
Abstract
Spaceflight stressors such as microgravity and radiation disrupt mitochondria in ocular tissues, leading to impaired energy production, oxidative stress, and reduced repair capacity. The anatomical distribution of mitochondria and disease localization presents an interesting relationship: cortical lens mitochondria align with the type of cataracts seen in spaceflight, while retinal mitochondria correspond to the pathology of SANS. These observations suggest mitochondrial damage may be more central to spaceflight-associated pathologies than previously recognized.
Similar content being viewed by others


Introduction
Spaceflight missions conducted to date have proven that the space environment imposes significant risks to the human eye. As the objectives of space missions have changed over the decades, so have the conditions that can affect astronauts’ ocular health. Apollo 11 astronauts reported seeing “light flashes” which presented as various shapes and colors that appeared intermittently in their vision1,2. Human space exploration progressed through numerous programs and cataract formation emerged as a recognized risk associated with human spaceflight3,4. Ocular health continued to be a focus during the Skylab and Space Shuttle eras, particularly as mission durations and stressors increased. The main hazards of spaceflight were recognized as elevated radiation exposure, microgravity, isolation and confinement, the significant distance from Earth, and the challenges posed by hostile, enclosed environments. As International Space Station (ISS) missions routinely extended mission durations to multiple months in Low Earth Orbit (LEO), Spaceflight Associated Neuro-Ocular Syndrome (SANS) was identified as a critical concern5. Characterized by a unique set of clinical features including optic disc edema, globe flattening, choroidal retinal folds, and hyperopic refractive error shifts, SANS can lead to decreased visual acuity. Thus, it has become a significant focus of human spaceflight research to understand the pathophysiology and what consequences the syndrome may have on short- and long-term visual impairment, structural changes to the eye and how these changes are managed during long-duration missions where advanced medical care may be limited. Currently, the exact pathophysiology of SANS is unknown, despite numerous hypotheses6,7.
On Earth, mitochondrial dysfunction can occur through genetic disorders, such as Leber Hereditary Optic Neuropathy (LHON) and Dominant Optic Atrophy (DOA), or because of other diseases processes, such as neurodegenerative disease and Type 2 Diabetes Mellitus8,9. Metabolic disturbances, particularly impaired vitamin B9 (folate) and B12 reduce glutathione synthesis and antioxidant defense, causing mitochondrial dysfunction. Impaired mitochondrial function blunts cellular metabolism, compromising energy needs and leading to potential cellular damage and loss of function which can result in cataracts, age-related macular degeneration, glaucoma, and other eye disorders10. There are multiple mechanisms by which damage occurs, such as mitochondrial DNA (mtDNA) damage, oxidative stress, and radiation. The mitochondrial genome is particularly prone to damage, and the accumulation of mutations leads to dysfunction and susceptibility to further damage10. It has been reported that mitochondrial DNA acquires mutations up to 100 times more often than nuclear DNA11. This is due to high levels of reactive oxygen species (ROS) in the mitochondria, lack of protective histones, and poor proofreading of mitochondrial DNA. Coupled with more frequent damage, mitochondrial DNA also has less ability to repair damage than nuclear DNA, and elements of the repair mechanism can be inactivated by oxidative stress10. The mitochondria are more likely to sustain oxidative damage because they are the primary site of the production of ROS10. Importantly, a moderate level of ROS is necessary for proper mitochondrial function12. The dysfunction results in disrupted energy production and increased oxidative stress, leading to cellular damage and visual loss. It is known that mitochondria are under significant stress during spaceflight, and there have been proposals that mitochondrial dysfunction may be a cause of SANS7.
As future missions extend beyond LEO, the environmental stressors are expected to be increased as well. Thus, it will be crucial for future research to explain the mechanism behind these conditions so that appropriate countermeasures are developed. This review explores how the spaceflight environment affects mitochondrial function and could potentially contribute to the development of SANS and other ocular pathologies in astronauts.
Space radiation environment
Astronauts are exposed to ionizing energy in space, including Van Allen Belt radiation, solar cosmic radiation, and galactic cosmic radiation (GCR). These radiation sources pose a risk to astronaut health and have been associated with visual anomalies13. Other negative biological effects of space radiation include an increased risk of cancer, deleterious effects on the central nervous system, and damage to the cardiovascular system.
The Van Allen Belts are formed by charged particles trapped within Earth’s geomagnetic field14. The Inner Belt is composed of protons and extends to an altitude of ~20,000 km. The Outer Belt consists of electrons and extends to ~30,000 km. Astronauts aboard the ISS are particularly vulnerable to radiation exposure when traveling through the South Atlantic Anomaly, an area of concentrated ionized particles where the Inner Belt extends into LEO15. Solar cosmic radiation consists of solar wind and solar particle events (solar flares). Solar wind is the constant flux of low-energy protons and electrons ejected by the sun. Solar particle events are intermittent bursts of photons, high energy protons, and electrons and high atomic number (“HZE,” or atomic number with ‘Z’ ≥ 2) particles15,16. Solar flares vary in frequency and intensity depending on the timeframe within the solar cycle. Surveillance is performed by terrestrial and space-based instruments, and astronauts aboard the ISS have procedures for emergency sheltering in the event of a strong solar flare. GCR is the continuous, omnidirectional flux of protons, electrons and, HZE particles originating outside the solar system. When GCR collides with other nuclei, such as spacecraft shielding, secondary radiation is produced, posing an additional hazard to astronaut health16.
Although most protons, especially high-energy ones, are considered low linear energy transfer radiation (low-LET), GCR consists of not only protons but also high-LET heavy-charged particles17. LET radiation ionizes and deposits energy in a medium (such as human tissue) as it travels along the path of the particle. It has been known that for a given absorbed dose, high-LET radiation induces greater levels of damage in biological systems17. The effectiveness of high-LET radiation is quantified through the relative biological effectiveness (RBE), defined as the ratio of the dose of gamma rays or X-rays to that of high-LET radiation that causes the same biological impact (RBE). RBE is 2–5 for survival of cells and can be as high as 30 for solid tumors.
While no RBE values for high-LET radiation-induced eye impacts in humans have been reported in the literature, the value is expected to be high. In studies with rats exposed to X-rays and Fe ions, the RBE—defined as the ratio of doses required to produce the same cataract incidence—was approximately 3018. In addition, the threshold dose for low-LET radiation-induced cataracts was estimated to be 0.5 Gy19; the data reported in this early study by Brenner et al. suggests that the threshold could be much lower for Fe ions18.
