
Abstract
Contemporary plans to establish human habitation on the Earth’s Moon have increased interest in the ability of humans to establish extraterrestrial pregnancies. There is a lack of data to identify if humans could safely reproduce away from the Earth, and even less guidance with regard to whether we should attempt to do so. This work was developed to stimulate investigation into the likely biological and ethical challenges facing the establishment and maintenance of a healthy human extraterrestrial pregnancy.
Similar content being viewed by others


Introduction
Whether or not humans can establish and maintain a successful pregnancy away from the Earth’s protective environment remains largely unknown. In engaging in this discussion, it is important to note that there is a lack of direct data on human reproduction in space, necessitating informed and careful extrapolation of potential effects from simulated and directly relevant (i.e. terrestrial radiation and/or stress exposures) data. Key challenges in extrapolating these data relate to applying in vitro data (which lack the complexity of in vivo tissue architecture and multi-system signaling inputs) and animal data (generally rodents, which have very short gestations and a distinct pattern of fetal development relative to the human) to human pregnancy. Moreover, much of the available data derive from single input (i.e. microgravity only) simulations, whereas a real lunar or Mars exposure (for example) would involve a fluid combination of microgravity, radiation, stress and potentially regolith exposures. To this end, innovations such as the NASA ground-based Galactic Cosmic Ray Simulator1, and studies investigating combined effects of key exposures (i.e. radiation, microgravity), such as that by Todd and colleagues, are of particular importance2. Similarly, there is a lack of discussion regarding the ethical implications of extraterrestrial pregnancy. Addressing these ethical considerations is important given immediate space exploration plans, as well as longer term questions regarding the ability of humans to explore and colonize planets at great distances from Earth.
Announcements from several governmental and private space organizations have conveyed an intention to return astronauts to the Earth’s Moon. The 2017 NASA Artemis Program, in particular, aims to establish a long-term presence on the Earth’s Moon as a precursor to human missions to Mars3. Although relatively short-term periods of habitation on the Earth’s Moon are conceivable (i.e. similar in duration to those of the International Space Station missions), the distances, transit radiation doses, and limited opportunities for travel to Mars will likely necessitate extended stays4. It is not unreasonable to predict that an extended or even permanent human presence on Mars will eventually result in extraterrestrial pregnancy—planned or otherwise. From a longer-term perspective, the ability of humans to live at great distances from the Earth will likely be determined by our capacity to reproduce away from its protective atmosphere and familiar environment.
Spaceflight exerts a sizable and generally negative physiological and functional challenge to healthy adult humans, with impacts reported on a majority of systems analysed5. Other than for a small number of historical lunar missions wherein astronauts have been exposed to both greatly reduced gravity (e.g. 0.16 G on the lunar surface) and greatly increased radiation once outside the Earth’s geomagnetosphere, spaceflight exposures assessed to date are a composite of low earth orbit microgravity (e.g. 0.89 G at the International Space Station but effectively 0 G due to orbital free fall) and more modest radiation exposures, interacting with physical and psychological stress, circadian rhythm disruption, and the transient effects of hypergravity during launch and re-entry procedures. Due to difficulties in isolating individual exposures in space, along with the cost and inconvenience of space access, investigators have used parabolic flights6, sounding rockets7 or ground-based simulators (i.e. random positioning machines8, clinostats9 or limb suspensions)10 to model microgravity effects. The use of ground-based microgravity simulators such as random positioning machines also has the advantage of allowing investigators to modify simulated microgravity as a continuous variable. Centrifuge studies have been employed to model transient hypergravity, demonstrating intrauterine growth and development impacts in rats11. As might be expected, each of the above microgravity and hypergravity simulations convey their own set of advantages and constraints which are important to consider when assessing data from these models.
We will begin by introducing four key potential space exposures (microgravity, cosmic radiation, regolith exposure, social stress) that individually and in combination have the potential to impact the viability of a human pregnancy. We will additionally highlight potential exposure effects on the human reproductive system, the fetal skeleton and central nervous system. Given the data available, much of this discussion will be framed around findings from cellular and in vitro studies, and in ground-based simulations. An overview of biological effects dealt with is provided in Fig. 1. Having introduced a cross-section of potential biological risks to extraterrestrial pregnancy we will then move to discussing the merits of off-world pregnancy through an ethical lens.

Space exposures with the potential to impact human pregnancy viability and development.
Space exposures
Microgravity
Gravity is a fundamental attractive force that acts on matter. Weight is a function of local gravitational force (which according to the work of Newton is itself a function of the gravitational constant (G; 6.67 × 10−11 m3 kg−1 s−2) multiplied by the product of the masses of two attracting objects (m1, m2) divided by the square of their separating distance (R); thus F = G(m1 * m2/R2). Thus, weight, measured in Newtons = mass (in kg) x gravity (m/s2). On the Earth’s surface, gravity has an accelerative downwards force of ~9.8 m/s2. Thus, an object with a mass of 1 kg on the Earth’s surface has a weight of 9.8 Newtons. Microgravity is used synonymously with reference to relative or absolute weightlessness, referring to a state in which the apparent force of gravity on mass is less than that experienced at the Earth’s surface, which is annotated as 1.0 G12. Accordingly, an object with a mass of 1 kg on the surface of the Earth’s moon exposed to a gravitational force of 1.62 m/s2 (or ~0.16 G) has a weight of 1.62 Newtons. Objects undergoing orbital freefall in the absence of an atmosphere experience apparent weightlessness or microgravity, which is why microgravity aboard the International Space Station is ~10-6 G despite being exposed to downward acceleration of 0.89 G from the Earth’s gravitational field.
Living organisms have evolved on Earth under the influence of a constant gravitational force of 9.8 m/s2. Unsurprisingly, gravity unloading, or microgravity, exerts a wide range of effects on living systems. Precisely how different cell populations, and the tissues they in turn comprise, respond to microgravity remains to be established, with both mechanical and chemical inputs likely responsible for observed adaptations. Irrespective, there is a sizable amount of experimental evidence to show that exposure to microgravity rapidly induces large transcriptional changes in cells, with alterations in cytoskeletal structure and function proposed to play an important role in these observed microgravity effects.
Given its importance to early embryo formation processes13, it is not unreasonable to speculate that microgravity-induced cytoskeletal disruption may play a role in determining the success of mammalian pregnancy off-world. Accordingly, the cytoskeleton serves as a useful example of how microgravity might impact a system critical to human reproduction. It is important to note that the effect of microgravity exposure on the cytoskeleton is just one example of how a fundamental cellular system important for embryogenesis and normal tissue homeostasis can be impacted by space travel exposures. Similar overviews could be provided for a range of key processes including DNA replication, extracellular matrix formation, immune regulation, and protein production, each of which are essential to various stages of normal pregnancy.
The human cell cytoskeleton is comprised of three classes of structures: the actin network, the microtubule network, and the intermediate filament network. As reviewed by Fletcher and Mullins, the key differences in these polymer networks include their stiffness, assembly dynamics, polarity, and their associated molecular motors14. It is also important to note that there is sizable heterogeneity in the composition of these networks between cell types and at different stages of differentiation.
Microgravity has been reported to exert rapid disruptive changes on the cytoskeleton and although cytoskeletal reorganization has been shown to occur around 20–72 h post gravity unloading, the adaptive organization of these networks may be abnormal relative to 1.0 G conditions15. However, effects may be cell specific, as analyses of actin and vimentin networks in primary human macrophages had no quantitative or structural changes after 11 days of low Earth orbit on the International Space Station16. Human capillary endothelial cells cultured under space flight conditions had reduced motility, fewer actin fibers and disrupted distribution of microtubules and intermediate filaments17. Human vascular (umbilical vein) endothelial cells cultured on a random positioning machine platform (simulated microgravity) reported alterations in morphology (rounding), reduced cell stiffness in association with a reduction in the amount of cytoskeletal proteins present in cell lysates and actin and microtubule disorganization18. Similar findings have been shown in human umbilical cord mesenchymal cells cultured under simulated microgravity, showing reduced growth in association with downregulation of beta actin and alpha tubulin19.
