
Abstract
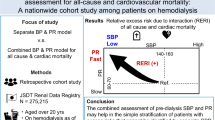
Blood pressure (BP) is reportedly a predictor of mortality in hemodialysis (HD) patients; however, it is unclear whether pre- or postdialysis BP has greater predictive power. To evaluate the association of pre- and postdialysis BP with patient survival in Japanese HD patients, we enrolled the entire phase 3 and 4 Japan Dialysis Outcomes and Practice Patterns Study populations. Among 3176 patients, 486 were excluded because of missing data. The remaining 2690 patients were divided into five groups according to pre- or postdialysis systolic BP (SBP): <100, 100–119, 120–139, 140–159, and ≥160 mmHg; diastolic BP (DBP): <60, 60–79, 80–89, 90–99, and ≥100 mmHg; or pulse pressure (PP): <50, 50–59, 60–69, 70–79, and ≥80 mmHg. The hazard ratios for all-cause and cardiovascular mortalities were estimated according to pre- and postdialysis SBP, DBP, and PP using a Cox proportional hazards model. During the follow-up period, 495 and 193 subjects died because of any cause and cardiovascular disease (CVD), respectively. In the multivariable-adjusted Cox proportional hazards model, U-shaped associations of postdialysis SBP and PP with mortality rates were observed, but no significant associations were observed with predialysis SBP or PP. A stratified analysis showed significant interactions between history of CVD and postdialysis SBP with all-cause and cardiovascular mortality. Compared with predialysis values, postdialysis SBP and PP are better predictors of all-cause and cardiovascular mortality, showing U-shaped associations with these outcomes in Japanese HD patients.
Similar content being viewed by others
Introduction
In contrast to the general population, in which a higher blood pressure (BP) is recognized as a strong risk factor for mortality and cardiovascular events [1], lower BP has reportedly been associated with a higher mortality in patients receiving hemodialysis (HD) [2, 3]. This finding has been termed “reverse epidemiology” [4].
More recently, we reported the prognostic value of predialysis BP for all-cause mortality and cardiovascular events in 3436 patients receiving chronic HD in the Q-Cohort Study in Japan [5]. Furthermore, postdialysis BP is also considered an excellent predictor of mortality, equivalent to predialysis BP [3, 4]. In addition, higher pulse pressure (PP), regardless of predialysis or postdialysis measurement, is reportedly associated with mortality [6].
The weekly average BP, on the basis of 20 readings (twice a day at home for 1 week plus twice during each dialysis session, three times a week in the hospital), is also reportedly of greater predictive value for cardiovascular disease (CVD) than a single-point BP measurement [7]. However, calculation of the weekly average BP is inconvenient, and home BP readings may be unreliable.
The association of BP values with patient outcomes reportedly differs according to age and the presence of comorbidities such as diabetes mellitus and CVD [8]. Thus, the BP measurement in HD patients with the best predictive value remains unclear; in particular, the predictive values of predialysis and postdialysis BP have been disputed because of their highly variable nature [9,10,11]. This study investigated which parameters (predialysis or postdialysis BP; systolic BP (SBP), diastolic BP (DBP), or PP) are the best predictors of all-cause and cardiovascular mortality in patients receiving HD and determined the ideal BP target for the best prognosis in HD patients.
Methods
Study population
The Dialysis Outcomes and Practice Patterns Study (DOPPS) is based on a prospective cohort. We enrolled the entire Japan DOPPS phase 3 (J-DOPPS 3; 2005–2008; n = 2321) and 4 (J-DOPPS 4; 2009–2012; n = 2254) populations. The characteristics of the populations and data collection methods have been described previously [12, 13]. Within the DOPPS cohort, patients treated in Japan were considered the target population. The exclusion criteria were as follows: missing critical demographic or laboratory data such as age, dialysis vintage, sex, primary cause of end-stage renal disease, and BP. Written informed consent for inclusion in the DOPPS was obtained from all subjects. The DOPPS protocol is compliant with the Declaration of Helsinki.