Radiation exposure among LEO, Lunar and Martian surfaces
The amount and type of radiation that astronauts are exposed to can be highly variable based on the type and length of mission, destination, solar cycles, and individual susceptibilities. Thus, standards have been put in place to protect the health of NASA astronauts with total career effective radiation dose limit of 600 mSv. As planning for missions to the Moon and Mars are underway, these limits are being re-evaluated.
When considering the effects of spaceflight, and thus radiation, on mitochondria it is important to understand what levels of radiation have been experienced previously and what can be expected in the future. Figure 1 illustrates the average radiation exposure for Earth surface, ISS, Lunar surface, and Martian surface are 2.6 mSv/year, 200 mSv/year, 380 mSv/year, and 260 mSv/year, respectively20,21,22,23. The recorded and estimated radiation doses of past and future missions are critical in evaluating risk. For example, the Apollo 14 mission was 9 days and recorded 11.4 mSv. It is estimated that total radiation dose from Artemis missions based on available data from the uncrewed Artemis I mission will be approximately 30 mSv but will vary based on duration and destination of the mission. Artemis I (Nov 2022) took approximately 25 days and was closer to a solar minimum, whereas the next maximum is expected around 2025. Based on current mission objectives, Artemis II (Feb–Apr 2026) is expected to take 20 days with a possible range of 10–45 days and is intended to go beyond the moon, further than any human mission to date. Artemis III (late 2028) is expected to last 45 days and will mark the return of human presence on the Moon. These variable mission objectives will therefore confer different radiation risks. Mars missions present a greater challenge as the current estimated dose based on two 180 day journeys and 500 days on the Martian surface is roughly 1000 mSv, which exceeds the current acceptable NASA career limit20. Astronauts are partially protected from this radiation by materials that constitute the spacecraft hull and possibly additional shielding within the spacecraft. Additionally, recent studies from Artemis I Lunar Mission indicate that a change in orientation of the spacecraft during proton-belt transit reduced the dose rate of radiation by approximately 50%, presenting a key countermeasure to reduce risk to the health of the crew24.

Average radiation dose per year (mSv/year) across multiple environments (blue) compared to total radiation dose (mSv) from previous and future missions (red) are depicted. Recorded and estimated total doses for specific missions, such as Apollo 14 (11.4 mSv), Artemis missions (~30 mSv), and Mars missions (~1000 mSv), are also presented, highlighting variability in radiation risk. This comparison illustrates how deep-space missions dramatically increased radiation exposure and exceed recommended limit. Therefore, methods of reducing exposure or mitigating the effects of sustained radiation will be essential as humans venture to Mars. Figure generated based on the following references25,20,21,22,23. This representation is based on averages as the actual radiation dose will vary based on the Solar Cycle. Estimation for Airline Pilot Career is based on 2 mSv/year across a 30-year career.
*Moon mission estimation is based on Artemis I data, approximately 25 days, and Mars mission is estimated for two 180-day journeys and 500 days on the Martian surface.
Measured ocular radiation exposure, such as radiotherapy, serves as a useful terrestrial analog to understand the risks of spaceflight radiation. Currently, the International Commission on Radiation Protection (ICRP) suggests a dose limit from occupational exposure to 20 mSv per year averaged over 5 years with no single year greater than 50 mSv, with the same amounts applying to the lens of the eye. One of the most studied groups exposed to radiation in the eye are patients being treated for cancer of the orbit or nearby structures. In comparison to spaceflight radiation exposure which is typically reported in mSv to reflect effective dose and account for variable biologic impact, health effects due to radiation therapy (RT) such as cataractogenesis or retinal damage are reported in Gy which measures the exact energy delivered during treatment (Fig. 2). Patients treated for orbital cancer with RT dose greater than 2.5–6.5 Gy increase risk of cataracts by 33% and doses greater than 6.51–11.5 Gy increases risk by 66%26. These effects were worsened by higher doses given during a shorter period of time. Thresholds for radiation-induced retinal damage are typically greater than 30 Gy with risk greatly increasing above 50 Gy26. RT induces radiation retinopathy which leads to loss of capillary endothelial cells and pericytes which manifests clinically as microaneurysms, cotton wool spots, and neovascularization among other signs, sharing some similarities to SANS27. Importantly, there are key differences between patients exposed to radiation as a form of treatment and astronauts exposed during spaceflight. The former group receives focal, high-dose radiation that can lead to rapid, irreversible losses in vision while SANS develops under low, chronic, and mixed radiation exposure which have not been associated with permanent changes. For both lens and retinal radiation injury, the severity of the injury is highly dependent on the location. Small and stationary lens injuries may have minimal impact on vision and retinal injuries may become significantly more disabling if there is macular involvement26. Additionally, studies show that there is a latency period between radiation treatment and symptoms onset correlated with radiation dose, fraction size, and radiation field28.

Estimated radiation exposure in Gy in MALT Lymphoma, a form of cancer where radiation therapy to the eye is common. Notably, the amount of radiation an individual is exposed to can vary drastically during treatment (20–70 Gy) which will cause variable effects. Airline Pilot Career exposure is based on an estimate of 0.85 mGy per year across a 30 year career29. These thresholds suggest that even relatively low-dose radiation may induce mitochondrial or ocular changes, raising concern for astronauts exposed to mixed radiation fields in space. Translating these values to mSv is challenging because the effective dose is dependent on radiation weighting factors and tissue sensitivities, particularly under spaceflight conditions where high-LET radiation dominates. Therefore, while Fig. 1 contextualizes mission dose profiles, Fig. 2 shows experimental and clinical thresholds that emphasize risk for ocular pathology.
Initial evidence of visual anomalies caused by space radiation
The earliest ophthalmic phenomena associated with spaceflight include light flashes and cataractogenesis. Ionizing radiation has been identified as a primary or contributing factor in these conditions.
Light flashes were predicted in 1952 by biophysicist Cornelius Tobias and first reported by Buzz Aldrin in 1969 following Apollo 111,2. They are a common phenomenon in spaceflight and are described as spots, stars, streaks, or clouds appearing in one or both eyes. Color perception is predominantly white, though other colors are also reported. Several mechanisms have been proposed to explain light flashes, including photon emission from particles slowed within eye humor (Cherenkov radiation), light emission from particles ionizing within eye humor, and light stimuli from radiation interacting with the retina15. The Anomalous Long-Term Effects on Astronauts study in 2006–07 was the first to report ion-flux through the eyes of astronauts with LF perception30. There is currently no evidence linking LF to ophthalmic pathology.
Cataractogenesis was associated with ionizing radiation in the 1940s after being found in nuclear physicists working with cyclotrons and in victims of the Hiroshima and Nagasaki bombings. In 2009 and 2012, the NASA Study of Cataract in Astronauts (NASCA) described higher rates of cortical cataract formation and progression in astronauts who had flown in space, compared to controls including astronauts who had not flown to space and military aircrew personnel3,4. Cataractogenesis is considered a multifactorial disease process, and radiation dose limits for astronauts have been established by NASA for the prevention of early (< 5 years) severe cataract development.
