
Abstract
Subclinical paranoia is present in the relatives of patients with psychosis but it is also relatively common in the general population. Dopamine neurotransmission is increased in people with psychosis and is linked with positive symptoms, such as paranoia. Here, we examined if neuromelanin-sensitive MRI, a proxy of long-term dopamine turnover, is different between those with (n = 25) and without (n = 77) a first-degree relative with psychosis (N = 102). We further tested whether neuromelanin-sensitive MRI was associated with the experience of subclinical paranoia as measured by the paranoia checklist. We found that there was no difference in neuromelanin-sensitive MRI signal between those with and without a first-degree relative. However, neuromelanin-sensitive MRI was significantly associated with the frequency subscore of the paranoia checklist, irrespective of familial risk (255 of 1879 voxels at p < 0.05, pcorrected = 0.03). This relationship was further supported by the association of neuromelanin-sensitive MRI and community assessment of psychic experience paranoia frequency subscore (316 of 1879 voxels at p < 0.05, pcorrected = 0.01). In summary, we show that subclinical paranoid thoughts are associated with a proxy of long-term dopamine turnover regardless of whether the person has a relative with psychosis or not. Thus, neuromelanin-MRI associates with positive subclinical symptomatology in those without psychotic illness, in addition to the link observed in patients.
Similar content being viewed by others


Introduction
Schizophrenia is a neurodevelopmental disorder with a large genetic component1,2. Many symptoms of schizophrenia, including paranoia, are present at subclinical levels in the relatives of individuals with psychotic disorders3,4. In the general population, the prevalence of psychotic experiences is reported to be 5–8%, which is substantially higher than the prevalence of psychotic illness at 3%. That is, psychotic experiences exist along a continuum with a much larger cohort having subclinical psychotic experiences without a full-blown illness5,6.
Paranoia is one such psychotic experience. It is common, heritable and exacerbated by exposure to environmental risk factors7,8,9,10,11,12. The two fundamental components of paranoia are i) a belief that harm will occur and ii) attribution of the belief to the malicious intent of others. It is thought that paranoia may serve to be evolutionarily advantageous, particularly if the belief is true, unlike hallucinations which do not confer an evolutionary advantage at face value; however, paranoia becomes less advantageous as the conviction and distress due to these beliefs become disabling13.
It is thought that paranoia may arise from maladaptive belief updating, caused by excess dopamine function14. More generally, elevated dopamine system function in the striatum is a hallmark of psychotic illness and represents a convergence of both genetic and environmental risk factors15,16,17. Individuals with schizophrenia show elevated dopamine synthesis capacity, increased release and synaptic dopamine levels compared to healthy controls18,19,20,21,22. Moreover, dopamine releasing drugs induce psychosis23, dopamine blocking drugs attenuate psychosis24 and dopamine synthesis capacity correlates with positive symptoms in psychotic illness25,26. Elevated dopamine system function has also been shown in those at clinical high-risk, i.e. those that present with attenuated symptomatology, using PET27,28,29,30. Similarly, people with a first-degree relative with schizophrenia (FDR) as well as those with higher polygenic risk scores have higher dopamine synthesis capacity in the striatum31,32.
Striatal dopamine neurons largely originate from the midbrain substantia nigra and ventral tegmental area (SN/VTA complex)33. These dopamine producing neurons accumulate neuromelanin as a by-product of dopamine catabolism. Neuromelanin contains iron-rich deposits, which may be exploited and imaged using neuromelanin-sensitive MRI (NM-MRI)34,35. Accumulating evidence suggests NM-MRI can be a non-invasive means to capture this elevation in dopamine system function in psychotic illnesses34,36,37,38,39 within the SN/VTA complex, that correlates to measures of dopamine synthesis and release34,36,40. Higher NM-MRI signal has been associated with positive symptom severity in individuals with schizophrenia and clinical high-risk34,41, although results are mixed in clinical high-risk35.
The extent to which familial risk factors and subclinical psychotic symptoms like paranoid thoughts are linked with SN/VTA NM-MRI CNR signal remains completely unexplored. Thus, the two objectives of the current study were to first test if substantia nigra NM signal is elevated in those with an FDR with psychosis compared to healthy controls without an FDR with psychosis (controls; CTRs). Secondly, to determine whether occurrence of self-reported paranoid thoughts per se, regardless of risk, is associated with substantia nigra NM signal. In the present study, we enrolled participants with and without an FDR with a diagnosis of schizophrenia, schizoaffective disorder or bipolar disorder with psychotic features to undergo a neuromelanin-MRI scan. We hypothesized that 1) the FDR group would have an elevated NM-MRI CNR signal (hereinafter referred to as NM signal) in the SN/VTA complex and 2) that NM signal correlates positively with the frequency of self-reported paranoid thoughts.
