
Abstract
The relationship between frailty and blood pressure (BP) is inconsistent, and limited research has compared BP by frailty status using long-term home BP measurements. We aimed to identify office and home BP and determine differences according to frailty status, stratified by taking antihypertensives in community-dwelling older adults. This cross-sectional study was part of the ongoing non-randomized intervention NOSE study. Participants were aged ≥ 64 years. Frailty was categorized robust, pre-frailty, or frailty using the revised Japanese version of the Cardiovascular Health Study criteria. Office BP was measured in survey settings, and each participant was instructed to take home BP. We used the average home BP for 4 weeks post-survey. An analysis of covariance analyzed the relationship between frailty and office and home BP, and their differences stratified by antihypertensive use. We included 418 older participants (mean age: 72.8 years); 39.5% were male, 40.4% were taking antihypertensives, and 6.7% had frailty. Individuals with frailty taking antihypertensives had higher home morning systolic BP (SBP) than those with robust (134.2 vs. 145.7 mmHg, P = 0.018) and pre-frailty (135.6 vs. 145.7 mmHg, P = 0.024). The difference between office and morning home SBP in treated participants was 7.1 mmHg (robust), 4.7 mmHg (pre-frailty), and −5.1 mmHg (frailty), showing significant differences (robust vs. frailty: P = 0.005, pre-frailty vs. frailty: P = 0.016). Home morning SBP was higher in individuals with frailty taking antihypertensives compared to those without frailty, and it may be higher than office BP. Individuals with frailty should measure home BP for good BP control.

Similar content being viewed by others

Introduction
Hypertension is a key risk factor for cardiovascular diseases (CVD) worldwide. Home blood pressure (BP) measurements are crucial for good BP management. Home BP values are more reproducible than office BP values [1]. In addition, healthcare professionals can detect the white-coat effect, morning hypertension, or masked hypertension by reviewing home BP values [2]. Compared to well-controlled hypertension, masked hypertension leads to the progression of atherosclerosis and CVD events [3, 4]. Additionally, home BP measurements are available for untreated individuals and may enable to the early detection of hypertension [5]. Therefore, measuring home BP is considered a useful strategy for maintaining good health status for the entire population [6, 7].
Frailty is commonly seen in older adults, indicating increased vulnerability to stressors and a greater risk of poor health outcomes including disability, hospitalization, and mortality [8, 9]. The relationship between frailty and BP status has shown inconsistent results in previous studies. One study of community-dwelling Japanese older adults (mean age, 68.6 years) reported that individuals with impaired physical function (but not frailty) had higher home BP than those with normal physical function [10]. However, Bastos-Barbosa found no association between frailty and home BP among community-dwelling older adults (mean age: 74.5 years) [11]. In a study of outpatients with cardiometabolic diseases (mean age: 79.2 years), the relationship between frailty and lower office BP was stronger than with higher BP [12]. Similar findings were observed in a cross-sectional study among community-dwelling adults aged 80 years who were taking antihypertensives [13]. Only a few previous studies have evaluated BP using home BP [10, 11] or ABPM [11], whereas the majority relied on office BP measurements [12,13,14,15,16] to investigate the relationship between frailty and BP status.
Maintaining adequate control of morning BP through home BP measurements is very important for CVD prevention [17] because CVD events are more likely to occur in the morning [18]. Morning hypertension, the most common type of masked hypertension, is associated with a higher risk of stroke and need for care in individuals older than 75 years than hypertension defined by office BP value [19, 20]. In Japan, home BP measurements are recommended to be taken upon waking and before bed [6], while office BP values are measured during the day. According to the 2019 Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH), home BP values are considered more important than office BP values because they are closely associated with CVD events [6]. Moreover, frailty is a risk factors of CVD [21]. Therefore, the relationship between frailty and BP should be investigated using home BP values taken in the morning. However, few studies have investigated this relationship. In addition, identifying the differences between office and home morning BP can ensure more accurate BP control. Previous studies reported greater BP variability in frailty older adults [22], suggesting that office BP may not accurately reflect an individual’s normal BP. As this discrepancy could lead to overtreatment or insufficient BP management, it is necessary to clarify such differences in individuals with frailty. Mori analyzed data stratified by whether participants were receiving antihypertensive treatment [23]. Assessing the association of BP, antihypertensive therapy, and frailty may help us understand these complex interactions and provide insight for BP treatment evidence in the older adults [14]. Furthermore, previous studies investigating the difference between office and home BP measured home BP over 3 days [23] and 2 weeks [24]. Therefore, long-term measurements of home BP, such as over 4 weeks, may provide more accurate BP levels.