Microgravity environment
Pathologic effects of microgravity on the musculoskeletal, cardiovascular, and immune systems have been documented in human and animal models31,32,33. The nervous system, and more specifically the eye and its supporting structures, also undergo significant changes in response to the microgravity environment34,35. Numerous experiments has shown that microgravity leads to oxidative stress and possibly cell death in retinal cells: vertebrate retinal cells in vitro and mice aboard ISS showed increased inflammation, fish studies showed increased expression of stress-related genes within the retina, and a human RPE cell line (ARPE19) demonstrated activation of signaling pathways leading to oxidative stress, increased ROS production, and apoptosis36. Simulated microgravity experiments (through the rotating wall vessel bioreactor) have also shown that human retinal pigmented epithelial (RPE) cells develop inflammatory responses37.
Arguably the most important ocular manifestation of extended microgravity exposure is SANS. It has become a focal point of human spaceflight research in recent years due to the prevalence among astronauts and potential implications. Two of the hypothesized etiologies of SANS are cerebrospinal fluid dysregulation due to cephalad fluid shifts that occur in extended microgravity exposure, and accumulation of cerebrospinal fluid within the optic nerve sheath38. The cephalad shift impairs resorption of CSF at the arachnoid granulations and reduces translaminar gradient across the optic nerve head, causing edema and globe flattening. Accumulation in the optic nerve sheath may be due to impaired drainage (venous or lymphatic) and causes compression of the optic nerve. This compression may impair axonal transport and lead to some of the described structural changes that define SANS. Other hypotheses have proposed that changes due to microgravity will be more pronounced in larger individuals because of greater pressure changes39. There have also been suggestions that the changes in SANS may be related to mitochondrial changes7. When taken together these data, observations, and theories indicate SANS may be a multifactorial consequence of the spaceflight environment.
Spaceflight effects on mitochondria function
Spaceflight has previously been shown to impact oxidative phosphorylation and induce mitochondrial dysfunction. A comprehensive multi-omics analysis from human and animal samples in space also identified mitochondrial dysregulation as a central hub across different species and organ tissues40. The impact of spaceflight on mitochondria has also been reported previously in the muscle tissue from rats41,42. In fact, some of the earliest traces of spaceflight-induced mitochondrial dysfunction came from mice studies. Transcriptomic analysis of C57BL/6 and BALB/C mice from the Rodent Research (RR) missions, RR1 and RR3, showed gene expression changes in mitochondrial pathways in kidney, liver, and ocular tissues40. Interestingly, gene alterations in energy-related pathways involving mitochondria varied based on tissue location. Another study using female C57BL/6 mice that were flown in space for a 13-day mission (Space Shuttle mission STS-135) demonstrated that spaceflight-induced ROS dysregulates mitochondria in ocular tissue43.
Human studies, such as an astronaut in the NASA Twins Study44, have also shown mitochondrial dysfunction as a prominent phenotype during spaceflight7. Prolonged exposure (~6 months) to space conditions reduced mtDNA and mtRNA production in astronauts’ hair follicles45. The cell-free mitochondrial DNA concentration in circulating blood increased in astronauts and has been a suggested biomarker for stress or immune responses related to environmental space factors46. Furthermore, proteome analysis conducted on astronauts revealed the downregulation of the mitochondria, including the inner membrane and matrix47. Similar to studies on mice, it was demonstrated that mitochondrial dysfunction in astronauts occurred in a variety of tissues and was not localized to any specific region. This is notable because comparisons are often drawn between SANS and LHON, where mtDNA mutations impair oxidative phosphorylation, increase ROS production, causing a pseudo edema secondary to microangiopathy. Although LHON primarily affects the eye, the mechanism by which damage takes place is similar to mitochondrial damage which would theoretically contribute to SANS. The fact that a primary mitochondrial defect can directly cause optic neuropathy underscores that mitochondrial dysfunction may be critically important in understanding the downstream pathophysiology of SANS.
Mitochondria and the eye
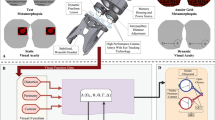
The human eye and visual system are highly intricate and metabolically active. It is one of the most energy-demanding systems within the brain48. This demand is met by an abundance of mitochondria, especially within the retina and periphery of the lens. Within the eye, mitochondria have a distinct distribution based on where energy is needed and where transparency for the passage of light is needed. For example, mitochondria are distributed throughout the retina, with the greatest amount in the fovea, where cones are predominant49. A retinal area of particular importance is the RPE, which supports retinal ganglion cell function by regulating metabolism and redox balance. When these mitochondria are impaired, excess ROS accumulate and complex 1 of the electron transport chain becomes dysfunctional, disrupting energy supply and providing a mechanistic link to optic diseases such as LHON, DOA, and Leigh Syndrome. Comparatively, in the lens, mitochondria are highly abundant in the epithelium and differentiating fibers but absent in the core, where transparency is necessary for unimpeded light passage50 (Fig. 3).

Illustration of the anatomy of the human eye with expansions of the lens (left) and retina (right). Expanded images display green shading to represent relative abundance of mitochondria with the highest in the fovea and macula, followed by the retina, cuboidal epithelium, then differentiating fibers. The mature fibers and nucleus of the lens are shaded blue to indicate an absence of mitochondria. This distribution is key in the argument that the ocular pathology that astronauts develop is related to mitochondrial damage as evidenced by the pathology that develops: peripheral (cortical) cataracts, and retinal vascular/nerve damage leading to SANS.
The type of damage and mechanistic sequence that follows is crucial to understanding how mitochondria are impacted during spaceflight. As oxidative damage occurs and excess ROS accumulate, mutations occur at a much higher rate within the mitochondrial genome due to a lack of protected histones and limited repair capacity. These mutations disrupt the complexes of the electron transport chain (ETC), especially complex 1 leading to impaired oxidative phosphorylation, reduced ATP production, and excess ROS51. This elevation in ROS damages mitochondrial proteins and lipids, creating a feed-forward cycle of destruction and a dysregulation of mitochondrial autophagy11. The net result is compromised photoreceptor survival and RPE support of ganglion cells. Ionizing radiation is linked to the oxidative damage previously discussed and is especially damaging to sensitive cells within structures like the lens52. It can also lead to fragmentation of the mitochondria, collapsing the membrane potential and compounding on the effects described above53. Therefore, maintaining mitochondrial function is critical in preventing ocular damage during spaceflight.