Methods
Participants
A total of 80 controls and 25 FDR individuals (N = 105) were pooled from two studies using identical NM-MRI sequences (n = 75 [study 1]; n = 30 [study 2]). The study protocols were approved by The Royal Ottawa Healthcare Group Research Ethics Board (REB #s: 2019003 [study 1] and 2018042 [study 2]) and Declaration of Helsinki. All participants gave a written informed consent before entering the study.
Participants with severe medical illness, head trauma resulting in unconsciousness, current substance use disorders, past psychosis, positive urine drug test on the day of scanning (amphetamines, barbiturates, benzodiazepines, codeine, fentanyl, MDMA, methadone, methamphetamine, opiates, oxycodone, phencyclidine and/or THC; using VeriCheck [Verify Diagnostics, Barrie, Ontario]), and/or contraindications for MRI scanning were excluded from the study.
Two FDR participants screened positively for a current mental health disorder (one with social anxiety disorder and the other with generalized anxiety disorder) as determined by a combination of medical history and the MINI international neuropsychiatric interview for DSM-542. Although they screened positively, these two FDRs were included in the study. They were not taking any medication to treat their disorders. Additionally, a total of 30 combined CTR and FDR individuals screened positively for a past mental health episode or disorder. This included 22 individuals with a past major depressive episode, 6 individuals with past major depressive disorder; 3 individuals with a past manic episode; 1 individual with a past hypomanic episode; 4 individuals with lifetime panic disorder; 2 individuals with past alcohol use disorder; 4 individuals with past substance use disorder; 1 individual with past generalized anxiety disorder; and 2 individuals with lifetime antisocial personality disorder.
FDRs were recruited by referral from psychiatrists at the Royal Ottawa Mental Health Centre or from the community. FDR status was confirmed using the family interview for genetic studies - psychosis checklist43. None of the control participants had first or second-degree relatives with psychotic illness. After discarding three scans due to misplacement of the field of view stack during scanning, a final sample of 77 controls and 25 FDRs (n = 102) were included in the analysis. Table 1 presents the demographic variables and self-reported paranoia scores by FDR status44,45,46,47.
Measures
Paranoia was primarily assessed using the paranoia checklist (PCL-18), an 18-item self-report questionnaire used to evaluate trait-like paranoid ideation on three dimensions: frequency, distress and conviction44,45. The frequency, distress and conviction of each item are rated on a five-point scale. Thus, the minimum score that can be acquired in each dimension is 18 and the minimum total score that can be acquired is 54. Two controls scored more than three standard deviations above the mean on the PCL-18 conviction subscore (raw score > 70). All analyses were conducted with and without these two participants, which did not alter the main results (Supplementary Table S4). Thus, the results for the full sample (n = 102) are reported in the main article.
We further support the primary analysis in two ways. We first support our primary analysis using a revised 13-item state paranoia checklist (PCL-13), in which five items were dropped due to poor sensitivity in experimental manipulations of paranoia45. In the PCL-13 (to evaluate state-like paranoid ideation), individuals are asked how the statement applies at the moment on a 10-point scale rather than asking about frequency, distress and conviction separately. For the purpose of this study, we used the PCL-13 but retained the 3-dimensional split (frequency, conviction, distress).
We also support the primary analysis using the Community Assessment of Psychic Experience (CAPE). The CAPE is a 42-item questionnaire, where the frequency and distress of each item is rated on a four-point Likert scale. The 42 items assess one of positive, negative or depressive symptom dimensions46,47,48. However, a factor analysis of the positive dimension revealed a 5-factor solution including paranoia as a subfactor49,50. Thus, the paranoia subscale of the CAPE was included as another analysis to support the brain-behavior relationship as seen with the PCL.
MRI acquisition
MRI data were acquired using a 3 T mMR Biograph PET-MR system with a 12-channel head coil (Siemens, Erlangen, Germany). NM-MRI, first developed by Chen et al.51, were collected as previously described52. Briefly, images were collected using a 2-dimensional gradient recalled echo sequence with magnetization transfer pulse; repetition time = 337 ms, echo time = 3.97 ms, flip angle = 50, in-plane resolution = 0.43 × 0.43 mm, field of view = 165 × 220, 10 slices, slice thickness = 3 mm, magnetization transfer frequency offset = 1200 Hz, number of excitations = 6, acquisition time = 7.24 minutes. The 10 slices were positioned along the anterior commissure-posterior commissure line, starting 3 mm above the floor of the third ventricle. Additionally, T1-weighted MRI images were acquired using a multi-echo MPRAGE sequence53; spatial resolution = 1 mm isotropic; matrix = 256 × 256, number of slices = 192, repetition time (TR) = 2500 ms, echo time (TE) = 1.69, 3.55, 5.41, and 7.27 ms, flip angle = 7 degrees.
