
Abstract
Antihypertensive therapy has reduced cardiovascular mortality; however, challenges remain, including residual risk in treated patients and the population burden associated with borderline hypertension. Previous Japanese estimates of the population attributable fraction (PAF) are derived from older cohorts and often lacked stratification by treatment status. We conducted a prospective study of 61,495 participants (women: 56.7%, aged 60.7 ± 11.0 years) from the Tohoku Medical Megabank Community-Based Cohort Study. Participants were classified into six blood pressure (BP) categories based on the JSH 2019 guidelines, and further stratified by hypertension treatment status, resulting in 12 groups. Using untreated individuals with normal BP as the reference, we calculated multivariable-adjusted hazard ratios (HR), 95% confidence intervals (CI), and PAF for the remaining groups using Cox proportional hazards model. During a median follow-up of 6.5 years, 1909 deaths were recorded. HRs increased with rising BP in both untreated and treated participants. The overall PAF for all-cause mortality due to non-normal BP was 9.45%, with a marked sex difference (12.25% in male and 5.16% in female). The highest PAF contributions were observed in the treated Grade I hypertension group (2.18%) and the untreated elevated BP group (1.28%). In this contemporary Japanese cohort, non-normal BP accounts for 9.45% of all-cause mortality, representing a substantial public health burden, particularly among men. The substantial PAF contributions from both treated patients and untreated individuals with elevated BP highlight the importance of effective BP management for both primary and secondary prevention.

Similar content being viewed by others

Introduction
Blood pressure (BP) lowering therapy is a cornerstone of modern cardiovascular disease prevention, and its widespread adoption has substantially reduced mortality from cardiovascular diseases (CVD), including stroke and myocardial infarction [1,2,3]. Despite these advances, significant clinical challenges remain. One such factor is the residual risk observed even in patients who achieve target BP levels under treatment [4, 5]. Furthermore, untreated borderline conditions, such as prehypertension and elevated BP, which are not typically targeted for pharmacological intervention but are highly prevalent, represent a major contributor to the overall burden of CVD in the population [6].
Most existing research has focused on assessing relative risk at the individual level, whereas large-scale studies quantifying the population attributable fraction (PAF) of non-normal BP for all-cause mortality in contemporary Japan remain limited [7, 8]. PAF is a public health indicator that estimates the proportion of a disease burden across an entire population attributable to a specific risk factor.
Therefore, this study aimed to quantitatively assess the impact of non-normal BP on all-cause mortality using PAF, based on recent guidelines, and leveraging large-scale community-based cohort data from the Tohoku Medical Megabank (TMM) Project. Particular emphasis was placed on strict stratification of participants according to antihypertensive treatment status to enable a more precise risk assessment.
Methods
Study setting, design
The TMM Project was conducted jointly by the Tohoku University Tohoku Medical Megabank Organization (ToMMo) and Iwate Medical University Iwate Tohoku Medical Megabank Organization (IMM) [9]. The TMM Project includes two prospective cohort studies in Miyagi and Iwate: the TMM Community-Based Cohort Study (TMM CommCohort Study), which is a population-based adult cohort study [10, 11] and the TMM Birth and Three-Generation Cohort Study (TMM BirThree Cohort Study), which is a birth and three-generation cohort study [12].
The baseline survey for the TMM CommCohort Study was conducted between May 2013 and March 2016 among residents aged ≥20 years living in Miyagi and Iwate, through two approaches. Type 1 surveys were administered at specific municipal health check-ups, while Type 2 survey was conducted at the Community Support Center in ToMMo and IMM. In both surveys, blood and urine tests were collected, and self-administered questionnaires were obtained. This prospective study utilized data exclusively from the Type 1 survey.
Ethical considerations
The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki, and was reviewed and approved by the Ethics Committee of ToMMo, Tohoku University (first edition: 2012-4-617, latest edition: 2024-4-049). At the IMM, approval from the Ethics Committee of Iwate Medical University was obtained on April 4, 2013 (HGH25-2). The latest approval (revised 17th edition) was obtained on December 14, 2023. Written informed consent was obtained from each participant before participation in the study.