Lens and cataracts
Cataracts are an eye condition affecting the lens characterized by clouding and distorted passage of light to the retina. This clouding results from modification and damage to crystalline proteins within the lens. Notably, the lens is the most hypoxic tissue in the human body, retaining minimal cellular machinery to maximize uninterrupted passage of light to the retina54. Numerous factors can contribute to the development of cataracts, such as protein cross-linking, aggregation, and oxidation55. The majority of cataracts are classified as one of three types based on the location within the lens. Cortical cataracts occur in the equatorial area of the lens and can cause glare and photophobia. Nuclear cataracts are most common, occurring in the center of the lens and are associated with aging. Posterior subcapsular cataracts develop anterior to the posterior capsule and thus have the potential to impair vision significantly56. Cataracts can also be of congenital origin caused by mutations that result in protein damage and lead to an unfolded protein response and apoptosis of the cells of the lens57.
The development of cataracts was noted in astronauts across numerous programs. To investigate this phenomenon, the NASCA was conducted. Astronauts exposed to space radiation had a significantly higher rate of cortical cataracts compared to controls (astronauts who had not flown in space, military aircrew, and ground comparison subjects). Progression of cortical cataracts was associated with increasing radiation dose and astronaut age. Conversely, there was no association between radiation and the progression of nuclear cataracts or aggregate area of posterior subcapsular cataracts4. Cataract development has also been compared between military aviators and astronauts. Findings from these studies suggest that cataract development in military aviators occurred at a younger age and with decreased prevalence. Additionally, the military aviators’ cataracts occur predominantly in the posterior subcapsular region, while astronauts develop cataracts in the cortical region58. Ophthalmologic studies on airline pilots have suggested cosmic radiation as a causative factor in the development of nuclear cataracts59. However, there is limited evidence of an increased prevalence of cataracts in commercial airline pilots60.
The maintenance of a habitable spacecraft atmosphere has been the subject of many engineering challenges and successes throughout the decades. Importantly, the early human spaceflight missions (Mercury, Gemini, Apollo) took place in spacecraft that used a 100% oxygen atmosphere, while more recent missions (Shuttle and ISS) use a 21% oxygen atmosphere that more closely mimics earth-like sea-level atmosphere. The high oxygen environment in the early spacecraft was likely an important driver of oxidative stress associated with increased cataractogenesis54. Thus, a proposed “Goldilocks Range”54 that maintains physiologic conditions is necessary to prevent deviation from homeostasis to mitigate risk of disease. Military aviators flying high performance aircraft breath 100% O2 during flight, thus predisposing them to a high oxygen environment and indicating a possible cause of oxidative stress and cataracts. Although these commonalities may provide some insight as to the development of cataracts, questions remain as to why certain groups are more susceptible to particular types of cataracts.
Cataract formation is a multifactorial process and includes mitochondrial damage and ionizing radiation. In addition to reduced mitochondrial function and weak repair mechanisms in response to oxidative stress, ionizing radiation is another known cause of cataractogenesis to which the human lens is especially sensitive52. The result of ionizing radiation within the lens is damage to DNA base pairs, membranes, and lysosomes. This can result in abnormal proliferation and differentiation of lens epithelial cells, greater oxidative stress, and aggregation of crystallin proteins52. The most frequent result of this type of radiation damage is posterior subcapsular cataracts61. Importantly, there is not a clear threshold of ionizing radiation that induces the development of cataracts in the human eye52. A notable difficulty is determining the effect of ionizing radiation on the development of cataracts because of whether it affects mitochondria or other parts of the lens. Also, it will be important in future studies to determine if and how different forms of radiation (GCR, trapped radiation, and solar particle events) lead to the development of cataracts62,63.
The effects of ionizing radiation in the development of cataracts are not only limited to lens cells but also affect mitochondria that are present within the epithelium of the lens. As stated previously, mitochondrial DNA is more susceptible to damage than nuclear DNA. Similar to other forms of mitochondrial damage, radiation can also alter function, increase oxidative stress, and ultimately lead to apoptosis of the mitochondria64. Alternatively, ionizing radiation can increase the mitochondrial DNA copy number and the total number of mitochondria, which has been noted as a response to oxidative stress64. This results in a possible increase in the production of ROS and damage signals being perpetuated64.
As previously mentioned, ionizing radiation is linked to mitochondrial damage and oxidative stress within the lens. Additionally, systemic oxidative stress can play a role in the development of cataracts65. Based on these data, it is plausible that the development of cataracts in astronauts is multifactorial and can be attributed partially to each effect. Mitochondrial stress is a well-documented effect of spaceflight and results in ribosomal and translational changes, altered metabolites, reduced antioxidant defenses, increased oxidative stress, and impaired ocular lipid metabolism40. The association of spaceflight and the development of cortical cataracts may be explained by the association of mitochondrial oxidative stress and the effect of ionizing radiation on both protein modification and mitochondrial damage. As the mitochondria within the epithelium are performing metabolism, homeostasis, and antioxidant activities, the types of damage explained above may impact the mitochondria and differentiating lens fibers in the periphery50. These effects would lead to protein modifications and altered mitochondrial function, resulting in the characteristic opacification of the outer portions of the lens. Parkin is a protein that counteracts ROS within lens epithelial cells. Thus, it could be used to study its activity and effects on ocular tissue undergoing characteristic spaceflight-related oxidative stress66. Other markers, such as 4-HNE and 8-OHdG (both products of lipid peroxidation, frequently measured in the urine), which indicate general oxidative stress, are possible biomarkers to be explored specifically within the lens11,67. Proteomic analysis can be used to evaluate mitochondrial inner membrane and matrix proteins, as it has been shown that energy related pathways are altered during flight which is consistent with impaired oxidative phosphorylation40. Use of these markers (4-HNE, 8-OHdG, cell free mitochondrial DNA, and proteomic analysis) in conjunction with ocular measurement tools currently aboard ISS such as Optical Coherence Tomography (OCT) and Angiography (OCTA) could provide a comprehensive assessment of molecular damage, anatomical changes, and blood flow dynamics, correlated with symptoms experienced by astronauts. The awareness of increased oxidative stress has also led to suggestions for antioxidant therapy during spaceflight, which may benefit cataracts and other consequences of the stresses of spaceflight67. Newer antioxidant therapies are frequently referred to as “cocktails” due to the need to target multiple metabolic pathways and account for individual susceptibilities, as well as mission specific needs. Gómez et al. propose a workflow that emphasizes early identification of ROS vulnerability, continuous inflight ROS monitoring, and personalized formulations68. In addition to antioxidants received through diet, supplemental N-acetylcysteine, vitamins B9, B12, C, and E have been proposed as countermeasures but require proper dosing and safety validation. There have been developments of pharmacologic antioxidants such as MitoQ which neutralizes ROS and protects the mitochondrial membrane, and Elamipretide which stabilizes mitochondrial structure and enhances ETC efficiency69,70. However, these medications carry numerous side effects that may confer a greater risk than the consequences of spaceflight and would require intense examination of their efficacy.
