
Abstract
Cognitive impairment associated with schizophrenia (CIAS) places a significant burden on patients and caregivers. This study explored the burden experienced by primary (informal) and secondary (formal) caregivers. A secondary qualitative analysis was performed on interviews from a Schizophrenia Cognition Rating Scale (SCoRS) confirmation study. Thematic analysis was utilised to investigate the characteristics of caregiver burden. Quotes were analysed across 3 levels (Level 1: caregiver experience of patient cognitive symptoms; Level 2: caregiver experience of patient burden; Level 3: overarching caregiver burden) to establish themes. Subsequently, themes were mapped to SCoRS domains. Twenty primary caregivers and 20 secondary caregivers were enrolled. Caregivers described patient difficulties with memory, learning, social communication, and everyday tasks. Caregivers assisted patients by engaging in sustained teaching for new activities, encouraging social communication and repeating reminders to accomplish tasks. Caregiver burden was substantial among both groups. Thematic analysis identified 2 main themes: caregiving difficulty and caregiving necessity. These themes reflected the extensive roles and responsibilities assumed by caregivers due to the impacts of CIAS symptoms. Illustrative quotes were reported for 60% of primary caregivers and 55% of secondary caregivers. Six of the 8 SCoRS domains (memory, learning, attention, problem-solving, language, social cognition)were mapped to themes identified at each level. A high level of objective caregiving burden was found in relation to CIAS symptoms among primary and secondary caregivers. The SCoRS domains of memory, learning, attention, problem-solving, language and social cognition are key areas to treat in patients with schizophrenia to reduce caregiver burden.
Similar content being viewed by others

Introduction
Schizophrenia is a complex, chronic psychiatric disorder that presents many challenges; impairments in daily functioning and quality of life can be difficult for patients to manage, and the impact of these challenges often extends to caregivers1,2,3. In addition, the role of society in supporting patients with schizophrenia entails the provision of healthcare services, such as long-term psychosocial care, inpatient and outpatient hospital visits/stays, as well as economic support, resulting in high direct and indirect costs1,2,3. Although prevalence estimates of schizophrenia show variation, a systematic literature review that included data from 46 countries reported a median lifetime morbid risk of 0.72%, which means that about 7 individuals per 1000 will be affected4. The disorder typically manifests in late adolescence or early adulthood, with onset occurring earlier in men than in women3,5.
Schizophrenia is characterised by a combination of positive, negative and cognitive symptoms6. Positive symptoms, such as delusions and hallucinations, are typically the initial reasons for clinical presentation6. Negative symptoms, including amotivation and social withdrawal, and cognitive symptoms such as deficits in working memory, executive function and processing speed, contribute to the disorder’s long-term burden6. Cognitive symptoms are often present at the first signs of schizophrenia, affecting approximately 80% of individuals with the condition7,8. Cognitive impairment associated with schizophrenia (CIAS) affects daily life and is a major determinant of functional outcomes7, as well as affecting healthcare costs9.
The EU5 National Health and Wellness Survey found that schizophrenia caregivers reported greater activity impairment, resource utilisation, costs and worse health-related quality of life than non-caregivers and caregivers of other conditions10,11. The substantial costs associated with schizophrenia, including caregiver healthcare needs, productivity loss, and reliance on caregivers, have led Health Technology Assessments, payers and prescribers worldwide to recognise the value of evidence demonstrating alleviation of caregiver burden12. Assessing caregiver burden in clinical trials and practice can enhance awareness and management, offering opportunities for increased support that may reduce the direct and indirect costs associated with caregivers’ healthcare needs, loss of productivity and reliance on formal caregivers12. Improving family and social support systems may reduce the burden on schizophrenia caregivers and healthcare systems, ultimately decreasing the societal cost of schizophrenia globally10.
Informal caregivers (i.e., primary caregivers) for patients are unpaid family members, friends or neighbours involved in daily care, whereas formal caregivers (i.e., secondary caregivers) are paid professionals, for example, psychiatrists, nurses or social workers, and are likely to be unrelated to the patient. Caregivers experience substantial economic impacts, including greater absenteeism, presenteeism, overall work impairment, and indirect costs associated with their caregiving roles compared with non-caregivers10. The financial burden for caregivers can be significant, with annual average costs ranging from $1586 in China to $30,591 in the US13. While research shows that primary caregivers are affected emotionally, financially and physically, experiencing restricted daily routines and by other burdens such as stigma, blame and dissatisfaction with family dynamics14, secondary caregivers have so far received minimal attention in research. Nevertheless, secondary caregivers are a relevant group that is involved in the care of people with schizophrenia, and a previous study that included secondary caregivers and that focused on economic impact has shown that there is at least an economic cost to secondary caregivers of people with schizophrenia13.
