
Abstract
This study aimed to evaluate associations between plant-based diets and the prevalence of depressive symptoms (DepS) among Chinese middle-aged and older adults. This study included 3153 participants aged 45 and older. Dietary intake was collected using a food frequency questionnaire, and DepS was evaluated using the 9-item Patient Health Questionnaire. Foods were classified into 17 groups and three plant-based diet indices were created, including the overall plant-based diet index (PDI), healthful plant-based diet index (hPDI), and unhealthful plant-based diet index (uPDI). Compared to the lowest quartile, participants in the highest quartile of hPDI had lower odds of DepS (OR = 0.60; 95% CI: 0.40, 0.89). Conversely, the highest quartile of the uPDI was associated with higher odds of DepS (OR = 1.81; 95% CI: 1.16, 2.82). These findings supported that the quality of plant-based diets matters for mental health.
Similar content being viewed by others

Introduction
Depressive symptoms (DepS) are one of the most universal mental disorders1, that frequently show up in a combination of mental and physical symptoms, accompanied by psychomotor and cognitive disorders2. Middle-aged and older populations are a high prevalence of DepS, and the detection rate among Chinese adults aged 45 and above was as high as 32.7% in 20183. Previous studies showed that DepS have been associated with an increased risk of dementia4, acute myocardial infarction5, and suicide6. With the challenge of population aging and the substantial public health problem of DepS, it is imperative to find potentially modifiable risk factors to protect against the onset of DepS.
Sociodemographic characteristics, unhealthy habits, and poor health status are typically described as risk factors for DepS7. In the field of nutritional psychiatry, it’s recognized that diet patterns may play a critical role in DepS. For instance, the Mediterranean dietary pattern8 was positively associated with decreased risks of DepS, whereas the animal food pattern9 and pro-inflammatory diet10 were shown an inverse association. Plant-based diets (plant-based dietary patterns), which emphasize a higher intake of plant-source foods and a lower intake of animal-source foods11, have been associated with decreased risks of hypertension12, type 2 diabetes13, and mortality14. Raising questions about whether these numerous potential benefits to human health extend to DepS.
Earlier research on vegetarian diets has not distinguished between healthier (high-quality) and unhealthier (low-quality) plant foods. However, mounting evidence shows that not all plant-source foods have health benefits15, and the quality of plant-based diets has received considerable attention in recent years. For healthful plant-based diets, which contain more high-quality healthy plant foods (e.g., whole grains, fresh fruits, fresh vegetables, nuts, legumes, and tea) and less low-quality unhealthy plant foods (e.g., fruit juices, refined grains, sugar-sweetened beverages, sweets and desserts, and salt-preserved vegetable) and animal foods. While unhealthful plant-based diets indicate higher consumption of unhealthy plant foods and animal foods under the background of overall plant-based diets11.
Up to now, many studies on the associations between various dietary patterns and mental health, but only three studies have explored the relationship between plant-based diets and DepS16,17,18. However, previous studies’ results have been an inconsistent, and rare concern for general middle-aged and older adults, and no prior research on plant-based diets and DepS has been conducted in China. China was originally an East Asian country with predominantly grains and vegetables, but with rapid transition in dietary structure in the past decades, including an increased intake of animal products and more processed food19. Thus, we aimed to examine the associations between plant-based diets (reflected by the plant-based diet indices) and DepS risks among Chinese middle-aged and older adults, to discover potentially achievable dietary recommendations that may benefit mental health across minor changes in dietary nutrition consumption.
Results
The baseline characteristics of participants across quartiles of PDI are presented in Table 1. A total of 3153 participants were included in the current study, and the mean age was 62 (SD, 6.4) years, 6.76% of whom were reported with DepS. Participants with higher scores of PDI were more likely to have higher total energy intake (Table 1).
We initially examined the association between three plant-based diet indices and the risk of DepS, and the results are shown in Table 2. In the multivariable-adjusted model, a strong negative association was observed between higher hPDI scores and DepS. Compared with Q1, participants in Q4 of the hPDI scores had lower odds of DepS (OR = 0.60; 95% CI: 0.40, 0.89; Ptrend < 0.01). In contrast, participants in the highest quartile of uPDI were associated with higher odds of DepS (OR = 1.81; 95% CI: 1.16, 2.82; Ptrend < 0.01), compared with the lowest quartile (Table 2). Each 10-unit increment in uPDI was associated with a 51% (OR = 1.51; 95% CI: 1.20, 1.91) increased odds of DepS, whereas a per 10-unit increment of hPDI was associated with a 35% (OR = 0.65; 95% CI: 0.50, 0.85) decreased odds of DepS.