Retina and SANS
The retina is essential for processing vision and requires an abundance of energy generated by mitochondria to do so. On a per mass basis, the retina consumes the most oxygen of any tissue in the human body, and its neurons have the greatest metabolic rate of any cell within the central nervous system71. The retina consists of 10 layers and 6 cell types, with the outer retina, photoreceptors, and retinal pigment epithelium containing the most mitochondria72. As discussed previously, these mitochondria are especially prone to damage from stressors such as oxidative stress, mtDNA alteration, and radiation. Spaceflight conditions can induce oxidative stress in the retina and can damage sensitive rod and cone photoreceptors, which, like mitochondria, are more susceptible to environmental damage than other cell types73. It has been shown that oxidative stress will diminish the function of the murine retina, cause degradation of photoreceptors, and lead to subsequent apoptosis in the inner and outer nuclear layers73. The result of this damage is decreased thickness of the retinal structures and loss of capillarization, implicating spaceflight in retinal degeneration and vision loss73. This compromise in the vascular integrity is a plausible mechanism that underlies the optic disc edema and choroidal folds seen in SANS. Other studies have shown similar results of microgravity and spaceflight environments impairing retinal vasculature and causing oxidative stress in humans36.
Retinal function decreases with age and systemic disease, such as age-related macular degeneration and diabetic retinopathy10. Much of this effect on the retina can be attributed to processes that occur in mitochondria. Mitochondria in older study subjects provide less energy production through oxidative phosphorylation, have increased ROS generation, and have increased mtDNA mutations71. Baseline rate of ROS production is necessary for normal mitochondrial function. However, excess ROS will cause oxidative damage to DNA, lipids, and proteins12,71. The total number of mitochondria in the retina will decrease with age through normal mitochondrial autophagy. This process, called mitophagy, becomes less efficient in recycling old and faulty mitochondria, leading to an increased proportion within the retina12. Characteristic morphologic changes in aged mitochondria, include organelle rounding with disorganized cristae and accumulation of lipofuscin12. These changes become even more pronounced in diseases of aging, such as age-related macular degeneration, where there is major membrane disorganization, substantial loss of cristae, and drusen accumulation12. It has been suggested that space flight is, in some ways, representative of accelerated aging74. This includes the visual changes that occur with spaceflight. Experiments in mice have shown that spaceflight, like aging, increases oxidative stress and apoptosis of the inner nuclear layer75. More specifically Overbey et al. demonstrated mice flown on ISS for 35 days showed approximately 17% loss of total retinal thickness (0.064 mm vs 0.077 mm), 21% in the RPE (0.030 mm vs 0.038 mm), and 22% in the choroid (0.032 mm vs 0.041 mm)73. Thus, astronauts may have a greater risk of developing late retinal degeneration from accumulated mitochondrial damage75.
The retina, similar to the lens, is susceptible to damage from radiation. Although the accumulated dose during a 6-month mission is in the order of several cGy, high-LET radiation at low doses can cause mitochondrial dysfunction. Very few studies have been published to compare low- and high-LET effects on mitochondria. Among them, mitochondria fragmentation was reported in Hela cells after carbon ion exposure in a dose and LET-dependent manner. However, fragmentation was observed by X-rays only when the dose reached 1 Gy76. Results from investigations of non-targeted (bystander) effects may also suggest greater impacts of high-LET radiation on the mitochondria. In non-targeted studies, mutations and other changes in the nuclear DNA were detected in cells hit by high-LET charged particles in the cytoplasm77. These non-targeted effects were believed to be mediated by mitochondria78. These effects are unique to high-LET radiation. Targeted irradiation with charged particles has also been shown to cause loss of the mitochondria membrane potential79. Experiments in mice have shown that radiation doses as low as 0.1 Gy led to oxidative damage and apoptosis of the retina and retinal endothelial cells, with additional differences between radiation types80. A recent study revealed dose-dependent effects of radiation on mitochondria within microvascular endothelial cells81. Low doses of radiation caused abnormal elongation of mitochondria without fragmentation and swelling, leading to an increase in the survival of the endothelial cells81. Future studies should investigate the morphologic and functional effects of spaceflight-like radiation on mitochondria in the retina. Additionally, it will be important to determine the interplay between structure and function, and whether these effects will counteract one another or be additive or synergistic.
Many of the ocular pathologies discussed so far occur terrestrially with age or disease. One disease of particular concern to astronauts is SANS, a syndrome that occurs in as much as 40−60% of astronauts, more so in those who fly long-duration missions82. SANS is characterized by a set of signs and symptoms, including optic disc edema, globe flattening, choroidal retinal folds, and hyperopic refractive error shifts38. Waisberg et al. have hypothesized that mitochondrial dysfunction is implicated in the development of SANS7. In addition to the types of mitochondrial stresses discussed previously, alterations in B vitamin metabolism may be another contributing factor to mitochondrial damage and SANS development7. In astronauts with ophthalmologic signs and/or symptoms, serum folate was low during spaceflight, and methylmalonic acid was increased after spaceflight83. Folate (vitamin B9) is necessary for the metabolism of glutathione, which is an essential antioxidant in mitochondria, and elevated methylmalonic acid is a marker for functional vitamin B12 deficiency, which is necessary for the synthesis of folate and glutathione84. As these vitamins are essential for redox balance within mitochondria, these systemic changes could exacerbate retinal vulnerability to oxidative stress and result in microvascular damage and characteristic findings of SANS. To study SANS, strict Head-Down Tilt Bed Rest studies have been used as an analog of spaceflight effects. Some signs of SANS, such as choroidal folds, hyperopic shift, and cotton wool spots, have not yet been replicated in analog studies85. Many factors, such as fluid shift and intracranial pressure changes, have been hypothesized as factors related to the development of SANS. Future best rest studies might consider the effect that impaired mitochondrial function has on endothelial cell function within the vasculature of the eye and if this contributes to SANS.
