
Abstract
In West Africa, the long-term consequences of poor early psychosis recovery include poverty, neglect, and community ostracization. To understand the potential for digital health approaches to support early psychosis care in Ghana, we conducted a survey study among early psychosis patients and their caregivers about mental health needs, technology use and access, and interest in digital mental health. Hospital staff at Accra Psychiatric Hospital reviewed hospital medical records from January 2023 - December 2023 identifying young adults (≥18 years old) who had experienced psychosis symptoms for the first time within the prior five years. Trained data assessors contacted these individuals via telephone and invited them and their caregivers to participate; those providing informed consent were interviewed via phone in Twi or English. Overall, 256 individuals participated in the survey, including 121 young adults experiencing early psychosis and 135 caregivers of early psychosis patients. The majority (80%) of early psychosis patients and their caregivers expressed interest in digital mental health for early psychosis and had access to a mobile phone (91%) and necessary mobile infrastructure. Early psychosis patients were most interested in information about managing stress and improving mood via a digital resource (72%). Caregivers desired a digital tool to provide information about psychosis symptoms (86%). Our study among those experiencing early psychosis and their caregivers in Ghana suggests readiness and acceptability of digital mental health for early psychosis care.
Similar content being viewed by others

Introduction
Access to mental health services is low in West Africa1 where those with untreated serious mental illness are at particularly high risk for poverty, community ostracization, neglect, and abuse2,3,4. Early psychosis—the period when an individual first experiences hallucinations, delusions, or difficulties in reality testing—is a critical period for intervention to improve the long-term trajectory of psychotic disorders5,6. Specialized treatments (e.g., medications, cognitive behavioral therapy for psychosis) are effective in reducing symptom severity, psychiatric hospitalization, and impaired functioning, particularly when delivered during the earlier stages of psychotic illness7,8,9. Evidence suggests that early psychosis recovery rates following evidence-based treatment may be higher among those in low- and middle-income countries (LMICs) than in higher-income settings, potentially due to the bolstering effect of strong social connectedness and family support in LMIC communities10. However, few adolescents and adults with early psychosis in West Africa receive these interventions11.
Stigma surrounding mental health conditions and spiritual beliefs about the origin of psychosis symptoms (e.g., prophetic abilities, witchcraft by an enemy) are compounded by health system challenges (e.g., far distances to mental health facilities, long clinic queues, overstretched healthcare workers), discouraging mental healthcare-seeking in formal facility settings. These infrastructural limitations characterize the health system at large, hindering the integration of mental health services into primary care settings. Individuals experiencing early psychosis and their families (“caregivers”) often initially seek support from traditional or religious healers, delaying or preventing specialized treatment12,13. Further, those formally diagnosed with early psychosis frequently discontinue medication use and medical mental health services14. Caregivers play a pivotal role in the recovery support and community integration of their loved ones with early psychosis15. The World Health Organization (WHO) recommends family-inclusive early psychosis interventions in LMICs to harness the dynamic strengths of interconnectedness and reciprocity of care that often characterize LMIC communities16. However, caregivers in West Africa lack access to resources supporting their capacity for early psychosis care.
Innovative approaches are needed to address these significant unmet mental health needs among those experiencing early psychosis in West Africa17. Digital approaches to providing early psychosis information and skills could be particularly useful in West Africa18 where most countries report high penetration of phone ownership (over 75%)19. Digital interventions leverage prevalent delivery resources (e.g., mobile phones, radios, internet) and help overcome access barriers to facility-based resources, such as long travel and wait times and privacy or stigma concerns. In high-income countries, several digital or mobile health interventions for early psychosis show promise in alleviating psychiatric symptoms, reducing relapse, and supporting family communication about mental health20,21,22,23. Digital interventions are rapidly expanding in Africa for a range of behavioral health topics (e.g., HIV medication adherence, maternal child health support)24. Despite WHO support of digital interventions to address service gaps in LMICs25, none exist that are adapted to the cultural and services context of those impacted by early psychosis in Africa.