The Schizophrenia Cognition Rating Scale (SCoRS) is an interview-based measure designed to assess cognitive impairment and impact on day-to-day functioning in the real world in patients with schizophrenia, with questions relating to specific cognitive domains, such as memory, learning, attention, working memory, problem solving, speed of processing, language and social cognition15,16. Assessment with the SCoRS requires input from the patient, the caregiver and the clinician. Prior studies have shown SCoRS to have strong psychometric properties, with excellent test-retest reliability and that it is highly related to cognitive performance (per the MATRICS Consensus Cognitive Battery), in addition to being sensitive to treatment16.
One recent study, the SCoRS concept confirmation, further established the relevance of the content and usability of the SCoRS from the perspective of both primary and secondary caregivers looking after patients with schizophrenia. The study reported here is a secondary analysis of the primary SCoRS concept confirmation study and had the following objectives: first, to identify primary and secondary caregiver burden experience in relation to CIAS when caring for patients with schizophrenia, based on data collected during the SCoRS content confirmation study17; second, to describe core themes related to caregiver burden of CIAS; and third, to identify SCoRS domains that are related to these themes to determine which domains can be targeted with new treatments to alleviate caregiver burden of CIAS.
Methods
Study design
This study employed a secondary, qualitative, inductive thematic analysis using qualitative interviews from the SCoRS concept confirmation study17. The primary study was a qualitative, cross-sectional, non-interventional study conducted in the US, in which caregivers who cared for patients with schizophrenia participated in one-on-one, 90-minute, semi-structured interviews conducted by trained researchers17.
Approval for primary data collection was granted by the Salus Institutional Review Board. All participants provided written informed consent prior to participating in interviews and provided consent for secondary analyses.
Participants
In the primary (SCoRS concept confirmation) study, caregivers were recruited through US patient/caregivers and professional association groups, or via clinical trial sites if the caregiver did not care for a patient taking part in an ongoing clinical trial. A total of 50 primary and secondary caregivers of patients with schizophrenia were identified between October 2021 and March 2023. Caregivers were included in the study if they were ≥18 years old, knew the patient well, regularly interacted with them (≥1 hour/week with ≥1 in-person interaction/week) could read, write and speak English, and exhibited reliability and physiologic capability (e.g., sufficient hearing and vision) to comply with protocol procedures (in the investigator’s opinion). In addition, primary carers were required to be educated to at least 8th grade and secondary carers needed to have formal training as a health or social care professional. The final sample size was 40 caregivers (20 primary caregivers; 20 secondary caregivers). Most primary caregivers were female (85%), with a mean age of 51 years (range 28–82), while secondary caregivers also showed a predominance of female participants (60%), with a mean age of 41 years (range 22–60). Further details on caregiver demographics and characteristics are reported in the SCoRS concept confirmation study17.
Primary caregivers were defined as individuals providing informal (unpaid), live-in care to the patient, offering direct or indirect support such as organising tasks, making phone calls, managing bills or paperwork, shopping, cooking, cleaning and doing laundry. Secondary caregivers were defined as individuals with formal training who worked with patients with schizophrenia in outpatient and/or home settings, such as case managers, group home staff members, psychiatric social workers, social workers and psychiatric mental health nurses.
Measures
The 20-item SCoRS is an interview-based assessment that evaluates cognitive impairment and the impact of cognitive impairment on the daily functioning of patients with schizophrenia. The SCoRS measure includes 8 cognitive domains: memory, learning, attention, working memory, problem-solving, processing/motor speed, language and social cognition. Items are rater-assessed (a final rating based on the clinical judgement of the interviewer with input from patients and caregivers) on a 4-point scale; higher scores indicate a greater degree of cognitive impairment15,17,18.
Procedures
Interviews with caregivers were conducted remotely via video call using Microsoft Teams, and the audio was recorded and subsequently transcribed. Transcripts were de-identified prior to being uploaded to ATLAStiTM software package for the primary data analysis.
