
Abstract
Elevated blood pressure (BP) has been linked to brain structure changes and cognitive decline. However, few studies have accounted for long-term cumulative BP exposure. We investigated the association between cumulative BP exposure, brain volume, cerebral blood flow (CBF), and cognitive decline. Furthermore, we explored whether alterations in brain volume and CBF mediated the association between cumulative BP and cognitive decline. We included 1012 adult participants from the Kailuan study. Cumulative BP exposure was calculated from 2006 to 2020. Brain MRI scans and the Montreal Cognitive Assessment (MoCA) were performed in 2020. Generalized linear regression models were used to investigate the associations between cumulative BP, brain volume, CBF, and cognitive function. Mediation analysis was performed to examine whether alterations in brain volume and CBF mediated the association between cumulative BP and cognitive decline. Compared with the lowest tertiles, the highest tertiles of cumulative SBP were associated with lower volumes in total brain (−9.11 [−16.25, −1.97]), total GM (−5.53 [−10.02, −1.04]), frontal lobe (−2.46 [−4.15, −0.78]), temporal lobe (−1.37 [−2.51, −0.23]) and hippocampus (−0.15 [−0.26, −0.03]), and the highest tertiles of cumulative DBP were associated with lower volume in frontal lobe (−2.33 [−3.98, −0.68]) and temporal lobe (−1.15 [−2.27, −0.04]). Higher cumulative SBP and DBP were associated with lower total and regional CBF and MoCA scores (all P < 0.05). The associations between cumulative DBP and cognitive decline were mediated by the volumes in total GM, frontal lobe and temporal lobe. Early intervention in cumulative BP may help preserve brain structure and function.

Similar content being viewed by others

Introduction
With improvements in social progress, living standards and medical conditions, the global aging population has increased significantly, which is accompanied by an increased prevalence of cognitive decline and dementia [1]. The pathological basis of cognitive decline is changes in brain structure [2]. The maintenance of normal brain structure and function requires a good blood supply to the brain and the clearance of metabolites [3]. The main factor that ensures a normal cerebral blood flow (CBF) supply is maintaining blood pressure (BP) within a certain range; a BP that is too high or too low can affect the cerebral blood supply and subsequently damage brain structure and impair brain function [4]. Previous studies have shown that hypertension is a risk factor for structural brain damage and cognitive decline, but most studies have analyzed the associations between a single BP value and structural brain damage or cognitive decline [5].
Cumulative exposure accounts for not only the cumulative exposure to risk factors but also the duration of exposure. Compared with a single exposure, cumulative exposure is more reliably associated with adverse outcomes. Previous studies have shown that cumulative BP, fasting blood glucose (FBG), blood lipid and body mass index (BMI) exposures are more strongly associated with atherosclerotic cardiovascular disease than are single measurements of BP, FBG, blood lipids and BMI [6,7,8,9]. Mahinrad S. et al. reported that higher cumulative BP exposure is a risk factor for cognitive decline [10]. In theory, cumulative BP exposure could impair cognitive function by affecting brain structure [10]. To confirm the above hypothesis, we used multimodal brain imaging data embedded in the Kailuan study to systematically explore the associations among cumulative BP exposure, brain volume, CBF, and cognitive function and to further analyze whether brain alterations mediate the association between cumulative BP exposure and cognitive decline.
Methods
Participants
The study was approved by the ethics committees of Kailuan General Hospital. All participants provided informed consent in accordance with the protocol. A prospective cohort study was conducted by the Kailuan Study in Tangshan, China [11]. From July 2006 to October 2007, a total of 101,510 individuals older than 18 years from the Kailuan community were included in the first survey and followed up every 2 years. The questionnaire assessment, clinical assessment and laboratory examination were conducted by professionals. The seventh follow-up began in December 2020, and some participants underwent head magnetic resonance imaging (MRI) and cognitive function assessment on the basis of the original protocol. The criteria for the inclusion of participants in this study were as follows: (1) participated in the 7th follow-up and underwent cognitive function assessment and head MRI examination beginning in December 2020; (2) underwent the first physical examination between 2006 and 2007; and (3) participated in at least 1 follow-up visit between 2008 and 2018. Participants with a history of tumor, stroke or incomplete imaging data were excluded. The flow chart is shown in Fig. 1. Overall, 1012 participants were included in the study.