To understand the potential for digital health approaches to support early psychosis care in Ghana, we conducted a survey study among early psychosis patients and their caregivers. We explored mental health and psychosocial support needs, technology use and access, and interest in digital mental health for early psychosis among these groups to inform potential digital intervention development.
Methods
Study population and setting
We conducted a cross-sectional survey among young adults experiencing early psychosis and their caregivers at Accra Psychiatric Hospital in Accra, Ghana. Accra Psychiatric Hospital is the largest psychiatric hospital in Ghana, accommodating up to 300 inpatients at a time and serving over 28,000 outpatients per year. This facility is the national psychiatric referral hospital serving Ghana and the surrounding region.
Study procedures
Hospital staff reviewed hospital medical records from January 2023—December 2023 to identify young adults (≥18 years old) who had received a diagnosis of early psychosis, defined as experiencing psychosis symptoms for the first time within the prior five years. Trained data assessors contacted individuals who provided a phone number to inquire whether they would be interested in participating in the study. Caregivers of early psychosis patients were invited to participate in the survey if their names and telephone contact information were available. Both groups were offered independent participation which was not contingent on the participation of their loved one. Data assessors explained that participation was entirely voluntary and unassociated with clinical care. All early psychosis patients and caregivers who participated in the survey provided verbal consent. Data were collected using tablet-based REDCap questionnaires administered in Twi or English. Study surveys were administered over the phone among the majority of participants and in-person among individuals who visited Accra Psychiatric Hospital during the data collection period. Study participants received reimbursement for their transportation and participation commensurate with regional standards.
Measures
Study measures included items about demographics, mental health service utilization, technology access and use, psychosocial factors, and preferences for digital mental health for early psychosis. We administered the 10-item Brief Internalized Stigma of Mental Illness Inventory (ISMI-10) which measures one’s stigma surrounding their mental health condition. We adapted this measure for caregivers (e.g., original: “Having a mental illness has spoiled my life”, adapted: “Having a loved one with a mental illness has spoiled my life”). Moderate-to-severe internalized stigma was defined according to the published cutpoint (ISMI-10 score ≥ 2.51)26. To evaluate social support levels, we used the 3-item Oslo Social Support Scale (OSSS-3), defining “poor social support” according to the published cutpoint (OSSS-3 score≤8)27. Besides adapting the ISMI-10 for caregivers, no further adaptations of ISMI-10 or OSSS-3 were needed to ensure the understandability of the scale items based on cultural review by study team members with experience engaging with the population of interest. We defined household crowding as having over three household residents per room, which is a common proxy for socioeconomic status28.
Access and use of technology (e.g., electricity, cellular service, WIFI) was self-reported by participants. Survey questions assessed mobile phone ownership (whether a mobile phone was shared, number of phones owned, type of phone [smartphone, basic phone]) and utilization (e.g., calling, texting, social media, watching videos). Participants reported their level of interest (1 - not at all, 2 - slightly, 3 - moderately, 4 - very, 5 - extremely) in a digital mental health tool for early psychosis, including potential content areas (e.g., psychoeducation about early psychosis symptoms, skill practices to reduce stress) and activities (e.g., watching videos, responding to writing prompts).
Statistical analysis
Survey responses were descriptively analyzed using counts and proportions (categorical variables) or medians and interquartile ranges (continuous variables). Differences between early psychosis caregiver and patient responses are reported using Mann-Whitney-Wilcoxon tests (continuous variables) and chi-squared tests (categorical variables). Statistical analyzes were performed in Stata version 17.0.
Ethical considerations
All participants provided verbal consent prior to participating in the survey. This study was approved by the University of Washington Institutional Review Board (STUDY00020314) and the ethical committee at Accra Psychiatric Hospital (APH-ERC 00020/24).