The aim of our study was to identify office and home BP and determine differences according to frailty status, stratified by antihypertensive use, among community-dwelling older adults. This study may advance our understanding of the good BP control in older adults and provide clinical and policy implications regarding the need for BP management.
Methods
Study participants
The study participants were recruited from the NOSE study, an ongoing non-randomized intervention study focusing on self-measuring home BP. The main objective of the NOSE study was to determine whether long-term home BP measurements could prevent cognitive decline, frailty, nursing care requirements, and CVD as well as extend the healthy life expectancy. The participants in the NOSE study were recruited between August 2020 and August 2021. We conducted surveys in Nose Town, a regional town with approximately 10,000 inhabitants in Osaka Prefecture. Since the stroke mortality rate is higher in Nose Town than in Osaka Prefecture, a strategy against hypertension is desired. Therefore, the NOSE study was initiated in collaboration with our group and supported by a TOP-Z research grant from OMRON HEALTHCARE Co., Ltd. Participants in the NOSE study were recruited through the town’s newsletter, health checkup settings, community activity sites, and coronavirus disease 2019 vaccination centers. We examined 1,151 community-dwelling adults aged ≥40 years old, representing 15.9% of the Nose Town residents aged at least 40 years. The participants were grouped based on their residential districts into an early intervention group, which started measuring home BP values in 2020, and a late intervention group, which started in 2022. The details of the NOSE study have been published previously [25]. The Ethics Committee of Osaka University Graduate School of Medicine proved the study (approval numbers: 19433-4). Written informed consent was obtained from all participants.
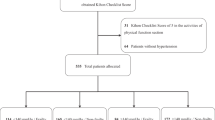
Out of 1151 participants, we excluded 476 allocated to the late intervention group, 213 aged <64 years, 20 with missing data on frailty, and 24 who measured their home BP for less than 4 weeks, resulting in a total of 418 older participants being included. The participant selection method is depicted in Fig. 1. This was a cross-sectional study.

Schematic flow diagram of the selection of study participants
Definition of frailty
Frailty was determined using the revised Japanese version of the Cardiovascular Health Study (J-CHS) criteria [26], which include weakness, slow walking speed, weight loss, low activity, and exhaustion. Frailty, pre-frailty, and robust were defined by having 3–5, 1–2, and 0 items, respectively. Weakness was defined by grip strength, which was established according to a sex-specific cutoff (<28 kg for men and <18 kg for women). The grip strength of the dominant hand was measured twice using a Smedley hand dynamometer (Model YD-100; Yagami, Ltd., Tokyo, Japan). Measurements were performed in a standing position with the arms resting on the side of the body. Mean values were calculated and used in the analyses. Walking speed was measured over a 5-m walking course at normal speed. Slow walking speed was established using a cutoff <1.0 m/s. Weight loss was assessed using a response of “yes” to the question, “Have you lost 2 kg or more in the past 6 months?” Physical activity was evaluated by asking “Do you engage in moderate levels of physical exercise or sports aimed at health?” and “Do you engage in low levels of physical exercise aimed at health?” If participants answered “no” to both questions, they were classified as having low physical activity. Exhaustion was assessed using a response of “yes” to the following question: “In the past 2 weeks, have you felt tired without a reason?”
BP measurements
Office BP was measured by medical professionals during the survey and was taken twice consecutively in a sitting position on the right and left upper arms using a portable automated device (HEM-7281T, Omron, Kyoto, Japan). Office BP was defined as the average of four measurements from both arms. Each participant was instructed to take home BP measurements using the same device (HEM-7281T) with the arm that is easier to measure twice a day and record their BP values in their notebooks. Home morning BP was measured twice consecutively in a sitting position within 1 hour of awakening, before taking antihypertensives and breakfast, and after urination, if relevant. Home evening BP was measured before bed. The measurement procedure was in accordance with the recommendations of JSH 2019 [6]. Home BP was determined using the mean of the first and second measurements and the mean home BP levels from all measurements for each participant over a 4-week period after participating in the survey. The difference between office and home BP was calculated as the average of office BP minus the home morning BP for each participant.