Flowchart of enrolment for participants in this study
Cumulative BP exposure
Systolic BP (SBP) and diastolic BP (DBP) were measured by trained professionals via a digital BP monitor (Omron HBP-1100U). After the participants sat in a quiet room for 5 min, the BP of the right brachial artery was measured. The average value of 3 measurements was taken for analysis. The cumulative BP exposure (unit: mm Hg × years) for each participant was calculated as the sum of the mean BP of two consecutive follow-up visits multiplied by the time interval between follow-up visits (unit: year) [12]: cumulative BP = [BP2006 + BP2008] / 2 × [Visit2008 − Visit2006] + [BP2008 + BP2010] / 2 × [Visit2010 − Visit2008] + …… + [BP2018 + BP2020] / 2 × [Visit2020 − Visit2018]). The cumulative SBP and DBP were calculated.
MRI data acquisition
All participants were scanned via a 3.0 T MRI scanner (GE, 750 W, Milwaukee, WI, USA). The imaging protocol included 3D T1-brain volume images (echo time (TE) = 2.6 ms; repetition time (TR) = 6.7 ms; flip angle (FA) = 15°; slice thickness = 1 mm; field of view (FOV) = 256 mm × 256 mm; gap = 1 mm; 170 slices) and 3D pseudocontinuous arterial spin labeling (3D-pc ASL) images (TR = 5313 ms; TE = 10.7 ms; slice thickness=4 mm; flip angle=111°; in-plane resolution, 3.37 mm × 3.37 mm; FOV = 256 mm × 256 mm; and postlabel delay = 2525 ms).
MRI data processing
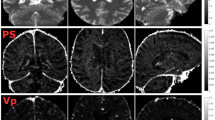
3D-PC ASL images were processed via SPM12 as described previously [13]. The CBF maps were automatically generated via 3D ASL Functool software (AW4.6 Workstation, GE Healthcare). The CBF images were subsequently registered into the MNI space. Finally, the average CBF values of the total brain and areas of interest (frontal lobe, parietal lobe, temporal lobe and hippocampus) closely related to cognition were extracted (Supplementary Fig. 1) [14, 15].
SPM12 software was used to preprocess the 3D T1-brain volume image data. The detailed processing steps, including reorientation, segmentation, and normalization, have been described in previous studies [16]. Finally, total GM volume and white matter volume were computed for all participants. The total brain volume was defined as the sum of the total GM volume and white matter volume [17]. Additionally, regional brain volumes (frontal lobe, parietal lobe, temporal lobe, and hippocampus) closely related to cognition were extracted (Supplementary Fig. 1).
Covariate measurement
The demographic characteristics of the participants, including age, sex, medical history and family medication information, were collected by trained professionals via standard questionnaires. The participants self-reported their lifestyle habits, including smoking status, alcohol consumption status and physical exercise. The physical examination involved an evaluation of weight, height, and BMI. Laboratory tests were conducted by using venous blood samples collected at 7–9 a.m. on the second day following a 12-hour fast. Biochemical markers, including FBG, triglyceride, total cholesterol, low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol levels, were measured via an automated analyzer (Hitachi 747; Hitachi Ltd., Tokyo, Japan).
Cognitive function assessment
Cognitive function was assessed by psychiatrists via the Montreal Cognitive Assessment (MoCA). This scale covers major cognitive functions, including visuospatial/executive functions, language, attention, naming, abstraction, orientation, and recall, and is widely used to screen for cognitive decline [18]. MoCA scores are adjusted for educational attainment. When a participant has less than 12 years of education, the MoCA score is increased by 1. The total MoCA score ranges from 0 to 30 points, with lower scores indicating poorer cognitive function.
Statistical analysis
Statistical analysis was performed via SAS 9.4 software. Cumulative BP exposure was assessed via continuous and tripartite variables. The general characteristics of the participants were evaluated according to cumulative SBP tertiles and are expressed as count (percentage) for categorical variables, mean ± standard deviation for continuous variables if normally distributed, and median (interquartile range) if skewed. Generalized linear regression models were used to investigate the associations between cumulative BP exposure, CBF, brain volume, and cognitive function. All analyses in this study were based on the following 3 models. Model 1 was adjusted for sex and age at baseline. Model 2 was based on Model 1 and was further adjusted for baseline smoking status, drinking status, physical exercise, BMI, FBG level, LDL-C level, antihypertensive drug use, hypoglycemic drug use, lipid-lowering drug use, and total intracranial volume. Considering the possible changes in BMI, FBG levels, LDL-C levels and drug use during follow-up, the average BMI, FBG level, LDL-C level, antihypertensive drug use, hypoglycemic drug use, and lipid-lowering drug use during follow-up were used in Model 3 to replace the BMI, FBG level, LDL-C level, antihypertensive drug use, hypoglycemic drug use, and lipid-lowering drug use in Model 2. Because Model 3 is adjusted for all confounding variables, the result obtained from this model is reported as the main result. In all the statistical analyses, P < 0.05 was considered to indicate statistical significance. Multiple imputation by chained equations was used to compensate for missing values of covariates. The results are expressed with regression coefficients β and 95% confidence intervals.