Patients were divided into five groups according to pre- or postdialysis SBP: <100, 100–119, 120–139, 140–159, and ≥160 mmHg; DBP: <60, 60–79, 80–89, 90–99, and ≥100 mmHg; or PP: <50, 50–59, 60–69, 70–79, and ≥80 mmHg. The hazard ratios (HRs) with 95% confidence intervals (CIs) for all-cause and cardiovascular mortality were estimated according to pre- and postdialysis SBP, DBP, and PP using a Cox proportional hazards model.
Measurements of predialysis and postdialysis BP
Predialysis BP was measured in the nonaccess arm after a few minutes of rest with the patients in a sitting position on the dialysis chair or bed before placement of a dialysis needle at the beginning of the last HD of the week, that is, on Friday or Saturday. Postdialysis BP was measured in the nonaccess arm with the patients in a sitting position after the same HD session in which predialysis BP was measured.
Outcomes
The primary outcomes were all-cause and cardiovascular mortality.
Statistical analyses
Baseline data are shown as the mean ± standard deviation for normally distributed continuous variables, median (interquartile range) for nonnormally distributed continuous variables, or number (percentage) for categorical variables. The distribution of baseline data according to BP level was compared using trend analysis. A highly skewed variable (vintage) was transformed with the natural logarithm function prior to use in models [ln(vintage)]. The unadjusted and multivariable-adjusted HRs with 95% CIs for all-cause or cardiovascular mortality according to each BP level were calculated using the Cox proportional hazards model. The multivariable model was adjusted for age, sex, log-transformed dialysis vintage, diabetic nephropathy as primary kidney disease, smoking habits, ultrafiltration rate, body mass index, history of cancer, history of CVD, hemoglobin, albumin-corrected calcium, serum phosphate, use of calcium channel blockers (CCBs), use of renin–angiotensin system inhibitors (RASIs), and use of vasopressor agents. Other established prognostic factors, such as C-reactive protein and erythropoiesis-stimulating agent resistance index, were not used as adjustment factors because of the large amount of missing data for these parameters. In the subgroup analysis, multivariable-adjusted HRs with 95% CIs for BP and mortality were calculated. We tested for heterogeneity between each BP parameter and cardiovascular comorbidity by adding a multiplicative interaction term to our statistical model. These analyses were conducted using SAS version 9.4 (SAS, Inc., NC, USA). P < 0.05 was considered indicative of significance.
Results
During a median follow-up period of 2.7 years, 495 and 193 subjects died due to any cause or CVD, respectively. Clinical features of the 2690 participants are shown in Supplementary Tables 1–3, according to the levels of pre- or postdialysis SBP, DBP, and PP, respectively. Increases in pre- and postdialysis SBP and DBP (Supplementary Tables 1 and 2) were associated with male sex, increases in pre- and postdialysis DBP (Supplementary Table 2) were associated with younger age, and increases in pre- and postdialysis PP (Supplementary Table 3) were associated with older age. Moreover, increases in predialysis SBP and PP were associated with a higher ultrafiltration rate, while increases in postdialysis SBP and PP (Supplementary Tables 1 and 3) were associated with a lower ultrafiltration rate. Increases in pre- and postdialysis SBP, DBP, and PP (Supplementary Tables 1–3) were associated with higher use of CCBs and RASIs and lower use of vasopressor agents.