Physical measurements and self-administered questionnaire
Participants were interviewed and physically assessed by physicians, nurses, and physical therapists. Questionnaires were administered to assess the following items: living arrangements, medical history, medication use, smoking habits, and alcohol consumption. Smoking habits were categorized as current smokers or nonsmokers. Those with alcohol consumption habits were classified as regular drinkers. Height, weight, and office BP were measured in the survey settings. Body mass index (BMI) was calculated as weight (kg) divided by height (m) squared. Laboratory data were collected from the medical checkup records (ALT and estimated glomerular filtration rate [eGFR]). Medical history of diabetes, dyslipidemia, stroke, heart disease, and joint disease was assessed using a questionnaire. CVD was defined as individuals who had a stroke or heart disease.
Statistical analyses
Descriptive statistics are presented as the mean ± standard deviation or frequency. Group differences were assessed by Student’s t-test or analysis of variance for continuous variables, while Kruskal-Wallis test was used with non-normal distributions. Frequency differences were assessed by chi-squared test.
An analysis of covariance (ANCOVA) was further performed to clarify whether the differences in morning and evening home BP according to frailty status were independent of possible covariates and to calculate covariate-adjusted means and standard errors. The adjusted factors in the ANCOVA were age, sex, regular drinking, body mass index, history of CVD, and measurement season. Post hoc analysis was performed using Bonferroni’s test. Seasons were defined by the Japan Meteorological Agency as follows: spring from March to May; summer from June to August; autumn from September to November; and winter from December to February. Additionally, we calculated covariate-adjusted mean office and home morning BP differences. Group differences were assessed using ANCOVA after adjusting for age, sex, regular drinking, body mass index, office BP, and measurement season. Post hoc analysis was performed using Bonferroni’s test. Two-tailed P-values < 0.05 were considered significant. Statistical analyses were performed using IBM SPSS Statistics version 26 for Windows (IBM Japan, Tokyo, Japan).
Results
Characteristics of the participants
Among the 418 older participants, the mean age was 72.8 years old; 39.5% were male, 40.4% were taking antihypertensives. One hundred and twenty-three (29.4%) were classified as robust, 267 (63.9%) as pre-frailty, and 28 (6.7%) as frailty. Table 1 shows the clinical characteristics of the study population according to frailty status. Significant differences in age, regular drinking, and joint disease were found. Supplementary Table 1 represents the class differences in prescribed antihypertensive drugs. Individuals with frailty were more likely to take angiotensin II receptor blockers (ARB) plus calcium channel blockers (CCB) combination therapy and have lower eGFR levels.
Office and home BP according to frailty status
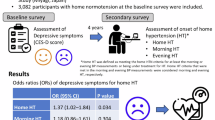
Table 2 presents office and home BP measured in the morning and evening according to frailty status, stratified by whether they were treated. A significant difference in the morning home SBP was observed according to frailty status among treated individuals (robust vs. pre-frailty vs. frailty: 134.3 vs. 135.7 vs. 144.8 mmHg, P = 0.018). A significant difference in the evening home SBP was also observed among treated individuals (robust vs. pre-frailty vs. frailty: 125.8 vs. 127.2 vs. 135.3 mmHg, P = 0.029). No significant differences were found in untreated participants. Figure 2 illustrates the covariate-adjusted mean home morning and evening SBP according to frailty status in participants receiving antihypertensive treatment. Although the home morning SBP was higher in the frailty group (robust vs. frailty: 134.2 vs. 145.7 mmHg, P = 0.018; pre-frailty vs. frailty:135.6 vs. 145.7 mmHg, P = 0.024), home evening SBP did not show significant differences (robust vs. frailty:126.6 vs. 135.4 mmHg, P = 0.153; pre-frailty vs. frailty: 128.1 vs. 135.4 mmHg, P = 0.095). No significant differences were found in DBP according to frailty status.