Results
Participant characteristics
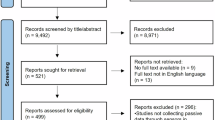
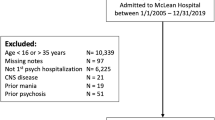
Among 266 individuals screened for eligibility, 256 (96%) participated in the survey, including 121 young adults experiencing early psychosis and 135 caregivers of early psychosis patients. Median age among early psychosis patients was 31 years (interquartile range [IQR]: 25–41); median age among caregivers was 47 years (IQR: 36–55) (Table 1). Approximately half of early psychosis patients surveyed were female (56%, N = 68) while less than half of caregivers surveyed were female (43%, N = 58). A quarter of early psychosis patients were married or cohabitating with a partner (27%, N = 32) while over half of caregivers were married or cohabitating (59%, N = 80). The majority of participants had secondary education or lower (early psychosis patients: 73%, N = 88, caregivers: 57.8%, N = 78). Participants predominantly identified as Christian (92%, N = 236). Participants predominantly lived outside of Accra city center, taking over 1 h to travel to Accra Psychiatric Hospital (median [IQR]: 75 min, [60–120]). Nine early psychosis patients (7%) and two caregiver (2%) reported being homeless in the prior year.
Household characteristics
Most caregivers reported being parents (77%, N = 103), while approximately a third of early psychosis patients were parents (40%, N = 48). The majority of early psychosis patients reported having someone they consider their “caregiver” (91%, N = 110). Caregivers were most commonly the early psychosis patient’s mother (32%, N = 39), spouse or partner (19%, N = 23), or sibling (19%, N = 23). Household crowding (3 or more household residents per room) was experienced by about one-tenth of participants (early psychosis patients [EP]: 7%, N = 8, caregivers [C]: 14%, N = 17).
Psychosocial characteristics
Poor social support was reported in about one in five early psychosis patients (17%, N = 20, OSSS-3 score: median [IQR]: 11.0 [9.0–12.0]) and caregivers (22%, N = 29, OSSS-3 score: median [IQR]: 10.0 [9.0–12.0]). Half of early psychosis patients (50%, N = 58) and under half of caregivers (40%, N = 52) endorsed having only 0–2 people they could count on if they had a problem. Moderate-to-severe internalized stigma for having a mental disorder was reported among a third of early psychosis patients (32%, N = 36, ISMI-10 score: median [IQR]: 2.3 [2.0–2.7]). Reporting stigma for having a loved one with a mental disorder was about half as common among caregivers (14%, N = 18, ISMI-10 score: median [IQR]: 2.0 [1.7–2.4])). The most frequently endorsed (“agree”/“strongly agree”) stigma items among early psychosis patients and caregivers were “mentally ill people tend to be violent” (EP: 62%, N = 72; C: 71%, N = 92) and “People without a (loved one with a) mental illness could not possibly understand me” (EP: 63%, N = 74, C: 58%, N = 73).
Mental health service utilization
Participants self-reported their lifetime use of a range of mental health support services. The majority of early psychosis patients reported utilizing counseling services (84%, N = 102) and medication (98%, N = 118) for mental health (Table 2). About a third of caregivers (35%, N = 47) reported using mental health counseling and only two (2%, N = 2) reported medication use for mental health. Over a quarter of both early psychosis patients and caregivers reported use of herbal medicine for mental health (EP: 33%, N = 40; C: 30%, N = 40). A fifth of early psychosis patients (21%, N = 25) reported using traditional healing methods (e.g., rituals, divination) for mental health. One in ten early psychosis patients (13%, N = 16) had history of a psychiatric hospitalization for mental health concerns. One of the caregivers reported using traditional healing methods; none reported being hospitalized for mental health concerns.
Mobile phone and technology use
Most participants (91%, N = 232) reported owning a mobile phone and using it daily (median [IQR]: 7.0 days per week [7.0–7.0]) (Table 2). However, fewer early psychosis patients than caregivers reported owning a mobile phone (83% vs. 98%, p < 0.001). The majority of mobile phone users had a smartphone (79%, N = 183) which was similar across groups. Under 10% of participants reported sharing the mobile phone with others (8%, N = 18). Over 10% of participants reported owning two mobile phones (13%, N = 30). While most participants reported being able to pay for mobile data most months (93%, N = 213), this financial capacity was less common among early psychosis patients than caregivers (87% vs. 98%, p < 0.001).