Associations between predialysis and postdialysis SBP and outcomes
HRs (95% CIs) for all-cause and cardiovascular mortality after adjustment for confounding factors were higher in patients with predialysis SBP < 100 mmHg than in those with a predialysis SBP of 120–139 mmHg, although the differences were not significant: 1.85 (0.95–3.60) for all-cause mortality and 2.42 (0.92–6.38) for cardiovascular mortality. On the other hand, more significant associations were observed between postdialysis SBP and outcomes. HRs (95% CIs) for all-cause and cardiovascular mortality after adjustment for confounding factors showed U-shaped associations: 2.06 (1.37–3.10), 1.23 (0.91–1.65), 1.00 (Ref), 1.25 (0.98–1.59), and 1.42 (1.10–1.84) for all-cause mortality in patients with postdialysis SBP < 100, 100–119, 120–139, 140–159, and ≥160 mmHg, respectively; 2.94 (1.50–5.77), 1.81 (1.11–2.96), 1.00 (Ref), 1.59 (1.05–2.40), and 1.72 (1.12–2.65) for cardiovascular mortality in patients with postdialysis SBP < 100, 100–119, 120–139, 140–159, and ≥160 mmHg, respectively (Fig. 1). Thus, lower SBP was associated with higher all-cause and cardiovascular mortality, regardless of the predialysis or postdialysis measurement. Higher postdialysis SBP was significantly associated with these outcomes, whereas higher predialysis SBP did not show such an association.

Hazard ratios and 95% confidence intervals for all-cause and cardiovascular mortality according to the levels of pre- and postdialysis SBP. Closed squares and vertical lines show hazard ratios and 95% confidence intervals, respectively, for all-cause (a) and cardiovascular (b) mortality according to the levels of predialysis (black squares and vertical lines) and postdialysis (blue squares and vertical lines) SBP. *P < 0.05 vs. SBP 120–139 mmHg, SBP systolic blood pressure
Associations between predialysis and postdialysis DBP and outcomes
There was no significant association of predialysis or postdialysis DBP with all-cause mortality, while a significantly higher HR (95% CI) for cardiovascular mortality [1.86 (1.13–3.04)] was observed in patients with a predialysis DBP of <60 mmHg than in those with predialysis DBP of 80–89 mmHg (Fig. 2).

Hazard ratios and 95% confidence intervals for all-cause and cardiovascular mortality according to the levels of pre- and postdialysis DBP. Closed squares and vertical lines show hazard ratios and 95% confidence intervals, respectively, for all-cause (a) and cardiovascular (b) mortality according to the levels of predialysis (black squares and vertical lines) and postdialysis (blue squares and vertical lines) DBP. *P < 0.05 vs. DBP 70–79 mmHg, DBP diastolic blood pressure
Associations between predialysis and postdialysis PP and outcomes
There was no significant association of predialysis PP with all-cause or cardiovascular mortality, whereas U-shaped associations were observed between postdialysis PP and these outcomes: HRs (95% CIs) after adjustment for confounding factors were 1.37 (1.00–1.88), 1.22 (0.90–1.64), 1.00 (Ref), 1.31 (0.98–1.77), and 1.48 (1.13–1.94) for all-cause mortality and 1.89 (1.10–3.23), 1.38 (0.82–2.34), 1.00 (Ref), 1.50 (0.91–2.48), and 1.94 (1.24–3.05) for cardiovascular mortality in patients with postdialysis PP of <50, 50–59, 60–69, 70–79, ≥80 mmHg, respectively, (Fig. 3).

Hazard ratios and 95% confidence intervals for all-cause and cardiovascular mortality according to the levels of pre- and postdialysis PP. Closed squares and vertical lines show hazard ratios and 95% confidence intervals, respectively, for all-cause (a) and cardiovascular (b) mortality according to the levels of predialysis (black squares and vertical lines) and postdialysis (blue squares and vertical lines) PP. *P < 0.05 vs. PP 60–69 mmHg, **P < 0.01 vs. PP 60–69 mmHg, PP pulse pressure
Stratified analyses according to the history of CVD
Stratified analyses were conducted according to the history of CVD for the associations of postdialysis SBP with all-cause and cardiovascular mortality. Lower postdialysis SBP (<100 mmHg) was associated with a significantly higher HR (95% CI) for all-cause [2.14 (1.38–3.33)] and cardiovascular [3.02 (1.48–6.15)] mortality in patients with CVD but not in those without CVD, whereas higher postdialysis SBP (≥160 mmHg) was associated with a significantly higher HR (95% CI) for all-cause [2.05 (1.17–3.62)] and cardiovascular [3.62 (1.38–9.45)] mortality in patients without CVD but not in those with CVD (P for interaction; 0.0342 in Fig. 4a, 0.0049 in Fig. 4b). We also carried out stratified analyses according to sex, age, and DM; however, there were no significant interaction effects on all-cause mortality between postdialysis SBP and sex (P = 0.40), age (P = 0.40), or DM (P = 0.40).