Processing of T1-weighted images and NM-MRI
T1-weighted and NM-MRI scans were preprocessed using a previously validated pipeline in Matlab v9.1 (MathWorks, Natick, MA)34,54. First, T1-weighted images were inhomogeneity field corrected using the ‘N4BiasFieldCorrection’ function (advanced normalization tools [ANTs; v2.3.5]). Then, brains were extracted using the ‘antsBrainExtraction’ function (ANTs). Transformation matrices for 1) NM-MRI to skull-stripped brain and 2) skull-stripped brain to MNI152 space were calculated using the ‘antsRegistrationSyN’ function (ANTs). Then, these transformations were applied to the NM-MRI image using the ‘antsApplyTransforms’ function in ANTs. The spatial normalized NM-MRI images were intensity normalized using the crus cerebri as a reference region. Finally, a 1 mm gaussian smoothing kernel was applied using the smooth3 function in SPM (v12.0)55. The final smoothed image was used for voxelwise analysis after visual inspection. Finally, the SN/VTA, psychosis and VTA NM-MRI averages were extracted for ROI-based robust regressions. The SN/VTA, psychosis, VTA and crus cerebri masks were generated from a previous study34.
Visualization and statistical analysis
All visualizations were made with seaborn 0.13.256 in python version 3.11. Independent-samples t-tests and chi-square tests on the demographic data were conducted using R (v4.5.1). To assess the voxelwise relationship between paranoia and NM-MRI, an SN/VTA voxelwise analysis controlling for age and sex was conducted in Matlab (MathWorks, Natick, MA) as previously described34. For each analysis, a robust regression was conducted for each voxel using the specified independent predictors and covariates (Supplementary Tables S2, 4, 5). The total number of significant positive voxels was computed and reported in Supplementary Tables S2, 4, 5. Then, permutation testing with 10,000 iterations was conducted, where subjects were randomly shuffled. Prior to permutation testing, voxels with CNR below −2.9% and above 21.5% were excluded to prevent undue influence of any single voxel. The lower and upper CNR thresholds were set to the lowest and highest 1% of values based on the distribution of all SN/VTA voxels in all subjects. Because some subjects have null (NaNs) on some values, we ensure that the permutation also excludes these values on a voxel-by-voxel basis. For each permutation, the total count of voxels that passed a one-tailed p-value threshold of 0.05 was computed. The observed count of significant voxels from the original analysis was compared against the null distribution generated from the 10,000 permutations. This max-T permutation test was conducted to preserve power while stringently correcting for false positives57. We supported the voxelwise analyses with independent-samples t-tests on whole SN/VTA, psychosis and VTA only masks using R (v4.5.1). Robust regressions on whole SN/VTA, psychosis, and VTA only masks were conducted using R (v4.5.1) as well.
Results
Sample characteristics
Before comparing SN/VTA NM-MRI signals between groups, we looked for differences in age, sex, and paranoia frequency scores (Table 1). Individuals with an FDR and without a FDR had similar age and sex distributions (Table 1). There was no difference in PCL subscores or total score between groups (Table 1). Finally, the distribution of frequency, conviction and distress in the total group were not normal and differed from each other (Table 1; Supplementary Fig. S1A).
SN/VTA NM signal is unaltered in FDRs
We first sought to examine differences in NM signal between CTRs and FDRs. Because the NM signal is a proxy of dopamine turnover over the lifespan, it is important to control for age58,59. A voxelwise analysis examining the effect of FDR status, controlling for age and sex, revealed scattered bidirectional changes with minimal clustering in the ventral SN that did not survive permutation testing (Supplementary Table S2). Furthermore, ROI-based analysis using the whole SN/VTA, voxels previously associated with psychotic symptoms (referred to as the psychosis mask) or VTA34 revealed no difference between CTR and FDR groups (t-test; p’s > 0.05; Supplementary Table S1; Supplementary Fig. S2A; but also a robust regression controlling for age and sex; p’s > 0.05; data not shown). We also examined the same ROIs with a binarized age variable (younger/older than 30 for both CTR and FDR) as in a previous analysis39,60. Here, we binarize groups by age because younger individuals are at a higher risk for psychosis. We found no differences in NM signal between younger CTRs and FDRs, or older CTRs and FDRs (t-test; p’s > 0.05; Supplementary Fig. S2B). We examined the same ROIs across four groups: those with sibling, parent FDRs or both, separately as in a previous analysis31. Here, the rationale for splitting FDRs by genetic relationship is because children of affected individuals have a higher risk of developing psychosis relative to siblings4. We found no differences in NM signal between those without an FDR, siblings or children FDRs (one-way ANOVA; p’s > 0.05; Supplementary Fig. S2C). Lastly, we examined these same ROIs across CTRs and FDRs with and without a past diagnosis to examine how past diagnosis could affect NM signal. In the whole group, past diagnosis was not associated with the ROI-based SN/VTA NM signal, controlling for age and sex (F(1,98) = 0.26, p > 0.05, robust regression, n = 102; data not shown). However, in an exploratory subgroup analysis, we found that FDRs with past diagnosis had elevated VTA NM signal compared to FDRs without a past diagnosis (t-test; p < 0.05, uncorrected; Supplementary Fig. S2D).