To test the hypothesis that cumulative BP affects cognitive function through alterations in brain volume and CBF, mediation analyses were conducted via the SAS CAUSALMED procedure. Mediation analysis adopts asymptotic theory for maximum likelihood estimation and uses the bootstrap method based on resampling (Monte Carlo simulation times = 1000) to calculate confidence intervals (CIs) [19]. It quantifies the direct effect (the effect not affected by the mediator), indirect effect (the effect of the independent variable on the mediator multiplied by the effect of the mediator on the outcome), and total effect (the association between the independent variable and the outcome, which is equal to the sum of the direct effect and the indirect effect) [20]. The proportion mediated is calculated by dividing the natural indirect effect by the total effect. The analyses were adjusted for sex, age at baseline, smoking status, drinking status, physical exercise, mean BMI, mean FBG level, mean LDL-C level, antihypertensive drug use, hypoglycemic drug use, and lipid-lowering drug use during follow-up.
Results
Demographic characteristics
A total of 1012 participants were enrolled in this study, including 505 males and 507 females. The mean age at MRI examination was 57.76 ± 9.99 years. All participants underwent an average of 6 BP measurements, and the average time interval from the first physical examination to the head MRI examination was 14.69 ± 0.71 years. Table 1 shows the baseline characteristics of participants according to the cumulative SBP tertiles. The participants in the highest cumulative SBP tertile were more likely to be older men, were more likely to smoke, drink, exercise, take antihypertensive drugs, and use hypoglycemic drugs; had higher FBG levels, LDL-C levels, and BMIs (P < 0.05).
Cumulative BP exposure and brain volume, CBF
Figure 2 and Supplementary Table 1 show the associations between cumulative BP exposure and brain volume. Compared with the lowest tertiles, the highest cumulative SBP tertiles were associated with lower volume in total brain (β [95% CI]: −9.11 [−16.25, −1.97]), total GM (β [95% CI]: -5.53 [−10.02, −1.04]), frontal lobe (β [95% CI]: −2.46 [−4.15, −0.78]), temporal lobe (β [95% CI]: −1.37 [−2.51, −0.23]) and hippocampus (β [95% CI]: −0.15 [−0.26, −0.03]). The highest cumulative DBP tertiles were associated with the volume in frontal lobe (β [95% CI]: −2.33[−3.98, −0.68]) and temporal lobe (β [95% CI]: −1.15[-2.27, −0.04]) (Supplementary Table 1). When the cumulative BP was a continuous variable, for each 1-SD increase in cumulative SBP exposure, the total brain, total GM, frontal lobe, parietal lobe, temporal lobe and hippocampal volumes decreased by 6.11, 3.09, 1.30, 0.42, 0.72 and 0.09 cm3, respectively. With each 1-SD increase in cumulative DBP exposure, the total brain, total GM, frontal lobe, temporal lobe and hippocampal volumes decreased by 4.57, 2.75, 1.45, 0.64 and 0.05 cm3, respectively (Fig. 2). Figure 3 and Supplementary Table 2 show the associations between cumulative BP exposure and total and regional CBF. Compared with the lowest tertiles, the highest cumulative SBP tertiles were associated with lower CBF in the total brain (β [95% CI]: −3.10 [−4.49, −1.71]), frontal lobe (β [95% CI]: −2.32 [−3.84, -0.81]), parietal lobe (β [95% CI]: −4.03 [−5.65, −2.41]), temporal lobe (β [95% CI]: −2.52 [−3.98, −1.06]), and hippocampus (β [95% CI]: −2.61 [−4.06,−1.16]). Compared with the lowest tertiles, the highest cumulative DBP tertiles were associated with lower CBF in the total brain (β [95% CI]: −3.02 [−4.38, −1.66]), frontal lobe (β [95% CI]: −2.10 [−3.58, −0.62]), parietal lobe (β [95% CI]: −3.60 [−5.19, −2.01]), temporal lobe (β [95% CI]: −2.45 [-3.88, −1.02]), and hippocampus (β [95% CI]: −2.66[−4.08, −1.24]) (Supplementary Table 2). When the cumulative BP was a continuous variable, for each 1-SD increase in cumulative SBP exposure, the CBF in the total brain, frontal lobe, parietal lobe, temporal lobe, and hippocampus decreased by 1.54, 1.14, 1.94, 1.29, and 1.17 ml/100 g/min, respectively. With each 1-SD increase in cumulative DBP exposure, the CBF in the total brain, frontal lobe, parietal lobe, temporal lobe, and hippocampus decreased by 1.47, 1.07, 1.76, 1.20, and 1.00 ml/100 g/min, respectively (Fig. 3).

