
Abstract
The KEYNOTE-522 regimen is the standard of care for stage II–III triple-negative breast cancer (TNBC). However, older patients were underrepresented in the pivotal trial. We evaluated the effectiveness and safety of this regimen in patients aged ≥65 years enrolled in the Neo-Real/GBECAM-0123 multicenter real-world study conducted across institutions in Brazil and Argentina. Among 724 patients, 80 (11%) were aged ≥65 years and presented distinct baseline characteristics, including lower frequencies of grade 3 tumors, Ki67 ≥ 50%, and germline BRCA1/2 mutations, alongside a higher prevalence of impaired performance status. The pathologic complete response (pCR) rate in older patients was 54.9% in comparison with 64.5% in younger patients, although age was not independently associated with pCR in multivariable analysis, including other relevant baseline variables. Older patients experienced a significantly higher toxicity burden, with increased rates of treatment discontinuation, dose reductions, treatment delays, hospitalizations, and grade ≥3 neutropenia. Taken together, these data indicate that older patients with TNBC harbor distinct biological and clinical features with numerically lower pCR rates, and that the increased toxicity burden underscores the need for personalized treatment strategies and dedicated research in this population.
Similar content being viewed by others

Introduction
Triple-negative breast cancer (TNBC) accounts for approximately 15–20% of all breast cancer cases and is known for its aggressive clinical behavior and unfavorable prognosis, typically affecting younger women1. Nevertheless, TNBC also occurs in older patients, with studies reporting that 16–22% of TNBC occurs in patients over 65 years2,3,4,5. Although tumors in older TNBC patients may display less aggressive pathological features, outcomes remain inferior compared to younger cohorts, with higher early mortality and worse long-term survival—even after adjusting for stage and other clinicopathological factors5,6,7.
Older patients are a heterogeneous population often burdened by comorbidities, functional limitations, cognitive impairment, polypharmacy, nutritional deficiencies, psychological distress, and social vulnerability. These factors can significantly affect treatment decisions, adherence, efficacy, and tolerability. Importantly, chronological age alone is a poor surrogate for functional status and treatment fitness. Geriatric assessments are essential for tailoring treatment strategies, especially when quality of life considerations may outweigh survival benefits8. Despite their growing numbers, older adults remain markedly underrepresented in clinical trials and are less frequently offered guideline-concordant care9,10. This pattern of management—driven by concerns about frailty, toxicity, or clinician bias—may contribute to considerable variability in care delivery.
The KEYNOTE-522 (KN522) phase III trial was a landmark study that established the combination of neoadjuvant pembrolizumab with an anthracycline- and taxane-based chemotherapy backbone, followed by adjuvant pembrolizumab, as the standard of care for patients with stage II–III TNBC. The addition of pembrolizumab significantly improved the pathologic complete response rate (pCR) (64.8% vs. 51.2%; p < 0.001), and this benefit was translated into superior long-term outcomes, with a 5-year event-free survival of 81.3% vs. 72.3% (hazard ratio [HR] 0.63; 95% CI, 0.49–0.81) and a 5-year overall survival of 86.6% vs. 81.7% (HR 0.66; 95% CI, 0.50–0.87; p = 0.002). However, only 11% of participants were aged ≥65, limiting the generalizability of these results to older, potentially frailer individuals. Moreover, given the regimen’s intensity, older adults may be at increased risk for adverse events and treatment modifications, which may compromise treatment completion and outcomes11,12,13.
To address this scientific gap, we analyzed data from the Neo-Real/GBECAM-0123 study, a multicenter real-world initiative designed to evaluate the safety and effectiveness of the KN522 regimen in patients with high-risk early-stage TNBC14. This analysis specifically aims to compare clinical outcomes and toxicity profiles between patients aged ≥65 years and those younger than 65, providing much-needed insight into the applicability of the KN522 regimen in older adults.