Hazard ratios and 95% confidence intervals for all-cause and cardiovascular mortality according to the levels of postdialysis SBP in hemodialysis patients with and without CVD. Closed squares and vertical lines show hazard ratios and 95% confidence intervals, respectively, for all-cause (a) and cardiovascular (b) mortalities according to the levels of postdialysis SBP in patients with (black squares and vertical lines) and without (blue squares and vertical lines) a history of CVD. *P < 0.05 vs. SBP 120–139 mmHg, **P < 0.01 vs. SBP 120–139 mmHg, CVD cardiovascular disease, SBP systolic blood pressure
Discussion
This study found U-shaped associations of postdialysis SBP and PP with all-cause and cardiovascular mortality, whereas no significant associations were seen between predialysis SBP or PP and these outcomes; however, nonsignificant increases in HRs were seen in patients with predialysis SBP < 100 mmHg compared with patients with a predialysis SBP of 120–139 mmHg.
Previous studies have shown conflicting findings on the relationship between postdialysis SBP and mortality. Zager et al. [3] reported an U-shaped association between postdialysis SBP and mortality; thus, a low postdialysis SBP < 120 mmHg and a high postdialysis SBP ≥ 180 mmHg were associated with an increased risk of cardiovascular mortality. Foley et al. [14] also found that postdialysis SBP, but not predialysis SBP, was associated with all-cause mortality. However, Agarwal [15] reported that 44-h ambulatory and home SBP were associated with all-cause mortality, whereas pre- and postdialysis BP showed no prognostic importance. Stidley et al. [16] demonstrated that the association between SBP and mortality changes over time. Thus, a predialysis SBP < 120 mmHg was associated with a higher risk of mortality during the first 2 years, but this association was not observed among patients with a HD vintage of ≥3 years. In addition, such associations were different according to age or the presence of comorbidities.
The involvement of a high volume status has been considered in the association between high postdialysis SBP and cardiovascular mortality. Recently, Nongunuch et al. [17] prospectively audited 531 patients who underwent multiple frequency bioelectrical impedance to determine whether volume status plays a role in dialysis-associated hypertension. The authors found that patients with increased postdialysis BP had greater hydration status because of increased extracellular water and concluded that such patients should have lower postdialysis target weights. In our recent report [18], high volume status, determined using the cardiothoracic ratio on a chest X-ray before an HD session, was associated with all-cause mortality and increased incidence of major adverse cardiovascular events. This finding supports the results of the present study.
In contrast, the association of low postdialysis SBP with mortality is thought to reflect antecedent cardiac disease, low cardiac function, and/or poor overall health status, as described in a report by Zager et al. [3]. This supposition was proven by the finding in this study that low postdialysis SBP was a significant risk factor for all-cause and cardiovascular mortality in patients with CVD but not in those without CVD, presumably because the former group had lower cardiac function than the latter group. Myers et al. [8] also reported that low SBP was associated with increased mortality, and the association was more pronounced in older patients and those with diabetes, although it was not significant in younger patients without diabetes. These findings were presumably due to the higher prevalence of impaired cardiac function in the former than in the latter and were similar to those observed in our previous report [18], in which the correlation between a high cardiothoracic ratio and cardiovascular events was more pronounced in patients with lower BP than in those with higher BP because the combination of a high cardiothoracic ratio and low BP is regarded as a reflection of low cardiac function.