Associations between cumulative BP measurements and brain volume. All analyses were adjusted for sex, age at baseline, smoking status, drinking status, physical exercise, mean BMI, mean FBG level, mean LDL-C level, antihypertensive drug use, hypoglycemic drug use, and lipid-lowering drug use. BP blood pressure, SBP systolic blood pressure, DBP diastolic blood pressure, FBG fasting blood glucose, LDL-C low-density lipoprotein cholesterol, BMI body mass index, GM gray matter

Associations between cumulative BP exposure and total and regional CBF. All analyses were adjusted for sex, age at baseline, smoking status, drinking status, physical exercise, mean BMI, mean FBG level, mean LDL-C level, antihypertensive drug use, hypoglycemic drug use, and lipid-lowering drug use. BP blood pressure, SBP systolic blood pressure, DBP diastolic blood pressure, FBG fasting blood glucose, LDL-C low-density lipoprotein cholesterol, BMI body mass index, GM gray matter, CBF cerebral blood flow
Cumulative BP exposure and cognitive function
Figure 4 and Supplementary Table 3 show the associations between cumulative BP exposure and MoCA scores. Compared with the lowest tertiles, the highest cumulative SBP (β [95% CI]: −1.06 [−1.69, −0.42]) and cumulative DBP tertiles (β [95% CI]: −0.99 [−1.61, −0.37]) were associated with lower MoCA scores. When cumulative BP exposure was a continuous variable, for each 1-SD increase in cumulative SBP and DBP exposure, the MoCA scores decreased by 0.48 and 0.41, respectively.

Associations between cumulative BP exposure and MoCA scores. All analyses were adjusted for sex, age at baseline, smoking status, drinking status, physical exercise, mean BMI, mean FBG level, mean LDL-C level, antihypertensive drug use, hypoglycemic drug use, and lipid-lowering drug use. BP blood pressure, SBP systolic blood pressure, DBP diastolic blood pressure, FBG fasting blood glucose, LDL-C low-density lipoprotein cholesterol, BMI body mass index, MoCA Montreal Cognitive Assessment
Brain volume, CBF and cognitive function
Supplementary Table 4 shows the associations among brain volume, CBF, and MoCA scores. For each 1-SD decrease in the total brain, total GM, frontal lobe, parietal lobe, temporal lobe, and hippocampal volumes, the MoCA scores decreased by 0.37, 0.48, 0.40, 0.39, 0.48 and 0.27, respectively. There were no significant associations between CBF and MoCA scores with respect to total or regional brain regions (P > 0.05).
Mediation analysis
After adjusting for potential confounding factors, mediation analysis revealed that the associations between cumulative DBP exposure and MoCA scores were mediated by total GM volume (indirect effect: −0.04 [−0.08, −0.01]; direct effect: −0.37 [−0.63, −0.11]; proportion: 10.20%), frontal lobe volume (indirect effect: −0.05 [−0.09, −0.01]; direct effect: −0.37 [−0.63, −0.11]; proportion: 11.47%) and temporal lobe volume (indirect effect: −0.04 [−0.08, −0.01]; direct effect: −0.37 [−0.63, −0.11]; proportion: 10.02%) (Fig. 5). Altered brain volume did not mediate the association between cumulative SBP exposure and MoCA scores.

Mediation effect by brain volume in the association between cumulative blood pressure and cognitive function. DE direct effect, GM gray matter, IE indirect effect, SBP systolic blood pressure, DBP diastolic blood pressure, MoCA Montreal Cognitive Assessment
Discussion
This study revealed that in the general population, cumulative SBP and DBP exposure were not only negatively associated with total and regional brain volume and CBF but also risk factors for cognitive decline. Decreased total brain, total GM, frontal lobe, parietal lobe, temporal lobe, and hippocampal volumes were significantly associated with lower MoCA scores. More importantly, decreased total GM, frontal lobe, and temporal lobe volumes mediated the association between cumulative DBP exposure and cognitive decline.