Results
Patients’ characteristics
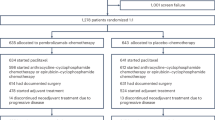
A total of 724 patients were included, of whom 80 (11%) were aged ≥65 years. Compared with younger patients, those aged ≥65 years were less likely to present with grade 3 tumors (60.8% vs. 76.8%, p = 0.004) and high Ki-67 expression (55.3% vs. 76.9%, p < 0.001). They were also more frequently classified with an ECOG performance status ≥1 (27.1% vs. 4.9%, p < 0.001), less frequently carried a BRCA mutation (5.0% vs. 15.5%, p = 0.010), and more frequently omitted anthracycline (0.95% vs. 6.58%, p = 0.003). No significant differences were observed in tumor-infiltrating lymphocytes, clinical stage, or the use of dose-dense AC scheduling (Table 1).
Among the 80 patients aged ≥65 years, 55 were aged 65–75 years, and 25 were older than 75 years. Across baseline and treatment characteristics, the only statistically significant difference between patients aged 65–75 years and those older than 75 years was a lower utilization of dose-dense AC in the >75-year subgroup (p = 0.019; Supplementary Table 1). Anthracycline omission was rare in both age subgroups, with 50 of 53 patients (94.3%) aged 65–75 years and 21 of 23 patients (91.3%) older than 75 years receiving an anthracycline (p = 0.635).
Pathologic complete response
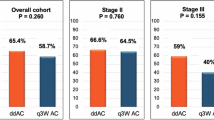
A pCR, defined as ypT0/is ypN0, was achieved in 423 of 666 patients (63.5%). The pCR rate was numerically lower but not statistically different in patients aged ≥65 years compared with those <65 years (54.9% [39/71] vs. 64.5% [384/595]; OR 0.67, 95% CI 0.41–1.10, p = 0.114). Similarly, among evaluable patients aged ≥65 years, no significant difference in pCR was observed between those aged 65–75 years (27/44, 61.4%) and those older than 75 years (9/17, 52.9%; p = 0.574).
In a multivariable analysis including age, histological subtype, tumor grade, Ki-67 index, BRCA status, clinical stage, and AC schedule, age ≥65 years was not independently associated with pCR (OR 1.17, 95% CI 0.65–2.13, p = 0.588). Independent predictors of higher pCR in the whole cohort included BRCA mutation (OR 1.81, 95% CI 1.05–3.11, p = 0.031) and high proliferative index (Ki-67 ≥ 50%; OR 2.10, 95% CI 1.36–3.24, p = 0.001). Conversely, stage III disease (OR 0.50, 95% CI 0.33–0.75, p = 0.001), non–NST histology (OR 0.46, 95% CI 0.22–0.96, p = 0.040), and less than 6 cycles of neoadjuvant pembrolizumab (OR 0.54, 95% CI 0.36–0.82) were associated with significantly lower odds of achieving pCR (Table 2).
Safety
Older patients experienced significantly higher rates of treatment modifications and toxicities (Table 3). Drug discontinuation was more frequent among patients ≥65 years (35.5% vs. 21.8%, p = 0.025), particularly for anthracyclines (16.3% vs. 3.9%, p < 0.001). Dose reductions were also more common in this group (24.1% vs. 11.6%, p = 0.012), especially for carboplatin (10.0% vs. 1.7%, p < 0.001). Treatment delays occurred in 42.1% of older patients compared with 23.2% in younger patients (p = 0.003). Hospitalizations due to adverse events (35.9% vs. 18.1%, p = 0.005) and antibiotic use (43.9% vs. 25.3%, p = 0.004) were also significantly more frequent in older patients, with a large proportion of older patients requiring hospitalization and antibiotic use during neoadjuvant treatment. Regarding grade ≥3 adverse events, neutropenia was more common in older patients (22.5% vs. 12.1%, p = 0.014), and fatigue was also increased (5.0% vs. 1.1%, p = 0.025). (Fig. 1). In line with these safety results, a higher proportion of older patients received less than 6 cycles of neoadjuvant pembrolizumab (36.8% vs 15%, p < 0.001). No statistically significant differences were observed between patients aged 65–75 years and those older than 75 years with respect to adverse events, treatment discontinuation, dose reductions, treatment delays, hospitalizations, or antibiotic use. (Supplementary Tables 2 and 3).