BP classification
Each participant was measured systolic BP (SBP) and diastolic BP (DBP) in a sitting position using an upper arm automatic sphygmomanometer at the site of the specific municipal health checkup. BP was measured twice in accordance with the instructions of the Ministry of Health, Labor, and Welfare. However, depending on the situation at the municipalities’ health check-up sites, one measurement was allowed. The first value was used in the analysis.
Based on JSH2019 [13], each participant was classified into six categories: Normal BP, SBP < 120 mmHg and DBP < 80 mmHg; High normal BP, 120 ≤ SBP ≤ 129 mmHg and DBP < 80 mmHg; Elevated BP, 130 ≤ SBP ≤ 139 mmHg and/or 80 ≤ DBP ≤ 89 mmHg; Grade I hypertension (HT), 140 ≤ SBP ≤ 159 mmHg and/or 90 ≤ DBP ≤ 99 mmHg; Grade II HT, 160 ≤ SBP ≤ 179 mmHg and/or 100 ≤ DBP ≤ 109 mmHg; and Grade III HT, 180 mmHg ≤ SBP and/or 110 mmHg ≤ DBP. The JSH 2019 classification was originally designed for individuals not receiving antihypertensive treatment; however, in this study, it was applied to all participants, including those undergoing treatment, for consistency. Additionally, “non-normal BP” was defined as either having untreated high-normal BP or higher, or receiving antihypertensive treatment.
Treatment status for hypertension
Hypertension treatment status was assessed at baseline using a self-administered questionnaire. Participants who responded “I am currently under treatment,” were classified as the treatment group; all others were classified under untreated group. Participants who did not respond to the hypertension treatment status question were also classified as untreated.
Covariates
A self-administered questionnaire was used to collect information on smoking status, alcohol status, educational attainment, marital status, physical activity, depressive symptoms, diabetes treatment status, dyslipidemia treatment status, history of CVD (cerebral hemorrhage, cerebral infarction, subarachnoid hemorrhage, myocardial infarction, and angina pectoris), and history of cancer.
Smoking status was classified as current, ex-, or never-smoker. Participants who reported smoking fewer than 100 cigarettes in their lifetime were classified as never smokers. Those who smoked 100 or more cigarettes but were not currently smoking were classified as ex-smokers. Participants who had smoked 100 or more cigarettes and continued to smoke were classified current smokers.
Drinking status was classified into three categories: current, ex-, and never-drinkers. Participants were classified as current drinkers if they answered ‘yes’ to the question ‘Do you drink alcohol?’, ex-drinkers if they answered “quit”, and never drinkers if they answered “rarely (never) drink” or “constitutionally unable to drink.” Metabolic equivalent (MET) hours/day was calculated by multiplying the MET score for a specific activity by the hours per day spent on that activity [14]. Participants were then grouped into quartiles (Q1–Q4) based on their MET・hours per day.
Depressive symptoms were assessed using a self-administered Center for Epidemiologic Studies Depression Scale (CES-D) questionnaire [15, 16]. A CES-D score of ≥ 16 was defied as indicative of depression symptom [16]. Missing data were categorized as unknown.
Estimated 24-h sodium and potassium excretion levels were calculated using Tanaka’s formula [17]. The urinary sodium-to-potassium (Na/K) ratio was calculated by dividing the estimated 24-h sodium excretion by the potassium excretion. Body mass index (BMI) was calculated as weight (kg) divided by height squared (m). Height and weight were measured at a specific municipal health checkup site.
Confirmation of all-cause mortality
ToMMo and IMM employed different methods for participant follow-up. ToMMo reviewed the municipal basic resident register almost annually to identify participants who met any of the following categories: 1) death was reported by family members, 2) the address was unknown and mail could not be delivered, and 3) withdrawal from the National Health Insurance was confirmed due to death. In contrast, IMM identified deaths and relocations by annually collating municipal basic resident register data electronically or by requesting a certificate of residence from all participants.
‘Death’ was defined from the date of death. Participants who relocated and could not be followed for vital status were censored on the date of relocation. For participants without these events, the follow-up period extended to the last day of follow-up. The follow-up period for the survival analysis ended on December 31, 2021. Withdrawal of consent was monitored using data available up to December 11, 2023.