This study revealed that elevated cumulative BP exposure had disparate effects on total brain volume and regional brain volume. Both cumulative SBP and DBP exposure were negatively associated with total brain, total GM, frontal lobe, temporal lobe and hippocampal volumes. Additionally, cumulative SBP exposure was negatively associated with parietal lobe volume. These associations remained significant even after adjusting for potential confounding variables, including total intracranial volume and medication history. Furthermore, our findings indicated that cumulative SBP exposure exerted a more profound influence on the aforementioned brain regions than did cumulative DBP exposure. Hajjar et al. investigated the association between BP levels and brain volume in an elderly population and revealed a significant negative association between SBP and frontal‒parietal lobe volume [21]. A cohort study based on older adults (60–90 years old) without dementia demonstrated that in participants with untreated hypertension, elevated DBP was associated with a greater degree of hippocampal atrophy [22]. Additionally, Li et al. reported that both SBP and DBP were negatively associated with total and regional brain volume in the general adult population [13]. However, the above studies adopted single BP measurements, which cannot effectively reflect participants’ true BP levels within a certain period. This may be the cause of the resulting differences. In this study, we calculated the cumulative BP exposure over time using BP data across 14.7 years and investigated the associations between cumulative BP exposure and the volume of cognitively relevant brain regions in the general population. The hippocampus is the key brain region responsible for cognitive function. It is also the brain area that is most sensitive to fluctuations in BP [23]. We found that both higher cumulative SBP and DBP exposure are associated with lower hippocampal volume. Furthermore, our findings revealed a negative association between cumulative SBP exposure and parietal lobe volume, whereas no such association was observed with cumulative DBP exposure. Atrophy of the parietal lobe has been linked to both cognitive decline and the early stages of Alzheimer’s disease [24]. The results of our study indicate that the effect of cumulative SBP exposure on parietal lobe volume is specific. Furthermore, the present study investigated the associations between cumulative BP exposure and CBF. The findings revealed that both elevated cumulative SBP and DBP exposure resulted in a reduction in total and local CBF.
Although the underlying mechanisms of the associations between cumulative BP exposure and brain volume and perfusion remain unclear, the available literature reports that sustained BP elevation can lead to cerebral vascular remodeling by inducing damage to small artery endothelial cells [25] and the basement membrane [26] and a reduction in the number of vascular smooth muscle cells [27], leading to reduced CBF [28]. Consequently, sustained reductions in CBF result in endothelial dysfunction, oxidative stress, and aberrant protein expression, which in turn lead to further reductions in cerebral perfusion [23]. Second, elevated BP also disrupts the coordinated coupling among neurons, glial cells, and CBF in the cerebral microcirculation [29], affecting the transport of oxygen and glucose, which further leads to neuronal loss [30], resulting in a reduction in GM volume [31]. Furthermore, elevated BP can increase the number of peripheral blood inflammatory cytokines [32] through disruption of the blood‒brain barrier axis [33], resulting in damage to organs and the brain’s influence on the autonomic nervous system [34]. Additionally, the activation of glial cells associated with inflammation-induced nerve inflammation [35] can lead to additional structural and functional brain damage.
We found that cumulative SBP and DBP exposure were both inversely associated with cognitive decline after adjustment for conventional vascular risk factors. The Indo-US Cross National Dementia Epidemiology Study (INDO study) revealed that in participants older than 75 years, for every 10 mm Hg increase in DBP and SBP, the Mini-Mental State Examination (MMSE) score was reduced by more than 10% [36]. The Coronary Artery Risk Development in Young Adults (CARDIA) cohort study demonstrated that elevated cumulative SBP and DBP exposure in early adulthood was associated with diminished cognitive function in middle-aged individuals: for each 1-SD increase in cumulative SBP exposure, there was a statistically significant decrease in executive function, memory function, and global cognitive function, with effect sizes of 0.16, 0.12, and 0.12, respectively, for every 1-SD increase in cumulative DBP exposure, memory function decreased by 0.16 [10]. However, the above studies focused on specific ages in European and American individuals, some of whom were symptomatic patients. Our study, which was based on a general community population aged 29.7 to 83.9 years, confirmed the inverse association between cumulative BP exposure and cognitive decline. The underlying mechanism may be that long-term elevated cumulative BP exposure can lead to cerebral microcirculation disturbance and neuronal damage by reducing the vascular response, which in turn leads to cognitive decline [23]. Accordingly, the implementation of early intervention protocols pertaining to BP is instrumental in the attainment of cognitive function protection.