The severity, progression, and outcome are key considerations in the exploration of mitochondrial involvement in cataracts and SANS. Cataracts are an irreversible ophthalmic disease that develop over a period of months to years. Even among astronauts who developed severe cortical cataracts, there was no impairment to vision for up to several years after being diagnosed4. In SANS, the progression can be rapid, occurring within weeks, causing visual impairment in some astronauts during both short and long-duration missions38. However, there have been no reports of permanent vision changes in astronauts who develop SANS, and it is uncertain if symptoms will persist and how much of normal vision will be regained38. One factor that could contribute to the difference in the rate of onset of these conditions is the efficiency with which nutrients can reach the given structures. For example, lens cells (especially those in the nucleus) rely on slow and passive diffusion of few nutrients and antioxidants to defend against damage11. The lens also requires significantly less energy. Comparatively, cells within the retina have a significant blood supply and make a large amount of energy, ROS, and antioxidants11. SANS and cataracts are distinct conditions but may be related in that mitochondrial damage could play a larger role in driving the disease process than currently understood. A recent study has theorized that the cotton-wool spots characteristic of SANS may be due to radiation in the posterior segment of the lens, further supporting the contention that SANS is a multifactorial consequence of the stressors of spaceflight61. Future missions will be important to better understand these connections and differences in ocular disease in spaceflight and how maintaining mitochondrial function may be a preventive measure.
Conclusion
Spaceflight has many effects on ocular health and the development of ocular pathologies. As mission duration and associated stressors have changed in recent decades, so has the manifestation of ocular issues. Planned missions beyond LEO will have unique profiles, and the demands of these missions will undoubtedly increase the stressors experienced by astronauts. Mitochondria have been identified as a target of the damaging effects of spaceflight. Thus, understanding the effects of spaceflight on mitochondria in the eye (and throughout the body) will be crucial in developing countermeasures to preserve the health of astronauts on long-duration missions where advanced care is not easily accessible. Future studies aimed at elucidating the relative impact that the identified stressors have on mitochondrial function are warranted. In particular, a greater understanding of the RBE impact of protons and high-LET charged particles on mitochondria in the eye will be significant due to limited knowledge of how damaging the effects may be. Additionally, topics of focus that will establish a more thorough understanding include how different forms of radiation will impact mitochondrial function in the lens and retina in vivo, what morphologic changes occur in mitochondria during spaceflight and the impact on function, and what leads to greater susceptibility to ocular conditions in astronauts. Mitigating and preventing ocular (and other) diseases in astronauts will depend on a thorough understanding of the role of mitochondria in health and disease. These discoveries will support further exploration and the advancement of human spaceflight, while contributing to our understanding of biochemical underpinnings of human health and disease on Earth.
Limitations
This review synthesizes evidence from astronaut studies, animal models, and cellular experiments to evaluate the role of mitochondrial dysfunction in ocular pathology during spaceflight. There are multiple limitations that should be acknowledged. First, much of this mechanistic evidence is derived from analog or in vitro studies, which cannot fully replicate the complex radiation environment and microgravity conditions of spaceflight. Second, the thresholds for radiation doses that lead to mitochondrial damage are not completely defined, even more so in mixed radiation fields that include low and high LET components. Third, the effect size of systemic metabolic challenges imposed by spaceflight and local mitochondrial dysfunction within the eye are not delineated, making determination of origin difficult. Fourth, the sample size of subjects that travel to space and may develop SANS is small and creates challenges understanding nuances and patterns of pathogenesis and disease characteristics.
Future research
Future investigations should prioritize integrating data from multiple domains (biomarker, imaging, and functional changes) in subjects to attempt to correlate mitochondrial dysfunction with structural and functional ocular changes. Prospective studies should be designed to evaluate antioxidant formulations across possible mission radiation profiles. It would be beneficial for future studies to more precisely determine the thresholds for mitochondrial injury in retinal and lens tissue. To evaluate radiation effects, in vitro studies of human retinal endothelium, RPE, and lens epithelial cells exposed to low and high LET beams (0.05 Gy to 0.5 Gy) followed by measurement of membrane potential, ROS, oxidative phosphorylation, ETC activity, mtDNA damage, and mitochondrial autophagy would provide valuable insights. Evaluating these measures with parallel countermeasures could investigate their efficacy. Analogs such as head-down tilt bed rest will remain critical in modeling the spaceflight environment to understand ocular pathophysiology. In addition to more contextual understanding of current biomarkers, the discovery of novel ocular biomarkers could offer tremendous insight for evaluating ocular damage in spaceflight and preserving human health on future deep-space missions.
Data availability
No datasets were generated or analysed during the current study.
References
Tobias, C. A. Radiation hazards in high altitude aviation. J. Aviat Med. 23, 345–372 (1952).
NASA Mission Operations Branch Flight Crew Support Division. Apollo 11 Technical Crew Debriefing. (1969).
Chylack, L. T. et al. NASA Study of Cataract in Astronauts (NASCA). Report 1: cross-sectional study of the relationship of exposure to space radiation and risk of lens opacity. Radiat. Res. 172, 10–20 (2009).
Chylack, L. T. et al. NASCA Report 2: longitudinal study of relationship of exposure to space radiation and risk of lens opacity. Radiat. Res. 178, 25–32 (2012).
Mader, T. H. et al. Optic disc edema, globe flattening, choroidal folds, and hyperopic shifts observed in astronauts after long-duration space flight. Ophthalmology 118, 2058–2069 (2011).
Ong, J., Mader, T. H., Gibson, C. R., Mason, S. S. & Lee, A. G. Spaceflight associated neuro-ocular syndrome (SANS): an update on potential microgravity-based pathophysiology and mitigation development. Eye 37, 2409–2415 (2023).
Waisberg, E. et al. Mitochondrial dysfunction in Spaceflight Associated Neuro-Ocular Syndrome (SANS): a molecular hypothesis in pathogenesis. Eye 38, 1409–1411 (2024).
Schrier, S. A. & Falk, M. J. Mitochondrial disorders and the eye. Curr. Opin. Ophthalmol. 22, 325 (2011).
Baduini, I. R. et al. Type 2 diabetes mellitus and neurodegenerative disorders: the mitochondrial connection. Pharmacol. Res. 209, 107439 (2024).
Jarrett, S. G., Lewin, A. S. & Boulton, M. E. The importance of mitochondria in age-related and inherited eye disorders. Ophthalmic Res. 44, 179–190 (2010).
Shu, D. Y. et al. Role of oxidative stress in ocular diseases: a balancing act. Metabolites 13, 187 (2023).
Tong, Y., Zhang, Z. & Wang, S. Role of mitochondria in retinal pigment epithelial aging and degeneration. Front. Aging 3, 926627 (2022).
Waisberg, E. et al. Radiation-induced ophthalmic risks of long duration spaceflight: current investigations and interventions. Eur. J. Ophthalmol. 34, 1337–1345 (2024).
Horne, R. B. et al. Wave acceleration of electrons in the Van Allen radiation belts. Nature 437, 227–230 (2005).