SN/VTA NM signal is associated with self-reported frequency of paranoid thoughts
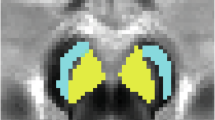
Despite no group difference in SN/VTA NM signal, we asked whether individuals from the CTR and FDR groups combined, have elevated NM signal with respect to reported subclinical paranoia. A voxelwise analysis including FDR status, age and sex as covariates revealed a large number of voxels in the dorsomedial SN/VTA complex that were positively associated with self-reported frequency of paranoid thoughts (255 of 1879 voxels at p < 0.05, pcorrected = 0.03, n = 102, robust regression, Fig. 1A; Supplementary Table S2). This effect survived permutation correction for multiple comparisons (10,000 iterations). We also conducted an analysis more sensitive to state paranoia using the truncated 13-item state PCL frequency score45 and further support our main finding (251 of 1879 voxels at p < 0.05, pcorrected = 0.03, n = 102, robust regression, Supplementary Table S2). The voxelwise effect was also supported by an ROI analysis using the whole SN/VTA ROI (F(1,97) = 4.4, p = 0.04, robust regression, n = 102; Fig. 1A; Supplementary Table S3). Lastly, we sought to supplement this brain-behavior relationship using the CAPE paranoia frequency subscores49,50. A similar voxelwise analysis revealed a large number of voxels in the dorsomedial SN were also associated with self-reported frequency using the CAPE (316 of 1879 voxels at p < 0.05, pcorrected = 0.01, n = 102, robust regression, Fig. 1B; Supplementary Table S2) but only trending when using the whole SN/VTA ROI (F(1,97) = 3.8, p = 0.06, robust regression, n = 102; Fig. 1B). We also examined other aspects of paranoia severity. Although the frequency subscore was associated significantly with conviction and distress subscores (Supplementary Fig. S1B), the conviction, distress and total scores were not significantly associated with NM signal in the SN/VTA complex (Supplementary Table S2). Interestingly, past diagnosis was also associated with the PCL frequency score while controlling for age and sex (F(1,98) = 13.5, p < 0.001, robust regression, n = 102; data not shown).

A Voxelwise t-map of significant voxels only (p < 0.05, uncorrected) between PCL frequency score and SN/VTA CNR (axial view, z = −14, −12, −10). 255/1879 voxels along the dorsomedial SN were positively correlated with PCL frequency score while controlling for group status, age and sex (pcorrected = 0.03, robust regression, permutations = 10,000). Similar to voxelwise results, ROI analysis of the whole SN/VTA complex showed a significant association (bottom; robust regression, F(1,97) = 4.4, p = 0.04, r = 0.22 [effect size]). Note that the size of the data point indicates relative age. B Voxelwise t-map of significant voxels only (p < 0.05, uncorrected) between CAPE paranoia frequency score and SN/VTA CNR (significant voxels only) (axial view, z = −14, −12, −10). 316/1879 voxels also along the dorsomedial SN were positively correlated with CAPE paranoia frequency score with controlling for group status, age and sex (pcorrected = 0.01, robust regression, permutations = 10,000). When looking at the whole SN/VTA complex, the CAPE paranoia frequency score showed a borderline significant positive association (bottom; robust regression, F(1,97) = 3.8, p = 0.06, r = 0.22 [effect size]). Note that the size of the data point indicates relative age.
Discussion
The first objective of the current study was to examine if FDRs have elevated NM signal relative to CTRs. We report no difference in NM signal between those without and with a FDR when examining the signal in the whole SN/VTA complex, a psychosis mask and the VTA only34 (Supplementary Fig. S2A). Additionally, there were no differences between CTRs and FDRs when examining younger versus older individuals, and FDR relationship status (Supplementary Fig. S2B, C). Our failure to find a difference in NM levels thus does not support the idea that dopamine neurons of the SN/VTA complex are overactive in this unaffected FDR sample. It is important to note, however, that our sample sizes were powered to detect moderate-to-large effect sizes; thus, we cannot rule out the existence of smaller group differences.
While increased NM signal in the SN/VTA complex is a well replicated result reported in several populations affected by psychosis36,37,39,61, several factors may explain our null finding. First, we investigated FDRs unaffected by psychosis. This is in line with recent results reporting increased NM signal in more severe but not less severe psychosis39 nor clinical high-risk individuals41. However, an exploratory analysis revealed those FDRs with a past mental health diagnosis may have higher NM signal (Supplementary Fig. S2D), suggesting dopamine neurons may be overactive in more mentally vulnerable FDRs.