Patients with either low postdialysis PP (<50 mmHg) or high postdialysis PP (≥80 mmHg) had a significantly high risk for all-cause and cardiovascular mortality in this study. Previous reports also demonstrated that high PP was associated with mortality [6, 19]. However, low PP did not show an association with increased mortality. The association between high PP and mortality may be attributed to the close relationship between PP and arterial stiffness; it was reported that the most typical clinical consequence of arterial stiffening is steepening of the slope of the pressure–volume curve, with increased systolic pressure during ventricular ejection and decreased diastolic pressure during diastolic runoff, resulting in high PP [20, 21]. Moreover, the mechanism underlying the association of low postdialysis PP with mortality is unclear; however, it may be attributed to a close relationship between postdialysis SBP and PP. Among 126 patients with a postdialysis SBP of <100 mmHg, 115 had a postdialysis PP of <50 mmHg, and multivariable logistic analysis showed that postdialysis SBP was significantly associated with low postdialysis PP in the present study.
To improve prognosis in chronic HD patients, the Japanese guideline for management of CVD [22] recommends a predialysis BP of <140/90 mmHg at the beginning of the week, although this is considered an “expert opinion” because of a lack of robust evidence. However, our recent study demonstrated that the risk thresholds of predialysis SBP for all-cause mortality and cardiovascular events were 152 and 143 mmHg, respectively, and that of predialysis DBP for all-cause mortality was 68 mmHg. In that report, we could not evaluate the usefulness of postdialysis BP because of the lack of data in the Q-Cohort Study. However, the present study suggests that postdialysis SBP is a better predictor of all-cause and cardiovascular mortality than predialysis SBP and that the target for optimal SBP control is between 120 and 140 mmHg. In fact, the National Kidney Foundation Kidney Disease Outcomes Quality Initiative [23] has recommended a postdialysis BP goal of <130/80 mmHg. The present findings support this recommendation.
Recently, practical guideline for the management of hypertension has been developed and launched in Japan [24]; however, no recommendations or suggestions have been addressed for HD patients because of the lack of high-quality evidence due to the heterogeneity of factors affecting BP among those patients. The guideline states that it is difficult to determine numerical targets for BP in HD patients at present, and it is realistic to define the safety margin for BP for each patient by taking care to not decrease vascular access blood flow or reduce BP during HD sessions while avoiding the development of hemorrhagic complications [24]. Thus, it is hoped that more robust evidence will be established by large-scale randomized controlled trials on target BP in those patients.
There are some limitations in this study. First, the observational nature limited the ability to ascribe a cause-and-effect relationship between BP and prognosis. Second, most data including BP were collected only at baseline, as was the case in most prior epidemiologic studies. This may cause a misclassification of BP level, which could have weakened the association found in this study, biasing the results toward the null hypothesis. We therefore believe these biases would not alter the conclusion. Further research is required to clarify the relationship between time-dependent changes in BP and worse outcomes. Third, the target population was limited to Japanese HD patients. Fourth, neither ambulatory BP monitoring, weekly average BP, nor home BP were measured, although measurements of these parameters have been recommended for evaluating BP. Fifth, fluctuation of BP by altering temperature was not considered due to a lack of information on temperature at the time of BP measurement. Sixth, neither intradialytic hypotension, orthostatic hypotension, nor visit-to-visit BP variability was evaluated in this study, although the associations of these parameters with poor outcomes, such as mortality, CVD, and cognitive impairment, have been reported in HD patients [25,26,27]. Finally, although we adjusted for factors considered likely to affect the association between BP and mortality, the effects of other established prognostic factors such as C-reactive protein and erythropoiesis-stimulating agent resistance index and unmeasured confounders may have influenced the results. However, in identifying some important factors associated with BP, our study can serve as a first step for more in-depth research in this area.
In conclusion, postdialysis SBP and PP are better predictors of all-cause and cardiovascular mortality than predialysis values and show U-shaped associations with these outcomes in Japanese HD patients. The present findings suggest that the target for postdialysis SBP control should be between 120 and 140 mmHg for optimal survival in HD patients.
References
Vasan RS, Larson MG, Leip EP, Evans JC, O'Donnell CJ, Kannel WB, et al. Impact of high-normal blood pressure on the risk of cardiovascular disease. N Engl J Med. 2001;345:1291–7.