Two discussion guides were used in the interviews; 1 for primary caregivers and 1 for secondary caregivers (Supplementary methods). The interviews were structured in 3 parts: caregiver and patient characteristics, concept elicitation, and cognitive debriefing of the SCoRS. The results of the concept elicitation and cognitive debriefing are reported in the SCoRS concept confirmation study17. Interview questions included caregiver demographics and characteristics, caregiver perception of the patient’s CIAS severity (none, mild, moderate or severe) in the previous 2 weeks, caregiver experience of caring for or spending time with the patient with schizophrenia. Interviews investigated the relevance of the SCoRS content to assess the impact of cognitive functions on the patient’s daily life and were not designed to directly ask about the caregiver’s experience of caring for patients with schizophrenia.
Data analysis
Inductive thematic analysis was selected as the optimal approach for data analysis19, following a search within the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) database to identify qualitative methodologies focusing on participant experience. This method is widely used in psychology and social sciences for reporting themes within data and offers a highly flexible approach to analysing participant experience data19. In this secondary analysis, data were extracted from interview feedback provided by the 40 participating caregivers, comprising 20 primary and 20 secondary caregivers, during the SCoRS content confirmation study. Quotes from the interviews were analysed across 3 levels (Level 1: caregiver experience of patient cognitive symptoms; Level 2: caregiver experience of patient burden; Level 3: overarching caregiver burden; Fig. 1). A separate inductive thematic analysis was conducted for each level, with codes assigned and themes established at each step. The process was iterative, moving between the levels to establish the 3 sets of themes. The analysis was conducted by an individual researcher, whose work was then reviewed by a second, senior individual researcher. Any disagreements were resolved with consensus between the data analyst and the senior researcher. Themes from each level were mapped to SCoRS domains (memory, learning, attention, working memory, problem-solving, processing/motor speed, language and social cognition) to indicate which cognitive domains are relevant to the burden experiences of caregivers.

Caregiver analysis data levels.
Results
Caregiver rating of patient CIAS burden
In the 2 weeks prior to the interviews, a similar proportion of primary caregivers rated patient cognitive impairment as mild, moderate or severe, with only 10% reporting patients as having no impairment. In contrast, secondary caregivers mainly reported patient cognitive impairment as moderate and none reported it as severe. Care settings varied, with 25% of patients with primary caregivers in outpatient settings, 25% of patients in home care and 50% in community settings. Among patients with secondary caregivers, 55% were in outpatient settings, 30% in inpatient settings, 25% in home care, and 5% in community settings (some patients had care in more than one setting). Hospitalisation for schizophrenia in the past year was reported for 30% of patients with primary caregivers and 40% with secondary caregivers. The mean duration of hospital stays during the past year was longer for those with secondary caregivers, at 18.3 weeks compared with 1.7 weeks for primary caregivers. Further details are reported in the SCoRS concept confirmation study17.
Caregiver burden findings
Level 1: Caregiver experience of patient cognitive symptoms
Four themes concerning the caregiver experience of patient symptoms were identified. These themes were: problems with memory, notably issues remembering names, appointments and frequent misplacing of items; difficulty learning new things, characterised by slow learning and the necessity for repeated, one-on-one instruction; difficulties with social communication, including a lack of response to social cues and difficulties engaging in group conversations; and finding it hard to fulfil everyday living activities, such as finance management, cooking and personal care routines (Table 1).
Level 2: Caregiver experience of patient burden
Four themes were identified concerning the caregiver experience of patient burden. The themes were “Support required for memory recall”, where caregivers provide prompts, reminders and assist with remembering names and places; “New activities/technology use requires sustained teaching assistance”, indicating the need for consistent one-on-one instruction; “Multiple elements of social communication assistance are required (e.g., support for the patient to listen, follow, respond and express)”, highlighting challenges in helping patients engage in and follow conversations, especially in group settings; and “Everyday living tasks require repetitive verbal support”, where caregivers assist with tasks related to finance management, cooking, self-care and maintaining a daily routine (Table 2).