When the outcome variable was included as a continuous variable in the multivariable-adjusted model, a significant association of hPDI and uPDI with DepS was observed. There was an inverse association between hPDI scores and PHQ-9 scores, with a per 10-unit increment of hPDI scores associated with 28% lower odds of DepS (β = -0.28, 95% CI: −0.42, −0.15; P < .001), whereas uPDI scores were positively associated with a higher odds of DepS (β = 0.36, 95% CI: 0.25, 0.48; P < .001) (Table 3).
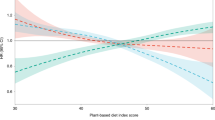
The RCS regression model was used to examine the non-linear relationships between PDIs and the risk of DepS. No significant non-linear relationship was observed between PDI and DepS odds. We found that higher hPDI scores were associated with monotonically decreasing DepS odds, while higher uPDI scores were related to monotonically increasing DepS odds. (Pnonlinear for PDI = 0.363; Pnonlinear for hPDI = 0.461; Pnonlinear for uPDI = 0.102) (Fig. 1).

PDIs plant-based diet indices, PDI overall plant-based diet index, hPDI healthful plant-based diet index, uPDI unhealthful plant-based diet index, DepS depressive symptoms. The RCS curves incorporating all confounders, sex, age, education level, household income, marital status, physical activity, smoking status, alcohol consumption, total energy intake, BMI, diabetes, CVD, and hypertension.
The relationship between individual food groups and DepS are reported in the Supplementary Material (Supplementary Table 2). For individual plant-based foods items, fresh fruits (ORå 1 time/ d versus ≤1 time/ d = 0.60; 95% CI: 0.42, 0.85) and tea (OR≥1 time/ week versus never = 0.42; 95% CI: 0.21, 0.84) were the dominant factors contributing to the positive association between PDI and hPDI. On the contrary, higher intake of refined grains (ORå 1 time/ d versus ≤1 time/ d = 3.30; 95% CI: 1.03, 10.55), sugar-sweetened beverages (ORevery day versus never = 10.79; 95% CI: 3.43, 33.97), sweets and desserts (ORevery day versus never = 1.52; 95% CI: 1.01, 2.28), salt-preserved vegetables (OR≥1 time/ m versus never = 1.71; 95% CI: 1.14, 2.57), and eggs (ORå 1 time/ d versus ≤1 time/d = 1.36; 95% CI: 1.01, 1.82) contributed to the association between uPDI with higher odds of DepS. Interestingly, we also observed that daily intake of milk or dairy products was associated with lower odds of DepS (ORevery day versus never = 0.63; 95% CI: 0.42, 0.95).
Discussion
In this cross-sectional study among Chinese middle-older aged adults, we found that adherence to healthy plant-based diets was associated with lower odds of DepS. In contrast, unhealthy plant-based diets were markedly associated with higher odds of DepS. These associations were independent of socioeconomic factors, lifestyles, and major chronic diseases.
A dietary pattern based on a high amount of plant foods (Planetary Health Diet, Mediterranean Diet, Vegetarian Diet) is not the same as plant-based diets. The key difference between plant-based diets and other dietary patterns is the unique three plant-based dietary indices. To date, only three studies have examined the relationship between plant-based diets and depression, two studies were conducted on adults (not over 55 years old) and the other was studied in a diabetic population. In a cross-sectional study of 435 women aged 20–50 years old, a plant-based diet, particularly healthful-rich plant foods, was associated with a decreased risk of depression compared with an unhealthy plant diet16. Mousavi et al. have reported that there was a reverse association between adherence to an overall plant-based diet, and a healthy plant-based diet and depression, but no significant association was found between an unhealthy plant-based diet and depression17. Among 230 women with diabetes, an unhealthy plant diet had a greater risk of depression, while a healthy plant-based diet was associated with a lower risk of depression18. Our research showed that a healthy plant-based diet was significantly associated with lower odds of DepS, and an unhealthy plant-based diet was related to increased odds of DepS among Chinese middle-aged and older adults.