Covariate-adjusted mean home morning and evening SBP according to frailty status in participants receiving antihypertensive treatment. Values are presented as the adjusted mean ± standard error. Group differences were assessed by an analysis of covariance adjusted for age, sex, regular drinking, body mass index, history of cardiovascular disease, and measurement season. Post-hoc analysis was performed using Bonferroni’s test. SBP Systolic blood pressure
Differences between office and home BP according to frailty status
Figures 3 and 4 show covariate-adjusted mean office minus home morning BP differences according to frailty and antihypertensive treatment status. The SBP difference among treated participants was 7.1 mmHg in the robust group, 4.7 mmHg in the pre-frailty group, and −5.1 mmHg in the frailty group, showing significant differences (robust vs. frailty: P = 0.005, pre-frailty vs. frailty: P = 0.016). No significant differences were found in untreated participants (robust vs. frailty: 3.9 vs. 5.7 mmHg, P = 1.000; pre-frailty vs. frailty: 2.1 vs. 5.7 mmHg, P = 1.000). For DBP in treated participants, the differences were 2.7 mmHg (robust), 0.5 mmHg (pre-frailty), and −5.5 mmHg (frailty), with significant differences among frailty status (robust vs. frailty: P = 0.003, pre-frailty vs. frailty: P = 0.021).

Covariate-adjusted mean office–home morning SBP differences according to frailty and antihypertensive treatment status. Values are presented as the adjusted mean ± standard error. Differences in SBP were calculated by subtracting the home morning SBP from the office SBP. Group differences were assessed by an analysis of covariance adjusted for age, sex, regular drinking, body mass index, office SBP, and measurement season. Post-hoc analysis was performed using Bonferroni’s test. SBP Systolic blood pressure

Covariate-adjusted mean office–home morning DBP differences according to frailty and antihypertensive treatment status. Values are presented as the adjusted mean ± standard error. Differences in DBP were calculated by subtracting the home morning DBP from the office DBP. Group differences were assessed by an analysis of covariance adjusted for age, sex, regular drinking, body mass index, office DBP, and measurement season. Post-hoc analysis was performed using Bonferroni’s test. DBP Diastolic blood pressure
Comparison of office and home BP according to frailty
Supplementary Table 2 shows the comparison of office and home BP according to frailty subitems: slow walking speed, weak grip strength, weight loss, exhaustion, and low activity. Home morning SBP was significantly higher in the slow walking speed group (slow vs. normal: 141.0 vs. 132.9 mmHg, P = 0.034). Office DBP was significantly lower in weak grip strength group (weak vs. normal: 77.5 vs. 81.6 mmHg, P = 0.004).
Discussion
The home morning SBP was higher in the frailty group than in the robust and pre-frailty groups in individuals receiving antihypertensive treatment. The difference between office and home morning BP tended to vary according to frailty status. In treated participants, office BP was higher than home morning BP in the robust and pre-frailty groups, whereas office BP was lower than home morning BP in the frailty group. In untreated participants, office BP was higher than home BP in all groups. In the sub-analysis, the home morning SBP was higher in the slow walking speed group. Office DBP was lower in the weak grip strength group. This is the first study to identify office and home BP and determine differences according to frailty status among community-dwelling older adults.
In this study, the prevalence of frailty was 6.7%, which is consistent with a previous study on the Japanese general population, suggesting that the study participants are representative of the older Japanese community [27].
Individuals with frailty who took antihypertensives had higher home morning SBP. This finding contrasts with those of previous studies that identified a relationship between frailty and a lower office SBP [12,13,14]. This may be attributed to differences in the timing of BP measurements. In our study, morning home BP was recorded within 1 hour of awakening. Given that treated individuals with frailty may exhibit an elevated morning SBP, monitoring home BP is particularly important for older adults with frailty to ensure good BP control and CVD prevention.
Regarding the mechanisms underlying an elevated home morning SBP among individuals with frailty, frailty may experience morning or nocturnal hypertension. Frailty had higher BP during sleep compared to non-frailty individuals [11, 28]. Heart failure and poor renal function, which are risk factors for frailty [29, 30], can induce nocturnal hypertension [6]. In our study, individuals with frailty receiving antihypertensive therapy exhibited lower renal function (Supplementary Table 1), which could have influenced their home morning BP values.
The relationship between frailty and differences (office BP minus home morning BP) differed according to frailty status and whether participants were taking antihypertensives, even after controlling for covariates. Office BP was higher than home morning BP among treated participants without frailty, whereas those with frailty had a higher morning BP than office BP. This cannot be ascertained by measuring office BP alone, as it may lead to inadequate hypertension treatment and CVD onset or progression. Thus, we highlight the importance of home BP monitoring in older adults, particularly those with frailty who are undergoing antihypertensive therapy.