Level 3: Overarching caregiver burden
The final overarching analysis identified 2 main themes, ‘caregiving difficulty’ and ‘caregiving necessity’, both shown in Fig. 2. Caregiving difficulty and caregiving necessity (distinct but related topics) were both depicted as high. Consequently, a substantial level of objective caregiver burden was reported across the data set for both primary and secondary caregivers. ‘Caregiving difficulty’ includes subthemes such as the difficulty of continuing outpatient care, the effort to improve patient quality of life, additional workload, teaching new skills to patients, and the frequent need to communicate repeatedly. ‘Caregiving necessity’ highlights the high need for caregiver help in daily activities and financial management, emphasizing the patient’s dependence on caregiver support for basic functioning and safety. Illustrative quotes that provide real-life examples of these themes are shown in Table 3 for ‘Caregiving difficulty’ and in Table 4 for ‘Caregiving necessity’.

Thematic map of caregivers experience of burden.
Across all 3 thematic analysis levels, illustrative quotes were identified for 12/20 (60%) primary caregivers and 11/20 (55%) secondary caregivers from the interviews in the SCoRS concept confirmation study.
Mapping of thematic findings onto SCoRS domains
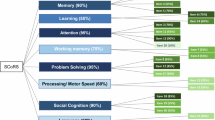
Six out of 8 SCoRS domains—memory, learning, attention, problem-solving, language and social cognition—were identified as relevant to the caregiver burden reported by both primary and secondary caregivers (Fig. 3). Specific caregiving challenges mapped to these domains include difficulties with daily living tasks, communication and teaching new skills. The working memory and processing/motor speed SCoRS domains were not identified to be relevant to caregiver burden.

SCoRS Schizophrenia Cognition Rating Scale.
Discussion
This study identified a substantial level of burden among this sample of primary and secondary caregivers for patients with CIAS. Caregivers reported the need to assume extra role responsibilities in relation to the patients’ CIAS symptoms, which was central to their extent of burden. The final thematic analysis identified caregiving difficulty (Theme 1) and caregiving necessity (Theme 2) as the 2 main themes. Illustrative quotes were provided by an equal proportion of primary and secondary caregivers. Memory, learning, attention, problem-solving, language and social cognition were identified as SCoRS domains relevant to caregiver burden.
Primary caregivers reported a more evenly distributed severity (ranging from none to severe) of CIAS symptoms in patients 2 weeks prior to the interview compared with secondary caregivers, who reported only mild or moderate CIAS symptoms. However, it should be noted that the nature of secondary caregiver provision is likely the result of recent and/or ongoing hospitalisations; secondary caregivers reported higher hospitalisation frequency and duration over the past year and 30% were reporting on current inpatients. Therefore, secondary caregivers may have a more clinical approach and definition of severity compared with primary caregivers who are usually exposed to a broader range of behaviours and challenges. Future research should refine the matching of the caregiver groups in relation to the recall period and time of patient CIAS symptom presentation.
The main themes identified were caregiver difficulty (Theme 1) and caregiver necessity (Theme 2). These findings are in accordance with an existing study that identified daily hassles (i.e., assumption of extra responsibilities/caregiver necessity), emotional burden, and financial troubles among the main areas of caregiver burden14. Other interview-based qualitative studies also found heavy involvement of caregivers (i.e., caregiver necessity) and challenges in caregiving (i.e., caregiver difficulty) as key themes20,21. A correlational study reported that caregivers had a substantial burden, with 38.2% of primary caregivers experiencing severe burden22. The caregiver’s age, gender, education level, job loss due to caregiving responsibilities, income, relationship with the patient, disease duration and frequency of caregiving were identified as statistically significant predictive factors for the caregiving burden in schizophrenia22. Unlike previous research14, physical aspects were not reported in the present study. The themes identified at each level were mapped to 6 of the 8 SCoRS domains, including memory, learning, attention, problem solving, language and social cognition. Therefore, these domains may serve as potential outcome areas in clinical trials to assess the impact of schizophrenia treatments on caregivers.
The burden experienced by caregivers in relation to cognitive impairment among people with schizophrenia demonstrated in this analysis, highlights an unmet need for treatment of CIAS. Current recommendations suggest patients with schizophrenia should be administered second-generation antipsychotics to manage their cognitive symptoms, as there is a favourable cognitive profile as compared with first-generation antipsychotics23. Furthermore, psychosocial interventions such as cognitive remediation and physical exercise have been specifically demonstrated to provide some benefit to cognition in people with CIAS23,24,25,26,27,28. Though these approaches may ameliorate cognitive symptoms to some extent, there are no US Food and Drug Administration (FDA)-approved pharmacological treatments specifically targeted for cognitive symptoms. This unmet need will be critical to fill as CIAS is associated with poor functional outcomes, poorer quality of life, and increased healthcare resource utilisation than those without cognitive impairment, in addition to the impacts on and costs incurred by caregivers1,2,3,7,9,10,13.