Several potential mechanisms may explain the observed association. First, plant foods are rich in antioxidants (e.g., vitamins and carotenoid compounds) and have potential protective effects against DepS by reducing the level of oxidative stress20,21. Second, vegetables and fruits are rich in folate, which is deficient and may lead to reduced availability of S-adenosylmethionine and increased homocysteine concentrations, which are important in the pathophysiology of depression22. Third, healthy plant-based diets such as yellow vegetables, green leafy vegetables, whole grains, coffee, and tea, rich in anti-inflammatory compounds (e.g., vitamins, fiber, flavonoids, and carotenoids)23 were shown to influence the concentration of monoamines, which play a key role in regulating emotions24. On the contrary, unhealthy plant-based and animal-based foods containing sugar-sweetened beverages, refined grains, red or processed meat, and organ meats are pro-inflammatory foods25. Furthermore, healthy plant-based foods, including whole grains, vegetables, fruits, nuts, coffee, tea, and legumes, are rich in naturally occurring plant compounds polyphenols (e.g., soy isoflavones, tea, and cocoa flavanols, curcumin and coffee hydroxycinnamic acid, walnut flavanols, and citrus flavanones) that benefit mental health by upregulating the body’s natural defense systems and stabilizing free radicals, decreasing oxidative damage, as well as producing neuroprotective properties by regulating specific cellular signaling pathways26,27,28.
DepS are suffered by more than 300 million people worldwide29. In China, late-life DepS is also a serious public concern30. At the same time, China’s food consumption patterns have changed considerably in the past decades, with growth in the consumption of processed foods and animal foods19. To the best of our knowledge, this study was the first to show the association between three types of plant-based diets and DepS in Chinese middle-aged and older adults. The findings may contribute to the literature in that previous studies have focused on Iranian populations, while we were concerned with Chinese with unique dietary habits. For the food components, considering the greater consumption of preserved vegetables in China, we have creatively included salt-preserved vegetables in the category of unhealthy plant foods. Instead of consuming a single nutrient or food, individuals commonly consume several combinations of nutrients and foods daily, and our plant-based dietary model considers the cumulative and synergic effects of the overall diet. We also classified plant-based foods as healthy and unhealthy to better evaluate the potential association between the quality of plant-based diets and DepS. In addition, a series of covariate variables were taken into account in the adjustment model, including sociodemographic, lifestyle, and multimorbidity factors. Several limitations to the current study should be acknowledged. First, this study is a cross-sectional design and provides a hint for the benefits of healthy plant-based diets on DepS, but causality cannot be established. Notably, longitudinal evidence in this regard is needed. Second, the assessment measures used for outcomes only assess DepS and are not representative of a clinical diagnosis of depression. However, the PHQ-9 is the most widely used scale to assess nine DepS in the global background31. Furthermore, although numerous covariates were considered, we cannot rule out the residual confounder because of the observational study’s nature.
Adherence to a healthy plant-based diet is associated with lower DepS odds, whilst an unhealthy plant-based diet is associated with higher DepS odds. Our findings suggested that a plant-based diet rich in healthier plant food may benefit DepS. More studies with high-quality and prospective designs are needed to corroborate our findings.
Materials and methods
Study design and population
The Lifestyle and Healthy Aging of Chinese Square Dancer Study (Healthy Dance Study) are designed to monitor the dietary nutrition and physical-psychological health of the Chinese population aged 45 and older. The inclusion criteria of the Healthy Dance Study were applied as follows: (i) age ≥45 years; (ii) regular participation in square dance currently, with frequency at least once a week; (iii) permanent resident population in the survey area (living in the area for more than 6 months before the survey); (iv) no participation in any clinical trial or other intervention programs in the past 3 months or the future. Participants who were diagnosed with deafness, dumb, or serious mental illness and were unable to complete the survey under the assistance of research staff were excluded. The present study was conducted from August 2020 to December 2021 in seven counties in China, including Beijing, Shanghai, Wuhan, Yichang, Xiangyang, Xiamen, and Chengdu. Each participant was given a face-to-face questionnaire by the trained researcher in a private, quiet room. All procedures adhered to the principles outlined in the Declaration of Helsinki. The study was approved by the Ethics Committee of Wuhan University (ethics number: WHU-LFMD-IRB2023046), and Wuhan University of Science and Technology (ethics number: 201925). All participants submitted an informed consent form.
