
Abstract
We conducted a systematic review and meta-analysis to review the association of lockdowns with adverse birth and pregnancy outcomes (ABPOs) and related inequalities, in high-income countries (HICs). Databases (EMBASE, MEDLINE/PubMed and Web of Science) were searched from 1 January 2019 to 22 June 2023 for original observational studies based in HICs that compared the rates of ABPOs, before and during lockdowns. The risk of bias was assessed using the Newcastle–Ottawa tool for cohort studies. We ran random-effects meta-analyses and subgroup analyses per region, lockdown period, ethnicity group and deprivation level and adjusted for underlying temporal trends. A total of 132 studies were meta-analysed from 28 HICs. Reduced rates of preterm birth (reported by 26 studies) were associated with the first lockdown (relative risk 0.96, 95% confidence interval 0.93–0.99), 11 studies adjusted for long-term trends and the association remained (0.97, 0.95–0.99), and subgroup analysis found that this association varied by continental region. Ten studies reported positive screening rates for possible depression antenatally, and lockdown was associated with increases in positive screening rates (1.37, 1.06–1.78). No other ABPOs were associated with lockdowns. Investigation of inequalities was limited due to data availability and heterogeneity; further research is warranted on the effect of lockdowns on health inequalities. This study was funded by the National Institute of Health Research, School of Primary Care Research and registered on PROSPERO (CRD42022327448).
Similar content being viewed by others
Main
In early 2020, the global spread of severe acute respiratory syndrome coronavirus 2 (leading to coronavirus disease 2019 (COVID-19)) prompted governments around the world to announce a variety of non-pharmaceutical interventions, largely referred to as lockdowns, to reduce infection rates1,2. There is increasing evidence that lockdowns were associated with changes in adverse birth and pregnancy outcomes (ABPOs), which were not directly related with the COVID-19 infection and are usually considered an indirect effect of lockdowns3,4,5,6. Initial studies reported heterogeneous associations with ABPOs and lockdowns that varied according to country income level; these included decreases in preterm birth (PTB) in high-income countries (HICs) and increases in stillbirth in low-to-middle income countries (LMICs)3,4,5,6,7.
The associations between ABPOs and lockdowns in HICs needs to be examined separately from LMICs, as each setting differed in lockdown measures, healthcare systems, COVID-19 infection and testing rates. Even within HICs, there was considerable variability in the implementation of lockdown measures across countries, which could have led to different associations with ABPOs1,8. Furthermore, the nature of these lockdown measures evolved over time, with distinct phases of the pandemic marked by the first and second lockdowns8. Therefore, associations with ABPOs were not consistent during and between lockdowns7,9,10. To gain a better picture of how lockdowns were associated with ABPOs, analysis by region and defined period of lockdown is necessary.
ABPOs are unequally distributed between ethnic groups and deprivation levels within HICs, heavily burdening minorities and those living in high deprivation11,12,13. Lockdowns probably exacerbated such inequalities; however, the evidence from HICs is conflicting8,14. In the UK, national data suggest that lockdowns are associated with worsened inequalities in ABPOs between ethnicity groups, but inequalities in PTB rates between deprivation quintiles may have been unaffected or even associated with reductions4,5. The associations between lockdowns and inequalities in ABPOs within HICs are unclear, and research is required to develop guidance and policies that would enable health equity in the future8,14.
Lockdowns are associated differently with ABPOs in HICs compared with LMICs. While inequalities in ABPOs are present in both LMICs and HICs, within HICs, there is accumulating evidence that associations with lockdowns were inconsistent between regions, time periods, ethnicity groups and deprivation levels. The aim of this systematic review and meta-analysis is to assess the evidence on the associations between COVID-19 lockdowns and ABPOs in HICs and whether any associations differed by ethnicity or deprivation, timing of lockdown or continental region.
Results
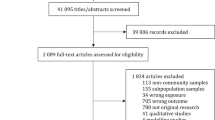
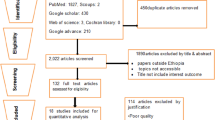
The database search yielded 14,215 results. After deduplication, 9,870 titles and abstracts were screened. A total of 416 met the criteria for full text screening, among which 207 were identified as eligible studies. After accounting for studies that had a cohort overlap (different studies that overlap in population, outcome and time periods) (31 studies), and studies with missing, unreported, illegible or wrongly formatted data (44 studies), 132 studies were included in the meta-analysis (Supplementary Material 4)5,7,9,10,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141,142,143. Eleven were included in time-adjusted analysis (Supplementary Material 5)7,10,28,29,52,67,117,144,145,146,147. The study selection process is summarized in a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart (Supplementary Material 6). Most papers included in this review had low risk of bias, although two studies exploring maternal mental health scored poorly on the bias assessment (Supplementary Materials 4 and 5). Twenty-eight countries were included; the countries with the most studies were the USA (46 studies), Italy (13 studies) and Canada (11 studies). Europe and North America were overrepresented in the dataset (59 studies (45%) and 54 studies (41%), respectively). There were fewer studies from Asia (10 studies, 7.6%), the Middle East (11 studies, 8.3%), Oceania (5 studies, 3.8%) and South America (1 study, 0.8%). Most studies were cohort studies (114 studies, 86%), followed by cross-sectional studies (15 studies, 11%), two prevalence proportion studies and a single case–control study. Half of the studies were based on data from single sites, such as individual hospitals or clinics (66 studies, 50%). Thirty-eight studies used regional- or state-level data (29%), and 28 used national datasets (21%).
PTB was reported in 26 studies with a total of 3,330,921 livebirths during lockdown and 31,969,791 livebirths in the pre-lockdown cohort. Overall, there was a 4% decrease in the risk of PTB associated with lockdown, compared with pre-lockdown (relative risk (RR) 0.96, 95% confidence interval (CI) 0.93–0.99) (relative risk is a ratio which compares the risk of an event (in this case an ABPO) in two groups (in this case a group exposed to lockdown restrictions and a group unexposed to lockdown restrictions); 95% confidence interval is the range of values that is likely to contain the true population value) (Supplementary Fig. 1a). There was high heterogeneity between studies (I2 = 96.1%, P < 0.001), so regional subgroup differences were explored. Subgroup analysis found that the associations between PTB and lockdown differed according to continental region (Supplementary Fig. 1b, P < 0.001). Lockdown was associated with decreases in PTB in Europe (RR 0.94, 95% CI 0.92–0.96) and Australia (RR 0.94, 95% CI 0.90–0.99), but there was no credible evidence of an association between PTB and lockdown in North America (RR 1.01, 95% CI 1.00–1.01), the Middle East (RR 0.91, 95% CI 0.81–1.03), Asia (RR 1.02, 95% CI 0.89–1.18) or South America (RR 1.01, 95% CI 0.96–1.06) (Supplementary Fig. 1b). Fourteen studies on PTB reported data stratified according to ethnicity and deprivation. The test for subgroup differences suggests that there is no evidence of a subgroup effect by ethnicity (P = 0.268) or deprivation (P = 0.503) on PTB (Supplementary Fig. 1c,d). Nine studies included time-adjusted estimates of PTB in the first lockdown. Calvert and colleagues reported time-adjusted estimates for multiple populations; each estimate was included with the population in brackets. When underlying temporal trends of PTB were adjusted for, there was still a decrease of 3% associated with the lockdown period (RR 0.97, 95% CI 0.95–0.99) (Supplementary Fig. 1e).
Supplementary Material 7 includes subgroup analyses on PTB and shows that there was insufficient evidence to support an association between the risk of PTB and the second lockdown (RR 0.95, 95% CI 0.90–1.00) or post-lockdown (RR 0.98, 95% CI 0.93–1.04) compared with pre-lockdown. Supplementary analysis also found that spontaneous PTB was associated with a decrease during lockdown (RR 0.95, 95% CI 0.90–0.99), whereas evidence was insufficient to support an association between the risk of iatrogenic PTB and lockdowns (RR 0.95, 95% CI 0.88–1.03) (Supplementary Material 7).
Twenty-six studies, including 2,424,824 births in lockdown and 9,101,854 births pre-lockdown, reported stillbirth. Meta-analysis found no credible evidence of an association between stillbirth and lockdown (RR 1.04, 95% CI 1.00–1.08) (Supplementary Fig. 2a). Five studies reported time-adjusted estimates of stillbirth during lockdown. No credible evidence supported an association between stillbirths and the lockdown period when underlying temporal trends were considered (RR 1.02, 95% CI 0.98–1.06) (Supplementary Fig. 2b).