The most common mobile phone uses across both groups were making calls (91%, N = 232), sending SMS messages (53%, N = 136), and using social media (66%, N = 170). Other highly endorsed uses were listening to music (44%, N = 113), and watching videos (42%, N = 107). Early psychosis patients endorsed making calls less frequently than caregivers (p < 0.05), yet these activities were still common.
Nearly all participants reported access to electricity (97%, N = 248). The majority of participants had mobile phone service (73%, N = 186). Access to WiFi was low (9%, N = 22), as was access to a power generator (4%, N = 9). Among those without a mobile phone (N = 23), only one reported not knowing how to use a phone. Cost was the most frequently reported barrier to phone ownership (64%, N = 18).
Interest in digital mental health for early psychosis
Overall, 90% of caregivers and 74% of early psychosis patients were interested (moderately/very/extremely) in using a mobile device to provide mental health support (Table 3). Early psychosis patients were most interested in information about managing stress and improving mood (very/extremely interested: 72%, N = 83) and in information about symptoms of early psychosis (very/extremely interested: 71%, N = 82). Caregivers were most interested in information about mental health disorders (very/extremely interested: 86%, N = 114) and in information about symptoms of psychosis (very/extremely interested: 86%, N = 112). A large proportion of participants (EP: >40%, C: >60%) expressed interest in each separate content area provided (e.g., skills for managing social relationships, strategies to improve sleep, tracking changes in symptoms over time, etc.). When asked to rate their interest in engaging with a mobile app-based activity about early psychosis, participants were most interested in watching videos (EP: 83%, N = 98; C: 90%, N = 117). Both groups reported less interest in listening to audio, reading written text, or completing journal prompts.
Discussion
A growing body of work suggests that people in Africa who are struggling with mental health problems have access to personal technologies and that they are interested in technology-assisted interventions17,18,29,30. This study reports on the needs, device ownership, and digital intervention preferences of people with early psychosis and their caregivers in West Africa. These are key target populations for intervention; individuals with early psychosis stand to benefit from early treatments that could greatly impact the lifelong trajectory of their illness8,9,31. Caregivers of people with early psychosis often provide holistic care for a loved one, with limited resources to support their own health, well-being, and coping15. Our findings suggest that in Ghana, the majority of both groups have high access to mobile devices (>90%), including smartphones (>75%), and that most (>80%) are interested in digital health interventions that can help address their unmet mental health needs.
Several additional findings can inform digital early psychosis intervention development in Ghana. First, caregivers of early psychosis patients demonstrated higher interest in digital mental health approaches compared to patients themselves (>90% vs. >65%). Early psychosis patients endorsed wanting self-management and stress reduction content in a potential digital intervention, similar to a US-based population of youth experiencing early psychosis32. Caregivers endorsed desiring psychoeducation about mental health disorders and early psychosis as a top priority. They also preferred interventions that provide skill-building content for improving stress management and communication about psychosis with their loved ones. These findings align with a US population of caregivers of young adults with early psychosis33.
The unique responsibilities and stressors associated with caregiving for people with severe mental illness are well documented15. Caregivers are involved in recognizing their loved one’s mental health symptoms, health decision-making, providing financial support, and acquiring and dispensing medication. Family members or other friends or community members providing lay care are often ill-prepared and ill-equipped with necessary skills to handle this role. Ghana’s mental healthcare strategy aims to deinstitutionalize care and promote community-based care34. Thus, people with severe mental illness are more frequently cared for in the home by lay caregivers as opposed to formal facility-based care. Psychoeducational support for caregivers of people with chronic illnesses including severe mental illness reduces caregiver burden and improves well-being35. Psychoeducation for caregivers consequently leads to improved patient outcomes, including reduced rate of relapse36,37,38,39. Our findings support early psychosis caregivers as a promising population to reach with digital content to improve outcomes among caregivers and their loved ones. This direction is well-aligned with WHO encouragement of family-based interventions for psychotic disorders16.