The study presented several limitations that should be considered when interpreting the findings. First, the secondary nature of the study is the main limitation: the study used pre-existing interview data from the SCoRS concept confirmation study with a different objective. Therefore, the conclusions should be interpreted in respect to this limitation as specific questions about caregiver burden were not asked in the interviews. Nevertheless, the study was rigorous due to the application of an inductive thematic analysis that analysed quotes iteratively across 3 levels, thereby the results provide preliminary information that can be used to design a prospective approach in future studies. Second, the impact of issues related to working memory and processing/motor speed on caregiver burden may not have been adequately captured owing to the design of the study interviews (direct questions were not asked). This approach may lead to the incorrect conclusion that these domains are not relevant. Therefore, further studies are needed to explore these aspects more thoroughly. Third, no evidence emerged on physical aspects of caregiver burden (e.g., somatic issues, less energy, tiredness and exhaustion) in the study, most likely attributed to the cognitive focus of the SCoRS assessment tool and the secondary nature of this study (i.e., burden was spontaneously reported by caregivers in the primary study). Fourth, results from primary and secondary caregivers were combined, and secondary analyses could not link specific primary or secondary caregivers to specific patients, thereby also not allowing to link caregiver burden to the reported cognitive impairment of the patient. Lastly, the study was conducted within the United States, and its findings may not be generalisable to countries with different social welfare and healthcare systems, where caregiver burden may be different, families (primary caregivers) may be driven by different social norms, or there are differences in secondary caregiver qualifications or community services. Future research should aim to explore caregiver burden of CIAS on a global and regional scale, and separately for primary and secondary caregivers as well as relate the caregiver burden to their assessment of the cognitive burden of the patient to better understand the full extent of the impact of patient cognitive impairment on caregivers.
In conclusion, this qualitative, secondary, thematic analysis study of caregivers for people with schizophrenia indicated a high level of objective caregiver burden related to CIAS symptoms among both primary and secondary caregivers. The principal themes identified were caregiver difficulty (Theme 1) and caregiver necessity (Theme 2). The requirement for both primary and secondary caregivers to assume extra roles and responsibilities due to the impacts of CIAS symptoms was central to these themes. The SCoRS domains of memory, learning, attention, problem-solving, language and social cognition were identified as areas to target with new treatments in patients with schizophrenia to alleviate caregiver burden. Further research is required to investigate the subjective burden experienced by primary and secondary caregivers of patients with schizophrenia.
Data availability
Parexel was contracted by Boehringer Ingelheim to conduct the analyses, interpret the results, as well as write, review and revise the manuscript. To ensure independent interpretation of clinical study results and enable authors to fulfil their role and obligations under the ICMJE criteria, Boehringer Ingelheim grants all external authors access to relevant clinical study data. In adherence with the Boehringer Ingelheim Policy on Transparency and Publication of Clinical Study Data, scientific and medical researchers can request access to clinical study data, typically, 1 year after the approval has been granted by major Regulatory Authorities or after termination of the development programme. Researchers should use the https://vivli.org/ link to request access to study data and visit https://www.mystudywindow.com/msw/datasharing for further information.
References
Awad, A. G. & Voruganti, L. N. The burden of schizophrenia on caregivers: a review. Pharmacoeconomics 26, 149–162 (2008).
Kahn, R. S. et al. Schizophrenia. Nat. Rev. Dis. Prim. 1, 15067 (2015).
WHO. Schizophrenia, https://www.who.int/news-room/fact-sheets/detail/schizophrenia (2022).
McGrath, J., Saha, S., Chant, D. & Welham, J. Schizophrenia: a concise overview of incidence, prevalence, and mortality. Epidemiol. Rev. 30, 67–76 (2008).
Solmi, M. et al. Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol. Psychiatry 27, 281–295 (2022).