Low birth weight (LBW), reported by 18 studies, had insufficient evidence to support an association with lockdown (RR 0.97, 95% CI 0.93–1.01) (Supplementary Fig. 3a). Due to high heterogeneity (I2 = 81.9%, P < 0.001), regional subgroups were analysed, but the test for subgroup differences suggested that there was no evidence to support that the association differed by region (P = 0.292) (Supplementary Material 7). Neonatal mortality, reported by nine studies, was associated with an 18% decrease during lockdown (RR 0.82, 95% CI 0.74–0.91) (Supplementary Fig. 3b). Neonatal admissions, reported by 23 studies, had no credible evidence to support an association with lockdown (RR 1.03, 95% CI 0.98–1.08) (Supplementary Fig. 3c); however, due to considerable heterogeneity (I2 = 88.2%, P < 0.001) regional subgroup analysis was run. The test for subgroup differences supported that the association differed by region (P = 0.018), in which a decrease in neonatal admissions was associated with lockdown in the Middle East (RR 0.84, 95% CI 0.72–0.97), an increase in neonatal admissions was associated with lockdown in Asia (RR 1.38, 95% CI 1.05–1.83), and no credible evidence supported associations between lockdown and neonatal admissions in North America (RR 1.03, 95% CI 0.97–1.10), Europe (RR 1.03, 95% CI 0.96–1.10) or Australia (RR 1.00, 95% CI 0.90–1.10) (Supplementary Material 7). Hypoxic ischaemic encephalopathy was reported in only one study that found insufficient evidence to support an association with lockdown94. Prolonged neonatal stay in hospital was reported by two studies; both studies reported lower rates of prolonged neonatal stay in the lockdown110,116.
Caesarean section was reported by 25 studies and did not have sufficient evidence to indicate that it was associated with lockdown (RR 1.01, 95% CI 1.00–1.03) (Supplementary Fig. 4a). Due to high heterogeneity between studies in the overall caesarean section meta-analysis (I2 = 82.8%, P < 0.001), subgroup analysis by region was run. The test for subgroup differences suggested no evidence of a subgroup effect by region (P = 0.189) (Supplementary Material 7). Evidence was also insufficient to support an association between lockdown and subclassifications of caesarean section (emergency (RR 0.99, 95% CI 0.97–1.02) or planned (RR 1.03, 95% CI 0.99–1.07)). Obstetric anal sphincter injuries (OASI) were reported by five studies, and peripartum hysterectomy was reported by four, neither of which had sufficient evidence to support an association with lockdown (RR 1.02, 95% CI 0.93–1.11 and RR 0.89, 95% CI 0.60–1.31, respectively) (Supplementary Fig. 4b,c).
Sepsis was reported by two studies, neither of which reported a change in risk or sufficient evidence to support an association with lockdown127,135. Prolonged maternal hospital stay was reported by three studies, but it was not meta-analysed as it was below the study limit for meta-analysis and outcome definitions varied considerably between studies; all studies reported decreased risk of prolonged maternal stay associated with lockdown5,43,110.
Maternal readmission was reported by nine studies and had no credible evidence to support an association with lockdown (RR 0.98, 95% CI 0.79–1.21) (Supplementary Fig. 4d). Due to considerable heterogeneity (I2 = 97%, P < 0.001), regional subgroup analysis found associations between maternal readmission and lockdown differed by continental region (P < 0.001). There was a decrease in maternal readmission in Europe only, specifically the UK, associated with lockdown compared with pre-lockdown (RR 0.69, 95% CI 0.66–0.71). No credible evidence supported an association with lockdown in North America (RR 1.02, 95% CI 0.99–1.05) or the Middle East (RR 1.40, 95% CI 0.67–2.90) (Supplementary Material 7). Meta-analysis of ten studies explored positive screening for depression antenatally with questionnaires. The risk of screening positive (clinically relevant scores) for depression antenatally was associated with a 37% increase during lockdown compared with the pre-pandemic period (RR 1.37, 95% CI 1.06–1.78) (Supplementary Fig. 4e). However, evidence was insufficient to support an association between lockdown and screening positively for depression postpartum (RR 1.01, 95% CI 0.90–1.14) (Supplementary Fig. 4f). There was no evidence to support an association between the risk of screening positive for maternal anxiety antenatally and lockdown (RR 1.08, 95% CI 0.81–1.44) (Supplementary Fig. 4g). Heterogeneity was considerable for both positive screening for depression and anxiety antenatally (I2 = 75.9%, P < 0.001, and 89.4%, P < 0.001, respectively), so subgroup analysis by continent was run for each. There was insufficient evidence to support that associations differed by continental region for either outcome (anxiety antenatally P = 0.797 and depression antenatally P = 0.662) (Supplementary Material 7). Three studies reported on positive screening for anxiety postpartum, below the limit for meta-analysis, but all studies reported insufficient evidence to support an association with lockdown46,78,140.
Sensitivity analyses
When only the four studies that stratified data according to area deprivation composite indices were included in the analysis of PTB and lockdown according to deprivation level, the test for subgroup differences according to deprivation level again found no evidence of an effect by deprivation on the association between PTB and lockdowns (P = 0.201) (Supplementary Fig. 5).
The possibility of publication bias was explored in outcomes that had over ten studies meta-analysed, including PTB, stillbirth, LBW, neonatal admissions, caesarean section and screening for depression postpartum. There was no evidence of publication bias or small study effects for any pooled estimates (Supplementary Fig. 6a–f).
The statistical power of samples to detect the pooled estimate obtained from meta-analysis and the minimum detectable effect of each meta-analysis was investigated in all outcomes and subgroups that had insufficient evidence to support an association with lockdown.
The following outcomes and subgroups were sufficiently powered (>80%) to investigate the pooled effect estimate obtained by meta-analyses. Each outcome or subgroup is reported with the estimated power of the sample to investigate the pooled estimate and minimum detectable risk ratio, both in parentheses.
-
PTB subgroup analyses by region:
-
North America (power to investigate subgroup pooled estimate: 98%, minimum detectable risk ratio of subgroup: 1.0069),
-
Middle East (94%, 0.9276).
-
-
PTB subgroup analyses by deprivation:
-
Medium deprivation (83%, 0.9518)
-
High deprivation (81%, 0.9801).
-
-
Stillbirth (97%, 1.0287)
-
LBW (100%, 0.9926)
-
Neonatal admissions (100%, 1.0148)
-
Caesarean section (100%, 1.0033)
The following outcomes and subgroups were not sufficiently powered (<80%) to investigate the pooled effect estimate obtained by meta-analyses.
-
PTB subgroup analyses by region:
-
Asia (60%, 1.0254)
-
South America (7%, 1.0671)
-
-
PTB subgroup analyses by ethnicity:
-
Black (10%, 0.9588)
-
Other (52%, 0.9176)
-
Hispanic (12%, 0.9628)
-
Asian (76%, 0.9581)
-
-
OASI (7.65%, 1.1235)
-
Peripartum hysterectomy (17%, 0.7171)
-
Maternal readmission (54%, 0.9728)
-
Positive screening for depression postpartum (11%, 1.0394)
-
Positive screening for anxiety antenatally (55%, 1.1079)
Discussion
Our review provides an assessment of the association of lockdowns with ABPOs and inequalities in HICs. We provided evidence that PTB was associated with decreases during the first lockdown (by 4%) even after accounting for temporal trends (by 3%), which is consistent with other reviews. However, we provide evidence that the associated decrease was evident only in Europe and Australia3,6,7. Supplementary analyses showed that lockdowns were associated with decreases in spontaneous PTB and PTB, which occurred at moderate-to-late gestational age (Supplementary Material 7).
It is widely accepted that ABPOs, particularly PTB, are influenced by socio-environmental or modifiable lifestyle risk factors, including social support, work conditions and access to care13,148,149,150,151,152,153,154,155. Many such determinants were dramatically affected during lockdowns and may contribute to the association between lockdowns and decreases in PTB. Before the pandemic, these socio-environmental determinants of health were unequally distributed between ethnic groups and deprivation levels, resulting in substantial inequalities in ABPOs11,156. Lockdowns could have had a synergistic effect and compounded such inequalities14; ethnic minorities and those in the most deprived areas were hit harder by restrictions, suffered increased barriers to care, had higher morbidity and mortality rates from COVID-19 and had higher rates of job loss and financial insecurity157,158,159,160,161,162,163,164, whereas individuals with higher financial and social security probably benefitted from the flexibility of remote work conditions8. However, this review had insufficient evidence to support that the association between lockdown and decreased PTB varied according to ethnicity group or deprivation level.