Statistical analyses
The basic characteristics of participants were summarized by BP category according to the JSH2019 classification, separately for treated and untreated participants. Cox proportional hazard model was used to calculate the multivariable adjusted hazard ratio (HR) and 95% confidence intervals (CI) for all-cause mortality by BP classification in both groups. Covariates used in the model comprised age in years (20–39, 40–49, 50–59, 60–69, ≥70), sex, study area (Miyagi, Iwate), fiscal year of survey participation (FY2013, FY2014, FY2015), season of the survey (spring or autumn, summer or winter), BMI (<18.5 kg/m2, 18.5–24.9 kg/m2, ≥25.0 kg/m2), smoking status (current, ex-, never-smoker, unknown), drinking status (current, ex-, never-drinker, unknown), educational attainment (elementary/junior high/high school, vocational school/junior college/technical college, university or higher, other, unknown), marital status (married, unmarried, separated, widowed, unknown), physical activity (Q1–Q4, unknown), depressive symptom (presence, absence, unknown), treatment of diabetes (presence, absence, unknown), treatment of dyslipidemia (presence, absence, unknown), history of cardiovascular disease (presence, absence), history of cancers (presence, absence), and Na/K ratio. The analyses were conducted according to sex.
We further calculated the PAF as pd × {HR-1}/HR, where pd is the proportion of cases exposed to the risk factor [18]. PAF was calculated for each group except for the normal BP group. Additionally, the sum of the PAFs calculated for each group was used to determine the overall PAF of all-cause mortality attributable to the non-normal BP.
In addition, two sensitivity analyses were performed. First, to align with previous studies [7, 8], the analysis was restricted to participants aged ≥40 years with no history of CVD. Second, participants who did not respond to the question regarding hypertension treatment status were excluded.
All statistical analyses were performed using SAS version 9.4 (SAS Inc., Cary, NC, USA). Two-tailed p-values < 0.05 were considered statistically significant.
Results
There were 62,542 participants who were enrolled in the baseline survey and had not withdrawn their consent as of December 2023 (Fig. 1). The following participants were excluded: those who did not return the questionnaire (n = 861); those who had an observation period of 0 days (n = 142); those with missing BP data (n = 40); those with missing BMI data (n = 1), and those with missing sodium-to-potassium ratio data (n = 89). Ultimately, 61,495 participants were included in the analysis. The total observation period was 401,902 person-years, with 1909 deaths.

Flowchart of study participants
The basic characteristics of untreated and treated participants according to BP classification are shown in Table 1. Among untreated participants, those with higher BP tended to be older, male, obese with a BMI of ≥25 kg/m2, current smoker, current drinker, physically active, exhibit high Na/K ratio, and low rates of depression. Among treated participants, higher BP was associated with greater proportion of obesity, higher physical activity, higher prevalence of dyslipidemia treatment, elevated Na/K ratio, and lower prevalence of depression.
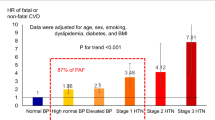
Table 2 presents the multivariable adjusted HR for all-cause mortality according to BP classification and hypertension treatment status. Using untreated normal BP participants as the reference group, HRs increased progressively with higher BP for both untreated and treated participants. The PAF for all-cause mortality in participants with non-normal BP was 9.45%. Among all groups, the highest PAF was observed in the treated Grade I group (2.18%), followed by the untreated elevated BP group (1.28%).
Table 3 presents the multivariable adjusted HR for all-cause mortality according to BP classification and hypertension treatment status, stratified by sex. Among males, higher BP was associated with an increased risk of all-cause mortality in both untreated and treated groups, except for treated Grade III. Similarly, among females, higher BP was associated with a higher risk for all-cause mortality in both untreated and treated participants. The PAF for all-cause mortality associated with non-normal BP was 12.25% in male and 5.16% in female.
Tables 4 and 5 present the results of the analysis restricted to participants aged ≥40 years with no history of CVD. The PAF for all-cause mortality associated with non-normal BP was 8.00% overall, 9.26% in male, and 5.44% in female.