Port FK, Hulbert-Shearon TE, Wolfe RA, Bloembergen WE, Golper TA, Agodoa LY, et al. Predialysis blood pressure and mortality risk in a national sample of maintenance hemodialysis patients. Am J Kidney Dis. 1999;33:507–17.
Zager PG, Nikolic J, Brown RH, Campbell MA, Hunt WC, Peterson D, et al. "U" curve association of blood pressure and mortality in hemodialysis patients. Medical Directors of Dialysis Clinic, Inc. Kidney Int. 1998;54:561–9.
Kalantar-Zadeh K, Kilpatrick RD, McAllister CJ, Greenland S, Kopple JD. Reverse epidemiology of hypertension and cardiovascular death in the hemodialysis population: the 58th annual fall conference and scientific sessions. Hypertension. 2005;45:811–7.
Hara M, Tanaka S, Taniguchi M, Fujisaki K, Torisu K, Masutani K, et al. Prognostic value of pre-dialysis blood pressure and risk threshold on clinical outcomes in hemodialysis patients: the Q-Cohort Study. Medicine. 2018;97:e13485.
Klassen PS, Lowrie EG, Reddan DN, DeLong ER, Coladonato JA, Szczech LA, et al. Association between pulse pressure and mortality in patients undergoing maintenance hemodialysis. JAMA. 2002;287:1548–55.
Moriya H, Oka M, Maesato K, Mano T, Ikee R, Ohtake T, et al. Weekly averaged blood pressure is more important than a single-point blood pressure measurement in the risk stratification of dialysis patients. Clin J Am Soc Nephrol. 2008;3:416–22.
Myers OB, Adams C, Rohrscheib MR, Servilla KS, Miskulin D, Bedrick EJ, et al. Age, race, diabetes, blood pressure, and mortality among hemodialysis patients. J Am Soc Nephrol. 2010;21:1970–8.
Alborzi P, Patel N, Agarwal R. Home blood pressures are of greater prognostic value than hemodialysis unit recordings. Clin J Am Soc Nephrol. 2007;2:1228–34.
Agarwal R, Peixoto AJ, Santos SF, Zoccali C. Pre- and postdialysis blood pressures are imprecise estimates of interdialytic ambulatory blood pressure. Clin J Am Soc Nephrol. 2006;1:389–98.
Agarwal R, Brim NJ, Mahenthiran J, Andersen MJ, Saha C. Out-of-hemodialysis-unit blood pressure is a superior determinant of left ventricular hypertrophy. Hypertension. 2006;47:62–8.
Mapes DL, Lopes AA, Satayathum S, McCullough KP, Goodkin DA, Locatelli F, et al. Health-related quality of life as a predictor of mortality and hospitalization: the Dialysis Outcomes and Practice Patterns Study (DOPPS). Kidney Int. 2003;64:339–49.
Pisoni RL, Gillespie BW, Dickinson DM, Chen K, Kutner MH, Wolfe RA. The Dialysis Outcomes and Practice Patterns Study (DOPPS): design, data elements, and methodology. Am J Kidney Dis. 2004;44:7–15.
Foley RN, Herzog CA, Collins AJ. United States Renal Data System. Blood pressure and long-term mortality in United States hemodialysis patients: USRDS Waves 3 and 4 Study. Kidney Int. 2002;62:1784–90.
Agarwal R. Blood pressure and mortality among hemodialysis patients. Hypertension. 2010;55:762–8.
Stidley CA, Hunt WC, Tentori F, Schmidt D, Rohrscheib M, Paine S, et al. Medical Directors of Dialysis Clinic I. Changing relationship of blood pressure with mortality over time among hemodialysis patients. J Am Soc Nephrol. 2006;17:513–20.
Nongnuch A, Campbell N, Stern E, El-Kateb S, Fuentes L, Davenport A. Increased postdialysis systolic blood pressure is associated with extracellular overhydration in hemodialysis outpatients. Kidney Int. 2015;87:452–7.