The investigation of inequalities in ABPOs between ethnicity and deprivation groups was limited due to data availability and heterogeneity between studies and settings. Very few studies reported data stratified according to ethnicity and deprivation, and fewer used the same ethnicity groups or deprivation levels. This is understandable as ethnicity distribution varies between settings, and deprivation indicators such as maternal education and neighbourhood income are contextually specific. We addressed this limitation pragmatically by synthesizing available data on deprivation or by using proxy variables for deprivation, and harmonizing composite and proxy variables to obtain aggregated estimates of deprivation. Data synthesis meant that all subgroups in the analyses of deprivation had sufficient power to detect the pooled estimate obtained in meta-analyses. In the subgroup meta-analyses of PTB by ethnicity, only the white ethnicity group had sufficient power to detect the pooled estimate. All non-white ethnicity groups were insufficiently powered, and further research is required on larger, more consistent data to estimate these subgroups’ association with lockdown.
In terms of deprivation, area-level estimates of deprivation have an inherent limitation of misclassification of individuals, for instance, those who live in areas of high deprivation but are not themselves deprived; this non-differential misclassification blunts the gradient of observed differences in deprivation. When these estimates are combined, this is compounded, underestimating the association which biases towards the null. Our results indicate that lockdown’s association with PTB did not vary according to socio-economic deprivation and ethnicity; however, the magnitude of the association may be underestimated and analysis using individual deprivation indices is warranted.
Access to high-quality maternity care is a key determinant of maternal and neonatal health, which was considerably altered by lockdown restrictions149,165. Authors hypothesize about the causal mechanisms in the relationship between lockdowns and ABPOs, such as the influence of lockdowns on the delivery of and access to maternity services. However, due to data limitations and lack of sufficient evidence, the association between lockdowns and the supply and demand of maternity care could not be explored in greater detail in this review.
Nevertheless, the surrounding literature indicates that in HICs maternity services largely remained open throughout lockdowns, but services were altered to protect patients and practitioners from infection risks; care alterations in HICs included remote consultations via telephone and home blood pressure monitoring158,165. During the pandemic, there were decreases in antenatal visits and screening uptake, indicating that the lockdowns substantially influenced care-seeking behaviour among pregnant women165. It appears that the influence of these service adaptations varied according to an individual’s income level and resource165. The multifaceted influences of the pandemic and lockdowns on maternity service provision and care-seeking behaviour requires further investigation to ascertain how these care-related factors may have affected ABPOs.
We identified a decrease of 18% in neonatal mortality associated with the lockdown3,6. However, the neonatal mortality estimate was dominated mainly by a study by Shukla and colleagues, weighted 60%; in their study, when previous long-term trends in neonatal mortality were accounted for, they found no substantial change during lockdown121. Therefore, the estimated 18% decrease in the risk of neonatal mortality should be interpreted with caution and emphasizes the need for further investigation using time-adjusted analysis to precisely assess the association with lockdown measures3,6.
Our review aggregates data on positive screening scores for maternal mental health outcomes during lockdown. While previous reviews have reported increased perinatal depression associated with the pandemic, our pooled estimates found evidence to support this association antenatally, but no credible evidence of an association between positive screening rates of postpartum depression and lockdowns166,167,168. Other studies have suggested that limited access to care, multidisciplinary support and treatment in lockdowns aggravated depression among both pregnant and postpartum women166,167. It is important to note there was variation in measurement modalities and timing of screening, and most studies used screening questionnaires without final diagnostic outcomes, which all may have introduced bias into results, thereby underestimating the association with lockdown and warranting further research.
The present review has various strengths, including a comprehensive search with optimal subgroup and time-adjusted analysis that accounted for temporal trends in outcomes and explored inequalities between and within HICs. Publication bias was not present in any analyses. However, interpretation of our findings also requires consideration of limitations. For some outcomes, heterogeneity was concerning, a common challenge with aggregated data. To overcome this, we ran subgroup and stratified analysis where we had sufficient data. Discrimination, inequalities, health systems, lockdown restrictions and definitions vary between regions and countries and could contribute to high heterogeneity and limit comparability of data between studies1. However, we attempted to account for this variability by focusing on HICs, using random-effect estimates, and subgroup analysis by region and time period8.
Methods
We conducted a systematic review and meta-analysis of studies that explored the association between COVID-19 lockdowns and ABPOs in HICs. The review was registered on PROSPERO (CRD42022327448), where amendments and progress have been updated accordingly, and followed the relevant PRISMA guidance.
Eligibility criteria
The intervention of interest was COVID-19 lockdowns, defined as those non-pharmaceutical, home-confinement and non-essential service closure interventions imposed by governments in 2020 with the aim of reducing the spread of COVID-19.
To be included in the review, studies had to report on at least one of the following ABPOs or outcome subclassifications (definitions in Supplementary Material 1).
ABPOs
Perinatal/neonatal outcomes:
-
PTB
-
Stillbirth
-
LBW
-
Neonatal mortality
-
Neonatal (neonatal intensive care unit) admissions
-
Hypoxic ischaemic encephalopathy
-
Prolonged stay in hospital
Maternal outcomes:
-
Caesarean section
-
OASI
-
Peripartum hysterectomy
-
Sepsis (in puerperium)
-
Prolonged stay in hospital
-
Readmission to hospital
-
Maternal mental health (depression or anxiety antenatally or postpartum)
The outcomes of this review were decided upon on the basis of current literature, expert advice, importance to patients and pragmatic considerations. Patients’ perspectives and priorities were obtained from a women’s reference group; the group was formed to consult on the COVID Maternity Equality Project study169, where S.I. was the principal investigator. Their insights and priorities informed which outcomes were included and explored in this review and research. Pragmatic considerations included data access and availability.
The population was restricted to those residing in HICs, as defined by the World Bank Classifications170. To be included, studies had to present a comparator cohort from before lockdowns or the pandemic in 2020. We included the following study types: observational studies, case–control studies, cohort studies and brief reports comparing outcomes before and during lockdowns. Studies had to be published between 1 January 2019 and 22 June 2023. Language requirements entailed that title and abstracts had to be written in English.
We excluded non-HIC populations or countries that did not enforce lockdowns, such as Sweden. We excluded studies that explored only COVID-19 infection in pregnancy and neonates. We also excluded qualitative studies, systematic reviews, narrative reviews, discussion articles, viewpoints/opinion articles and editorials.
Search strategy and selection
Search terms were developed to include all key perinatal, neonatal and maternal health outcomes and word variants of COVID-19 lockdowns (Supplementary Material 2). We searched EMBASE, MEDLINE/PubMed and Web of Science. We also searched for preprints (MedRxiv) and unpublished reports; these were identified by co-authors through research networks. References of eligible studies were reviewed to identify additional eligible studies. Search results were exported to Endnote, where duplicates were removed, both automatically and manually. The results were then independently reviewed by two reviewers (H.N.S. and I.H.), who applied the eligibility criteria first to titles, then to abstracts and full texts. Reviewers then compared selections, and any disagreements were resolved by discussion between reviewers and a third author arbitrated (S.I.).
Data extraction
Key characteristics of studies and data on outcomes and total births were extracted using a data extraction tool developed in Microsoft Excel version 16.85. Aggregated data stratified according to deprivation and ethnicity were also extracted. Multiple indicators of deprivation were used (Supplementary Material 3). Deprivation was an indicator variable, where data on maternal education, mean neighbourhood income and deprivation indices were pragmatically combined and harmonized to indicate high, medium or low deprivation (details available in Supplementary Material 3). Where data were missing, illegible or presented in the wrong format, we emailed authors to ask them to provide relevant aggregated data. If the authors did not respond, then the raw values were calculated on the basis of available information; however, in cases where information was insufficient for calculations, the study was excluded from meta-analysis. Risk of bias in each study was assessed and scored using the Newcastle–Ottawa risk of bias assessment tool for cohort studies171. After extraction, studies that had a cohort overlap were removed, where the smaller study was removed in favour of the larger study.
Statistical analysis
Meta-analysis was conducted on outcomes that had more than three studies presenting relevant data, to calculate accurate and meaningful pooled estimates. For each outcome, we determined the random-effects estimate pooled risk ratio to account for heterogeneity across studies and populations, and 95% confidence intervals were calculated, as well as an I2 value summarizing interstudy heterogeneity172. All statistical tests were two-tailed. Where heterogeneity was considerable (that is, >75%) and sufficient data were available, subgroup and stratified meta-analyses were conducted to explore potential sources of heterogeneity172.