A second key finding of our study is that NM signal correlates with subclinical measures of paranoid thought frequency (Fig. 1). There are very few studies examining dopaminergic measures and their relation to psychotic experiences in healthy individuals62,63. Examining associations between dopaminergic measures and more common and more heritable symptoms, such as paranoia8, may increase sensitivity. This interpretation may explain a lack of association of dopaminergic measures with auditory hallucination but not schizotypal personality traits62,63. Building on this, we show for the first time that a proxy of dopamine function localized roughly to the dorsomedial SN correlates with the PCL frequency subscale, and that this association holds true regardless of FDR status. We further support this association using the CAPE paranoia frequency subscale as a comparable measure. This aligns with previous NM-MRI and PET studies where dopamine activity in the SN/VTA complex correlates with positive symptoms in schizophrenia and clinical high-risk in some, but not all, reports25,30,34,41,64,65. Our study adds to the literature by showing that this association exists for subclinical paranoia in a non-clinical population, irrespective of familial risk.
Interestingly, this correlation was present for the frequency of paranoid thoughts, but not their conviction or distress. This dissociation may be explained in several ways. One possibility is selection bias; by excluding participants with clinical psychosis, we may have also excluded those with high preoccupation and distress scores, which are factors that tend to differentiate clinical from non-clinical populations66. Alternatively, the frequency of paranoid thoughts may be directly reflected by elevated SN/VTA NM signal, while the associated distress and/or conviction are mediated by other mechanisms. This interpretation is supported by pharmacological studies, which show that the early phases of antipsychotic treatment reduce preoccupation and distress but not the conviction of delusional symptoms67,68. This implies that dopamine may be differently involved with distinct aspects of delusion severity.
The fact that NM signal accumulates slowly over the lifespan is more congruent with it being a trait marker of paranoia. Furthermore, state paranoia was not more strongly associated with NM-MRI than the total PCL score (Supplementary Table S2). Paranoia is indeed present in the general population, suggesting paranoia exists on a continuum with clinical paranoid delusion9,11,69. Thus, paranoia may represent a sort of psychosis proneness70,71. Here, our data suggests overactive SN/VTA dopamine neurons, reflected by an increase in SN/VTA CNR, may be associated with the occurrence of paranoid thoughts, but relatively greater SN/VTA dopaminergic activity of the magnitude observed here is not sufficient to make these paranoid thoughts distressful.
There are several limitations to the current study. First, we used only familial status as a pseudo-quantitative marker of genetic risk. Studies examining the total burden of several genetic factors, such as polygenic risk score, may be more sensitive when examining differences in NM signal related to genetic risk. Furthermore, our subgroup analyses (binarized age, FDR relationship type, past diagnosis) may have been underpowered to detect small between-group differences in NM signal; as with our primary analysis, effects below a moderate-to-large size level cannot be ruled out.
In conclusion, this is the first study to examine self-reported paranoia in relation to NM signal in the SN/VTA complex in healthy individuals with and without an FDR. Our results suggest that elevated dopamine signaling, as indexed by NM-MRI, confers susceptibility to the experience (i.e., frequency) of subclinical paranoia, regardless of familial risk. These data support the idea that while elevated SN/VTA NM signal is associated with the experience of subclinical paranoia, other factors, be it biological or environmental, may be necessary for these experiences to transition into distressing, convicted paranoia, as in clinical psychosis.
Data availability
The data are available upon reasonable request.
References
Sullivan, P. F., Yao, S. & Hjerling-Leffler, J. Schizophrenia genomics: genetic complexity and functional insights. Nat. Rev. Neurosci. 25, 611–624 (2024).
Trubetskoy, V. et al. Mapping genomic loci implicates genes and synaptic biology in schizophrenia. Nature 604, 502–508 (2022).
Torti, M. C. et al. Schizotypy and personality profiles of Cluster A in a group of schizophrenic patients and their siblings. BMC Psychiatry 13, 245 (2013).
Tsuang, M. T., Stone, W. S. & Faraone, S. V. Schizophrenia: a review of genetic studies. Harv. Rev. Psychiatry 7, 185–207 (1999).
McGrath, J. J. et al. Psychotic experiences in the general population: a cross-national analysis based on 31,261 respondents from 18 countries. JAMA Psychiatry 72, 697–705 (2015).
van Os, J., Linscott, R. J., Myin-Germeys, I., Delespaul, P. & Krabbendam, L. A systematic review and meta-analysis of the psychosis continuum: evidence for a psychosis proneness-persistence-impairment model of psychotic disorder. Psychol. Med. 39, 179–195 (2009).
van Os, J. Is there a continuum of psychotic experiences in the general population? Epidemiol. Psichiatr. Soc. 12, 242–252 (2003).