Yotsueda R, Taniguchi M, Tanaka S, Eriguchi M, Fujisaki K, Torisu K, et al. Cardiothoracic ratio and all-cause mortality and cardiovascular disease events in hemodialysis patients: the Q-Cohort Study. Am J Kidney Dis. 2017;70:84–92.
Tozawa M, Iseki K, Iseki C, Takishita S. Pulse pressure and risk of total mortality and cardiovascular events in patients on chronic hemodialysis. Kidney Int. 2002;61:717–26.
Briet M, Boutouyrie P, Laurent S, London GM. Arterial stiffness and pulse pressure in CKD and ESRD. Kidney Int. 2012;82:388–400.
Georgianos PI, Pikilidou MI, Liakopoulos V, Balaskas EV, Zebekakis PE. Arterial stiffness in end-stage renal disease-pathogenesis, clinical epidemiology, and therapeutic potentials. Hypertens Res. 2018;41:309–19.
Hirakata H, Nitta K, Inaba M, Shoji T, Fujii H, Kobayashi S, et al. Japanese Society for Dialysis Therapy guidelines for management of cardiovascular diseases in patients on chronic hemodialysis. Ther Apher Dial. 2012;16:387–435.
Workgroup KD. K/DOQI clinical practice guidelines for cardiovascular disease in dialysis patients. Am J Kidney Dis. 2005;45:S1–153.
Hoshide S, Kario K, Tomitani N, Kabutoya T, Chia YC, Park S, et al. Highlights of the 2019 Japanese Society of Hypertension Guidelines and perspectives on the management of Asian hypertensive patients. J Clin Hypertens. 2019. https://doi.org/10.1111/jch.13763.
Shoji T, Tsubakihara Y, Fujii M, Imai E. Hemodialysis-associated hypotension as an independent risk factor for two-year mortality in hemodialysis patients. Kidney Int. 2004;66:1212–20.
Liu W, Wang L, Huang X, Yuan C, Li H, Yang J. Orthostatic blood pressure reduction as a possible explanation for memory deficits in dialysis patients. Hypertens Res. 2019;42:1049–56.
Amari Y, Morimoto S, Iida T, Yurugi T, Oyama Y, Aoyama N, et al. Characteristics of visit-to-visit blood pressure variability in hemodialysis patients. Hypertens Res. 2019;42:1036–48.
Acknowledgements
We would like to thank the Arbor Research Collaborative for Health, Ann Arbor, MI, USA, for administering the J-DOPPS and express our appreciation for the support of Kyowa Hakko Kirin, without restrictions on publication. The DOPPS.org website lists the full details. We also thank the study nurses, physicians, and medical directors for all the time and attention that they devoted to our study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
KT has received speaker’s fees, consultant fees, and a research grant from Kyowa Kirin. EK has been a member of a biostatistics support group for the J-DOPPS program, which is supported by Kyowa Kirin. TN is a current employee of Kyowa Kirin. KI has received speaker’s fee from Kyowa Kirin. HH has received speaker’s fees from Kyowa Kirin.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Tsuruya, K., Kanda, E., Nomura, T. et al. Postdialysis blood pressure is a better predictor of mortality than predialysis blood pressure in Japanese hemodialysis patients: the Japan Dialysis Outcomes and Practice Patterns Study. Hypertens Res 43, 791–797 (2020). https://doi.org/10.1038/s41440-020-0425-1
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41440-020-0425-1
Keywords
This article is cited by
-
Optimal timing for post-dialysis blood pressure measurement: relationship with home blood pressure monitoring
Hypertension Research (2025)
-
Post-dialysis blood pressure: inaccuracy or lack of standardization?
Hypertension Research (2025)
-
Prediction Model of Intradialytic Hypertension in Hemodialysis Patients Based on Machine Learning
Journal of Medical Systems (2025)
-
Seasonal variation and predictors of intradialytic blood pressure decline: a retrospective cohort study
Hypertension Research (2021)
-
Intradialytic systolic blood pressure variation can predict long-term mortality in patients on maintenance hemodialysis
International Urology and Nephrology (2021)