Grade ≥ 3 adverse events by age group.
Discussion
In this real-world multicenter analysis of patients with early-stage TNBC treated with the KN522 regimen, we found that older adults (≥65 years) experienced comparable efficacy but significantly higher rates of treatment-related toxicities and treatment modifications compared with younger counterparts. Although the pCR rate was numerically lower in older patients, age itself was not an independent predictor of response after adjustment for tumor biology and treatment variables. Indeed, older patients differed from the younger group in relevant baseline characteristics.
Prior evidence suggests that older adults with TNBC have poorer outcomes despite potentially less aggressive histological features.5,6,7 Moreover, some analysis found that younger age was an independent predictor of pCR for those who received neoadjuvant chemotherapy without immunotherapy15,16 Although subset data based on age was not reported in the majority of randomized trials evaluating the addition of neoadjuvant immunotherapy to chemotherapy17, a single-institution retrospective analysis found an association between younger age and higher pCR rates in an univariate analysis (p = 0.04), suggesting that age may still play a role in response, potentially reflecting tumor biology18.
Several real-world cohorts have reported overall pCR rates, treatment feasibility, and patterns of adverse events associated with pembrolizumab-based neoadjuvant therapy in early-stage TNBC. However, they consistently present aggregate outcomes and do not provide efficacy or safety data stratified by age group14,19,20,21. Notably, an abstract-level analysis specifically evaluated patients aged ≥65 years in comparison with younger patients treated with neoadjuvant chemo-immunotherapy versus chemotherapy alone. In that analysis, pCR rates did not differ significantly between older and younger patients (49% vs 58%, p = 0.20). With respect to safety, the only toxicity-related statement indicated no significant increase in immune-related adverse events or difference in treatment completion rates among older patients receiving immunotherapy22. Given that these data were reported at an abstract level, without detailed toxicity grading, treatment-modification metrics, or denominators, robust interpretation and cross-study comparison remain limited.
In our cohort, older adults experienced substantially higher toxicity, highlighting the challenges of delivering intensive chemoimmunotherapy to this population. These results are consistent with a prior retrospective study of neoadjuvant chemotherapy (without immunotherapy) in older breast cancer patients, which reported increased rates of dose reductions and early treatment discontinuation in the geriatric cohort23,24. In the KN522 trial, the overall treatment discontinuation rate was 23.3%, and although age-specific safety data were not reported, older adults are generally more prone to treatment interruptions due to comorbidities and toxicity11,12,13. Consistent with this expectation, our real-world cohort showed an even higher discontinuation rate among older patients, reaching 35.5%.
From a clinical perspective, our findings support a more personalized approach to treating older patients with high-risk early TNBC. Despite achieving comparable pCR rates, this subgroup experienced higher toxicity and more frequent treatment modifications. This raises an important clinical question: could a less intensive or modified regimen provide similar efficacy in appropriately selected older patients? While some fit older adults may tolerate and benefit from standard chemoimmunotherapy, others may require tailored dose adjustments or de-escalated strategies to balance efficacy, safety, and quality of life. Incorporating geriatric assessment into routine care is essential to better define treatment fitness, as chronological age alone is an inadequate surrogate for physiologic reserve25,26,27. In clinical practice, treatment intensity must therefore be carefully balanced, while in the research setting, exploring optimized, less toxic regimens represents a rational path forward.