Supplementary Tables 1, 2 present the results of the analysis after excluding participants who did not respond to questions on hypertension treatment status. The overall PAF for all-cause mortality in the non-normal BP group was 8.35% (13.06% in male and 6.45% in female). When the analysis was restricted to participants aged ≥40 years with no history of CVD, the PAF was 7.46% overall (10.76% in male and 7.20% in female).
Discussion
This study was a large-scale cohort survey of ~60,000 individuals from the general population, quantitatively evaluating the impact of non-normal BP on all-cause mortality using PAF. The overall PAF for all-cause mortality attributable to non-normal BP was 9.45%, suggesting that ~10% of total deaths could potentially be avoided if all participants were normotensive.
A notable finding in our results is the non-linear relationship between the ascending BP categories and their respective contributions to the PAF. Each category’s contribution is determined not only by its associated hazard ratio (HR) but also by the frequency of deaths within that category. Consequently, the treated Grade I hypertension group, which combines substantial risk with high prevalence, contributed most to the total PAF. This finding highlights the considerable public health burden imposed by moderately elevated but highly prevalent BP categories, suggesting that prevention strategies should target both high-risk individuals and this large, moderate-risk population.
The study also revealed a sex difference in the PAF of all-cause mortality attributable to non-normal BP. The PAF in men (12.25%) was more than twice that in women (5.16%), indicating a greater impact on male mortality. Comparison of HRs across BP categories showed no consistent sex-based differences in individual risk. For instance, in the treated “High normal BP” category, the adjusted HR was 1.11 in men versus 1.28 in women, indicating slightly higher risk in women for this category. Therefore, differences in individual relative risk alone are unlikely to account for the observed sex disparity in PAF. Conversely, a clear sex difference was observed in the distribution of participants across BP categories. The proportion of women with normal BP was 33.5%, compared with 20.0% of men, leaving 80% of the male cohort exposed to some level of hypertension risk versus 66.5% of women. This distribution bias, rather than differences in individual risk, largely explains the higher PAF observed in men.
Past Japanese studies have reported the PAF of all-cause mortality attributable to non-normal BP. A meta-analysis of 13 cohort studies (baseline 1977–1993) reported values of 22.7% for men and 17.9% for women [7], while a nationwide cohort study across nine public health center districts (baseline 1990–1993) reported 17.9% for men [8]. In the present study, a sensitivity analysis restricted participants to those aged ≥40 years with no history of CVD, consistent with these earlier studies. The resulting PAF was 9.26% for men and 5.44% for women (Supplementary Table 2), indicating lower values than previously reported. Several methodological factors may explain this difference. First, the follow-up period in this study (median 6.5 years) was shorter than in previous reports (mean 9.6 years for men and 9.9 years for women in one study [7]; median 11.0 years in the other [8]). Consequently, the full long-term impact of non-normal BP on mortality may not have been entirely captured, potentially contributing to a lower PAF. Second, regional heterogeneity in medical care could influence HRs for a given BP level, as the quality and intensity of management for comorbid cardiovascular risk factors—such as dyslipidemia and diabetes—varies geographically. Third, differences in statistical adjustment likely contributed to the discrepancy. This study controlled for an extensive range of confounding factors, including educational attainment, marital status, physical activity, depressive symptoms, and urinary sodium-to-potassium ratio [19,20,21,22,23,24,25,26], whereas previous studies included fewer covariates, possibly leading to overestimated HRs and PAFs. Generally, more comprehensive adjustment refines risk estimates and can reduce the apparent PAF.
In addition to these methodological factors, the historical context differs substantially. Previous studies had baseline surveys between 1977 and 1993, whereas this study’s baseline was 2013–2016. Over the past two decades, antihypertensive therapy has advanced, with effective, well-tolerated drugs, such as ARBs, becoming widely available [27]. Management of other cardiovascular risks, including dyslipidemia with statins, has also been standardized [28]. These advances may have reduced the impact of a given BP level on mortality, potentially contributing to a lower PAF, although this cannot be directly demonstrated in the current study design.