Participants with missing baseline dietary information (n = 4) or who without complete the 9-item Patient Health Questionnaire (PHQ-9) (n = 16), or who had extreme energy consumption (<600 or >3500 kcal/d for women, <800 or >4200 kcal/d for men, n = 428) were excluded, and finally included 3153 individuals.
Assessment of depressive symptoms
DepS were evaluated by the most widely used (in the global context)31 PHQ-9 depression scale of validated PRIME-MD diagnostic instrument, which has shown both sensitivity and specificity of 88% for depression32. The PHQ-9 evaluates each of the 9 DSM-IV criteria on a scale of 0 (not at all) to 3 (nearly every day) and finally adds them up to give a total score ranging from 0 to 27. The higher PHQ-9 score indicates greater symptoms of depression, with five categories none (0–4), mild (5–9), moderate (10–14), moderately severe (15–19), and severe depression (20–27)32.
Plant-based diet indices
Dietary intake was assessed using a semi-quantitative food frequency questionnaire (SFFQ)33. Participants were asked how often they consumed an average of 64 food items in the past year, with eight response categories including “rarely or never”, “1 time/month”, “2–3 times/month”, “1–2 times/week”, “3–4 times/week”, “5–6 times/week”, “1 time/day”, “2 times/day”, and “≥3 times/day”.
We classified all foods mentioned in SFFQ into 17 food groups34,35, and three categories of food groups, including healthy plant foods (i.e., whole grains, fruits, vegetables, nuts, legumes, vegetable oil, tea), unhealthy plant foods (i.e., fruit juices, refined grains, sugar-sweetened beverage, sweets and desserts, and salt-preserved vegetable), and animal foods (i.e., animal fat, milk or dairy products, eggs, fish or seafood, and meat).
Binary scoring of the three food groups of vegetable oils, refined grains, and animal fats, with positive (“no” 1 point, “yes” 5 points) or negative (“no” 5 points, “yes” 1 point). The other fifteen food groups were ranked into quintiles and given either a positive or negative score. Positive scores were given as 5 points to participants in the highest quintile and 1 point to those in the lowest quintile; reverse scores were given as 1 point to participants in the highest quintile and 5 points to those in the lowest quintile.
Three plant-based diet indices (PDIs) were subsequently generated, the overall plant-based diet index (PDI), which emphasizes the consumption of more plant-based foods; the healthful plant-based diet index (hPDI), which is full of healthy plant-based foods; and conversely, the unhealthful plant-based diet index (uPDI), which is enriched with unhealthy plant foods36. In brief, all animal food groups were assigned a negative score. The overall PDI scored positively in all plant foods (healthy and less healthy). The hPDI scored positively in only healthy plant foods and negatively in less healthy plant foods. In contrast, the uPDI scored positively in less healthy plant foods and negatively in healthy plant foods. Minimum 1 point, maximum 5 points, and 17 food groups total theoretical score range 17–85. The higher the PDIs score of a participant, the greater his adherence to the various versions of plant-based diets. The components and score of plant-based diet indices are reported in the Supplementary Material (Supplementary Table 1).
Potential covariates
We collected demographic information, including age (years), sex (men/women), education (primary/secondary/university), household income (<20,000/ 20,000–39,999/≥40,000 CNY/year), marital status (married/ single, divorced, or widowed), alcohol drinking (current/ past or never), smoking status (current/ past or never), CVD (presence/absence), diabetes (presence/absence), hypertension (presence/ absence) through self-report on the structured questionnaires. Body mass index (BMI, in kg/m2) was assessed by dividing the weight in kilograms by the square of the height in meters and was included in the analysis as a continuous variable.
Total energy intake (kcal/d) was measured using the SFFQ and calculated according to the Chinese Food Composition Table (6th edition). Physical activity was calculated from the Physical Activity Scale for the Elderly (PASE)37. We divided all participants into two categories according to the World Health Organization’s recommendations for adult physical activity25: participants who met the guideline were considered physically active, and those who did not meet the guideline defined as physically inactive.
Statistical methods
All data were analyzed using R software version 4.1.3 and SAS software version 9.4, and a two-sided P < 0.05 was considered statistically significant.