Importantly, decreased total GM, frontal lobe and temporal lobe volumes mediated the negative association between cumulative DBP exposure and cognitive function, and the mediating effects accounted for 10.199, 11.469 and 10.023% of the total effect, respectively. The GM is primarily composed of neurons, which are the fundamental units responsible for executing neural functions [37]. The temporal lobe serves as the network center for functions associated with memory, navigation, and time perception [38]. The frontal lobe is responsible for executive abilities, coordinating complex planning, organization, and multitasking activities [39]. A previous study demonstrated that for each 1-SD increase in DBP, the total GM volume, frontal lobe volume, and temporal lobe volume decreased by 4.04, 1.81, and 1.02, respectively [13]. In addition, DBP was negatively associated with cognitive functions, including memory and information processing speed [10, 40]. Both the frontal and temporal lobes are responsible for the processing of cognitive information [41, 42]. It can be reasonably deduced that prolonged exposure to elevated chronic SBP may result in cognitive decline through the impairment of neurons in the GM of these brain regions. Although no similar studies have been conducted, animal and human studies have confirmed that hypertension can not only lead to neuronal damage and apoptosis by inducing vascular dysfunction but also affect signal transmission between neurons, thereby affecting brain function [43, 44]. Increased DBP can also accelerate intracranial atherosclerosis and arteriolar sclerosis [45]. Therefore, long-term elevated cumulative DBP exposure can lead to further cognitive decline by causing damage to neurons in the supply region [46, 47].
Our study has several limitations. First, it should be noted that the present study was a cross-sectional study, which is unable to accurately reflect the causal associations among cumulative BP exposure, brain volume, CBF and cognitive function. Therefore, the mediation analysis in this study is exploratory and hypothesis-generating. Future longitudinal studies on the association between BP exposure, brain volume, CBF and cognitive function will be helpful in addressing this issue. Second, this study employed the MoCA to evaluate global cognitive function; however, this instrument may not be particularly sensitive to specific cognitive domains. Third, this study included an Asian population, and whether the findings of this study can be generalized to other populations remains unknown. Fourth, long-term cumulative BP exposure, which may ignore BP changes in the short term, was calculated in this study. Fifth, the types of antihypertensive drugs may have an impact on the association between cumulative BP, brain structure and cognitive function. However, detailed information on types of antihypertensive drugs was available for only a small subset of participants. In subsequent studies, we plan to collect medication information more comprehensively and further examine the potential effects of antihypertensive drug types on these associations.
In summary, we found that in the general population, cumulative BP exposure is negatively associated with total and regional brain volumes and CBF and is also a risk factor for cognitive decline. Decreased total and regional brain volumes are associated with cognitive decline. Mediation analysis revealed that decreased total brain, frontal lobe and temporal lobe volumes mediated the association between cumulative DBP exposure and cognitive decline. This study provides a theoretical basis for better understanding the harm of high cumulative BP exposure in clinical work and clarifies the importance of daily BP control. Our findings highlight that consistent control of BP can protect brain structure and function and prevent subsequent cognitive decline.
References
Chen LH, Liu YC. Interface design for products for users with advanced age and cognitive impairment. Int J Environ Res Public Health. 2022;19:2466.
Park DC, Reuter-Lorenz P. The adaptive brain: aging and neurocognitive scaffolding. Annu Rev Psychol. 2009;60:173–96.
Kisler K, Nelson AR, Montagne A, Zlokovic BV. Cerebral blood flow regulation and neurovascular dysfunction in Alzheimer's disease. Nat Rev Neurosci. 2017;18:419–34.
Gorelick PB. Blood pressure and the prevention of cognitive impairment. JAMA Neurol. 2014;71:1211–3.
Levine DA, Springer MV, Brodtmann A. Blood pressure and vascular cognitive impairment. Stroke. 2022;53:1104–13.
Xiong Z, Li J, Lin Y, Ye X, Xie P, Zhang S, et al. Intensity of hypertensive exposure in young adulthood and subclinical atherosclerosis in middle age: evidence from the CARDIA study. Front Cardiovasc Med. 2022;9:959146.
Iribarren C, Karter AJ, Go AS, Ferrara A, Liu JY, Sidney S, et al. Glycemic control and heart failure among adult patients with diabetes. Circulation. 2001;103:2668–73.
Kim H, Kim S, Han S, Rane PP, Fox KM, Qian Y, et al. Prevalence and incidence of atherosclerotic cardiovascular disease and its risk factors in Korea: a nationwide population-based study. BMC Public Health. 2019;19:1112.
Abdullah A, Amin FA, Stoelwinder J, Tanamas SK, Wolfe R, Barendregt J, et al. Estimating the risk of cardiovascular disease using an obese-years metric. BMJ Open. 2014;4:e005629.