The higher office vs. home BP can be explained by the white-coat effect [31]. This phenomenon may not have been observed among participants with frailty, possibly because of antihypertensive-use and dosages. Individuals with frailty were more likely to take them after breakfast (94.1% in frailty vs. 80% in robust group) and more often took ARBs and CCBs in combination (Supplementary Table 1). Therefore, in the frailty group, it is likely that morning home BP was higher because it was measured before medication intake, whereas the medication had taken effect by the time office BP was measured. In addition, the effects of antihypertensive medications may be stronger among participants with frailty. Physiological changes that lead to pharmacokinetic changes such as decreased drug clearance in the liver and kidneys are more likely to occur in the setting of frailty [32]. If the morning home BP was higher than office BP in the frailty group owing to the effects of antihypertensive medication, it is reasonable that office BP was higher than home BP in the untreated frailty group.
In the sub-analysis, home morning SBP was significantly higher in the slow walking speed group, whereas office DBP was significantly lower in the weak grip strength group. A study of community-dwelling older adult participants in the Framingham Heart Study reported that higher levels of frailty were associated with higher levels of arterial stiffness [33]. Arterial stiffness, which occurs when arterial elasticity is diminished, leads to increased blood vessel rigidity, resulting in widened pulse pressure [34, 35]. Consequently, it can lead to higher SBP and lower DBP levels. This result indicates that arterial stiffness may be reflected in BP among older individuals with a slow walking speed or weak grip strength.
This study has some limitations. First, home BP readings were handwritten in notebooks and may contain inaccuracies, leading to measurement bias. Second, healthy, cognitively well older individuals may continue to measure home BP for some time, introducing selection bias. Third, the number of participants with frailty was small. Fourth, we were unable to consider the number and class of antihypertensive medications. Finally, the causal relationship is unclear because of the cross-sectional design. A longitudinal study is needed to identify the causal relationship.
Perspective of Asia
BP management in Asia has some challenges [36]. The association between BP and the risk of CVD is stronger in Asians than in Western populations [37], especially elevated BP is higher risk for the stroke that is the major cause for long-term care in Asians than in in Western populations [6], and morning BP surge is more commonly observed in Asians [38]. These factors emphasize the critical need for Asians to monitor home BP, especially morning BP, as part of efforts to prevent CVD. Our findings highlight the clinical relevance of home morning BP, particularly in older adults with frailty receiving antihypertensive treatment. Promoting home BP monitoring in Asia is essential for addressing these unique challenges, improving BP control for effective CVD prevention, and extending healthy life expectancy.
Conclusion
Home morning SBP was higher in individuals with frailty who were undergoing antihypertensive treatment compared to those without frailty. The difference between office and home morning BP varied according to frailty status, suggesting that home morning BP may be higher than office BP in treated individuals with frailty. It is crucial for healthcare professionals to promote home BP measurement, especially among older adults with frailty receiving antihypertensive therapy. This approach allows for personalized and responsive care tailored to each patient’s unique needs—such as the adjustment of antihypertensive medications and guidance on lifestyle factors, including diet and exercise—and contributes to good BP control and CVD prevention.
References
Imai Y, Obara T, Asamaya K, Ohkubo T. The reason why home blood pressure measurements are preferred over clinic or ambulatory blood pressure in Japan. Hypertens Res. 2013;36:661–72.
Oikawa T, Obara T, Ohkubo T, Kikuya M, Asayama K, Metoki H, et al. Characteristics of resistant hypertension determined by self-measured blood pressure at home and office blood pressure measurements: the J-HOME study. J Hypertens. 2006;24:1737–43.
Matsui Y, Eguchi K, Ishikawa J, Hoshide S, Shimada K, Kario K. Subclinical arterial damage in untreated masked hypertensive subjects detected by home blood pressure measurement. Am J Hypertens. 2007;20:385–91.
Bobrie G, Chatellier G, Genes N, Clerson P, Vaur L, Vaisse B, et al. Cardiovascular prognosis of “masked hypertension” detected by blood pressure self-measurement in elderly treated hypertensive patients. JAMA. 2004;291:1342–9.
Stergiou GS, Bliziotis IA. Home blood pressure monitoring in the diagnosis and treatment of hypertension: a systematic review. Am J Hypertens. 2011;24:123–34.
Umemura S, Arima H, Arima S, Asayama K, Dohi Y, Hirooka Y, et al. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2019). Hypertens Res. 2019;42:1235–481.