Both early psychosis patients and caregivers endorsed watching videos as their preferred content delivery method. Short, video storytelling is an innovative format for mental health content delivery which enables culturally appropriate and appealing esthetics while overcoming the need for written or literacy or complex technological capacity40. Using video-based mHealth interventions, past studies have shown improvements in clinical outcomes in persons with serious mental illness, such as reductions in psychotic and depressive symptoms and improvements in quality of life41,42. In addition to improved clinical outcomes, engagement in video-based mHealth interventions can exceed engagement in other traditional in-person methods with similar patient satisfaction ratings while increasing the number of people commencing treatment41. By culturally adapting videos aimed at teaching evidence-based skills and techniques, we have the potential to reach people in low-resourced settings that face a variety of barriers such as stigma and health system challenges. Our results point to the potential acceptability, feasibility, and cultural appropriateness of a video-based mobile intervention for early psychosis.
Among both early psychosis patients and their caregivers, we found internalized stigma due to mental illness was high (early psychosis patients: 32%, caregivers: 14%) and low social support was common ( ~ 20%). These findings are consistent with other settings among early psychosis patients and their caregivers43,44,45. High stigma and low social support have been demonstrated to correlate with more severe symptom scores and poorer long-term illness outcomes43,44,45. Our finding that nearly a third of early psychosis patients have used traditional methods to address their psychosis symptoms (e.g., traditional healing, herbal remedies) highlights the common practice of opting for more “hidden” traditional care prior to formal mental health services, potentially to avoid anticipated stigma. Ghana’s high mobile phone penetration in the context of stigma for mental health conditions and cultural beliefs in the spiritual origins of psychosis symptoms create a unique circumstance wherein digital interventions have high-potential for improving access to culturally appropriate psychotherapy. A digital intervention to support early psychosis patients and/or caregivers could incorporate messages that normalize psychosis symptoms and mental health challenges to reduce internalized stigma43,46,47 Studies have found that individuals who engaged with a mobile mental health intervention perceived increased social connectivity and improved social skills, even if the application did not involve communication with a human48,49. Overall, there is a clear need for psychosocial support among early psychosis patients and caregivers in Ghana, which could be addressed via digital mental health approaches. Early psychosis patients and caregivers should be directly engaged in developing digital mental health interventions using user-centered approaches, and caregivers could be leveraged to enhance intervention success.
Limitations
Our study had several limitations. We recruited study participants via medical record review at Accra Psychiatric Hospital among patients who provided telephone contact information. Our procedures may have disproportionately excluded individuals lacking access to telecommunications, however our estimates of mobile phone coverage align with Ghana national reports (92.5% of households own a mobile phone)50. We enrolled participants based on their care attendance at one hospital located in the capital city, Accra. Our findings may not be generalizable to patients seeking care in other facilities or those who do not seek facility-based care. However, we intentionally based our survey in Accra Psychiatric Hospital as it is the largest and most prominent psychiatric hospital in the region. Patients and their families often travel far distances to receive specialized mental healthcare (median 1 h travel time from home to Accra Psychiatric Hospital), thus enhancing the potential generalizability of our study population. Early psychosis patients in our sample were older (median: 31 years) than the expected age of those experiencing early psychosis (late teens—early 20 s). This may reflect delays in seeking health facility-based care after spending a longer period identifying and making sense of symptoms, recognizing them as a concern, and in some cases attempting other care approaches (e.g., traditional or faith healing) prior to reaching the health system. As a cross-sectional study using participant self-reported data, our study does not reflect variation over time in participant experiences.