Due to the differing measures and implementation of lockdowns between countries, a high degree of spatial heterogeneity was expected and subgroup analyses were conducted according to continent8. Studies that reported data on a second defined lockdown period and/or a post-lockdown period were also meta-analysed as subgroup analysis. The reference period for both was the pre-pandemic epoch. This analysis attempted to explore whether the associations with the second lockdown varied greatly from associations with the first lockdown. To improve insight into lockdowns’ association with distinct pathological processes, subclassifications of clinical outcomes were explored where data were available in supplementary analyses, for instance, spontaneous compared with iatrogenic (medically induced) PTB8. There are various subclassifications of outcomes included; these are listed with outcome definitions (Supplementary Material 1).
To explore inequalities within HICs, stratified meta-analysis according to deprivation and ethnicity was conducted where more than three studies presented sufficient data. Studies with stratified data were included, and subgroup pooled estimates were calculated and compared.
We also controlled for underlying temporal trends in outcomes when data were available. Failing to account for such trends can lead to spurious results8,173. Therefore, we conducted a meta-analysis of time-adjusted studies; we excluded studies without adjustment for underlying temporal trends using a quasi-experimental design173,174. The same pathway as the main analysis was followed for selection and data extraction. Two reviewers (B.G. and I.H.) independently screened studies previously identified as eligible for inclusion. Additional data were extracted from the studies, including total sample sizes, time-adjusted risk and odds ratios, and corresponding upper and lower confidence intervals. In papers where odds ratios were presented, they were converted to risk ratios using the formula described by Faber and colleagues175. Once data were extracted, an inverse-variance meta-analysis was conducted using the random-effects pooled estimate172.
Sensitivity analyses
Deprivation included several proxy variables to indicate an area’s level of deprivation. To explore the association between area deprivation and ABPOs (when available) during lockdown more closely, a sensitivity analysis was conducted in which only studies reporting data stratified by an area deprivation composite index scores were included. Data harmonization of area deprivation index scores is outlined in Supplementary Material 3.
Funnel plots were constructed, and Egger’s tests were run on outcomes that had data aggregated from more than ten studies to explore asymmetry and publication bias. For the Egger’s test, a significance threshold of P < 0.1 was adopted. All analyses were conducted in Stata 17.0.
Among outcomes that had insufficient evidence to support an association with lockdown, we investigated the statistical power of samples to detect the pooled estimate and the minimum detectable effect.
Role of funding source
The funder of the study is the National Institute of Health Research: School of Primary Care Research. The funder had no role in the study design, data collection and analysis, or presentation of the report.
Conclusion
In conclusion, our systematic review and meta-analyses showed that, in HICs, a decrease in the likelihood of PTB was associated with lockdowns; however, this reduction was unequal among HICs and was apparent only in Europe and Australia. COVID-19 lockdowns were a natural experiment that imposed system and wider socio-environmental interventions. The uneven associations between ABPOs and lockdowns need to be explored further through mixed-methods investigation to assess the health determinants, societal structures and barriers to care that drive ABPOs8,14. Our findings provide evidence that an umbrella lockdown approach has unequal consequences for ABPOs; targeted policies and tailored support structures are warranted to achieve and promote maternal and neonatal health14.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
All data used in the meta-analysis were generated from deidentified, aggregated data extracted from studies included in the meta-analysis or were shared with authors upon request. This study makes use of publicly available data and data already published in primary research studies. In terms of a minimum dataset, all aggregated data used in meta-analysis are listed on corresponding forest plots. Individuals seeking access to unpublished data require relevant permissions from individual study authors.
Code availability
All code used in the meta-analysis was based on predeveloped code available in Stata 17.0 meta-analysis manuals. All code is available upon request.
References
Haider, N. et al. Lockdown measures in response to COVID-19 in nine sub-Saharan African countries. BMJ Global Health 5, e003319 (2020).
Timeline of UK Government Coronavirus Lockdowns and Restrictions (Institute for Government, 2022); https://www.instituteforgovernment.org.uk/data-visualisation/timeline-coronavirus-lockdowns
Chmielewska, B. et al. Effects of the COVID-19 pandemic on maternal and perinatal outcomes: a systematic review and meta-analysis. Lancet Global Health 9, e759–e772 (2021).
Greenbury, S. F. et al. Changes in neonatal admissions, care processes and outcomes in England and Wales during the COVID-19 pandemic: a whole population cohort study. BMJ Open 11, e054410 (2021).
Gurol-Urganci, I. et al. Obstetric interventions and pregnancy outcomes during the COVID-19 pandemic in England: a nationwide cohort study. PLoS Med 19, e1003884 (2022).
Yang, J. et al. COVID-19 pandemic and population-level pregnancy and neonatal outcomes in general population: a living systematic review and meta-analysis (update#2: November 20, 2021). Acta Obst. Gynecol. Scand. https://doi.org/10.1111/aogs.14206 (2022).
Calvert, C. et al. Changes in preterm birth and stillbirth during COVID-19 lockdowns in 26 countries. Nat. Hum. Behav. 7, 529–544 (2023).
Been, J. V., Vermeulen, M. J. & Kazemier, B. M. in COVID-19 and Perinatology (eds De Luca, D. & Benachi, A.) 207–227 (Springer, 2023).
Gemmill, A. et al. Changes in preterm birth and caesarean deliveries in the United States during the SARS-CoV-2 pandemic. Paediatr. Perinat. Epidemiol. 36, 485–489 (2021).
Stumpfe, F. M. et al. Limited effects of SARS-CoV-2 pandemic-related lockdowns and reduced population mobility on preterm birth rates: a secondary analysis of bavarian obstetric quality parameters from 2010 to 2020. Geburtshilfe Frauenheilkd. 82, 842–851 (2022).
Draper, E. S. et al. MBRACE-UK Perinatal Mortality Surveillance Report: UK Perinatal Deaths for Births from January to December 2019 (Leicester University, 2021).
Jardine, J. et al. Adverse pregnancy outcomes attributable to socioeconomic and ethnic inequalities in England: a national cohort study. Lancet 398, 1905–1912 (2021).
Howell, E. A. Reducing disparities in severe maternal morbidity and mortality. Clin. Obstet. Gynecol. 61, 387–399 (2018).
Bambra, C., Lynch, J., Smith, K. E. & Pickett, K. Collateral Damage Inequalities in the Lockdown. The Unequal Pandemic 35–54 (Bristol Univ. Press, 2021).
Aboulatta, L. et al. Preterm birth and stillbirth rates associated with socioeconomic disparities during COVID-19 pandemic: a population-based cross-sectional study. BMJ Paediatr. Open 7, e001686 (2023).
Watson, H., Adeluwoye, T. & Mehta, M. 510 A cross-sectional study of the impact of the COVID-19 pandemic on preterm birth rates on an inner-city population. BJOG 128, 187 (2021).
Afonina, M., Lagrasta, F., Simonetti, S. C. & Marconi, A. M. Impact of the lockdown period on reproductive health in a single center in Milan, Italy. J. Matern. Fetal Neonatal Med. 34, 6 (2021).
Allegri, B. et al. The impact of the second COVID-19 lockdown on anxiety and depressive symptoms in pregnant women: a case study of pregnant women in northern Italy. Brain Behav. Immun. Health 30, 100633 (2023).
Alshaikh, B., Cheung, P. Y., Soliman, N., Brundler, M. A. & Yusuf, K. Impact of lockdown measures during COVID-19 pandemic on pregnancy and preterm birth. Am. J. Perinatol. 39, 329–336 (2022).
Amadori, R. et al. What may happen if you are pregnant during COVID-19 lockdown? A retrospective study about peripartum outcomes. Minerva Obstet. Gynecol. 74, 319–324 (2021).
Ameh, S., Kither, H., Pappala, S. & Williams, A. COVID-19 pandemic: impact on obstetric services and outcomes: a retrospective study. BJOG 128, 186 (2021).
Arnaez, J. et al. Lack of changes in preterm delivery and stillbirths during COVID-19 lockdown in a European region. Eur. J. Pediatr. 180, 1997–2002 (2021).
Athar, S. et al. Continuity of maternal care during COVID-19 pandemic in Qatar: aiming to reduce neonatal morbidity. J. Emerg. Med. Trauma Acute Care 2022, 15 (2022).