In the sensitivity analysis limiting participants to those aged ≥40 years without CVD, the overall PAF decreased from 9.45% to 8.00% (Table 4). This decline is likely attributable to the exclusion of high-risk individuals with prior CVD, in whom elevated BP confers a markedly higher risk of recurrence or death. Excluding this group lowered the average HR, resulting in a reduced PAF. These findings underscore the importance of BP management in secondary prevention of CVD, while highlighting that non-normal BP accounts for approximately 8% of deaths even among individuals without CVD history.
A further sensitivity analysis excluded individuals who did not respond regarding hypertension treatment status. In the primary analysis, non-respondents were classified as “untreated.” Excluding them resulted in a slight decrease in overall PAF from 9.44% to 8.35% (Supplementary Table 1). Non-respondents were older (64.6 ± 8.2 years vs. 60.0 ± 11.3 years) and had higher mortality rates (5.8 vs. 4.5 deaths per 1000 person-years), suggesting that their exclusion modestly lowered the PAF. Nevertheless, the difference was limited, confirming that the primary analysis’ treatment of non-respondents did not materially affect the study’s conclusions.
This study has several limitations. First, participation was voluntary, which may have introduced selection bias by producing a relatively healthier study population. Nevertheless, this is unlikely to have substantially affected the observed association between BP categories and all-cause mortality. Second, the study was conducted at two facilities using different mortality follow-up methods. Although some deaths may have been overlooked in the ToMMo data, the extent of potential under-ascertainment remains unknown.
Despite these limitations, this study quantitatively demonstrated, using PAF, that non-normal BP continues to impose a substantial public health burden on all-cause mortality among contemporary Japanese community residents. Overall, ~10% of deaths were attributable to non-normal BP, with the effect notably more pronounced in men, where the contribution to mortality exceeded twice that observed in women. Furthermore, even when restricted to a relatively healthy population without a history of CVD, non-normal BP accounted for 8% of deaths. These findings reaffirm the importance of BP management in primary and secondary prevention.
Perspective of Asia
Japan is a leading country facing demographic challenges, having entered a “super-aging society” ahead of the rest of the world. This situation in Japan is also a microcosm of the major changes facing the entire Asia region. Rapid demographic change, aging, and rapid urbanization in Asia have been noted to be increasing the burden of CVD [29]. PAF calculated in this study quantitatively demonstrates the impact of non-normal blood pressure on mortality in this context. Therefore, the disease burden quantified in Japan, which has become a super-aging society, provides important insights into the importance of public health measures for Asian countries experiencing similar societal changes in the future.
Conclusion
In conclusion, non-normal BP remains a major contributor to preventable death in contemporary Japan, accounting for ~10% of all-cause mortality. The public health burden is disproportionately high in men, with the PAF more than twice that observed in women, highlighting the need for sex-specific strategies in BP management. Furthermore, our findings indicate that the greatest portion of this burden arises not from the highest-risk individuals, but from the large population with moderately elevated but highly prevalent BP, such as those with treated Grade I hypertension. These results underscore the importance of implementing population-wide risk-reduction strategies alongside targeted management of high-risk groups.
References
SPRINT Research Group, Wright JT Jr, Williamson JD, Whelton PK, Snyder JK, Sink KM, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373:2103–16. https://doi.org/10.1056/NEJMoa1511939.
Turnbull F. Blood Pressure Lowering Treatment Trialists’ Collaboration. Effects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively-designed overviews of randomised trials. Lancet. 2003;362:1527–35. https://doi.org/10.1016/s0140-6736(03)14739-3.
ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA. 2002;288:2981–97. https://doi.org/10.1001/jama.288.23.2981.
Almgren T, Persson B, Wilhelmsen L, Rosengren A, Andersson OK. Stroke and coronary heart disease in treated hypertension - a prospective cohort study over three decades. J Intern Med. 2005;257:496–502. https://doi.org/10.1111/j.1365-2796.2005.01497.x.