We compared the characteristics of the study population at baseline by quartiles of the PDI. Continuous variables were analyzed by analysis of variance (ANOVA), presented as means and standard deviations (SD), and categorical variables were expressed as numbers and percentages by the Chi-square test. Logistic regression analysis was conducted to determine the association between three versions of plant-based diets and DepS, and odds ratios (ORs) and 95% confidence intervals (CIs) were estimated. P trend was tested using the median values of the quartiles for each PDIs. Linear regression analysis was used to explore the associations between PDIs (per 10-score increment) and PHQ-9. We successively adjusted for covariates regarding sociodemographic, lifestyle, and multimorbidity factors. Model 1 was adjusted for age and sex. Model 2 was further adjusted for education level, household income, marital status, physical activity, smoking status, alcohol drinking, and total energy intake. Model 3 was additionally adjusted for BMI and chronic diseases (CVD, diabetes, and hypertension). Restricted cubic splines (RCS) with four knots were used to examine the shape of the non-linear relationships. We further explored the associations of individual food groups in the plant-based diets with DepS by conducting logistic regression analyses for each of the individual food groups.
Data availability
The datasets used to support the findings of this study are available from the corresponding author upon reasonable request.
Code availability
The code generated during the current study are available from the corresponding author on reasonable request.
References
Amiri, S. & Behnezhad, S. Depression symptoms and risk of sick leave: a systematic review and meta-analysis. Int. Arch. Occup. Environ. Health 94, 1495–1512 (2021).
Damm, J. et al. Core symptoms of depression. effectiveness of antidepressant therapy. Nervenarzt 80, 515–516, (2009).
Yan, H. et al. Mediating effect of cognitive function on the relationship between chronic diseases and depression in middle-aged and elderly people in China. Mod. Prevent. Med. 49, 1345 (2022). (in Chinese).
Kaup, A. R. et al. Trajectories of depressive symptoms in older adults and risk of dementia. JAMA Psychiatry 73, 525–531 (2016).
Gustad, L. T., Laugsand, L. E., Janszky, I., Dalen, H. & Bjerkeset, O. Symptoms of anxiety and depression and risk of acute myocardial infarction: the HUNT 2 study. Eur. Heart J. 35, 1394–1403 (2014).
Cui, R. & Fiske, A. Relation between depression symptoms and suicide risk in adults and older adults: a brief report. J. Appl. Gerontol. 41, 176–180 (2022).
Xie, Y. et al. Factors associated with depressive symptoms among the elderly in China: structural equation model. Int. Psychogeriatr. 33, 157–167 (2021).
Rienks, J., Dobson, A. J. & Mishra, G. D. Mediterranean dietary pattern and prevalence and incidence of depressive symptoms in mid-aged women: results from a large community-based prospective study. Eur. J. Clin. Nutr. 67, 75–82 (2013).
Zhang, M. et al. The association between dietary patterns and depressive symptoms in Chinese adults. Biomed. Res. Int. 2020, 8380151 (2020).
Shakya, P. R. et al. Dietary inflammatory index (DII®) and the risk of depression symptoms in adults. Clin. Nutr. 40, 3631–3642 (2021).
Chen, H. et al. Plant-based dietary patterns in relation to mortality among older adults in China. Nat. Aging 2, 224–230 (2022).
Kim, J., Kim, H. & Giovannucci, E. L. Quality of plant-based diets and risk of hypertension: a Korean genome and examination study. Eur. J. Nutr. 60, 3841–3851 (2021).
McMacken, M. & Shah, S. A plant-based diet for the prevention and treatment of type 2 diabetes. J. Geriatr. Cardiol. 14, 342–354 (2017).
Li, H. et al. A prospective study of healthful and unhealthful plant-based diet and risk of overall and cause-specific mortality. Eur. J. Nutr. 61, 387–398 (2022).
Hemler, E. C. & Hu, F. B. Plant-based diets for cardiovascular disease prevention: all plant foods are not created equal. Curr. Atheroscler. Rep. 21, 18 (2019).
Zamani, B. et al. Association of plant-based dietary patterns with psychological profile and obesity in Iranian women. Clin. Nutr. 39, 1799–1808 (2020).
Mousavi, S. M. et al. The association of plant-based dietary patterns and psychological disorders among Iranian adults. J. Affect. Disord. 300, 314–321 (2022).
Daneshzad, E. et al. Association of dietary acid load and plant-based diet index with sleep, stress, anxiety and depression in diabetic women. Br. J. Nutr. 123, 901–912 (2020).