Conclusions
Closing access gaps in early psychosis treatment in West Africa requires innovative approaches that leverage family- and community-level resources and overcome logistical and psychosocial barriers. Our study among those experiencing early psychosis and their caregivers in Ghana demonstrated that they are open to digital mental health approaches and have access to the digital infrastructure and hardware to facilitate such approaches. Mobile phone interventions that utilize video-based content to provide psychoeducation and stress management skills for caregivers of patients with early psychosis may be particularly useful in the West African context. Young adults experiencing early psychosis and their caregivers’ prominent use of mobile phones, interest in digital interventions, and demonstrated need for psychosocial support suggest readiness and acceptability of digital mental health for early psychosis care in West Africa.
Data availability
The data that support the findings of this study will be openly available from the corresponding author upon reasonable request at the time of publication.
References
WHO Team. Mental Health Atlas 2020. WHO Publication 1–136 (2021).
Ofori-Atta, A., Read, U. M. & Lund, C. A situation analysis of mental health services and legislation in Ghana: challenges for transformation. Afr. J. Psychiatry 13, 99–108 (2010).
Read, U. M., Adiibokah, E. & Nyame, S. Local suffering and the global discourse of mental health and human rights: An ethnographic study of responses to mental illness in rural Ghana. Glob. Health 5, 1–16 (2009).
Esan, O. et al. Mental health care in Anglophone West Africa. Psychiatr. Serv. 65, 1084–1087 (2014).
Malla, A. K., Norman, R. M. G. & Joober, R. First-episode psychosis, early intervention, and outcome: what have we learned? Can. J. Psychiatry 50, 881–891 (2005).
Fusar-Poli, P., McGorry, P. D. & Kane, J. M. Improving outcomes of first-episode psychosis: an overview. World Psychiatry 16, 251–265 (2017).
Kane, J. M. et al. Comprehensive versus usual community care for first episode psychosis: two-year outcomes from the NIMH RAISE early treatment program. Am. J. Psychiatry 173, 362 (2016).
Dixon, L. B., Goldman, H. H., Srihari, V. H. & Kane, J. M. Transforming the treatment of schizophrenia in the United States: the RAISE initiative. Annu Rev. Clin. Psychol. 14, 237–258 (2018).
Correll, C. U. et al. Comparison of early intervention services vs treatment as usual for early-phase psychosis: a systematic review, meta-analysis, and meta-regression. JAMA Psychiatry 75, 555–565 (2018).
Padma, T. V. Developing countries: the outcomes paradox. Nature 508, S14–S15 (2014).
Hunt, X. et al. Interventions for adolescents and adults with psychosis in Africa: a systematic review and narrative synthesis. Glob. Ment. Health 9, 223–240 (2022).
Abiodun, O. A. Pathways to mental health care in Nigeria. Psychiatr. Serv. 46, 823–826 (1995).
Lilford, P., Wickramaseckara Rajapakshe, O. B. & Singh, S. P. A systematic review of care pathways for psychosis in low-and middle-income countries. Asian J. Psychiatr. 54, 102237 (2020).
Doyle, R. et al. First-episode psychosis and disengagement from treatment: a systematic review. Psychiatr. Serv. 65, 603–611 (2014).
Cham, C. Q. et al. Caregiver burden among caregivers of patients with mental illness: a systematic review and meta-analysis. Healthcare (Basel) 10, 2423 (2022).
Morillo, H., Lowry, S. & Henderson, C. Exploring the effectiveness of family-based interventions for psychosis in low- and middle-income countries: a systematic review. Soc. Psychiatry Psychiatr. Epidemiol. 57, 1749–1769 (2022).
Chibanda, D. The future of psychiatry in Africa—thinking outside the box. Lancet Psychiatry 4, 741–742 (2017).
Ben-Zeev, D. Mobile health for mental health in west africa: the case for Ghana. Psychiatr. Serv. 69, 741–743 (2018).
Africa: five countries have near 100% mobile phone ownership (survey) - Ecofin Agency. https://www.ecofinagency.com/telecom/1601-44176-africa-five-countries-have-near-100-mobile-phone-ownership-survey.
Terp, M., Jørgensen, R., Laursen, B. S., Mainz, J. & Bjørnes, C. D. A smartphone app to foster power in the everyday management of living with schizophrenia: qualitative analysis of young adults’ perspectives. JMIR Ment. Health 5, e10157 (2018).