Mahinrad S, Kurian S, Garner CR, Sedaghat S, Nemeth AJ, Moscufo N, et al. Cumulative blood pressure exposure during young adulthood and mobility and cognitive function in midlife. Circulation. 2020;141:712–24.
Wu S, Huang Z, Yang X, Zhou Y, Wang A, Chen L, et al. Prevalence of ideal cardiovascular health and its relationship with the 4-year cardiovascular events in a northern Chinese industrial city. Circ Cardiovasc Qual Outcomes. 2012;5:487–93.
Shi H, Cui L, Hui Y, Wu S, Li X, Shu R, et al. Enlarged perivascular spaces in relation to cumulative blood pressure exposure and cognitive impairment. Hypertension. 2023;80:2088–98.
Li X, Hui Y, Shi H, Zhao X, Li R, Chen Q, et al. Association of blood pressure with brain perfusion and structure: a population-based prospective study. Eur J Radio. 2023;165:110889.
Li Y, Ying Y, Yao T, Jia X, Liang H, Tang W, et al. Decreased water exchange rate across the blood-brain barrier in hereditary cerebral small vessel disease. Brain. 2023;146:3079–87.
Bang J, Spina S, Miller BL. Frontotemporal dementia. Lancet. 2015;386:1672–82.
Chen Q, Lv H, Wang Z, Wei X, Zhao P, Yang Z, et al. Outcomes at 6 months are related to brain structural and white matter microstructural reorganization in idiopathic tinnitus patients treated with sound therapy. Hum Brain Mapp. 2021;42:753–65.
Ma Y, Yilmaz P, Bos D, Blacker D, Viswanathan A, Ikram MA, et al. Blood pressure variation and subclinical brain disease. J Am Coll Cardiol. 2020;75:2387–99.
Yu J, Li J, Huang X. The Beijing version of the Montreal cognitive assessment as a brief screening tool for mild cognitive impairment: a community-based study. BMC Psychiatry. 2012;12:156.
Gupta D, Jyani G, Ramachandran R, Bahuguna P, Ameel M, Dahiya BB, et al. Peritoneal dialysis-first initiative in India: a cost-effectiveness analysis. Clin Kidney J. 2021;15:128–35.
Fazeli PL, Casaletto KB, Woods SP, Umlauf A, Scott JC, Moore DJ, et al. Everyday multitasking abilities in older HIV+ adults: neurobehavioral correlates and the mediating role of metacognition. Arch Clin Neuropsychol. 2017;32:917–28.
Hajjar I, Zhao P, Alsop D, Abduljalil A, Selim M, Novak P, et al. Association of blood pressure elevation and nocturnal dipping with brain atrophy, perfusion and functional measures in stroke and nonstroke individuals. Am J Hypertens. 2010;23:17–23.
den Heijer T, Launer LJ, Prins ND, van Dijk EJ, Vermeer SE, Hofman A, et al. Association between blood pressure, white matter lesions, and atrophy of the medial temporal lobe. Neurology. 2005;64:263–7.
Walker KA, Power MC, Gottesman RF. Defining the relationship between hypertension, cognitive decline, and dementia: a review. Curr Hypertens Rep. 2017;19:24.
Mandal PK, Joshi J, Saharan S. Visuospatial perception: an emerging biomarker for Alzheimer’s disease. J Alzheimers Dis. 2012;31:S117–135.
Matin N, Fisher C, Jackson WF, Diaz-Otero JM, Dorrance AM. Carotid artery stenosis in hypertensive rats impairs dilatory pathways in parenchymal arterioles. Am J Physiol Heart Circ Physiol. 2018;314:H122–H130.
Van Agtmael T, Bailey MA, Schlötzer-Schrehardt U, Craigie E, Jackson IJ, Brownstein DG, et al. Col4a1 mutation in mice causes defects in vascular function and low blood pressure associated with reduced red blood cell volume. Hum Mol Genet. 2010;19:1119–28.
Castrejón-Téllez V, Rubio-Ruiz ME, Cano-Martínez A, Pérez-Torres I, Del Valle-Mondragón L, Carreón-Torres E, et al. High sucrose ingestion during a critical period of vessel development promotes the synthetic phenotype of vascular smooth muscle cells and modifies vascular contractility, leading to hypertension in adult rats. Int J Hypertens. 2022;2022:2298329.
Fugate JE, Rabinstein AA. Posterior reversible encephalopathy syndrome: clinical and radiological manifestations, pathophysiology, and outstanding questions. Lancet Neurol. 2015;14:914–25.