Given these safety concerns, de-escalation strategies have been actively explored in early TNBC, regardless of age. The NeoPACT phase II trial evaluated pembrolizumab in combination with carboplatin and docetaxel, an anthracycline-free regimen, and reported a pCR rate of 58%28. This regimen is being further investigated in the ongoing SCARLET phase III trial (NCT05632939), which directly compares it to the KN522 chemotherapy backbone. Similarly, the NeoImmunoBoost (AGO-B-041) phase II trial investigated pembrolizumab with nab-paclitaxel followed by epirubicin/cyclophosphamide, omitting platinum, and achieved a pCR rate of 60.6% in the intention-to-treat population29. A chemotherapy-free strategy was explored in the BELINI trial: in Cohort C, nivolumab plus low-dose ipilimumab for 6 weeks in TIL-high tumors, defined as ≥50%, was associated with a 33% pCR, while in Cohort D, nivolumab plus relatlimab (anti-LAG antibody) for 8 weeks, led to a pCR rate of 47%, providing proof of concept for chemo-free immunotherapy regimens30,31. While these regimens are supported by phase II data, randomized validation is pending, and the current standard of care remains the anthracycline-, taxane- and platinum-containing backbone32,33. Other ongoing trials, such as OPTImaL (NCT06476119), ETNA (NCT06078384), and DespaTIL (NCT07074106), are evaluating biomarker-driven treatment de-escalation strategies, with TILs emerging as a promising biomarker for this purpose. Given the toxicity profile reported here, the evaluation of these de-escalation strategies in the older patients is highly warranted.
The limitations of this study reflect the inherent challenges of collecting real-world data across multiple institutions, including variability in data availability and the retrospective nature of the analysis. In this context, selection bias may influence both treatment decisions and outcomes, particularly given that the initiation of the KN522 regimen was based on physician discretion. Moreover, important geriatric-specific metrics—such as frailty, comorbidities, and cognitive reserve—were not systematically captured; there was a modest number of older individuals, and patient-reported outcomes were not included, limiting a more comprehensive assessment of treatment fitness and tolerability. Despite these limitations, the multicenter design and use of standardized data collection methods enhance the generalizability of our findings.
Overall, our findings indicate that older patients with TNBC treated with the KN522 regimen exhibited distinct tumor biology and numerically lower pCR rates compared with younger counterparts, without a statistically significant difference, while experiencing substantially higher toxicity and treatment modifications. These findings highlight the need for individualized treatment strategies in older adults. Future prospective studies specifically focused on older patients are essential to validate de-intensified approaches and to develop geriatric-adapted treatment protocols that balance efficacy, safety, and quality of life in this underrepresented and vulnerable population.
Methods
Study design and population
NEOREAL/GBECAM-0123 is a retrospective, multicenter, real-world study conducted across fourteen Brazilian cancer centers, plus centers from Argentina associated with SUMA (Argentine group of studies in breast cancer). Eligible patients included in the present analysis had TNBC and received at least one cycle of neoadjuvant pembrolizumab plus chemotherapy between July 2020 and July 2024. Patients with estrogen/ progesterone low expression (ER-low), defined as those with expression lower than 10%, could also be included. The choice to initiate the KN522 regimen was made at the discretion of the treating physician.
Endpoints and data collection
The objective of this analysis was to evaluate the effectiveness and safety of the KN522 regimen in patients aged ≥65 years compared to those younger than 65 years. The primary effectiveness endpoint was pCR (ypT0/is ypN0). Safety outcomes included the incidence of grade ≥3 adverse events, treatment discontinuation due to adverse events, dose reductions, treatment delays, hospitalizations, and use of antibiotics. Subgroup analyses were conducted among older patients aged 65–75 years and >75 years.
Clinical data were retrospectively extracted from electronic medical records and entered into a centralized REDCap database. Toxicities were graded according to the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0.