McCutcheon, R. A., Reis Marques, T. & Howes, O. D. Schizophrenia-An Overview. JAMA Psychiatry 77, 201–210 (2020).
Carbon, M. & Correll, C. U. Thinking and acting beyond the positive: the role of the cognitive and negative symptoms in schizophrenia. CNS Spectr. 19, 38–52 (2014).
Harvey, P. D. et al. Cognitive dysfunction in schizophrenia: An expert group paper on the current state of the art. Schizophr. Res Cogn. 29, 100249 (2022).
Correll, C. U., Xiang, P., Sarikonda, K., Bhagvandas, N. & Gitlin, M. The Economic Impact of Cognitive Impairment and Negative Symptoms in Schizophrenia: A Targeted Literature Review With a Focus on Outcomes Relevant to Health Care Decision-Makers in the United States. J. Clin. Psychiatry 85, 24r15316 (2024).
Gupta, S., Isherwood, G., Jones, K. & Van Impe, K. Productivity loss and resource utilization, and associated indirect and direct costs in individuals providing care for adults with schizophrenia in the EU5. Clinicoecon Outcomes Res. 7, 593–602 (2015).
Gupta, S., Isherwood, G., Jones, K. & Van Impe, K. Assessing health status in informal schizophrenia caregivers compared with health status in non-caregivers and caregivers of other conditions. BMC Psychiatry 15, 162 (2015).
Gater, A. et al. Assessing the impact of caring for a person with schizophrenia: development of the Schizophrenia Caregiver Questionnaire. Patient 8, 507–520 (2015).
Han, X., Travers, C., Dembek, C. & Kulkarni, A. HSD86 economic attributes of caregiver burden among schizophrenia patients: a targeted literature review. Value Health 26, S310 (2023).
von Kardorff, E., Soltaninejad, A., Kamali, M. & Eslami Shahrbabaki, M. Family caregiver burden in mental illnesses: The case of affective disorders and schizophrenia - a qualitative exploratory study. Nord J. Psychiatry 70, 248–254 (2016).
Harvey, P. D., Khan, A., Atkins, A., Walker, T. M. & Keefe, R. S. E. Comprehensive review of the research employing the schizophrenia cognition rating scale (SCoRS). Schizophr. Res. 210, 30–38 (2019).
Keefe, R. S. et al. Reliability, validity and treatment sensitivity of the Schizophrenia Cognition Rating Scale. Eur. Neuropsychopharmacol. 25, 176–184 (2015).
Correll, C. U. et al. Concept confirmation of the Schizophrenia Cognition Rating Scale (SCoRS) among unpaid and professional caregivers. Schizophrenia https://doi.org/10.1038/s41537-025-00674-2 (2025) (in press).
Keefe, R. S., Poe, M., Walker, T. M., Kang, J. W. & Harvey, P. D. The Schizophrenia Cognition Rating Scale: an interview-based assessment and its relationship to cognition, real-world functioning, and functional capacity. Am. J. Psychiatry 163, 426–432 (2006).
Braun, V. & Clarke, V. Using thematic analysis in psychology. Qualit. Res. Psychol. 9, 3–26 (2006).
Tamizi, Z. et al. Caregiving burden in family caregivers of patients with schizophrenia: A qualitative study. J. Educ. Health Promot 9, 12 (2020).
Soni, A., Kumar, R. & Das, A. Experiences of the family caregivers of persons with schizophrenia in north Indian region: A qualitative inquiry. Arch. Psychiatr. Nurs. 51, 17–24 (2024).
Rahmani, F., Roshangar, F., Gholizadeh, L. & Asghari, E. Caregiver burden and the associated factors in the family caregivers of patients with schizophrenia. Nurs. Open 9 (2022).
Vita, A. et al. European Psychiatric Association guidance on treatment of cognitive impairment in schizophrenia. Eur. Psychiatry 65, e57 (2022).
Wykes, T., Bowie, C. R. & Cella, M. Thinking about the future of cognitive remediation therapy revisited: what is left to solve before patients have access?. Schizophr. Bull. 50, 993–1005 (2024).
Wykes, T., Huddy, V., Cellard, C., McGurk, S. R. & Czobor, P. A meta-analysis of cognitive remediation for schizophrenia: methodology and effect sizes. Am. J. Psychiatry 168, 472–485 (2011).