Athiraman, N. K., Patience, A., Onwuneme, C., Zalewski, S. & Skeath, T. Impact of COVID-19 on maternity and neonatal services—three year-on-year review data from the North East of England. Acta Paediatr. Int. J. Paediatr. 111, 1039–1041 (2022).
Ayyash, M. et al. Black–White disparities and preterm births comparisons following the COVID-19 pandemic in Michigan. Am. J. Obstet. Gynecol. 226, S152 (2022).
Bajaj, M. et al. Population-level study on fetal deaths and preterm births during SARS-CoV-2 pandemic in the State of Michigan. Am. J. Perinatol. 41, e236–e248 (2022).
Bajaj, M. A., Salimgaraev, R., Zhaunova, L. & Payne, J. L. Rates of self-reported postpartum depressive symptoms in the United States before and after the start of the COVID-19 pandemic. J. Psychiatr. Res. 151, 108–112 (2022).
Balsa, A. I. & Triunfo, P. The COVID-19 pandemic and birth outcomes in 2020: the role of prenatal care and other channels. Econ. Hum. Biol 47, 101167 (2022).
Been, J. V. et al. Impact of COVID-19 mitigation measures on the incidence of preterm birth: a national quasi-experimental study. Lancet Public Health. 5, e604–e611 (2020).
Benyamini Raischer, H. et al. Impact of COVID-19 mandatory lockdown on maternal gestational weight gain and neonatal macrosomia rate at an academic medical center in Israel. J. Matern. Fetal Neonatal Med. 36, 2204391 (2023).
Berghella, V., Boelig, R., Roman, A., Burd, J. & Anderson, K. Decreased incidence of preterm birth during coronavirus disease 2019 pandemic. Am. J. Obstet. Gynecol 2, 100258 (2020).
Berthelot, N. et al. Uptrend in distress and psychiatric symptomatology in pregnant women during the coronavirus disease 2019 pandemic. Acta Obstet. Gynecol. Scand. 99, 848–855 (2020).
Boehler-Tatman, M., Howard, E. & Russo, M. L. Examining outcomes for nulliparous, at term, singleton and vertex deliveries during the first wave of the COVID-19 pandemic in Rhode Island. R. I. Med. J. 105, 37–41 (2022).
Boekhorst, M. G. B. M. et al. The COVID-19 outbreak increases maternal stress during pregnancy, but not the risk for postpartum depression. Arch. Womens Ment. Health 24, 1037–1043 (2021).
Cate, J. et al. Preterm birth rates and race disparities pre and post COVID vaccination. Am. J. Obstet. Gynecol. 226, S625 (2022).
Chen, J. et al. Changes and geographic variation in rates of preterm birth and stillbirth during the prepandemic period and COVID-19 pandemic, according to health insurance claims in the United States, April–June 2019 and April–June 2020. Am. J. Obstet. Gynecol 4, 100508 (2022).
Cheung, P. Y., Alshaikh, B. & Yang, C. COVID-19 pandemic: different associative relationships of city lockdown with preterm births in three cities—an ecological study. Front. Pediatr. 9, 644771 (2021).
Chrzan-Dętkoś, M., Walczak-Kozłowska, T. & Lipowska, M. The need for additional mental health support for women in the postpartum period in the times of epidemic crisis. BMC Pregnancy Childbirth 21, 114 (2021).
Clifton, V. L. et al. Associations between COVID-19 lockdown and post-lockdown on the mental health of pregnant women, postpartum women and their partners from the Queensland family cohort prospective study. BMC Pregnancy Childbirth 22, 468 (2022).
Dagelić, A., Mulic, E., Kuzmic Prusac, I. & Zekic Tomas, S. The impact of the COVID-19 pandemic on adverse fetal outcomes: a cross-sectional study. Medicine 102, e33887 (2023).
David, M. & Reutter, T. Fewer preterm births in the first COVID-19 pandemic year? An evaluation of the Berlin perinatal data for the years 2017 to 2020. Geburtshilfe Frauenheilkd. 83, 184–191 (2023).
De Chiara, L. et al. The impact of the COVID-19 pandemic on postpartum maternal mental health. J. Pers. Med. 13, 56–72 (2022).
DeBolt, C. A. et al. The Impact of the COVID-19 pandemic on postpartum readmission rates at a single tertiary care center in New York City. Am. J. Perinatol. 39, 1145–1150 (2022).
Deli, T. et al. How the cesarean delivery rate decreased at the Department of Obstetrics and Gynecology, University of Debrecen during the COVID-19 pandemic. Orv. Hetil. 162, 811–823 (2021).
Delius, M. et al. Changes in the rate of preterm infants during the COVID-19 pandemic lockdown period—data from a large tertiary German University Center. Arch. Gynecol. Obstet. 309, 1925–1933 (2023).
Dol, J. et al. Impact of COVID-19 restrictions on the postpartum experience of women living in Eastern Canada during the early pandemic period: a cross-sectional study. J. Nurs. Scholarsh. 55, 178–186 (2023).
Einarsdóttir, K., Swift, E. M. & Zoega, H. Changes in obstetric interventions and preterm birth during COVID-19: a nationwide study from Iceland. Acta Obstet. Gynecol. Scand. 100, 1924–1930 (2021).
Esposito, G. et al. Impact of the first and second lockdown for COVID-19 pandemic on preterm birth, low birth weight, stillbirth, mode of labor, and of delivery in Lombardy, Italy. J. Pers. Med. 13, 499–507 (2023).
Facco, F. & Himes, K. 993 Did health care delivery changes driven by COVID alter pregnancy and postpartum visits? Am. J. Obstet. Gynecol. 224, S615–S616 (2021).
Feldman, K. M. et al. 12 Observations from an inner city hospital during COVID-19: preterm birth rate and mode of delivery. Am. J. Obstet. Gynecol. 224, S8 (2021).
Fisher, S. A., Sakowicz, A., Barnard, C., Kidder, S. & Miller, E. S. Neighborhood deprivation and preterm delivery during the coronavirus 2019 pandemic. Am. J. Obstet. Gynecol. 4, 100493 (2022).
Fresson, J. et al. Decreases in preterm birth during the first COVID-19 lockdown in France by gestational age sub-groups and regional COVID-19 incidence. Ann. Epidemiol. 72, 74–81 (2022).
Gallo, L. A. et al. A decline in planned, but not spontaneous, preterm birth rates in a large Australian tertiary maternity centre during COVID-19 mitigation measures. Aust. N. Z. J. Obstet. Gynaecol. 62, 62–70 (2022).
Garabedian, C. et al. Impact of COVID-19 lockdown on preterm births, low birthweights and stillbirths: a retrospective cohort study. J. Clin. Med. 10, 5649–5658 (2021).
Green, D. et al. Prevalence of postpartum depression following the COVID-19 pandemic at an urban academic institution. Obstet. Gynecol. 139, 68S (2022).
Gulersen, M. et al. The risk of readmission after early postpartum discharge during the COVID-19 pandemic. Am. J. Perinatol. 39, 354–360 (2022).
Gustafsson, H. C. et al. Trajectories of perinatal depressive symptoms in the context of the COVID-19 pandemic. Child Dev 92, e749–e763 (2021).
Handley, S. C. et al. Postpartum length of stay and hospital readmission before and during the coronavirus disease 2019 (COVID-19) pandemic. Obstet. Gynecol. 139, 381–390 (2022).
Handley, S. C. et al. Changes in preterm birth phenotypes and stillbirth at 2 Philadelphia hospitals during the SARS-CoV-2 pandemic, March–June 2020. JAMA 325, 87–89 (2021).
Harvey, E. M. et al. Association of preterm birth rate with COVID-19 statewide stay-at-home orders in Tennessee. JAMA Pediatr 175, 635–637 (2021).
Herzberger, E. H., Efros, O., Herzberger, S., Biron-Shental, T. & Shechter-Maor, G. Differences in obstetric healthcare utilization and delivery complications before and after the COVID-19 pandemic—a retrospective study. J. Matern. Fetal Neonatal Med. 28, 1–6 (2021).
Hiiragi, K., Obata, S., Misumi, T., Miyagi, E. & Aoki, S. Psychological stress associated with the COVID-19 pandemic in postpartum women in Yokohama, Japan. J. Obstet. Gynaecol. Res. 47, 2126–2130 (2021).
Hirsch, A. et al. 447 Incidence and characteristics of deliveries during COVID-19 epidemic lockdown. Am. J. Obstet. Gynecol. 224, S283–S284 (2021).