From an embryogenesis perspective, the cytoskeleton is of increasing interest in terms of its mechanosensing and signal transduction role in directing early morula growth through to formation of the gastrula20. As reviewed by Piszker and Simunovic, keratin abundance may play a role in trophoectoderm programming in combination with filamentous actin. Similarly, reorganisation of lamin A localisation (in particular, enrichment of lamin A at the nuclear lamina) may influence cell bifurication at the two to eight cell stage. Contraction of the actin-myosin network is also proposed to play a role in generating hydraulic pressure involved in directing cavity formation in the blastocyst20. It remains to be understood to what extent these processes would be impacted by microgravity. Moreover, whether the gravitational forces exerted on cells are a function of the differential gravity effects on individual organelles, or on entire tissues transmitted between cell-cell and cell-extracellular matrix junctions remains to be established.
Whether these temporal and population-specific cytoskeletal changes directly translate into altered embryo viability warrants further investigation. A small number of low earth orbit studies with rats and mice have been performed, providing some initial data. As summarized by Crawford-Young, mating experiments using rats showed that fertilization occurred, but no successful pregnancies were generated15. Similarly, in separate experiments, 49 two cell stage mouse embryos flown aboard the space shuttle Columbia did not develop and died15. Clinostat-based work by Kojima and colleagues showed that although there were no differences in the efficiency of in vitro fertilization under simulated microgravity compared to stational control, there was a statistically significant decrease in the number of embryos reaching blastocyst phase after 96 h of culture under simulated microgravity21. An important point to note is that although ground-based and in vitro analyses provide useful data, determining whether mammals can establish a pregnancy under microgravity conditions will require further whole animal experiments.
Accordingly, in terms of future research directions, there are two areas of initial interest that could be addressed: (i) whether it is in fact possible to establish a mammalian pregnancy in space; and (ii) assuming that establishment of a pregnancy is possible, the degree to which a normal pattern of embryonic development occurs.
A good example of work undertaken to address point (ii) is studies performed in mid-gestation pregnant rats flown on the NASA-NIH R1 (gestational days 9−20) and R2 (gestational days 11−20) missions22, with reports detailing changes in the developing fetal vestibular system22, along with increased cardiac atrial natriuretic peptide (a marker of hypertension or myocardial hypertrophy) expression23. Interestingly, the investigators reported that ground control and shuttle-flown pups were similar in terms of weight and gross morphology22. Interestingly, recent work by Corti and colleagues reported a common microRNA signature between maternal plasma taken from small for gestational age pregnancies and female C57BL/6 mice data from NASA’s Open Science Data Repository. The investigators concluded that the 13 shared microRNAs suggested some overlap in space exposures with biological pathways observed in small for gestational age pregnancies24.
Cosmic radiation
Although both non-ionising (i.e. microwaves, ultraviolet light) and ionising radiation are potentially harmful, ionising radiation is of the greatest concern beyond low Earth orbit and in free space given difficulties in effectively shielding against it25,26. Ionising radiation in space is comprised of particles (e.g. protons and electrons) trapped in the Earth’s geomagnetosphere, solar particle events (e.g. protons or heavier particles ejected during coronal eruptions) and galactic cosmic radiation (protons, helium nuclei, or heavier ions). In low Earth orbit, astronauts are comparably protected from solar particle events and galactic cosmic radiation exposure by the geomagnetosphere or by shielding or shadowing from the Earth and the Earth’s Moon26. Transiting radiation belts in low Earth orbit (notably the South Atlantic Anomaly) accounts for delivery of around half of the radiation exposure to the International Space Station Crew25. Galactic cosmic radiation is of the greatest concern to human pregnancy given its ubiquitous nature and the potential for cumulative damage, especially by high energy heavy ions25,26. The estimated annual exposure to galactic cosmic radiation while on Earth is 0.33mSv27, around 11% of an estimated normal annual exposure of 3.1 mSv27. Acute radiation syndrome has been well-documented with radiation of ~1 Gy affecting the bone marrow28.
Radiation causes damage to cells via a variety of interacting mechanisms, including damage to cell membranes, the induction of reactive oxygen species, direct DNA damage (including base damage as well as single and double-stranded breaks), induction of cell cycle arrest and apoptosis29,30,31. Of particular importance to any discussion of pregnancy radiation effects is the observation that rapidly dividing and undifferentiated cells are most susceptible to radiation induced damage28. A dose of 10 mGy is estimated to represent an additional 0.4% lifetime cancer risk for a newborn infant32. As will be outlined further below, the effects of space radiation on the human reproductive system are important to understand both in terms of how it might impact a developing fetus, but also with regard to long-term reproductive health. In particular, the effects of radiation on the ovaries are of particular interest given the importance of ovarian function to healthy ageing in women33.
Regolith exposure
Lunar regolith is the loose layer of rock and dust covering the surface of the Earth’s Moon created as a result of meteorite impacts on the exposed bedrock34,35. Encompassing surface debris ranging from large rocks to ultrafine (<0.1 um) particles, regolith is not subject to the same weathering processes (e.g. wind, tidal action, water erosion) seen on Earth, resulting in a predominance of rough particles with large reactive surface areas. The chemical composition of lunar regolith varies with geography, but is broadly considered to contain around 50% SiO2, 15% Al2O3, 10% CaO, 10% MgO, 5% TiO3 with variable (5–15%) amounts of iron34,35,36. Toxicity assessments performed on animal models to date estimate the hazardous effects of lunar regolith somewhere between that of crystalline silica and titanium dioxide, however data are relatively limited37. Somewhere in the region of 10% of the fine particulate regolith is <10 µm in diameter and considered to be in the respirable range34. Astronauts from the later Apollo missions reported respiratory and visual irritation following exposure to lunar regolith34. Given the high levels of SiO2 it is not unreasonable to predict that extended exposure to regolith may induce respiratory disease similar to that of silicosis seen in industrial workers38. It is important to note that the lunar microgravity environment may increase the penetration of ultra-fine regolith particles into the terminal alveoli, as well as inhibit clearance of inhaled particles from the lungs, both of which are likely to induce an inflammatory response34,35,36. Studies in mice have concluded that although acute maternal pulmonary inflammation is not transmitted to the fetus, changes in systemic inflammation induced fetal metabolic adaptations consistent with those observed during periods of starvation39.
Particulate matter <100 nm in diameter is also able to exert an effect by entering the blood system from the terminal alveoli, and ambient air pollution is now known to be associated with adverse pregnancy outcomes40. From a pregnancy perspective, it is tempting to speculate that regolith exposure may pose an inflammatory risk to the fetus via haematogenous spread to the placenta. Although rare, there is a case report of fetal growth restriction in association with pregnancy silicosis38. Rats exposed to TiO2 particles (188 nm diameter) had increased placental vascular resistance and impairments in vascular reactivity41. Exposure to intravenously administered silica nanoparticles in mice resulted in uterine inflammation and trophoblast apoptosis via a Caspase-3-dependent mechanism42.
The impacts of regolith exposure on reproductive health are not of the same immediate interest as for other space exploration exposures such as microgravity and radiation. Irrespective, there is now a reasonable likelihood of increasing regolith exposure risk because of plans to return humans to the Earth’s Moon. How exposure to very fine regolith particles might directly or indirectly impact reproductive and pregnancy health is an important question. For example, oxidative stress and endothelial cell dysfunction is associated with increased risk of preeclampsia43. Work by Pavan and colleagues sought to use synthetic regolith to investigate the redox activity of a simulant moon agglutinate incorporating metallic iron. They demonstrated significant redox activity even after 1 month of oxidative ageing44. Additional studies have used regolith samples taken from the Apollo 16 mission to explore in vitro allerginicity responses in several different cell populations. Assessments of primary human blood immunocytes did not show any allergy-like response to regolith, although purified allergic cell lines did have a modest lunar dust response45. In light of established adverse health effects of microparticle exposure on Earth, regolith effects on reproductive system function and pregnancy merit further investigation.
Stress
The psychological and social aspects of space travel, including isolation and confinement, may influence maternal well-being and, consequently, fetal neurodevelopment. Maternal stress during pregnancy is known to affect fetal brain development as well as childhood behavior and cognitive performance46,47,48,49.
Circadian rhythm, termed as the internal body clock, refers to the natural oscillation which repeats every 24-h and controls body function and homeostasis. While on board the ISS, astronauts experience 16 sunrises and 16 sunsets in 24 h. Therefore, windows or viewing panes are typically closed during night hours in an attempt to minimise impact on circadian rhythms which control hormone levels and influence sleep cycles, wound healing rates and stress management50.
