umesawa and Tomoko Sankai, University of Tsukuba; Koutatsu Maruyama, Ehime University; Ai Ikeda and Takeshi Tanigawa, Juntendo University, and Masanori Nagao and Tetsuya Ohira, Fukushima Medical University.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Members of the CIRCS investigators are listed below the Acknowledgements.
Rights and permissions
About this article

Cite this article
Li, J., Muraki, I., Imano, H. et al. Serum uric acid and risk of stroke and its types: the Circulatory Risk in Communities Study (CIRCS). Hypertens Res 43, 313–321 (2020). https://doi.org/10.1038/s41440-019-0385-5
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41440-019-0385-5
Keywords
This article is cited by
-
Association between serum urate levels and all-cause mortality, cardiovascular and renal outcomes among gout patients in Singapore
BMC Rheumatology (2024)
-
Moderate elevation of serum uric acid levels improves short-term functional outcomes of ischemic stroke in patients with type 2 diabetes mellitus
BMC Geriatrics (2023)
-
Annual reports on hypertension research 2020
Hypertension Research (2022)
-
Impact of hyperuricemia on chronic kidney disease and atherosclerotic cardiovascular disease
Hypertension Research (2022)
-
J-shaped curve for the association between serum uric acid levels and the prevalence of blood pressure abnormalities
Hypertension Research (2021)