Schlosser, D. A. et al. Efficacy of PRIME, a mobile app intervention designed to improve motivation in young people with schizophrenia. Schizophr. Bull. 44, 1010–1020 (2018).
Peck, C. E. et al. Development of a lived experience-based digital resource for a digitally-assisted peer support program for young people experiencing psychosis. Front. Psychiatry 11, 474058 (2020).
Bonet, L., Torous, J., Arce, D., Blanquer, I. & Sanjuán, J. ReMindCare, an app for daily clinical practice in patients with first episode psychosis: a pragmatic real-world study protocol. Early Inter. Psychiatry 15, 183–192 (2021).
McCool, J., Dobson, R., Whittaker, R. & Paton, C. Mobile health (mHealth) in low- and middle-income countries. Annu. Rev. Public Health 43, 525–539 (2022).
Global strategy on digital health 2020–2025, https://www.who.int/publications/i/item/9789240020924 (2021).
Boyd, J. E., Otilingam, P. G. & Deforge, B. R. Brief version of the Internalized Stigma of Mental Illness (ISMI) scale: psychometric properties and relationship to depression, self esteem, recovery orientation, empowerment, and perceived devaluation and discrimination. Psychiatr. Rehabil. J. 37, 17–23 (2014).
Kocalevent, R. D. et al. Social support in the general population: standardization of the Oslo social support scale (OSSS-3). BMC Psychol. 6, 1–8 (2018).
Melki, I. S., Beydoun, H. A., Khogali, M., Tamim, H. & Yunis, K. A. Household crowding index: a correlate of socioeconomic status and inter-pregnancy spacing in an urban setting. J. Epidemiol. Commun. Health 58, 476–480 (2004).
Sharma-Misra, S., Maru, M., Tomita, A. & Paruk, S. Access and use of digital technology by patients with psychosis at a hospital in South Africa. S. Afr. J. Psychiatr. 29, 2151 (2023).
Kola, L., Abiona, D., Adefolarin, A. O. & Ben-Zeev, D. Mobile phone use and acceptability for the delivery of mental health information among perinatal adolescents in Nigeria: survey study. JMIR Ment. Health 8, e20314 (2021).
Kane, J. C. et al. A scoping review of health-related stigma outcomes for high-burden diseases in low- and middle-income countries. BMC Med. 17, 17 (2019).
Buck, B. et al. mHealth for young adults with early psychosis: user preferences and their relationship to attitudes about treatment-seeking. J. Technol. Behav. Sci. 6, 667 (2021).
Buck, B. et al. Mobile health for caregivers of young adults with early psychosis: a survey study examining user preferences. 72, 955–959 (2021).
Sumah, A. M. & Baatiema, L. Decentralisation and management of human resource for health in the health system of ghana: a decision space analysis. Int. J. Health Policy Manag. 8, 28 (2019).
Sin, J. et al. Effectiveness of psychoeducational interventions for family carers of people with psychosis: a systematic review and meta-analysis. Clin. Psychol. Rev. 56, 13–24 (2017).
Tessier, A., Roger, K., Gregoire, A., Desnavailles, P. & Misdrahi, D. Family psychoeducation to improve outcome in caregivers and patients with schizophrenia: a randomized clinical trial. Front. Psychiatry 14, 1171661 (2023).
Lobban, F. et al. A systematic review of randomised controlled trials of interventions reporting outcomes for relatives of people with psychosis. Clin. Psychol. Rev. 33, 372–382 (2013).
Pharoah, F., Mari, J., Rathbone, J. & Wong, W. Family intervention for schizophrenia. Cochrane Database Syst. Rev. https://doi.org/10.1002/14651858.CD000088.PUB2 (2010).
Zhang, M., Wang, M., Li, J. & Phillips, M. R. Randomised-control trial of family intervention for 78 first-episode male schizophrenic patients: an 18-month study in Suzhou, Jiangsu. Br. J. Psychiatry 165, 96–102 (1994).