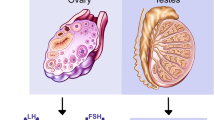
In females, ovulation is the result of carefully timed hormonal surges (GnRH stimulates FSH and LH which in turn promote oocyte maturation and estrogen increase) which result in a mature oocyte being released and a receptive uterus for embryo implantation should successful fertilization occur51. Disrupted circadian rhythms affect the hypothalamus-pituitary-ovary axis and menstrual cycles (estrus cycles in mice) as seen in women exposed to shift work schedules52. It was also reported that in male mice, the lack of circadian rhythm caused decreased sperm motility and a reduction of testis enzymes (G6PDH, SDH, LDH and ACP)53.
Though astronauts experience unique opportunities of individual accomplishment as well as advancing space exploration for humankind, space travel brings astronauts away from their familial network, friendships and social interactions which they would otherwise have on Earth. This isolation has been shown to pose a mental and emotional strain on astronauts54.
In addition, it was reported that female astronauts tend to postpone childbearing and take oral contraceptives to suppress menstrual cycles while on space missions. Recently, the need for research into space sexology has also been discussed as astronauts experience limited access to intimacy partners, mandated hygiene procedures and abstinence protocols55.
While astronauts experience high psychological and emotional stress, space travel is also associated with physical stress which is extremely demanding on the human body, for example during ascent and re-entry, when astronauts experience hypergravity. This causes vision disturbances, disrupted vestibular system and even loss of consciousness. In a mammalian model, it was shown that rats were able to mate and become pregnant while in space, though these pregnancies were resorbed and attributed to maternal stress during the space flight, possibly due to travel turbulence56. However, both male and female mice which returned to Earth, after their 18.5-day space flight, were still able to have subsequent litters on Earth, thus suggesting potentially minimal effects on gametogenesis if the space travel was short. In a study of airline stewardesses, first-trimester miscarriage risk was increased in stewardesses who flew > 15 h during their home-base sleep time and who had increased physical job demands, further compounding the impact of stress on the reproductive system57.
Along with radiation, stress is perhaps the best understood space exposure in terms of its risk profile for reproductive health and pregnancy. What is not well understood, however, is how stress might modify or perhaps exacerbate the effects of other space exposures, such as microgravity or radiation. Unpacking this potential interactive effect may not only provide useful information in terms of mitigating reproductive risk in astronauts, but also inform strategies to improve pregnancy health more generally.
Specific examples of space exposure on reproduction and the developing fetus
Reproductive System Development and Function
Although contemporary astronaut training programs are approaching an equal mix of males and females, females have historically comprised a small minority of the astronaut population58; accordingly the impact of space travel on the female reproductive system and pregnancy safety is an important, under-addressed area of research. In male mammals, microgravity has been shown to affect total sperm count and lowers testosterone levels59, although male mice caged in the ISS were still able to sire healthy offspring60. There were no changes to in vitro fertilization rates, but the number of embryos reaching the morula and blastocyst stage were decreased in simulated microgravity conditions. It was thus reported that microgravity affects spermatogenesis, sperm motility and early embryonic lethality61.
Female space exposure has been predicted to increase the risk of infertility, along with increased risk of early menopause58. Rose has suggested that, for example, a standard Mars mission may reduce a woman’s ovarian reserve by some 50%, potentiating early menopause and increased risk of associated disease58. Space effects on human female reproduction may be assessed from several perspectives, including impacts on the individual’s reproductive ability (including establishing and maintaining a pregnancy) and on their long-term health (i.e. early menopause). A recent systemic review and meta-analysis on male and female spaceflight effects identified important reproductive risks for both sexes; in females, thromboembolism risk from combined oral contraceptive use and functional insufficiency of the corpus luteum are of particular interest—and concern62. Of the space exposures, radiation is a key concern for both pregnancy and long-term reproductive system health. Straume and colleagues have noted that the critical (radiosensitive) health impact associated with the colonization of Mars by humans may be female infertility resulting from in utero radiation exposure. Guo and colleagues have estimated that the total effective radiation dose for a round trip to Mars (180 day one-way flight, 500 day Mars surface stay) would be ~1.01 Sv63. Straume and colleagues note that the effective threshold for serious fetal developmental abnormalities to occur during organogenesis is around 0.1 Sv acute gamma rays64. Estimations of ovarian and fetal risk are complicated by variations in solar activity, shielding (from craft as well as the maternal tissues), duration of exposure and biological susceptibility. Irrespective, the available data suggests that space exposure conveys a sizable risk to the female reproductive system. For an in-depth treatment of radiation hazards associated with Mars colonisation, the reader is referred to a review by Straume, Blattnig and Zeitlin64.
In a study quantifying radiation exposure due to cancer treatment, it was reported that 50% of human oocytes can be destroyed by radiation exposure of 2 Gy. At 15 Gy radiation, premature ovarian failure sets in and if a woman is pregnant, risk of adverse pregnancy outcomes rises to 90%65. In a space-simulated environment of cosmic radiation, destruction of mouse ovarian follicles occurred in a dose-dependent manner (0, 5, 30, 50 cGy) and caused elevated FSH and LH levels66. Lipid peroxidation, H2AX phosphorylation, protein nitration and elevated apoptosis markers were also noted in female mice exposed to high radiation levels. In males, radiation was shown to increase sperm DNA fragmentation. However, healthy offspring were still obtained from frozen mouse spermatozoa which had been stored on the ISS for 9-months67.
Exposure to space radiation poses significant risks, as high-energy particles can penetrate biological tissues, leading to DNA damage and oxidative stress64. These factors are particularly concerning for developing fetuses, where the rapid proliferation of NSCs, the differentiation and maturation of neurons, and the establishment of neural circuits are highly sensitive to environmental perturbations. However, there are few published studies evaluating the effect of the space radiation environment on NSC homeostasis and neurogenesis. Most research on the effects of galactic cosmic rays (GCRs) on neurogenesis has been conducted in facilities that simulate the space radiation environment and focus on adult NSCs68. Various experimental protocols suggest that adult NSCs are particularly sensitive to ionizing radiation, with GCR-like irradiation increasing oxidative stress levels, inducing apoptosis, and impairing NSC homeostasis69,70,71. On the other hand, primary fetal mouse neuronal cultures exposed to microgravity, and especially those subjected to both microgravity and radiation, exhibited altered morphology (reduced neurite length) and increased apoptosis. These synergistic effects were associated with changes in the expression levels of genes involved in neurite extension, synaptic communication, and cell survival72.
Lastly, both cosmic radiation and microgravity have been linked to alterations in oxidative stress status, with potential to impact both reproductive tissue health and pregnancy viability. Studies in rats have shown that hind limb unloading (simulating microgravity) was associated with increased markers of oxidative stress in a wide range of tissues73. Similarly, exposure of rats to proton or heavy ion irradiation resulted in cardiac, and CNS oxidative damage. Perturbations in oxidative stress are also associated with accelerated ovarian ageing and pregnancy complications73. Long-term oxidative stress exposure has been associated with decreased follicle quality and progesterone production73,74. A review by Steller and colleagues provides an excellent assessment of space-related oxidative stress on female reproductive health73.
Fetal skeletal development
The effects of space travel on the human skeleton have been well documented, with reports from the 1970s documenting bone loss in astronauts at a rate of 1–2% per month75. A key driver of these changes is believed to be adaptive changes derived from gravity unloading—with weight bearing bones exhibiting greater changes than non-weight bearing bones75. Exposure to cosmic radiation may also exacerbate microgravity-induced bone loss64. Given the well characterized pattern of gravity-induced bone loss, muscle atrophy, and delayed fracture healing in adult astronauts, the developing fetal skeleton is also likely to be impacted by microgravity76. Given the peculiarities of fetal skeleton formation and its ossification, which begins early in pregnancy but continues into adulthood, the effect of gravity will likely differ at various stages of development. However, despite decades of research into the impact of microgravity on systemic physiology, there remains a paucity of evidence concerning its direct effects on embryonic skeletal development. This evidence necessitates interpretation within the context of microgravity’s influence on the underlying biological mechanisms.
The formation of the human fetal skeleton, initiates around the 6th to 7th weeks of gestation through two primary processes: intramembranous and endochondral ossification. In intramembranous ossification, mesenchymal tissue precursors from the cranial neural crest cells directly transform into flat bone. Conversely, in endochondral ossification, precursors from somites and the lateral plate mesoderm develop into a cartilage intermediate, which is subsequently replaced by bone. Endochondral ossification contributes to the formation of the axial skeleton and the long bones77. The ossification process requires a developmental cartilage template, derived from embryonic mesoderm, and undifferentiated mesenchyme, which specifies the sites for bone formation. By birth, a significant portion of this cartilage has been substituted by bone, although ossification persists until ~25 years of age as growth advances.