Taylor, M. J., Freeman, D., Lundström, S., Larsson, H. & Ronald, A. Heritability of psychotic experiences in adolescents and interaction with environmental risk. JAMA Psychiatry 79, 889–897 (2022).
Eaton, W., Romanoski, A., Anthony, J. & Nestadt, G. Screening for psychosis in the general population with a self-report interview. J. Nerv. Ment. Dis. 179, 689–693 (1991).
Bebbington, P. E. et al. The structure of paranoia in the general population. Br. J. Psychiatry 202, 419–427 (2013).
Elahi, A., Perez Algorta, G., Varese, F., McIntyre, J. C. & Bentall, R. P. Do paranoid delusions exist on a continuum with subclinical paranoia? A multi-method taxometric study. Schizophr. Res. 190, 77–81 (2017).
Freeman, D. et al. Concomitants of paranoia in the general population. Psychol. Med. 41, 923–936 (2011).
Raihani, N. J. & Bell, V. An evolutionary perspective on paranoia. Nat. Hum. Behav. 3, 114–121 (2019).
Nour, M. M. et al. Dopaminergic basis for signaling belief updates, but not surprise, and the link to paranoia. Proc. Natl. Acad. Sci. USA. 115, E10167–E10176 (2018).
Dahoun, T. et al. The relationship between childhood trauma, dopamine release and dexamphetamine-induced positive psychotic symptoms: a [11C]-(+)-PHNO PET study. Transl. Psychiatry 9, 287 (2019).
Egerton, A. et al. Adversity in childhood linked to elevated striatal dopamine function in adulthood. Schizophr. Res. 176, 171–176 (2016).
Schalbroeck, R., van Hooijdonk, C. F. M., Bos, D. P. A., Booij, J. & Selten, J.-P. Chronic social stressors and striatal dopamine functioning in humans: a systematic review of SPECT and PET studies. Mol. Psychiatry 29, 3841–3856 (2024).
Reith, J. et al. Elevated dopa decarboxylase activity in living brain of patients with psychosis. Proc. Natl. Acad. Sci. USA. 91, 11651–11654 (1994).
Hietala, J. et al. Depressive symptoms and presynaptic dopamine function in neuroleptic-naive schizophrenia. Schizophr. Res. 35, 41–50 (1999).
Brugger, S. P. et al. Heterogeneity of striatal dopamine function in schizophrenia: meta-analysis of variance. Biol. Psychiatry 87, 215–224 (2020).
Lindström, L. H. et al. Increased dopamine synthesis rate in medial prefrontal cortex and striatum in schizophrenia indicated by L-(beta-11C) DOPA and PET. Biol. Psychiatry 46, 681–688 (1999).
McCutcheon, R. A., Abi-Dargham, A. & Howes, O. D. Schizophrenia, dopamine and the striatum: from biology to symptoms. Trends Neurosci 42, 205–220 (2019).
Bell, D. S. The experimental reproduction of amphetamine psychosis. Arch. Gen. Psychiatry 29, 35–40 (1973).
Seeman, P., Chau-Wong, M., Tedesco, J. & Wong, K. Brain receptors for antipsychotic drugs and dopamine: direct binding assays. Proc. Natl. Acad. Sci. USA. 72, 4376–4380 (1975).
Jauhar, S. et al. A test of the transdiagnostic dopamine hypothesis of psychosis using positron emission tomographic imaging in bipolar affective disorder and schizophrenia. JAMA Psychiatry 74, 1206–1213 (2017).
Jauhar, S. et al. The relationship between cortical glutamate and striatal dopamine in first-episode psychosis: a cross-sectional multimodal PET and magnetic resonance spectroscopy imaging study. Lancet Psychiatry 5, 816–823 (2018).
Howes, O. D. et al. Dopamine synthesis capacity before onset of psychosis: a prospective [18F]-DOPA PET imaging study. Am. J. Psychiatry 168, 1311–1317 (2011).
Howes, O. et al. Progressive increase in striatal dopamine synthesis capacity as patients develop psychosis: a PET study. Mol. Psychiatry 16, 885–886 (2011).
Mizrahi, R. et al. Increased stress-induced dopamine release in psychosis. Biol. Psychiatry 71, 561–567 (2012).
Girgis, R. R. et al. Imaging synaptic dopamine availability in individuals at clinical high-risk for psychosis: a [11C]-(+)-PHNO PET with methylphenidate challenge study. Mol. Psychiatry 26, 2504–2513 (2021).
Huttunen, J. et al. Striatal dopamine synthesis in first-degree relatives of patients with schizophrenia. Biol. Psychiatry 63, 114–117 (2008).