Adam, M. et al. Effect of short, animated video storytelling on maternal knowledge and satisfaction in the perinatal period in south africa: randomized controlled trial. J. Med Internet Res. 25, e47266 (2023).
Ben-Zeev, D. et al. Mobile health (mHealth) versus clinic-based group intervention for people with serious mental illness: a randomized controlled trial. Psychiatr. Serv. 69, 978–985 (2018).
Ben-Zeev, D. et al. Transdiagnostic mobile health: smartphone intervention reduces depressive symptoms in people with mood and psychotic disorders. JMIR Ment. Health 6, e13202 (2019).
Jameel, H. T. et al. Observed social support and willingness for the treatment of patients with schizophrenia. Psychol. Res. Behav. Manag 13, 193 (2020).
Chu, R. S. T. et al. Rate and correlates of self-stigma in adult patients with early psychosis. Front. Psychiatry 14, 1200568 (2023).
Liu, Y., Liu, H., Chen, S., Ren, J. & Tian, X. Association between social support and the severity of positive symptoms in rural community-dwelling patients with schizophrenia during the COVID-19 pandemic. BMC Psychiatry 24, 1–7 (2024).
Dennard, S., Patel, R., Garety, P., Edwards, C. & Gumley, A. A systematic review of users experiences of using digital interventions within psychosis: a thematic synthesis of qualitative research. Soc. Psychiatry Psychiatr. Epidemiol. https://doi.org/10.1007/S00127-024-02692-4 (2024).
Goh, Y. S., Ow Yong, Q. Y. J. & Tam, W. S. W. Effects of online stigma-reduction programme for people experiencing mental health conditions: a systematic review and meta-analysis. Int. J. Ment. Health Nurs. 30, 1040–1056 (2021).
Williams, A., Fossey, E., Farhall, J., Foley, F. & Thomas, N. Recovery after psychosis: qualitative study of service user experiences of lived experience videos on a recovery-oriented website. JMIR Ment. Health 5, e37 (2018).
Valentine, L. et al. Young people’s experience of a long-term social media-based intervention for first-episode psychosis: qualitative analysis. J. Med. Internet Res. 22, e17570 (2020).
Ghana: mobile phone ownership in households | Statista. https://www.statista.com/statistics/1139236/distribution-of-households-owning-mobile-telephones-in-ghana/.
Acknowledgements
We thank the staff at Accra Psychiatric Hospital for generously fostering our visits. The co-authors would like to thank the patients receiving care at Accra Psychiatric Hospital for contributing their time and energy as study participants.
Author information
Authors and Affiliations
Contributions
Conceptualization: A.L., J.A., D.B.Z. Formal analysis and writing—original draft: A.L., A.B. Investigation: A.L., J.A., B.B., K.O., A.O.A., D.B.Z. Methodology: A.L., J.A., B.B., A.B., K.O., D.B.Z. Project administration: A.L., J.A., A.B., E.Q.S., K.O., A.O.A. Resources: K.O., A.O.A., D.B.Z. Data collection: E.Q.S., D.K., F.K.D., M.I.I., P.E.O.D., O.O.A.T., O.B.E. Writing—review and editing: A.L., J.A., A.B., B.B., E.Q.S., K.O., B.K., F.K.D., M.I.I., P.E.O.D., O.O.A.T., O.B.E., A.O.A., D.B.Z.
Corresponding author
Ethics declarations
Competing interests
Dr. Ben-Zeev has financial interests in Merlin LLC and FOCUS technology. He has provided consultation services to Trusst Health, K Health, Boehringer Ingelheim, eQuility, Deep Valley Labs, Butler Hospital, and Otsuka Pharmaceuticals. The remaining authors have no competing interests to disclose.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Larsen, A., Agorinya, J., Beaulieu, A. et al. Digital health for early psychosis in Ghana: patient and caregiver needs and preferences. Schizophr 11, 5 (2025). https://doi.org/10.1038/s41537-025-00554-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41537-025-00554-9