Microgravity can impact both precursor stem cells and the growth processes of the skeleton during later stages of fetal development. Embryonic stem cells (ESCs), act as pivotal regulators of embryonic development, with their self-renewal and pluripotency regulated by a complex network involving signal transduction pathways, transcription factors, and chromatin remodeling complexes78. While some research has indicated that Oct479, a transcription factor involved in the maintenance of ESC identity, exhibits increased expression compared to the ground-based control group, other studies have revealed heightened apoptosis and reduced cell adhesion of ESCs under microgravity conditions, consequently leading to decreased cell expansion80. These alterations may be associated with changes in the expression of genes related to the cell cycle and cell proliferation, suggesting that microgravity has the potential to influence the self-renewal of ESC81. Moreover, multiple studies have also shown that microgravity can affect the differentiation of ESCs82,83 promoting their differentiation into mesoderm, endoderm, and their differentiated cells76. Considering that self-renewal and differentiation are crucial processes in the early stages of embryo development, its comprehensible that the impact on mammals like mice is more pronounced during early-stage pregnancies, resulting in a failure to develop and produce offspring. Conversely, mice in the second half of pregnancy have demonstrated the capability to successfully produce viable offspring84, but few studies examine the effects beyond juvenile stages. Edsall et al., evaluated the impact of microgravity in cranial neural crest migration in zebrafish embryos, and what happened with the skeletons of adult fish85. They found underdeveloped growth, reduced ossification, and severe distortion of skeletal elements, highlighting the significance of studying altered gravitational forces’ long-term effects on embryonic development. In fetal mice, microgravity did not change the percent length increase and collagen synthesis in long bones but there was a decrease in glucose utilization and mineralization85.
Fetal central nervous system development
Microgravity, a defining characteristic of space environments, induces stress-related alterations in cellular structure and gene expression86, which can significantly impact cellular processes and alter the development of the fetal nervous system. Despite its importance, there are relatively few studies specifically investigating the effects of microgravity (either simulated or actual outer space conditions) on neural stem cells (NSCs). Moreover, the impacts of cosmic radiation on the developing fetal nervous system warrant further attention, especially given that the fetus is more susceptible to adverse radiation effects than adults64.
Silvano et al. reported that murine cerebellar NSCs subjected to simulated microgravity experience cell cycle arrest in the S-phase accompanied by increased apoptosis87. Conversely, research by the Espinosa-Jeffrey group demonstrated that human NSCs exposed to outer space microgravity exhibited enhanced proliferation, a shortened cell cycle, and increased cell diameter compared to ground control cells88. Notably, the effects were more pronounced under actual outer space conditions than under simulated microgravity89. Furthermore, their study highlighted an increase in abnormal cell divisions, including incomplete cytokinesis, among NSCs exposed to microgravity90. They also found that the secretome from microgravity-exposed NSCs induced similar incomplete cytokinesis, indicating a significant role of secreted molecules in microgravity-associated effects90.
Additionally, exposure to space for 3 days altered the metabolites secreted by NSCs, reflecting increased glycolytic activity91. Similarly, Han et al. observed that microgravity enhanced the proliferation capacity of neural crest stem cells and was associated with specific changes in the expression of genes related to proliferation92. They also found that microgravity altered the microRNA content of extracellular vesicles derived from neural crest stem cells, enriching miRNAs involved in cell cycle regulation, stem cell maintenance, and brain development92. These findings strongly suggest that microgravity induces several alterations in NSC homeostasis, including metabolic changes, increased proliferation, and defects in cell cytokinesis. These alterations are not solely due to changes in mechanical forces but also involve modifications in the NSC secretome. Moreover, the data suggest that the effects of outer space conditions are more severe than those of simulated microgravity, with outer space radiation and other environmental factors likely contributing to these differences.
Biological studies—in summary
As outlined above, data from space flight exposures (on animals, cell systems and adult astronauts) and simulated (parabolic flights, random positioning machines) space exposures demonstrate a host of tissue specific adverse effects that appear likely to impact the viability and development of human pregnancy. Exposure to microgravity, radiation, regolith and stress each have the potential to impact a human pregnancy. Determining the effects on a fetus developing under microgravity and associated conditions is difficult given current data—however it does seem very reasonable to conclude that, if early-stage embryogenesis and implantation could successfully occur, there would likely be multi-system adverse impacts on fetal development. It is unclear what the threshold limits might be for an exposure such as microgravity (i.e. would Martian gravity but not Lunar gravity be sufficient for successful embryogenesis?), and to what extent these might be modified by additional exposures such as radiation or stress. The potential role for emerging pregnancy technologies, such as assisted reproduction58, and artificial placenta technology (allowing ex-utero gestation) also warrant consideration in a broader discussion regarding off-world human reproduction93,94,95. Given limited resources, and the imminent increase in low Earth orbit, cis-lunar and lunar activity, it seems reasonable that initial efforts in this area should be directed at first establishing safe exposure levels, and appropriate countermeasures, for male and female reproductive systems given their central importance to health and ageing. Looking further ahead, establishing the potential viability of human pregnancy in space has important implications for planned attempts to explore Mars (and beyond), and may also help us better understand the fundamental biology underpinning human reproduction and fetal programming more generally.
Ethical considerations
A multi-staged research ethics approach
The ethics of reproduction in a space environment have largely been viewed in academic literature at a macro level, i.e., which either takes a broad-brush approach in signaling the future emergence of ethical issues arising from any attempt to research reproduction in space96,97, or which addresses long-range issues, either through a focus on human enhancement for space98,99,100 or a more general concern with species survival. The so-called “longtermist” view, beloved of philosophers of existential risk101,102, and echoed by space entrepreneur Elon Musk103, espouses the value of future generations of human beings who may be brought into being in faraway places such as Mars as a hedge against any calamitous terrestrial event that would see humanity die out. Longtermism thus leverages the projected benefits to humanity in the distant future against more immediate near-term considerations. Despite arguments that might be mounted against the presumed inevitability of human-induced extinction events such as runaway climate change or nuclear war, it cannot be gainsaid that on a cosmic timescale Earth-dwelling humans are indeed doomed. Assuming they were able to avoid self-destruction or being consumed by natural catastrophes such as pandemics or meteor strikes, they would ultimately die as the Sun’s evolution leads to the heating of the Earth past the point where any species could survive104.
However, whatever the intuitive or intellectual appeal of longtermism, the justification of research programmes—not least those which have welfare implications for mothers and their nascent children—must inevitably deal with short-term and foreseeable consequences as a priority. Many research articles that purport to justify what might broadly be called space pregnancy research on the basis of a perceived need to ensure humanity’s future among the stars neglect to acknowledge much less address the multiple ethical considerations that would have to be entertained between the immediate research topics under discussion and presumedly successful future human settlement of space105,106.
Notwithstanding the fact that once a greater degree of certainty is obtained about the larger calamity that we seek to insure our species’ longevity against there may be insufficient time to do the necessary research to make space reproduction as safe as possible, scientific research operates within a present-day reality of ethically guided decision-making. Despite Szocik & Reiss’s reasonable observation that “space bioethics, compared, for example, to conventional medical bioethics, may give more weight to utilitarian considerations and less to such deontological considerations as informed consent and autonomy” (p.95)107, the bioethics that precedes finding ourselves in space and which guides research in the life sciences does indeed give priority to values such as autonomy and the potential for human development over broader utility. To the extent that human biological research has utility in serving the public good, it is typically not at the expense of individual welfare.
If we are serious about charting an ethical course for research that could make the challenges of pregnancy and childbirth in extraterrestrial environments sufficiently understandable for us to decide whether and how to plan for long-term space settlement, we must also reckon with the various stages from conception through gestation to birth and the specific ethical issues that arise for the various stakeholders (not least mother and nascent child) at those stages. The ethical conduct of space research matters, whether publicly or privately funded, and good research ethics requires that we take account of the potential harms that occur in the conduct of research and not just putative future benefits.
Although arguments have been made for ectogenesis (embryo development in artificial wombs) as a means of ensuring the future survival of the species that does not at the same time risk the health of the mother in a space environment108, this does not address risks to the fetus and future child. Moreover, in this paper we are concerned with how far scientific research may be carried out into pregnancy from conception onwards under genuine or simulated space conditions while adhering to values hitherto upheld in human life science research. In other words, our concern is to navigate the ethical questions that arise in researching the linear process of pregnancy109 using the ethical standards of the present-day terrestrial research environment rather than an ethics that may be favored in more abstract philosophical discussions.