The study was conducted under the auspices of the GBECAM (Grupo Brasileiro de Estudos em Câncer de Mama) and was approved by the Institutional Review Boards of all participating centers. In Brazil, approval was obtained under protocol number 67950623.0.1001.0068 and included the following institutions: Instituto D’Or de Pesquisa e Ensino, A.C.Camargo Cancer Center, Hospital Moinhos de Vento, Hospital Sírio-Libanês, Hospital Beneficência Portuguesa, Hospital 9 de Julho, Hospital Santa Paula, Clínica AMO, Instituto do Câncer do Ceará, Brasília Hospital, Centro Integrado de Pesquisa da Amazônia, Hospital São Domingos, Hospital Samaritano, and Instituto Américas. In Argentina, approval was granted by the CEMIC Institutional Review Board under protocol number 12805. All procedures complied with the ethical principles outlined in the Declaration of Helsinki. Written informed consent was obtained from participants who could be contacted, while the ethics committees granted a waiver of consent for deceased or unreachable patients, as only anonymized data were analyzed. Data collection and analysis were performed by the Research Unit of Instituto D’Or de Pesquisa e Ensino (São Paulo, Brazil). The manuscript was drafted by the first and senior authors without medical writing assistance from industry, and all co-authors reviewed and approved the final version, confirming the integrity and accuracy of the data.
Statistical analysis
Baseline characteristics were summarized using descriptive statistics. Continuous variables were reported as medians with ranges, and categorical variables as absolute and relative frequencies. Statistical comparisons of categorical variables were performed using Fisher’s exact test. Student’s t-test and the Mann–Whitney U test were used for normally and non-normally distributed continuous variables, respectively. Univariate and multivariable logistic regression analysis were conducted to identify predictors of pCR. Statistical significance was defined as a p-value < 0.05. All analyses were performed using Stata version 15.1 (StataCorp, College Station, TX, USA).
Declaration statements
Partial results of this study were presented as a poster at the 2025 ASCO Annual Meeting (DOI: 10.1200/JCO.2025.43.16_suppl.609). This study did not receive funding.
Data availability
The datasets generated and/or analyzed during the current study are not publicly available in order to protect patient privacy, but are available from the corresponding author on reasonable request. Data analysis methods have been described thoroughly in the Methods section.
References
Siegel, R. L., Miller, K. D. & Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 70, 7–30 (2020).
Syed, B. M. et al. Biological characteristics and clinical outcome of triple-negative primary breast cancer in older women—comparison with their younger counterparts. PLoS ONE 9, e100573 (2014).
Königsberg, R. et al. Tumor characteristics and recurrence patterns in triple-negative breast cancer: a comparison between younger (<65) and elderly (≥65) patients. Eur. J. Cancer 48, 2962–2968 (2012).
Carvalho, F. M., Bacchi, L. M., Santos, P. P. & Bacchi, C. E. Triple-negative breast carcinomas are a heterogeneous entity that differs between young and old patients. Clinics 65, 1033–1036 (2010).
Zhu, W. et al. Age-related disparity in immediate prognosis of patients with triple-negative breast cancer: a population-based study from SEER cancer registries. PLoS ONE 10, e0128345 (2015).
Tzikas, A. K., Nemes, S. & Linderholm, B. K. Comparison between young and old patients with triple-negative breast cancer: biology, survival and metastatic patterns. Breast Cancer Res. Treat. 182, 643–654 (2020).
Vihervuori, H. et al. Varying outcomes of triple-negative breast cancer in different age groups: prognostic value of clinical features and proliferation. Breast Cancer Res. Treat. 196, 471–482 (2022).
Soto-Perez-de-Celis, E. et al. Functional versus chronological age: geriatric assessments to guide decision making in older patients with cancer. Lancet Oncol. 19, e305–e316 (2018).
Li, N. H. Y. & Li, C. I. Incidence-rate trends of breast cancer overall and by molecular subtype by race, ethnicity and age. JAMA Netw. Open 8, e2456142 (2025).
Derks, M. G. M. et al. Variation in treatment and survival of older patients with non-metastatic breast cancer in five European countries: a population-based cohort study from the EURECCA Breast Cancer Group. Br. J. Cancer 119, 121–129 (2018).
Schmid, P. et al. Event-free survival with pembrolizumab in early triple-negative breast cancer. N. Engl. J. Med. 386, 556–567 (2022).
Schmid, P. et al. Neoadjuvant pembrolizumab or placebo plus chemotherapy followed by adjuvant pembrolizumab or placebo for early-stage triple-negative breast cancer: updated event-free survival results from the phase 3 KEYNOTE-522 study. Abstract LBO1-01. Cancer Res. 84, LBO1–01 (2024).