Hui, L. et al. Increase in preterm stillbirths in association with reduction in iatrogenic preterm births during COVID-19 lockdown in Australia: a multi-centre cohort study. Am. J. Obstet. Gynecol. 227, 491.e1–491.e17 (2022).
Hui, P. W., Ma, G., Seto, M. T. Y. & Cheung, K. W. Effect of COVID-19 on delivery plans and postnatal depression scores of pregnant women. Hong Kong Med. J 27, 113–117 (2021).
Huseynova, R. et al. Prevalence of preterm birth rate during COVID-19 lockdown in a tertiary care hospital, Riyadh. Cureus 13, e13634 (2021).
Hwang, J. et al. Changes in preterm birth and birthweight during the SARS-CoV-2 pandemic: a nationwide study in South Korea. Sci. Rep. 12, 16288 (2022).
Hwang, S. S., Weikel, B. W., Hannan, K. E. & Bourque, S. L. Impact of coronavirus disease-19 ‘stay-at-home’ orders on preterm birth in Colorado. J. Pediatr. 242, 238–241 (2022).
Janevic, T. et al. Racial/ethnic disparities in very preterm birth and preterm birth before and during the COVID-19 pandemic. JAMA Netw. Open 4, e211816 (2021).
Jasper, B., Stillerova, T., Anstey, C. & Weaver, E. Reduction in preterm birth rates during and after the COVID-19 lockdown in Queensland Australia. Aust. N. Z. J. Obstet. Gynaecol. 62, 851–858 (2022).
Jeyamurugan, K., Jung, M. K. & Ericksen, K. Preterm birth rates in a deprived American community only differed before and during COVID-19 when maternal risks were factored in. Acta Paediatr. Int. J. Paediatr. 112, 151–153 (2023).
Jones, H. et al. Population birth outcomes and experiences of expectant mothers during the COVID-19 pandemic in Wales: a mixed methods study. Lancet 398, S57 (2021).
Justman, N. et al. Lockdown with a price: the impact of the COVID-19 pandemic on prenatal care and perinatal outcomes in a tertiary care center. Isr. Med. Assoc. J. 22, 533–537 (2020).
Khalil, A. et al. Change in the incidence of stillbirth and preterm delivery during the COVID-19 pandemic. J. Am. Med. Assoc. 324, 705–706 (2020).
Kim, S.-Y., Kim, S.-Y., Kil, K. & Lee, Y. Impact of COVID-19 mitigation policy in South Korea on the reduction of preterm or low birth weight birth rate: a single center experience. Children 8, 332–342 (2021).
Kirchengast, S. & Hartmann, B. Pregnancy outcome during the first COVID 19 lockdown in Vienna, Austria. Int. J. Environ. Res. Public Health 18, 3782 (2021).
Klumper, J. et al. Association between COVID-19 lockdown measures and the incidence of iatrogenic versus spontaneous very preterm births in the Netherlands: a retrospective study. BMC Pregnancy Childbirth 21, 767–776 (2021).
Kuipers, Y. J. et al. Psychological health of pregnant and postpartum women before and during the COVID-19 pandemic. PLoS ONE 17, e0267042 (2022).
Lantigua-Martinez, M. V. et al. Perinatal depression before and during the coronavirus pandemic. Am. J. Obstet. Gynecol. 226, S686–S687 (2022).
Lau, M. et al. Observational study on the neonatal outcome during the COVID-19 pandemic in Germany. Acta Paediatr 112, 1892–1897 (2023).
Leibovitch, L. et al. Preterm singleton birth rate during the COVID-19 lockdown: a population-based study. Am. J. Perinatol. 39, 1020–1026 (2021).
Lemon, L., Edwards, R. P. & Simhan, H. N. What is driving the decreased incidence of preterm birth during the coronavirus disease 2019 pandemic? Am. J. Obstet. Gynecol. 3, 100330 (2021).
Liu, S. et al. Pregnancy outcomes during the COVID-19 pandemic in Canada, March to August 2020. J. Obstet. Gynaecol. Can. 43, 1406–1415 (2021).
Llorca, J. et al. Results of pregnancy control before and during the COVID-19 pandemic: a comparison of two cohorts. Int. J. Environ. Res. Public Health 18, 8182–8189 (2021).
Lo, A. C. Q., Kemp, M. & Kabacs, N. Impact of the COVID-19 pandemic on perinatal mental health screening, illness and pregnancy outcomes: a cohort study. Obstet. Med. 16, 178–183 (2022).
Loehr, F. W. et al. Postpartum depression in cohorts before and after the start of the COVID-19 pandemic. Am. J. Obstet. Gynecol. 226, S666–S667 (2022).
Main, E. K. et al. Singleton preterm birth rates for racial and ethnic groups during the coronavirus disease 2019 pandemic in California. Am. J. Obstet. Gynecol. 224, 239–241 (2021).
Mak, A. H. M., Cicero, S. & Hui, P. W. Impact of COVID-19 pandemic on preterm delivery. J. Obstet. Gynaecol. Res. 49, 1539–1544 (2023).
Maki, Y. et al. No significant changes in preterm birth, low-birth-weight, and small-for-gestational-age infants during the first year of the COVID-19 pandemic in a rural area in Japan. J. Obstet. Gynaecol. Res. 49, 175–181 (2023).
Mariño-Narvaez, C., Puertas-Gonzalez, J. A., Romero-Gonzalez, B. & Peralta-Ramirez, M. I. Giving birth during the COVID-19 pandemic: the impact on birth satisfaction and postpartum depression. Int. J. Gynaecol. Obstet. 153, 83–88 (2021).
Maslin, K. et al. Preterm births in South-West England before and during the COVID-19 pandemic: an audit of retrospective data. Eur. J. Pediatr. 181, 859–863 (2022).
McDonnell, S., McNamee, E., Lindow, S. W. & O’Connell, M. P. The impact of the COVID-19 pandemic on maternity services: a review of maternal and neonatal outcomes before, during and after the pandemic. Eur. J. Obstet. Gynecol. Reprod. Biol. 255, 172–176 (2020).
McKee, K. S. et al. Perinatal outcomes during vs. prior to the COVID-19 pandemic and the role of maternal depression and perceived stress: a report from the ECHO program. Am. J. Perinatol. 41, e1404–e1420 (2023).
Meyer, R. et al. A marked decrease in preterm deliveries during the coronavirus disease 2019 pandemic. Am. J. Obstet. Gynecol. 224, 234–237 (2021).
Meyer, R., Levin, G., Hendin, N. & Katorza, E. Impact of the COVID-19 outbreak on routine obstetrical management. Isr. Med. Assoc. J. 22, 417–422 (2020).
Mikus, M., Karadjole, V. S., Kalafatic, D., Oreskovic, S. & Sarcevic, A. Increase of stillbirths and unplanned out-of-hospital births during coronavirus disease 2019 lockdown and the Zagreb earthquake. Acta Obstet. Gynecol. Scand. 100, 2119–2120 (2021).
Mølholm Hansen, B. et al. Preterm birth rates were slightly lower in Denmark during the first year of the COVID-19 pandemic compared to the previous 4 years. Acta Paediatr. 111, 1695–1700 (2022).
Molina-Merino, A., Martínez-Rodríguez, L., Cubells-García, E., Hortelano-Platero, V. & Estañ-Capell, J. Effect of lockdown on the preterm births in a Valencian Comunity. An. Pediatr. 95, 379–381 (2021).
Mor, M. et al. Impact of the COVID-19 pandemic on excess perinatal mortality and morbidity in Israel. Am. J. Perinatol. 38, 398–403 (2021).
Muin, D. A. et al. Antepartum stillbirth rates during the COVID-19 pandemic in Austria: a population-based study. Int. J. Gynaecol. Obstet. 156, 459–465 (2022).
Niehaus, S. C., Brown, T. M., Kempner, M. E., Skarha, J. E. & Ayala, N. K. Maternal and neonatal outcomes before and during the COVID-19 pandemic. R. I. Med. J. 106, 58–62 (2023).
Oakley, L. L. et al. Preterm birth after the introduction of COVID-19 mitigation measures in Norway, Sweden, and Denmark: a registry-based difference-in-differences study. Am. J. Obstet. Gynecol. 226, 550.e1–550.e22 (2022).
Okawa, S., Hosokawa, Y., Nanishi, K., Zaitsu, M. & Tabuchi, T. Threatened abortion, threatened premature labor, and preterm birth during the first state of emergency for COVID-19 in 2020 in Japan. J. Obstet. Gynaecol. Res. 48, 1116–1125 (2022).