Wang T-D, Ohkubo T, Bunyi ML, Chadachan VM, Chia YC, Kario K, et al. Current realities of home blood pressure monitoring from physicians’ perspectives: results from Asia HBPM survey 2020. Hypertens Res. 2023;46:1638–49.
Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. 2013;381:752–62.
Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56:M146–56.
Murakami K, Asayama K, Satoh M, Hosaka M, Matsuda A, Inoue R, et al. Home blood pressure predicts stroke incidence among older adults with impaired physical function: the Ohasama study. J Hypertens. 2017;35:2395–401.
Bastos-Barbosa RG, Ferriolli E, Coelho EB, Moriguti JC, Nobre F, Lima NK. Association of frailty syndrome in the elderly with higher blood pressure and other cardiovascular risk factors. Am J Hypertens. 2012;25:1156–61.
Ishikawa J, Toba A, Tamura Y, Araki A, Harada K. Changes in blood pressure associated with frailty and sarcopenia in elderly outpatients with cardiometabolic diseases. Geriatr Gerontol Int. 2023;23:506–16.
Kabayama M, Kamide K, Gondo Y, Masui Y, Nakagawa T, Ogawa M, et al. The association of blood pressure with physical frailty and cognitive function in community-dwelling septuagenarians, octogenarians, and nonagenarians: the SONIC study. Hypertens Res. 2020;43:1421–29.
Rouch L, Rolland Y, Hanon O, Vidal J-S, Cestac P, Sallerin B, et al. Blood pressure, antihypertensive drugs, and incident frailty: The Multidomain Alzheimer Preventive Trial (MAPT). Maturitas. 2022;162:8–14.
Coelho-Junior HJ, Uchida MC, Picca A, Calvani R, Landi F, de Oliveira Gonçalves I, et al. Frailty is not associated with hypertension, blood pressure or antihypertensive medication in community-dwelling older adults: A cross-sectional comparison across 3 frailty instruments. Exp Gerontol. 2021;146:111245.
Anker D, Carmeli C, Zwahlen M, Rodondi N, Santschi V, Henchoz Y, et al. How blood pressure predicts frailty transitions in older adults in a population-based cohort study: a multi-state transition model. Int J Epidemiol. 2022;51:1167–77.
Shimada K, Kario K, Kushiro T, Teramukai S, Zenimura N, Ishikawa Y, et al. Prognostic significance of on-treatment home and clinic blood pressure for predicting cardiovascular events in hypertensive patients in the HONEST study. J Hypertens. 2016;34:1520–7.
Elliott WJ. Circadian variation in the timing of stroke onset: a meta-analysis. Stroke. 1998;29:992–6.
Kario K, Ishikawa J, Pickering TG, Hoshide S, Eguchi K, Morinari M, et al. Morning hypertension: the strongest independent risk factor for stroke in elderly hypertensive patients. Hypertens Res. 2006;29:581–7.
Nishinaga M, Takata J, Okumiya K, Matsubayashi K, Ozawa T. High morning home blood pressure is associated with a loss of functional independence in the community-dwelling elderly aged 75 years or older. Hypertens Res. 2005;28:657–63.
Afilalo J, Karunananthan S, Eisenberg MJ, Alexander KP, Bergman H. Role of frailty in patients with cardiovascular disease. Am J Cardiol. 2009;103:1616–21.
Rouch L, De Souto Barreto P, Hanon O, Vidal J-S, Amar J, Andrieu S, et al. Visit-to-visit blood pressure variability and incident frailty in older adults. J Gerontol A. 2021;76:1369–75.
Mori H, Ukai H, Yamamoto H, Yuasa S, Suzuki Y, Chin K, et al. Blood pressure differences between office and home settings among Japanese normotensive subjects and hypertensive patients. Hypertens Res. 2017;40:277–83.
Obara T, Ohkubo T, Satoh M, Mano N, Imai Y. Home and Office Blood Pressure Control among Treated Hypertensive Patients in Japan: Findings from the Japan Home versus Office Blood Pressure Measurement Evaluation (J-HOME) Study. Pharmaceuticals. 2010;3:419–32.
Wada A, Kabayama M, Godai K, Kido M, Ohata Y, Murakami N, et al. Factors influencing the continuation of home blood pressure measurement in community-dwelling older adults: the NOSE study. J Hypertens. 2024;42:694–700.
Satake S, Arai H. The revised Japanese version of the Cardiovascular Health Study criteria (revised J‐CHS criteria). Geriatr Gerontol Int. 2020;20:992–3.