Schmid, P. et al. Overall survival with pembrolizumab in early-stage triple-negative breast cancer. N. Engl. J. Med. 391, 1981–1991 (2024).
Bonadio, R. C. et al. Dose-dense versus 3-weekly AC during neoadjuvant chemoimmunotherapy for triple-negative breast cancer. npj Breast Cancer 10, 73 (2024).
Loibl, S. et al. Outcome after neoadjuvant chemotherapy in young breast cancer patients: a pooled analysis of individual patient data from eight prospectively randomized controlled trials. Breast Cancer Res. Treat. 152, 377–387 (2015).
Chou, H.-H. et al. Impact of age on pathological complete response and locoregional recurrence in locally advanced breast cancer after neoadjuvant chemotherapy. Biomed. J. 42, 66–74 (2019).
Roy, A. M. et al. Predictors of complete pathological response with chemoimmunotherapy in triple-negative breast cancer: a meta-analysis. Oncology 101, 1–14 (2023).
Perry, L. M. et al. Predictors of pathologic complete response with neoadjuvant chemo-immunotherapy in early-stage triple-negative breast cancer. Ann. Surg. Oncol. 32, 3991–4001 (2025).
Park, W. K. et al. Real-world evidence of the efficacy of neoadjuvant pembrolizumab in triple-negative breast cancer: a surgeon’s point of view. Eur. J. Surg. Oncol. 51, 110011 (2025).
Karci, E. et al. Neoadjuvant pembrolizumab plus chemotherapy in early-stage triple-negative breast cancer: a nationwide retrospective Turkish Oncology Group study. Cancers 16, 3389 (2024).
Andrade, M. O. et al. Immune-related adverse events among patients with early-stage triple-negative breast cancer treated with pembrolizumab plus chemotherapy: real-world data from the Neo-REAL/GBECAM-0123 study. Breast 83, 104473 (2025).
Polidorio, N. et al. Outcomes in elderly patients with triple-negative breast cancer receiving neoadjuvant chemo-immunotherapy and chemotherapy alone. Abstract P5-11-16. Clin. Cancer Res. 31, P5-11-16 (2025).
Brown, L. et al. Tolerance and outcomes of neoadjuvant chemotherapy in geriatric breast cancer patients. J. Surg. Res. 283, 329–335 (2023).
Yildirim, E. C. et al. Achieving treatment goals in older breast cancer patients receiving neoadjuvant chemotherapy. Sci. Rep. 15, 9866 (2025).
Hurria, A. et al. Predicting chemotherapy toxicity in older adults with cancer: a prospective multicenter study. J. Clin. Oncol. 29, 3457–3465 (2011).
Extermann, M. et al. Predicting the risk of chemotherapy toxicity in older patients: the CRASH score. J. Clin. Oncol. 30, 3378–3384 (2012).
Wildiers, H. et al. International Society of Geriatric Oncology consensus on comprehensive geriatric assessment in older patients with cancer. J. Clin. Oncol. 32, 2595–2603 (2014).
Sharma, P. et al. Clinical and biomarker findings of neoadjuvant pembrolizumab and carboplatin plus docetaxel in triple-negative breast cancer: NeoPACT phase 2 clinical trial. JAMA Oncol. 10, 227–235 (2024).
Schneeweiss, A. et al. Neoadjuvant nab-paclitaxel and epirubicin/cyclophosphamide with pembrolizumab for early triple-negative breast cancer: neoImmunoBoost trial. Ann. Oncol. 34, 511–519 (2023).
Nederlof, I. et al. Neoadjuvant nivolumab or nivolumab plus ipilimumab in early-stage triple-negative breast cancer: a phase 2 adaptive trial. Nat. Med. 30, 3223–3235 (2024).