Panzer, A., Reed-Weston, A., Friedman, A., Goffman, D. & Wen, T. Expedited postpartum discharge during the COVID-19 pandemic and acute postpartum care utilization. J. Matern. Fetal Neonatal Med. 35, 9585–9592 (2022).
Pariente, G. et al. Risk for probable post-partum depression among women during the COVID-19 pandemic. Arch. Womens Ment. Health 23, 767–773 (2020).
Pereira, D. et al. The impact of COVID-19 on anxious and depressive symptomatology in the postpartum period. Int. J. Environ. Res. Public Health 19, 7833–7846 (2022).
Philip, R. K. et al. Unprecedented reduction in births of very low birthweight (VLBW) and extremely low birthweight (ELBW) infants during the COVID-19 lockdown in Ireland: a ‘natural experiment’ allowing analysis of data from the prior two decades. BMJ Global Health 5, e003075 (2020).
Quibel, T. et al. Impact of COVID-19-related lockdown on delivery and perinatal outcomes: a retrospective cohort study. J. Clin. Med. 11, 756–767 (2022).
Quistorff, J. L., Saeed, H., Lopez, C., Andescavage, N. N. & Limperopoulos, C. 938 Pregnancy and COVID-19: the impact on maternal mental health. Am. J. Obstet. Gynecol. 224, S582–S583 (2021).
Racine, J. L., Hetzel, S. J., Iruretagoyena, J. I. & Hoppe, K. K. Perinatal outcomes associated with institutional changes early in the COVID-19 pandemic. WMJ 121, 201–204 (2022).
Rao, M. G. et al. Pregnancy during a pandemic: a cohort study comparing adverse outcomes during and before the COVID-19 pandemic. Am. J. Perinatol. 40, 445–452 (2023).
Rasmussen, M. I. et al. Extremely preterm infant admissions within the SafeBoosC-III consortium during the COVID-19 lockdown. Front. Pediatr. 9, 647880 (2021).
Richter, F. et al. Neonatal outcomes during the COVID-19 pandemic in New York City. Pediatr. Res. 91, 477–479 (2022).
Riley, T., Nethery, E., Chung, E. K. & Souter, V. Impact of the COVID-19 pandemic on perinatal care and outcomes in the United States: an interrupted time series analysis. Birth 49, 298–309 (2021).
Roberts, N. F. et al. Maternal-newborn health system changes and outcomes in Ontario, Canada, during wave 1 of the COVID-19 pandemic—a retrospective study. J. Obstet. Gynaecol. Can. 44, 664–674 (2022).
Rolnik, D. L. et al. Impact of COVID-19 pandemic restrictions on pregnancy duration and outcome in Melbourne, Australia. Ultrasound Obstet. Gynecol. 58, 677–687 (2021).
Rusconi, F. et al. Pregnancy outcomes in Italy during COVID-19 pandemic: a population-based cohort study. BJOG 130, 276–284 (2023).
Sangtani, A. et al. 702 Postpartum depression screening during the COVID-19 pandemic. Am. J. Obstet. Gynecol. 224, S440 (2021).
Shah, P. S., Ye, X. Y., Yang, J. & Campitelli, M. A. Preterm birth and stillbirth rates during the COVID-19 pandemic: a population-based cohort study. CMAJ 193, E1164–E1172 (2021).
Shukla, V. V. et al. Association between the COVID-19 pandemic and fetal, neonatal, and maternal outcomes: an Alabama population-based study. J. Invest. Med. 70, 644–645 (2022).
Shukla, V. V. et al. Trends in fetal and neonatal outcomes during the COVID-19 pandemic in Alabama. Pediatr. Res. 94, 756–761 (2023).
Silverman, M. E. et al. Postpartum mood among universally screened high and low socioeconomic status patients during COVID-19 social restrictions in New York City. Sci. Rep. 10, 22380 (2020).
Simeone, R. M. et al. Changes in rates of adverse pregnancy outcomes during the COVID-19 pandemic: a cross-sectional study in the United States, 2019–2020. J. Perinatol. 42, 617–623 (2022).
Simpson, A. N. et al. Perinatal outcomes during the COVID-19 pandemic in Ontario, Canada. JAMA Netw. Open 4, e2110104 (2021).
Sinnott, C. M., Freret, T. S., Clapp, M. A., Reiff, E. & Little, S. E. Investigating decreased rates of nulliparous cesarean deliveries during the COVID-19 pandemic. Am. J. Perinatol. 38, 1231–1235 (2021).
Smorti, M. et al. The impact of COVID-19 restrictions on depressive symptoms in low-risk and high-risk pregnant women: a cross-sectional study before and during pandemic. BMC Pregnancy Childbirth. 22, 191–200 (2022).
Snelgrove, J. W. et al. Preeclampsia and severe maternal morbidity during the COVID-19 pandemic: a population-based cohort study in Ontario, Canada. J. Obstet. Gynaecol. Can. 44, 777–784 (2022).
Speyer, L. G., Marryat, L. & Auyeung, B. Impact of COVID-19 public health safety measures on births in Scotland between March and May 2020. Public Health 202, 76–79 (2022).
Sun, S., Savitz, D. A. & Wellenius, G. A. Changes in adverse pregnancy outcomes associated with the COVID-19 pandemic in the United States. JAMA Netw. Open 4, e2129560 (2021).
Suzuki, S. Psychological status of postpartum women under the COVID-19 pandemic in Japan. J. Matern. Fetal Neonatal Med. 35, 1798–1800 (2020).
Suzuki, S. Psychological status during the first trimester of pregnancy under the COVID-19 epidemic in Japan. J. Matern. Fetal Neonatal Med. 35, 3007–3008 (2020).
Tate, D. et al. Stillbirth during a pandemic: a retrospective cohort study in a high-risk population. Am. J. Obstet. Gynecol. 228, S794 (2023).
Vacaru, S. et al. The risk and protective factors of heightened prenatal anxiety and depression during the COVID-19 lockdown. Sci. Rep. 11, 20261 (2021).
Vitale, E., Galatola, V. & Mea, R. Anxiety and depression levels in post-partum women before and during the COVID-19 pandemic in Italy: an online cross-sectional survey. Minerva Psychiatry 62, 65–73 (2021).
Wagner, M. et al. Perinatal and postpartum care during the COVID-19 pandemic: a nationwide cohort study. Birth 49, 243–252 (2022).
Waschmann, M. et al. Evaluating the impact of the COVID-19 pandemic on postpartum depression. J. Womens Health 31, 772–778 (2022).
Wikarek, A. et al. Does the COVID-19 pandemic affect labor-related anxiety and prevalence of depressive symptoms in pregnant women? J. Clin. Med. 11, 6522–6535 (2022).
Wood, R. et al. Preterm birth during the coronavirus disease 2019 (COVID-19) pandemic in a large hospital system in the United States. Obstet. Gynecol. 137, 403–404 (2021).
Zanardo, V. et al. Psychological impact of COVID-19 quarantine measures in northeastern Italy on mothers in the immediate postpartum period. Int. J. Gynaecol. Obstet. 150, 184–188 (2020).
Zhang, C. X. W. et al. Evaluating depression and anxiety throughout pregnancy and after birth: impact of the COVID-19 pandemic. Am. J. Obstet. Gynecol. 4, 100605 (2022).
Zilver, S. J. M. et al. Stress, anxiety and depression in 1466 pregnant women during and before the COVID-19 pandemic: a Dutch cohort study. J. Psychosom. Obstet. Gynaecol. 42, 108–114 (2021).
Ohashi, M. et al. Amelioration of prevalence of threatened preterm labor during the COVID-19 pandemic: nationwide database analysis in Japan. Sci. Rep. 12, 15345 (2022).
Ibrahim, B. et al. Impact of pandemic service changes on ethnic inequalities in maternal and perinatal outcomes in England: a population-based study. BMJ Open 15, e090359–e090368 (2025).
Maeda, Y. et al. Trends in intensive neonatal care during the COVID-19 outbreak in Japan. Arch. Dis. Child Fetal Neonatal Ed 106, 327–329 (2021).
Morgan, A. S., Bradford, C., Farrow, H., Draper, E. S. & Harrison, C. Effects of the SARS-CoV-2 pandemic on perinatal activity in Yorkshire and the Humber region during 2020: an interrupted time series analysis. Arch. Dis. Child Fetal Neonatal Ed. https://doi.org/10.1136/archdischild-2021-323466 (2022).