In this paper, we eschew the adoption of classical normative ethical frameworks such as utilitarianism (in any of its forms), Kantian deontology or virtue ethics since research ethics as practiced by ethics review boards internationally is typically driven by principles such as harm minimization, informed consent, justice, and the weighing of benefit to the public good against potential risks to research participants; in other words, the kinds of obligations articulated within the principlist approach of Beauchamp and Childress110. It is review boards that would first be confronted with the ethical challenges related to researching human reproduction for the outer space context and their deliberations are not typically led by the traditional philosophical approaches to ethics.
Stages of human pregnancy research at which different ethical issues arise
Fertilization
Fertilization of human oocytes under space conditions (real or simulated) is of essential interest in any attempt to understand reproduction in space for the sake of any intended future long-term settlement of space105,111. However, the fertilization of an oocyte under space conditions for research purposes would be subject to just as strict a review and oversight process as fertilization for terrestrial research purposes among nations that have reproductive research guidelines or regulations in place.
Although sexual intercourse in space has been considered taboo to date (albeit no space agency currently has an explicit prohibition of it), any initial attempt at studying fertilization in a simulated or actual space environment would no doubt take place in vitro. Some research has been conducted into fertilization of other mammalian species’ oocytes in both a simulated and a genuine microgravity environment106,112 and a study of human follicle development in simulated microgravity has been conducted113, but to date no fertilized human oocytes have been studied in simulated or genuine microgravity.
The conduct of any such study of human fertilization in a microgravity environment, whether simulated or genuine, would require careful justification to an Institutional Review Board (IRB) in terms of its necessity (i.e. as opposed to alternative means of generating the necessary data) and the balance of anticipated benefits against any foreseeable harms. Oversight of how fertilized oocytes are stored, researched on, and ultimately disposed of would, of course, provide further practical challenges if the process of fertilization were conducted in space, a challenge which has even more profound implications when it comes to embryo research.
In vitro embryo research
Although there is no firm international consensus on whether embryo research should be allowed or to what stage of development, there is broad agreement among many advanced scientific nations that research should be allowed up to 14 days of development, i.e., prior to gastrulation and the individuation of the embryo marked by the appearance of the primitive streak114. There are also currently arguments being made to extend this to 28 days given the possibility of culturing embryos in vitro and the lack of neuronal development that takes place within this additional period which means that the embryo will not feel pain regardless of the interventions performed115. The lack of capacity for pain, of course, blunts just one kind of moral objection that might be made to experimentation on an embryo which has already individuated itself116,117.
It has been argued that allowing for research during this additional 2-week period may facilitate better understanding of poorly understood processes involved in implantation as well as the possible merging of embryo and organoid research115. The International Society for Stem Cell Research (ISSCR) while recommending the dropping of the 14-day rule has deferred final adjudication on this to national regulators and recommended assessment on a case-by-case basis118,119,120. In considering whether to grant such an extension, the benefits to scientific knowledge and the public good (via maternal health and positive pregnancy outcomes) need to be weighed against moral concerns held by at least certain sections of a given community regarding the sanctity of the individual life whose onward development is curtailed. As Hyun, Wilkerson and Johnston point out: “The 14-day rule was never intended to be a bright line denoting the onset of moral status in human embryos. Rather, it is a public policy tool designed to carve out a space for scientific inquiry and simultaneously show respect for the diverse views on human-embryo research” (p. 170)114.
Post-implantation research in a space environment
Obtaining knowledge of how pregnancies might fare in space from the point of implantation onwards presents profound ethical challenges once we move past animal models and wish to study actual human pregnancies in a space environment. If the intention is to terminate a pregnancy before it can be brought to term to avoid the likely harms caused by radiation, microgravity or other hazards to an actual child, then there would still be potentially insurmountable problems to overcome from a regulatory point of view. No nation that currently regulates embryo research would tolerate deliberately terminating an implanted embryo or subsequent fetus as part of a research protocol. Furthermore, many jurisdictions such as the United Kingdom prohibit the implantation of any embryo that has been used in research in the first place121.
A utilitarian argument for opening a pathway to humans becoming a sustainably multiplanetary species as a hedge against future extinction would cut no ice with regulators given current guidelines and regulations. Nevertheless, it is conceivable that sometime in the future an expert body guided by views gathered via public consultation might decide otherwise, though how the public good were served by such an affordance would lie in a very speculative realm about: (i) the practical need for humans to form permanent, self-sustaining settlements in space, (ii) there being no alternative means of obtaining the necessary knowledge about human space pregnancies to make them sufficiently safe and viable, and (iii) the potential harms of the research being outweighed by the foreseeable benefits. These considerations of need, alternatives, and harms versus benefits are quite standard ones in justifying research projects in human life science and there is no clear reason why they should be circumvented for space pregnancy research. The valid consent of a woman to participate in any pregnancy research study would, of course, be essential. Valid consent requires that consent be given voluntarily by a person who possesses mental capacity to understand information sufficient for them to form a properly informed decision to participate. The nature of the risks mother and fetus would be exposed to would need to be clearly explained as far as they are understood, and the reasonableness of the risks considered against the presumed benefits.
The occurrence of “unintended” pregnancies in space would not provide a workaround to ethical prohibitions on space pregnancy research by presenting a kind of fait accompli since a de facto prohibition on sex during missions and/or the mandated adoption of any preventive measures such as contraception or sterilization122 would have had to have been violated and any after-the-fact birth prevention via termination (e.g. using abortion pills mifepristone or misoprostol) eschewed. (We assume that the early detection of pregnancy in an astronaut who is subject to regular medical screenings and the generally prohibitive environment would allow for early-stage (i.e. non-surgical) abortion.) Thus, ethical violations would have been committed that effectively “poison the well.” Consequently, any opportunity taken to conduct ad hoc research would not meet the standards of ethical review and whatever observational results were obtained would not be embraced by the scientific community as a legitimate contribution to knowledge.
Research ethics considerations aside, given the multiple threats to pregnancies and maternal wellbeing already identified, we would recommend that space agencies and commercial space operators take all reasonable steps to avoid pregnancies occurring in space, e.g., through mandatory pre-mission pregnancy testing and mandatory contraception on longer duration mixed-sex missions (e.g., by long-acting contraceptive implants). The mandating of chemical abortions should pregnancies still occur could, as Szocik and Reiss recognize107, come into tension with notions of reproductive autonomy, though we would argue that the commitments made voluntarily by astronauts as a condition of going to space would render any appeal to autonomy weaker than it would be in any terrestrial context. Without going so far as to require their forcible administering, we certainly recommend that abortion pills be part of the standard provisioning of spacecraft on long-duration missions beyond Earth orbit and that a reasonable expectation is established among crew for their potential use should a pregnancy occur.
Without prejudice to how—or indeed whether—the considerations already raised in this paper are resolved, we might assume for the sake of discussion that a time has come where some reasonable ethical case has been made for allowing research to take place on an actual space pregnancy that it is intended to carry to term. Under such circumstances, we should still proceed to take a staged approach in dealing with ethical issues that arise, guided primarily by concern about the welfare of mother and child.
First, consideration would need to be given to whether to fly an already pregnant woman to space in preference to allowing conception to take place in space. Doing so would allow for a more predictable and safer implantation though it would subject the woman to the rigours of space launch and bodily adaptation to the space environment which could affect not only her but her embryo. At some subsequent point, no doubt, researchers would want to track an entire pregnancy from conception to birth in space, but the first consideration in researching an actual pregnancy that it is intended to take to term in space is how to make that pregnancy as safe as possible in its totality.
Second, it would be prudent to ensure that any planned space pregnancy only be allowed to proceed in a near-Earth context, i.e. at the International Space Station (or a successor space station)123, the Tiangong Space Station, or a future Moon base, such that evacuation of the mother to Earth would be feasible in an emergency. The risks of transportation would obviously have to be weighed against the risks of handling a particular emergency in situ. Saving the life of the mother would be the paramount consideration in such a scenario.