Nederlof, I. et al. Neoadjuvant nivolumab/relatlimab or nivolumab/ipilimumab in triple-negative breast cancer with high tumour-infiltrating lymphocytes. Abstract LBA11. Ann. Oncol. 35, S1206 (2024).
Gradishar, W. J. et al. Breast cancer, version 3.2024: NCCN clinical practice guidelines in oncology. J. Natl. Compr. Canc. Netw. 22, 331–357 (2024).
Loibl, S. et al. Early breast cancer: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Ann. Oncol. 35, 159–182 (2024).
Acknowledgements
None.
Author information
Authors and Affiliations
Contributions
Study concept and design: M.C.G., R.B.-S., L.T., M.C.T., C.H.A., D.M.G., M.L.B., D.A.-S., D.D.R., J.B., B.M.Z., A.F., P.M.H., and R.C.B. Data collection, analysis, and interpretation: M.C.G., R.B.-S., L.L., L.T., M.C.T., F.C.B., C.H.A., D.M.G., M.L.B., G.C., D.A.-S., D.D.R., N.J.B.G., N.C.C.N., I.M.S., M.O.A., F.M., J.B., M.S., R.D.P.F., C.L.S., M.T., M.R.M., Z.S.S., A.M.U.G., B.M.Z., A.F., M.M.F.M., P.A.S., S.S., P.M.H., C.P., M.D.P.E.-D., and R.C.B. Manuscript drafting and critical revision: M.C.G., R.B.-S., L.L., L.T., M.C.T., F.C.B., C.H.A., D.M.G., M.L.B., G.C., D.A.-S., D.D.R., N.J.B.G., N.C.C.N., I.M.S., M.O.A., F.M., J.B., M.S., R.D.P.F., C.L.S., M.T., M.R.M., Z.S.S., A.M.U.G., B.M.Z., A.F., M.M.F.M., P.A.S., S.S., P.M.H., C.P., M.D.P.E.-D., and R.C.B. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
M.C.G.: Speaker fees and/or honoraria for consulting or advisory functions: Novartis, Knight Therapeutics, AstraZeneca, AbbVie, Daiichi-Sankyo, and GSK. Financial support for educational programs and symposia: AstraZeneca, AbbVie, Pfizer, and GSK. R.B.-S.: Speaker fees and/or honoraria for consulting or advisory functions: AstraZeneca, Daiichi-Sankyo, Eli Lilly, Gilead, Libbs, Pfizer, Novartis, MSD, and Roche. Financial support for educational programs and symposia: AstraZeneca, Daiichi-Sankyo, Gilead, Eli Lilly, and MSD. Institutional research grant: AstraZeneca, Daiichi-Sankyo. L.L.: Speaker fees and/or honoraria for consulting or advisory functions: Adium. Travel grants: MSD, Gador. L.T.: Speaker fees and/or honoraria for consulting or advisory functions: Daiichi-Sankyo, MSD, AstraZeneca, Pfizer, Lilly, and Novartis. Financial support for educational programs and symposia: AstraZeneca, Roche, and Gilead. Institutional research grant: Novartis. M.C.T.: Declares no conflict of interest. F.C.B.: Declares no conflict of interest. C.H.A.: Speaker fees and/or honoraria for consulting or advisory functions: Daiichi-Sankyo, Gilead, AstraZeneca, Novartis, and MSD. Financial support for educational programs and symposia: AstraZeneca, Daiichi-Sankyo, MSD, Lilly, Roche, Novartis, Gilead, and Medscape. D.M.G.: Speaker fees and/or honoraria for consulting or advisory functions: Daiichi-Sankyo, Teva, Roche, AstraZeneca, Pfizer, Lilly, and Novartis. Financial support for educational programs and symposia: AstraZeneca, Libbs, and Roche. Research grant: Novartis. M.L.B.: Speaker fees and/or honoraria for consulting or advisory functions: Daiichi Sankyo, Roche, Pfizer, Novartis, Lilly, AstraZeneca. G.C.: Speaker fees and/or honoraria for consulting or advisory functions: Amgen, AstraZeneca. Travel grants: Roche. D.A.