Kojima G, Iliffe S, Taniguchi Y, Shimada H, Rakugi H, Walters K. Prevalence of frailty in Japan: A systematic review and meta-analysis. J Epidemiol. 2017;27:347–53.
Blauth FG, Vilar LAdS, Pontes VdCB, Moriguti JC, Ferriolli E, Lima. NKdC. The effect of frailty on the 24‐hour blood pressure pattern in the very elderly. J Clin Hypertens. 2022;24:67–73.
Goldwater DS, Pinney SP. Frailty in Advanced Heart Failure: A Consequence of Aging or a Separate Entity? Clin Med Insights Cardiol. 2015;9:39–46.
Walker SR, Gill K, Macdonald K, Komenda P, Rigatto C, Sood MM, et al. Association of frailty and physical function in patients with non-dialysis CKD: a systematic review. BMC Nephrol. 2013;14:228.
Mancia G, Bertinieri G, Grassi G, Parati G, Pomidossi G, Ferrari A, et al. Effects of blood-pressure measurement by the doctor on patient’s blood pressure and heart rate. Lancet. 1983;2:695–8.
Maher D, Ailabouni N, Mangoni AA, Wiese MD, Reeve E. Alterations in drug disposition in older adults: a focus on geriatric syndromes. Expert Opin Drug Metab Toxicol. 2021;17:41–52.
Orkaby AR, Lunetta KL, Sun FJ, Driver JA, Benjamin EJ, Hamburg NM, et al. Cross-sectional association of frailty and arterial stiffness in community-dwelling older adults: the Framingham Heart Study. J Gerontol A Biol Sci Med Sci. 2019;74:373–9.
Lee H-Y, Oh B-H. Aging and arterial stiffness. Circ J. 2010;74:2257–62.
Steppan J, Barodka V, Berkowitz DE, Nyhan D. Vascular stiffness and increased pulse pressure in the aging cardiovascular system. Cardiol Res Pract. 2011;2011:263585.
Zhou B, Carrillo-Larco RM, Danaei G, Riley LM, Paciorek CJ, Stevens GA, et al. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 2021;398:957–80.
Lawes CM, Rodgers A, Bennett DA, Parag V, Suh I, Ueshima H, et al. Blood pressure and cardiovascular disease in the Asia Pacific region. J Hypertens. 2003;21:707–16.
Hoshide S, Kario K, de la Sierra A, Bilo G, Schillaci G, Banegas JR, et al. Ethnic differences in the degree of morning blood pressure surge and in its determinants between Japanese and European hypertensive subjects: data from the ARTEMIS study. Hypertension. 2015;66:750–6.
Acknowledgements
We sincerely appreciate all NOSE study participants for their kind cooperation. We are grateful to all relevant members of the Nose Town Office staffs, and the Osaka University Graduate School staffs, especially Mio Kubo, Keigo Kobayashi, Motoko Nogami, Werayuth Srithumsuk, Nonglak Klinpudtan, Haruna Kikuchi, Minori Eguchi, Ayano Tamura, Mayuka Iguchi, Toshiki Mizuno, Tomoko Yano, Yuka Yokoyama, Riko Kinjo, Natsumi Fujiwara, Ayaka Hiratsuka, Fang Wen, Masaaki Isaka, Chisato Hori, Maya Mitani, Yui Toshimitsu, Reina Yokokawa, Mei Nishida and Yuri Tominaga. We would like to thank Editage (www.editage.jp) for English language editing.
Funding
This study was supported by the Top-Z Research Grant from OMRON HEALTHCARE Co., Ltd. Open Access funding provided by Osaka University.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
This study was supported by the Top-Z Research Grant from OMRON HEALTHCARE Co., Ltd. K.K., T.O., and Y.T. have received research grants from OMRON HEALTHCARE Co., Ltd. T.O. and K.A. are consultants of OMRON HEALTHCARE Co., Ltd. F.M. and S.N. are employees of OMRON HEALTHCARE Co., Ltd.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ohata, Y., Kabayama, M., Godai, K. et al. Office and home blood pressure and their difference according to frailty status among community-dwelling older adults: the NOSE study. Hypertens Res 48, 1389–1398 (2025). https://doi.org/10.1038/s41440-025-02145-8
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41440-025-02145-8
Keywords
This article is cited by
-
Frailty and blood pressure: an unresolved relationship
Hypertension Research (2025)