Clement, G. & Slenzka, K. Fundamentals of Space Biology: Research on Cells, Animals, and Plants in Space. (Springer, New York, 2006).
Buckey, J. C. Space Physiology (Oxford University Press, 2006).
Report No. 098 – Guidance on Radiation Received in Space Activities (1989) - NCRP | Bethesda, MD. https://ncrponline.org/shop/reports/report-no-098-guidance-on-radiation-received-in-space-activities-1989/ (2018).
Brenner, D. J., Medvedovsky, C., Huang, Y. & Worgul, B. V. Accelerated heavy particles and the lens. VIII. Comparisons between the effects of acute low doses of iron ions (190 keV/microns) and argon ions (88 keV/microns). Radiat. Res. 133, 198–203 (1993).
Frey, G. D. Radiation cataracts: new data and new recommendations. Am. J. Roentgenol. 203, W345–W346 (2014).
Tomsia, M. et al. Long-term space missions’ effects on the human organism: what we do know and what requires further research. Front. Physiol. 15, 1284644 (2024).
Reitz, G., Berger, T. & Matthiae, D. Radiation exposure in the moon environment. Planet. Space Sci. 74, 78–83 (2012).
Dishongh, L. Moon to MARS (M2M) LUNAR SURFACE DATA BOOK (National Aeronautics and Space Administration, 2025).
Hassler, D. M. et al. Mars’ surface radiation environment measured with the Mars Science Laboratory’s Curiosity rover. Science 343, 1244797 (2014).
George, S. P. et al. Space radiation measurements during the Artemis I lunar mission. Nature 1–5, https://doi.org/10.1038/s41586-024-07927-7 (2024).
Hendry, J. H. et al. Human exposure to high natural background radiation: what can it teach us about radiation risks? J Radiol. Prot. 29, A29–A42 (2009).
Jeganathan, V. S. E., Wirth, A. & MacManus, M. P. Ocular risks from orbital and periorbital radiation therapy: a critical review. Int. J. Radiat. Oncol.*Biol.*Phys. 79, 650–659 (2011).
Oakey, Z., Yeşiltaş, Y. S. & Singh, A. D. Radiation optic neuropathy: management options. Ocul Oncol. Pathol. 9, 166–171 (2023).
Nuzzi, R. et al. Ocular complications after radiation therapy: an observational study. Clin. Ophthalmol. 14, 3153–3166 (2020).
Grajewski, B. et al. Airline pilot cosmic radiation and circadian disruption exposure assessment from logbooks and company records. Ann. Occup. Hyg. 55, 465–475 (2011).
Narici, L. et al. ALTEA: anomalous long term effects in astronauts. A probe on the influence of cosmic radiation and microgravity on the central nervous system during long flights. Adv. Space Res. 31, 141–146 (2003).
Akiyama, T. et al. How does spaceflight affect the acquired immune system? npj. Microgravity 6, 1–7 (2020).
Juhl, O. J. et al. Update on the effects of microgravity on the musculoskeletal system. npj Microgravity 7, 1–15 (2021).
Patel, S. The effects of microgravity and space radiation on cardiovascular health: From low-Earth orbit and beyond. Int. J. Cardiol. Heart Vasc 30, 100595 (2020).
Taibbi, G., Cromwell, R. L., Kapoor, K. G., Godley, B. F. & Vizzeri, G. The effect of microgravity on ocular structures and visual function: a review. Surv. Ophthalmol. 58, 155–163 (2013).
Mao, X., Stanbouly, S., Holley, J., Pecaut, M. & Crapo, J. Evidence of spaceflight-induced adverse effects on photoreceptors and retinal function in the mouse eye. Int. J. Mol. Sci. 24, 7362 (2023).
Grigoryan, E. N. Impact of microgravity and other spaceflight factors on retina of vertebrates and humans in vivo and in vitro. Life 13, 1263 (2023).
Roberts, J. E. et al. Simulated microgravity induced damage in human retinal pigment epithelial cells. Mol. Vis. 12, 633–638 (2006).
Lee, A. G. et al. Spaceflight associated neuro-ocular syndrome (SANS) and the neuro-ophthalmologic effects of microgravity: a review and an update. NPJ Microgravity 6, 7 (2020).
Buckey, J. C. et al. Microgravity-induced ocular changes are related to body weight. Am. J. Physiol. Regul. Integr. Comp. Physiol. 315, R496–R499 (2018).
da Silveira, W. A. et al. Comprehensive multi-omics analysis reveals mitochondrial stress as a central biological hub for spaceflight impact. Cell 183, 1185–1201.e20 (2020).
Nikawa, T. et al. Skeletal muscle gene expression in space-flown rats. FASEB J. 18, 522–524 (2004).
Michaletti, A., Gioia, M., Tarantino, U. & Zolla, L. Effects of microgravity on osteoblast mitochondria: a proteomic and metabolomics profile. Sci Rep. 7, 15376 (2017).
Mao, X. W. et al. Biological and metabolic response in STS-135 space-flown mouse skin. Free Radic. Res. 48, 890–897 (2014).
Garrett-Bakelman, F. E. et al. The NASA twins study: a multidimensional analysis of a year-long human spaceflight. Science 364, eaau8650 (2019).
Indo, H. P. et al. Changes in mitochondrial homeostasis and redox status in astronauts following long stays in space. Sci Rep. 6, 39015 (2016).
Bisserier, M. et al. Cell-free mitochondrial DNA as a potential biomarker for Astronauts’ Health. J. Am. Heart Assoc. 10, e022055 (2021).
Murgia, M. et al. Spaceflight on the ISS changed the skeletal muscle proteome of two astronauts. npj Microgravity 10, 1–13 (2024).
Wong-Riley, M. Energy metabolism of the visual system. Eye Brain 2, 99–116 (2010).
Hoang, Q. V., Linsenmeier, R. A., Chung, C. K. & Curcio, C. A. Photoreceptor inner segments in monkey and human retina: mitochondrial density, optics, and regional variation. Vis. Neuroscim 19, 395–407 (2002).
Kubota, M. et al. Mitochondrial oxygen metabolism in primary human lens epithelial cells: Association with age, diabetes and glaucoma. Free Radic. Biol. Med. 97, 513–519 (2016).
Guo, C., Sun, L., Chen, X. & Zhang, D. Oxidative stress, mitochondrial damage and neurodegenerative diseases. Neural Regen. Res. 8, 2003–2014 (2013).
Hamada, N., Azizova, T. V. & Little, M. P. An update on effects of ionizing radiation exposure on the eye. Br. J. Radiol. 93, 20190829 (2020).