-S.: Speaker fees and/or honoraria for consulting or advisory functions: Daiichi-Sankyo. Financial support for educational programs and symposia: AstraZeneca. D.D.R.: Speaker fees and/or honoraria for consulting or advisory functions: AstraZeneca, Daiichi-Sankyo, Lilly, Libbs, Pfizer, Novartis, Roche, GSK, Sanofi, Amgen, and Zodiac Pharma. Financial support for educational programs and symposia: Roche. N.J.B.G.: Participation in courses, symposia, lectures, and advisory boards for AstraZeneca, Daiichi-Sankyo, Gilead, Novartis, and Lilly. Declares no participation in sponsored clinical trials or continuous contracts/stock ownership in pharmaceutical companies. N.C.C.N.: Speaker fees and/or honoraria for consulting or advisory functions: AstraZeneca, Daiichi-Sankyo, Roche, Pfizer, Lilly, Novartis, and MSD. I.M.S.: Declares no conflict of interest. M.O.A.: Declares no conflict of interest. F.M.: Declares no conflict of interest. R.D.P.F.: Declares no conflict of interest. C.L.S.: Declares no conflict of interest. M.S.: Speaker fees and/or honoraria for consulting or advisory functions: Adium, GSK. Travel grants: Roche, AstraZeneca, MSD. M.R.M.: Speaker fees and/or honoraria for consulting or advisory functions: AstraZeneca, Daiichi-Sankyo, Pfizer, Novartis, Roche, MSD, and Knight. Financial support for educational programs and symposia: MSD, AstraZeneca, Knight, and Novartis. Z.S.S.: Declares no conflict of interest. A.M.U.G.: Declares no conflict of interest. B.M.Z.: Speaker fees and/or honoraria for consulting or advisory functions: AstraZeneca, Daiichi-Sankyo, Eli Lilly, Gilead, Pfizer, Novartis, MSD, Roche, and Adium. A.F.: Speaker fees and/or honoraria for consulting or advisory functions: Daiichi-Sankyo, Novartis, Gilead, MSD, BMS, AstraZeneca, and Pfizer. Financial support for educational programs and symposia: AstraZeneca, Daiichi-Sankyo, MSD, and Novartis. M.M.F.M.: Speaker fees and/or honoraria for consulting or advisory functions: AstraZeneca, Daiichi-Sankyo, Eli Lilly, Gilead, Adium, Novartis, MSD, and Roche. Financial support for educational programs and symposia: AstraZeneca, Daiichi-Sankyo, Gilead, Eli Lilly, Roche, MSD, and Novartis. P.A.S.: Speaker fees and/or honoraria for consulting or advisory functions: AstraZeneca, Eli Lilly, Pfizer, Novartis, Johnson & Johnson, Takeda, and Adium. S.S.: Declares no conflict of interest. P.M.H.: Speaker fees and/or honoraria for consulting or advisory functions: Daiichi-Sankyo. C.P.: Speaker fees and/or honoraria for consulting or advisory functions: Knight. Travel grants: AstraZeneca, Gador, Novartis, Pfizer, Raffo, and Roche. M.D.P.E.-D.: Declares no conflict of interest. R.C.B.: Speaker fees and/or honoraria for consulting or advisory functions: Daiichi-Sankyo, Nestlé Health Science, Adium, Gilead, MSD, BMS, AstraZeneca, Aché, Pfizer, Roche, Libbs, Lilly, Novartis, and GSK. Financial support for educational programs and symposia: AstraZeneca, Daiichi-Sankyo, and MSD. Institutional research grants: Novartis and AstraZeneca.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Gouveia, M.C., Barroso-Sousa, R., Lapuchesky, L. et al. Neoadjuvant pembrolizumab plus chemotherapy in older patients with early-stage triple-negative breast cancer: real-world insights from neo-real/GBECAM-0123. npj Breast Cancer 12, 55 (2026). https://doi.org/10.1038/s41523-026-00919-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41523-026-00919-y