Twamley, E. W. et al. Compensatory cognitive training for people with severe mental illnesses in supported employment: A randomized controlled trial. Schizophr. Res. 203, 41–48 (2019).
Solmi, M. et al. Efficacy and acceptability of psychosocial interventions in schizophrenia: systematic overview and quality appraisal of the meta-analytic evidence. Mol. Psychiatry 28, 354–368 (2023).
Solmi, M. et al. Exercise as a transdiagnostic intervention for improving mental health: An umbrella review.J. Psychiatr. Res. 184, 91–101 (2025).
Food and Nutrition Service. U.S. Department of Agriculture. Supplement Nutrition Assistance Program (SNAP). (2025).
Hudon, C. et al. Opportunities of integrated care to improve equity for adults with complex needs: a qualitative study of case management in primary care. BMC Prim. Care 25, 391 (2024).
Acknowledgements
The authors would like to thank all the participants/patients, caregivers, healthcare professionals and collaborators at investigator sites who participated in this study. Medical writing support (in the form of writing assistance, including preparation of the draft manuscript under the direction and guidance of the authors, collating and incorporating authors’ comments for each draft, assembling tables and figures, grammatical editing and referencing) was provided by Sarah Meadows, MRes, at Avalere Health Global Limited, and was funded by Boehringer Ingelheim International GmbH. This study was funded by Boehringer Ingelheim. Boehringer Ingelheim International GmbH was given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations. The sponsor had no control over the content and the decision to submit the paper.
Author information
Authors and Affiliations
Contributions
All authors made substantial contributions to either (i) the conception or design of the work, (ii) the acquisition, analysis or interpretation of data, or (iii) drafting the work or substantively revising it. In addition, all authors approved the submitted version and take responsibility for the accuracy and integrity of the work.
Corresponding author
Ethics declarations
Competing interests
AGir is an employee of Parexel, and MR and KR were employees of Parexel at the time of the study. Parexel was contracted by Boehringer Ingelheim to conceptualise the study, write the protocol and discussion guide, conduct the interviews, analyse and/or interpret the results, as well as write, review and revise the manuscript. CUC has been a consultant and/or advisor to or has received honoraria from: AbbVie, Alkermes, Allergan, Angelini, Aristo, Boehringer Ingelheim, Bristol Meyers Squibb, Cardio Diagnostics, Cerevel, CNX Therapeutics, Compass Pathways, Darnitsa, Delpor, Denovo, Eli Lilly, Eumentis Therapeutics, Gedeon Richter, Hikma, Holmusk, IntraCellular Therapies, Jamjoom Pharma, Janssen/J&J, Karuna, LB Pharma, Lundbeck, MedInCell, MedLink, Merck, Mindpax, Mitsubishi Tanabe Pharma, Maplight, Mylan, Neumora Therapeutics, Neuraxpharm, Neurocrine, Neurelis, Newron, Noven, Novo Nordisk, Otsuka, PPD Biotech, Recordati, Relmada, Reviva, Rovi, Saladax, Sanofi, Seqirus, Servier, Sumitomo Pharma America, Sunovion, Sun Pharma, Supernus, Tabuk, Takeda, Teva, Terran, Tolmar, Vertex, Viatris and Xenon Pharmaceuticals. He provided expert testimony for Janssen, Lundbeck and Otsuka. He served on a Data Safety Monitoring Board for Compass Pathways, IntraCellular Therapies, Relmada, Reviva and Rovi. He has received grant support from Boehringer Ingelheim, Janssen and Takeda. He received royalties from UpToDate and is also a stock option holder of Cardio Diagnostics, Kuleon Biosciences, LB Pharma, Medlink, Mindpax, Quantic and Terran. AGold has no competing interests to declare. RK receives consulting income from Kynexis, Merck, WCG, Boehringer Ingelheim, Neurocrine, Gedeon-Richter, Novartis, Vandria, Damona and received royalties from the BACS. ST, CH, and CRF are employees of Boehringer Ingelheim.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Affiliation at the time of the study: Matthew Ridley, Katja Rudell.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tulliez, S., Girardi, A., Ridley, M. et al. Primary and secondary caregiver burden of cognitive impairment associated with schizophrenia: a qualitative study based on caregiver interviews. Schizophr 11, 127 (2025). https://doi.org/10.1038/s41537-025-00675-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41537-025-00675-1