Yuan, M., Seale, J. L. Jr, Wahl, T. & Bai, J. The changing dietary patterns and health issues in China. China Agric. Econ. Rev. 11, 143–159 (2018).
Szeto, Y. T., Kwok, T. C. & Benzie, I. F. Effects of a long-term vegetarian diet on biomarkers of antioxidant status and cardiovascular disease risk. Nutrition 20, 863–866 (2004).
Li, Y. et al. Dietary patterns and depression risk: a meta-analysis. Psychiatry Res. 253, 373–382 (2017).
Beydoun, M. A., Shroff, M. R., Beydoun, H. A. & Zonderman, A. B. Serum folate, vitamin B-12, and homocysteine and their association with depressive symptoms among U.S. adults. Psychosom. Med. 72, 862–873 (2010).
Li, J. et al. Dietary inflammatory potential and risk of cardiovascular disease among men and women in the U.S. J. Am. Coll. Cardiol. 76, 2181–2193 (2020).
Kiecolt-Glaser, J. K. Stress, food, and inflammation: psychoneuroimmunology and nutrition at the cutting edge. Psychosom. Med. 72, 365–369 (2010).
WHO. WHO Guidelines on Physical Activity and Sedentary Behaviour (World Health Organization, 2020).
Gomez-Pinilla, F. & Nguyen, T. T. Natural mood foods: the actions of polyphenols against psychiatric and cognitive disorders. Nutr. Neurosci. 15, 127–133 (2012).
Bayes, J., Schloss, J. & Sibbritt, D. Effects of polyphenols in a Mediterranean diet on symptoms of depression: a systematic literature review. Adv. Nutr. 11, 602–615 (2020).
Pathak, L., Agrawal, Y. & Dhir, A. Natural polyphenols in the management of major depression. Expert Opin. Invest. Drugs 22, 863–880 (2013).
WHO (ed.) Depression and Other Common Mental Disorders: Global Health Estimates (World Health Organization, 2017).
Tang, T., Jiang, J. & Tang, X. Prevalence of depressive symptoms among older adults in mainland China: a systematic review and meta-analysis. J. Affect. Disord. 293, 379–390 (2021).
Herrman, H. et al. Time for united action on depression: a Lancet-World Psychiatric Association Commission. Lancet 399, 957–1022 (2022).
Kroenke, K., Spitzer, R. L. & Williams, J. B. The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613 (2001).
Li, Y. et al. Validity of food frequency questionnaire to investigate the dietary energy and nutrients intake. Acta Nutr. Sin. 28, 143–147 (2006).
Satija, A. et al. Healthful and unhealthful plant-based diets and the risk of coronary heart disease in U.S. adults. J. Am. Coll. Cardiol. 70, 411–422 (2017).
Zhu, A. et al. Interaction between plant-based dietary pattern and air pollution on cognitive function: a prospective cohort analysis of Chinese older adults. Lancet Region. Health West. Pac. 20, 100372 (2022).
Satija, A. et al. Plant-based dietary patterns and incidence of type 2 diabetes in US men and women: results from three prospective cohort studies. PLoS Med. 13, e1002039 (2016).
Washburn, R. A., Smith, K. W., Jette, A. M. & Janney, C. A. The physical activity scale for the elderly (PASE): development and evaluation. J. Clin. Epidemiol. 46, 153–162 (1993).
Acknowledgements
The research was funded by the Square Dance Cohort Fund of CNS Academy of Nutrition and Health (Beijing Zhongyinghui Nutrition and Health Research Institute), the Scientific Research Start-up Fund of Wuhan University and Hubei Provincial Administration of Traditional Chinese Medicine Research Project (ZY2023M007).
Author information
Authors and Affiliations
Contributions
S.R.: study conception and design; S.C., L.Z., and L.X.: data collection and data management; L.Z. and L.X.: data curation; S.C., S.T., C.H., and L.T.: data analysis of all sub-studies; J.Z., L.C., and W.Z.: data visualization; S.T., C.L., and S.C.: first manuscript draft; S.W. and Y.C.: revisions. All authors contributed to and accepted the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhang, L., Chen, S., Xu, L. et al. Association between plant-based diets and depressive symptoms among Chinese middle-aged and older adults. npj Sci Food 9, 42 (2025). https://doi.org/10.1038/s41538-025-00399-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41538-025-00399-7