Third, any study of an ongoing pregnancy in deep space beyond the possibility of return to Earth for delivery should compel not only the provisioning of the spacecraft or Martian base for successful full-term delivery but also for premature delivery in the form of incubators and other life support equipment for pre-term neonates. In other words, justice and beneficence would dictate that as much provisioning should be made for the well-being of fetuses and babies that are part of any study of pregnancy in space as possible; ideally, as would be available in a well-resourced delivery suite in an advanced terrestrial economy. After all, the children of these particular parents if born on Earth would surely have access to advanced levels of care and to deny their space-born counterparts similar benefit would be discriminatory. This is particularly the case as they would by design be research subjects and not just children who are subject to the life choices and birth preferences of their parents.
Ultimately, these are just some of the more foreseeable issues that would challenge ethicists and research oversight bodies in the linear process of managing space pregnancy research going forward. We make no presumptions about exactly when or how the issues should be resolved; only that in line with our overall argument there would need to be a considered, incremental approach that is sensitive to the specific contexts in which these issues arise.
Conclusion
The regulation of research into the viability and safety of space pregnancies will be an ongoing challenge that will involve consideration of an evolving understanding of harms and potential countermeasures as pertain to the space environment alongside consideration of the public benefit that might plausibly be obtained through such research. Only a staged approach to determining how research should proceed will ensure that cherished ethical principles are respected and purposefully modified, supplemented, or suspended where appropriate. In other words, the arguments for adhering to existing research ethics principles or deviating from them should be made explicit, and in the latter case should seek the concurrence of the appropriate authorities and preferably be informed by the outcomes of public consultation exercises.
To the extent that we can make any policy-level recommendations here based on our understanding of the practical and ethical challenges of conducting research for human reproduction in space surveyed in this paper, they would be to exhaust the potential of non-human reproductive models for the space environment (animal and computer-based) as well as human stem cell-derived embryoids that lack viability before considering a move towards a truly first-in-human protocol for space reproduction. Further, given our rejection of longtermist (or other broadly utilitarian) arguments for ensuring species survival by facilitating human propagation in space in favor of a staged approach to confronting ever more ethically challenging possibilities, such as allowing research on embryos past the 14-day stage or implanting an embryo in either an artificial or a natural womb in space, we would want to see open public policy discussion in which national populations were given a voice in the process of establishing potentially more permissive regulation through public consultation exercises.
The purported growth of commercial space activity and the ambition of the likes of entrepreneurs such as Elon Musk to establish permanent human settlements on Mars may threaten to circumvent the kinds of ethical oversight and control of life science and human subject research that are required of national space agencies such as NASA or supranational entities such as the European Space Agency (ESA). Currently, privately funded, non-institutional research projects on Earth are required to conform to established ethical principles and regulations within the jurisdictions in which they operate. In terms of space law, i.e., as established under the 1967 Outer Space Treaty, it is also worth noting that countries whose citizens operate in space, even in a private capacity, have an obligation under Article VI to authorize and oversee their activities in space124.
Operating in space, particularly deep space, i.e. beyond the Earth-Moon system, may make oversight and regulation of such entities all but impossible, though to the extent that these entities wish to maintain public support and the goodwill of investors, contractors and other stakeholders125, they would do well to cleave to the careful, progressive work of research ethics of the kind this paper recommends be undertaken in attempting to make Homo sapiens a truly multiplanetary species.
Data availability
All data is contained within the manuscript.
References
Simonsen, L. C., Slaba, T. C., Guida, P. & Rusek, A. NASA’s first ground-based galactic cosmic ray simulator: enabling a new era in space radiobiology research. PLoS Biol. 18, e3000669 (2020).
Todd, P., Pecaut, M. J. & Fleshner, M. Combined effects of space flight factors and radiation on humans. Mutat. Res. 430, 211–219 (1999).
NASA. Artemis. https://www.nasa.gov/humans-in-space/artemis/ (2024).
Genta, G. & Maffione, P. F. A graphical tool to design two-ways human Mars missions. Acta Astronaut. 154, 301–310 (2019).
Garrett-Bakelman, F. E. et al. The NASA Twins Study: A multidimensional analysis of a year-long human spaceflight. Science 364, 6436 (2019).
Du, Y. et al. Lunar and Martian gravity alter immune cell interactions with endothelia in parabolic flight. npj Microgravity 11, 4 (2025).
Kopp, S. et al. Thyroid cancer cells in space during the TEXUS-53 sounding rocket mission – The THYROID Project. Sci. Rep. 8, 10355 (2018).
Subramanian, A. et al. Simulated lunar microgravity transiently arrests growth and induces osteocyte-chondrocyte lineage differentiation in human Wharton’s jelly stem cells. NPJ Microgravity 10, 51 (2024).
Choi, D. H. et al. 3D cell culture using a clinostat reproduces microgravity-induced skin changes. NPJ Microgravity 7, 20 (2021).
Dai, S. et al. Effect of simulated microgravity conditions of hindlimb unloading on mice hematopoietic and mesenchymal stromal cells. Cell Biol. Int. 44, 2243–2252 (2020).
Nguon, K., Ladd, B. & Sajdel-Sulkowska, E. M. Exposure to altered gravity during specific developmental periods differentially affects growth, development, the cerebellum and motor functions in male and female rats. Adv. Space Res. 38, 1138–1147 (2006).
Santomartino, R. et al. No effect of microgravity and simulated mars gravity on final bacterial cell concentrations on the international space station: applications to space bioproduction. Front. Microbiol. https://doi.org/10.3389/fmicb.2020.579156 (2020).
Lim, H. Y. G. & Plachta, N. Cytoskeletal control of early mammalian development. Nat. Rev. Mol. Cell Biol. 22, 548–562 (2021).
Fletcher, D. A. & Mullins, R. D. Cell mechanics and the cytoskeleton. Nature 463, 485–492 (2010).
Crawford-Young, S. J. Effects of microgravity on cell cytoskeleton and embryogenesis. Int J. Dev. Biol. 50, 183–191 (2006).
Tauber, S. et al. Cytoskeletal stability and metabolic alterations in primary human macrophages in long-term microgravity. PLoS One 12, e0175599 (2017).
Barravecchia, I. et al. Microgravity and space radiation inhibit autophagy in human capillary endothelial cells, through either opposite or synergistic effects on specific molecular pathways. Cell Mol. Life Sci. 79, 28 (2021).
Janmaleki, M., Pachenari, M., Seyedpour, S. M., Shahghadami, R. & Sanati-Nezhad, A. Impact of simulated microgravity on cytoskeleton and viscoelastic properties of endothelial cell. Sci. Rep. 6, 32418 (2016).
Quynh Chi, H. N. et al. Simulated microgravity reduces proliferation and reorganizes the cytoskeleton of human umbilical cord mesenchymal stem cells. Physiol. Res 69, 897–906 (2020).
Piszker, W. & Simunovic, M. In Current Topics in Developmental Biology (eds Celeste M. Nelson & Lance A. Davidson) 31−64 (Academic Press, 2024).
Kojima, Y. et al. Effects of simulated microgravity on mammalian fertilization and preimplantation embryonic development in vitro. Fertil. Steril. 74, 1142–1147 (2000).
Ronca, A. E., Fritzsch, B., Bruce, L. L. & Alberts, J. R. Orbital spaceflight during pregnancy shapes function of mammalian vestibular system. Behav. Neurosci. 122, 224–232 (2008).
Davet, J. et al. Cardiac atrial natriuretic peptide (ANP) in rat dams and fetuses developed in space (NIH-R1 and NIH-R2 experiments). Life Sci. 64, 1533–1541 (1999).
Corti, G. et al. To boldly go where no microRNAs have gone before: spaceflight impact on risk for small-for-gestational-age infants. Commun. Biol. 7, 1268 (2024).
Shavers, M. R. et al. Comparison of dose and risk estimates between ISS partner agencies for a 30-day lunar mission. Z. für Medizinische Phys. 34, 31–43 (2024).
Moreno-Villanueva, M., Wong, M., Lu, T., Zhang, Y. & Wu, H. Interplay of space radiation and microgravity in DNA damage and DNA damage response. NPJ Microgravity 3, 14 (2017).
Control, C. f. D. Facts About Radiation from Space (Cosmic Radiation). https://www.cdc.gov/radiation-health/data-research/facts-stats/cosmic-radiation.html (2024).
Macià, I. G. M., Lucas Calduch, A. & López, E. C. Radiobiology of the acute radiation syndrome. Rep. Pr. Oncol. Radiother. 16, 123–130 (2011).
Stone, H. B., Coleman, C. N., Anscher, M. S. & McBride, W. H. Effects of radiation on normal tissue: consequences and mechanisms. Lancet Oncol. 4, 529–536 (2003).