Averbeck, D. & Rodriguez-Lafrasse, C. Role of mitochondria in radiation responses: epigenetic, metabolic, and signaling impacts. Int. J. Mol. Sci. 22, 11047 (2021).
Richardson, R. B. The role of oxygen and the Goldilocks range in the development of cataracts induced by space radiation in US astronauts. Exp. Eye Res. 223, 109192 (2022).
Karakosta, C., Samiotaki, M., Panayotou, G., Papaconstantinou, D. S. & Moschos, M. M. Lens cytoskeleton: an update on the etiopathogenesis of human cataracts. Cureus 16, e56793 (2024).
Nizami, A. A., Gurnani, B. & Gulani, A. C. Cataract. in StatPearls (StatPearls Publishing, 2024).
Shiels, A. & Hejtmancik, J. F. Inherited cataracts: genetic mechanisms and pathways new and old. Exp. Eye Res. 209, 108662 (2021).
Jones, J. A. et al. Cataract formation mechanisms and risk in aviation and space crews. Aviat. Space Environ. Med. 78, A56–A66 (2007).
Rafnsson, V. et al. Cosmic radiation increases the risk of nuclear cataract in airline pilots: a population-based case-control study. Arch. Ophthalmol. 123, 1102–1105 (2005).
Chorley, A. C., Evans, B. J. W. & Benwell, M. J. Civilian pilot exposure to ultraviolet and blue light and pilot use of sunglasses. Aviat. Space Environ. Med. 82, 895–900 (2011).
Waisberg, E., Ong, J. & Lee, A. G. Space radiation and the potential for early cataract development. Eye 38, 416–417 (2024).
Furukawa, S. et al. Space radiation biology for “living in space. Biomed. Res. Int. 2020, 4703286 (2020).
Chancellor, J. C., Scott, G. B. I. & Sutton, J. P. Space radiation: the number one risk to astronaut health beyond low earth orbit. Life 4, 491–510 (2014).
Kam, W. W.-Y. & Banati, R. B. Effects of ionizing radiation on mitochondria. Free Radic. Biol. Med. 65, 607–619 (2013).
Kaur, J., Kukreja, S., Kaur, A., Malhotra, N. & Kaur, R. The oxidative stress in cataract patients. J. Clin. Diagn. Res. 6, 1629–1632 (2012).
Brennan, L., Khoury, J. & Kantorow, M. Parkin elimination of mitochondria is important for maintenance of lens epithelial cell ROS levels and survival upon oxidative stress exposure. Biochim. Biophys. Acta Mol. Basis Dis. 1863, 21–32 (2017).
Masalkhi, M., Ong, J., Waisberg, E. & Lee, A. G. Ocular oxidative changes and antioxidant therapy during spaceflight. Eye 38, 1034–1035 (2024).
Gómez, X. et al. Key points for the development of antioxidant cocktails to prevent cellular stress and damage caused by reactive oxygen species (ROS) during manned space missions. NPJ Microgravity 7, 35 (2021).
Rondeau, J. D. et al. Mitochondria-targeted antioxidant MitoQ radiosensitizes tumors by decreasing mitochondrial oxygen consumption. Cell Death Discov. 10, 514 (2024).
Zhao, W. et al. Elamipretide (SS-31) improves mitochondrial dysfunction, synaptic and memory impairment induced by lipopolysaccharide in mice. J. Neuroinflamm. 16, 230 (2019).
Eells, J. T. Mitochondrial dysfunction in the aging retina. Biology 8, 31 (2019).
Chen, B. S., Harvey, J. P., Gilhooley, M. J., Jurkute, N. & Yu-Wai-Man, P. Mitochondria and the eye—manifestations of mitochondrial diseases and their management. Eye 37, 2416–2425 (2023).
Overbey, E. G. et al. Spaceflight influences gene expression, photoreceptor integrity, and oxidative stress-related damage in the murine retina. Sci Rep. 9, 13304 (2019).
Capri, M. et al. Long-term human spaceflight and inflammaging: does it promote aging? Ageing Res. Rev. 87, 101909 (2023).
Mao, X. W. et al. Spaceflight environment induces mitochondrial oxidative damage in ocular tissue. Radiat. Res. 180, 340–350 (2013).
Jin, X. et al. Different mitochondrial fragmentation after irradiation with X-rays and carbon ions in HeLa cells and its influence on cellular apoptosis. Biochem. Biophys. Res. Commun. 500, 958–965 (2018).
Wu, L.-J. et al. Targeted cytoplasmic irradiation with alpha particles induces mutations in mammalian cells. Proc. Natl. Acad. Sci. USA 96, 4959–4964 (1999).
Ariyoshi, K. et al. Radiation-induced bystander effect is mediated by mitochondrial DNA in exosome-like vesicles. Sci. Rep. 9, 9103 (2019).
Walsh, D. W. M. et al. Live cell imaging of mitochondria following targeted irradiation in situ reveals rapid and highly localized loss of membrane potential. Sci. Rep. 7, 46684 (2017).
Mao, X. W. et al. Acute effect of low-dose space radiation on mouse retina and retinal endothelial cells. Radiat. Res. 190, 45–52 (2018).
Wang, L. et al. Dose-dependent effects of radiation on mitochondrial morphology and clonogenic cell survival in human microvascular endothelial cells. Cells 13, 39 (2023).
Barisano, G. et al. The effect of prolonged spaceflight on cerebrospinal fluid and perivascular spaces of astronauts and cosmonauts. Proc. Natl. Acad. Sci. USA 119, e2120439119 (2022).
Smith, S. M., Zwart, S. R., Douglas, G. L. & Heer, M. Human Adaptation to Spaceflight: The Role of Food and Nutrition (Government Publishing Office, 2014).
Janssen, J. J. E., Grefte, S., Keijer, J. & de Boer, V. C. J. Mito-nuclear communication by mitochondrial metabolites and its regulation by B-Vitamins. Front. Physiol. 10, 78 (2019).
Ong, J., Lee, A. G. & Moss, H. E. Head-down tilt bed rest studies as a terrestrial analog for spaceflight associated neuro-ocular syndrome. Front. Neurol. 12, 648958 (2021).
Author information
Authors and Affiliations
Contributions
D.L., B.B., and H.W. conceptualized the idea of review. D.L., B.B, L.J.C., and H.W. wrote the draft of the review. D.L. created the figures. D.L., B.B., S.Z., S.S., X.M., B.M., and H.W. edited the draft and finalized the review. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
LeBlanc, D.P., Butterfield, B., Jimenez-Chavez, L. et al. Spaceflight stressors impact on mitochondrial function and the risk for development of ocular pathology. npj Microgravity 12, 30 (2026). https://doi.org/10.1038/s41526-026-00565-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41526-026-00565-5