Girouard H, Iadecola C. Neurovascular coupling in the normal brain and in hypertension, stroke, and Alzheimer's disease. J Appl Physiol. 2006;100:328–35.
Zlokovic BV. Neurovascular pathways to neurodegeneration in Alzheimer’s disease and other disorders. Nat Rev Neurosci. 2011;12:723–38.
Aliev G, Smith MA, Seyidov D, Neal ML, Lamb BT, Nunomura A, et al. The role of oxidative stress in the pathophysiology of cerebrovascular lesions in Alzheimer’s disease. Brain Pathol. 2002;12:21–35.
Zhang JY, Cao XX, Wen HX, Zhang HY. Correlation analysis of levels of inflammatory cytokines and nitric oxide in peripheral blood with urine proteins and renal function in patients with gestational hypertension. Exp Ther Med. 2019;17:657–62.
Haruwaka K, Ikegami A, Tachibana Y, Ohno N, Konishi H, Hashimoto A, et al. Dual microglia effects on blood-brain barrier permeability induced by systemic inflammation. Nat Commun. 2019;10:5816.
Chavan SS, Pavlov VA, Tracey KJ. Mechanisms and therapeutic relevance of neuro-immune communication. Immunity. 2017;46:927–42.
Linnerbauer M, Wheeler MA, Quintana FJ. Astrocyte crosstalk in CNS inflammation. Neuron. 2020;108:608–22.
Pandav R, Dodge HH, DeKosky ST, Ganguli M. Blood pressure and cognitive impairment in India and the United States: a cross-national epidemiological study. Arch Neurol. 2003;60:1123–8.
Koser DE, Moeendarbary E, Hanne J, Kuerten S, Franze K. CNS cell distribution and axon orientation determine local spinal cord mechanical properties. Biophys J. 2015;108:2137–47.
Komolovaitė D, Maskeliūnas R, Damaševičius R. Deep convolutional neural network-based visual stimuli classification using electroencephalography signals of healthy and Alzheimer’s disease subjects. Life. 2022;12:374.
Voytek B, Kayser AS, Badre D, Fegen D, Chang EF, Crone NE, et al. Oscillatory dynamics coordinating human frontal networks in support of goal maintenance. Nat Neurosci. 2015;18:1318–24.
Tsivgoulis G, Alexandrov AV, Wadley VG, Unverzagt FW, Go RC, Moy CS, et al. Association of higher diastolic blood pressure levels with cognitive impairment. Neurology. 2009;73:589–95.
Raichle ME. The brain’s dark energy. Sci Am. 2010;302:44–9.
Zhang D, Raichle ME. Disease and the brain’s dark energy. Nat Rev Neurol. 2010;6:15–28.
Humbert M, Montani D, Perros F, Dorfmüller P, Adnot S, Eddahibi S, et al. Endothelial cell dysfunction and cross-talk between endothelium and smooth muscle cells in pulmonary arterial hypertension. Vasc Pharmacol. 2008;49:113–38.
Singh-Bains MK, Linke V, Austria MDR, Tan AYS, Scotter EL, Mehrabi NF, et al. Altered microglia and neurovasculature in the Alzheimer’s disease cerebellum. Neurobiol Dis. 2019;132:104589.
Hollander W. Role of hypertension in atherosclerosis and cardiovascular disease. Am J Cardiol. 1976;38:786–800.
Stern JE, Sonner PM, Son SJ, Silva FC, Jackson K, Michelini LC. Exercise training normalizes the increased neuronal excitability of NTS-projecting neurons of the hypothalamic paraventricular nucleus in hypertensive rats. J Neurophysiol. 2012;107:2912–21.
Sica DA. Angiotensin-converting enzyme inhibitors side effects-physiologic and non-physiologic considerations. J Clin Hypertens. 2004;6:410–6.
Funding
National Natural Science Foundation of China 82202109. Beijing Municipal Natural Science Foundation 7232335. Beijing Scholars Program (No. [2015] 160). Beijing Key Clinical Discipline Funding (No.2021-135). Medical Science Research Program of Health Commission of Hebei Province No. 20240974. Beijing Natural Science Foundation Youth Science Fund Key Project (JR25018).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Consent Statement
All human subjects provided informed consent.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Li, X., Zhu, Z., Hui, Y. et al. Cumulative blood pressure exposure and cognition: the potential mediating role of brain volume. Hypertens Res 49, 1361–1370 (2026). https://doi.org/10.1038/s41440-025-02534-z
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41440-025-02534-z