Stansfield, S., Rattan, A., Mol, B. W., Rolnik, D. L. & Malhotra, A. Impact of the COVID-19 pandemic and multiple community lockdowns on total live birth rates and preterm births in Melbourne, Australia. Aust. N. Z. J. Obstet. Gynaecol. 62, 786–789 (2022).
Stumpfe, F. M. et al. Lack of evidence for effects of lockdowns on stillbirth rates during the SARS-CoV-2 pandemic in Bavaria: analysis of the Bavarian perinatal survey from 2010 to 2020. Arch. Gynecol. Obstet. 308, 1457–1462 (2022).
Floyd, R. L., Rimer, B. K., Giovino, G. A., Mullen, P. D. & Sullivan, S. E. A review of smoking in pregnancy: effects on pregnancy outcomes and cessation efforts. Annu. Rev. Public Health 14, 379–411 (1993).
Green, J., Petty, J., Whiting, L. & Fowler, C. Exploring modifiable risk-factors for premature birth in the context of COVID-19 mitigation measures: a discussion paper. J. Neonatal Nurs. 27, 172–179 (2021).
Better for Women: Improving the Health and Wellbeing of Girls and Women (Royal College of Obstetricians & Gynaecologists, 2019).
Hogue, C. J. R., Hoffman, S. & Hatch, M. C. Stress and preterm delivery: a conceptual framework. Paediatr. Perinatal Epidemiol. 15, 30–40 (2001).
Hollowell, J., Kurinczuk, J. J., Brocklehurst, P. & Gray, R. Social and ethnic inequalities in infant mortality: a perspective from the United Kingdom. Semin. Perinatol. 35, 240–244 (2011).
Jones, G. L., Mitchell, C. A., Hirst, J. E. & Anumba, D. O. C. Understanding the relationship between social determinants of health and maternal mortality: Scientific Impact Paper No. 67. BJOG 129, 1211–1228 (2022).
Katz, V. L. Work and work-related stress in pregnancy. Clin. Obstet. Gynecol. 55, 765–773 (2012).
Stieb, D. M., Chen, L., Eshoul, M. & Judek, S. Ambient air pollution, birth weight and preterm birth: a systematic review and meta-analysis. Environ. Res. 117, 100–111 (2012).
Bailey, Z. D. et al. Structural racism and health inequities in the USA: evidence and interventions. Lancet 389, 1453–1463 (2017).
Adams-Prassl, A., Boneva, T., Golin, M. & Rauh, C. Inequality in the impact of the coronavirus shock: evidence from real time surveys. J. Public Econ. 189, 104245 (2020).
Jardine, J. et al. Maternity services in the UK during the coronavirus disease 2019 pandemic: a national survey of modifications to standard care. BJOG 128, 880–889 (2021).
Jephcote, C., Hansell, A. L., Adams, K. & Gulliver, J. Changes in air quality during COVID-19 ‘lockdown’ in the United Kingdom. Environ. Pollut. 272, 116011 (2021).
McKinlay, A. R., Simon, Y. R., May, T., Fancourt, D. & Burton, A. How did UK social distancing restrictions affect the lives of women experiencing intimate partner violence during the COVID-19 pandemic? A qualitative exploration of survivor views. BMC Public Health 23, 123–140 (2023).
Francis-Devine, B., Powell, A. & Clark, H. Coronavirus: Impact on the Labour Market (House of Commons Library, 2022).
Seedat, S. & Rondon, M. Women’s wellbeing and the burden of unpaid work. BMJ 374, n1972 (2021).
Xue, B. & McMunn, A. Gender differences in unpaid care work and psychological distress in the UK COVID-19 lockdown. PLoS ONE 16, e0247959 (2021).
Saunders, C. L., Abel, G. A., Turabi, A. E., Ahmed, F. & Lyratzopoulos, G. Accuracy of routinely recorded ethnic group information compared with self-reported ethnicity: evidence from the English Cancer Patient Experience survey. BMJ Open 3, e002882 (2013).
Townsend, R. et al. Global changes in maternity care provision during the COVID-19 pandemic: a systematic review and meta-analysis. eClinicalMedicine 37, 100947 (2021).
Iyengar, U., Jaiprakash, B., Haitsuka, H. & Kim, S. One year into the pandemic: a systematic review of perinatal mental health outcomes during COVID-19. Front. Psychiatry 12, 674194 (2021).
Almeida, M., Shrestha, A. D., Stojanac, D. & Miller, L. J. The impact of the COVID-19 pandemic on women’s mental health. Arch. Womens Ment. Health 23, 741–748 (2020).
Thomson, K. et al. Socioeconomic inequalities and adverse pregnancy outcomes in the UK and Republic of Ireland: a systematic review and meta-analysis. BMJ Open 11, e042753 (2021).
COVID Maternity Equality Project (CMEP). October 2022. RCOG https://www.rcog.org.uk/about-us/quality-improvement-clinical-audit-and-research-projects/covid-maternity-equality-project-cmep/ (2023).
World Bank country and lending groups. World Bank https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (2023).
Wells, G. A. Newcastle–Ottawa quality assessment form for cohort studies. NCBI https://www.ncbi.nlm.nih.gov/books/NBK115843/bin/appe-fm3.pdf (2021).
Deeks, J. J., Higgins, J. P. T., Altman, D. G., McKenzie, J. E. & Veroniki, A. A. in Cochrane Handbook for Systematic Reviews of Interventions (eds Higgins J. T. et al.) Ch. 10 (Cochrane, 2022).
Ochoa, L. B., Brockway, M., Stock, S. J. & Been, J. V. COVID-19 and maternal and perinatal outcomes. Lancet Global Health 9, e1063–e1064 (2021).
What Study Designs Can Be Considered for Inclusion in an EPOC Review and What Should They Be Called? (Cochrane Effective Practice and Organisation of Care (EPOC), 2017).
Faber, T. et al. Effect of tobacco control policies on perinatal and child health: a systematic review and meta-analysis. Lancet Public Health 2, e420–e437 (2017).
Acknowledgements
We thank the funder of this project, the National Institute of Health Research: School of Primary Care Research (grant number SPCR C007) and Tommy’s National Preterm Birth Research Centre.
Author information
Authors and Affiliations
Contributions
I.H., S.I. and D.Z. conceptualized the study aims, study design, inclusion and exclusion criteria and data curation. I.H., H.N.S. and B.Y.G. conducted data searches and independent screening of studies. I.H. and H.N.S. conducted data extraction. I.H. was responsible for data organization and analysis. S.I. and D.Z. participated in and advised study selection, data analysis and visualization. I.H., J.V.B. and L.B.-O. conceptualized and provided input on secondary nested time-adjusted analysis, including providing input on study selection, data organization, analysis and visualization. I.H. wrote all drafts of the paper with input from J.J., S.I., D.Z., J.V.B. and L.B.-O. All authors had full access to all the data in the study and agreed to submit for publication. I.H., S.I., D.Z. and L.B.-O. have accessed and verified the data included in meta-analysis.
Corresponding author
Ethics declarations
Competing interests
J.J. was a co-author of the Royal College of Obstetrics and Gynecology (RCOG) guidelines, which determined changes to maternity care during the COVID-19 pandemic. The other authors declare no competing interests.
Peer review
Peer review information
Nature Human Behaviour thanks John Allotey, Emma Miller and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Peer reviewer reports are available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary Information (download PDF )
Supplementary Material 1–3 (materials related to the methodology). Supplementary Material 1. Outcome definitions. Supplementary Material 2. Search term. Supplementary Material 3. Details regarding the deprivation indicator variable. Supplementary Material 4. Table of included studies. Supplementary Material 5. Table of included studies (time-adjusted analysis). Supplementary Material 6. PRISMA flowchart. Supplementary Material 7–9 (supplementary results). Results and analyses of outcomes’ subclassifications and subgroup analysis by region. Supplementary Material 8. Investigation of publication bias. Supplementary Material 9. Investigation of power and minimum detectable effects. Supplementary Material 10 and 11 (supplementary methods information). List of excluded studies from meta-analysis and full text screening. Supplementary Material 12. PRISMA checklist (information relevant to discussion). Supplementary Material 13. List of supplementary figures titles and captions. Supplementary Figs. 1–15.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hindes, I., Sarwar, H.N., Gravesteijn, B.Y. et al. The association of COVID-19 lockdowns with adverse birth and pregnancy outcomes in 28 high-income countries: a systematic review and meta-analysis. Nat Hum Behav 9, 1420–1430 (2025). https://doi.org/10.1038/s41562-025-02139-z
Received:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41562-025-02139-z