Liu K, Colangelo LA, Daviglus ML, Goff DC, Pletcher M, Schreiner PJ, et al. Can Antihypertensive Treatment Restore the Risk of Cardiovascular Disease to Ideal Levels?: The Coronary Artery Risk Development in Young Adults (CARDIA) Study and the Multi-Ethnic Study of Atherosclerosis (MESA). J Am Heart Assoc. 2015;4:e002275. https://doi.org/10.1161/JAHA.115.002275.
Kuwahara K, Ohkubo T, Inoue Y, Honda T, Yamamoto S, Nakagawa T, et al. Blood pressure classification using the Japanese Society of Hypertension Guidelines for the Management of Hypertension and cardiovascular events among young to middle-aged working adults. Hypertens Res. 2024;47:1861–70. https://doi.org/10.1038/s41440-024-01653-3.
Murakami Y, Hozawa A, Okamura T, Ueshima H. Evidence for Cardiovascular Prevention From Observational Cohorts in Japan Research Group (EPOCH-JAPAN). Relation of blood pressure and all-cause mortality in 180,000 Japanese participants: pooled analysis of 13 cohort studies. Hypertension. 2008;51:1483–91.
Ikeda A, Iso H, Yamagishi K, Inoue M, Tsugane S. Blood pressure and the risk of stroke, cardiovascular disease, and all-cause mortality among Japanese: the JPHC Study. Am J Hypertens. 2009;22:273–80.
Kuriyama S, Yaegashi N, Nagami F, Arai T, Kawaguchi Y, Osumi N, et al. The Tohoku Medical Megabank Project: Design and Mission. J Epidemiol. 2016;26:493–511.
Hozawa A, Tanno K, Nakaya N, Nakamura T, Tsuchiya N, Hirata T, et al. Study Profile of the Tohoku Medical Megabank Community-Based Cohort Study. J Epidemiol. 2021;31:65–76.
Hozawa A, Nakaya K, Nakaya N, Nakamura T, Kogure M, Hatanaka R, et al. Progress Report of the Tohoku Medical Megabank Community-based Cohort Study: Study Profile of the Repeated Center-based Survey During Second Period in Miyagi Prefecture. J Epidemiol. 2024;34:434–43.
Kuriyama S, Metoki H, Kikuya M, Obara T, Ishikuro M, Yamanaka C, et al. Cohort Profile: Tohoku Medical Megabank Project Birth and Three-Generation Cohort Study (TMM BirThree Cohort Study): rationale, progress and perspective. Int J Epidemiol. 2020;49:18–9.
Umemura S, Arima H, Arima S, Asayama K, Dohi Y, Hirooka Y, et al. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2019). Hypertens Res. 2019;42:1235–481.
Nakaya N, Xie T, Scheerder B, Tsuchiya N, Narita A, Nakamura T, et al. Spousal similarities in cardiometabolic risk factors: A cross-sectional comparison between Dutch and Japanese data from two large biobank studies. Atherosclerosis. 2021;334:85–92.
Radloff LS. The CES-D Scale: A self-report depression scale for research in the general population. Appl Psychological Meas. 1977;1:385–401.
Shima S, Kano T, Kitamura T, Asai M. New self-rating scales for depression. Seishinigaku. 1985;27:717–23. [In Japanese]
Tanaka T, Okamura T, Miura K, Kadowaki T, Ueshima H, Nakagawa H, et al. A simple method to estimate populational 24-h urinary sodium and potassium excretion using a casual urine specimen. J Hum Hypertens. 2002;16:97–103.
Rockhill B, Newman B, Weinberg C. Use and misuse of population attributable fractions. Am J Public Health. 1998;88:15–9. https://doi.org/10.2105/ajph.88.1.15.
Satoh A, Arima H, Ohkubo T, Nishi N, Okuda N, Ae R, et al. Associations of socioeconomic status with prevalence, awareness, treatment, and control of hypertension in a general Japanese population: NIPPON DATA2010. J Hypertens. 2017;35:401–8.
Dickinson HO, Mason JM, Nicolson DJ, Campbell F, Beyer FR, Cook JV, et al. Lifestyle interventions to reduce raised blood pressure: a systematic review of randomized controlled trials. J Hypertens. 2006;24:215–33.