Lomax, M. E., Folkes, L. K. & O’Neill, P. Biological consequences of radiation-induced DNA damage: relevance to radiotherapy. Clin. Oncol. 25, 578–585 (2013).
Cohen–Jonathan, E., Bernhard, E. J. & McKenna, W. G. How does radiation kill cells? Curr. Opin. Chem. Biol. 3, 77–83 (1999).
Mainprize, J. G., Yaffe, M. J., Chawla, T. & Glanc, P. Effects of ionizing radiation exposure during pregnancy. Abdom. Radiol. 48, 1564–1578 (2023).
Recognizing the importance of ovarian aging research. Nat. Aging 2, 1071−1072 (2022).
Cain, J. R. Lunar dust: The Hazard and Astronaut Exposure Risks. Earth, Moon, Planets 107, 107–125 (2010).
Miranda, S. et al. A dusty road for astronauts. Biomedicines 11, 1921 (2023).
Pohlen, M., Carroll, D., Prisk, G. K. & Sawyer, A. J. Overview of lunar dust toxicity risk. NPJ Microgravity 8, 55 (2022).
Morimoto, Y. et al. [Effect of lunar dust on humans: -lunar dust: regolith. Nihon Eiseigaku Zasshi 65, 479–485 (2010).
Sivabalasubramaniam, G., Sagili, H., Dasari, P. & Gowda, M. Burst abdomen: an unusual complication of silicosis in pregnancy. BMJ Case Rep. 2015, bcr2014207132 (2015).
Hansen, S. S. K. et al. Pulmonary maternal immune activation does not cross the placenta but leads to fetal metabolic adaptation. Nat. Commun. 15, 4711 (2024).
Saenen, N. D. et al. Air pollution-induced placental alterations: an interplay of oxidative stress, epigenetics, and the aging phenotype? Clin. Epigenetics 11, 124 (2019).
Abukabda, A. B. et al. Maternal titanium dioxide nanomaterial inhalation exposure compromises placental hemodynamics. Toxicol. Appl. Pharmacol. 367, 51–61 (2019).
Tian, J. et al. In vitro and in vivo uterine metabolic disorders induced by silica nanoparticle through the AMPK signaling pathway. Sci. Total Environ. 762, 143152 (2021).
Sánchez-Aranguren, L. C., Prada, C. E., Riaño-Medina, C. E. & Lopez, M. Endothelial dysfunction and preeclampsia: role of oxidative stress. Front Physiol. 5, 372 (2014).
Pavan, C. et al. Atmospheric environment shapes surface reactivity of Fe(0)-doped lunar dust simulant: potential toxicological implications. J. Hazard Mater. 492, 138096 (2025).
Colorado, A. A. et al. Hazards of lunar surface exploration: determining the immunogenicity/allergenicity of lunar dust. Front Immunol. 16, 1539163 (2025).
King, S. & Laplante, D. P. The effects of prenatal maternal stress on children’s cognitive development: project ice storm. Stress 8, 35–45 (2005).
van den Bergh, B. R. H., Dahnke, R. & Mennes, M. Prenatal stress and the developing brain: risks for neurodevelopmental disorders. Dev. Psychopathol. 30, 743–762 (2018).
Weinstock, M. Prenatal stressors in rodents: effects on behavior. Neurobiol. Stress 6, 3–13 (2017).
Batiz, L. F. et al. Maternal exposure to a high-magnitude earthquake during pregnancy influences pre-reading skills in early childhood. Sci. Rep. 11, 9244 (2021).
Otsuka, K. et al. Anti-aging effects of long-term space missions, estimated by heart rate variability. Sci. Rep. 9, 8995 (2019).
Simonneaux, V. & Bahougne, T. A multi-oscillatory circadian system times female reproduction. Front Endocrinol. (Lausanne) 6, 157 (2015).
Sellix, M. T. Circadian clock function in the mammalian ovary. J. Biol. Rhythms 30, 7–19 (2015).
Qin, F. et al. Circadian effects of ionizing radiation on reproductive function and clock genes expression in male mouse. Environ. Health Prev. Med 26, 103 (2021).
Yin, Y. et al. Long-term spaceflight composite stress induces depression and cognitive impairment in astronauts—insights from neuroplasticity. Transl. Psychiatry 13, 342 (2023).
Dubé, S., Santaguida, M., Anctil, D., Giaccari, L. & Lapierre, J. The case for space sexology. J. Sex. Res. 60, 165–176 (2023).
Proshchina, A. et al. Reproduction and the early development of vertebrates in space: problems, results, opportunities. Life (Basel) 11, 109 (2021).
Grajewski, B. et al. Miscarriage among flight attendants. Epidemiology 26, 192–203 (2015).
Rose, B. I. Female astronauts: Impact of space radiation on menopause. Eur. J. Obstet. Gynecol. Reprod. Biol. 271, 210–213 (2022).
Ahrari, K., Omolaoye, T. S., Goswami, N., Alsuwaidi, H. & du Plessis, S. S. Effects of space flight on sperm function and integrity: a systematic review. Front. Physiol. 13, 904375 (2022).
Matsumura, T. et al. Male mice, caged in the international space station for 35 days, sire healthy offspring. Sci. Rep. 9, 13733 (2019).
Sasaki, S. et al. Male fertility in space]. Hinyokika Kiyo 50, 559–563 (2004).
Gimunová, M., Paludo, A. C., Bernaciková, M. & Bienertova-Vasku, J. The effect of space travel on human reproductive health: a systematic review. NPJ Microgravity 10, 10 (2024).
Guo, Z., Zhou, G. & Hu, W. Carcinogenesis induced by space radiation: a systematic review. Neoplasia 32, 100828 (2022).
Straume, T., Blattnig, S. & Zeitlin, C. Radiation hazards and the colonization of Mars: brain, body, pregnancy, in-utero development, cardio, cancer, degeneration. J. Cosmol. 12, 3992–4033 (2010).
Kim, S. Y., Kim, S. K., Lee, J. R. & Woodruff, T. K. Toward precision medicine for preserving fertility in cancer patients: existing and emerging fertility preservation options for women. J. Gynecol. Oncol. 27, e22 (2016).
Mishra, B., Ortiz, L. & Luderer, U. Charged iron particles, components of space radiation, destroy ovarian follicles. Hum. Reprod. 31, 1816–1826 (2016).
Wakayama, S. et al. Healthy offspring from freeze-dried mouse spermatozoa held on the international space station for 9 months. Proc. Natl Acad. Sci. USA 114, 5988–5993 (2017).
McNerlin C., et al. Targeting hippocampal neurogenesis to protect astronauts’ cognition and mood from decline due to space radiation effects. Life Sci. Space Res. 35, 170–179 (2022).
Acharya, M. M. et al. Consequences of ionizing radiation-induced damage in human neural stem cells. Free Radic. Biol. Med. 49, 1846–1855 (2010).
Cucinotta, F. A., Alp, M., Sulzman, F. M. & Wang, M. Space radiation risks to the central nervous system. Life Sci. Space Res. 2, 54–69 (2014).
Tseng, B. P. et al. Functional consequences of radiation-induced oxidative stress in cultured neural stem cells and the brain exposed to charged particle irradiation. Antioxid. Redox Signal. 20, 1410–1422 (2014).
Hetman, M. et al. Combined exposure to simulated microgravity and acute or chronic radiation reduces neuronal network integrity and survival. PLoS One 11, e0155260 (2016).
Steller, J. G., Alberts, J. R. & Ronca, A. E. Oxidative stress as cause, consequence, or biomarker of altered female reproduction and development in the space environment. Int. J. Mol. Sci. 19, 3729 (2018).
Yan, F. et al. The role of oxidative stress in ovarian aging: a review. J. Ovarian Res. 15, 100 (2022).
Man, J., Graham, T., Squires-Donelly, G. & Laslett, A. L. The effects of microgravity on bone structure and function. npj Microgravity 8, 9 (2022).
Li, F., Ye, Y., Lei, X. & Zhang, W. Effects of microgravity on early embryonic development and embryonic stem cell differentiation: phenotypic characterization and potential mechanisms. Front Cell Dev. Biol. 9, 797167 (2021).
Breeland, G., Sinkler, M. A. & Menezes, R. G. StatPearls (StatPearls Publishing LLC., 2024).