Eisenberg, D. P. et al. Genetic risk for treatment resistant schizophrenia and corresponding variation in dopamine synthesis capacity and D2/3 receptor availability in healthy individuals. Mol. Psychiatry 30, 2645–2652 (2024).
Weinstein, J. J. et al. Pathway-specific dopamine abnormalities in schizophrenia. Biol. Psychiatry 81, 31–42 (2017).
Cassidy, C. M. et al. Neuromelanin-sensitive MRI as a noninvasive proxy measure of dopamine function in the human brain. Proc. Natl. Acad. Sci. USA. 116, 5108–5117 (2019).
Wengler, K., Trujillo, P., Cassidy, C. M. & Horga, G. Neuromelanin-sensitive MRI for mechanistic research and biomarker development in psychiatry. Neuropsychopharmacology 50, 137–152 (2024).
Vano, L. J. et al. Mesostriatal dopaminergic circuit dysfunction in schizophrenia: A multimodal neuromelanin-sensitive magnetic resonance imaging and [18F]-DOPA positron emission tomography study. Biol. Psychiatry 96, 674–683 (2024).
Wieland, L., Fromm, S., Hetzer, S., Schlagenhauf, F. & Kaminski, J. Neuromelanin-sensitive magnetic resonance imaging in schizophrenia: a meta-analysis of case-control studies. Front. Psychiatry 12, 770282 (2021).
van Hooijdonk, C. F. M. et al. Striatal dopamine synthesis capacity and neuromelanin in the substantia nigra: a multimodal imaging study in schizophrenia and healthy controls. Neurosci. Appl. 2, 101134 (2023).
Ueno, F. et al. Neuromelanin accumulation in patients with schizophrenia: a systematic review and meta-analysis. Neurosci. Biobehav. Rev. 132, 1205–1213 (2022).
Zucca, F. A. et al. Neuromelanin of the human substantia nigra: an update. Neurotox. Res. 25, 13–23 (2014).
Wengler, K. et al. Generalizability and out-of-sample predictive ability of associations between neuromelanin-sensitive magnetic resonance imagingand psychosis in antipsychotic-free individuals. JAMA Psychiatry 81, 198–208 (2024).
Sheehan, D. V. et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 59, 22–33 (1998).
Maxwell, M. E. Manual for the FIGS (National Institute of Mental Health, 1992).
Freeman, D. et al. Psychological investigation of the structure of paranoia in a non-clinical population. Br. J. Psychiatry 186, 427–435 (2005).
Schlier, B., Moritz, S. & Lincoln, T. M. Measuring fluctuations in paranoia: Validity and psychometric properties of brief state versions of the Paranoia Checklist. Psychiatry Res. 241, 323–332 (2016).
Brenner, K. et al. Validation of the English and French versions of the Community Assessment of Psychic Experiences (CAPE) with a Montreal community sample. Schizophr. Res. 95, 86–95 (2007).
Mossaheb, N. et al. The Community Assessment of Psychic Experience (CAPE) questionnaire as a screening-instrument in the detection of individuals at ultra-high risk for psychosis. Schizophr. Res. 141, 210–214 (2012).
Stefanis, N. C. et al. Evidence that three dimensions of psychosis have a distribution in the general population. Psychol. Med. 32, 347–358 (2002).
Wigman, J. T. W. et al. The structure of the extended psychosis phenotype in early adolescence—a cross-sample replication. Schizophrenia Bull. 37, 850–860 (2011).
Wigman, J. T. W. et al. Replication of the five-dimensional structure of positive psychotic experiences in young adulthood. Psychiatry Res. 197, 353–355 (2012).
Chen, X. et al. Simultaneous imaging of locus coeruleus and substantia nigra with a quantitative neuromelanin MRI approach. Magn. Reson. Imaging 32, 1301–1306 (2014).
McCall, A. et al. Evidence for locus coeruleus-norepinephrine system abnormality in military posttraumatic stress disorder revealed by neuromelanin-sensitive magnetic resonance imaging. Biol. Psychiatry 96, 268–277 (2024).
van der Kouwe, A. J. W., Benner, T., Salat, D. H. & Fischl, B. Brain morphometry with multiecho MPRAGE. Neuroimage 40, 559–569 (2008).
Wengler, K., He, X., Abi-Dargham, A. & Horga, G. Reproducibility assessment of neuromelanin-sensitive magnetic resonance imaging protocols for region-of-interest and voxelwise analyses. Neuroimage 208, 116457 (2020).
Ashburner, J. et al. SPM12 manual. Wellcome Trust Centre forNeuroimaging (2014).
Waskom, M. seaborn: statistical data visualization. J. Open Source Softw. 6, 3021 (2021).