Tokioka S, Nakaya N, Hatanaka R, Nakaya K, Kogure M, Chiba I, et al. Depressive symptoms as risk factors for the onset of home hypertension: a prospective cohort study. Hypertens Res. 2024;47:2989–3000.
Hisamatsu T, Kogure M, Tabara Y, Hozawa A, Sakima A, Tsuchihashi T, et al. Practical use and target value of urine sodium-to-potassium ratio in assessment of hypertension risk for Japanese: Consensus Statement by the Japanese Society of Hypertension Working Group on Urine Sodium-to-Potassium Ratio. Hypertens Res. 2024;47:3288–302.
Leung CY, Huang HL, Abe SK, Saito E, Islam MR, Rahman MS, et al. Association of Marital Status With Total and Cause-Specific Mortality in Asia. JAMA Netw Open. 2022;5:e2214181.
Inoue M, Iso H, Yamamoto S, Kurahashi N, Iwasaki M, Sasazuki S, et al. Daily total physical activity level and premature death in men and women: results from a large-scale population-based cohort study in Japan (JPHC study). Ann Epidemiol. 2008;18:522–30.
Meng R, Yu C, Liu N, He M, Lv J, Guo Y, et al. Association of Depression With All-Cause and Cardiovascular Disease Mortality Among Adults in China. JAMA Netw Open. 2020;3:e1921043.
Gan L, Zhao B, Inoue-Choi M, Liao LM, Graubard BI, Weinstein SJ, et al. Sex-specific associations between sodium and potassium intake and overall and cause-specific mortality: a large prospective U.S. cohort study, systematic review, and updated meta-analysis of cohort studies. BMC Med. 2024;22:132.
Satoh M, Kurosawa K, Obara T, Matsuura M, Inoue R, Takahashi N, et al. Trends in Antihypertensive Drug Prescriptions Based on Claims Data in a Japanese Hospital. Iryo Yakugaku Jpn J Pharm Health Care Sci. 2017;43:9–17. [In Japanese].
Teramoto T, Sasaki J, Ishibashi S, Birou S, Daida H, Dohi S, et al. Comprehensive risk management for the prevention of cardiovascular disease: executive summary of the Japan Atherosclerosis Society (JAS) guidelines for the diagnosis and prevention of atherosclerotic cardiovascular diseases in Japan - 2012. J Atheroscler Thromb. 2013;20:603–15. https://doi.org/10.5551/jat.15867.
Dalakoti M, Lin NHY, Yap J, Cader A, Dipanker P, Lee D, et al. Primary Prevention of Cardiovascular Disease in Asia: Opportunities and Solutions. JACC Adv. 2025;4:101676. https://doi.org/10.1016/j.jacadv.2025.101676.
Acknowledgements
The authors thank all participants and municipal staff who assisted with our project. We also thank the members of ToMMo, including the Genome Medical Research Coordinators, office and administrative personnel, and software engineers for their assistance with the project. The complete list of members is available at https://www.megabank.tohoku.ac.jp/english/a240901/.
Funding
This work was supported by grants from the Tohoku Medical Megabank Project from the Ministry of Education, Culture, Sports, Science, and Technology (MEXT), and Japan Agency for Medical Research and Development, AMED [Grant Number JP20km0105001, JP22tm0124005], the Japanese Society for the Promotion of Science (JSPS) through a Grant-in-Aid for Scientific Research (C) [Grant Number 22K10575]. This research used a supercomputer system provided by the Tohoku Medical Megabank Project (funded by AMED under Grant Number JP21tm0424601).
Author information
Authors and Affiliations
Contributions
RH, NN, KN, KT and AH contributed to the study design and RH, NN and AH for statistical analysis, and RH, NN, KN, MT, KT and AH wrote the manuscript. NN, KN and AH supported data analysis. KT and AH collected data. All the authors contributed intellectually to the manuscript and approved its final version.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hatanaka, R., Nakaya, N., Kogure, M. et al. Population attributable fraction of all-cause mortality due to non-normal blood pressure: results from the 2013 to 2016 baseline survey of the TMM CommCohort Study. Hypertens Res 49, 303–314 (2026). https://doi.org/10.1038/s41440-025-02436-0
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41440-025-02436-0