Ye, Y., Chen, X. & Zhang, W. Mammalian SWI/SNF chromatin remodeling complexes in embryonic stem cells: regulating the balance between pluripotency and differentiation. Front Cell Dev. Biol. 8, 626383 (2020).
Lei, X. et al. Effect of microgravity on proliferation and differentiation of embryonic stem cells in an automated culturing system during the TZ-1 space mission. Cell Prolif. 51, e12466 (2018).
Wang, Y., An, L., Jiang, Y. & Hang, H. Effects of simulated microgravity on embryonic stem cells. PLoS ONE 6, e29214 (2011).
Acharya, A. et al. Modulation of differentiation processes in murine embryonic stem cells exposed to parabolic flight-induced acute hypergravity and microgravity. Stem Cells Dev. 27, 838–847 (2018).
Blaber, E. A. et al. Microgravity reduces the differentiation and regenerative potential of embryonic stem cells. Stem Cells Dev. 24, 2605–2621 (2015).
Shinde, V. et al. Simulated microgravity modulates differentiation processes of embryonic stem cells. Cell Physiol. Biochem 38, 1483–1499 (2016).
Mishra, B. & Luderer, U. Reproductive hazards of space travel in women and men. Nat. Rev. Endocrinol. 15, 713–730 (2019).
Edsall, S. C. & Franz-Odendaal, T. A. An assessment of the long-term effects of simulated microgravity on cranial neural crest cells in zebrafish embryos with a focus on the adult skeleton. PLoS ONE 9, e89296 (2014).
Corydon, T. J. et al. Current knowledge about the impact of microgravity on gene regulation. Cells 12, 1043 (2023).
Marianna, S. Consequences of simulated microgravity in neural stem cells: biological effects and metabolic response. J. Stem Cell Res. Ther. 5, 6 (2015).
Espinosa-Jeffrey, A. Human neural stem cells in space proliferate more than ground control cells: implications for long-term space travel. J. Stem Cells Res. Dev. Ther. 7, 1–10 (2021).
Shaka, S., Carpo, N., Tran, V., Cepeda, C. & Espinosa-Jeffrey, A. Microgravity significantly influences neural stem cells size and numbers: implications for long-term space missions. J. Stem Cells Res. Dev. Ther. 7, 1–9 (2021).
Shaka, S., Carpo, N., Tran, V., Cepeda, C. & Espinosa-Jeffrey, A. Space microgravity alters neural stem cell division: implications for brain cancer research on earth and in space. Int. J. Mol. Sci. 23, 14320 (2022).
Biancotti, J. C. & Espinosa-Jeffrey, A. Metabolomic profiling of the secretome from human neural stem cells flown into space. Bioengineering 11, 11 (2023).
Han, Y. et al. Effects of microgravity on neural crest stem cells. Front Neurosci. 18, 1379076 (2024).
Usuda, H. et al. Artificial placenta support of extremely preterm ovine fetuses at the border of viability for up to 336 h with maintenance of systemic circulation but reduced somatic and organ growth. Front Physiol. 14, 1219185 (2023).
Usuda, H. et al. Successful use of an artificial placenta-based life support system to treat extremely preterm ovine fetuses compromised by intrauterine inflammation. Am. J. Obstet. Gynecol. 223, 755.e751–755.e720 (2020).
Usuda, H. et al. Artificial placenta technology: History, potential and perception. Placenta 141, 10–17 (2023).
Ghaffari, E. Ethics and practicality of childbirth in space. Int. J. Sci. Res. Arch. 13, 3331–3334 (2024).
Sharma, P., Malik, S. & Sarkar, A. Exploring the idea of human reproduction in space: a potential area for future research. Cureus 16, e73712 (2024).
Szocik, K. In Space and Society (ed D. A. Vakoch) 291 (Springer, Cham, Switzerland, 2020).
Szocik, K. The Bioethics of Space Exploration, Vol. 192 (Oxford University Press, 2023).
Mason, C. E. The Next 500 Years: Engineering Life to Reach New Worlds, Vol. 296 (MIT Press, 2021).
Bostrom, N. Existential risk prevention as global priority. Glob. Policy 4, 15–31 (2013).
Ord, T. The Precipice: Existential Risk and the Future of Humanity. (Hachette Books, 2020).
Musk, E. Making humans a multi-planetary species. N. Space 5, 46–61 (2017).
Cohen, A. & Cox, B. The Planets, Vol. 288 (William Collins, 2019).
Mathyk, B. et al. Understanding how space travel affects the female reproductive system to the Moon and beyond. npj Women’s Health 2, 1–19 (2024).
Rydze, R., Schutt, A., Gibbons, W. & Nodler, J. Gravity and embryo development. Curr. Obstet. Gynecol. Rep. 6, 51–54 (2017).
Szocik, K. & Reiss, M. J. The final frontier: what is distinctive about the bioethics of space missions? the cases of human enhancement and human reproduction. Monash Bioeth. Rev. 41, 87–102 (2022).
Edwards, M. R. Blueprint for forever: securing human far futures with ectogenesis. Futures 146, 103085 (2023).
Völke, L. & Wettmann, N. The process of pregnancy: paradoxical temporalities of prenatal entities. Hum. Stud. 44, 595–614 (2021).
Beauchamp, T. L. & Childress, J. F. Principles of biomedical ethics. 8th edn, Vol. 496 (Oxford University Press, 2019).
Beheshti, A. et al. Genomic changes driven by radiation-induced DNA damage and microgravity in human cells. Int. J. Mol. Sci. 22, 10507 (2021).
Lei, X., Cao, Y., Zhang, Y. & Duan, E. Life science in space: Experiments on board the SJ-10 recoverable satellite. In Research for development (eds E. Duan & M. Long) 281−315 (Springer, 2019).
Cheng, K. et al. Simulated microgravity reduces quality of ovarian follicles and oocytes by disrupting communications of follicle cells. npj Microgravity 9, 1–10 (2023).
Hyun, I., Wilkerson, A. & Johnston, J. Embryology policy: revisit the 14 day rule. Nature 533, 169–171 (2016).
Appleby, J. B. & Bredenoord, A. L. Should the 14 day rule for embryo research become the 28 day rule?. EMBO Mol. Med. 10, e9437 (2018).
Cavaliere, G. A 14 day limit for bioethics: the debate over human embryo research. BMC Med. Ethics 18, 38 (2017).
Blackshaw, B. P. & Rodger, D. Why we should not extend the 14 day rule. J. Med. Ethics 47, 712–714 (2021).
ISSCR. Guidelines for stem cell research and clinical translation. Stem Cell Rep. 16, 1398−1408 (2021).
Lovell-Badge, R. et al. ISSCR guidelines for stem cell research and clinical translation: the 2021 update. Stem Cell Rep. 16, 1398–1408 (2021).
Subbarraman, N. Limit on lab-grown human embryos dropped by stem-cell body. Nature 594, 18–19 (2021).
(UK), H. F. a. E. A. Human Fertilisation and Embryology Act 2008. https://www.legislation.gov.uk/ukpga/2008/22/contents (2008).
Schuster, H. & Peck, S. L. Mars ain’t the kind of place to raise your kid: Ethical implications of pregnancy on missions to colonize other planets. Life Sci. Soc. Policy 12, 10 (2016).
NASA. FAQs : The International Space Station Transition Plan. https://www.nasa.gov/faqs-the-international-space-station-transition-plan/ (2024).
Nations, U. Treaty On Principles Governing The Activities Of States In The Exploration And Use Of Outer Space, Including The Moon And Other Celestial Bodies. https://www.unoosa.org/oosa/en/ourwork/spacelaw/treaties/introouterspacetreaty.html (1967).
Layendecker, A. B. & Pandya, S. in Handbook of life support systems for Spacecraft and Extraterrestrial Habitats (eds E. Seedhouse & D. Shayler) 1−16 (Springer, 2019).
Acknowledgements
The authors report no specific funding for this work.
Author information
Authors and Affiliations
Contributions
V.M.C., J.S., M.A.C., and M.W.K. conceptualized and designed the project. V.M.C., J.S., S.E.I., F.B., P.B.A.T.B., Z.H., S.W.D.C. and M.W.K. wrote the manuscript. V.M.C. and M.W.K. edited the manuscript. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Cole, V.M., Savulescu, J., Illanes, S.E. et al. A biological and ethical assessment of whether humans could or should reproduce in space. npj Microgravity 11, 80 (2025). https://doi.org/10.1038/s41526-025-00535-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41526-025-00535-3