Nichols, T. E. & Holmes, A. P. Nonparametric permutation tests for functional neuroimaging: a primer with examples. Hum. Brain Mapp. 15, 1–25 (2002).
Shibata, E. et al. Age-related changes in locus ceruleus on neuromelanin magnetic resonance imaging at 3 Tesla. Magn. Reson. Med. Sci. 5, 197–200 (2006).
Xing, Y., Sapuan, A., Dineen, R. A. & Auer, D. P. Life span pigmentation changes of the substantia nigra detected by neuromelanin-sensitive MRI. Mov. Disord. 33, 1792–1799 (2018).
Watanabe, Y. et al. Neuromelanin magnetic resonance imaging reveals increased dopaminergic neuron activity in the substantia nigra of patients with schizophrenia. PLoS One 9, e104619 (2014).
Ahrens, J. et al. Convergence of cannabis and psychosis on the dopamine system. JAMA Psychiatry, https://doi.org/10.1001/jamapsychiatry.2025.0432 (2025).
Woodward, N. D. et al. Correlation of individual differences in schizotypal personality traits with amphetamine-induced dopamine release in striatal and extrastriatal brain regions. Am. J. Psychiatry 168, 418–426 (2011).
Howes, O. D. et al. Dopaminergic function in the psychosis spectrum: an [18F]-DOPA imaging study in healthy individuals with auditory hallucinations. Schizophr. Bull. 39, 807–814 (2013).
Howes, O. D. et al. Midbrain dopamine function in schizophrenia and depression: a post-mortem and positron emission tomographic imaging study. Brain 136, 3242–3251 (2013).
Tseng, H.-H. et al. Nigral stress-induced dopamine release in clinical high risk and antipsychotic-naïve schizophrenia. Schizophr. Bull. 44, 542–551 (2018).
Sisti, D. et al. Preoccupation and distress are relevant dimensions in delusional beliefs. Compr. Psychiatry 53, 1039–1043 (2012).
Mizrahi, R. et al. The selective effect of antipsychotics on the different dimensions of the experience of psychosis in schizophrenia spectrum disorders. Schizophr. Res. 88, 111–118 (2006).
So, S. H.-W., Peters, E. R., Swendsen, J., Garety, P. A. & Kapur, S. Changes in delusions in the early phase of antipsychotic treatment - an experience sampling study. Psychiatry Res. 215, 568–573 (2014).
Ellett, L., Lopes, B. & Chadwick, P. Paranoia in a nonclinical population of college students. J. Nerv. Ment. Dis. 191, 425–430 (2003).
Thewissen, V., Bentall, R. P., Lecomte, T., van Os, J. & Myin-Germeys, I. Fluctuations in self-esteem and paranoia in the context of daily life. J. Abnorm. Psychol. 117, 143–153 (2008).
Ellett, L. et al. Experimental studies of paranoid thinking in clinical and nonclinical populations: a systematic review and meta-analysis. Psychol. Med. 53, 5933–5944 (2023).
Acknowledgements
We would like to acknowledge our research participants, especially family members of patients with psychosis, for their participation. This research was supported by the Emerging Research Innovators in Mental Health Award (The Royal) to L.T., the Brain and Behavior foundation NARSAD Young Investigator Award to L.T. and the Canadian Institute of Health Research Project Grant to L.T. and S.G.
Author information
Authors and Affiliations
Contributions
Rami Hamati: Investigation, Data Curation, Writing - Original Draft, Writing - Review & Editing, Formal Analysis, Visualization. Bianca Chidiac: Investigation, Data Curation. Nour Kanaa: Writing - Review & Editing Synthia Guimond: Resources, Writing - Review & Editing Clifford. Cassidy: Methodology, Software, Supervision, Writing - Review & Editing. Lauri Tuominen: Conceptualization, Methodology, Supervision, Writing - Review & Editing, Funding acquisition.
Corresponding author
Ethics declarations
Competing interests
R.H. previously owned shares in Karuna Therapeutics Inc. and received two knowledge dissemination grants from Otsuka Canada Pharmaceutical Inc. to organize local trainee conferences. S.G. received honoraria/has been a consultant for Boehringer-Ingelheim (Canada) Ltd. C.M.C. is inventor on a patent using the methodology employed in this study that is licensed to Terran Biosciences Inc. but has not received royalties. L.T. and S.G. received a knowledge dissemination grant from Otsuka Canada Pharmaceutical Inc. and Abbvie Inc. to organize a pan-Canadian schizophrenia conference. The remaining authors have nothing to disclose.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Hamati, R., Kanaa, N., Chidiac, B. et al. SN/VTA neuromelanin signal is associated with subclinical paranoia irrespective of familial risk for psychosis. Schizophr 12, 25 (2026). https://doi.org/10.1038/s41537-026-00731-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41537-026-00731-4
